Introduction
The uterine round ligament is a round, rope-like
band of fibromuscular connective tissue (1). One side of the ligament is attached to
the superior and lateral aspect of the uterus at the anatomical
location of the uterine cornu. Arising from the cornu of the
uterus, the round ligament is covered by peritoneum over a length
of 10-12 cm, crosses the pelvis via the deep inguinal ring, then
traverses the inguinal canal and finally enters the labia majora,
where it terminates with its fibres blending into the mons pubis
(1).
Leiomyomas are benign tumours that may arise in any
anatomical structure containing smooth muscle (2). However, in contrast to typical
leiomyomas, which are a relatively common gynaecological problem,
leiomyomas of the uterine round ligament are rare (2). Tumours of the round ligament are
exceedingly rare, with roughly 300 cases previously published in
the literature (3). Although rare,
leiomyomas are the most frequent tumour of the uterine round
ligament (3). Other tumours
encountered at the uterine round ligament according to histological
type include adenomyomas, mesothelial cysts, endometriotic cysts,
leiomyosarcomas and other, even rarer entities (4).
Leiomyomas of the uterine round ligament may appear
in multiple different anatomical locations at any point along the
length of this structure, and are commonly classified as intra- or
extra-abdominal (inguinal or labial). Intra-abdominal leiomyomas of
the uterine round ligament typically remain asymptomatic. On pelvic
and ultrasound examination, the differential diagnosis of
leiomyomas from pedunculated subserosal myomas or solid ovarian
