Introduction
Recently, endovascular therapy has been proved as a
safe alternative treatment strategy to surgical clipping for
several intracranial aneurysms. However, in the field of middle
cerebral artery (MCA) aneurysms, microsurgery remains superior to
endovascular therapy, as these aneurysms are easily accessible and
may be safely manipulated following splitting of the sylvian
fissure (1-3).
Furthermore, MCA aneurysms frequently have broad necks and branches
often originate from the wall of the aneurysm, which may contribute
to a higher risk of recurrence or retreatment with coiling and
unintended occlusions with stent-assisted coiling (4,5).
Complex MCA aneurysms, accounting for 4-17.4% of all
MCA aneurysms, including aneurysms that are sizeable (large or
giant), fusiform, wide-necked or feature intraluminal thrombi or
incorporation of branches, remain a significant challenge to
microsurgical clipping or endovascular coiling (6). Previous studies indicated that
patients with complex MCA aneurysms had a mortality rate of 65-85%
within 2 years due to rupture or re-rupture. Furthermore, survivors
are frequently left with severe neurological deficits (7,8).
Complex MCA aneurysms are technically difficult to manage and a
subset of them require management with bypass techniques as part of
a treatment strategy with deliberate occlusion of a parent artery
(9-13).
Bypass techniques for MCA aneurysms include
extracranial-to-intracranial (EC-IC) bypass, which comprises
low-flow superficial temporal artery (STA)-M3 (or M4) bypass and
high-flow external carotid artery-radial artery graft-M2
(ECA-RAG-M2) bypass, and intracranial-to-intracranial (IC-IC)
bypass, including end-to-end reanastomosis, interpositional bypass,
side-to-side anastomosis and reimplantation techniques. A study
comprising 1,426 MCA aneurysms demonstrated that only 2.1% of MCA
aneurysms required bypasses (14).
To date, however, only a small number of studies have focused on
cerebral revascularization for the treatment of complex MCA
aneurysms (14-17).
The present study reports on microsurgical treatment strategies for
complex MCA aneurysms.
Materials and methods
Study design and patient
selection
The protocol of the present study was approved by
the Institutional Review Board and Ethics committee of The First
Affiliated Hospital of Soochow University (Suzhou, China). The
medical records of all patients with complex MCA aneurysm treated
using revascularization between August 2012 and December 2019 at
The First Affiliated Hospital of Soochow University (Suzhou, China)
were retrospectively reviewed. Complex MCA aneurysms were defined
as those having been previously reported in the literature,
including MCA aneurysms with a non-saccular morphology (dissecting,
serpentine or fusiform) or with a large (10-24 mm in diameter) or a
giant size (≥25 mm in diameter) or aberrant branch arteries arising
from the side wall of the aneurysms (14). These aneurysms were considered
complex when traditional treatment methods, such as clipping,
stenting or coiling, were considered to be associated with high
treatment risks. The patients' demographic and clinical data were
reviewed, including patient age and sex, aneurysm characteristics
(size, location and morphology), operative records, preoperative
and postoperative images, complications, clinical outcomes and
follow-up.
Surgical strategy
According to their locations, the aneurysms were
divided into three subtypes: i) Prebifurcation; ii) bifurcation;
and iii) postbifurcation. It was not possible to treat any of the
MCA aneurysms included in the present study with direct clipping or
clip reconstruction alone. The bypass types used in the present
study were determined according to the preoperative aneurysm
characteristics. The IC-IC bypass included the following subtypes:
i) Reanastomosis (where the aneurysm was treated by excision and
the arterial ends were sutured end-to-end); ii) interpositional
bypass (where the aneurysm was excised and transected arterial ends
were sutured with placement of an interposed graft); iii)
reimplantation (with an end-to-side anastomosis between the
transected end of the efferent artery of the aneurysm and an
adjacent parallel donor artery) (6). The EC-IC bypass included STA-M3 (or
M4) bypass (low-flow bypass) and the ECA-RAG-M2 bypass (high-flow
bypass) (18).
The treatment strategy for each patient was
determined by neurovascular surgeons and endovascular specialists,
according to the aneurysm morphology, location, size and vascular
anatomy. For aneurysms that lacked perforating arteries in the
aneurysm dome, clip trapping the parent vessel with bypass was the
preferred strategy. If there were perforating arteries
[particularly the lenticulostriate artery (LSA)] arising from the
aneurysm dome, these lesions were treated by proximal parent vessel
occlusion with revascularization or clip reconstruction. The
patency of the parent vessel and bypass were assessed by
intra-operative Doppler flow probes and indocyanine green (ICG)
angiography.
Imaging analysis and follow-up
Angiographic follow-up was performed using computed
tomography (CT) angiography or digital subtraction angiography
(DSA) to assess the bypass patency and aneurysm status 6 months
postoperatively. The pre- and postoperative neurological outcomes
(at 3, 6 and 12 months postoperatively) were assessed by the same
author using the modified Rankin Scale (mRS) score (19).
