Introduction
Atopic dermatitis (AD) is a complex disease
(1) caused by numerous
environmental factors, such as stress from various types of
environmental pollution, immunological factors (2), including increased serum
immunoglobulin-E (IgE) levels and imbalance between T helper type 1
(Th1) and Th2 cells, and genetic factors (3,4). Th2
cells secrete cytokines, including interleukin (IL)-4, IL-5, IL-6,
and IL-10, and are therefore involved in humoral immunity, while
Th1 cells secrete interferon (IFN)-γ and IL-2, which are involved
in cellular immunity. In AD, the levels of IL-4, IL-6 and tumor
necrosis factor-α (TNF-α) tend to increase, whereas IFN-γ level
tends to decrease (5). Furthermore,
the number of Langerhans cells and activation of mast cells are
increased in AD (6).
The main treatments for AD include local steroids,
antihistamine creams and immunomodulators. Furthermore, IFN-γ-based
drugs and immunosuppressants are typically administered. However,
previous studies have focused on phototherapy, including UV
phototherapy and infrared light emitting diode therapy (5,7-11).
Low-level laser (LLL) therapy (LLLT), which is a
method using phototherapy, uses low power (≤500 mW) and produces
minimal heat. Its therapeutic effect is mainly driven by the
stimulation of cells with photo-energy (12,13).
In addition, unlike sunlight, LLLT has a narrow wavelength
bandwidth, allowing emission from a specific light source to be
directed onto a focused and localized area. This technique is
therefore effective for the treatment of a specific area.
The effects of LLLT in human tissues are mainly
driven by the absorption of energy by specific photoreceptors, such
as porphyrin and cytochrome c oxidase. Absorption of energy by
these receptors promotes intracellular oxygen synthesis,
mitochondrial ATP synthesis, chemiosmosis, DNA replication and
infiltration of Ca2+ into the cell cytoplasm (14). These effects subsequently promote
cell proliferation and migration, increase tissue oxygenation and
control cytokine concentration, growth factors and inflammation
(12,15). Furthermore, LLLT treatment increases
blood flow to regenerate tissues, provides tension to the skin by
promoting collagen production by fibroblasts, promotes cell
division to stimulate cell growth, promotes bone regeneration and
rearrangement, corrects abnormal hormones level and reduces pain
(15-17).
Based on these effects, numerous studies have reported that laser
therapy displays some positive effects on several musculoskeletal
diseases, rheumatoid arthritis, post-herpetic neuralgia, pain,
inflammation, edema, cut wounds, nerve damage and neural
regeneration (18-26).
Previous studies have examined the use of laser
therapy in the treatment of AD (18,27-32).
However, these studies used different types of laser and dosages
and only demonstrated that laser therapy is clinically effective
against AD. To the best of our knowledge, only few studies have
thoroughly assessed the underlying mechanism of laser therapy
therapeutic effect and suggested an optimal dosage.
The present study aimed to investigate the effects
of LLLT on AD using clinical skin severity testing, scratch
testing, total serum IgE and IL-4 level evaluation, as well as
examined the gene expression of various cytokines (IL-4, IL-6,
TNF-α, IFN-γ), epidermal thickness and mast cell counts.
Materials and methods
Animals
All experimental procedures and animal handling were
performed following approval from the animal research ethics board
of Sahmyook University (approval no. SYUIACUC2017-004). A total of
71 4-week-old BALB/c mice (weight, 16-18 g) were purchased from the
laboratory animal center of Hallym Co. (Gyeonggi, South Korea).
Mice were acclimatized for seven days in the animal room at the
Center for Neurological Sciences, Sahmyook University. Animals had
free access to food and water, and the temperature, humidity and
day-night cycle were automatically controlled at 23±2˚C, 55±10% and
a 12-h cycle, respectively.
Sensitization and challenge
The backs of all the mice were shaved clean and a
24-h recovery period was provided for the micro-wounds on the skin
to heal. To induce AD, compound 1-chloro-2,4-di-nitrobenzene (DNCB;
Sigma-Aldrich; Merck KGaA) solution (at 2.5%) was prepared by
mixing acetone and olive oil in a 3:1 ratio to which DNCB was
added. The compound DNCB solution (200 µl; volume given on day 1)
was applied to the backs of the mice to induce immune responses.
From day 3, 1.0% DNCB solution (150 µl) was applied once every
three days, and eschar formation and more severe scratching were
observed by the second application of the solution. The eschars
started to fall off after the fourth application and had completely
disappeared before the fifth application when AD was observed. At
this time point, physical intervention with a LLL was initiated. To
prevent natural healing while LLLT was performed, 1.0% DNCB
solution (150 µl) was applied to the backs of the mice once every
three days (33,34).
LLL irradiation
A diode laser therapy instrument (StraTek Co., Ltd.)
at a wavelength of 650 nm and power of 50 mW was used for LLLT. The
laser was emitted at a minimum intensity of 2 J/cm2 and
a maximum intensity of 8 J/cm2. The scanning method was
used for laser emission by setting the scanning speed to ‘fast’ in
order to reproduce the same effect as that of a continuous laser
emission.
An area of 3 cm2 on the back of each
mouse was treated, and the energy density (J/cm2) was
calculated from the laser output (W), duration (sec) and
therapeutic area (J/cm2) as follows (35): Energy density=(laser output x
duration)/therapeutic area.
There were six different groups in total. In the
normal control group (n=8), only the solvent (acetone and olive oil
mix in a 3:1 ratio; 200 µl) was applied to the backs of the mice.
The five experiment groups were the following: One control group
with induced AD (n=10) and four experimental groups with induced AD
followed by treatment with LLLT at difference energy density [Laser
2 at 2 J/cm2 (n=10); Laser 4 at 4 J/cm2
(n=10); Laser 6 at 6 J/cm2 (n=9); and Laser 8 at 8
J/cm2 (n=10)]. Laser therapy was administered daily for
two weeks (14 times in total).
Clinical skin severity test
Sensory evaluation is a clinical assessment
involving physical examination. In total, two researchers performed
this evaluation, and if there were differences, the results was
determined via discussion. The outcome was represented as the sum
of scores from five different categories. These five categories
include erythema, pruritus and dry skin, edema and excoriation,
erosion and lichenification. For each category, appropriate
evaluation was performed and a score was assigned as follows: None
(0), weak (1), intermediate (2) and severe (3). Subsequently, the
final score ranged from 0 to 15 (36,37).
