Introduction
Serous otitis media (SOM) is a common inflammatory
process of the middle ear, frequent in early childhood. It is
commonly accompanied by mild to moderate hearing loss (HL),
alongside a sensation of pressure in the ear that infants cannot
always describe or indicate. The functional deficiencies of the
auditory organ, especially if it is bilateral, can have an
important influence in the development of a small child. SOM is
defined as the presence of fluid (effusion) in the middle ear, with
no signs or symptoms of acute ear infection (1,2). This
is usually due to Eustachian tube dysfunction.
The presence of serous fluid in the middle ear acts
like a barrier in sound conduction, accompanied by a decrease in
the efficiency of transmitting sound to the middle ear (ear drum
and ossicles) (1). If we consider
SOM to be a continuous dynamic process, there are several factors
that influence and transform the character of the effusion such as
time, the body's reaction and repeated infections. There are
different stages of serous otitis, varying from tubotympanic
catarrh, acute serous otitis, chronic serous otitis or progression
to fibro-adhesive otitis (3).
From a functional point of view, the final stage of
these conditions can be hearing impairment. Regarding the impact
and importance of this condition, in the USA, 2.2 million episodes
of common serous otitis are diagnosed annually, with a cost of $4
billion (3).
In fact, indirect costs are much higher, because the
average serous otitis is usually asymptomatic, and many episodes
remain undetected, including children with hearing impairments and
reduced school performance (3).
There are many risk factors associated with SOM
development. Some are related to inflammatory and immune reactions
against rhinopharyngeal infections leading to cytokine production
and the secretion of an exudate rich in protein and inflammatory
mediators, allergy, genetic conditions, pollutants, biofilm
formation and persistence, and gastro-esophageal reflux (4).
Different treatment options are available, including
medical treatment (anti-inflammatory, antihistaminic, mucolytic,
antibiotic), mechanic inflation through the Eustachian tube
(Politzer maneuver), surgery (intratympanic injections and grommet
placement), with various results, being also influenced by the
individual particularity of the pathology and patient (4).
The aim of the study was to investigate the
frequency of SOM by age groups, in relation with different possible
etiopathogenic causes, considering early and correct diagnosis, as
well as obtaining optimal therapeutic results.
Patients and methods
Patient characteristics
The present study was conducted on 285 patients
diagnosed with SOM that were hospitalized in the ENT Department,
Clinical Rehabilitation Hospital and the ENT Department, ‘Sf.
Andrei’ Emergency Hospital Galati (Galati, Romania), over a period
of two years (2016-2017) and followed up for a minimum of three
years after initial management.
Each patient underwent general ENT evaluation that
included audiometry and tympanometry with an Interacoustics AA222
AudioTraveller (SC Sonorom SRL). This study was approved by the
Ethics Committee of ‘Grigore T. Popa’ University of Medicine and
Pharmacy (Iasi, Romania). Written informed consent was obtained
from all patients and/or guardians prior to publication.
Inclusion and exclusion criteria
The design of the study was based on a retrospective
analytical investigation with etiopathogenesis analysis of all
patients.
Inclusion criteria were patients with type B
tympanogram and positive otomicroscopic image of SOM. Exclusion
criteria were patients with atelectatic ear pathology,
otosclerosis, acute or chronic suppurative otitis media, external
otitis, or foreign bodies in the external ear canal. Patients
referred for grommet insertion or failing to return for follow-up
were also excluded.
Methods
The treatment for SOM included nasal drops with
decongestant drugs up to 3 times a day. Phenylephrine was commonly
used for short periods (3-5 days) in acute episodes and colloidal
silver 1% solution. In some patients, this treatment was
inefficient, with SOM persistence for more than 3 months; for this
situation, intratympanic dexamethasone (DXM) (ITD) injection
treatment was performed under sedation (for the majority of cases),
with the placement of 0.5 ml/4 mg/mm DXM directly into the
antero-inferior quadrant of the tympanic membrane through a small
tympanotomy. The procedure was performed during day
hospitalization, with patients leaving the hospital 3 h after the
ITD placement.
