Introduction
ST-segment elevation myocardial infarction (STEMI)
remains the most dangerous type of acute coronary syndrome (ACS),
causing >30% of all mortalities and significantly increasing the
familial and social health burden (1). Particularly patients with multiple
vessel disease have a higher mortality and morbidity (2). Long-term outcomes of STEMI are
associated with complex factors, including demographics,
comorbidities and severity of STEMI. Various tools have been
developed (3) and biomarkers have
been used (4,5) for predicting outcomes for patients
with STEMI. Risk stratification helps to identify high-risk
patients and apply prevention measures. However, those tools have
certain disadvantages, including unstable performance, complex
calculation and low predictive value. Sakamoto et al
(6) compared the HEART, TIMI and
GRACE scores for the prediction of 30-day major adverse cardiac
events in patients with high acuity chest pain in the emergency
department and found that the HEART score to be superior to the
TIMI and GRACE scores in predicting 30-day MACE. In addition,
Hammami et al (7)
demonstrated that the GRACE and TIMI scores correlated moderately
with the extent of coronary disease assessed by the SYNTAX score,
and they could predict obstructive CAD but not severe disease.
Depending on coronary angiography, the SYNTAX score
is widely applied in evaluating the severity of ACS and predicting
outcomes (8). Compared with the
SYNTAX score, the thrombolysis in myocardial infarction (TIMI) risk
index is a far simpler tool (9).
Calculated using only the age, heart rate and systolic blood
pressure (SBP), the TIMI risk index has been used to predict
mortality in patients with STEMI (10). Pieces of evidence indicated that the
TIMI risk index holds value in predicting early mortality of
patients with STEMI (9). However,
the value of the TIMI risk index in long-term outcome prediction
has rarely been investigated, particularly for patients with
multiple vessel disease. The present study aimed to investigate the
efficacy of TIMI risk index in prediciting long-term outcomes of
patents with ST-elevation myocardial infarction and multiple vessel
disease.
Materials and methods
Patients
In the present prospective observational cohort
study, all patients encountered from Department of Cardiology,
Xianyang Hospital of Yan'an University (Shanxi, China) between June
2013 and July 2014 meeting the following criteria were enrolled: i)
Age of 18-80 years; ii) examination with digital subtraction
angiography and diagnosis of STEMI and multiple vessel disease;
iii) revascularization treatment of percutaneous coronary
intervention (PCI); iv) survival of the patient in the hospital; v)
the patient and family must be willing to participate and signed
informed consent. The exclusion criteria were as follows: i)
Patients diagnosed with non-(N)STEMI or unstable angina; ii)
patients in a coma or condition of unconsciousness; iii) patients
and family do not cooperate with the follow-up. According to the
2017 ESC Guidelines for the Management of STEMI, STEMI was defined
as electrocardiographic ST-segment elevation of ≥2 mm in 2 or more
contiguous chest leads or ≥1 mm in 2 or more limb leads or new
onset of left bundle-branch block, together with chest pain or
other typical symptoms and elevated troponin levels >99th
percentile [Immunoscattering turbidimetric method; cardiac troponin
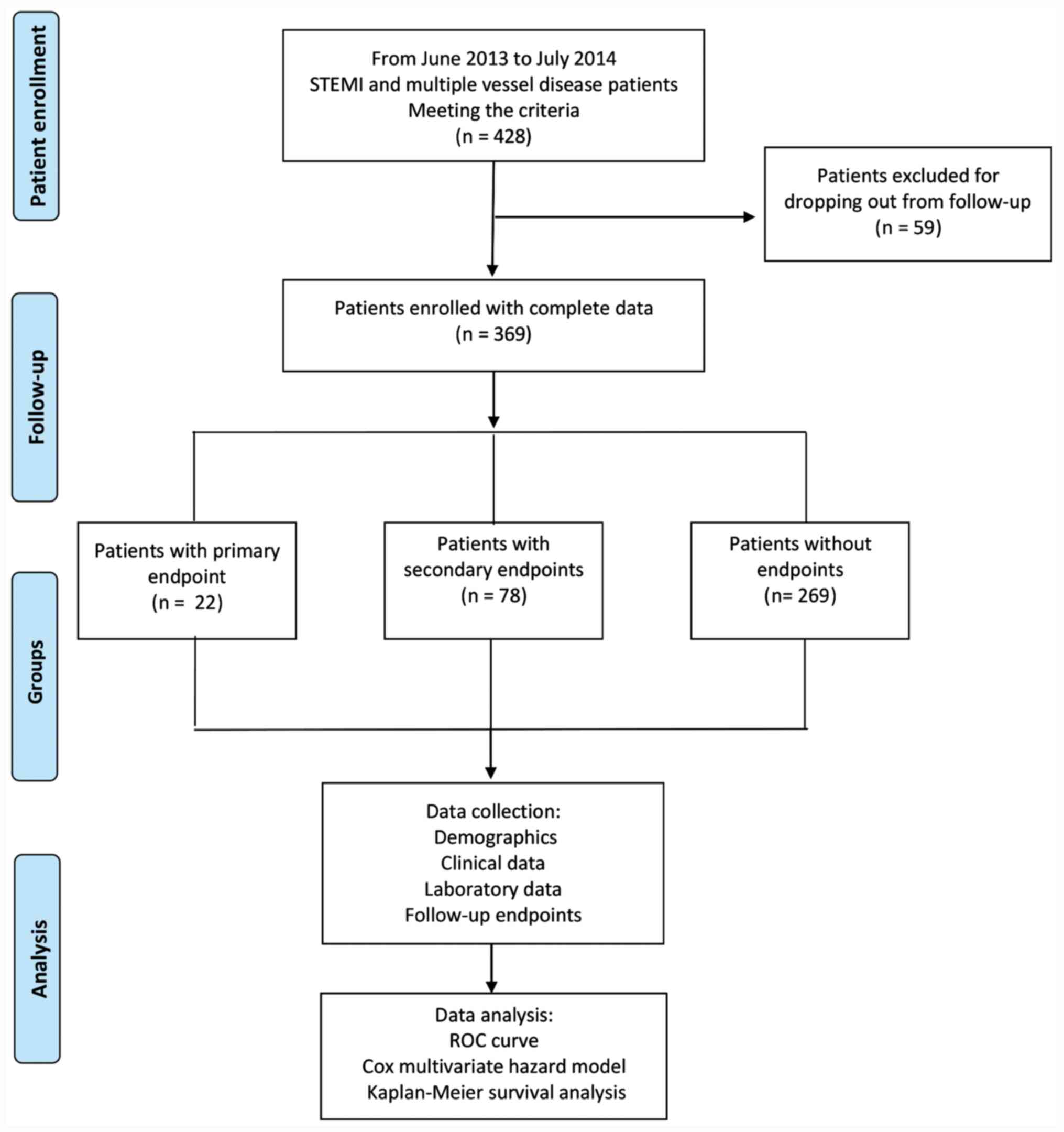
T (cTnT) <0.5 mg/l, cardiac troponin I <0.03 mg/l] (11). A flow chart depicting the study
design is presented in Fig. 1.