After five applications of DNCB solution (150 µl), a
clinical skin severity test of the mice was performed. A total of
13 mice with sensory evaluation scores of ≤12 points were then
excluded.
An LLL was emitted, at a wavelength of 650 nm and
power of 50 mW, 14 times in total over a 2-week period. Each group
were exposed to each particular duration only (for 2, 4, 6 and 8
min each time/day). Sensory evaluation (clinical skin severity
test) and a scratch test were performed at the following time
points: Before therapy and at days 1, 3, 7 and 14 of therapy. On
day 14 of therapy, the experiment was complete, and the mice were
sacrificed via cervical dislocation after anesthesia. The serum
levels of IgE and IL-4 and the mRNA expression of IL-4, IL-6, TNF-α
and IFN-γ were then evaluated. Finally, the tissues were stained
using hematoxylin and eosin (H&E) and toluidine blue to
evaluate the tissue condition and mast cell count.
Scratch test
Scratching behavior was observed and the numbers of
scratching episodes counted for 14 days. Scratching was evaluated
using a slightly modified version of the traditional method, which
was performed for 1 h from 30 min before and after application of
the test substance (37,38). The number of scratching movements
made by the mice was measured during a 60-min time period before
LLLT, a 30-min time period after LLLT, a 30-min time period after
stabilization and a 30-min time period after 24 h on days 1, 3, 7
and 14 of LLLT.
Measurement of serum IgE and IL-4
levels
On the last day of the experiment, 0.6-0.8 ml of
mouse blood was collected by cardiac puncture after euthanasia and
left at room temperature to allow blood coagulation. The sample was
centrifuged (-18˚C) at 1,000 x g for 7 min, and the separated serum
was stored at -80˚C.
IgE and IL-4 concentrations in mouse serum were
measured by ELISA. Mouse IgE and IL-4 ELISA kits (cat. nos. 555248
and 555232; BD OptEIA™; BD Biosciences) were provided by BD
Pharmingen; BD Biosciences. The ELISA plates were coated with
coating buffer that contains the capture antibody, one day before
the experiment. On the day of the experiment, the plate was washed
with washing buffer containing 0.05% Tween-20 in PBS. The plates
were blocked with PBS containing 10% FBS (cat. no. FBS001-HI,
Sigma-Aldrich; Merck KGaA). After additional washing with the
washing buffer, 100 µl of standard IgE and mouse serum were added
into each well. After incubation at room temperature for 2 h, the
plate was washed, the detection antibody solution was added and the
plate was incubated at room temperature for an additional 1 h for
the reaction to occur. After the final wash with washing buffer,
the substrate solution was added, and the plate was incubated in
the dark. After 30 min, the color was confirmed and 2 N sulfuric
acid was added to stop the reaction. The optical density was
measured at 450 nm on an ELISA plate reader to determine the
concentrations of IgE and IL-4.
Weight of spleen
At the end of the experiment, the mice were
sacrificed by cervical dislocation and the spleen was extracted.
The weight of the spleen was evaluated using an Electronic Scale
(cat. no. CP224S; Sartorius AG) (33,39)
and tissues were stored at -80˚C.
Reverse transcription-quantitative
(RT-q)PCR
The mRNA expression of IL-4, IL-6, TNF-α, and IFN-γ
was evaluated in spleen tissues by RT-qPCR as previously described
(40). Spleen tissues stored at
-80˚C were thawed on ice and homogenized in an e-tube containing 1
ml Total RNA isolation solution (RiboEX™; GeneAll
Biotechnology Co., Ltd.) using a homogenizer. Gene extraction
solution (GeneAll®Hybrid-R™; GeneAll
Biotechnology Co., Ltd.) was used to extract RNA from the tissues.
The concentration of extracted RNA was measured with a NanoDrop
ND-1,000 Spectrometer (NanoDrop products), and cDNA was obtained
using AccuPower® CycleScript RT PreMix (Bioneer
Corporation). Samples were stored at -80˚C until further analysis.
RT-qPCR was run using SYBR® Green (SolGent Co., Ltd.).
RT-qPCR was performed. The sequences of the primers used are
presented in Table I. The relative
expression levels were normalized to endogenous control and were
expressed as 2-ΔΔCq (41).
 | Table ISequence of the primers used for
reverse transcription-quantitative PCR. |
Table I
Sequence of the primers used for
reverse transcription-quantitative PCR.
| Gene | Sequences |
|---|
| IL-4 | |
|
Forward |
5'-AAGAACACCACAGAGAGTGAGCTC-3' |
|
Reverse |
5'-TTTCAGTGATGTGGACTTGGACTC-3' |
| IL-6 | |
|
Forward |
5'-CAAGAGACTTCCATCCAGTTGC-3' |
|
Reverse |
5'-TTGCCGAGTAGATCTCAAAGTGAC-3' |
| TNF-α | |
|
Forward |
5'-ATGAGCACAGAAAGCATGATC-3' |
|
Reverse |
5'-TACAGGCTTGTCACTGGAATT-3' |
| IFN-γ | |
|
Forward |
5'-GCCATCAGCAACAACATAAGCGTC-3' |
|
Reverse |
5'-CCACTCGGATGAGCTCATTGAATG-3' |
| GAPDH | |
|
Forward |
5'-GAGGGGCCATCCACAGTCTTC-3' |
|
Reverse |
5'-CATCACCATCTTCCAGGAGCG-3' |
Histopathological analysis of mast
cells and tissues
As soon as mice were sacrificed and at the end of
the full protocol, mouse skin tissues from the lesions were
biopsied from the backs of mice. To ensure that skin biopsies were
performed at identical positions in all mice, the biopsies were
collected from an area (1.5x1.5 cm2) immediately above
the line dividing the back of the mouse in half. Fixed tissues in
10% formalin (18-20˚C, 2 days) were embedded in paraffin and 5
µm-thick blocks were prepared. H&E staining was subsequently
performed to identify edema and measure the epidermal thickness in
different tissues. Toluidine blue staining was also used to
identify mast cells and to observe any potential infiltration of
mast cells into the tissues. The number of mast cells that were
stained by toluidine blue within one square of the grid lines
(magnification, x40 and x100, HNM005 HiMaxthe®) was
counted and the value was represented as cell count/mm2
(42). When mast cells are
activated, substances contained in granules, such as histamine, are
degranulated, and lipid mediators such as cytokines, prostaglandins
and leukotriene, are newly synthesized and secreted. These
substances cause symptoms such as vasodilation, extravasation of
white blood cells and inflammatory reactions (43). Therefore, the current experiment
observed the number of granulated cells and degranulated cells.