Results
Patient characteristics
During a 7-year period between August 2012 and
December 2019, 13 patients with 15 complex MCA aneurysms were
surgically treated at The First Affiliated Hospital of Soochow
University (Suzhou, China) (Table
I). A total of 7 males and 6 females were included in the
present study with an average age of 39.0 years (range, 13-65
years). In total, four patients presented with subarachnoid
hemorrhage (SAH), of which three patients were Hunt and Hess grade
II, and one patient was Hunt and Hess grade IV (20). Other presenting symptoms included
headache, dizziness and epilepsy. Furthermore, one patient
presented with a giant recurrent thrombotic aneurysm after a
primary microsurgical clipping 8 years previously. The mean
pretreatment mRS score was 1.4 (range, 1-5).
 | Table IClinical characteristics of the
patients with complex middle cerebral artery aneurysms treated by
cerebral revascularization (n=13). |
Table I
Clinical characteristics of the
patients with complex middle cerebral artery aneurysms treated by
cerebral revascularization (n=13).
| Case no. | Sex/age (years) | Location of
aneurysm | Rupture | Size (mm) | mRS score
(preoperative) | Aneurysm
treatment | Bypass patency | mRS
scorea
(postoperative) |
|---|
| 1 | M/27 | R-M1 | No | 26 | 1 | PO, ECA-RAG-M2 bypass
(high flow) | Patent | 2 |
| 2 | M/37 | R-M1, R-M2 | No | 16, 9 | 1 | PO, ECA-RAG-M3 bypass
(high flow) | Patent | 1 |
| 3 | M/30 | R-M1 | No | 26.5 | 1 | PO, ECA-RAG-M2 bypass
(high flow) | Occluded | 1 |
| 4 | F/23 | L-M1, L-M2 | No | 18.1, 18.0 | 1 | PO, STA-M4, double
bypass (low flow) | Patent | 1 |
| 5 | M/57 | L-M1 | No | 10 | 1 | PO, STA-M4, double
bypass (low flow) | Patent | 0 |
| 6 | F/48 | L-M1 | Yes | 10.7 | 2 (H&H: II) | Clip
reconstruction+STA-M2 bypass (high flow) | Patent | 0 |
| 7 | F/50 | R-M3 | No | 15 | 1 | Excision, M3-STA-M3
interpositional bypass | Patent | 0 |
| 8 | F/51 | R-M3 | No | 29 | 1 | Excision, STA-M3
bypass (low flow) | Patent | 0 |
| 9 | F/49 | R-M3 | Yes | 3.9 | 1 (H&H:
II) | Excision, M3-M3
reanastomosis | Patent | 0 |
| 10 | M/13 | L-M2 | Yes | 10.5 | 1 (H&H:
II) | Trapping, M3-M2
reimplantation | Patent | 1 |
| 11 | M/17 | R-M1 | Yes | 35 | 5 (H&H:
IV) | Trapping,
ECA-RAG-M2 bypass (high flow) | Patent | 3 |
| 12 | F/40 | R-M3 | No | 20.0 | 1 | Excision, STA-M3
bypass (low flow) | Patent | 0 |
| 13 | F/65 | R-M2 | No | 15 | 1 | Excision, STA-M2
bypass (high flow) | Patent | 1 |
The mean size of the 15 aneurysms was 17.5 mm, with
a range of 3.9-35.0 mm. The locations of these aneurysms were
classified as pre-bifurcation in three patients (20.0%),
bifurcation in five patients (33.3%) and postbifurcation in seven
patients (46.7%).
Treatment with cerebral
revascularization
All of the aneurysms were exposed through pterional
craniotomy and a transsylvian approach (14). In total, seven aneurysms were
managed by proximal occlusion of the parent artery, seven were
managed by trapping and excision and one was managed by clip
reconstruction plus partial occlusion. In total, 10 patients
underwent EC-IC bypass, including six STA-MCA bypasses and four
ECA-RAG-MCA bypasses. The IC-IC bypass treatments included one
reanastomosis, one interpositional bypass and one
reimplantation.
Surgical results and follow-up
No mortality occurred as a result of surgery. The
mean follow-up time was 28.3 months (range, 9-97 months). The mean
mRS score was 0.8 (range, 0-3) at 3 months postoperatively. The
condition of all patients either improved or was equal to that of
the preoperative state except for one patient, whose postoperative
mRS score increased from 1 to 2 (Table
I). In total, 92.3% of the bypasses (12/13) were patent, which
was confirmed by postoperative angiography at 6 months
postoperatively. The angiographic images indicated that 9 of the 10
EC-IC bypasses were patent (90.0%) and the IC-IC bypass was patent
in all patients at follow-up. The bypass was occluded in one
patient, which was indicated by the angiography at 6 months
postoperatively. However, the aneurysm almost disappeared and there
were no neurological deficits. Thus, no further treatment was
needed for this patient. There was no recurrence or mortality
during the follow-up period.