A total of 428 patients with STEMI were enrolled in
the present prospective observational cohort study. All patients
and their family were informed of the present study and provided
written informed consent. The present study was approved by the
Medical Ethics Committee of Xianyang Hospital of Yan'an University
(Xianyang, China).
PCI procedure and treatment
Coronary angiography and interventional therapy were
performed using conventional methods. PCI strategy and stent
selection were determined by the surgeon according to the condition
of each patient. PCI was successfully defined as coronary
angiography exhibiting residual lumen stenosis <10% and blood
flow classification was TIMI grade 3. In patients with emergency
PCI, aspirin (300 mg) was administered as soon as possible prior to
surgery and oral clopidogrel (300-600 mg) or (ticagrelor 180 mg)
was orally administered. Patients with elective PCI who had no
contraindications and no history of long-term oral anti-platelet
drug treatment prior to surgery received oral aspirin (300 mg) and
clopidogrel (300 mg) or ticagrelor (180 mg) at least 24 h prior to
surgery. Patients were given oral aspirin (100 mg/day) and
clopidogrel (75 mg/day) or telgrelor (90 mg twice daily) for at
least one year after surgery and oral secondary prevention drugs
according to the guidelines.
Group and data collection
Clinical data were collected from the electronic
database of the hospital. Routine myocardial injury markers,
including cardiac troponin T (cTnT), as well as creatine
kinase-myocardial band and other laboratory indicators, including
creatinine, NT-proB-type natriuretic peptide and high-sensitivity
C-reactive protein (hsCRP), were also tested and recorded. The TIMI
risk index was defined as follows: [Heart rate x
(age/10)2]/SBP (heart rate measured in bpm; age measured
in years and SBP measured in mmHg). Heart rate, age and SBP were
the values on admission. The SYNTAX score was calculated with all
required parameters at admission via the website (http://www.syntaxscore.com/). The required coronary
angiography results for the SYNTAX score were confirmed by at least
two cardiologists or radiologists (12). Receiver operating characteristic
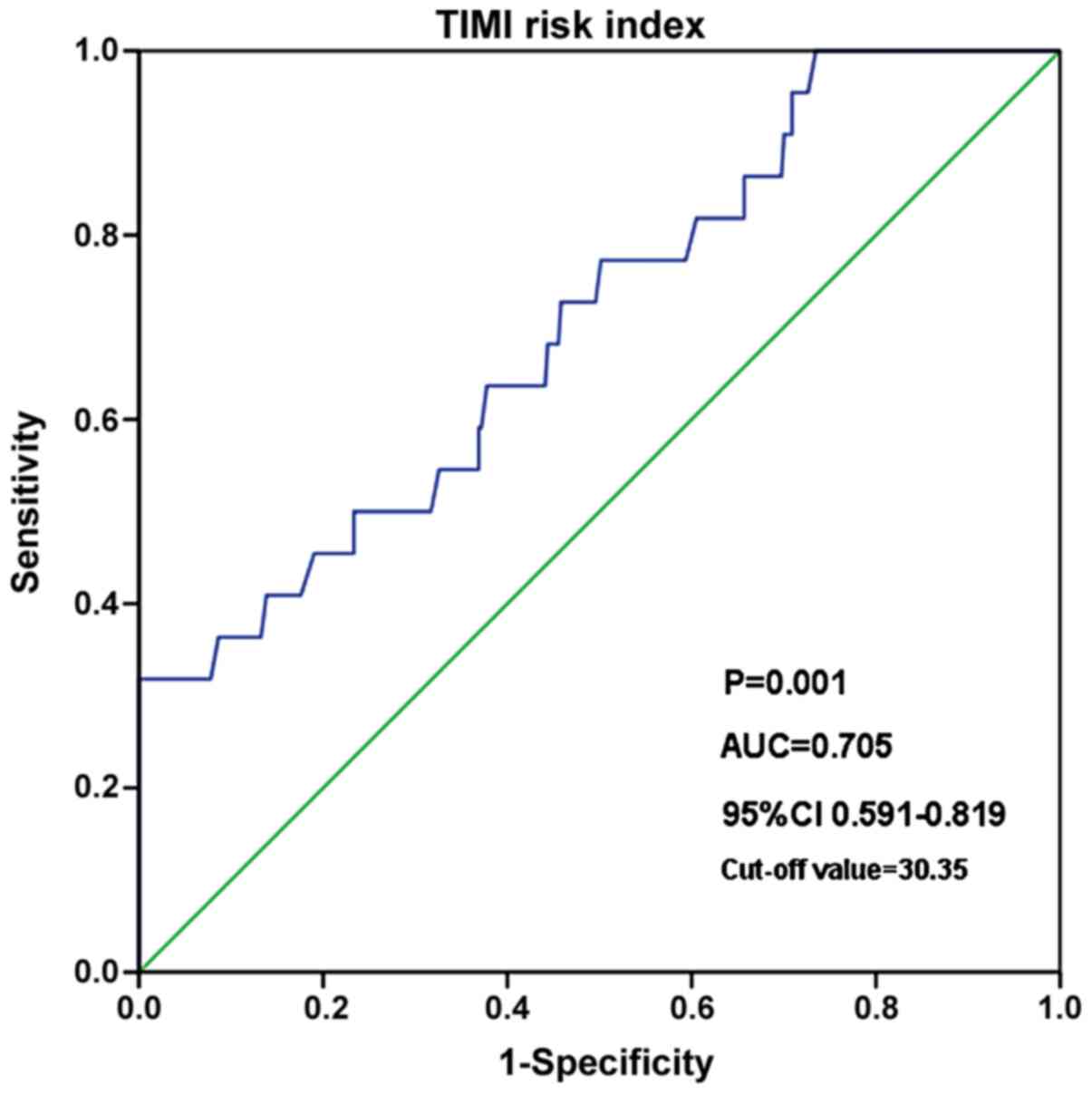
(ROC) curve analysis was performed to determine the value of the
TIMI risk index in predicting all-cause death and the best cut-off
value was determined to be 30.35. The enrolled patients were
divided into the high TIMI group (>30.35) and low TIMI group
(<30.35).