Statistical analysis
All data were presented as the means ± standard
error of the mean. For evaluations involving temporal variables,
including sensory evaluation and scratch test, two-way mixed
repeated ANOVA was used followed by Bonferroni post hoc test.
One-way ANOVA followed by Dunnett's post hoc test was used to
compare the weights of the spleen and levels of IgE, IL-4, IL-6,
TNF-α and IFN-γ between different groups. P<0.05 was considered
to indicate a statistically significant difference. All statistical
analyses were performed using GraphPad Prism software version 5.02
(GraphPad Software, Inc.).
Results
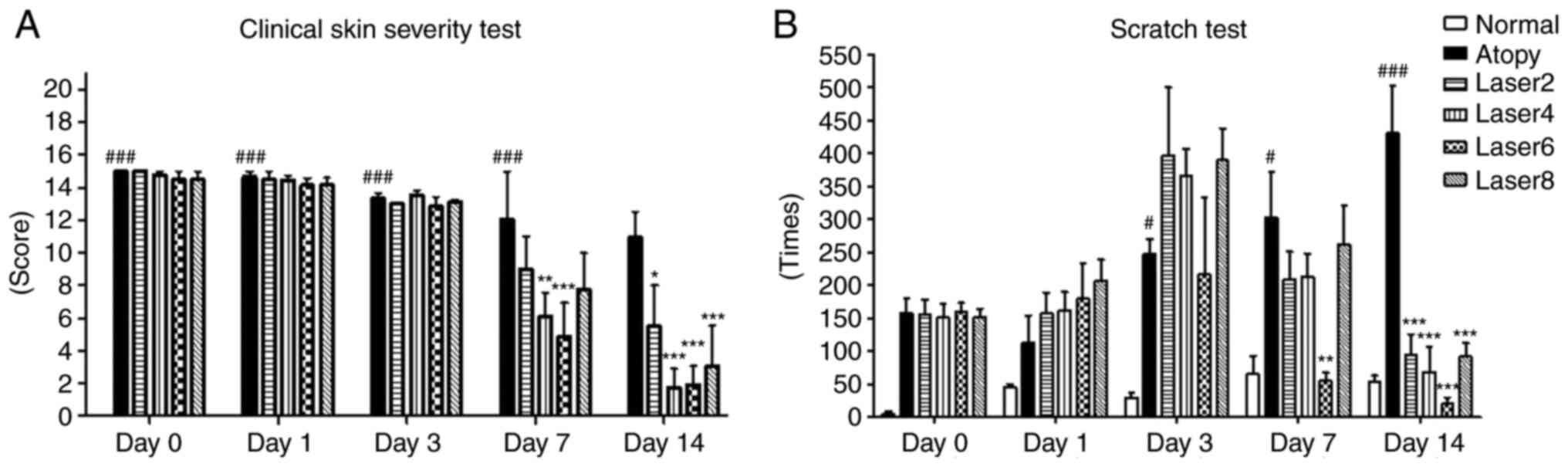
Effects of LLLT on the clinical skin
severity and scratch tests
To understand the effects of LLL irradiation on
sensory evaluation and scratching, mice were evaluated using a
clinical skin severity test and a scratch test before LLLT and on
days 1, 3, 7 and 14 of LLLT. From day 7 of LLLT, decrease in the
clinical skin severity test in the Laser 4 (P<0.01) and Laser 6
groups (P<0.001) compared with the AD group was observed.
Furthermore on day 7 of LLLT mice in the Laser 6 group showed
significantly reduced scratching compared with the atopy group
(P<0.01). By day 14, all experimental groups exhibited
significant decrease in scratching and the clinical skin severity
test compared with the AD group (P<0.001; Fig. 1).
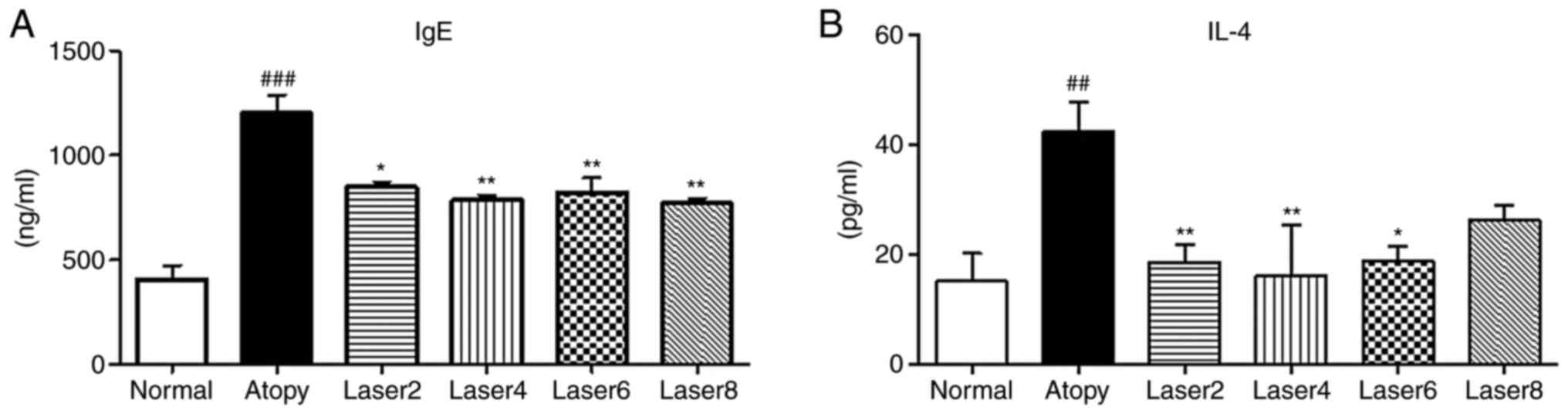
Effects of LLLT on serum IgE and IL-4
concentrations
We measured the serum concentrations of IgE and IL-4
using ELISA in experimental mice with induced AD. In the AD control
group, IgE concentration was significantly increased compared with
normal control group (P<0.001). In addition, IgE concentration
was significantly decreased in the experimental groups treated with
LLLT compared with AD control group (Fig. 2A). Similarly, IL-4 concentration in
the AD control group was significantly elevated compared with
normal control group (P<0.01). Furthermore, IL-4 level was
significantly decrease in all experimental groups treated with LLLT
compared with AD control group (P<0.01; Fig. 2B).
