1. Introduction
Obesity is a metabolic disease with increasing
prevalence over the past decades, becoming an important economic
and health care burden (1). In
2016, the World Health Organization estimated that worldwide more
than 650 million adults were obese (2). Obesity is associated with multiple
chronic comorbidities, being the leading risk factor for type 2
diabetes mellitus (T2DM) (3).
The term ‘diabesity’ describes the pathophysiologic
link between obesity and T2DM and was first introduced by Sims
et al (4) in 1973. In 2019,
the International Diabetes Federation estimated that 463 million
individuals worldwide have diabetes, projecting that by 2045, there
will be >700 million cases (5).
The presence of ‘diabesity’ enhances the risk of developing
cardiovascular disease, thus increasing morbidity and mortality
(6,7). Managing diabesity is challenging,
considering that numerous frequently used antidiabetic agents, such
as sulfonylureas, meglitinides, thiazolidinediones and insulin, may
lead to weight gain and therefore cause a vicious cycle (8).
One of the most modern drug classes available that
is able to achieve both glycemic control and weight loss are
glucagon-like peptide 1 (GLP-1) receptor agonists (GLP-1 RAs).
GLP-1 RAs are widely used as a glucose-lowering therapy with weight
reduction and cardiovascular benefits in T2DM, having also
beneficial effects in non-diabetic obesity as a weight loss
adjuvant therapy (9,10). The present narrative review aimed
to highlight the effects of semaglutide, the most recently approved
GLP-1 RA for T2DM as indicated in the existing literature, and to
emphasize the emerging role of semaglutide in managing diabesity
and non-diabetic obesity.
2. GLP-1-biological effects and development
of GLP-1 RAs
Biological effects
GLP-1 is an incretin hormone secreted in a biphasic
pattern by the neuroendocrine L cells in the distal ileum and colon
after consumption of nutrients, particularly glucose and other
carbohydrates (11,12). It has a short elimination half-life
(1-2 min) due to proteolysis by dipeptidyl peptidase IV and renal
elimination (12). GLP-1 receptors
are expressed in numerous organs, mainly occurring in the pancreas,
central nervous system (hypothalamus) and the gastrointestinal
tract, but also in the heart and kidneys (12). GLP-1 stimulates insulin secretion
from the β-pancreatic cells in a glucose-dependent manner, also
promoting β-pancreatic cell survival and proliferation (13,14).
Furthermore, GLP-1 reduces glucagon secretion by α-pancreatic cells
through complex endocrine mechanisms, which include somatostatin
stimulation and insulinotropic effects on the β-pancreatic cells
(12). By slowing down gastric
emptying, GLP-1 further reduces blood glucose and appetite
(15). This effect on appetite is
not only attributed to the delayed gastric emptying but also to its
influence on the hypothalamus as a neurotransmitter, particularly
on the lateral hypothalamus, and the paraventricular and arcuate
nucleus (16,17). Other effects of endogenous GLP-1
include reduction in systolic blood pressure, increased myocardial
contraction, improved endothelial vasodilation, increased glycogen
storage, improved lipid profile, diuresis and natriuresis induction
(18-21).
Development of GLP-1 RAs
At present, six injectable (subcutaneous) GLP-1 RAs
and one oral formulation are available in Europe for T2DM
treatment. Based on their pharmacological properties, GLP-1 RAs are
classified into short- or long-acting agents. Short-acting GLP-1
RAs include exenatide standard-release (Byetta) and lixisenatide
(Lyxumia). Their major mechanism of action is based on slowing
gastric emptying and lowering postprandial glucose. Long-acting
GLP-1 RAs include exenatide modified-release (Bydureon),
liraglutide (Victoza), dulaglutide (Trulicity) and semaglutide
(Ozempic). Compared to short-acting compounds, long-acting agents
have a mechanism of action that mainly comprises stimulating
insulin secretion and inhibiting glucagon release, thus influencing
both postprandial and fasting glucose. The posology of GLP-1 RAs in
T2DM is illustrated in Table I
(22,23).
 | Table IPosology of GLP-1 RA in type 2
diabetes mellitus. |
Table I
Posology of GLP-1 RA in type 2
diabetes mellitus.
| GLP-1 RA | Structure | Posology |
|---|
| Exenatide
standard-release | Exenatide-4
derivative | 5 µg twice daily
for first month, then increase to 10 µg twice daily, before
meals |
| Lixisenatide | Exenatide-4
derivative | 10 µg once daily
first two weeks, then increase to 20 µg once daily, before
meals |
| Exenatide
modified-release | Exenatide-4
derivative | 2 mg once weekly,
with or without meals |
| Liraglutide | Modified human
GLP-1 | 0.6 mg once daily
for first week, then increase to 1.2 mg once daily (further
increase up to 1.8 mg if poor glucose control), with or without
meals |
| Dulaglutide | Modified human
GLP-1 | 0.75 mg once weekly
in monotherapy (1.5 mg once weekly as add-on therapy), with or
without meals |
| Semaglutide | Modified human
GLP-1 | 0.25 mg once weekly
for first month, then increase to 0.5 mg once weekly for at least
one month (further increase up to 1 mg in case of poor glycemic
control), with or without meals |
| Semaglutide
(oral) | Modified human
GLP-1 | 3 mg once daily for
one month, then increase to 7 mg once daily for at least one month
(further increase up to 14 mg in case of poor glycemic control),
before meals |
Liraglutide was the first antidiabetic treatment
approved as a weight reduction drug in non-diabetic obesity. Sold
under the name of Saxenda, liraglutide at a dose of 3.0 mg once
daily was approved by both Food and Drug Administration in 2014 and
the European Medicines Agency in 2015 for long-term weight
management (24).
3. Semaglutide in diabesity and non-diabetic
obesity
Excess weight, particularly when associated with
visceral fat, increases the risk of insulin resistance, metabolic
syndrome and T2DM (25,26). The link between excess weight and
T2DM supposably lies in the inflammatory state associated with
excess adipose tissue. Several pro-inflammatory mediators, such as
tumor necrosis factor-α, interleukin-6 and complement component 3,
along with fatty-acid lipotoxicity inhibit intracellular insulin
signaling, which may lead to pancreatic β-cell dysfunction and
subsequently to T2DM (27). When a
new diagnosis of T2DM is made, it is crucial to educate the patient
regarding the importance of a healthy lifestyle, which includes
avoiding excess calories (particularly high-glycemic-index
carbohydrates) and increasing physical activity to prevent
cardiovascular and metabolic complications. Nicola et al
(28) noted a significantly higher
low-density lipoprotein cholesterol, hypertriglyceridemia, low
high-density lipoprotein cholesterol and a higher prevalence of
micro- and macroalbuminuria in hypertensive diabetic patients.
The American Diabetes Association recommends
metformin as the first-line drug for T2DM therapy, if not
contraindicated (10). GLP-1 RAs
are known to lower blood glucose by stimulating insulin production
in the pancreatic β-cells and inhibiting glucagon release by the
pancreatic α-cells, combined with slowing gastric emptying and
reducing appetite and food consumption (29). Therefore, given their beneficial
effects on glucose metabolism and weight loss potential, GLP-1 RAs
are currently recommended as a second-line therapy in T2DM.
Furthermore, their action of increasing insulin production and
lowering glucagon action is tailored in a glucose-dependent manner,
thus posing a low risk of hypoglycemia and making them one of the
most effective and safe options when a more intensive antidiabetic
treatment is required (30).
Semaglutide (Ozempic) is a long-acting GLP-1 RA and
its administration is once-weekly subcutaneously at doses of 0.5
and 1.0 mg, with 0.25 mg/week being the initiation dose for the
first 4 weeks. The safety and efficacy of semaglutide was
investigated in the Semaglutide Unabated Sustainability in
Treatment of Type 2 Diabetes (SUSTAIN) clinical trial program. A
summary of the major results from the SUSTAIN clinical program is
provided in Table II.
| Table IISummary of clinical trials from the
SUSTAIN program. |
Table II
Summary of clinical trials from the
SUSTAIN program.
| Clinical trial | Aim | Main results |
|---|
| SUSTAIN-1 | To assess the
safety and efficacy of semaglutide vs. placebo in T2DM patients
without prior drug therapy | Semaglutide 0.5 and
1.0 mg significantly reduced HbA1c vs. placebo (-1.45 vs. -1.55 vs.