Clinical endpoints
The primary endpoint was defined as all-cause
mortality during the follow-up, while the secondary endpoints were
considered to be a composite of adverse events, including
myocardial infarction, stroke, unscheduled revascularization or
rehospitalization for heart failure. Myocardial infarction was
confirmed using a commonly used criteria (11). Unscheduled revascularization was
defined as revascularization treatment of any coronary artery
disease driven by ischemic symptoms or events, including PCI and
coronary artery bypass grafting.
Follow-up
All enrolled patients were followed up by telephone
or visits to the clinic at 1, 3, 6 and 12 months every year
following discharge for a total of 5 years or until primary or
secondary endpoints. Items determined at the follow-up included
survival, myocardial infarction, stroke, unscheduled
revascularization or rehospitalization due to heart failure. Data
for patients with self-dropout or missed contact were presented as
censored data, which was included in the survival analysis.
Statistical analysis
SPSS version 19.0 (IBM Corp.) was used for
statistical analysis in the present study. Kolmogorov-Smirnov (K-S)
test was performed to assess the normality distribution of
variables. Continuous variables following a normal distribution
were expressed as the mean ± standard deviation and categorical
variables were presented as proportions, while continuous variables
not fitting the normal distribution were described as the median
and interquartile range. Comparison of continuous variables between
different groups was performed using one-way analysis of variance
and Tukey's multiple-comparisons test of independent samples. The
Kruskal-Wallis test and Dunn's multiple-comparisons test were
adopted for comparison between different groups for non-normal
variables of independent samples. The χ2 test was
performed for comparison of categorical variables.
The Cox hazards model was adopted as the regression
method to compare the relative hazard between the high TIMI group
and the low TIMI group. Univariate analysis between covariates and
endpoints was performed and covariates with P<0.10 were also
subjected to multivariate analysis. Kaplan-Meier survival curves
and log-rank tests were used to compare the survival status between
subgroups. Receiver Operating Characteristic (ROC) analysis was
conducted to determine the cut-off value of TIMI index and SYNTAX
score for predicting long-term mortality, where the area under
curve (AUC) was also calculated. P<0.05 was considered to
indicate statistical significance.
Results
Demographics and clinical data
Among all 428 patients enrolled in the present
study, 369 patients completed the follow-up and passed the final
data integrity check after five years of follow-up. The average
follow-up time was 52.3±18.4 months. During the follow-up, 22
patients died (6.0%), while 78 patients developed secondary
endpoints (21.1%). The demographics and clinical data of patients
with or without endpoints are compared in Table I. Patients with primary endpoint
were significantly older compared with patients with secondary
endpoint (P=0.034). Patients with secondary endpoint were also
significantly older compared with patients without endpoints
(P=0.020). The BMI of patients with secondary endpoint was lower
compared with patient from the other two groups (P=0.029 vs.
patients without endpoints; P=0.013 vs. patients with primary
endpoint), whilst the BMI of patients from other two groups were
comparable (P=0.342). However, there was no statistical difference
among the three groups in terms of sex (P=0.096) and smoking status
(P=0.882). In terms of NYHA grade, patients with primary endpoint
was significantly associated with higher NYHA grade compared with
those from other two groups (both P<0.05), with no statistical
difference observed between patients with secondary endpoint and
patients without endpoints (P=0.908). Patients with primary
endpoint also had significantly higher proportions of hypertension
compared with the other two groups (P=0.006), while there was no
significant difference all for other comorbidities recorded (All
P>0.05). Patients with secondary endpoints had lower Peak cTnT
levels compared with those with primary endpoint (P=0.007), but no
statistical differences were found with the other two group
comparisons (P>0.05). With regards to the SYNTAX score, patients
with primary endpoint was higher compared with those in the other
two groups (P<0.05), whilst patients with second endpoint was
higher than those without endpoint (P<0.05). However, TIMI risk
index of patients with no endpoint was lower compared with patients
with primary endpoints and patients with secondary endpoints
(P<0.001), but there was no difference between those from
primary and secondary endpoints (P=0.399).
 | Table IDemographic characteristics and
clinical data of the patients enrolled stratified based on the
availability of data on endpoints. |
Table I
Demographic characteristics and
clinical data of the patients enrolled stratified based on the
availability of data on endpoints.