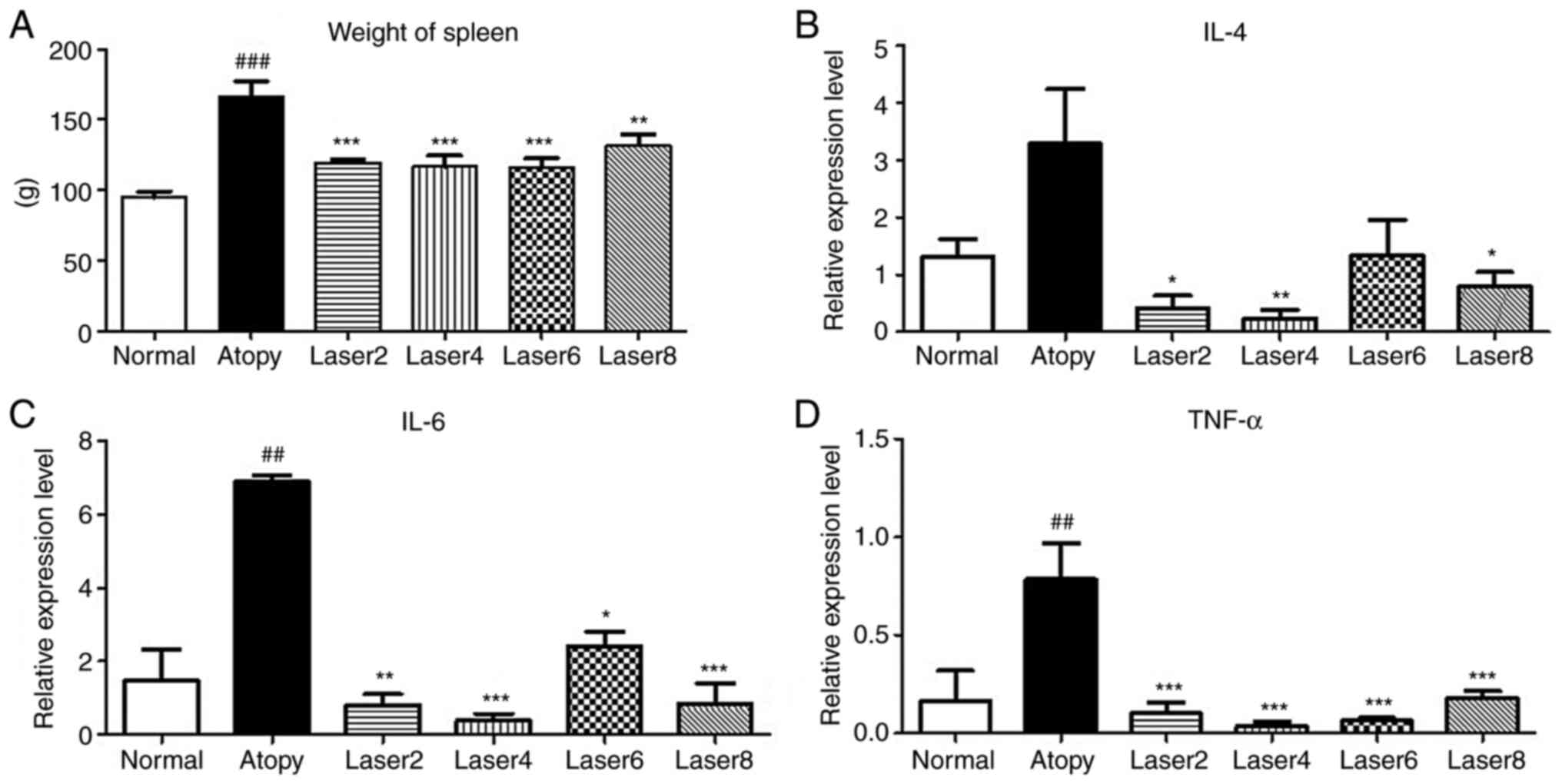
Weight of spleen
The weight of the spleen was measured at the end of
the experiments to determine the effect of LLL on the immunization
of laboratory animals caused by AD. The results demonstrated that
the weight of spleen was significantly increased in the AD group
compared with normal group (P<0.001). In addition, the
experimental groups Laser 2 (P<0.001), Laser 4 (P<0.001),
Laser 6 (P<0.001) and Laser 8 J/cm2 (P<0.01)
exhibited significantly decreased spleen weight compared with AD
control group (Fig. 3A).
Effects of LLLT on the mRNA expression
of IL-4, IL-6, TNF-α and IFN-γ
The expression levels of IL-4, IL-6, TNF-α and IFN-γ
in experimental mice with induced AD were assessed using RT-qPCR.
IL-6 and TNF- α expression levels in AD group were significantly
increased compared with normal group. Moreover, IL-4 expression
levels in AD group were not significantly increased compared with
normal group, but IL-4 expression was significantly decreased in
all experimental groups compared with AD group, except Laser 6
(Fig. 3B). IL-6 and TNF-α
expression was significantly decreased in all experimental groups
compared with AD group (Fig. 3C and
D).
