Introduction
Locally advanced colon cancers constitute 10% of all
colorectal malignancies at the time of diagnosis (1) and are more common in the rectosigmoid
(66-89%) (2).
The incidence of right-sided colon cancers (RSCCs)
invading adjacent organs is rare (11-28%) (3). Their management is particularly
challenging especially if invasion of the duodenum or pancreas
occurs. Multivisceral resections have proven their efficiency with
satisfactory outcomes concerning recurrence status and survival
rates (4). In duodenal and/or
pancreatic invasion, the optimal technique utilized is right
hemicolectomy (RH) with en bloc duodenopancreatectomy (DP)
(5). Therefore, radical resection
of the lesion in association with local lymph node dissection
provides the opportunity of maximal local control (6). Nevertheless, the complexity of the
procedure, the risks of postoperative morbidity and a poor patient
general condition in T4 RSCC prompt the surgeon to opt for
palliative treatment or limited duodenal resections. Limited
duodenal resections show promising survival results if the margins
of at least 1 cm from the invaded area are respected (7) and when the papilla of Vater and
pancreas are intact. The intestinal integrity must be restored by
one of the duodenal continuity reconstruction techniques if large
duodenal defects are present. Several procedures have been
proposed, including pedicled gastric flap (8), serosal jejunal patching (9), serosal ileal patching, mucosal jejunal
patching (10) and
duodenojejunostomy (11).
Herein, we present our experience regarding the
management of RSCC invading the duodenum or pancreas; the aim of
the study was to analyze the long-term outcomes after such
resections.
Patients and methods
We selected all of the patients with locally
advanced right-sided colon cancer (LARCC) including the proximal
two-thirds of the transverse colon, who were admitted into our
130-bed surgical department of ‘Fundeni’ Clinical Institute from
January 2004 to March 2020. RSCC was considered locally advanced
when adjacent structures or organs were involved. Patients who
presented distant metastasis, peritoneal spread, vascular invasion
or recurrent disease were excluded from the current study. From the
patients with LARCC, the medical records of 22 patients with colon
cancer invading the duodenum or pancreas were reviewed in detail.
The data analyzed, retrospectively, included demographics, site,
clinical presentation, imagistic findings, type of surgery,
postoperative course, pathologic staging of the tumor according to
the Union for International Cancer Control TNM system (www.uicc.org), pathologic grading, tumor size,
postoperative morbidity, adjuvant treatment modalities and
follow-up duration. Survival rates were calculated using Microsoft
Excel program.
Results
Among the 110 patients with LARCC who underwent
surgery at our department, the most frequently invaded structure
was perinephric fat. Pancreas and duodenum involvement was
encountered in 22 cases (19%). Other sites of invasion are listed
in Table I.
 | Table ISecondary sites of
invasiona. |
Table I
Secondary sites of
invasiona.
| Organ/tissue
involved | No. of patients
(N=110) |
|---|
| Psoas muscle | 4 |
| Stomach | 16 |
| Gallbladder | 10 |
| Abdominal wall | 27 |
| RLL/ovary | 9 |
| Liver | 5 |
| Small bowel | 19 |
| Perirenal fat | 32 |
| Kidney | 4 |
| Peritoneum | 9 |
| Ureter | 2 |
| Other parts of the
colon | 5 |
|
Duodenum/pancreas | 22 |
The mean age of the patients with pancreatic or
duodenal involvement of the disease was 49.5 years and ranged
between 25 and 77 years, with a prevalence of male patients over
female patients (16/6; 83%/17%). The most frequent site of origin
of RSCC involving the duodenum or pancreas was the hepatic flexure
of the colon in 18 cases (81%), followed by the ascending portion
of the colon in 3 (14%) cases and cecum in 1 case. Seventeen
patients (77%) had anemia at presentation. Other symptoms such as
pain, altered bowel habits or weight loss were found in 15 patients
(68%), whereas 3 patients underwent emergency surgery for tumor
perforation or hemorrhage. Eighteen patients (81%) underwent a
preoperative computed tomography (CT) scan. Duodenal/pancreatic
involvement on CT scan was suspected in 11/18 (61%) patients.
Intestinal bypass was practiced in 5/22 (22%) cases,
mostly due to patient comorbidities and age. Two of these patients
had liver cirrhosis, one had a history of acute myocardial ischemia
and stroke and two were over 75 years of age. The other 17 patients
underwent RH, RH en bloc with DP, RH en bloc with antrectomy and
proximal duodenal resection or RH with partial duodenectomy.