| Variables | Patients without
endpoints (n=269) | Patients with the
primary endpoint (n=22) | Patients with the
secondary endpoint (n=78) | P-value |
|---|
| Demographics | | | | |
|
Age
(years) | 62.2±16.0 |
74.2±10.8a |
66.7±10.0a,b | <0.001 |
|
Male
sex | 162 (60.2) | 17 (77.3) | 55 (70.5) | 0.096 |
|
BMI
(kg/m2) | 24.9±3.2 | 25.6±2.7 | 23.9±3.1a,b | 0.021 |
|
Smoking | 98 (36.4) | 9 (40.9) | 30 (38.5) | 0.882 |
| NYHA grade | | | | 0.011 |
|
I | 72 (26.8) | 3 (13.6) | 17 (21.8) | |
|
II | 87 (32.3) | 6 (27.3) | 31 (39.7) | |
|
III | 90 (33.5) | 6 (27.3) | 22 (28.2) | |
|
IV | 20 (7.4) | 7 (31.8)a | 8 (10.3)b | |
|
LVEF | 49.6±10.0 |
43.6±12.6a | 49.8±9.4b | 0.025 |
| Comorbidities | | | | |
|
Heart
failure | 69 (25.7) | 10 (45.5) | 20 (25.6) | 0.127 |
|
Hypertension | 64 (23.8) | 12
(54.5)a | 23
(29.5)b | 0.006 |
|
Diabetes
mellitus | 37 (13.8) | 4 (18.2) | 11 (14.1) | 0.848 |
|
Chronic
kidney disease | 13 (4.8) | 2 (9.1) | 4 (5.1) | 0.686 |
|
Chronic lung
disease | 35 (13.0) | 3 (13.6) | 5 (6.4) | 0.266 |
|
Cerebrovascular
disease | 18 (6.7) | 1 (4.5) | 5 (6.4) | 0.925 |
|
Tumor | 7 (2.6) | 1 (4.5) | 2 (2.6) | 0.861 |
| Laboratory test at
admission | | | | |
|
Peak cTnT
(ng/dl) | 4.87 (3.16,6.44) | 6.31 (3.85,6.99) | 4.14
(2.74,5.99)b | 0.019 |
|
Peak CK-MB
(ng/dl) | 549.3
(420.6,671.4) | 466.3
(387.0,663.1) | 603.2
(408.2,713.5) | 0.299 |
|
Creatinine
(µmol/l) | 104 (75,132.5) | 105 (74.25,136) | 92 (69.75,127) | 0.278 |
|
NT-proBNP
(ng/l) | 71.1
(27.25,123.1) | 91.3
(55.73,168.43) | 74.2
(35.88,123.15) | 0.212 |
|
hsCRP
(mg/l) | 21.5
(12.95,29.5) | 30.9
(24.7,42.65)a | 26.25
(17.5,35.08)a,b | <0.001 |
|
SYNTAX
score | 24.4
(18.9,30.35) | 29.9
(25.05,38.18)a | 27.65
(23.88,31.2)a,b | <0.001 |
|
TIMI risk
index | 13 (8.5,16) | 17.5
(13.5,23.25)a | 17.5
(12,22)a | <0.001 |
ROC analysis
Fig. 2 presents the
ROC analysis for the TIMI risk index to predict all-cause death.
ROC analysis demonstrated that the TIMI risk index was a
significant predictive factor with an area under the curve (AUC) of
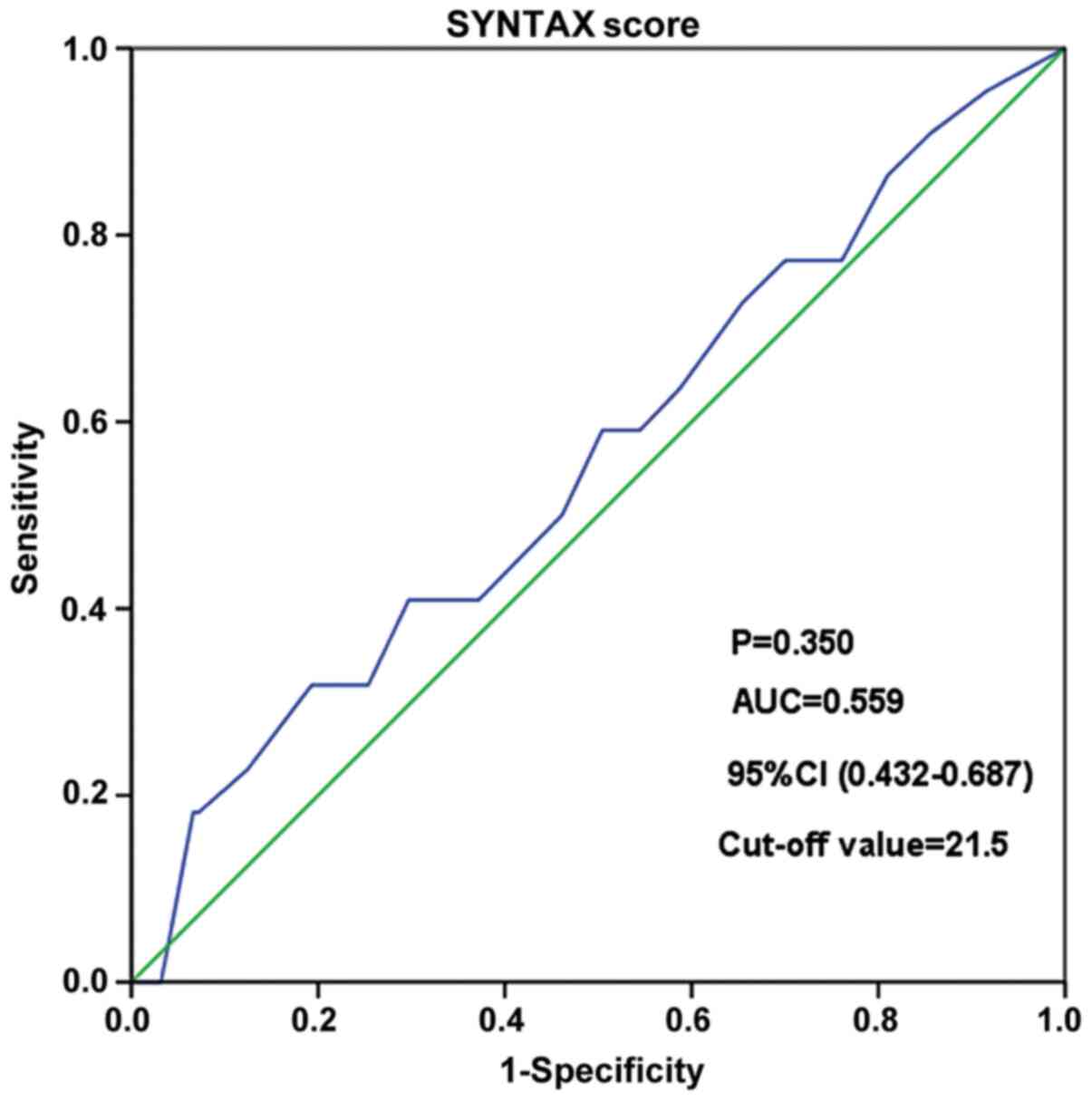
0.705 (95% CI: 0.591-0.819, P=0.001). As for the SYNTAX score,
there was no statistical significance for the prediction of
all-cause death [AUC=0.559, 95% CI: 0.432-0.687, P=0.350; Fig. 3].
