1. Introduction
The skin is the largest organ of the human body and
it is the site from which various types of tumors may arise, from
benign ones, such as seborrheic keratosis, nevi and spiradenomas
(some of which are considered even precursor lesions for their
malignant counterparts) to malignant masses, such as basal cell
carcinomas (BCCs) or squamous cell carcinomas (SCCs), melanomas or
spiradenocarcinomas.
BCCs are one of the most common malignant tumors
worldwide with skin involvement, being part of non-melanoma skin
cancers, alongside SCCs, with which it can coexist in the same
lesion, evolving at the site of a burn scar, or even from a benign
tumor-like lesion, such as a verruca vulgaris (1-4).
According to the World Health Organization (WHO), BCCs represent
malignant tumors which have originated from basal cells found in
the inter-follicular epidermis or in the hair follicle. BCC cases
further increase the burden to global cancer cases which are
constantly on the rise; it is estimated that 1 in 5 males and 1 in
6 females will suffer from one form of cancer during their lifetime
(5,6). Although the reporting of BCC cases is
not precise (data are rarely collected), its global incidence is
increasing, affecting approximately one million new patients each
year. It is one of the most common types of skin cancer in certain
populations such as among individuals of Asian, African or Hispanic
origin (7).
BCC has low mortality and extremely low metastatic
rates (although when present, it indicates a poor prognosis).
However, it has a high morbidity rate, exemplified through local
destruction and recurrence, particularly when perineural invasion
(PNI) is present, allowing BCC to spread in a contiguous manner
with secondary neuropathy. Extremely rare cases from the literature
(11 in total) have reported BCC with intravascular invasion, having
higher metastatic rates than BCC cases without this aggressive
trait (8-11).
2. Pathogenesis and risk factors
BCC pathogenesis is the direct result of
interactions between environmental factors and patient
characteristics, as well as genetic factors. As regards genetics,
the aberrant activation of the Hedgehog signaling pathway has been
shown to be pathognomonic for BCC development and it can interact
with other oncogenic pathways, such as EGFR, TGF-β, PI3K, NF-κB and
atypical protein kinase C (aPKC) (9,12).
The risk factors incriminated in BCC development are
classified as follows: Modifiable risk factors, such as ultraviolet
(UV) radiation and behavioral factors associated with an increased
exposure to this type of radiation (multiple sunburns at an early
age and occupational sun exposure), being the most incriminating
one; and non-modifiable risk factors, such as the elderly/aging
population (with cumulative sun exposure), a positive family
history of BCC and genetic factors, such as mutations of the
patched tumor suppressor genes 1 and 2 (PTCH1 and PTCH2), which can
be inherited as an autosomal dominant trait or can appear de
novo, in the basal cell nevus syndrome/nevoid BCC
syndrome/Gorlin-Goltz syndrome; other genetic syndromes associated
with BCC development, such as xeroderma pigmentosum and
Bazex-Dupré-Christol syndrome. The non-modifiable factors which are
mainly incriminated in BCC development in the Caucasian population
are the following: A fair skin (Fitzpatrick skin types I and II), a
light eye color, blonde/red hair, freckles, photosensitizing
medication (tetracyclins, hydrochlorothiazide and statins) and
exposure to carcinogenic substances (such as arsenic). Along with
other skin pathologies (Kaposi's sarcoma, herpes zoster, oral
candidiasis or hairy leucoplakia), BCC has been observed to develop
with a 2- and 5-fold increased frequency in patients who are human
immunodeficiency virus (HIV)-positive and, respectively, in those
who have received organ transplants (7,9,13-18).
As the main factor responsible for the development
of BCC, UV radiation exposure has been found to be responsible for
the release of interleukin (IL)-6 and tumor necrosis factor-α
(TNF-α) from keratinocytes. In some benign and malignant tumors or
in certain conditions, IL-6 is known to function as a growth factor
[acquired immunodeficiency syndrome (AIDS), Kaposi's sarcoma,
multiple myeloma, renal cell carcinoma, some T-cell or B-cell
lymphomas], while also preventing apoptosis and inducing the
expression of the anti-apoptotic protein, Bcl-xL. At the same time,
IL-6 stimulates vascular endothelial growth factor (VEGF)
expression in various cells, functioning as a pro-angiogenic factor
by enhancing angiogenesis. Thus, IL-6 is incriminated in the
pathogenesis of BCC (19,20). Neuroactive factors seem to also play
a role not only in BCC, but also in SCC development; the
interactions between the peripheral nervous system and skin cells
are mediated by several locally secreted, possibly stress-induced
neuroendocrine factors, such as substance P, catecholamines,
somatostatin, calcitonin gene-related peptide or neurohormones
(proopiomelanocortin, adrenocorticotropin and
α-melanocyte-stimulating hormone). These substances which are
dysregulated by chronic stress have been found to be involved in
the development and progression of BCC and SCC, by their
involvement in immune system suppression and by ensuring a
favorable tumor microenvironment (21).
BCC arising in uncommon locations, such as the oral
cavity or the vulva is not associated with UV radiation exposure as
a primary risk factor, as these are sun-protected areas. In such
rare primary site cases, other risk factors are involved, such as
chronic inflammation, immune suppression, Paget's disease of the
vulva or lichen sclerosus, addressing the genital location; as
regards the oral cavity, risk factors for BCC development remain
unknown (22-24).
Although vitiligo may be a predisposing factor for sunburn, and it
may potentiate the effects of UV radiation and subsequent
consequences, the available data reveal the contrary, a protective
effect; the association between vitiligo and BCC is rare, as it is
also in the case of melanoma (25-28).