Illustrative cases
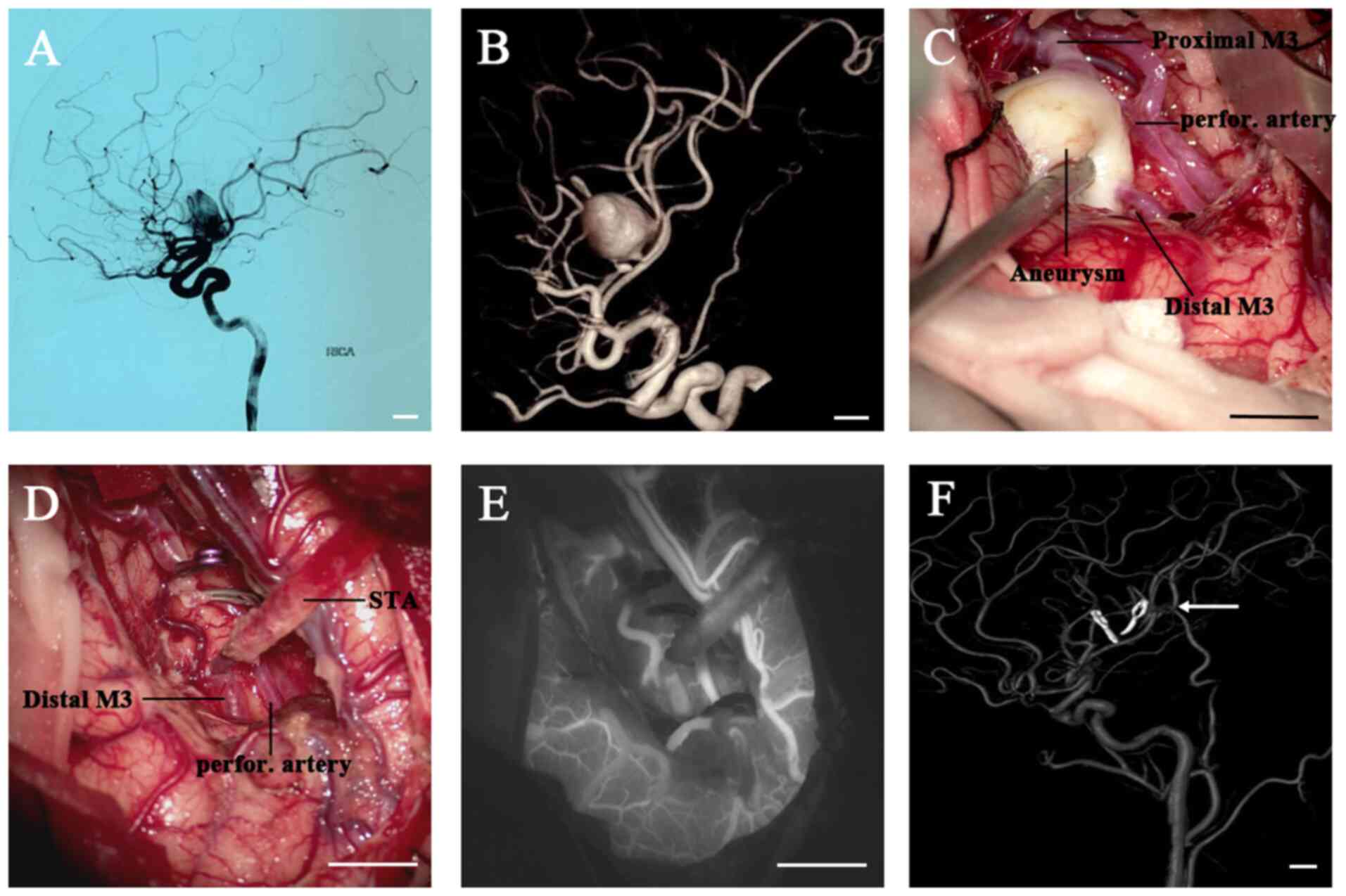
Case I. A 40-year-old female presented with
headache (Fig. 1; case 12 in
Table I). A CT scan revealed a
space-occupying lesion in the right sylvian fissure. The CT scan
and angiography (CTA) and DSA results revealed the presence of a
giant fusiform aneurysm originating from the right M3 segment
(diameter, 20.0 mm) (Fig. 1A). The
subsequent 3D reconstructive DSA indicated that the aneurysm had
one afferent artery (proximal M3) and two efferent arteries (the
distal M3 and a small perforating artery arising from the aneurysm
dome) (Fig. 1B), which was
confirmed during the operation. (Fig.
1C) The aneurysm was exposed using the right pterional
approach. Following STA-M3 end-to-end anastomosis, the proximal and
distal M3 segment were temporarily occluded. Since aneurysm
excision was impossible without sacrificing the small perforating
artery arising from the aneurysm, intra-operative ICG
videoangiography was used to determine whether there was any
collateral circulation to provide an adequate blood supply for the
perforating artery (Fig. 1D). ICG
videoangiography revealed simultaneous filling of the distal M3 and
the perforating arteries for this patient (Fig. 1E), indicating sufficient blood
supply. Therefore, the aneurysm was resected and no further
processing was necessary. After the surgery, the patient was free
of any neurological deficits and the postoperative DSA demonstrated
a patent bypass and complete exclusion of the aneurysm (6 months
after the operation) (Fig. 1F).