Cox regression analysis
Cox regression analysis was performed to evaluate
the risk factors for the primary and secondary endpoints. As
presented in Table II,
multivariate Cox regression analysis demonstrated that a high TIMI
risk index, age and hypertension were independent risk factors for
all-cause death (all P<0.05). Patients with a high TIMI risk
index had a hazard ratio of 3.709 (95% CI: 1.521-9.046) for
all-cause death compared to those with a low TIMI risk index
(P=0.004).
| Table IIMultivariate Cox regression analysis
of primary endpoints. |
Table II
Multivariate Cox regression analysis
of primary endpoints.
| Risk factor | B | SE | Wald | P-value | HR | 95% CI |
|---|
| TIMI risk
index | 1.311 | 0.455 | 8.304 | 0.004 | 3.709 | 1.521-9.046 |
| Age | 0.050 | 0.018 | 7.230 | 0.007 | 1.051 | 1.014-1.089 |
| BMI | 0.080 | 0.076 | 1.093 | 0.296 | 1.083 | 0.933-1.258 |
| NYHA grade | 0.431 | 0.244 | 3.115 | 0.078 | 1.539 | 0.953-2.485 |
| Hypertension | 1.524 | 0.471 | 10.463 | 0.001 | 4.589 | 1.823-11.552 |
| cTNT | 0.147 | 0.126 | 1.375 | 0.241 | 1.159 | 0.906-1.482 |
| hsCRP | 0.089 | 0.022 | 15.638 | 0.999 | 1.000 | 1.046-1.093 |
The risk factors for secondary endpoints were also
explored (Table III). The Cox
regression analysis, whether adjusted or unadjusted, indicated that
a high TIMI risk index was not an independent risk factor for the
composite of secondary endpoints and also not for each single