-0.2%); semaglutide 0.5 and 1.0 mg significantly reduced body
weight vs. placebo (-3.73 vs. -4.53 vs. -0.98 kg) |
| SUSTAIN-2 | To assess the
safety and efficacy of semaglutide vs. sitagliptin in T2DM patients
with poor control on metformin, thiazolidinediones or both | Semaglutide 0.5 and
1.0 mg achieved a greater HbA1c reduction vs. sitagliptin 100 mg
(-1.3 vs. -1.6 vs. -0.5%); semaglutide 0.5 and 1.0 mg achieved a
greater body weight reduction vs. sitagliptin 100 mg (-4.3 vs. -6.1
vs. -1.9 kg) |
| SUSTAIN-3 | To assess the
safety and efficacy of semaglutide vs. once-weekly exenatide in
T2DM patients on previous oral antidiabetic agents | Semaglutide 1.0 mg
achieved a greater HbA1c reduction vs. exenatide once weekly 2.0 mg
(-1.5 vs. -0.9%); semaglutide 1.0 mg achieved a greater body weight
reduction vs. exenatide once weekly 2.0 mg (-5.6 vs. -1.9 kg) |
| SUSTAIN-4 | To assess the
safety and efficacy of semaglutide vs. insulin glargine in T2DM
patients with poor control on metformin, with or without
sulfonylureas | Semaglutide 0.5 and
1.0 mg achieved a greater HbA1c reduction vs. insulin glargine
(-1.21 vs. -1.64 vs. -0.83%); semaglutide 0.5 and 1.0 mg achieved a
greater body weight reduction vs insulin glargine (-3.5 vs. -5.2
vs. +1.15 kg) |
| SUSTAIN-5 | To investigate the
superiority of semaglutide vs. placebo in T2DM patients on basal
insulin, with or without metformin | Semaglutide 0.5 and
1.0 mg achieved a greater HbA1c reduction vs. placebo (-1.4 vs.
-1.8 vs. -0.1%); semaglutide 0.5 and 1.0 mg achieved a greater body
weight reduction vs. placebo (-3.7 vs. -6.4 vs. -1.4 kg) |
| SUSTAIN-6 | To investigate the
cardiovascular safety of semaglutide in T2DM | Semaglutide arm had
a lower primary outcome (first occurrence of cardiovascular death,
nonfatal myocardial infarction or nonfatal stroke) occurrence vs.
placebo (6.6 vs. 8.9%); semaglutide arm had lower rates of new or
worsening nephropathy vs. placebo (3.8 vs. 6.1%); semaglutide arm
had a higher incidence of retinopathy complications vs. placebo
(3.0 vs. 1.8%) |
| SUSTAIN-7 | To assess the
safety and efficacy of semaglutide vs. dulaglutide in T2DM patients
with poor control on metformin | Semaglutide 0.5 mg
achieved a greater HbA1c reduction vs. dulaglutide 0.75 mg (-1.5
vs. -1.1%); semaglutide 1.0 mg achieved a greater HbA1c reduction
vs. dulaglutide 1.5 mg (-1.8 vs. -1.4%); semaglutide 0.5 mg
achieved a greater weight reduction vs. dulaglutide 0.75 mg (-4.6
vs. -2.3 kg); semaglutide 1.0 mg achieved a greater body weight
reduction vs. dulaglutide 1.5 mg (-6.5 vs. -3.0 kg) |
| SUSTAIN-8 | To assess the
safety and efficacy of semaglutide vs. canagliflozin in T2DM
patients with poor control on metformin | Semaglutide 1.0 mg
achieved a greater HbA1c reduction vs. canagliflozin 300 mg (-1.5
vs. -1.0%); semaglutide 1.0 mg achieved a greater body weight
reduction vs. canagliflozin 300 mg (-5.3 vs. -4.2 kg) |
| SUSTAIN-9 | To assess the
safety and efficacy of semaglutide when added to a SGLT-2 inhibitor
in patients with poorly controlled T2DM | Semaglutide
markedly reduced HbA1c when added to a SGLT-2 inhibitor vs. placebo
(-1.5 vs. -0.1%); semaglutide markedly reduced body weight when
added to a SGLT-2 inhibitor vs. placebo (-4.7 vs. -0.9 kg) |
| SUSTAIN-10 | To assess the
safety and efficacy of semaglutide vs. liraglutide in T2DM patients
on 1-3 oral antidiabetic agents | Semaglutide 1.0 mg
had a greater HbA1c reduction vs. liraglutide 1.2 mg (-1.7 vs.
-1.0%); semaglutide 1.0 mg had a greater body weight reduction vs.
liraglutide 1.2 mg (-5.8 vs. -1.9 kg) |
Semaglutide as a blood
glucose-lowering agent
SUSTAIN-1 was a phase IIIa clinical trial that
compared the safety and efficacy of semaglutide (0.5 and 1.0 mg)
over the course of 30 weeks vs. placebo in patients with T2DM that
had no prior drug therapy, only diet and exercise interventions.
Compared to the placebo, both doses of semaglutide produced a
significant reduction in glycated hemoglobin (HbA1c) [-1.45% with
semaglutide 0.5 mg vs. -1.55% with semaglutide 1.0 mg vs. -0.2%
with placebo; the estimated treatment difference (ETD) for
semaglutide 0.5 mg vs. placebo was -1.43% and the ETD for
semaglutide 1.0 mg vs. placebo was -1.53%; P for both doses of
semaglutide vs. placebo <0.0001] (31).
The SUSTAIN-2 clinical trial compared semaglutide
0.5 and 1.0 mg with sitagliptin 100 mg over the course of 56 weeks
in patients with T2DM inadequately controlled with metformin,
thiazolidinediones or both. HbA1c reduction was greater with both
doses of semaglutide vs. sitagliptin (-1.3% with 0.5 mg semaglutide
vs. -1.6% with 1.0 mg semaglutide vs. -0.5% with 100 mg of
sitagliptin; ETD -0.77% with semaglutide 0.5 mg and -1.06% with
semaglutide 1.0 mg; P for both doses of semaglutide vs. sitagliptin
<0.0001 for non-inferiority and superiority) (32). Semaglutide 1.0 mg was compared with
once-weekly exenatide in the SUSTAIN-3 clinical trial, which was
performed over the course of 56 weeks on 813 adults with T2DM on
previous oral antidiabetic agents. A reduction in HbA1c of 1.5%
with semaglutide and 0.9% with exenatide was noted (ETD, 0.62%;
P<0.0001 for noninferiority and superiority for semaglutide vs.
exenatide once-weekly) (33).
SUSTAIN-4 assessed the safety and efficacy of
semaglutide compared to insulin glargine in patients with T2DM
inadequately controlled with metformin (with or without
sulfonylureas). At week 30, semaglutide at 0.5 and 1.0 mg achieved
greater HbA1c reductions than insulin glargine (1.21 vs. 1.64 vs.
0.83%; ETD, -0.38% with semaglutide 0.5 mg and -0.81% with
semaglutide 1.0 mg with ETD; P<0.0001 for ETD for both doses of
semaglutide vs. insulin glargine) (34). In the SUSTAIN-5 clinical trial,
semaglutide was investigated as an add-on vs. placebo in patients
with T2DM on basal insulin, with or without metformin. At week 30,
HbA1c exhibited a significant reduction of 1.4 and 1.8% with
semaglutide 0.5 and 1.0 mg, respectively, vs. 0.1% with placebo (P
for both doses of semaglutide vs. placebo <0.0001) (35). The SUSTAIN-7 clinical trial proved
the superiority of 0.5 and 1.0 mg semaglutide in improving the mean
HbA1c when compared to dulaglutide 0.75 and 1.5 mg. Semaglutide 0.5
mg reduced the mean HbA1c by 1.5 vs. 1.1% with dulaglutide 0.75 mg.
Furthermore, 1.0 mg of semaglutide produced a reduction of 1.8% in
HbA1c vs. 1.4% with dulaglutide 1.5 mg (36).
SUSTAIN-8 compared once-weekly semaglutide 1.0 mg
with once-daily canagliflozin 300 mg in patients with T2DM
inadequately controlled with metformin. Semaglutide was superior to
canagliflozin in reducing HbA1c (ETD, -0.49%; P<0.0001)
(37). In SUSTAIN-9, the efficacy
and safety of semaglutide were assessed when added to a sodium
glucose cotransporter-2 (SGLT-2) inhibitor in patients with T2DM
with poor glycemic control. Semaglutide in addition to a SGLT-2
inhibitor significantly reduced HbA1c (ETD, -1.42%; P<0.0001)
compared with placebo. Semaglutide added to a SGLT-2 inhibitor was
well tolerated with significant improvements in glycemic control
(38).