Results
SOM and various parameters
Results showed a higher frequency of SOM in female
patients (58.6%), but without any explanation regarding sex
preference.
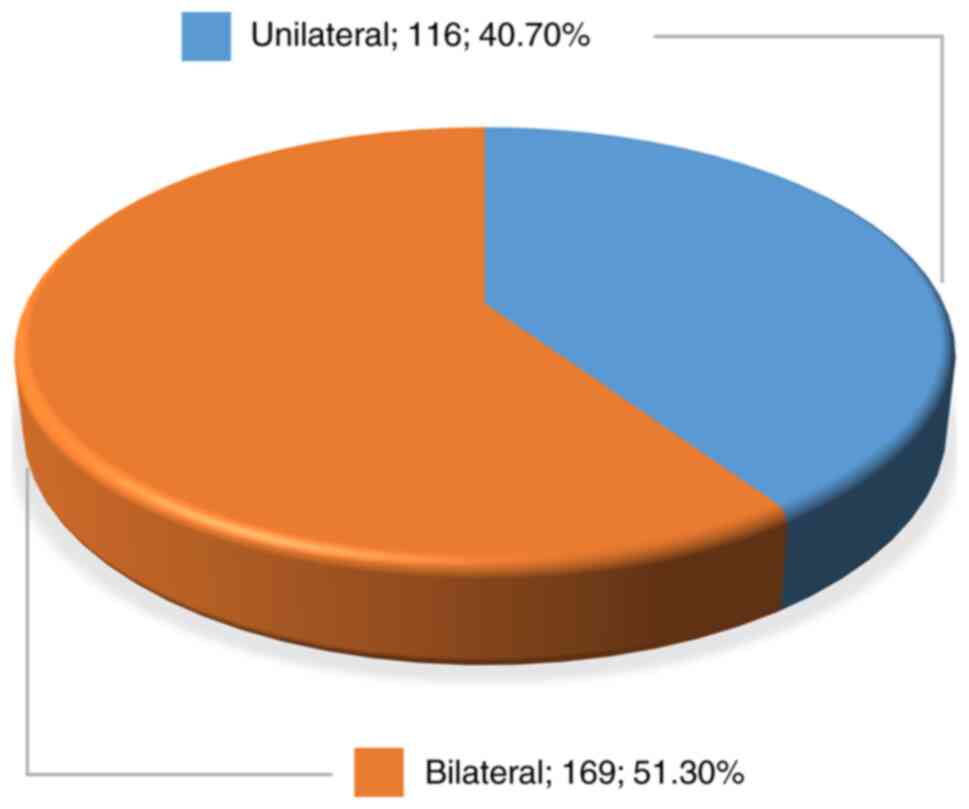
Out of the total number of patients, 59.3% of the
SOM cases were bilateral and 40.7% of cases were unilateral
(Fig. 1).