neoplasms is difficult (4). Even
following computed tomography and magnetic resonance imaging
examinations, the lack of specific findings, as leiomyomas appear
as encapsulated heterogeneous tumours, hinders final diagnosis
prior to surgical intervention and histological examination
(5). On the other hand,
extra-abdominal leiomyomas are frequently detected by the patient
as a mass lesion with synchronous symptoms, including pain, and
differential diagnosis from hernias or enlarged lymph nodes is
necessary (4,6).
In the present study, a rare case of a large
leiomyoma of the right uterine round ligament detected during
routine gynaecological examination is described, in line with the
Surgical CAse REport (SCARE) criteria (7). The aim was to underline the role of
routine gynaecological examination and the importance of complete
preoperative diagnostic evaluation in cases of large
intra-abdominal lesions to plan the appropriate surgical approach
and ensure optimal management.
Case report
A 51-year-old asymptomatic female patient (gravida
3, para 3) presented herself on October 2020 for a routine
gynaecological examination. The patient had obstetrical history of
three full-term vaginal deliveries and no previous surgical
interventions, while her medical history was unremarkable.
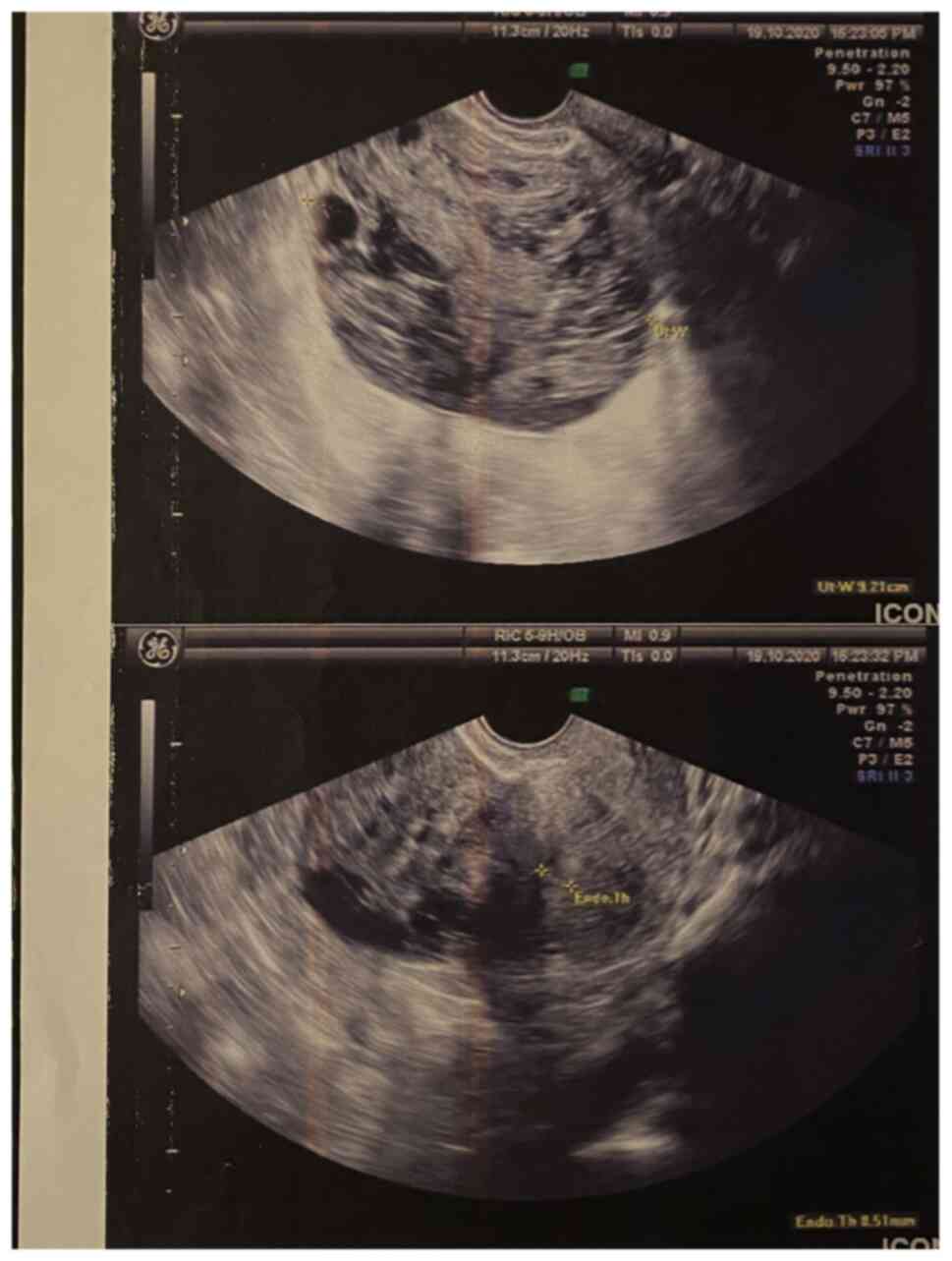
A transvaginal ultrasound examination revealed a
solid heterogeneous mass localized at the right parametrial space
with a maximum diameter of 9 cm, which was suggestive of a large
pelvic lesion with possible involvement of the right ovary
(Fig. 1). Routine blood