Clinical data of patients who underwent resections are detailed in
Table II.
| Table IIClinical data and outcome of the
patients who underwent resective surgery. |
Table II
Clinical data and outcome of the
patients who underwent resective surgery.
| Age (years)/sex | Surgerya | Grade | T stage | Org.
inv.b | CDF | N stage | 30DPOM | Chemo.c | Follow-up | Status |
|---|
| 25/M | DP | G1 | 4 | P | No | 0 | No | FOLFOX | 16 years | NED |
| 61/M | DP | G1 | 4 | D+P | Yes | 1 | Yes | - | - | - |
| 52/M | DP | G2 | 4 | D+P | Yes | 1 | No | FOLFOX | 12 months | DOD |
| 62/M | RH+G | G2-G3 | 4 | D1 | No | 1 | No | C | 15 years | NED |
| 71/M | RH | G1 | 3 | No | No | 0 | No | XELOX | 9 years | ROD |
| 65/M | DP+N | G2 | 4 | D+P+K | No | 2 | Yes | - | - | - |
| 64/F | PP-DP+N | G1-G2 | 4 | D+P+K | Yes | 0 | No | XELOX | 6 years | NED |
| 63//F | DP | G2 | 3 | No | No | 0 | No | C | 6 years | NED |
| 65/M | DP | G2 | 4 | D+P | No | 1 | No | FOLFOX | 4 years | NED |
| 75/M | RH | G2-G3 | 4 | D | No | 0 | No | XELOX | 11 months | DOD |
| 62/M | D | G1-G2 | 4 | D | No | 2 | No | XELOX | 39 months | NED |
| 69/M | DP | G2 | 4 | D+P | Yes | 1 | No | OX | 31 months | NED |
| 76/F | D | G3 | 4 | D | No | 0 | No | No | 24 months | NED |
| 74/F | RH | G3 | 4 | P | No | 1 | No | No | 7 months | DOD |
| 66/M | D | G1 | 4 | D | No | 0 | No | XELOX | 24 months | NED |
| 55/M | D | G2 | 4 | D | No | 2 | No | XELOX | 11 months | NED |
| 52/M | RH+G | G1-G2 | 4 | D1 | No | 0 | No | N/A | N/A | N/A |
Overall, 8/17 patients (47%) underwent en bloc DP
with standard reconstruction techniques. Palliative RH was
practiced in 3 patients (18%), because of the emergent nature of
the surgical procedure (tumor perforation or hemorrhage). Another 2
patients underwent right extended hemicolectomy en bloc with
antrectomy, when the first portion of duodenum was adherent to the
colonic tumor. The limited excision of the duodenum was practiced
in 4/17 patients (23, 5%), followed by simple duodenorrhaphy in 2