3. Clinical aspects
BCC may have a wide array of clinical presentations;
its medico-social importance resides in its prevalence, its
detrimental effects on health and associated complications, as well
as in its psychological burden, as with other pathologies (such as
diabetes or other tumors). Oftentimes, patients suffering from BCC
may present with a lesion which has enlarged with time, is
non-healing and which may bleed or ulcerate; these aspects may also
be accompanied by pruritus. The classical clinical description of
such a tumor is that of a shiny, pearly, smooth papule/nodule with
conspicuous, dilated and arborizing blood vessels, often with
erosions or ulcerations and rolled margins. The clinical aspects
vary with the histological type of the tumor (discussed below);
thus, the classical clinical description may correspond to the
nodular type of BCC, while the discovery of a circumscribed,
annular, thin patch or plaque with/without scales, central clearing
and rolled borders can be observed in superficial BCC; scar-like
lesions or poorly defined, infiltrative, shiny plaques (which can
be flat or depressed) can indicate the presence of an infiltrative
or morphoeic/sclerosing BCC, and the pigmented variant of BCC can
be clinically confused with melanoma or Spitz-Reed nevus. The
fibroepithelial variant of BCC is frequently mistaken for an
acrochordon or a seborrheic keratosis, presenting as sessile plaque
or pedunculated papule or nodule, which can be flesh-colored or
erythematous. Infundibulocystic BCCs present as pearly papules that
are well circumscribed, being frequently mistaken for benign
follicular processes (1,5,29-31).
4. Histopathology
The histopathology of BCC is largely characterized
by aggregates of basal cells with a small cytoplasm and large,
hyperchromatic nuclei, apoptotic cells, all included in a
fibromyxoid stroma, with tumor retraction spaces. Angiogenesis is
an indicator of tumor development and its progression; the stroma
surrounding BCC also reveals increased numbers of microvessels,
being associated with local aggressive behavior (1,5,32).
The BCC histopathologic subtypes are classified
according to the risk of tumor recurrence; BCCs with a low risk of
recurrence are nodular, superficial, pigmented and
infundibulocystic (BCC with adnexal differentiation) and
fibroepithelial. However, those with a high risk of are recurrence
are micronodular, infiltrating, sclerosing/morphoeic and
basosquamous BCCs, and BCCs with sarcomatoid differentiation.
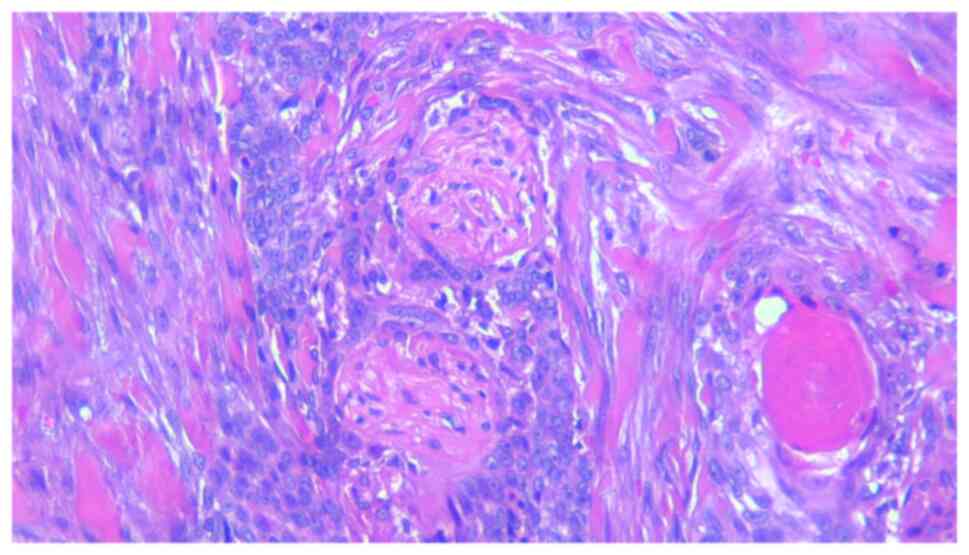
Nodular BCC presents microscopically as large nests
or islands of malignant basaloid cells with central, haphazard cell
arrangement and peripheral palisading, tumor-stroma clefting,
mucoid/myxoid stroma with spindle cells, with/without amyloid
deposits; sometimes the tumor stroma has a collagenous,
keloidal-type aspect. The malignant tumor nests extend deep into
the dermis and apoptotic cells can be found centrally. Nodular BCC
has several subtypes, according to the secondary findings that
characterize such tumors, keratotic (with mature keratin deposits
found central in the tumor islands, Fig. 1), cystic/nodulocystic (cystic
degeneration) and adenoid (with cribriform arrangement of tumor
nests) (1,5,33).
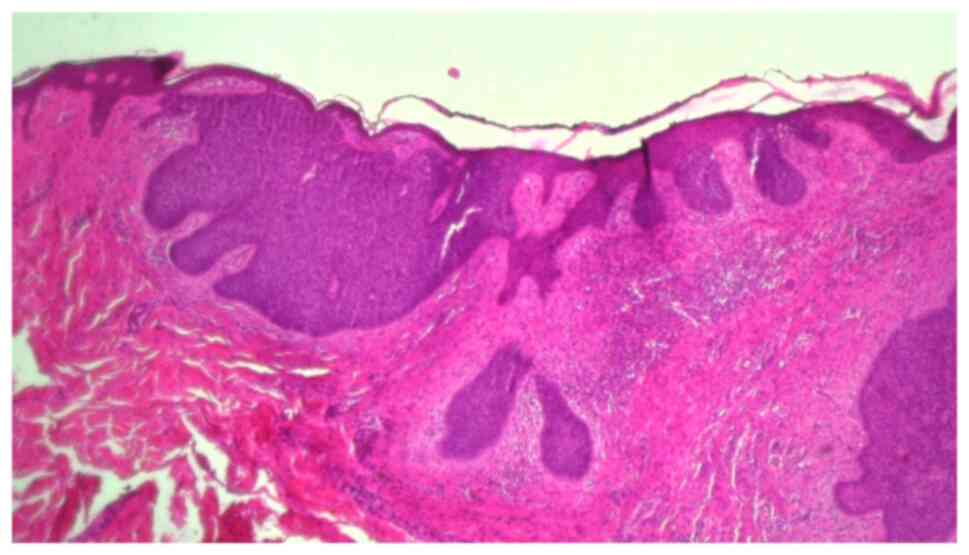
Superficial BCC (Fig.