In SUSTAIN-10, semaglutide (1.0 mg/week) was
compared with liraglutide (1.2 mg/day) in subjects with T2DM
treated with 1-3 oral antidiabetic drugs. A total of 577 subjects
were randomized to receive either semaglutide or liraglutide.
Patients receiving semaglutide had a superior reduction in HbA1c
(ETD, -0.69%; P<0.0001). Both treatments had similar safety
profiles, with semaglutide having a higher frequency of
gastrointestinal reactions compared to liraglutide (43.9 vs. 38.3%)
(39).
Semaglutide and body weight reduction
benefits
In SUSTAIN-1, a marked body weight loss was observed
with both doses of semaglutide when compared to placebo.
Specifically, with semaglutide at 0.5 and 1.0 mg, a weight
reduction of 3.73 and 4.53 kg kg was achieved, respectively, while
the placebo had an insignificant loss of 0.98 kg (ETD vs. placebo,
-2.75 and -3.56 kg with semaglutide 0.5 and 1.0 mg, respectively; P
for both doses of semaglutide vs. placebo <0.0001) (31). In SUSTAIN-2, at week 56, a weight
loss of 4.3 kg with semaglutide 0.5 mg and 6.1 kg with semaglutide
1.0 mg, and 1.9 kg with sitagliptin 100 mg was achieved (ETD, -2.35
kg with semaglutide 0.5 mg and -4.20 kg with semaglutide 1.0 mg vs.
sitagliptin; P for both doses of semaglutide vs. sitagliptin
<0.0001, with superiority of sitagliptin) (32).
The SUSTAIN-3 trial indicated that
semaglutide-treated subjects achieved a greater weight reduction
when compared to exenatide-treated subjects (-5.6 vs. -1.9 kg; ETD
-3.78 kg; P<0.0001) (33).
SUSTAIN-4 compared semaglutide vs. insulin glargine. Body weight
loss was observed in semaglutide-treated subjects and at week 30, a
loss of 3.5 kg with semaglutide 0.5 mg and 5.2 kg with semaglutide
1.0 mg, compared to a weight gain of 1.15 kg with insulin glargine
was observed (34). This result
came with no surprise given the appetite-reducing effects of GLP-1
and the anabolic effects of insulin. When added to basal insulin,
in patients with T2DM with or without metformin treatment,
semaglutide produced a significant body weight reduction vs.
placebo according to the results of SUSTAIN-5 (-3.7 kg with
semaglutide 0.5 mg vs. -6.4 kg with semaglutide 1.0 mg vs. -1.4 kg
with placebo; P for both doses of semaglutide vs. placebo
<0.0001) (35). In SUSTAIN-7,
semaglutide was superior to dulaglutide regarding body weight
reduction properties. Semaglutide 0.5 mg achieved a weight
reduction of 4.6 vs. 2.3 kg with dulaglutide 0.75 mg. Furthermore,
an even greater difference was observed between semaglutide 1.0 mg
vs. dulaglutide 1.5 mg (-6.5 vs. -3.0 kg) (36).
Semaglutide was superior to canagliflozin in
reducing body weight (ETD, -1.06 kg; P<0.0029) in
SUSTAIN-8(37). A sub-study of
SUSTAIN-8 compared the effects of semaglutide 1.0 mg and once-daily
canagliflozin 300 mg on body composition in individuals with T2DM
uncontrolled with metformin. The results indicated no significant
differences between semaglutide and canagliflozin regarding changes
in body composition (40). In
SUSTAIN-9, adding semaglutide to a SGLT-2 inhibitor achieved
significant improvements in body weight reduction compared to
placebo (ETD, -3.81 kg; P<0.0001) (38). Given the positive outcomes that
were obtained when adding semaglutide to canagliflozin, it is
indicated that combining a GLP-1 RA and a SGLT-2 inhibitor may
provide an additive effect in improving glycemic control and body
weight reduction and also in reducing cardiovascular risk and renal
impairment.
Patients receiving semaglutide in SUSTAIN-10 had a
superior reduction in body weight compared with the
liraglutide-treated group (ETD, -3.83 kg; P<0.0001) (39). Semaglutide was studied as a
possible chronic weight management drug in non-diabetic obesity. A
randomized, double-blinded, placebo-controlled trial performed on
957 individuals without diabetes was performed to evaluate the
safety and efficacy of semaglutide in comparison with liraglutide
and placebo in promoting weight loss. Participants received
semaglutide at dosages ranging from 0.05 to 0.4 mg or liraglutide
3.0 mg as once-daily subcutaneous injections. The estimated mean
loss for the 0.4 mg semaglutide group was -13.8 vs. -2.3% with
placebo. Mean body weight reductions with ≥0.2 mg semaglutide vs.
liraglutide were significant (-13.8 to -11.2 vs. -7.8%) (41). A double-blinded randomized clinical
trial, which included 1,961 adults without T2DM with a body mass
index of at least 30 or at least 27 kg/m2 with ≥1
weight-related coexisting comorbidity, investigated the role of 2.4
mg subcutaneous semaglutide vs. placebo in addition to lifestyle
interventions. At week 68, the mean body weight change was highly
significant in the semaglutide group vs. the placebo group (-14.9
vs. -2.4%; ETD, -12.4%; P<0.001). A weight reduction of at least
5% was achieved by 86.4% of the subjects in the semaglutide group
vs. 31.5% in the placebo group. A 10% weight reduction was achieved
by 69.1% of subjects in the semaglutide group vs. 12.0% of subjects
in the placebo group. A 15% weight reduction occurred in 50.5% of
patients of the semaglutide group vs. 4.9% in the placebo group
(42). Given the proven benefits
of semaglutide in managing chronic excess weight and its good
safety profile, the Food and Drug Administration recently approved
the use of semaglutide 2.4 mg/once-weekly as an add-on-therapy to
lifestyle modifications in adults with obesity or overweight with
at least one weight-related comorbidity (43). Therefore, semaglutide became the
second GLP-1 RA besides liraglutide that may be used in managing
non-diabetic excess weight. The Food and Drug Administration
approval was based on the results from the Semaglutide Treatment
Effect in People with Obesity (STEP) program, which consisted of
four phase III clinical trials. A summary of the STEP program is
illustrated in Table III
(42,44-46).
| Table IIISummary of clinical trials from the
STEP program. |
Table III
Summary of clinical trials from the
STEP program.
| Clinical trial | Design | Aim | Main results |
|---|
| STEP-1 | 68-week randomized,
double-blind, multicentre, placebo-controlled | To investigate the
efficacy and safety of semaglutide 2.4 mg/once-weekly vs. placebo
in 1,961 adults with obesity or overweight with comorbidities | Semaglutide 2.4 mg
achieved a weight loss of 14.9 vs. 2.4% with placebo; 86.4% of the
semaglutide 2.4 mg group achieved a weight loss of ≥5 vs. 31.5%
with placebo |
| STEP-2 | 68-week randomized,
double-blind, multicentre, placebo-controlled | To compare the
efficacy and safety of semaglutide 2.4 mg/once-weekly vs.
semaglutide 1.0 mg/once-weekly vs. placebo in 1,210 adults with
T2DM and obesity or overweight with comorbidities | Semaglutide 2.4 mg
achieved a weight loss of 9.6 vs. 7.0% with semaglutide 1.0 mg vs.
3.4% with placebo; 68.8% of semaglutide 2.4 mg group achieved a
weight loss of ≥5 vs. 28.5% with placebo |
| STEP-3 | 68-week randomized,
double-blind, multicentre, placebo-controlled | To investigate the
efficacy and safety of semaglutide 2.4 mg/once-weekly vs. placebo
in combination with intensive behavioral treatment in 611 adults
with obesity or overweight with comorbidities | Semaglutide 2.4 mg
achieved a weight loss of 16.0 vs. 5.7% with placebo; 86.6% of
semaglutide 2.4 mg group achieved a weight loss of ≥5 vs. 47.6%
with placebo |
| STEP-4 | 68-week randomized,
double-blind, multicentre, placebo-controlled | To investigate the
efficacy and safety of semaglutide 2.4 mg/once-weekly vs. placebo
in 902 adults with obesity or overweight | After 20 weeks
run-in, 803 adults reached the target dose of semaglutide 2.4 mg
and were randomized to continued treatment or placebo for 48 weeks;
after 48 weeks, semaglutide 2.4 mg achieved an additional weight
loss of 7.9 vs. 6.9% with placebo; after 68 weeks, semaglutide 2.4
mg achieved a total weight loss of 17.4% |
Oral semaglutide: Blood glucose and
body weight benefits
Oral semaglutide (Rybelsus), the first oral GLP-1
RA, was studied in 10 phase IIIa clinical trials as part of the
PIONEER program. PIONEER-1 was a 26-week randomized, double-blinded
clinical trial that compared the efficacy and safety of oral
semaglutide (3, 7 or 14 mg) as monotherapy with placebo in subjects
with T2DM managed by lifestyle interventions. It was demonstrated
that oral semaglutide at all doses was superior to the placebo in
improving HbA1c (ranging from -0.6 to -1.1%) and in body weight
reduction (14 mg dose) (47).