investigations and tumour marker levels were within the normal
range. Further preoperative evaluation using magnetic resonance
imaging revealed that the mass (maximum diameter, 9-cm) contained
solid as well as cystic components, which was suggestive of a
mesenchymal neoplasm, possibly originating from the right ovary.
There were no enlarged pelvic lymph nodes or ascites.
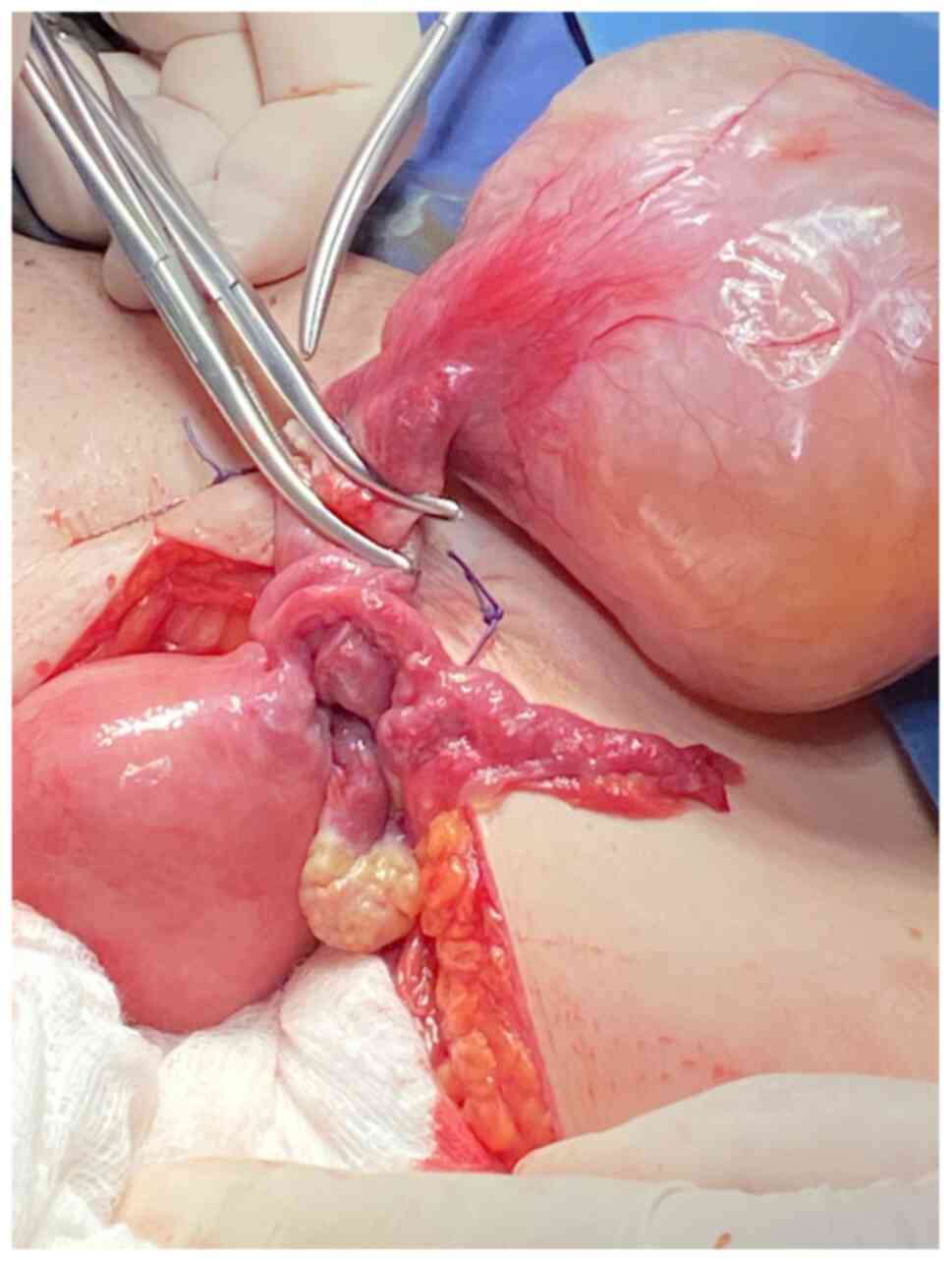
After obtaining informed consent from the patient, a
laparotomy was performed at Leto Maternity Hospital (Athens,
Greece) on November 2020, under general anaesthesia via a midline
vertical subumbilical incision. A large mobile solid mass arising
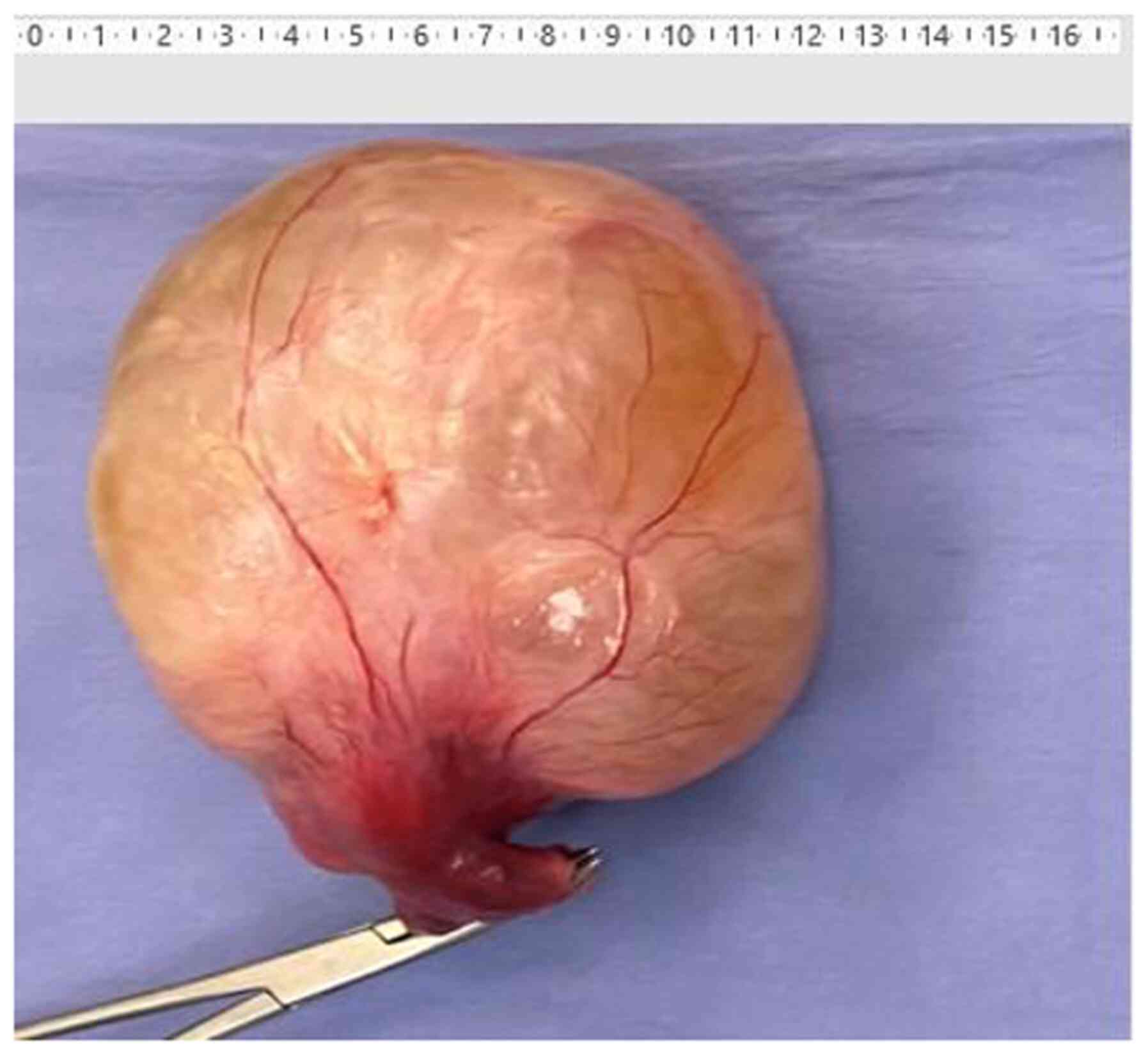
from the right uterine round ligament was detected (Fig. 2). Complete excision of the lesion
was performed (Fig. 3). The frozen
section biopsy revealed a mesenchymal neoplasm without mitotic
activity or signs of necrosis, with morphological characteristics
suggestive of a benign leiomyoma of the uterine round ligament.
Total abdominal hysterectomy and bilateral salpingo-oophorectomy
were subsequently performed.
Histological examination revealed a benign leiomyoma
with a maximum diameter of 10.5 cm, with signs of fibrosis,
hyalinosis and oedema. On immunohistological examination, the
neoplastic cells were positive for desmin and smooth muscle actin,
as expected. High density of mononuclear inflammatory cells, mainly
small lymphocytes with perivascular location, were detected. Among
them, rare eosinophil leukocytes and mastocytes were recognised
(data not shown). There were no malignant findings from the uterus,