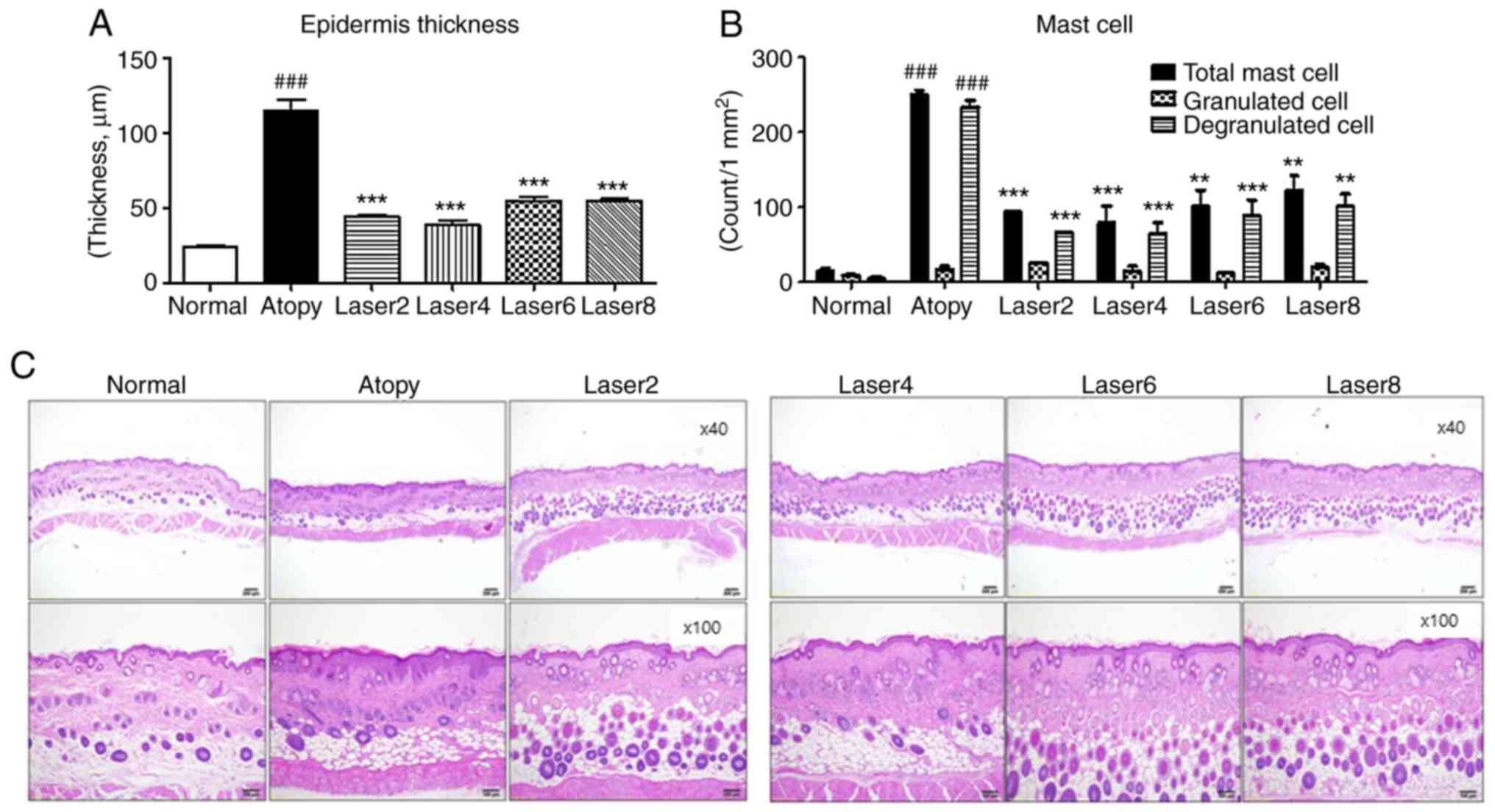
Effects of LLLT on skin tissue
Changes in epidermal thickness, structure and number
of mast cells in mouse tissues are presented in Fig. 4. The epidermal thickness was
determined in all tissues. The results revealed a significant
increase in epidermal thickness in the AD control group compared
with the normal group (P<0.001). Furthermore, all experimental
groups treated with LLLT exhibited significantly reduced epidermal
thickness compared with the AD group (P<0.001). Furthermore,
according to results from H&E staining, the AD group showed
increased epidermal and dermal thickness, as well as markedly
increased hyperkeratinization near the lesion, compared with the
normal group. Furthermore, the experimental groups treated with
LLLT showed decreased epidermal and dermal thickness similar to
that of the normal group, and the hyperkeratinization was
improved.
The total number of mast cells, granulated and
degranulated cells within an area of 1 mm2 of the
tissues was subsequently assessed in all tissues. The results
demonstrated that the total number of mast cells in the
experimental groups treated with LLLT was significantly lower
compared with that in the AD group (P<0.001). The number of
granulated cells in the AD control group was slightly higher than
that in the normal group. The experimental groups treated with LLLT
presented similar numbers of granulated cells to that in the AD
group. The number of degranulated cells in the AD group was
significantly increased compared with the normal group
(P<0.001). In addition, the experimental groups treated with
LLLT exhibited a significantly decreased number of degranulated
cells compared with the AD control group (P<0.001).
Discussion
The effects of LLLT on relieving the symptoms of
dermatitis have been previously demonstrated in clinical settings
(17,44). The present study attempted therefore
to confirm the curative effect of a ‘designed’ energy irradiation
dose of LLL towards AD.
The wavelength used in the present study was 650 nm,
which is within the range of suggested wavelengths (630-660 nm) for
inflammation therapy (45). It has
been reported that LLL at 1-6 J/cm2 is effective against
acute and subacute inflammations, while LLL at 4-8 J/cm2
is effective against chronic inflammations, such as atopic
dermatitis and arthritis (35).
According to the World Association for Laser Therapy, the red
wavelength doses used for superficial diseases tend to be ~4
J/cm2 (32). The present
study used therefore laser outputs of 2, 4, 6 and 8
J/cm2.
In the present study, the results from sensory
evaluation, which evaluates the therapeutic effectiveness by
assigning scores to different symptoms of AD, demonstrated that
after 7 days of LLLT, the experimental groups treated with LLLT
exhibited significantly decreased symptoms compared with the AD
group.
In the present study, a scratch test was performed
following treatment with LLLT. The results demonstrated that the AD
group exhibited increased scratching from day 3. All experimental
groups treated with LLLT exhibited increased scratching on day 3,
followed by significantly decreased scratching on days 7 and 14
compared with the AD group. The smallest decrease in scratching was
observed in the Laser 6 group.
In the present study, the onset of AD was confirmed
by changes in serum IgE and IL-4 concentrations. In previous
studies, it was demonstrated that LLLT can suppress the induction
of AD (1,32,36).
In addition, IL-4 serum concentration in mice with induced AD was
significantly elevated compared with that in mice in the normal
group. These findings were similar to previous studies, which
demonstrated that the level of the Th2 cell cytokine IL-4 is
elevated in patients with AD (1,6,36). In
the present study, except for the Laser 8 group, all experimental
groups treated with LLLT, showed significant reduction in serum
IL-4 concentration compared with the AD group. The Laser 4 group
exhibited the most efficient reduction. These findings indicated
that laser therapy was effective for relieving symptoms of AD.