endpoint (all P>0.05).
| Table IIIMultivariate Cox regression analysis
of secondary endpoints influenced by high TIMI vs. low TIMI. |
Table III
Multivariate Cox regression analysis
of secondary endpoints influenced by high TIMI vs. low TIMI.
| | Unadjusted |
Adjusteda |
|---|
| Secondary
endpoint | HR (95%CI) | P-value | HR (95%CI) | P-value |
|---|
| Myocardial
infarction | 1.336
(0.694-2.570) | 0.386 | 1.462
(0.756-2.830) | 0.259 |
| Stroke | 1.991
(0.333-11.916) | 0.451 | 2.457
(0.386-15.632) | 0.341 |
| Emergent
revascularization | 0.473
(0.140-1.600) | 0.487 | 1.413
(0.143-1.657) | 0.249 |
| Readmission due to
heart failure | 2.411
(0.647-8.979) | 0.190 | 2.333
(0.616-8.836) | 0.213 |
| Overall | 1.174 (0.
717-1.923) | 0.523 | 1.267
(0.770-2.082) | 0.352 |
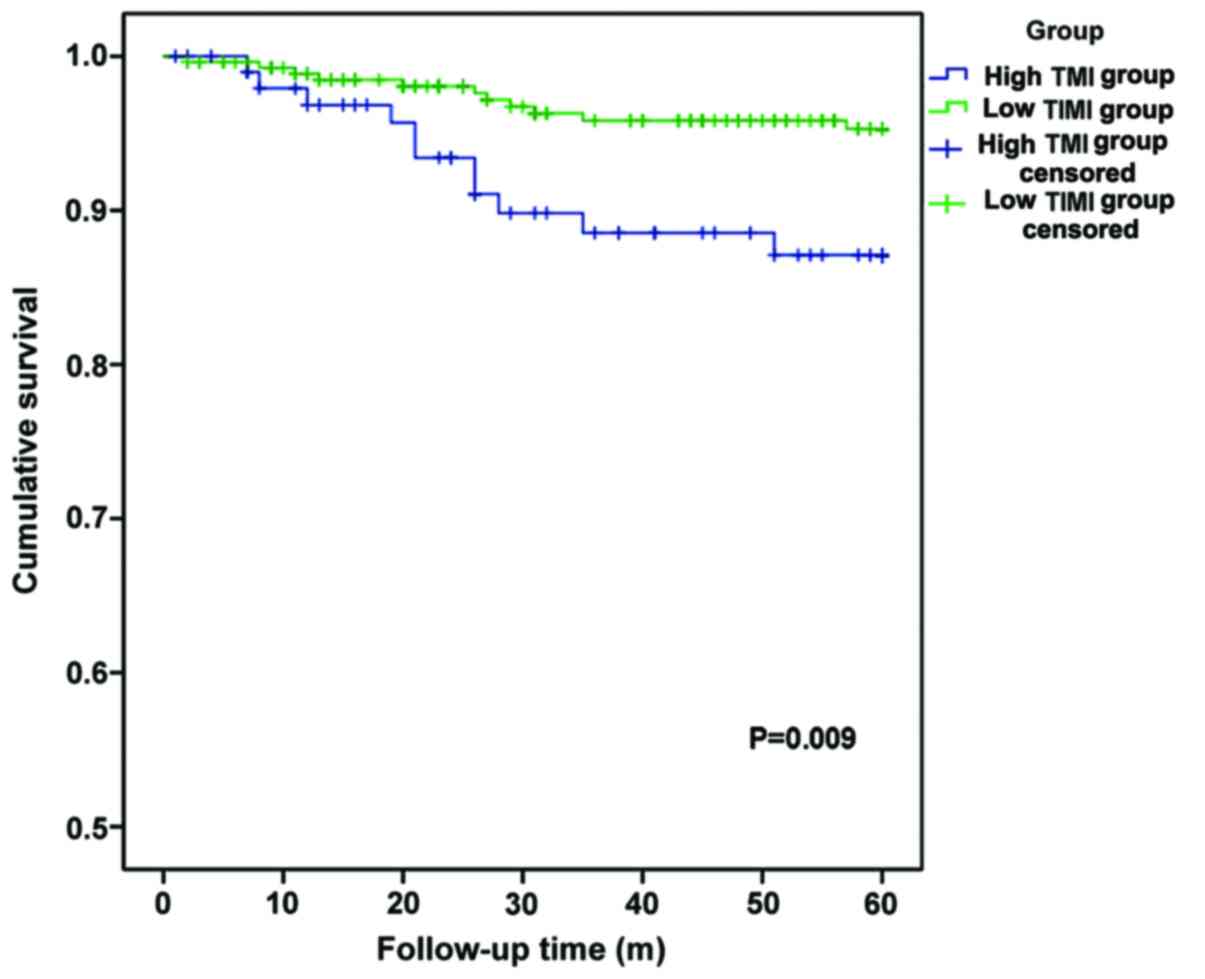
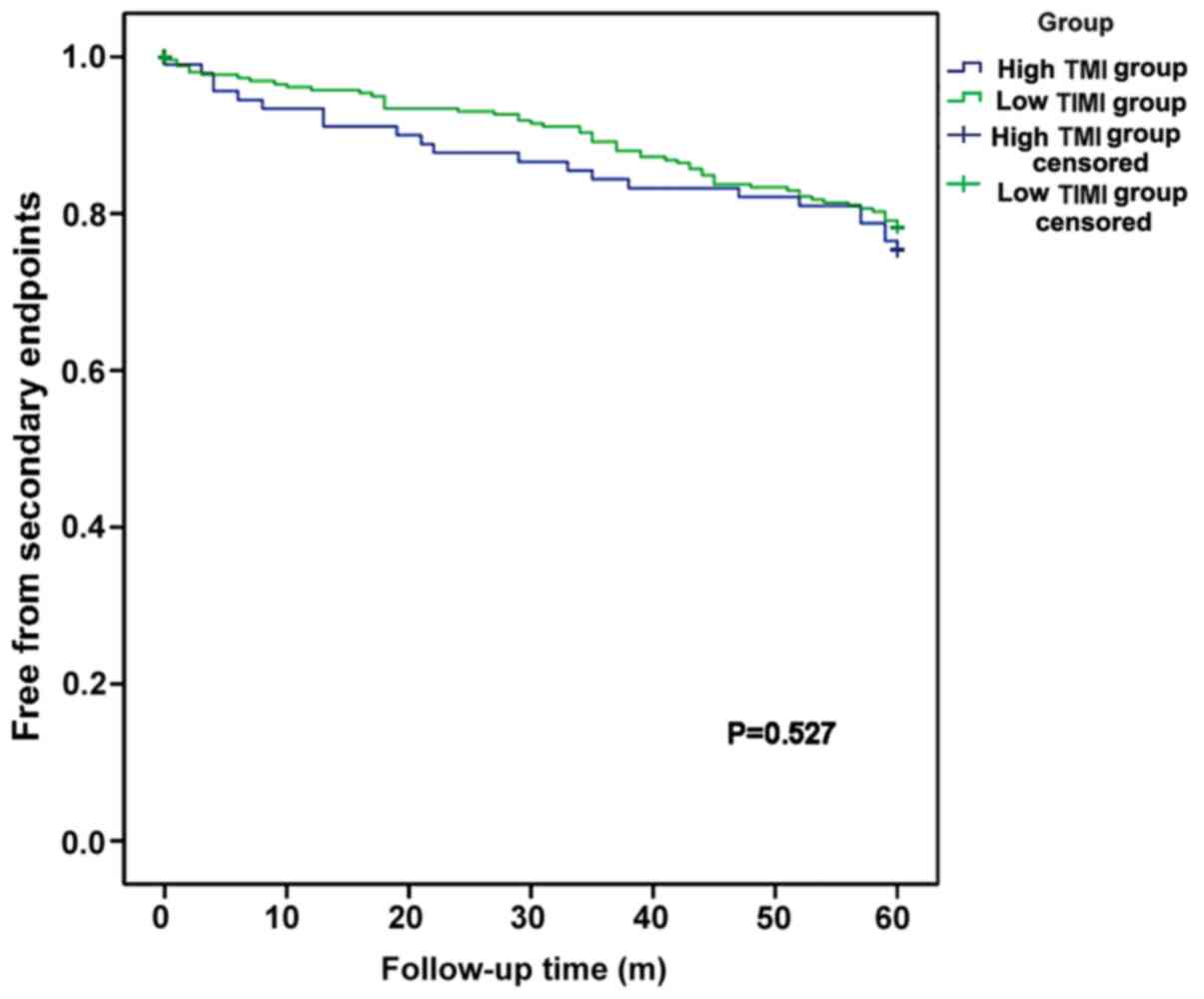
Survival analysis
To validate the long-term outcomes of the two
groups, a survival analysis was performed (Figs. 4 and 5). As presented in Fig. 4, patients with a high TIMI risk
index and patients with a low TIMI risk index had significantly
different survival curves. The high TIMI group had a significantly
lower five-year survival (P=0.009). However, there was no
significant difference between the high TIMI risk index and low
TIMI risk index groups in the curves for the incidence of secondary
endpoints (P=0.527).