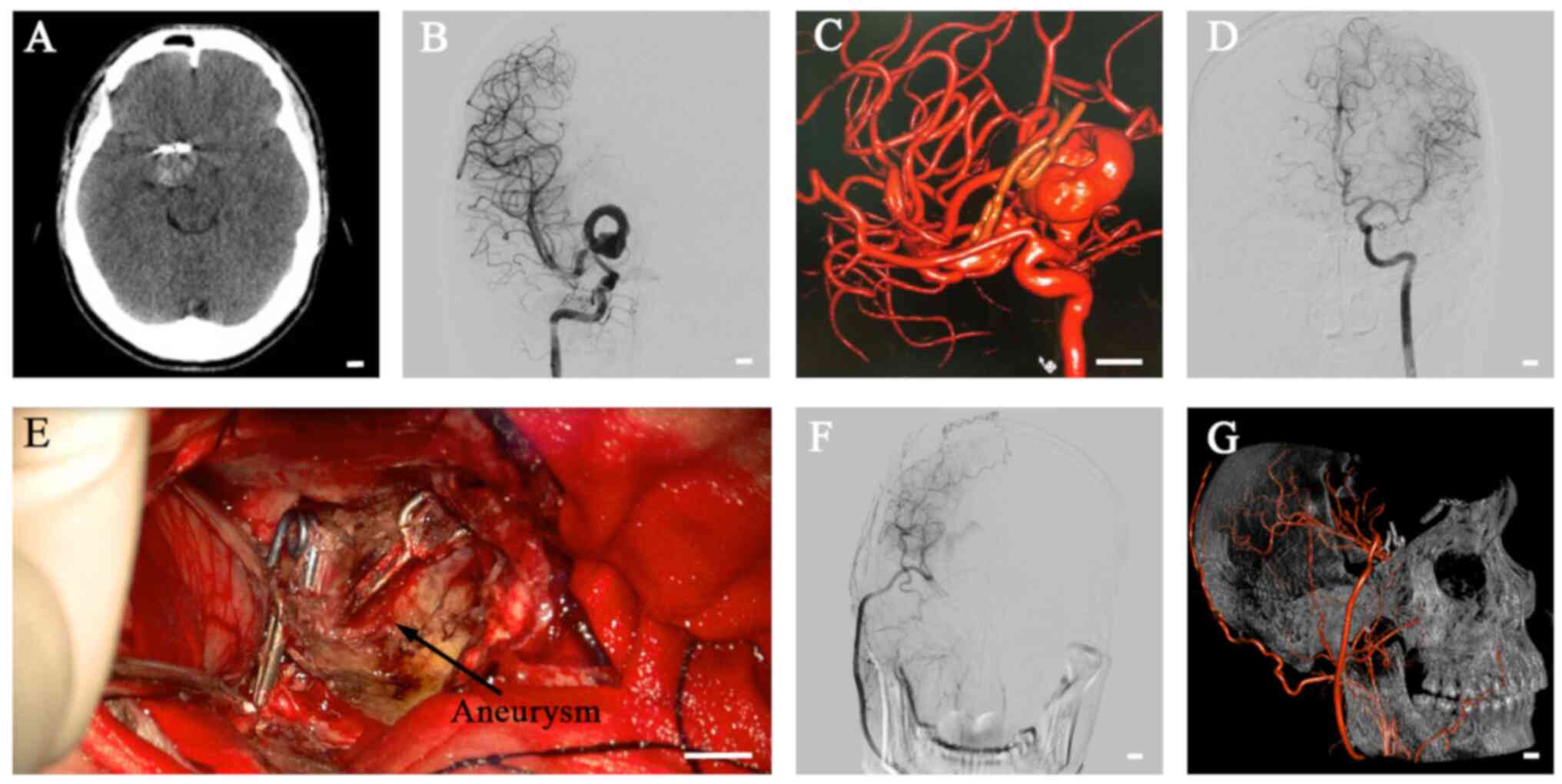
Case II. A 27-year-old male suffered from
numbness of the left limbs for 1 month and had received
microsurgical clipping of a right MCA aneurysm 8 years previously
(Fig. 2; case 1 in Table I). A CT scan revealed a giant lesion
in the right front-temporal lobe (Fig.
2A). A subsequent DSA assessment demonstrated a giant recurrent
thrombotic aneurysm originating from the right M1 segment and
direct clipping or endovascular treatment was therefore impossible
(Fig. 2B-D). The aneurysm was
treated with proximal occlusion and a right ECA-RA-M2 bypass was
performed to supply retrograde flow to the non-bypassed M2 artery
and LSA (Fig. 2E). Intraoperative
ICG videoangiography and Doppler ultrasonography confirmed the
patency of the bypass. The postoperative DSA demonstrated complete
obliteration of the aneurysm (Fig.
2F and G). However, the
postoperative mRS score increased from 1 (preoperative) to 2
(postoperative) with decreased myodynamia of the right limb, which
may have occurred since the ECA-RA-M2 bypass was not able to
sufficiently support the MCA territory.