As described in previous studies (33,39),
the weight of spleen in the present study was measured and the
immune response in mice with AD was analyzed. The results
demonstrated that mice in the AD groups had increased spleen
weight. However, the weight of spleen decreased significantly in
all laser irradiation groups compared with than in the AD group,
Increased spleen weight is associated with increased T lymphocytes.
However, a decreased weight means a decrease in inflammatory
reactions by T lymphocytes (39).
Thus, these findings suggested that LLLT may have an effect on
immunity.
Subsequently, the expression of some mRNA was
assessed in spleen tissues. In humans, ~10-15% of the lymphocytes
in the blood, ~20-25% of the lymphocytes in the lymph nodes and
~40-45% of the lymphocytes in the spleen cells are B cells
(46); the spleen has therefore the
largest amount of lymphocytes. If taken from the blood, cytokines,
represented by white blood cells, may also be sensitive to
differences in blood collection or sample manipulation methods
(47). Quantitative analysis of
cytokine mRNA expression levels suggests that these cytokines can
be considered as potential sensitive markers for determination of
the state of immune cell activation (48). In present study, total RNA was
extracted from the spleen tissues of each group, and the mRNA
expression of IL-4, IL-6 and TNF-α (factors of Th 2 immune
response) and IFN-γ (factor of Th1 immune response) was evaluated.
Th1 and Th2 cells maintain immune balance, where IL-4 suppresses
the Th1 type reaction and IFN-γ suppresses the Th2 type reaction
(1). T-cells in patients with AD
have decreased ability to produce IFN-γ and are highly reactive to
IL-4, which is thought to be the main reason for immune response by
type Th2 cells in AD (1). The
present study assessed the mRNA expression of IL-4, IL-6, TNF-α and
IFN-γ (data not shown) after LLLT treatment. The expression levels
of IL-4, IL-6 and TNF-α were significantly increased in the AD
group, which has been previously described (3-6).
Since IL-4 is the cytokine responsible for IgE release in AD,
patients with AD exhibit elevated levels of IL-4. In addition,
increased IL-6 and TNF-α levels in AD have been reported in several
studies (1,6,8,9,45,49,50).
Subsequently, the increased mRNA expression of these cytokines
described in the present study indicated that AD was successfully
induced. Furthermore, following LLLT treatment, the expression
level of IL-4 was significantly decreased in all experimental
groups except for the Laser 6 group. Among these groups, the Laser
4 group exhibited the lowest IL-4 mRNA expression. In addition, the
IL-6 expression level was decreased in all experimental groups
treated with LLLT, with Laser 4 group presenting the lowest IL-6
expression level. Furthermore, the mRNA expression of TNF-α in all
experimental groups treated with LLLT was significantly decreased
compared with that in the AD group. Once again, the Laser 4 group
showed the lowest expression level of TNF-α. Atopic dermatitis is
caused by abnormal activation of IL4, the Th2 cytokine (1). These findings suggested that LLLT may
suppress the immune response from Th2 cells, subsequently reducing
the inflammatory response in AD.
The current study also measured the expression of
IFN-γ and observed lower expression level of IFN-γ; however, the
difference was not significant. Since IFN-γ is the cytokine that
induces immune responses from Th1 cells (51), these findings indicated that AD
treatment with LLLT for two weeks was not sufficient to correct the
immune imbalance between Th1 and Th2 cells.
The epidermal thickness of AD lesions was assessed
by H&E staining. The results showed a significant reduction in
epidermal thickness in the experimental groups treated with LLLT,
particularly in the Laser 4 group that exhibited the greatest
reduction, compared with the AD group. Furthermore, the number of
mast cells after toluidine blue staining in the AD groups was
significantly increased compared with the normal group. In
addition, the number of degranulated cells in the AD control group
was significantly higher than in all experimental groups treated
with LLLT. This observation was due to the larger number of mast
cells in this group. These findings suggested that LLLT may be
considered as an effective treatment option for AD.
The wavelength of LLL used in this study (650 nm)
could effectively recover inflammation Although 1.0% DNCB solution
was frequently applied to prevent natural healing of AD, all
experimental groups treated with LLLT exhibited decreased IL-4,
IL-6, and TNF-α levels. Immunomodulation by the Th1 and Th2 cells
might have accounted for the elevated IFN-γ expression level in the
AD group compared with that in the other experimental groups
treated with LLLT. However, the present results indicated that gene
expression of IFN-γ in the AD control group did not differ from
that in the other experimental groups treated with LLLT (data not
shown). Therefore, the AD improvement observed in this study did
not result from immunomodulation by the Th1 and Th2 cells, but
rather from the intracellular activity promoted by LLLT to induce
recovery of inflammation and skin restoration (52) and to reduce the mRNA expression of
IL-4, IL-6 and TNF-α. Future investigation on immunomodulation by
the Th1 and Th2 cells is therefore required.
The findings from the present study suggested that
LLLT may be considered as an effective treatment for AD since it
may promote intracellular activation to reduce the release of
inflammatory cytokines from Th2 cells. Furthermore, comparisons of
the different treatment group outcomes suggested that the 4
J/cm2 laser output was more effective at improving the
symptoms of AD and reducing the levels of cytokines compared with
other output values.
The present study evaluated the changes in clinical
skin severity and scratching for 14 days. Further investigation
will therefore investigate IgE and IL-4 levels evolution over time.
IgE was evaluated because it is directly related to inflammation.
Furthermore, histamine is released when allergy antigens bind to
IgE antibodies that bind to obese cells. Increased IgE leads to
histamine release, causing inflammatory reactions. Histamine is one
of the organic substances that the body secretes for rapid defense
against external stimulation (stress). In other words, it is a
substance that causes inflammation, in which the wound swells red
and causes pain (53). Therefore,
IgE overproduction may be associated with the release of high
levels of histamine. The present study identified how LLL
irradiation affects IgE and cytokines (IL-4, IL-6 and TNF-α) in the
skin that caused atopic dermatitis. Future investigation will
therefore examine the release of histamine in this model.
Since the number of experimental animals used in
this study was relatively low, Clinical research, including a large
number of animal trials, will be needed. Taken together, the
findings from the present study may help determining clinically
appropriate energy outputs for LLLT against AD.