Results from PIONEER-2 suggested that oral semaglutide 14 mg was
superior in reducing HbA1c compared with empagliflozin 25 mg in a
52-week trial (1.3 vs. 0.9%; ETD -0.4%; P<0.0001). Furthermore,
at week 52, oral semaglutide achieved an average weight reduction
of 4.7 vs. 3.8 kg with empagliflozin, rendering oral semaglutide
significantly more effective (P=0.0114) (48). The PIONEER-4 clinical trial
demonstrated that oral semaglutide (14 mg) was non-inferior in
decreasing HbA1c to subcutaneous liraglutide (1.8 mg) at week 26
(ETD, -0.1%; P<0.0001) and superior to placebo (ETD, -1.1%;
P<0.0001). Furthermore, oral semaglutide achieved a greater
weight reduction than liraglutide and placebo (-4.4 vs. -3.1 vs.
0.5 kg; ETD, -1.2 kg vs. liraglutide and -3.8 kg vs. placebo;
P=0.0003 and P<0.0001, respectively) (49).
The PIONEER 10 clinical trial investigated the
efficacy and safety of oral semaglutide vs. dulaglutide in Japanese
patients with uncontrolled T2DM. Oral once-daily semaglutide (14
mg) achieved a significant HbA1c reduction vs. once-weekly
dulaglutide (0.75 mg) (ETD, -0.3%; P=0.0170). Furthermore, oral
semaglutide significantly reduced body weight vs. dulaglutide (ETD,
-2.6 kg for oral semaglutide 14 vs. 0.75 mg dulaglutide;
P<0.0001) (50).
Cardiovascular benefits of
semaglutide
The SUSTAIN-6 clinical trial investigated the
cardiovascular safety of once-weekly subcutaneous administration of
semaglutide. The primary outcome composite (first occurrence of
cardiovascular death, nonfatal myocardial infarction or nonfatal
stroke) occurred in 6.6% in the semaglutide group vs. 8.9% in the
placebo group (P<0.0001 for noninferiority). Mortality rates
from cardiovascular causes were similar among the studied groups,
while the semaglutide group had an advantage regarding lower rates
of new or worsening nephropathy [3.8 vs. 6.1%, hazard ratio
(HR)=0.64, P<0.01] (51).
Furthermore, by improving glucose metabolism, GLP-1 RAs are able to
prevent the development of macroalbuminuria and also maintain an
adequate glomerular filtration rate, and are an efficient and safe
option in diabetic nephropathy (52). However, semaglutide-treated
subjects had a higher incidence of retinopathy complications vs.
placebo (P=0.02) (51). Recently
published results demonstrated that semaglutide improved
health-related quality of life vs. placebo in patients with T2DM
with high cardiovascular risk in the SUSTAIN-6 trial, possibly
explained by the reduction of HbA1c and weight loss (53).
PIONEER-6 investigated the cardiovascular outcomes
for oral semaglutide in subjects with T2DM and with high
cardiovascular risk in an event-driven, randomized, double-blinded,
placebo-controlled trial. Oral semaglutide was non-inferior to
placebo regarding cardiovascular safety, with major cardiovascular
events occurring in 3.8% of the oral semaglutide-treated subjects
vs. 4.8% in the placebo group (HR=0.79; P<0.001 for
non-inferiority) (54). The study
did not have the statistical power to demonstrate superiority, as
it was an event-driven trial. Death from cardiovascular causes
occurred in 0.9% in the oral semaglutide group vs. 1.9% in the
placebo group (HR=0.49) and nonfatal myocardial infarction occurred
in 2.3% in the oral semaglutide group vs. 1.9% in the placebo group
(HR=1.18), while nonfatal stroke occurred in 0.8% in the oral
semaglutide group vs. 1.0% in the placebo group (HR=0.74).
All-cause mortality was encountered in 1.4% in the oral semaglutide
group vs. 2.8% in the placebo group (HR=0.51) (54).
Semaglutide and nonalcoholic fatty
liver disease (NAFLD)
NAFLD is a metabolic liver disease that has a broad
spectrum of clinical presentation, ranging from simple steatosis to
severe forms such as nonalcoholic steatohepatitis (NASH), cirrhosis
and hepatocellular carcinoma (55). Similar to that of T2DM and obesity,
the incidence of NAFLD is increasing worldwide. It is estimated
that up to 70-80% of patients with T2DM and/or obesity present with
NAFLD (56,57). T2DM is an important risk factor for
the progression of NAFLD to more severe forms (58-60).
The exact pathophysiological mechanisms which lead to NAFLD remain
to be completely elucidated, but several proposed hypotheses
include insulin resistance, environmental factors, polymorphisms,
adipose tissue expandability and spleen mechanisms to promote liver
fat accumulation (61). Currently,
lifestyle changes are the primary tool in managing NAFLD, as to
date, no pharmacological treatment has been approved.
GLP-1 RAs may be a potential therapeutic option
given their benefits in T2DM and obesity, the two major drivers of
NAFLD (62). In a systematic
review published in 2020 by Lv et al (63), GLP-1 RAs were determined to improve
liver enzymes and hepatic steatosis. A recently published
metanalysis by Mantovani et al (64) investigated the published data of
placebo-controlled, active-controlled or randomized controlled
trials that evaluated the efficacy and safety of GLP-1 RAs in
treating NAFLD or NASH in adults with or without T2DM. They
revealed GLP-1 RAs to be efficient in improving NAFLD, particularly
liraglutide and semaglutide. A randomized, double-blinded,
placebo-controlled, phase 2 trial compared daily semaglutide (0.1,
0.2 and 0.4 mg) with placebo in patients with biopsy-confirmed
NASH. NASH resolution without worsening of fibrosis was observed in
40% of cases in the semaglutide 0.1 mg group, in 36% of cases in
the semaglutide 0.2 mg group and in 59% in the semaglutide 0.4 mg
group, compared with 17% of cases in the placebo group (P<0.001,
semaglutide 0.4 mg vs. placebo). However, there was no significant
improvement regarding the fibrosis stage between semaglutide 0.4 mg
and the placebo (P=0.48) (65).