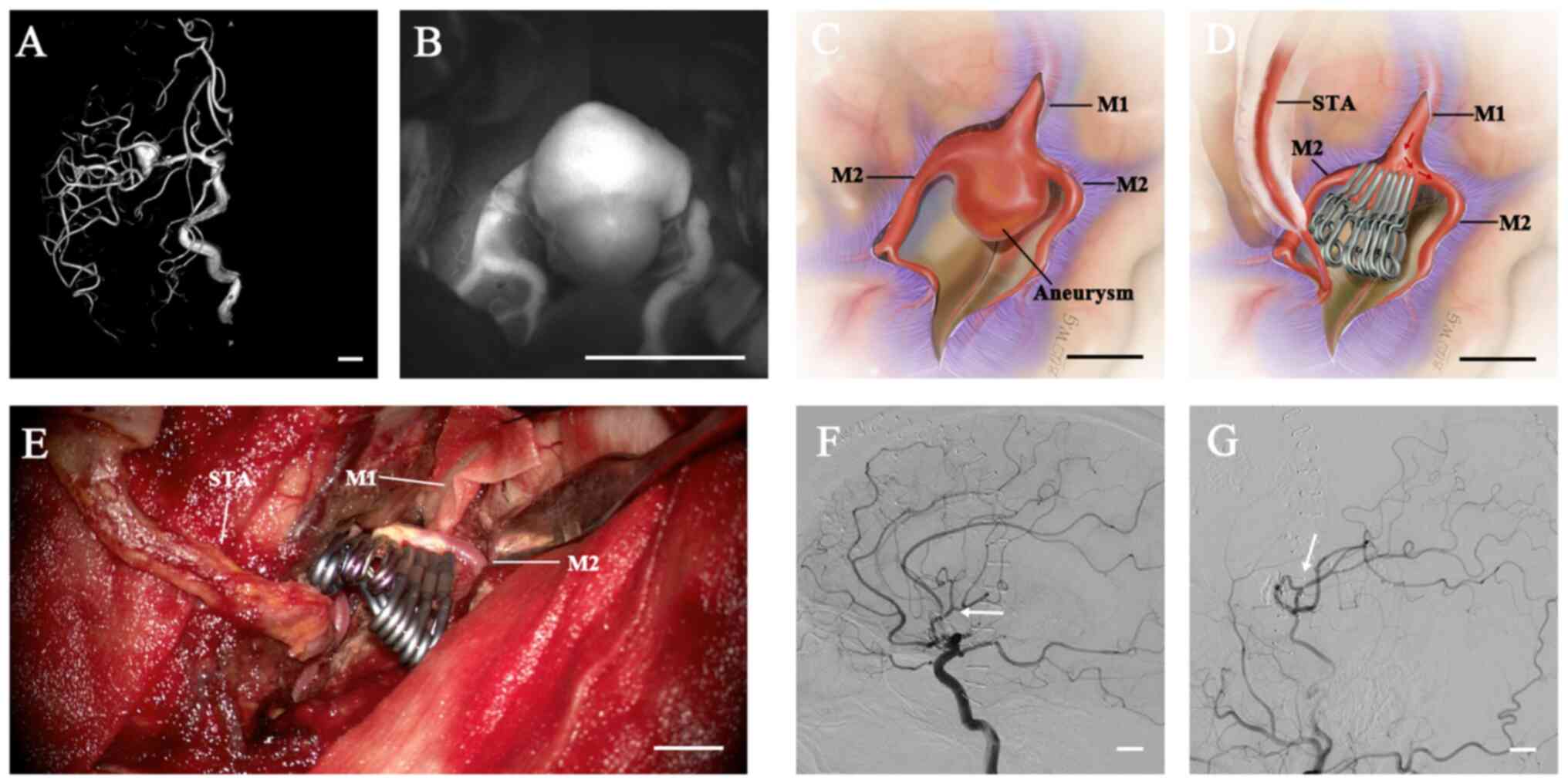
Case III. A 48-year-old female presented with
a sudden headache and was referred to our department (Fig. 3; case 6 in Table I). A CT scan revealed SAH in the
right sylvian fissure. The CTA and DSA analyses revealed a fusiform
aneurysm originating from the left M1 bifurcation (Fig. 3A). After the aneurysm had been
exposed, the intraoperative observation was that the inferior M2
trunk had arisen from the aneurysm, making direct clipping
impossible. The superior M2 trunk was not involved in the neck of
the aneurysm (Fig. 3B-D). Following
temporary occlusion, the aneurysm was opened, the aneurysmal neck
was completely transected to simplify the clipping and the
intraluminal thrombus was removed. Tandem clipping with stacked
straight fenestrated clips was applied to reconstruct the MCA
bifurcation and preserve the superior trunk. A straight clip was
used to completely obliterate the aneurysm between the M1 segment
and inferior trunk and an STA-M2 bypass was performed to supply
anterograde flow to the inferior trunk (Fig. 3E). The patient recovered well
without any neurological deficits. Postoperative DSA demonstrated
complete occlusion of the aneurysm, a reconstructive superior M2
trunk and patency of the STA-M2 (inferior) bypass (Fig. 3F and G).