Acknowledgements
The authors would like to thank Dr Miyung Kim, Dr
June Bryan, Dr Irene Joy, Dr Chrislean Jun and Dr Raly James
(Uimyung Research Institute. Sahmyook University) for their
assistance preparing animal experiuments and their support on this
paper.
Funding
Funding: This study was supported by a grant from Sahmyook
University in 2017.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YLK and HSL carry out the experiments. YLK and HSL
analyzed and interpreted the data regarding the cytokines. YLK and
SML made substantial contributions to conception and design of the
study, and confirmed the authenticity of all the raw data. All
authors read and approved the final manuscript
Ethics approval and consent to
participate
This study was approved by the Animal Research
Ethics Board of Sahmyook University (approval no.
SYUIACUC2017-004).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bieber T: Atopic dermatitis. Ann Dermatol.
22:125–137. 2010.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Sandstrom MH and Faergemann J: Prognosis
and prognostic factors in adult patients with atopic dermatitis: A
long-term follow-up questionnaire study. Br J Dermatol.
150:103–110. 2004.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Youssef DM, Elbehidy RM, El-Shal AS and
Sherief LM: T helper 1 and T helper 2 cytokines in atopic children
with steroid-sensitive nephrotic syndrome. Iran J Kidney Dis.
9:298–305. 2015.PubMed/NCBI
|
|
4
|
Hanzlikova J, Ulcova-Gallova Z, Malkusova
I, Sefrna F and Panzner P: TH1-TH2 response and the atopy risk in
patients with reproduction failure. Am J Reprod Immunol.
61:213–220. 2009.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Horsmanheimo L, Harvima IT, Jarvikallio A,
Harvima RJ, Naukkarinen A and Horsmanheimo M: Mast cells are one
major source of interleukin-4 in atopic dermatitis. Br J Dermatol.
131:348–353. 1994.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Jung JH and Kim GJ: Anti-inflammatory
effects of herbal medicines (Rubus coreanus, Rehmanniae Radix,
Houttuynia cordata, Betulae cortex) EtOH extract on acute atopic
dermatitis mice. J Korean Med Ophthalmol Otolaryngol Dermatol.
28:68–84. 2015.
|
|
7
|
Lim YY, Kim HM, Jang WS, Seo SH, Ahn HH,
Kim Mn and Kim BJ: Study on tests of skin safety and inhibition of
atopic dermatitis using a StoneTouch® infrared scanner
in a mouse model. Korean J Dermatol. 49:217–226. 2011.
|
|
8
|
Lim YY, Jang WS, Kim HM, Kim IS, Lee JW,
Kim MN and Kim BJ: Therapeutic effects of light emitting diode on
atopic dermatitis-like lesions in NC/Nga mice. Korean J Asthma
Allergy Clin Immunol. 31:207–214. 2011.
|
|
9
|
Kwon TR: UV-LED 310-nm and 340-nm of
phototherapy in the treatment of atopic dermatitis. PhD Thesis,
Chung-Ang University, Seoul, Korea, 2015.
|
|
10
|
Garritsen FM, Brouwer MW, Limpens J and
Spuls PI: Photo(chemo)therapy in the management of atopic
dermatitis: An updated systematic review with implications for
practice and research. Br J Dermatol. 170:501–513. 2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Jekal SJ, Park MS and Kim DJ: The combined
effects of curcumin administration and 630 nm LED phototherapy
against DNCB-induced atopic dermatitis-like skin lesions in BALB/c
mice. Korean J Clin Lab Sci. 49:150–160. 2017.
|
|
12
|
de Freitas LF and Hamblin MR: Proposed
mechanisms of photobiomodulation or low-level light therapy. IEEE J
Sel Top Quantum Electron. 22(7000417)2016.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Yu W, Naim JO and Lanzafame RJ: Effects of
photostimulation on wound healing in diabetic mice. Lasers Surg
Med. 20:56–63. 1997.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Barber AJ, Luger E and Karpfetal A:
Advances in laser therapy for bone repair. Laser Ther. 13:84–85.
2000.
|
|
15
|
Hamblin MR and Demidova TN: Mechanisms of
low level light therapy. In: Mechanisms for Low-Light Therapy.
Hamblin MR, Waynant RW and Anders J (eds). Proceedings of SPIE. Vol
6140. 1-12, 2006.
|
|
16
|
Kim KU: Effects of low level laser
irradiation with 904 nm pulsed diode laser on the extraction wound.
J Korean Academy of Oral Med. 23:301–309. 1998.
|
|
17
|
Marei MK, Abdel-Meguid SH, Mokhtar SA and
Rizk SA: Effect of low-energy laser application in the treatment of
denture-induced mucosal lesions. J Prosthet Dent. 77:256–264.
1997.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Joon YH, Sung YJ, Gon KD and Yong LJ: The
effects of low level laser therapy on decrease of atopic dermatitis
symptoms. Korean J Pediatr Med. 23:193–206. 2009.
|
|
19
|
Clokie C, Bentley KC and Head TW: The
effects of the helium-neon laser on postsurgical discomfort: A
pilot study. J Can Dent Assoc. 57:584–586. 1991.PubMed/NCBI
|
|
20
|
Kert J: Low level laser therapy used
pre-operatively. Laser News. 4:26–32. 1992.
|
|
21
|
Roynesdal AK, Bjornland T, Barkvoll P and
Haanaes HR: The effect of soft-laser application on postoperative
pain and swelling. A double-blind, crossover study. Int J Oral
Maxillofac Surg. 22:242–245. 1993.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Pick RM and Powell GL: Laser in dentistry:
Soft tissue procedure. Dent Clin North Am. 37:281–296.
1993.PubMed/NCBI
|
|
23
|
Miller M and Truhe T: Lasers in dentistry:
An overview. J Am Dent Assoc. 124:32–55. 1993.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Hall J, Clarke AK, Elvins DM and Ring EF:
Low level laser therapy is ineffective in the management of
rheumatoid arthritic finger joints. Br J Rheumatol. 33:142–147.
1994.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Basford JR: Laser therapy: Scientific
basis and clinical role. Orthopedics. 16:541–547. 1993.PubMed/NCBI
|
|
26
|
Beckerman H, de Bie RA, Bouter LM, De
Cuyper HJ and Oostendorp RA: The efficacy of laser therapy for
musculoskeletal and skin disorders: A criteria-based meta-analysis
of randomized clinical trials. Phys Ther. 72:483–491.