cervix oradnexae. The postoperative period was uneventful and the
patient was discharged on postoperative day 2 without
complications. No recurrence was identified until her last
follow-up visit on June 2021.
Discussion
Leiomyomas of the uterine round ligament are rare,
and may present with multiple clinical manifestations according to
the location along the anatomical course of the ligament. Symptoms
associated with leiomyomas largely depend upon location, size and
rate of growth (4). In the vast
majority of cases, intra-abdominal leiomyomas of the round ligament
remain asymptomatic, and diagnosis is often made incidentally
during routine ultrasound examination or surgical intervention for
other reasons (3,4). These literature data agree with the
history of the patient in the present case, as she was asymptomatic
and the tumour was detected on routine gynaecological examination.
The patient's last transvaginal ultrasound gynaecological
examination had been performed 4 years earlier, without signs of
pathology at the right parametrium, which suggested that the solid
heterogeneous mass identified in the present study was a pelvic
tumour with a high rate of growth. Surgical intervention with
oncological parameters was recommended as a safe therapeutic
strategy for a tumour with a potentially aggressive biological
behaviour. This was the reason for which laparotomy was suggested
instead of laparoscopic excision of the tumour in order to avoid
morcelation. In addition, the tumour was sent for frozen section
biopsy so as to have a first histological view and decide if
further pelvic/paraaortic lymphadenectomy was necessary or not.