2) develops as small islands or lobules of malignant basaloid
cells with peripheral palisading, localized in the superficial
dermis, with a connection to the epidermis and within a myxoid
stroma, associated with a lichenoid, band-like, inflammatory
infiltrate. It can appear as a multicentric tumor and may sometimes
be part of a mixed-pattern tumor, with micronodular, nodular, or
infiltrating components (1,5,34).
Micronodular BCC is characterized by small islands
or nests of malignant tumor cells which infiltrate deep into the
dermis, sometimes even into the subcutaneous tissue; the tumor has
a satellite-like arrangement of discrete nodules with irregular
contours, lined by a thin margin of stroma and separated by normal
dermal collagen (1,5,35).
Infiltrating BCC is a subtype composed mainly of
chords or thin nests of tumor cells (with a thickness of >5-8
cells) which infiltrate deeply, with angulated edges and have an
irregular, permeating invasion pattern at the tumor edge. It
frequently overlaps with morphoeic/sclerosing BCC and can be found
with a nodular component (1,5,35).
Sclerosing/morphoeic BCC is comprised of very thin
strands/chords of tumor cells (with a thickness of 1-5 cells, and
also with angulated ends) found in a collagenous type of stroma,
with seldom tumor-stroma clefting. It infiltrates deeply and
differs from the infiltrating subtype of BCC by the stromal
characteristics, the latter lacking the highly collagenous stroma
(1,5,34).
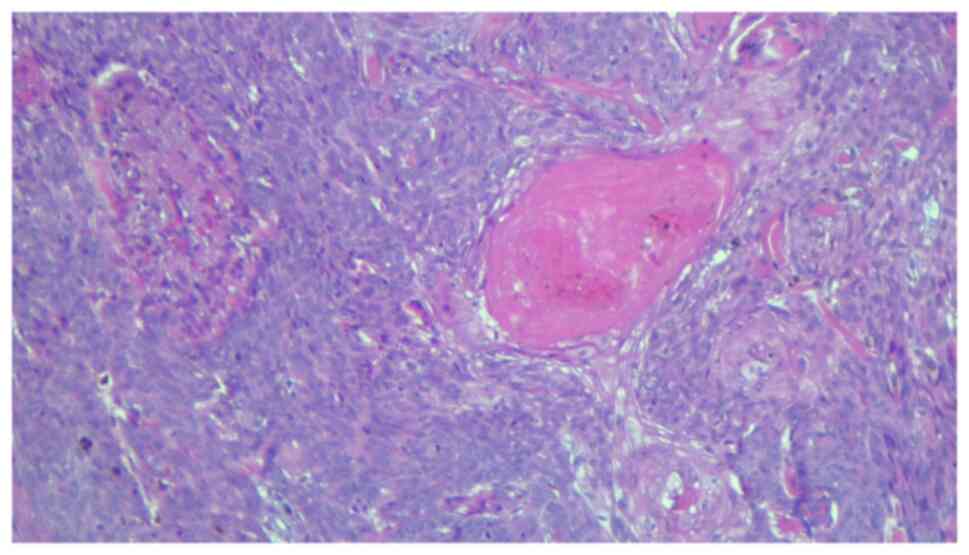
Basosquamous carcinoma (metatypical BCC, Fig. 3) is a subtype characterized by the
presence of both BCC and SCC tumor features, with transition areas
between the two. The tumor nests are comprised of basaloid cells,
which are intermingled with atypical squamous cells with
eosinophilic cytoplasm which are dispersed or have a focal
distribution; the stroma is oftentimes highly cellular, with a
fibrotic appearance (1,5,36).
Pigmented BCC is a variant of nodular or superficial
BCC, which contains melanin pigment derived from an increased
number of dendritic melanocytes within the malignant tumor nests,
being found within the malignant basaloid cells or the macrophages
which surround the malignant proliferation (1,5,37).
BCC with sarcomatoid differentiation (metaplastic
carcinoma) is characterized by a malignant proliferation of
basaloid cells found within a sarcomatous stroma with variable
histology. The malignant mesenchymal stromal component can take the
form of an osteosarcoma, chondrosarcoma, leiomyosarcoma,
pleomorphic undifferentiated sarcoma, or rhabdomyosarcoma (1,5).
BCC with adnexal differentiation defines a subtype
of BCC which is frequently found in the skin around the eyes,
exhibiting differentiation towards follicular, eccrine, apocrine or
sebaceous glands. Matrical differentiation in BCC is revealed by
the presence of shadow cells; the infundibulocystic variant is
characterized by the presence of small infundibular cyst-like
spaces inside the tumor nodules; mature sebocytes can be found in
BCC with sebaceous differentiation, while ductal structures, such
as those found in eccrine and apocrine glands (and decapitation
secretion in apocrine differentiation) are found in BCC with
differentiation towards eccrine or apocrine sweat glands (1,5,38).
Fibroepithelial BCC (fibroepithelioma of Pinkus or
Pinkus tumor) is a distinct variant composed of thin strands of
anastomosing basaloid cells with reticular pattern of development,
linked to the epidermis and within a fibroblastic stroma. Sometimes
rare basaloid islands can be found (1,5,39).
5. Dermoscopy
Dermoscopy is a non-invasive skin examination
procedure which allows the clinician to observe certain lesional
characteristics which are not visible to the naked eye. The BCC
examination and its positive diagnosis rely on three main features:
Vascular structures (arborizing vessels and pigmented structures),
nests with a blue-gray coloration and ovoid shape and the presence
of ulcerations; these three features, along with features of
melanocytic lesions (network areas) indicate the positive clinical
diagnosis of BCC. This in vivo technique has a sensitivity
of 89-91.2% and a specificity of 95% (34,40-42).