Discussion
MCA aneurysms have long been considered favorable
for clipping since they are easily accessible followed by splitting
of the sylvian fissure. Complex MCA aneurysms usually possess
unfavorable features, including intraluminal thrombi, fusiform
configurations, mural calcifications and the incorporation of
branches (21-23).
These features limit the feasibility of direct clipping or
endovascular coiling alone. In the present study, various cerebral
revascularization techniques used to treat complex MCA aneurysms
during a 7-year period were described. The analysis of 13 patients
with complex MCA aneurysms revealed that the patency rate was 92.3%
and 12 of 13 aneurysms were removed from the circulation. All
patients had a favorable outcome (mRS ≤2) at the last
follow-up.
Several surgical techniques have been reported for
the treatment of complex MCA aneurysms, including clip
reconstruction, aneurysmal excision with a reanastomosis, proximal
occlusion or surgical trapping with or without cerebral
revascularization (11,14,17,18).
Clip reconstruction is a commonly used direct occlusion strategy
for the treatment of complex MCA aneurysm with broad necks or giant
size and this is mediated through molding the neck, shrinking the
aneurysm with low-flow electrocoagulation or reconstructing the
efferent arteries (24,25). In the present study, a giant
fusiform aneurysm located in the M1 bifurcation was managed with
clip reconstruction and EC-IC bypass. Tandem clipping with stacked
straight fenestrated clips was used to reconstruct the M1/superior
M2 antegrade tube and STA-M2 bypass was applied to supply
anterograde flow to the inferior M2 trunk (case III). However, clip
reconstruction was impossible to perform in the majority of cases
of the present study, since most complex MCA aneurysms had a
dolichoectatic morphology or atherosclerotic necks.
Indirect occlusion with or without cerebral
revascularization remains the most important treatment strategy for
complex MCA aneurysms, which includes aneurysmal trapping,
aneurysmal excision, proximal occlusion or distal occlusion of the
parent artery. Complete trapping, exclusion of the aneurysm and the
total arterial territory may result in ischemic complications when
perforating arteries arise from the aneurysm. Therefore, complete
trapping or excision of the aneurysm plus IC-IC or EC-IC bypass is
an appropriate surgical strategy for the treatment of complex MCA
aneurysms located in the distal segment of the MCA and that lack
aberrant branch arteries or perforating arteries arising from the
aneurysm. In the present study, three patients were treated with
aneurysm trapping or excision followed by IC-IC bypass, of which
two aneurysms were treated by excision combined with M3-M3
reanastomosis or M3-STA-M3 reanastomosis, respectively. The other
one was treated with trapping and M3-M2 reimplantation.
Previous studies suggested that IC-IC bypass has
aneurysm obliteration rates, bypass patency rates and complication
rates similar to those of EC-IC bypass (26). However, anatomical constraints, such
as an aneurysm in the insular recess, may limit the IC-IC bypass
option (27). In addition, IC-IC
bypass is generally suitable for distally located aneurysms, as the
large hemispheric territory supplied by the MCA requires high-flow
bypass in prebifurcation or bifurcation aneurysms (27). EC-IC bypass is also a
well-established strategy for the treatment of complex aneurysms.
It is appropriate for pre-bifurcation and bifurcation MCA aneurysm,
as, unlike a distal efferent artery in postbifurcation aneurysm, a
proximal efferent artery calls for high flow (27). In the present study, 10 patients
were treated with proximal occlusion of the parent artery, trapping
or excision of aneurysms combined with EC-IC bypass, including 4
ECA-RAG-MCA bypasses and 6 STA-MCA bypasses.
Complete trapping or excision of the aneurysm may be
the best strategy for treating aneurysms free of perforating
vessels (6). However, in complex
MCA aneurysms, the aneurysm cannot be trapped or excised when the
LSA or aberrant branch arteries originate from the aneurysm and in
these cases, proximal occlusion is performed instead. In the
present study, six complex MCA aneurysms were managed with proximal
occlusion of the parent artery plus bypass. Proximal occlusion, a
subtype of partial trapping, is able to reduce the flow through the
aneurysm to facilitate intra-aneurysmal thrombosis and the bypass
provides anterograde flow to the recipient trunk and retrograde
blood flow for the perforators (18). Despite the perforating arteries, the
rupture status of the aneurysm also affects the type of parent
arterial occlusion. Ruptured MCA aneurysms should be excluded
completely with direct neck clipping or trapping together with
EC-IC/IC-IC bypass when clipping is impossible, since retrograde
filling of a ruptured aneurysm may lead to rerupture of the
aneurysm (18).
Recently, flow diversion devices have been reported
as an alternative endovascular treatment for complex MCA aneurysms.
Cimflova et al (28)
reported that the complete/near-complete occlusion rate was 70% in
consecutive subjects with 23 MCA aneurysms. Potentially severe
periprocedural or postprocedural events occurred in 17.4% of the
patients and severe complications (intraparenchymal hemorrhage and
rerupture of the aneurysm) occurred in half of those patients
(8.7%), which was consistent with previous studies (29,30).