Preoperative investigation via computed tomography
or magnetic resonance imaging often fails to distinguish the origin
of solid pelvic tumours. Leiomyomas appear as encapsulated
heterogeneous tumours on spontaneous contrast-enhanced computed
tomography and post-gadolinium contrast magnetic resonance imaging
(5). The definitive differential
diagnosis from subserosal myomas or solid ovarian neoplasms often
requires surgical intervention. In the present case, magnetic
resonance imaging was unable to identify the origin of the pelvic
mass, and final diagnosis was made intraoperatively.
Leiomyomas of the uterine round ligament are
primarily solitary and unilateral, although they have also been
reported to be multiple and bilateral (4). A number of studies have reported that
leiomyomas appear more frequently on the right compared with the
left uterine round ligament (4,8,9).
Although the aforementioned studies support this predilection for
the right round ligament, which was also the case in our patient,
there appears to be no medical explanation for this
observation.
Surgical intervention is currently considered as the
most appropriate therapeutic strategy in cases of large pelvic
tumours with uncertain differential diagnosis. Complete excision of
the lesions is necessary in cases of uterine leiomyomas, without
the requirement for hysterectomy in women of reproductive age
(2-4).
The patient presented herein was a perimenopausal 51-year-old
woman, and the total abdominal hysterectomy with bilateral
salpingo-oophorectomy that followed the excision of the leiomyoma
of the right uterine round ligament was performed as a preventive
measure.
Routine gynaecological examination is necessary to
prevent women from experiencing life-threatening pathological
conditions that affect the reproductive system. The vast majority
of patients may be asymptomatic, as abdominal tumours arising from
the ovaries or the uterus may not give rise to symptoms, even when
they reach a large size. Surgical intervention remains the optimal
therapeutic strategy (3,4), following appropriate preoperative
evaluation, as a means of definitive diagnosis, as well as curative
treatment in cases of large intra-abdominal tumours with a
challenging differential diagnosis.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
AT was involved in the study conception and design,
data collection and analysis and the writing of the manuscript. CG
participated in the writing of the manuscript, data collection and
data analysis. ET was involved in the study design and data
analysis. CG was involved in data analysis. AM was involved in
study conception and design. All authors have read and approved the
final manuscript. CG, ET and CG confirm the authenticity of the raw
data.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Leto Maternity Hospital (approval no. 38/2021).
Patient consent for publication
The patient provided written informed consent for
the publication of the case details and any associated images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Chaudhry SR and Chaudhry K: Anatomy,
abdomen and pelvis, uterus round ligament. In: StatPearls
[Internet]. StatPearls Publishing, Treasure Island, FL, 2021.
https://www.ncbi.nlm.nih.gov/books/NBK499970/.
Accessed July 26, 2021.
|
|
2
|
Kirkham JC, Nero CJ, Tambouret RH and Yoon
SS: Leiomyoma and leiomyosarcoma arising from the round ligament of
the uterus. J Am Coll Surg. 207(452)2008.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Klingbeil KD, Polcari AM, Azab B and
Franceschi D: Large, extra-abdominal leiomyoma of the round
ligament with carneous degeneration. BMJ Case Rep.
2017(bcr2017222454)2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Breen JL and Neubecker RD: Tumors of the
round ligament: A review of the literature and report of 25 cases.
Obstet Gynecol. 19:771–780. 1962.
|
|
5
|
Michel P and Viola D: Abdomino-pelvic
leiomyoma of the round ligament: Contribution of computed
tomography and magnetic resonance imaging. J Gynecol Obstet Biol
Reprod (Paris). 32:571–574. 2003.PubMed/NCBI(In French).
|
|
6
|
Christodoulou IM, Angelopoulos A, Siaperas
P, Ioannidis A, Skarpas A, Tellos A, Velimezis G and Karanikas I:
Leiomyoma of the round ligament of the uterus mimicking inguinal
hernia. Case Rep Surg. 2018(6702494)2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Agha RA, Borrelli MR, Farwana R, Koshy K,
Fowler A and Orgill DP: SCARE Group. The SCARE 2018 statement:
Updating consensus Surgical CAse REport (SCARE) guidelines. Int J
Surg. 60:132–136. 2018.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Emanuel R: Veber tumoren des ligamentum
rotundum uteri. Ztschr f Geburtsh u Gynak Stuttgart.
49(383)1903.
|
|
9
|
Taussig FG: Sarcoma of the round ligament
of the uterus. Surg Gynec Obst. 19(218)1914.
|