The dermoscopic features indicative of BCC are the
following: Arborizing vessels (the most prevalent feature), a
dotted or corkscrew appearance, or glomerular vascularization,
short and fine telangiectasia; shiny and white structures which
alternate with shiny white and red areas without a certain
structure; nests with blue-gray coloration and ovoid shape,
multiple blue and gray globules/dots (Table I). These features vary in prevalence
and distribution among BCC subtypes, with certain other
characteristics being found in those subtypes, such as concentric,
spoke wheel structures or leaf-like areas in nodular BCC, while
morpheaform BCC rarely presents with pigmentation.
 | Table IDermoscopic features of basal cell
carcinoma. |
Table I
Dermoscopic features of basal cell
carcinoma.
| Vascular
structures | Pigmented
structures | Other features |
|---|
| Arborizing
vessels | Ovoid nests with
blue-gray coloration | Ulceration |
| Short and fine
telangiectasia | Shiny, white
structures alternating with shiny white-red areas (no
structure) |
Erosion/erosions |
| Dotted
vascularization | Multiple blue and
gray globules/dots | |
| ‘Corkscrew’
vascularization | | |
| Glomerular
vascularization | | |
| Concentric, spoke
wheel structures | | |
| Leaf-like
areas | | |
The overall dermoscopic aspect of BCC is represented
by the mixture of the abovementioned features, with variation
according to the patient's age, sex, race, BCC subtype, tumor
location or the presence or absence of pigmentation (40-42).
6. Novel diagnostic approaches
In recent years, novel technologies have been
developed for the diagnosis of BCC; some of these technologies are
non-invasive, such as optical coherence tomography (OCT) and
reflectance confocal microscopy (RCM), which are both in
vivo diagnostic tools.
RCM uses a near-infrared laser in order to obtain
images of thin sections of the skin; the light is reflected back
from the selected focal point and enters the detector through a
special pinhole. It is a highly sensitive (sensitivity varying
between 100 and 91.7%) and specific (specificity varying between
91.3 and 88.5%) technique. This technique has the capacity for high
resolution imaging, which is equivalent to 30-fold the
magnification of an optical microscope; however, it can only
penetrate to depths of 250 µm and does not have the capacity to
evaluate tumor depth margins and invasion (12,43-48).
RCM criteria indicative of a BCC diagnosis can be
found in the superficial dermis (or at the dermo-epidermal
junction) and these include dark silhouettes (hyporeflective zones
surrounded by bright collagen bundles, bright tumor islands which
are often limited by a dark cleft, dendritic cells, plump, bright
cells and canalicular vessels). As regards superficial BCC,
features which are indicative of its diagnosis are epithelial
chords connected to the epidermis; nodular BCC has an additional
increased vascular density, while aggressive BCC subtypes are
evidenced by hyporeflective areas (12,43-49).
OCT uses infrared light in order to obtain a
real-time image of the examined skin; the technique is based on the
sum of light refractions of different skin components, with various
optical properties; it is capable of examining the skin at depths
of 500 µm (although at a depth >400 µm the image increases in
noise and decreases in resolution). Its sensitivity is 87% and its
specificity is 80%. This technique has the capacity for deeper
examination and is capable of en face and cross-sectional imaging;
however, it has limited use for pigmented lesions (12,43-48,50).
When identifying BCC with the help of OCT, the
following images have been found to be positively associated with
the diagnosis: Oval structures (with/without bright colored
centers), dark areas bordering the dermis (hyporeflective area as
the lateral tumor border), black zones or cones protruding into the
adjacent dermis and disruption of the epidermal layering. For the
nodular subtype of BCC, the most characteristic image is that of
oval structures, with the presence of dark or black zones or cysts.
For the superficial subtype, the presence of a dark area bordering
the dermis and the bulges or cones extending from the epidermis to
the dermis are the most characteristic and positively associated
images. The image compared to ‘a shoal of fish’ which translates as
elongated and narrow structures found in the dermis, is indicative
of the infiltrative subtype of BCC (12,43-48,50,51).
Both techniques can be combined for a more accurate
diagnosis (resulting in line-field confocal OCT, combining the
advantages of OCT, with vertical in-depth penetration and RCM with
its high resolution) and can be accompanied by the classic
dermoscopic examination, thus improving the accuracy of diagnosis
(12,43-48).
Other techniques that can be used in the diagnosis
of BCC are high-resolution ultrasonography, Raman spectroscopy or
terahertz pulse imaging.
High resolution ultrasonography is a diagnostic tool
using frequencies between 20-100 MHz, and it can measure the extent
of the tumor, including its depth or thickness, while evaluating
deep structure involvement. As regards the subtypes of BCC, the
nodular one is described as dermal or hypodermal hypo-echoic
nodules with various shapes (oval, irregular or ribbon-like
shapes), with variably defined margins (well or ill-defined), some
with or without an internal echo (which can be homogenous or
non-homogenous) or with hyper-echoic spots. The superficial subtype
has a less variable appearance, presenting as a hypo-echoic
ribbon-like area, which is homogenous in appearance, without any
internal echoes, posterior acoustic artifacts or hyper-echoic
spots. The micronodular subtype of BCC is characterized by the
presence of ill-defined, hypo-echoic tumor nodules located in the
dermis, having internal echoes, some with hyper-echoic spots, with
small, anechoic areas (cystic) or with posterior acoustic artifact.
Infiltrative BCC has similar characteristics, also having
ill-defined, hypo-echoic tumor nodules, but which were located both
in the dermis and hypodermis, with a number of internal
hyper-echoic spots and without a posterior reinforcement artifact.