Furthermore, the requirement for antiplatelet agents limits their
applicability in patients with a history of SAH. However, managing
complex MCA aneurysms with a combined approach of coil embolization
following protective EC-IC bypass has been reported in a recent
study (31), which may provide an
alternative treatment strategy for complex MCA aneurysms,
particularly when surgical trapping or proximal occlusion is
impossible due to anatomic limitations.
Of note, the present study had certain limitations.
First, the results are limited since the experience reported was
from a single surgeon at a single center, which may not be
representative of generalized neurosurgical results. Moreover, the
follow-up period of the present study was relatively short, and the
surgical strategies were based to the limited number of
patients.
In conclusion, surgical treatment strategies for
complex MCA aneurysm should depend on the status and
characteristics of the aneurysm, including aneurysm size, location
and morphology, and particularly the involvement of perforating
arteries. Favorable outcomes may be achieved with appropriate
surgical strategies.
Acknowledgements
Not applicable.
Funding
Funding: This work is supported by the National Natural Science
Foundation of China (grant no. 81601064). The funders had no role
in the preparation of this study or interpretation of the
results.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
YH, PZ and XL contributed to surgical treatment and
drafted the manuscript. WZ performed endovascular interventions.
PZ, XL, GC and ZW participated in case management, data extraction
and data analysis. YH and XL confirmed the authenticity of the raw
data. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
All procedures performed in studies involving human
participants were in accordance with the ethical standards of the
First Affiliated Hospital of Soochow University (Suzhou, China) and
with the 1964 Helsinki declaration and its later amendments or
comparable ethical standards. Written informed consent was obtained
from the participants.
Patient consent for publication
The patients provided consent for publication. There
were two patients under the legal age of consent and consent was
obtained from their parents.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Smith TR, Cote DJ, Dasenbrock HH, Hamade
YJ, Zammar SG, El Tecle NE, Batjer HH and Bendok BR: Comparison of
the efficacy and safety of endovascular coiling versus
microsurgical clipping for unruptured middle cerebral artery
aneurysms: a systematic review and meta-analysis. World Neurosurg.
84:942–953. 2015.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Diaz OM, Rangel-Castilla L, Barber S, Mayo
RC, Klucznik R and Zhang YJ: Middle cerebral artery aneurysms: A
single-center series comparing endovascular and surgical treatment.
World Neurosurg. 81:322–329. 2014.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Steklacova A, Bradac O, Charvat F, De Lacy
P and Benes V: ‘Clip first’ policy in management of intracranial
MCA aneurysms: Single-centre experience with a systematic review of
literature. Acta Neurochir (Wien). 158:533–546; discussion 546.
2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Lu P, Zhang Y, Niu H and Wang Y:
Comparison of endovascular treatment for middle cerebral artery
aneurysm with a low-profile visualized intraluminal support stent
or pipeline embolization device. Exp Ther Med. 18:2072–2078.
2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Jeong SM, Kang SH, Lee NJ and Lim DJ:
Stent-assisted coil embolization for the proximal middle cerebral
artery fusiform aneurysm. J Korean Neurosurg Soc. 47:406–408.
2010.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Nussbaum ES, Kallmes KM, Lassig JP,
Goddard JK, Madison MT and Nussbaum LA: Cerebral revascularization
for the management of complex intracranial aneurysms: A
single-center experience. J Neurosurg: Oct 1, 2018 (Epub ahead of
print).
|
|
7
|
Choi IS and David C: Giant intracranial
aneurysms: Development, clinical presentation and treatment. Eur J
Radiol. 46:178–194. 2003.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Drake CG and Peerless SJ: Giant fusiform
intracranial aneurysms: Review of 120 patients treated surgically
from 1965 to 1992. J Neurosurg. 87:141–162. 1997.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Fulkerson DH, Voorhies JM, Payner TD,
Leipzig TJ, Horner TG, Redelman K and Cohen-Gadol AA: Middle
cerebral artery aneurysms in children: Case series and review. J
Neurosurg Pediatr. 8:79–89. 2011.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Quiñones-Hinojosa A and Lawton MT: In situ
bypass in the management of complex intracranial aneurysms:
Technique application in 13 patients. Neurosurgery. 57 (Suppl
1):140–145; discussion 140-145. 2005.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Sekhar LN, Stimac D, Bakir A and Rak R:
Reconstruction options for complex middle cerebral artery
aneurysms. Neurosurgery. 56 (Suppl 1):66–74; discussion 66-74.
2005.PubMed/NCBI View Article : Google Scholar
|
|
12
|
van Doormaal TP, van der Zwan A, Verweij
BH, Han KS, Langer DJ and Tulleken CA: Treatment of giant middle
cerebral artery aneurysms with a flow replacement bypass using the
excimer laser-assisted nonocclusive anastomosis technique.