patients, doudenojejunostomy in 1 case and pedicled ileal patch in
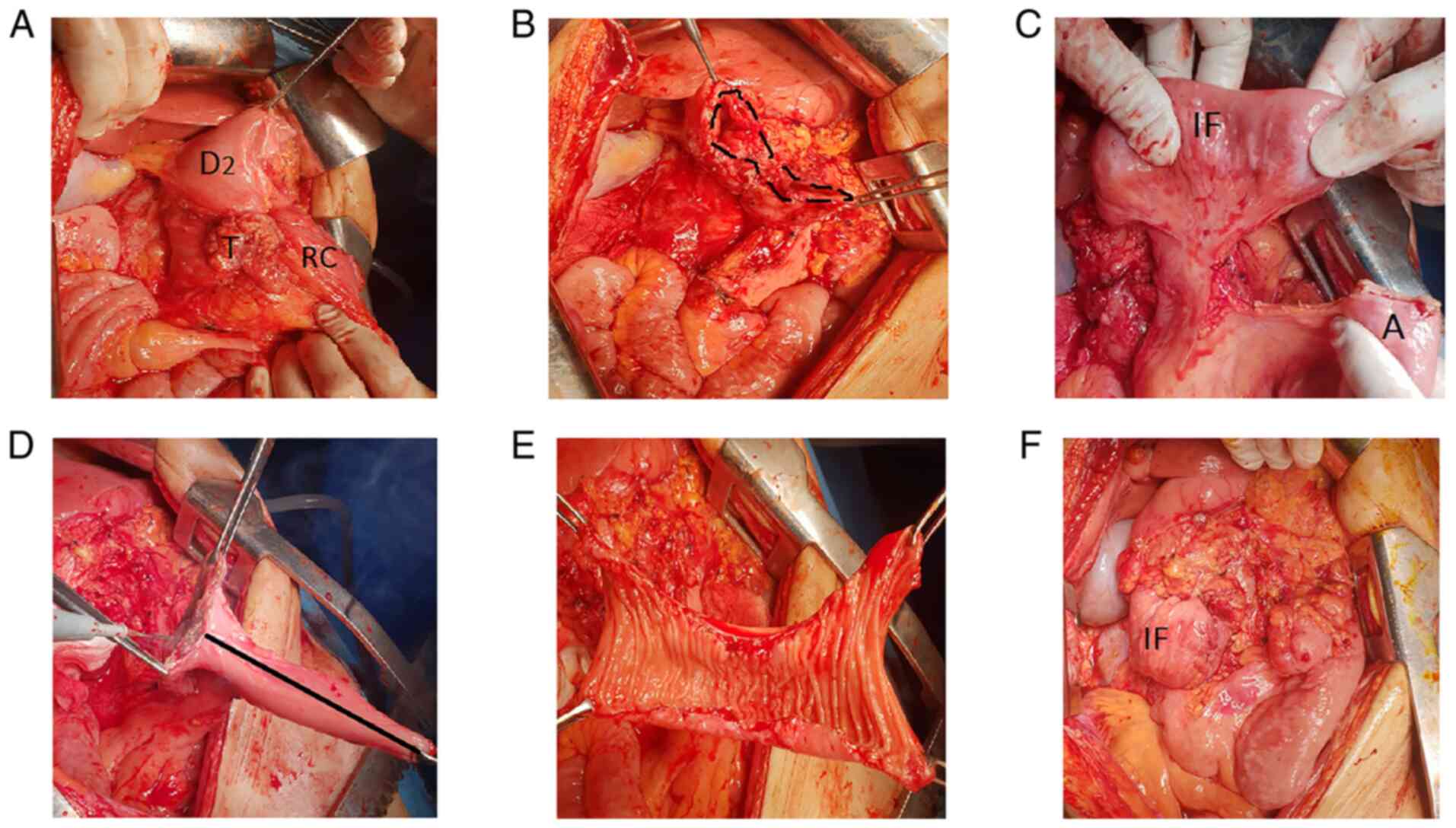
one case. Mean tumor size in all the patients who underwent
resection surgery was 7.5 cm and ranged between 3 and 15 cm. In our
ileal patch reconstruction case, the ileal patch was prepared from
the distal 8 cm of the terminal ileum. After mesenteric pedicle
preparation, the ileum was cut on the antimesenteric border,
trimmed dimensionally so that it fits the duodenal diameter and
sutured in double layer to the lateral wall of the duodenum
(Fig. 1).
Upon histopathological analysis, 6 specimens from
the RH with DP series presented pancreatic and duodenal invasion, 1
specimen presented pancreatic invasion alone, whereas in 1 case
inflammatory adhesions to the gland were encountered. Coloduodenal
fistula was present in 4 cases.
Among the 4 cases with limited duodenal resection, 3
patients presented invasion of the entire duodenal wall, including
mucosa while the fourth patient had extrinsic invasion of the
duodenal submucosa.
Meanwhile lymphatic node involvement was encountered
in 50% of the entire study group.
The majority of the patients (9/10; 90%) from both
the limited duodenal resection and DP series, that survived the
postoperative period, received adjuvant chemotherapy.
The 5-year survival rate in the RH with DP series
could be calculated in cases that had surgery between 2004 and 2015
(6 patients) and was 50%. Of the 3 patients with a lethal outcome,
2 patients died due to postoperative complications in the first 30
days; one of the patients died of pulmonary thromboembolism and the
other one developed pancreatitis of the pancreatic stump and
pneumonia. The third patient succumbed to local recurrence 12
months after surgery.
Postoperative morbidity was noted in 2 cases (25%).
Both patients developed pancreatic leakage, successfully treated
during postoperative recovery.
The 5-year survival data for the 2 patients that
underwent RH with DP between 2016 and 2020 is not yet available.