Basosquamous BCC is described as having dermal and hypodermal
ill-defined, hypo-echoic nodules with multiple internal,
hyper-echoic spots, some internal anechoic zones and without
posterior acoustic artifact. When using this diagnostic tool,
careful attention should be paid as tumor thickness is frequently
overestimated, and the inflammatory infiltrate which is found at
the base of the tumor nodules or islands may be confused as part of
the tumor. However, this technique yields promising results in the
pre-operative diagnosis of BCC, revealing important tumor traits,
such as tumor depth, associated lesions or margins (52,53).
Raman spectroscopy is an optical technique which
analyzes the vibrational molecule modes, and, apart from the other
techniques used for BCC diagnosis, it offers a special focus on
tumor vascularization.
Terahertz pulse imaging is a portable ex vivo
or in vivo diagnostic tool which uses terahertz radiation,
an electromagnetic spectrum found between the infrared and
microwave regions, having the ability to evaluate the low-frequency
type, vibrational and torsional motions in molecular systems and
registering its absorption. Studies have registered spectroscopic
differences between the normal tissue and that which is affected by
a tumor process, meaning that that the absorption coefficient and
refractive index are higher in areas affected by BCC, which are
consistent with a higher water content, providing information
regarding the extent of the tumor (54-56).
In vivo confocal laser scanning microscopy
(CLSM) is also an innovative technique which is currently used in
studying the morphological course of a disease by repeated, high
magnification examination, revealing its dynamic treatment
response. It is currently used in the study of inflammatory skin
diseases; however, it is a promising diagnostic and monitoring tool
for skin tumors, allowing the close inspection of the body's immune
response to the tumor and the response to the applied treatment.
However, further studies are required in order to evaluate BCC from
this perspective (57).
7. Treatment
The surgical treatment of BCC is the main approach
through which the entire tumor mass can be excised, and the
cosmetic and functional aspects can be preserved, providing optimal
results for the patient. The surgical excision needs to be made
with at least 4-mm margins in low-risk BCC, whereas for high-risk
ones, margins of at least 6 mm should be ensured.
Mohs micrographic surgery involves the complete
excision of the BCC with a microscopic examination of the surgical
margins. It is most frequently used in high-risk tumors, with
higher rates for long-term cure. This approach has a high success
rate, with dermatopathologists and Mohs surgeons agreeing on
surgical excision margin clearance (12,58).
Curettage or electrodessication are older
techniques, recommended in superficial BCC or low-risk tumors,
having the downside of not allowing a histopathological examination
of surgical margins. It is recommended that these two techniques
should not be used in parts of the body with terminal hair growth,
such as the scalp, beard area, axillae, or pubis, due to the risk
of tumor extension in the hair follicle (12,59).
Cryosurgery uses freeze-thaw cycles in order to
destroy the malignant tumor cells, and, as with curettage and
electrodessication, does not allow the microscopic examination of
tumor margins and is mostly recommended in low-risk cases, such as
superficial BCC (12).
Photodynamic therapy is a two-step therapeutic
approach; it involves the initial local application of a
photosensitizing chemical substance (methyl aminolevulinate or
aminolevulinic acid), followed by irradiation with the help of a
light source. It determines oxidative damage in the tumor mass with
the apoptosis and necrosis of tumor cells, along with vascular
damage, and without having major effects on the surrounding normal
tissue; it may be recommended in cases of periocular BCC, having a
good function preservation and cosmetic outcome. However, this
technique has high recurrence rates of up to 30.7% within 5 years,
and is mainly recommended for superficial BCC (12,60).
Radiotherapy is a less frequent treatment approach,
being used for unresectable tumors or in cases where surgery is not
recommended; brachytherapy and external beam
radiotherapy/teletherapy have been used in the treatment of BCC,
having lower recurrence rates as compared with cryosurgery
(12).
Topical treatments, such as 5-fluorouracil or
imiquimod 5% applications, are recommended in superficial BCC
subtypes and have registered histologic clearances ranging from
76-100%, in 6 to 12 weeks of treatment. The study by Williams et
al (61) reported the higher
effectiveness of surgical treatment over imiquimod 5% topical
applications, with recurrences being observed as early as 1 year
post-treatment concerning the local treatment. The 5-year success
rates were higher for the cases where surgical treatment was
applied (97.7%), as compared with those treated with imiquimod 5%
(82.5%). However, this type of treatment may be associated with
side-effects, such as erythema, erosions or swelling, affecting
patient compliance and treatment effectiveness (12,61).
Intralesional chemotherapy with 5-fluorouracil,
bleomycin, IL-2 or interferons have registered variable results and
can have local side-effects or even general ones, such as flu-like
manifestations.
Laser therapy, such as superpulsed carbon dioxide
laser therapy or pulsed neodymium-based laser therapy, can be used
alone or in combination with other therapeutic approaches. It has
proven to have small recurrence rates of up to 1.8% in 5 years,
although it presents with local adverse effects, such as soreness,
edema, hyperemia and scarring.
Hedgehog pathway inhibitors, such as Vismodegib, are
used in surgically advanced tumors as neoadjuvant therapy, prior to
Mohs micrographic surgery or radiotherapy, allowing the tumor to
decrease in size. As is the case with other treatment agents, its
long-term use is associated with adverse effects and in order to
combat such effects, treatment interruptions of up to 8 weeks have
been practiced (12,62,63).
8. Conclusions
The diagnosis and characterization of BCC needs to
be based on the clinical, imaging and histopathology features of
the tumor mass, combined with the patient's characteristics, in
order to select the most effective treatment option and yield
optimal results with the highest disease-free intervals and lowest
recurrence rates. BCC treatment aims for a complete resolution,
with minimal side-effects and high patient satisfaction, aiming for
optimal cosmetic results, particularly in key areas such as the
face.