Discussion
In the present study, the predictive value of the
TIMI risk index regarding the long-term outcomes of patients with
STEMI with multiple vessel disease was investigated. The ROC curve
analysis suggested that the TIMI risk index was able to predict
all-cause mortality within five years after PCI. Further analysis
validated this result by comparing the long-term outcomes for
patients with a high TIMI risk index and with a low TIMI risk
index, revealing a significant difference in all-cause mortality.
Risk factor analysis performed using the Cox regression model
proved that a high TIMI risk index (>30.35) was an independent
risk factor for all-cause death, but not for any secondary adverse
events, including myocardial infarction, stroke, unscheduled
revascularization or rehospitalization for heart failure.
Patients with STEMI have a poor prognosis and early
identification of high-risk patients is critical, particularly for
those with multiple vessel disease (2). A simple, cost-effective and sufficient
risk assessment approach helps clinicians take more aggressive
interventions and follow-up measures to improve outcomes. The
Global Registry of Acute Coronary Events (GRACE) scores is widely
used in the clinic for risk stratification of patients with ACS,
but these scoring systems require a more detailed medical history,
laboratory tests and even hemodynamic parameters to increase the
capacity of risk stratification (6). Therefore, these scoring systems may
have limitations in clinical applications. The TIMI risk index is
calculated using three parameters: Age, heart rate and systolic
blood pressure, which is convenient for clinicians to rapidly
determine the condition of the patient during the first medical
consultation and provide a necessary strategy for subsequent risk
stratification, including the accurate GRACE score (13). Based on the TIMI risk index, the
clinician may simply classify the patient as high- or low-risk
regarding long-term mortality and may then adopt different
treatment strategies.
Plenty of studies have suggested the value of the
TIMI risk index in risk stratification of patients with ACS. The
InTIME II substudy demonstrated that the TIMI risk index was useful
in the rapid triage of patients with STEMI outside the hospital or
on first arrival at the hospital as a simple tool and may predict
in-hospital mortality (14). The
Effective Cardiac Treatment study indicated that the TIMI risk
index is a simple, valid and moderately accurate tool for risk
stratification for early death in patients with STEMI and NSTEMI in
a community setting (9). In the
TIMI 2 clinical trial, the TIMI risk index was demonstrated to
predict long-term mortality and chronic heart failure (CHF) as well
as composite death and CHF in patients with STEMI (15). However, most studies focused on the
value of the TIMI risk index in the short term rather than
long-term outcomes. Of note, the revascularization rates of those
studies were 53-36% (9,10,16),
not as high as those in recent studies.
At present, there is limited evidence regarding the
predictive value of the TIMI risk index in STEMI patients with
multiple vessel disease. The present study demonstrated that the
TIMI risk index is of value in predicting long-term mortality of
patients with STEMI and multiple vessel disease. Multivariate Cox
regression analysis revealed that age, hypertension and the TIMI
risk index were independent risk factors for the primary endpoint.
As mentioned above, the TIMI risk index was calculated using the
age, heart rate and SBP. Hence, the TIMI risk index is associated
with age and hypertension. However, the TIMI risk index is a
comprehensive indicator reflecting the condition of the patient.
The regression model also demonstrated its independence from age
and hypertension.
Although the TIMI risk index was associated with the
primary endpoint, it had no predictive value regarding secondary
endpoints. This may be due to two reasons: On the one hand, the
sample size may have been insufficient to obtain a significant
difference, even regarding individual adverse events, including
heart failure. On the other hand, the TIMI risk index was not
associated with those adverse events, but with other possibly
lethal complications.
Comparison of the SYNTAX score and TIMI risk index
indicated that the SYNTAX score had a lower predictive value than
the TIMI risk index. Brkovic (17)
compared the prognostic value of the SYNTAX, GRACE, TIMI, Zwolle
risk score (ZRS), the Controlled Abciximab and Device Investigation
to Lower Late Angioplasty Complications (CADILLAC) and Primary
Angioplasty in Myocardial Infarction (PAMI) risk scores in patients
with acute STEMI treated by primary percutaneous coronary
intervention and indicated that the SYNTAX score improves the
prognostic performance of the well-established GRACE, TIMI, ZRS and
PAMI clinical scores, but not the CADILLAC risk score. A Chinese
study suggested that TIMI risk index (TRI) is independently
associated with a SYNTAX score of ≥33. TRI is also an independent
risk factor for 2-year all-cause death, cardiac death and stent
thrombosis in patients with AMI undergoing PCI (16). The cut-off value for the TIMI risk
index in the present study was 30.35 which was almost the
first-quartile level, with 100 patients (27.1%) above and 2.69
patients (72.9%) below this cut-off value. The proportion of
patients with a high TIMI risk index in the group of patients with
the primary endpoint was higher than that in the other two groups.
This cut-off value was higher than those in previous studies
(16), with a cut-off value of
23.05, which may be attributed to different follow-up times and
inclusion criteria. The sample size and observational nature of the
study were the limitations of the present study, and further cohort
studies and meta-analyses are required to validate the present
results.
In conclusion, the TIMI risk index was associated
with long-term mortality of patients with STEMI and multiple vessel
disease, and may be utilized for risk stratification for such
patients.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
XF and ZL designed and led this study. ML and JC
collected and analyzed the general patient data. XF and ML wrote
the manuscript. XF and ZL confirm the authenticity of all the raw
data. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Medical Ethics
Committee of Yueqing Third People's Hospital (Yueqing, China). The
patients provided written informed consent regarding the use of
their data.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ruff CT and Braunwald E: The evolving
epidemiology of acute coronary syndromes. Nat Rev Cardiol.