Both are alive without evidence of local recurrence at 4 years and
at 31 months respectively after surgery.
In the limited duodenal resection series, the 5-year
survival rates are not yet available. However, no 30-day mortality
was observed. All patients are alive at 11 to 39 months
postoperatively.
Of the 3 patients with palliative RH, only 1 patient
survived more than 5 years. It was determined that he presented T3
invasion with inflammatory adhesions to the duodenum on the
histopathological analysis. Although he was submitted to
chemotherapy, he developed lung metastasis 2 years after the first
intervention, which was successfully resected and liver metastasis
2 years after the second intervention, successfully resected as
well. Among the cases submitted to palliative surgery (intestinal
bypass) the maximum length of survival was 15 months.
Discussion
Colon cancer is one of the most frequent
malignancies, with 14,000 new cases being diagnosed annually in
Romania (12). Locally advanced
colon cancers invading the duodenum/pancreas are a less common
finding, with an incidence of 11% (13). We investigated only patients with
LARCC and found the prevalence of duodenum/pancreas involvement in
19%, being outweighed by perirenal fat invasion, in 29% of cases.
The rarity of pancreatic/duodenal involvement is reflected in the
paucity of the reported case series in the literature (14). Furthermore, the medical literature
may be deprived of studies because of the complexity of the
operative technique for en bloc resection of the right colon in
continuity with DP, which discourages the surgeons to make radical
decisions (15) and the lack of
popularity for limited duodenal resections, in cases of duodenal
involvement alone.
Despite advances in preoperative screening and
clinical imaging, adjacent organ involvement is often discovered
during surgery (16). Some authors
pointed out that palpable and immobile tumors are predictive for
local invasion (3,14). In our study the most persistent
symptom was anemia (77%), followed by abdominal pain, with tumor
palpability being described only in one case. However, the results
may be biased because of the tendency of modern surgeons to rely on
imaging exams rather than clinical features. Preoperative imaging
in our series was able to detect local duodenal/pancreatic invasion
in 60% of the cases. If duodenocolic fistula is present, then
barium enema is the best option for its detection, since increased
colic pressure redirects bowel contents towards the duodenum
(17). Of the 4 cases with
duodenocolic fistula in our series, one was investigated by means
of barium enema. The other 2 patients underwent endoscopy and in
the last case fistula was detected intraoperatively.
Even if adherence between the colon and duodenum is
easily assessed after mobilization of the colon, it is difficult
for the surgeon to rule out whether adherence is of a malignant
nature or due to inflammatory processes, since 40% of adhesions are
a result of local inflammatory response (18). Adhesion dissection may lead to
malignant dissemination (19) and
is associated with recurrence rates of 90-100% (20). Yet, in our study, histopathological
exam showed malignant infiltration of the adherent part to the
duodenum/pancreas in the majority of cases (15/17; 88%). Dissection
of adhesions in the setting of emergent RH was practiced in 3
patients, of which 2 patients had R1 margins on histopathology.
Generally, in making a decision on what type of
surgery to perform for patients with LARCC, one should remind
oneself of Hippocrates's quote: ‘For extreme diseases, extreme
remedies are most fitting’ (13).
Since patients undergoing digestive bypasses prove
to have a median survival of 9 months (21), this technique should be reserved to
cases with malignant distal spread, with poor survival because of
comorbidities or in cases with increased operative risk. In our
study, 5 patients underwent digestive bypass; although, it was hard
to determine retrospectively if any of these patients could have
benefited from resective surgery.
Incomplete resection including organ separation is
associated with a mean patient survival time of 11 months (21). In our study, out of 3 cases with
incomplete resection, 2 cases survived for 7 and 11 months,
respectively, which confirms low survival in this group.
By contrast, patients who undergo en bloc
multivisceral resection were found to exhibit a disease-free
survival rate of 56% at 1 to 5 years of follow-up (22). In addition, local invasion of
adjacent organs is not a statistically more unfavorable prognostic
factor than one to five lymph node metastases (3). However, lymph node involvement in
LARCC has a supplementary negative impact on survival (23). In our series, 8/14 patients with en
bloc resection had lymph node involvement, but no correlation was
noted between lymph node involvement and the survival rate.