Acknowledgements
The authors wish to acknowledge that the present
study was supported by the 'Dunarea de Jos' University of Galati,
Romania, through the research center - Multidisciplinary Integrated
Center of Dermatological Interface Research MIC-DIR (Centrul
Integrat Multidisciplinar de Cercetare de Interfata Dermatologica -
CIM-CID).
Funding
Funding: The present study was supported by the 'Dunarea de Jos'
University of Galati through an internal grant (grant no.
RF3668/01.10.2021).
Availability of data and materials
Not applicable.
Authors' contributions
EN, MC, CB, FN, DJS, ML and ALT were major
contributors to the writing of the manuscript and the literature
search. EN, MC, CB and FN were involved in all the stages of the
study (conception, design, revision, data collection, critical
analysis and language editing). DJS, ML and ALT contributed to the
conception and design of the study, as well as in the study
revision. EN, ALT, DJS and FN assisted in the collection of the
data for the review article. LR, GL, VC and LA revised the study
for important intellectual content. All authors have read and
approved the final version of the manuscript to be published. EN
and DJS confirm the authenticity of all the raw data. All authors
agree to be accountable for all aspects of the work in ensuring
that questions related to the accuracy or integrity of any part of
the work. All authors have had equal participation, contribution
and equal rights to this article.
Ethics approval and consent to
participate
The present study was approved by the ‘Sf. Apostol
Andrei’ Emergency Clinical Hospital Ethics Committee (decision no.
19758). The patients provided written informed consent for the
publication of any associated data and accompanying image.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Cameron MC, Lee E, Hibler BP, Barker CA,
Mori S, Cordova M, Nehal KS and Rossi AM: Basal cell carcinoma:
Epidemiology; pathophysiology; clinical and histological subtypes;
and disease associations. J Am Acad Dermatol. 80:303–317.
2019.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Matsui Y, Makino T, Takemoto K, Kagoyama K
and Shimizu T: Co-existence of basal cell carcinoma and squamous
cell carcinoma in a single burn scar region. Burns Open. 4:64–66.
2020.
|
|
3
|
Lai K, Chan E and Ko SC: Combination of
squamous cell carcinoma and basal cell carcinoma arising from a
giant verruca vulgaris involving the eyelid. Am J Ophthalmol Case
Rep. 21(100858)2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Rebegea LF, Firescu D, Dumitru M and
Patrascu A: Skin spiradenocarcinoma-case presentation. Rom J
Morphol Embryol. 57:327–330. 2016.PubMed/NCBI
|
|
5
|
Messina J, Epstein EH Jr, Kossard S,
McKenzie C, Patel RM, Patterson JW and Scolyer RA: Chapter
1-Keratinocytic/epidermal tumors. Basal cell carcinoma. In: WHO
Classification of skin tumors. Elder DE, Massi D, Scolyer RA and
Willemze R (eds). 4th edition. International Agency for Research on
Cancer, Lyon, pp26-24, 2017.
|
|
6
|
Rebegea L, Firescu D, Baciu G and Ciubara
A: Psycho-oncology support. Brain. 10:77–88. 2019.
|
|
7
|
Hogue L and Harvey VM: Basal cell
carcinoma, squamous cell carcinoma, and cutaneous melanoma in skin
of color patients. Dermatol Clin. 37:519–526. 2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Poignet B, Gardrat S, Dendale R, Lemaitre
S, Lumbroso-Le Rouic L, Desjardins L, Cassoux N and Levy Gabriel C:
Basal cell carcinomas of the eyelid: Results of an initial surgical
management. J Fr Ophtalmol. 42:1094–1099. 2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Kim DP, Kus KJB and Ruiz E: Basal cell
carcinoma review. Hematol Oncol Clin North Am. 33:13–24.
2019.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Ashraf DC, Kalin-Hajdu E, Levin MH and
Kersten RC: Mixed cranial neuropathies due to occult perineural
invasion of basal cell carcinoma. Am J Ophthalmol Case Rep.
13:136–139. 2018.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Muzumdar S, Stewart CL and Feng H: Rare
case of a basal cell carcinoma with intravascular invasion. Int J
Womens Dermatol. 6:334–335. 2020.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Fania L, Didona D, Morese R, Campana I,
Coco V, Di Pietro FR, Ricci F, Pallotta S, Candi E, Abeni D and
Dellambra E: Basal cell carcinoma: From pathophysiology to novel
therapeutic approaches. Biomedicines. 8(449)2020.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Nicoara M, Bain K, Patel R, Jaikaran O,
Hingorani A and Asher E: Malignant transformation of nonhealing
ulcer-basal cell carcinoma. Ann Vasc Surg. 70:565.e7–565.e10.
2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Coulombe C, Gagnon LP, Larouche V and
Dionne MC: Infantile-onset palmo-plantar basal cell carcinomas and
pits in Gorlin syndrome. JAAD Case Rep. 4:662–664. 2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Nwabudike LC and Tatu AL: Response
to-Chronic exposure to tetracyclines and subsequent diagnosis for
non-melanoma skin cancer in a large Mid-Western US population. J
Eur Acad Dermatol Venereol. 32(e159)2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Tatu AL, Ciobotaru OR, Miulescu M, Buzia
OD, Elisei AM, Mardare N, Diaconu C, Robu S and Nwabudike LC:
Hydrochlorothiazide: Chemical structure, therapeutic, phototoxic
and carcinogenetic effects in dermatology. Rev Chim (Bucharest).
69:2110–2114. 2018.
|
|
17
|
Nwabudike LC, Elisei AM, Buzia OD,
Miulescu M and Tatu AL: Statins. A review on structural
perspectives, adverse reactions and relations with non-melanoma
skin cancer Rev Chim. (Bucharest). 69:2557–2562. 2018.
|
|
18
|
Draganescu M, Baroiu L, Iancu A, Dumitru
C, Radaschin D, Polea ED, Bobeica C, Tatu AL, Niculet E and Fekete
GL: Perspectives on skin disorder diagnosis among people living
with HIV in southeastern Romania. Exp Ther Med.