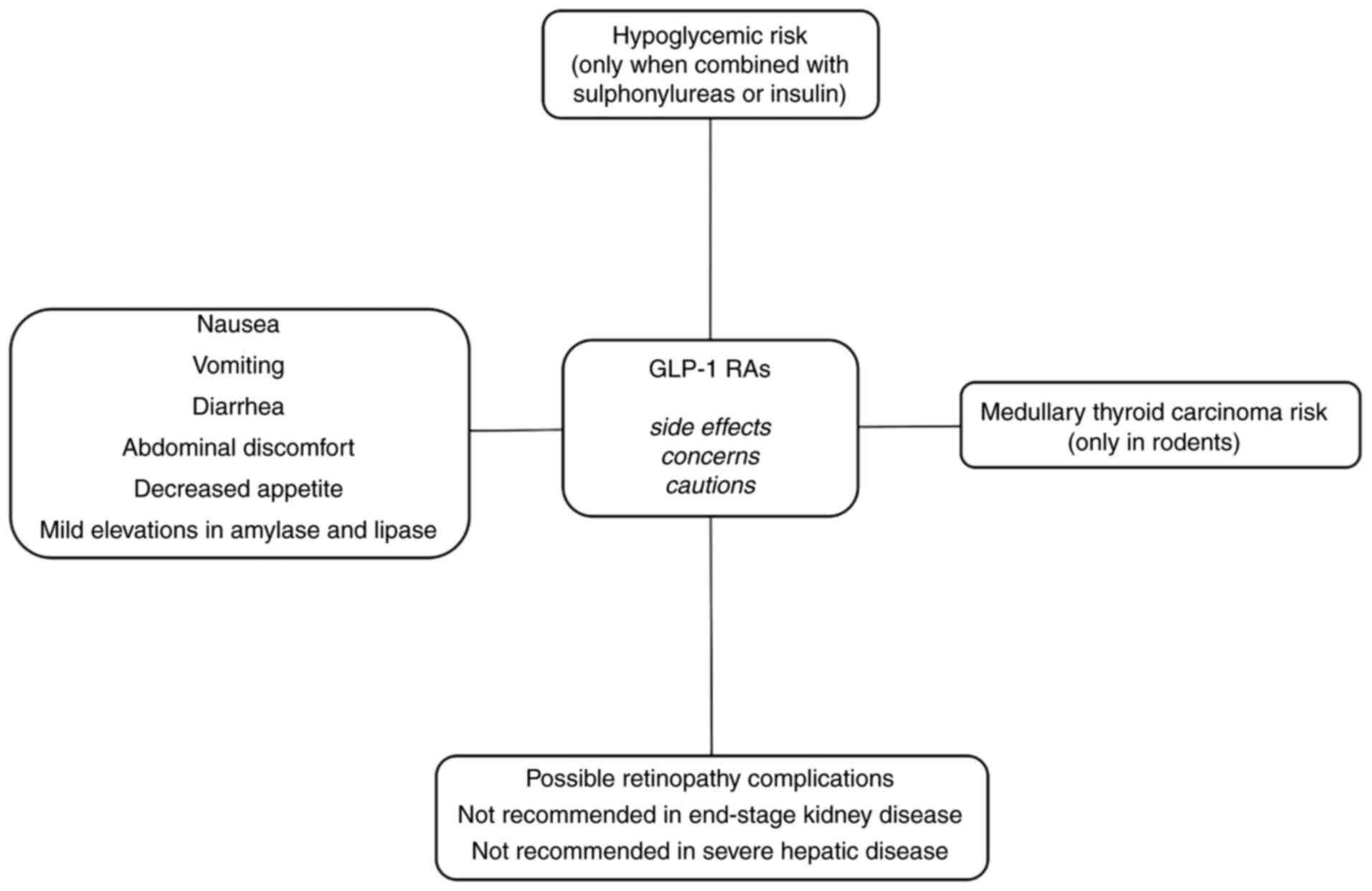
4. Semaglutide-side effects and
cautions
Semaglutide mainly shares the classically observed
side effects of other GLP-1 RAs (Fig.
1).
Gastrointestinal side effects
The common side effects associated with GLP-1 RAs
use are gastrointestinal reactions, mainly nausea, vomiting and
diarrhea. During the SUSTAIN program that assessed safety
parameters, the rate of discontinuation due to adverse events was
low (5-13%), with SUSTAIN-6 reporting a higher discontinuation rate
(almost 20%). The major reasons for the discontinuation were
gastrointestinal adverse events (31-36).
Nausea occurred in 17.0%, diarrhea in 12.2% and vomiting in 6.4% of
patients treated with semaglutide 0.5 mg. As for patients treated
with semaglutide 1.0 mg, nausea occurred in 19.9%, diarrhea in
13.3% and vomiting in 8.4% of cases (66,67).
Semaglutide has a similar gastrointestinal safety profile as other
GLP-1 Ras (68,69). A metanalysis from 2018 that
included nine phase III randomized controlled trials and 9,773
subjects highlighted that semaglutide did not increase the risk of
any adverse events, hypoglycemia or pancreatitis, but had a higher
risk of gastrointestinal reactions (mainly nausea, vomiting,
diarrhea, abdominal discomfort and decreased appetite) when
compared to other therapies [relative risk (RR)=1.98; P<0.001]
(70). Given that the occurrence
of gastrointestinal reactions is the main reason for treatment
discontinuation, a titration regimen is recommended for
semaglutide, starting with 0.25 mg once-weekly for 4 weeks,
increasing the dose to 0.5 mg once-weekly for at least 4 weeks. If
a higher dose is required to achieve proper glycemic control, the
dose may then be increased to 1.0 mg once-weekly, assuming the
tolerance is adequate. For oral semaglutide, the initial dose is 3
mg/day for the first month, then the dose should be increased to 7
mg/day for at least another month (the dose may be increased up to
14 mg/day in the case of poor glycemic control).
Risk of hypoglycemia
The frequency of hypoglycemia was observed to be
usually low (1-2%) when semaglutide was not combined with insulin
or sulphonylureas (31,32,36,71).
However, when added to sulphonylureas or insulin, hypoglycemia had
higher frequencies (4-10%) (33-35,71).
Shi et al (70) observed no
increased risk of hypoglycemia with semaglutide when compared to
other therapies (RR=1.07; P=0.317).
Medullary thyroid carcinoma and
pancreatitis concerns
Rodent studies have indicated an increased risk of
developing medullary thyroid carcinoma following treatment with
GLP-1 RAs, but without existing confirmation of these results in
humans (72,73). The SUSTAIN program suggested no
elevation in calcitonin levels. However, GLP-1 RAs should not be
used in individuals with a personal or family history of medullary
thyroid carcinoma or multiple endocrine neoplasia type 2A and 2B
(23,74). Concerns about pancreatitis in
incretin-based therapy have been raised due to mild elevations in
amylase and/or lipase levels (75). The risk of pancreatitis with
semaglutide was not significantly higher when compared with other
therapies (0.3 vs. 0.4%, RR=0.82; P=0.641) (70). In 2020, Abd El Aziz et al
(76) published a metanalysis
based on cardiovascular outcome trials and indicated no significant
risk of acute pancreatitis or any malignant disease.
Ocular and renal effects
SUSTAIN-6 noted an increased risk of retinopathy
complications (vitreous hemorrhage, blindness or conditions
requiring treatment with an intravitreal agent or photocoagulation)
in the semaglutide group vs. the placebo group (3.0 vs. 1.8%,
HR=1.76, P=0.02) (51). On the
contrary, SUSTAIN-1-5 and -7 did not report any similar results.
One explanation for these observations may be the HbA1c levels at
baseline and the rapidity of reduction of HbA1c, considering that
rapid improvement in glucose control has been associated with
aggravated diabetic retinopathy (77-79).
No dose adjustment is required based on age or in patients with
mild, moderate or severe renal or hepatic impairment; however, it
is not recommended in patients with end-stage kidney disease and
experience in severe hepatic disease is limited (66,67).
5. Future considerations
Weight loss induced by GLP-1 RAs is usually observed
after long-term treatment. GLP-1 RAs promote weight loss mainly by
reducing appetite, thus reducing food consumption and by increasing
satiety. Treatment adherence is important, as well as lifestyle
changes, which include dietary caloric deficit and increased
physical activity. It was observed that a higher dose of GLP-1 RA
is associated with a higher chance to obtain a higher weight
reduction. However, weight reduction usually lasts as long as the
treatment is continued, with near-baseline weight values returning
within months of discontinuation of pharmacological treatment as
reported by Kelly et al (80).
Semaglutide is the second GLP-1 RA that may be
safely and efficiently used in non-diabetic individuals with excess
weight, providing a new milestone in the pharmacological treatment
of obesity. Furthermore, oral semaglutide, given its posology, may
provide higher attractiveness and better treatment adherence, and
thus, future research into the use of oral semaglutide in
non-diabetic obese patients may provide novel insight and an
effective and safe weight-loss method. Combination therapy with
semaglutide is also being studied. A randomized,
placebo-controlled, multiple ascending dose, phase Ib trial
investigated the combination of semaglutide 2.4 mg with
cagrilintide, a long-acting amylin analogue. Concomitant treatment
with cagrilintide and semaglutide was well tolerated and produced a
greater weight loss than semaglutide alone (81). Further studies are required to
assess variable combination options with semaglutide to provide
novel treatments for long-term weight management.
The cardiovascular safety of semaglutide was
assessed in SUSTAIN-6 for once-weekly subcutaneous formulation and
in PIONEER-6 for the oral formulation, as discussed previously. A
Heart Disease Study of Semaglutide in Patients with Type 2 Diabetes
(SOUL) will bring additional data regarding the cardiovascular
outcomes with oral semaglutide vs. placebo (82,83).
Semaglutide, as with other agents from the GLP-1 RAs drug class,
reduces the risk of cardiovascular events in high-risk patients.
The American Diabetes Association currently recommends the use of
GLP-1 RAs as part of the antidiabetic treatment in patients with
T2DM with atherosclerotic cardiovascular disease or established
kidney disease (10). The positive
effects of GLP-1 RAs on cardiovascular function may be explained by
the beneficial effects of this drug class on glucose metabolism,
body weight and blood pressure. The exact mechanisms of how GLP-1
RAs provide cardiovascular benefits remain to be elucidated in
future research. Furthermore, long-term studies are required to
investigate the potential additive effects on the cardiovascular
and renal function of the combination between a GLP-1 RA and an
SGLT-2 inhibitor.