En bloc resection of the colon and pancreatic head
was initially performed by Linton in 1941, as a 2-stage procedure,
preceded by digestive bypass for patient nutritional status
improvement (24). A decade later,
several authors modified it to a 1-stage procedure (25,26).
Yet, the first reports and studies did not confirm a favorable
prognosis. It was only recently that RH with DP for LARCC began to
regain attention, with 5-year survival rates of 54% (4). The increase in the safeness of the
procedure is due to parenteral nutrition possibilities in patients
with preoperative bad health status and weight loss (27,28)
and to improvements in the surgical technique (23). In our series, however, a 25% 30-day
postoperative mortality rate occurred, possibly due to the lack of
careful selection of cases in the early RH with DP attempts.
Moreover, DP permits en bloc dissection of
peripancreatic and perigastric lymph nodes (29), a fact that may have additional
benefits on survival. In our DP series, a 1-year survival rate was
achieved in 75% of the patients and a 5-year survival in 50% of the
patients.
If the duodenal sidewall is affected, with papilla
of Vater free of invasion, a surgeon may take into consideration
limited duodenal resection, especially in patients with high
perioperative risks and comorbidities (15). No certain evidence exists that
survival in regards to limited duodenal resections is worse than in
DP, since randomized studies are absent and scientific data are
limited to several case reports and case series (15,30-33).
Nonetheless, the procedure of limited duodenal resection has been
described since 1963(34).
When less than one-third of the duodenal wall is
excised, the easiest method of defect closure is simple
duodenorrhaphy (5). In the current
series, simple transverse closure was used in 2 patients, with no
postoperative complications noted. If taking into consideration the
reported experience of the management of traumatic duodenal
injuries, there is a certain risk of tension development on the
suture line and duodenal disruption even in small defects (35). Therefore, patch repair should always
be considered. The usual duodenal defect repair is Roux-en-y
duodenojejunostomy (9).
Nonetheless, it has the disadvantages of delivering bile and
pancreatic juice more distally in the small intestine (36) and requires an additional
anastomosis. The intestinal loop can be difficult to mobilize in
cases of short mesentery (37).
Finally, it can lead to internal hernias because of the formation
of wide mesenteric defects (38).
Pedicled ileal grafting seems to be the perfect
solution for large defects. First of all, no additional cutting of
the digestive tract at other sites is needed. It does not create a
nonanatomical bypass (7,11) and can be retroperitonized without
affecting the ileocolic anastomosis. Finally, the patch width is
easily adaptable, avoiding the formation of duodenal stenosis or
pouchitis (38). Data on the
outcomes of en bloc limited duodenal resection are lacking, since a
limited number of cases have been performed and reported. Based on
the existing literature, Hamed et al estimated a 3-year
survival rate of 70% after limited duodenal resections, comparable
to the 3-year survival rate after DP (37). Our 4 patients with limited duodenal
resection are all alive after 1 year.
Recent studies have shown that neither tumor
diameter nor duodenocolic fistula presence (15) influence prognosis after en bloc
resection. Of the 4 patients with duodenocolic fistula in our
series, 2 are alive and disease-free at 6 years and 31 months,
respectively.
In conclusion, en bloc resection in RSCC invading
the duodenum/pancreas appears to control the disease in a
considerable number of patients. More studies are needed to
ascertain which method accompanying RH, DP or limited duodenal
resection, is preferable when duodenum alone is involved. When
limited duodenal resection is chosen, the ileal pedicled flap
technique provides the most benefit to the duodenal defect
closure.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
NC collected data, performed the literature search
and prepared the drafted paper. IB analyzed data and edited the
drafted paper. GVC and NB provided the supplementary material
(figure) and performed the statistical/grammatical revisions to the
manuscript. LD and NB provided revisions to the scientific content
of manuscript. All authors read and approved the final manuscript
for publication.
Ethics approval and consent to
participate
Not applicable as the study was retrospective and
the data were completely anonymized. Informed consent was obtained
from all individual participants involved in the study.
Patient consent for publication
Informed consent was obtained for use of all images
published in the study.
Competing interests
The authors declare that they have no competing
interests.
Authors' information
Nadejda Cojocari: ORCID ID: 0000-0003-3720-0869.
References
|
1
|
Gebhart C, Meyer W, Ruckriegel S and Meier
U: Multivisceral resection of advanced colorectal carcinoma.