21(97)2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Niculet E, Chioncel V, Elisei AM, Miulescu
M, Buzia OD, Nwabudike LC, Craescu M, Draganescu M, Bujoreanu F,
Marinescu E, et al: Multifactorial expression of IL-6 with update
on COVID-19 and the therapeutic strategies of its blockade
(Review). Exp Ther Med. 21(263)2021.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Jee SH, Shen SC, Chiu HC, Tsai WL and Kuo
ML: Overexpression of interleukin-6 in human basal cell carcinoma
cell lines increases anti-apoptotic activity and tumorigenic
potency. Oncogene. 20:198–208. 2001.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Lupu M, Caruntu A, Caruntu C, Papagheorghe
LML, Ilie MA, Voiculescu V, Boda D, Constantin C, Tanase C, Sifaki
M, et al: Neuroendocrine factors: The missing link in non melanoma
skin cancer (Review). Oncol Rep. 38:1327–1340. 2017.PubMed/NCBI View Article : Google Scholar
|
|
22
|
McEnery-Stonelake ME, Clark MA and Vidimos
AT: Vulvar basal cell carcinoma arising in the setting of repeated
perilamp exposure. JAAD Case Rep. 6:103–105. 2020.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Varadarajan VV, Nasri E and Dziegielewski
PT: Basal cell carcinoma of the oral cavity: A case report.
Otolaryngol Case Rep. 15(100159)2020.
|
|
24
|
Tatu AL and Nwabudike LC: The treatment
options of male genital lichen sclerosus et atrophicus short title
for a running head: Treatments of genital lichen sclerosus. In:
Proceedings of the 14th National Congress of Urogynecology and the
National Conference of the Romanian Association for the Study of
Pain, pp262-264, 2017.
|
|
25
|
Rustemeyer J, Günther L and Deichert L: A
rare association: Basal cell carcinoma in a vitiliginous macula.
Oral Maxillofac Surg. 15:175–177. 2011.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Mihăilă B, Dinică RM, Tatu AL and Buzia
OD: New insights in vitiligo treatments using bioactive compounds
from Piper nigrum. Exp Ther Med. 17:1039–1044. 2019.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Fiszon-Cerqueira L, Ramos-E-Silva M,
Guerreiro FB, Cistaro-Serrano M, Carneiro AHC and Gomes MK: Giant
basal cell carcinoma associated with vitiligo. Clin Case Rep.
7:1782–1786. 2019.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Byrne KT and Turk MJ: New perspectives on
the role of vitiligo in immune responses to melanoma. Oncotarget.
2:684–694. 2011.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Nwabudike LC, Tebeica T and Tatu AL:
Nodular, ulcerated seborrheic keratosis. Clin Exp Dermatol.
45:602–604. 2020.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Tatu AL: Umbilicated blue black lesion on
the lateral thorax. J Cutan Med Surg. 21(252)2017.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Earar K, Sirbu I, Onisor C and Luca E:
Oral rehabilitation on implants and introduction of pathogenic
mechanisms in relation to oral implants-sugar diabetes. Rev Chim
(Bucharest). 70:3750–3752. 2019.
|
|
32
|
Lupu M, Caruntu C, Popa MI, Voiculescu VM,
Zurac S and Boda D: Vascular patterns in basal cell carcinoma:
Dermoscopic, confocal and histopathological perspectives. Oncol
Lett. 17:4112–4125. 2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Căruntu C, Boda D, Guţu DE and Căruntu A:
In vivo reflectance confocal microscopy of basal cell carcinoma
with cystic degeneration. Rom J Morphol Embryol. 55:1437–1441.
2014.PubMed/NCBI
|
|
34
|
Mackiewicz-Wysocka M, Bowszyc-Dmochowska
M, Strzelecka-Węklar D, Dańczak-Pazdrowska A and Adamski Z: Basal
cell carcinoma-diagnosis. Contemp Oncol (Pozn). 17:337–342.
2013.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Dourmishev LA, Rusinova D and Botev I:
Clinical variants, stages, and management of basal cell carcinoma.
Indian Dermatol Online J. 4:12–17. 2013.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Lima NL, Verli FD, de Miranda JL and
Marinho SA: Basosquamous carcinoma: Histopathological features.
Indian J Dermatol. 57:382–383. 2012.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Abudu B and Cohen PR: Pigmented basal cell
carcinoma masquerading as a melanoma. Cureus.
11(e4369)2019.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Shash HA, Almarzouq SF, Alghamdi AA and
Alratroot JA: Basal cell carcinoma with sebaceous differentiation:
A case report and review of literature. Plast Reconstr Surg Glob
Open. 8(e3234)2020.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Haddock ES and Cohen PR: Fibroepithelioma
of pinkus revisited. Dermatol Ther (Heidelb). 6:347–362.
2016.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Reiter O, Mimouni I, Gdalevich M, Marghoob
AA, Levi A, Hodak E and Leshem YA: The diagnostic accuracy of
dermoscopy for basal cell carcinoma: A systematic review and
meta-analysis. J Am Acad Dermatol. 80:1380–1388. 2019.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Reiter O, Mimouni I, Dusza S, Halpern AC,
Leshem YA and Marghoob AA: Dermoscopic features of basal cell
carcinoma and its subtypes: A systematic review. J Am Acad
Dermatol. 85:653–664. 2019.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Álvarez-Salafranca M, Ara M and Zaballos
P: Dermoscopy in basal cell carcinoma: An updated review. Actas
Dermosifiliogr. 112:330–338. 2021.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Cameron MC, Lee E, Hibler BP, Giordano CN,
Barker CA, Mori S, Cordova M, Nehal KS and Rossi AM: Basal cell
carcinoma: Contemporary approaches to diagnosis, treatment, and
prevention. J Am Acad Dermatol. 80:321–339. 2019.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Suppa M, Fontaine M, Dejonckheere G,
Cinotti E, Yélamos O, Diet G, Tognetti L, Miyamoto M, Orte Cano C,
Perez-Anker J, et al: Line-field confocal optical coherence
tomography of basal cell carcinoma: A descriptive study. J Eur Acad
Dermatol Venereol. 35:1099–1110. 2021.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Holmes J, von Braunmühl T, Berking C,
Sattler E, Ulrich M, Reinhold U, Kurzen H, Dirschka T, Kellner C,
Schuh S and Welzel J: Optical coherence tomography of basal cell
carcinoma: Influence of location, subtype, observer variability and
image quality on diagnostic performance. Br J Dermatol.