Semaglutide achieved promising results in improving
NAFLD. Larger randomized clinical trials are required to confirm
its applicability in NAFLD. Furthermore, clinicians should focus on
preventing the development of NAFLD by promoting a healthy
lifestyle, particularly in individuals suffering from T2DM and
obesity who are at high risk of developing steatohepatitis.
6. Conclusions
The present review highlighted the benefits of
semaglutide not only as an antidiabetic agent but also as a drug
with effective weight reduction properties. Clinicians should be
aware that semaglutide therapy is one of the most modern methods of
treatment for patients with T2DM and obesity, and has recently been
approved for the treatment of non-diabetic excess weight.
Semaglutide (both subcutaneous and oral formulation) is an
efficient and safe therapeutic approach for diabesity, with an
excellent cardiovascular profile. Regarding the microvascular
complications, potential for reducing diabetic nephropathy was
noted, with concerns regarding a possible worsening of diabetic
retinopathy, thus requiring further studies for clarification. The
perspective of oral semaglutide as an antiobesity drug is promising
and may be associated with increased treatment adherence. There is
still increased potential for further research to enhance and
optimize the use of semaglutide in diabesity and non-diabetic
obesity to reduce morbidity and mortality associated with these
metabolic disorders and to improve quality of life.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
MCT and RAT contributed to the design and conception
of the study. RAT and CN searched and consulted the relevant
literature, selected the studies/data and wrote the first draft of
the manuscript. MCT, AV and IT substantially added contributions by
revising and editing the final manuscript. All authors have read
and approved the final version of the manuscript. Data
authentication is not applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Hasanzad M, Sarhangi N, Nikfar S, Ostad SN
and Aghaei Meybodi HR: A narrative review of current trends in
liraglutide: Insights into the unmet needs in management of type 2
diabetes and obesity. J Diabetes Metab Disord. 19:1863–1872.
2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
World Health Organization (WHO): Obesity
and Overweight, 2020. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
Accessed April 21, 2021.
|
|
3
|
Gadde KM, Martin CK, Berthoud HR and
Heymsfield SB: Obesity: Pathophysiology and management. J Am Coll
Cardiol. 71:69–84. 2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Sims EA, Danforth E Jr, Horton ES, Bray
GA, Glennon JA and Salans LB: Endocrine and metabolic effects of
experimental obesity in man. Recent Prog Horm Res. 29:457–496.
1973.PubMed/NCBI View Article : Google Scholar
|
|
5
|
International Diabetes Federation: IDF
Diabetes Atlas-9th edition. http://www.diabetesatlas.org/(2019). Accessed April
21, 2021.
|
|
6
|
Zhang PY: Cardiovascular disease in
diabetes. Eur Rev Med Pharmacol Sci. 18:2205–2214. 2014.PubMed/NCBI
|
|
7
|
Cercato C and Fonseca FA: Cardiovascular
risk and obesity. Diabetol Metab Syndr. 11(74)2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Apovian CM, Okemah J and O'Neil PM: Body
weight considerations in the management of type 2 diabetes. Adv
Ther. 36:44–58. 2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
American Diabetes Association. 8. Obesity
management for the treatment of type 2 diabetes: Standards of
medical care in diabetes-2021. Diabetes Care. 44 (Suppl
1):S100–S110. 2021.PubMed/NCBI View Article : Google Scholar
|
|
10
|
American Diabetes Association. 9.
Pharmacologic approaches to glycemic treatment: Standards of
medical care in diabetes-2021. Diabetes Care. 44 (Suppl
1):S111–S124. 2021.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Herrmann C, Göke R, Richter G, Fehmann HC,
Arnold R and Göke B: Glucagon-like peptide-1 and glucose-dependent
insulin-releasing polypeptide plasma levels in response to
nutrients. Digestion. 56:117–126. 1995.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Müller TD, Finan B, Bloom SR, D'Alessio D,
Drucker DJ, Flatt PR, Fritsche A, Gribble F, Grill HJ, Habener JF,
et al: Glucagon-like peptide 1 (GLP-1). Mol Metab. 30:72–130.
2019.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Holst JJ: The physiology of glucagon-like
peptide 1. Physiol Rev. 87:1409–1439. 2007.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Drucker DJ: Glucagon-like peptide-1 and
the islet beta-cell: Augmentation of cell proliferation and
inhibition of apoptosis. Endocrinology. 144:5145–5148.
2003.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Lee YS and Jun HS: Anti-diabetic actions
of glucagon-like peptide-1 on pancreatic beta-cells. Metabolism.
63:9–19. 2014.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Tang-Christensen M, Vrang N and Larsen PJ:
Glucagon-like peptide containing pathways in the regulation of
feeding behaviour. Int J Obes Relat Metab Disord. 25 (Suppl
5):S42–S47. 2001.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Rinaman L: Ascending projections from the
caudal visceral nucleus of the solitary tract to brain regions
involved in food intake and energy expenditure. Brain Res.
1350:18–34. 2010.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Chilton R, Wyatt J, Nandish S, Oliveros R
and Lujan M: Cardiovascular comorbidities of type 2 diabetes
mellitus: Defining the potential of glucagonlike peptide-1-based
therapies. Am J Med. 124 (Suppl):S35–S53. 2011.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Nikolaidis LA, Mankad S, Sokos GG, Miske
G, Shah A, Elahi D and Shannon RP: Effects of glucagon-like
peptide-1 in patients with acute myocardial infarction and left
ventricular dysfunction after successful reperfusion. Circulation.
109:962–965. 2004.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Meier JJ, Gethmann A, Götze O, Gallwitz B,
Holst JJ, Schmidt WE and Nauck MA: Glucagon-like peptide 1
abolishes the postprandial rise in triglyceride concentrations and
lowers levels of non-esterified fatty acids in humans.
Diabetologia. 49:452–458. 2006.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Gutzwiller JP, Tschopp S, Bock A, Zehnder
CE, Huber AR, Kreyenbuehl M, Gutmann H, Drewe J, Henzen C, Goeke B
and Beglinger C: Glucagon-like peptide 1 induces natriuresis in
healthy subjects and in insulin-resistant obese men. J Clin
Endocrinol Metab. 89:3055–3061. 2004.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Nauck MA and Meier JJ: Management of
endocrine disease: Are all GLP-1 agonists equal in the treatment of
type 2 diabetes? Eur J Endocrinol. 181:R211–R234. 2019.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Nauck MA, Quast DR, Wefers J and Meier JJ:
GLP-1 receptor agonists in the treatment of type 2
diabetes-state-of-the-art. Mol Metab. 46(101102)2021.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Iepsen EW, Torekov SS and Holst JJ:
Liraglutide for type 2 diabetes and obesity: A 2015 update. Expert
Rev Cardiovasc Ther. 13:753–767. 2015.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Pandey A, Chawla S and Guchhait P: Type-2
diabetes: Current understanding and future perspectives. IUBMB
Life. 67:506–513. 2015.PubMed/NCBI View
Article : Google Scholar
|
|
26
|
Paley CA and Johnson MI: Abdominal obesity
and metabolic syndrome: Exercise as medicine? BMC Sports Sci Med
Rehabil. 10(7)2018.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Siddiqui S: Obesity and diabetes:
Interrelationship. Adv Obes Weight Manag Control. 8:155–158.
2018.
|
|
28
|
Nicola P, Ardeleanu E, Gadau C, Dorobantu
M, Darabont R, Tilea I, Varga A, Folescu R, Zamfir AS, Boanca M, et
al: Evaluation of biochemical and clinical parametres of
hypertension with type 2 diabetes mellitus. Rev Chim. 69:2402–2406.
2018.
|
|
29
|
Nolen-Doerr E, Stockman MC and Rizo I:
Mechanism of glucagon-like peptide 1 improvements in type 2
diabetes mellitus and obesity. Curr Obes Rep. 8:284–291.
2019.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Hinnen D: Glucagon-like peptide 1 receptor
agonists for type 2 diabetes. Diabetes Spectr. 30:202–210.
2017.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Sorli C, Harashima SI, Tsoukas GM, Unger
J, Karsbøl JD, Hansen T and Bain SC: Efficacy and safety of
once-weekly semaglutide monotherapy versus placebo in patients with
type 2 diabetes (SUSTAIN 1): A double-blind, randomised,
placebo-controlled, parallel-group, multinational, multicentre
phase 3a trial. Lancet Diabetes Endocrinol. 5:251–260.