Langenbecks Arch Surg. 348:194–199. 1999.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Harish K, Narayanaswamy Y and Nirmala S:
Treatment outcomes in locally advanced colorectal carcinoma. Int
Semin Surg Oncol. 1(8)2004.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Polk Jr HC: Extended resection for
selected adenocarcinomas of the large bowel. Ann Surg. 175:892–899.
1972.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Curley SA, Evans DB and Ames FC: Resection
for cure of carcinoma of the colon directly invading the duodenum
or pancreatic head. J Am Coll Surg. 179:587–592. 1994.PubMed/NCBI
|
|
5
|
Kapoor S, Das B, Pal S, Sahni P and
Chattopadhyay TK: En bloc resection of right-sided colonic
adenocarcinoma with adjacent organ invasion. Int J Colorectal Dis.
21:265–268. 2006.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Lee WS, Lee WY, Chun HK and Choi SH: En
bloc resection for right colon cancer directly invading duodenum or
pancreatic head. Yonsei Med J. 50:803–806. 2009.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Lianwen Y, Jianping Z, Guoshun S, Dongcai
L and Jiapeng Z: Pedicled Ileal flap for duodenal defect after
right hemicolectomy. Hepatogastroenterology. 57:493–496.
2010.PubMed/NCBI
|
|
8
|
Moriura S, Ikeda S, Ikezawa T, Naiki K,
Sakai T, Yokochi K and Kuroda M: Hepatocellulcar carcinoma invading
the duodenum: Combined resection of the lateral duodenum and repair
with a pedicled gastric flap. Dig Surg. 12:136–139. 1995.
|
|
9
|
Walley B and Goco I: Duodenal patch
grafting. Am J Surg. 140:706–708. 1980.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Aswaf I, Thomson NW and Huang CL: The open
jejunum: A patch for large duodenal defects. Am J Surg.
131:601–602. 1976.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Ishiguro S, Moriura S, Kobayashi I, Tabata
T, Yoshioka Y and Matsumoto T: Pedicled ileal flap to repair large
duodenal defect after right hemicolectomy for right colon cancer
invading the duodenum. Surg Today. 34:386–388. 2004.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Ionescu EM, Tieranu CG, Maftei D, Grivei
A, Olteanu AO, Arbanas T, Calu V, Musat S, Mihaescu-Pintia C and
Cucu IC: Colorectal cancer trends of 2018 in romania-an important
geographical variation between northern and southern lands and high
mortality versus european averages. J Gastrointest Cancer.
52:222–228. 2021.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Hakimi A, Rosing D, Stabile B and Petrie
AB: En bloc resection of the duodenum for locally advanced right
colon adenocarcinoma. Am Surg. 73:1063–1066. 2007.PubMed/NCBI
|
|
14
|
Koea JB, Conlon K, Paty PB, Guillem JG and
Cohen AM: Pancreatic and duodenal resection or both for advanced
carcinoma of the right colon: Is it justified? Dis Colon Rectum.
43:460–465. 2000.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Cirocchi R, Partelli S, Castellani E,
Renzi C, Parisi A, Noya G and Falconi M: Right hemicolectomy plus
pancreaticoduodenectomy vs partial duodenectomy in treatment of
locally advanced right colon cancer invading pancreas and/or only
duodenum. Surg Oncol. 23:92–98. 2014.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Charnsangavej C and Whittey N: Metastases
to the pancreas and peripancreatic lymph nodes from carcinoma of
the right side of the colon: CT findings in 12 patients. AJR Am J
Roentgenol. 160:49–52. 1993.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Melissas J, Schoretsantis G, Daskalakis M
and Tsiftsis D: Sigmoidoduodenal fistula as a rare complication of
colonic carcinoma: Report of a case. Surg Today. 33:623–625.
2003.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Kroneman H, Castelein A and Jeekel J: En
bloc resection of colon carcinoma adherent to other organs: An
efficacious treatment? Dis Colon Rectum. 34:780–783.
1991.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Gall FP, Tonak J, Altendorf A and Kuruz U:
Operative tactics and results in extensive operations for
colorectal cancer. Langenbecks Arch Chir. 366:445–450.
1985.PubMed/NCBI View Article : Google Scholar : (In German).
|
|
20
|
McGlone T, Bernie W and Elliott D:
Survival following extended operations for extracolonic invasion by
colon cancer. Arch Surg. 117:595–599. 1982.PubMed/NCBI View Article : Google Scholar
|
|
21
|
McSherry CK, Cornell GN and Glenn F:
Carcinoma of the colon and rectum. Ann Surg. 169:502–509.