Neurosurgery. 63:12–20; discussion 20-22. 2008.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Aboukais R, Verbraeken B, Leclerc X,
Gautier C, Vermandel M, Bricout N, Lejeune JP and Menovsky T:
Protective STA-MCA bypass to prevent brain ischemia during
high-flow bypass surgery: Case series of 10 patients. Acta
Neurochir (Wien). 161:1207–1214. 2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Tayebi Meybodi A, Huang W, Benet A, Kola O
and Lawton MT: Bypass surgery for complex middle cerebral artery
aneurysms: An algorithmic approach to revascularization. J
Neurosurg. 127:463–479. 2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Lan J, Fu ZY, Zhang JJ, Ma C, Cao CJ, Zhao
WY, Jiang PC and Chen JC: Giant serpentine aneurysm of the middle
cerebral artery. World Neurosurg. 117:109–114. 2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Kivipelto L, Niemelä M, Meling T, Lehecka
M, Lehto H and Hernesniemi J: Bypass surgery for complex middle
cerebral artery aneurysms: Impact of the exact location in the MCA
tree. J Neurosurg. 120:398–408. 2014.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Wang L, Lu S, Cai L, Qian H, Tanikawa R
and Shi X: Internal maxillary artery bypass for the treatment of
complex middle cerebral artery aneurysms. Neurosurg Focus.
46(E10)2019.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Xu F, Xu B, Huang L, Xiong J, Gu Y and
Lawton MT: Surgical Treatment of Large or Giant Fusiform Middle
Cerebral Artery Aneurysms: A Case Series. World Neurosurg.
115:e252–e262. 2018.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Banks JL and Marotta CA: Outcomes validity
and reliability of the modified Rankin scale: implications for
stroke clinical trials: a literature review and synthesis. Stroke.
38:1091–1096. 2007.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Konczalla J, Seifert V, Beck J, Güresir E,
Vatter H, Raabe A and Marquardt G: Outcome after Hunt and Hess
Grade V subarachnoid hemorrhage: A comparison of pre-coiling era
(1980-1995) versus post-ISAT era (2005-2014). J Neurosurg.
128:100–110. 2018.PubMed/NCBI View Article : Google Scholar
|
|
21
|
al-Yamany M and Ross IB: Giant fusiform
aneurysm of the middle cerebral artery: Successful Hunterian
ligation without distal bypass. Br J Neurosurg. 12:572–575.
1998.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Rodríguez-Hernández A, Sughrue ME, Akhavan
S, Habdank-Kolaczkowski J and Lawton MT: Current management of
middle cerebral artery aneurysms: Surgical results with a ‘clip
first’ policy. Neurosurgery. 72:415–427. 2013.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Heros RC and Fritsch MJ: Surgical
management of middle cerebral artery aneurysms. Neurosurgery.
48:780–785; discussion 785-786. 2001.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Kim LJ, Klopfenstein JD and Spetzler RF:
Clip reconstruction and sling wrapping of a fusiform aneurysm:
Technical note. Neurosurgery. 61 (Suppl 3):79–80; discussion 80.
2007.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Yang I and Lawton MT: Clipping of complex
aneurysms with fenestration tubes: Application and assessment of
three types of clip techniques. Neurosurgery. 62 (Suppl
2):ONS371–ONS378; discussion 378-379. 2008.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Sanai N, Zador Z and Lawton MT: Bypass
surgery for complex brain aneurysms: An assessment of
intracranial-intracranial bypass. Neurosurgery. 65:670–683;
discussion 683. 2009.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Zhu W, Liu P, Tian Y, Gu Y, Xu B, Chen L,
Zhou L and Mao Y: Complex middle cerebral artery aneurysms: A new
classification based on the angioarchitecture and surgical
strategies. Acta Neurochir (Wien). 155:1481–1491. 2013.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Cimflova P, Özlük E, Korkmazer B, Ahmadov
R, Akpek E, Kizilkilic O, Islak C and Kocer N: Long-term safety and
efficacy of distal aneurysm treatment with flow diversion in the M2
segment of the middle cerebral artery and beyond. J Neurointerv
Surg: Oct 20, 2020 (Epub ahead of print).
|
|
29
|
Topcuoglu OM, Akgul E, Daglioglu E,
Topcuoglu ED, Peker A, Akmangit I, Belen D and Arat A: Flow
diversion in middle cerebral artery aneurysms: is it really an
all-purpose treatment? World Neurosurg. 87:317–327. 2016.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Zanaty M, Chalouhi N, Tjoumakaris SI,
Gonzalez LF, Rosenwasser R and Jabbour P: Flow diversion for
complex middle cerebral artery aneurysms. Neuroradiology.
56:381–387. 2014.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Shi ZS, Ziegler J, Duckwiler GR, Jahan R,
Frazee J, Ausman JI, Martin NA and Viñuela F: Management of giant
middle cerebral artery aneurysms with incorporated branches:
Partial endovascular coiling or combined extracranial-intracranial
bypass - a team approach. Neurosurgery. 65 (Suppl 6):121–129;
discussion 129-131. 2009.PubMed/NCBI View Article : Google Scholar
|