2017.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Ahrén B, Masmiquel L, Kumar H, Sargin M,
Karsbøl JD, Jacobsen SH and Chow F: Efficacy and safety of
once-weekly semaglutide versus once-daily sitagliptin as an add-on
to metformin, thiazolidinediones, or both, in patients with type 2
diabetes (SUSTAIN 2): A 56-week, double-blind, phase 3a, randomised
trial. Lancet Diabetes Endocrinol. 5:341–354. 2017.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Ahmann AJ, Capehorn M, Charpentier G,
Dotta F, Henkel E, Lingvay I, Holst AG, Annett MP and Aroda VR:
Efficacy and safety of once-weekly semaglutide versus exenatide ER
in subjects with type 2 diabetes (SUSTAIN 3): A 56-week,
open-label, randomized clinical trial. Diabetes Care. 41:258–266.
2018.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Aroda VR, Bain SC, Cariou B, Piletič M,
Rose L, Axelsen M, Rowe E and DeVries JH: Efficacy and safety of
once-weekly semaglutide versus once-daily insulin glargine as
add-on to metformin (with or without sulfonylureas) in
insulin-naive patients with type 2 diabetes (SUSTAIN 4): A
randomised, open-label, parallel-group, multicentre, multinational,
phase 3a trial. Lancet Diabetes Endocrinol. 5:355–366.
2017.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Rodbard HW, Lingvay I, Reed J, de la Rosa
R, Rose L, Sugimoto D, Araki E, Chu PL, Wijayasinghe N and Norwood
P: Semaglutide added to basal insulin in type 2 diabetes (SUSTAIN
5): A randomized, controlled trial. J Clin Endocrinol Metab.
103:2291–2301. 2018.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Pratley RE, Aroda VR, Lingvay I, Lüdemann
J, Andreassen C, Navarria A and Viljoen A: SUSTAIN 7 investigators.
Semaglutide versus dulaglutide once weekly in patients with type 2
diabetes (SUSTAIN 7): A randomised, open-label, phase 3b trial.
Lancet Diabetes Endocrinol. 6:275–286. 2018.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Lingvay I, Catarig AM, Frias JP, Kumar H,
Lausvig NL, le Roux CW, Thielke D, Viljoen A and McCrimmon RJ:
Efficacy and safety of once-weekly semaglutide versus daily
canagliflozin as add-on to metformin in patients with type 2
diabetes (SUSTAIN 8): A double-blind, phase 3b, randomised
controlled trial. Lancet Diabetes Endocrinol. 7:834–844.
2019.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Zinman B, Bhosekar V, Busch R, Holst I,
Ludvik B, Thielke D, Thrasher J, Woo V and Philis-Tsimikas A:
Semaglutide once weekly as add-on to SGLT-2 inhibitor therapy in
type 2 diabetes (SUSTAIN 9): A randomised, placebo-controlled
trial. Lancet Diabetes Endocrinol. 7:356–367. 2019.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Capehorn MS, Catarig AM, Furberg JK, Janez
A, Price HC, Tadayon S, Vergès B and Marre M: Efficacy and safety
of once-weekly semaglutide 1.0 mg vs once-daily liraglutide 1.2 mg
as add-on to 1-3 oral antidiabetic drugs in subjects with type 2
diabetes (SUSTAIN 10). Diabetes Metab. 46:100–109. 2020.PubMed/NCBI View Article : Google Scholar
|
|
40
|
McCrimmon RJ, Catarig AM, Frias JP,
Lausvig NL, le Roux CW, Thielke D and Lingvay I: Effects of
once-weekly semaglutide vs once-daily canagliflozin on body
composition in type 2 diabetes: A substudy of the SUSTAIN 8
randomised controlled clinical trial. Diabetologia. 63:473–485.
2020.PubMed/NCBI View Article : Google Scholar
|
|
41
|
O'Neil PM, Birkenfeld AL, McGowan B,
Mosenzon O, Pedersen SD, Wharton S, Carson CG, Jepsen CH, Kabisch M
and Wilding JPH: Efficacy and safety of semaglutide compared with
liraglutide and placebo for weight loss in patients with obesity: A
randomised, double-blind, placebo and active controlled,
dose-ranging, phase 2 trial. Lancet. 392:637–649. 2018.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Wilding JPH, Batterham RL, Calanna S,
Davies M, Van Gaal LF, Lingvay I, McGowan BM, Rosenstock J, Tran
MTD, Wadden TA, et al: Once-weekly semaglutide in adults with
overweight or obesity. N Engl J Med. 384:989–1002. 2021.PubMed/NCBI View Article : Google Scholar
|
|
43
|
U.S. Food and Drug Administration: FDA
Approves New Drug Treatment for Chronic Weight Management: First
Since 2014. https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-treatment-chronic-weight-management-first-2014.
Accessed June 25, 2021.
|
|
44
|
Davies M, Færch L, Jeppesen OK, Pakseresht
A, Pedersen SD, Perreault L, Rosenstock J, Shimomura I, Viljoen A,
Wadden TA, et al: Semaglutide 2·4 mg once a week in adults with
overweight or obesity, and type 2 diabetes (STEP 2): A randomised,
double-blind, double-dummy, placebo-controlled, phase 3 trial.
Lancet. 397:971–984. 2021.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Wadden TA, Bailey TS, Billings LK, Davies
M, Frias JP, Koroleva A, Lingvay I, O'Neil PM, Rubino DM, Skovgaard
D, et al: Effect of subcutaneous semaglutide vs placebo as an
adjunct to intensive behavioral therapy on body weight in adults
with overweight or obesity: The STEP 3 randomized clinical trial.
JAMA. 325:1403–1413. 2021.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Rubino D, Abrahamsson N, Davies M, Hesse
D, Greenway FL, Jensen C, Lingvay I, Mosenzon O, Rosenstock J,
Rubio MA, et al: Effect of continued weekly subcutaneous
semaglutide vs placebo on weight loss maintenance in adults with
overweight or obesity: The STEP 4 randomized clinical trial. JAMA.
325:1414–1425. 2021.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Aroda VR, Rosenstock J, Terauchi Y,
Altuntas Y, Lalic NM, Morales Villegas EC, Jeppesen OK,
Christiansen E, Hertz CL and Haluzík M: PIONEER 1 Investigators.
PIONEER 1: Randomized clinical trial of the efficacy and safety of
oral semaglutide monotherapy in comparison with placebo in patients
with type 2 diabetes. Diabetes Care. 42:1724–1732. 2019.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Rodbard HW, Rosenstock J, Canani LH,
Deerochanawong C, Gumprecht J, Lindberg SØ, Lingvay I, Søndergaard
AL, Treppendahl MB and Montanya E: PIONEER 2 Investigators. Oral
semaglutide versus empagliflozin in patients with type 2 diabetes
uncontrolled on metformin: The PIONEER 2 trial. Diabetes Care.
42:2272–2281. 2019.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Pratley R, Amod A, Hoff ST, Kadowaki T,
Lingvay I, Nauck M, Pedersen KB, Saugstrup T and Meier JJ: PIONEER
4 investigators. Oral semaglutide versus subcutaneous liraglutide
and placebo in type 2 diabetes (PIONEER 4): A randomised,
double-blind, phase 3a trial. Lancet. 394:39–50. 2019.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Yabe D, Nakamura J, Kaneto H, Deenadayalan
S, Navarria A, Gislum M and Inagaki N: PIONEER 10 Investigators.
Safety and efficacy of oral semaglutide versus dulaglutide in
Japanese patients with type 2 diabetes (PIONEER 10): An open-label,
randomised, active-controlled, phase 3a trial. Lancet Diabetes
Endocrinol. 8:392–406. 2020.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Marso SP, Bain SC, Consoli A, Eliaschewitz
FG, Jódar E, Leiter LA, Lingvay I, Rosenstock J, Seufert J, Warren
ML, et al: Semaglutide and cardiovascular outcomes in patients with
type 2 diabetes. N Engl J Med. 375:1834–1844. 2016.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Górriz JL, Soler MJ, Navarro-González JF,
García-Carro C, Puchades MJ, D'Marco L, Martínez Castelao A,
Fernández-Fernández B, Ortiz A, Górriz-Zambrano C, et al: GLP-1
receptor agonists and diabetic kidney disease: A call of attention
to nephrologists. J Clin Med. 9(947)2020.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Jódar E, Michelsen M, Polonsky W, Réa R,
Sandberg A, Vilsbøll T, Warren M, Harring S, Ziegler U and Bain S:
Semaglutide improves health-related quality of life versus placebo
when added to standard of care in patients with type 2 diabetes at
high cardiovascular risk (SUSTAIN 6). Diabetes Obes Metab.