1969.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Sugarbaker ED: Coincident removal of
additional structures in resections for carcinoma of the colon and
rectum. Ann Surg. 123:1036–1046. 1949.PubMed/NCBI
|
|
23
|
Fuks D, Pesaux P, Tuech JJ, Mauvais F,
Brehant O, Dumont F, Chatelain D, Yzet T, Joly JP, Lefebure B, et
al: Management of patients with carcinoma of the right colon
invading the duodenum or pancreatic head. Int J Colorectal Dis.
23:477–481. 2008.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Linton RR: Two stage operation for
carcinoma of transverse colon producing duodeno-colic fistula.
Report of two cases. Arch Surg. 48:197–207. 1944.
|
|
25
|
Van Prohaska J, Govostis MC and Wasick M:
Multiple organ resection for advanced carcinoma of the colon and
rectum. Surg Gynecol Obstet. 97:177–182. 1953.PubMed/NCBI
|
|
26
|
Mills JRM and Mills JR: Malignant
duodenocolic fistula-report of a case treated successfully by mass
resection. Con J Surg. 3:91–92. 1959.PubMed/NCBI
|
|
27
|
Yoshimi F, Asato Y, Kuroki Y, Shioyama Y,
Hori M, Itabashi M, Amemiya R and Koizumi S: Pancreatoduodenectomy
for locally advanced or recurrent colon cancer: Report of two
cases. Surg Today. 29:906–910. 1999.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Saiura A, Yamamoto J, Ueno M, Koga R, Seki
M and Kokudo N: Long-term survival in patients with locally
advanced colon cancer after en bloc pancreaticoduodenectomy and
colectomy. Dis Colon Rectum. 51:1548–1551. 2008.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Izumi Y, Ueki T, Naritomi G, Akashi Y,
Miyoshi A and Fukuda T: Malignant duodenocolic fistula: Report of a
case and considerations for operative management. Surg Today.
23:920–925. 1993.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Bacalbasa N, Balescu I, Tanase A, Pautov
M, brezean I, Vilcu M and Brasoveanu V: Spleno-pancreatectomy En
Bloc with parcelar gastrectomy for splenic artery aneurysm-a case
report and literature review. In Vivo. 32:915–919. 2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Bacalbasa N, Balescu I, Dima S, Brasoveanu
V and Popescu I: Pancreatic resection as part of cytoreductive
surgery in advanced-stage and recurrent epithelial ovarian cancer-a
single-center experience. Anticancer Res. 35:4125–4129.
2015.PubMed/NCBI
|
|
32
|
Bacalbasa N, Stoica C and Balescu I:
Multiple visceral resections for synchronous left and transverse
colon adenocarcinoma with gastrocolic-cutaneous fistula-case report
and literature review. Anticancer Res. 37:2601–2607.
2017.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Bacalbasa N and Balescu I: Infracolic
approach to the superior mesenteric vessels for a large pancreatic
tumor with right colon invasion-a case report and literature
review. Anticancer Res. 37:2609–2613. 2017.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Jones AS and Joergensen EJ: Closure of
duodenal wall defects. Surgery. 53:438–442. 1963.PubMed/NCBI
|
|
35
|
Yoshioka I, Matsui K, Okumura T, Yoshida
T, Shimada Y and Tsukada K: Pedicled jejunal patch duodenoplasty
for traumatic duodenal injury report of a successfully treated
case. Am Surg. 76:789–790. 2010.PubMed/NCBI
|
|
36
|
McIlrath DC and Larson RH: Surgical
management of large perforations of the duodenum. Surg Clin North
Am. 51:857–861. 1971.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Hamed S, Guilbaud T, Hardwigsen J and Le
Treut IP: Ileal flap duodenoplasty to repair large duodenal defects
after R0 resection for malignant tumor to avoid a complex
reconstruction:experience with 6 cases. Clin Surg. 3(2110)2018.
|
|
38
|
Maillet F, Bourgouin S, Gaubert L and
Balandraud P: Duodenal reconstruction following extended right
colectomy: The pedicled ileal flap technique. J Gastrointest Surg.
21:746–748. 2017.PubMed/NCBI View Article : Google Scholar
|