8:140–147. 2011.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Lee WC, Wu BJ, Fang CY, Chen CJ, Yang CH,
Yip HK, Hang CL, Wu CJ and Fang HY: Timing of staged percutaneous
coronary intervention for a non-culprit lesion in patients with
anterior wall ST segment elevation myocardial infarction with
multiple vessel disease. Int Heart J. 57:417–423. 2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Acet H, Ertas F, Bilik MZ, Aydın M, Yüksel
M, Polat N, Yıldız A, Özyurtlu F, Akıl MA, Çiftçi L, et al: The
relationship of TIMI risk index with SYNTAX and Gensini risk scores
in predicting the extent and severity of coronary artery disease in
patients with STEMI undergoing primary percutaneous coronary
intervention. Ther Adv Cardiovasc Dis. 9:257–266. 2015.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Damman P, Kampinga MA, van der Horst IC,
Woudstra P, Grundeken MJ, Kuijt WJ, Harskamp RE, Nijsten MW,
Zijlstra F, Tijssen JG, et al: Multiple biomarkers for the
prediction of short and long-term mortality after ST-segment
elevation myocardial infarction: The Amsterdam Groningen
collaboration. J Thromb Thrombolysis. 36:42–46. 2013.PubMed/NCBI View Article : Google Scholar
|
|
5
|
He J, Li J, Wang Y, Hao P and Hua Q:
Neutrophil-to-lymphocyte ratio (NLR) predicts mortality and
adverse-outcomes after ST-segment elevation myocardial infarction
in Chinese people. Int J Clin Exp Pathol. 7:4045–4056.
2014.PubMed/NCBI
|
|
6
|
Sakamoto JT, Liu N, Koh ZX, Fung NX,
Heldeweg ML, Ng JC and Ong ME: Comparing HEART, TIMI, and GRACE
scores for prediction of 30-day major adverse cardiac events in
high acuity chest pain patients in the emergency department. Int J
Cardiol. 221:759–764. 2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Hammami R, Jdidi J, Mroua F, Kallel R,
Hentati M, Abid L and Kammoun S: Accuracy of the TIMI and GRACE
scores in predicting coronary disease in patients with
non-ST-elevation acute coronary syndrome. Rev Port Cardiol.
37:41–49. 2018.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Tarasov RS, Ganiukov VI, Shilov AA,
Barbarash OL and Barbarash LS: Prognostic value of SYNTAX score for
outcomes and revascularization strategy choice in ST-segment
elevation myocardial infarction patients with multivessel coronary
artery disease. Ter Arkh. 84:17–21. 2012.PubMed/NCBI(In Russian).
|
|
9
|
Bradshaw PJ, Ko DT, Newman AM, Donovan LR
and Tu JV: Validation of the Thrombolysis In Myocardial Infarction
(TIMI) risk index for predicting early mortality in a
population-based cohort of STEMI and non-STEMI patients. Can J
Cardiol. 23:51–56. 2007.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Wiviott SD, Morrow DA, Frederick PD,
Giugliano RP, Gibson CM, McCabe CH, Cannon CP, Antman EM and
Braunwald E: Performance of the thrombolysis in myocardial
infarction risk index in the National Registry of Myocardial
Infarction-3 and -4: A simple index that predicts mortality in
ST-segment elevation myocardial infarction. J Am Coll Cardiol.
44:783–789. 2004.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Ibanez B, James S, Agewall S, Antunes MJ,
Bucciarelli-Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA,
Halvorsen S, et al: 2017 ESC Guidelines for the management of acute
myocardial infarction in patients presenting with ST-segment
elevation: The Task Force for the management of acute myocardial
infarction in patients presenting with ST-segment elevation of the
European Society of Cardiology (ESC). Eur Heart J. 39:119–177.
2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Karabag Y, Çağdaş M, Rencuzogullari I,
Karakoyun S, Artaç İ, İliş D, Yesin M, Öterkus M, Gokdeniz T, Burak
C and Tanboğa IH: Comparison of SYNTAX score II efficacy with
SYNTAX score and TIMI risk score for predicting in-hospital and
long-term mortality in patients with ST segment elevation
myocardial infarction. Int J Cardiovasc Imaging. 34:1165–1175.
2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Jakimov T, Mrdovic I, Filipovic B,
Zdravković M, Djoković A, Hinić S, Milić N and Filipović B:
Comparison of RISK-PCI, GRACE, TIMI risk scores for prediction of
major adverse cardiac events in patients with acute coronary
syndrome. Croat Med J. 58:406–415. 2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Morrow DA, Antman EM, Giugliano RP, Cairns
R, Charlesworth A, Murphy SA, de Lemos JA, McCabe CH and Braunwald
E: A simple risk index for rapid initial triage of patients with
ST-elevation myocardial infarction: An InTIME II substudy. Lancet.
358:1571–1575. 2001.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Truong QA, Cannon CP, Zakai NA, Rogers IS,
Giugliano RP, Wiviott SD, McCabe CH, Morrow DA and Braunwald E:
Thrombolysis in myocardial Infarction (TIMI) risk index predicts
long-term mortality and heart failure in patients with ST-elevation
myocardial infarction in the TIMI 2 clinical trial. Am Heart J.
157:673–679.e1. 2009.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Chen Y, Song Y, Xu JJ, Tang XF, Wang HH,
Jiang P, Jiang L, Liu R, Zhao XY, Gao LJ, et al: Relationship
between thrombolysis in myocardial infarction risk index and the
severity of coronary artery lesions and long-term outcome in acute
myocardial infarction patients undergoing percutaneous coronary
intervention. Zhonghua Xin Xue Guan Bing Za Zhi. 46:874–881.
2018.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
17
|
Brkovic V, Dobric M, Beleslin B, Giga V,
Vukcevic V, Stojkovic S, Stankovic G, Nedeljkovic MA, Orlic D,
Tomasevic M, et al: Additive prognostic value of the SYNTAX score
over GRACE, TIMI, ZWOLLE, CADILLAC and PAMI risk scores in patients
with acute ST-segment elevation myocardial infarction treated by
primary percutaneous coronary intervention. Int J Cardiovasc
Imaging. 29:1215–1228. 2013.PubMed/NCBI View Article : Google Scholar
|