22:1339–1347. 2020.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Husain M, Birkenfeld AL, Donsmark M,
Dungan K, Eliaschewitz FG, Franco DR, Jeppesen OK, Lingvay I,
Mosenzon O, Pedersen SD, et al: Oral semaglutide and cardiovascular
outcomes in patients with type 2 diabetes. N Engl J Med.
381:841–851. 2019.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Hardy T, Oakley F, Anstee QM and Day CP:
Nonalcoholic fatty liver disease: Pathogenesis and disease
spectrum. Annu Rev Pathol. 11:451–496. 2016.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Non-alcoholic Fatty Liver Disease Study
Group. Lonardo A, Bellentani S, Argo CK, Ballestri S, Byrne CD,
Caldwell SH, Cortez-Pinto H, Grieco A, Machado MV, et al:
Epidemiological modifiers of non-alcoholic fatty liver disease:
Focus on high-risk groups. Dig Liver Dis. 47:997–1006.
2015.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Hazlehurst JM, Woods C, Marjot T, Cobbold
JF and Tomlinson JW: Non-alcoholic fatty liver disease and
diabetes. Metabolism. 65:1096–1108. 2016.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Mantovani A, Scorletti E, Mosca A, Alisi
A, Byrne CD and Targher G: Complications, morbidity and mortality
of nonalcoholic fatty liver disease. Metabolism.
111S(154170)2020.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Lonardo A, Mantovani A, Lugari S and
Targher G: Epidemiology and pathophysiology of the association
between NAFLD and metabolically healthy or metabolically unhealthy
obesity. Ann Hepatol. 19:359–366. 2020.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Younossi ZM: Non-alcoholic fatty liver
disease-A global public health perspective. J Hepatol. 70:531–544.
2019.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Tarantino G, Citro V and Capone D:
Nonalcoholic fatty liver disease: A challenge from mechanisms to
therapy. J Clin Med. 9(15)2019.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Tarantino G and Balsano C:
Gastrointestinal peptides and nonalcoholic fatty liver disease.
Curr Opin Endocrinol Diabetes Obes. 27:11–15. 2020.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Lv X, Dong Y, Hu L, Lu F, Zhou C and Qin
S: Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) for the
management of nonalcoholic fatty liver disease (NAFLD): A
systematic review. Endocrinol Diabetes Metab.
3(e00163)2020.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Mantovani A, Petracca G, Beatrice G,
Csermely A, Lonardo A and Targher G: Glucagon-like peptide-1
receptor agonists for treatment of nonalcoholic fatty liver disease
and nonalcoholic steatohepatitis: An updated meta-analysis of
randomized controlled trials. Metabolites. 11(73)2021.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Newsome PN, Buchholtz K, Cusi K, Linder M,
Okanoue T, Ratziu V, Sanyal AJ, Sejling AS and Harrison SA:
NN9931-4296 Investigators. A placebo-controlled trial of
subcutaneous semaglutide in nonalcoholic steatohepatitis. N Engl J
Med. 384:1113–1124. 2021.PubMed/NCBI View Article : Google Scholar
|
|
66
|
European Medicines Agency: Ozempic:
summary of product characteristics; 2018. https://www.ema.europa.eu/en/documents/product-information/ozempic-epar-product-information_en.pdf.
Accessed April 24, 2021.
|
|
67
|
Gomez-Peralta F and Abreu C: Profile of
semaglutide in the management of type 2 diabetes: Design,
development, and place in therapy. Drug Des Devel Ther. 13:731–738.
2019.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Trujillo JM, Nuffer W and Ellis SL: GLP-1
receptor agonists: A review of head-to-head clinical studies. Ther
Adv Endocrinol Metab. 6:19–28. 2015.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Trujillo JM, Nuffer W and Smith BA: GLP-1
receptor agonists: An updated review of head-to-head clinical
studies. Ther Adv Endocrinol Metab.
12(2042018821997320)2021.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Shi FH, Li H, Cui M, Zhang ZL, Gu ZC and
Liu XY: Efficacy and safety of once-weekly semaglutide for the
treatment of type 2 diabetes: Protocol for a systematic review and
meta-analysis. Medicine (Baltimore). 97(e0420)2018.PubMed/NCBI View Article : Google Scholar
|
|
71
|
Røder ME: Clinical potential of treatment
with semaglutide in type 2 diabetes patients. Drugs Context.
8(212585)2019.PubMed/NCBI View Article : Google Scholar
|
|
72
|
Bjerre Knudsen L, Madsen LW, Andersen S,
Almholt K, de Boer AS, Drucker DJ, Gotfredsen C, Egerod FL,
Hegelund AC, Jacobsen H, et al: Glucagon-like Peptide-1 receptor
agonists activate rodent thyroid C-cells causing calcitonin release
and C-cell proliferation. Endocrinology. 151:1473–1486.
2010.PubMed/NCBI View Article : Google Scholar
|
|
73
|
Prasad-Reddy L and Isaacs D: A clinical
review of GLP-1 receptor agonists: Efficacy and safety in diabetes
and beyond. Drugs Context. 4(212283)2015.PubMed/NCBI View Article : Google Scholar
|
|
74
|
Sfairopoulos D, Liatis S, Tigas S and
Liberopoulos E: Clinical pharmacology of glucagon-like peptide-1
receptor agonists. Hormones. 17:333–350. 2018.PubMed/NCBI View Article : Google Scholar
|
|
75
|
Lando HM, Alattar M and Dua AP: Elevated
amylase and lipase levels in patients using glucagonlike peptide-1
receptor agonists or dipeptidyl-peptidase-4 inhibitors in the
outpatient setting. Endocr Pract. 18:472–477. 2012.PubMed/NCBI View Article : Google Scholar
|
|
76
|
Abd El Aziz M, Cahyadi O, Meier JJ,
Schmidt WE and Nauck MA: Incretin-based glucose-lowering
medications and the risk of acute pancreatitis and malignancies: A
meta-analysis based on cardiovascular outcomes trials. Diabetes
Obes Metab. 22:699–704. 2020.PubMed/NCBI View Article : Google Scholar
|
|
77
|
Diabetes Control and Complications Trial
Research Group. Nathan DM, Genuth S, Lachin J, Cleary P, Crofford
O, Davis M, Rand L and Siebert C: The effect of intensive treatment
of diabetes on the development and progression of long-term
complications in insulin-dependent diabetes mellitus. N Engl J Med.
329:977–986. 1993.PubMed/NCBI View Article : Google Scholar
|
|
78
|
Gorman DM, le Roux CW and Docherty NG: The
effect of bariatric surgery on diabetic retinopathy: Good, bad, or
both? Diabetes Metab J. 40:354–364. 2016.PubMed/NCBI View Article : Google Scholar
|
|
79
|
American Diabetes Association. 14.
management of diabetes in pregnancy: Standards of medical care in
diabetes-2021. Diabetes Care. 44 (Suppl 1):S200–S210.
2021.PubMed/NCBI View Article : Google Scholar
|
|
80
|
Kelly AS, Auerbach P, Barrientos-Perez M,
Gies I, Hale PM, Marcus C, Mastrandrea LD, Prabhu N and Arslanian
S: NN8022-4180 Trial Investigators. A Randomized, controlled trial
of liraglutide for adolescents with obesity. N Engl J Med.
382:2117–2128. 2020.PubMed/NCBI View Article : Google Scholar
|
|
81
|
Enebo LB, Berthelsen KK, Kankam M, Lund
MT, Rubino DM, Satylganova A and Lau DCW: Safety, tolerability,
pharmacokinetics, and pharmacodynamics of concomitant
administration of multiple doses of cagrilintide with semaglutide
2·4 mg for weight management: A randomised, controlled, phase 1b
trial. Lancet. 397:1736–1748. 2021.PubMed/NCBI View Article : Google Scholar
|
|
82
|
Nauck MA and Quast DR: Cardiovascular
safety and benefits of semaglutide in patients with type 2
diabetes: Findings from SUSTAIN 6 and PIONEER 6. Front Endocrinol
(Lausanne). 12(645566)2021.PubMed/NCBI View Article : Google Scholar
|
|
83
|
ClinicalTrials.gov NCT03914326: A heart disease study
of semaglutide in patients with type 2 diabetes (SOUL). https://clinicaltrials.gov/ct2/show/NCT03914326.
Accessed July 10, 2021.
|