1992.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Morita H, Kohno J, Hori M and Kitano Y:
Clinical application of low reactive level laser therapy (LLLT) for
atopic dermatitis. Keio J Med. 42:174–176. 1993.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Nistico SP, Saraceno R, Capriotti E,
Felice CD and Chimenti S: Efficacy of monochromatic excimer light
(308 nm) in the treatment of atopic dermatitis in adults and
children. Photomed Laser Surg. 26:14–18. 2008.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Baltas E, Csoma Z, Bodai L, Ignacz F,
Dobozy A and Kemeny L: Treatment of atopic dermatitis with the
xenon chloride excimer laser. J Eur Acad Dermatol Venereol.
20:657–660. 2006.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Brenninkmeijer EE, Spuls PI, Lindeboom R,
van der Wal AC, Bos JD and Wolkerstorfer A: Excimer laser vs.
Clobetasol propionate 0.05% ointment in prurigo form of atopic
dermatitis: A randomized controlled trial, a pilot. Br J Dermatol.
163:823–831. 2010.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Syed S, Weibel L, Kennedy H and Harper JI:
A pilot study showing pulsed-dye laser treatment improves localized
areas of chronic atopic dermatitis. Clin Exp Dermatol. 33:243–248.
2008.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Stich AN, Rosenkrantz WS and Griffin CE:
Clinical efficacy of low-level laser therapy on localized canine
atopic dermatitis severity score and localized pruritic visual
analog score in pedal pruritus due to canine atopic dermatitis. Vet
Dermatol. 25:464–474. 2014.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Lee KS, Jeong ES, Hea SH, Seo JH, Jeong DG
and Choi YK: A novel model for human atopic dermatitis: Application
of repeated DNCB patch in BALB/c mice, in comparison with NC/Nga
mice. Lab Anim Res. 26:95–102. 2010.
|
|
34
|
Suto H, Matsuda H, Mitsuishi K, Hira K,
Uchida T, Unno T, Ogawa H and Ra C: NC/Nga mice: A mouse model for
atopic dermatitis. Int Arch Allergy Immunol. 120 (Suppl 1):70–75.
1999.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Kim SH: Phototherapy. Hanlddlag, Gunggido,
p198, 2005.
|
|
36
|
Suzuki R, Shimizu T, Kudo T, Ohtsuka Y,
Yamashiro Y and Oshida K: Effects of n-3 polyunsaturated fatty
acids on dermatitis in NC/Nga mice. Prostaglandins Leukot Essent
Fatty Acids. 66:435–440. 2002.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Lee GS, Jung HM, Oh SK, Cheong JH and Kang
TJ: Effects of herbal complex on atopic dermatitis in BALB/c mice.
Kor J Pharmacogn. 43:59–65. 2012.
|
|
38
|
Umeda K, Noro Y, Murakami T, Tokime K,
Sugisaki H, Yamanaka K, Kurokawa I, Kuno K, Tsutsui H, Nakanishi K
and Mizutani H: A novel acoustic evaluation system of scratching in
mouse dermatitis: Rapid and specific detection of invisibly rapid
scratch in an atopic dermatitis model mouse. Life Sci.
79:2144–2150. 2006.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Ahn JY, Lee RI, Kim JH, Park JH, Kim DK
and Lee YM: Effects of rumecis radix water extract on development
of atopic dermatitis in BALB/c Mice. Korean J Pharmacogn.
40:218–223. 2009.
|
|
40
|
Kim M, Custodio RJ, Botanas CJ, de la Peña
JB, Sayson LV, Abiero A, Ryoo ZY, Cheong JH and Kim HJ: The
circadian gene, Per2, influences methamphetamine sensitization and
reward through the dopaminergic system in the striatum of mice.
Addict Biol. 24:946–957. 2019.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Livak KJ and Schmittgen TD: . Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-delta delta C(T)) method. Methods. 25:402–408.
2001.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Choy DF, Hsu DK, Seshasayee D, Fung MA,
Modrusan Z, Martin F, Liu FT and Arron JR: Comparative
transcriptomic analyses of atopic dermatitis and psoriasis reveal
shared neutrophilic inflammation. J Allergy Clin Immunol.
130:1335–1343.e5. 2012.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Owen J, Punt J and Stratford S: Kuby
Immunology. 7th edition. W.H. Freemand and Company, New York, NY,
USA, p372, 2013.
|
|
44
|
Moreira MS, Velasco IT, Ferreira LS, Ariga
SK, Abatepaulo F, Grinberg LT and Marques MM: Effect of laser
phototherapy on wound healing following cerebral ischemia by
cryogenic injury. J Photochem Photobiol B. 105:207–215.
2011.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Cooper D, Hales J and Camp R:
IgE-dependent activation of T cells by allergen in atopic
dermatitis: Pathophysiologic relevance. J Invest Dermatol.
123:1086–1091. 2004.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Abbas AK and Andrew H: Lichtmann, Shiv
Pillai: Cellular and Molecular Immunology. 6 edition. Saunders
Elsevier, Philadelphia, p50, 2007.
|
|
47
|
Hartel C, Bein G, Muller-Steinhardt M and
Kluter H: Ex vivo induction of cytokine mRNA expression in human
blood samples. J Immuno Methods. 249:63–71. 2001.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Whiteside TL: Cytokines and cytokine
measurements in clinical laboratory. Clin Diagn Lab Immunol.
1:257–266. 1994.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Taniuchi S, Kojima T, Hara Mt K, Yamamoto
A, Sasai M, Takahashi H and Kobayashi Y: Increased serum nitrate
levels in infants with atopic dermatitis. Allergy. 56:693–695.
2001.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Homey B, Steinhoff M, Ruzicka T and Leung
DY: Cytokines and chemokines orchestrate atopic skin inflammation.
J Allergy Clin Immunol. 118:178–189. 2006.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Abbas AK, Lichtman AH and Pober JS:
Cellular and Molecular Immunology. Bummoon-Education, Seoul,
pp320-321, 1998.
|
|
52
|
Huang YY, Sharma SK, Carroll J and Hamblin
MR: Biphasic dose response in low level light therapy-an update.
Dose Response. 9:602–618. 2011.PubMed/NCBI View Article : Google Scholar
|
|
53
|
MacDonald SM, Rafnar T, Langdon J and
Lichtenstein LM: Molecular identification of an IgE-dependent
histamine-releasing factor. Science. 269:688–690. 1995.PubMed/NCBI View Article : Google Scholar
|