178:1102–1110. 2018.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Hussain AA, Themstrup L and Jemec GB:
Optical coherence tomography in the diagnosis of basal cell
carcinoma. Arch Dermatol Res. 307:1–10. 2015.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Lupu M, Popa IM, Voiculescu VM, Boda D,
Caruntu C, Zurac S and Giurcaneanu C: A retrospective study of the
diagnostic accuracy of in vivo reflectance confocal microscopy for
basal cell carcinoma diagnosis and subtyping. J Clin Med.
8(449)2019.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Ghita MA, Caruntu C, Rosca AE, Kaleshi H,
Caruntu A, Moraru L, Docea AO, Zurac S, Boda D, Neagu M, et al:
Reflectance confocal microscopy and dermoscopy for in vivo,
non-invasive skin imaging of superficial basal cell carcinoma.
Oncol Lett. 11:3019–3024. 2016.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Sahu A, Yélamos O, Iftimia N, Cordova M,
Alessi-Fox C, Gill M, Maguluri G, Dusza SW, Navarrete-Dechent C,
González S, et al: Evaluation of a combined reflectance confocal
microscopy-optical coherence tomography device for detection and
depth assessment of basal cell carcinoma. JAMA Dermatol.
154:1175–1183. 2018.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Reddy N and Nguyen BT: The utility of
optical coherence tomography for diagnosis of basal cell carcinoma:
A quantitative review. Br J Dermatol. 180:475–483. 2019.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Navarrete-Dechent C, Rajadhyaksha M and
Nehal KS: Can optical coherence tomography improve the management
of basal cell carcinoma? Br J Dermatol. 180:448–449.
2019.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Wang SQ, Liu J, Zhu QL, Zhao CY, Qu T, Li
F, Wortsman X and Jin HZ: High-frequency ultrasound features of
basal cell carcinoma and its association with histological
recurrence risk. Chin Med J (Engl). 132:2021–2026. 2019.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Bobadilla F, Wortsman X, Muñoz C, Segovia
L, Espinoza M and Jemec GB: Pre-surgical high resolution ultrasound
of facial basal cell carcinoma: Correlation with histology. Cancer
Imaging. 8:163–172. 2008.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Wallace VP, Fitzgerald AJ, Pickwell E, Pye
RJ, Taday PF, Flanagan N and Ha T: Terahertz pulsed spectroscopy of
human Basal cell carcinoma. Appl Spectrosc. 60:1127–1133.
2006.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Woodward RM, Cole B, Wallace VP, Arnone
DD, Pye R, Linfield EH, Pepper M and Davies AG: Terahertz pulse
imaging of in-vitro basal cell carcinoma samples. Technical Digest.
Summaries of papers presented at the Conference on Lasers and
Electro-Optics. Postconference Technical Digest (IEEE Cat. No.
01CH37170), 329-330, 2001.
|
|
56
|
Zhang J, Fan Y, Song Y and Xu J: Accuracy
of Raman spectroscopy for differentiating skin cancer from normal
tissue. Medicine (Baltimore). 97(e12022)2018.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Ilie MA, Caruntu C, Lixandru D, Tampa M,
Georgescu SR, Constantin MM, Constantin C, Neagu M, Zurac SA and
Boda D: In vivo confocal laser scanning microscopy imaging
of skin inflammation: Clinical applications and research directions
(Review). Exp Ther Med. 17:1004–1011. 2019.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Cerci FB, Kubo EM and Werner B: Comparison
of basal cell carcinoma subtypes observed in preoperative biopsy
and Mohs micrographic surgery. An Bras Dermatol. 95:594–601.
2020.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Kopf AW, Bart RS, Schrager D, Lazar M and
Popkin GL: Curettage-electrodesiccation treatment of basal cell
carcinomas. Arch Dermatol. 113:439–443. 1977.PubMed/NCBI
|
|
60
|
Li X, Tan L, Kou H, Zhang J, Wang Y, Li G
and Lu Y: Ocular preservation through limited tumor excision
combined with ALA-PDT in patients with periocular basal cell
carcinoma. Photodiagnosis Photodyn Ther. 27:291–294.
2019.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Williams HC, Bath-Hextall F, Ozolins M,
Armstrong SJ, Colver GB, Perkins W and Miller PSJ: Surgery versus
imiquimod for nodular and superficial basal cell carcinoma (SINS)
study group. surgery versus 5% imiquimod for nodular and
superficial basal cell carcinoma: 5-year results of the SINS
randomized controlled trial. J Invest Dermatol. 137:614–619.
2017.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Sabu DM, Kroes J, Gilham C, Fleming A and
Kelleher FC: Neo-adjuvant Vismodegib followed by radiation in
locally advanced basal cell carcinoma. Curr Probl Cancer: Apr 1,
2021 (Epub ahead of print).
|
|
63
|
Chanu P, Musib L, Wang X, Cheeti S, Girish
S, Bruno R, Lu T, Reddy J, Jin JY and Caro I: Vismodegib efficacy
in advanced basal cell carcinoma maintained with 8-week dose
interruptions: A model-based evaluation. J Invest Dermatol.
141:930–933. 2021.PubMed/NCBI View Article : Google Scholar
|