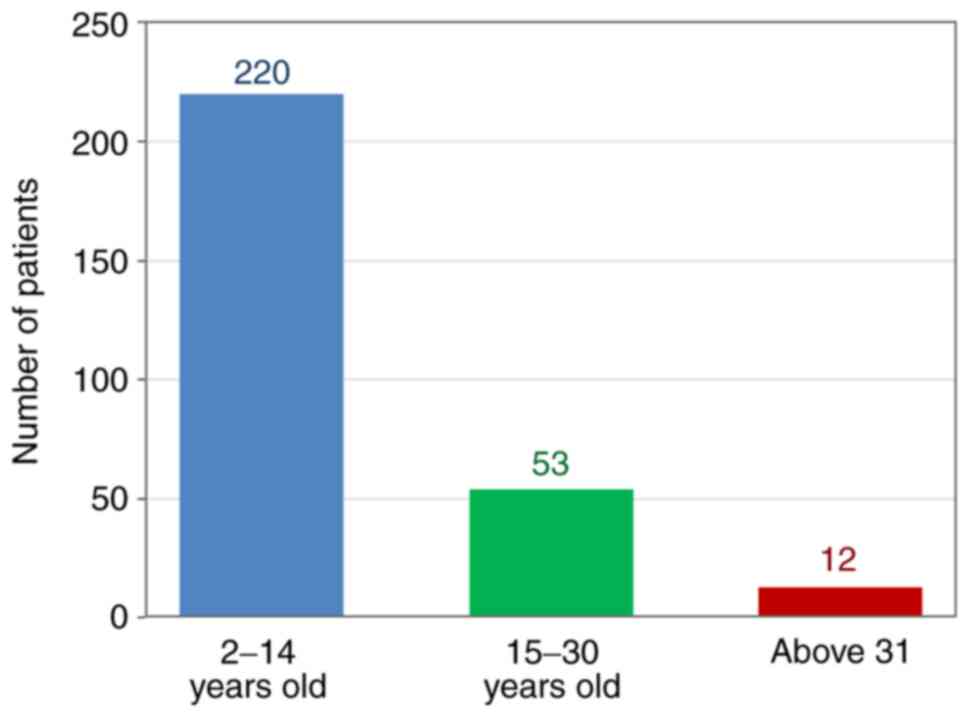
In regards to the patients with SOM, 220 patients
(77.2%) were between 2 and 14 years; 53 patients (18.6%) were in
the age range of 15-30 years, while 12 patients (4.2%) were over 31
years of age (Fig. 2).
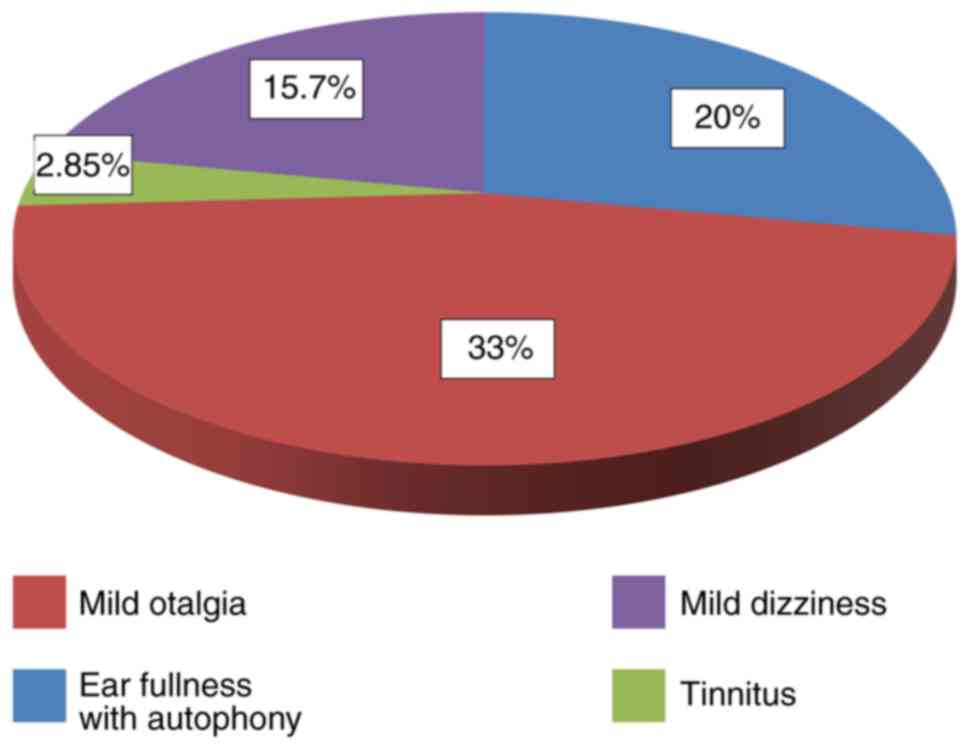
Most patients claimed HL as first symptom (58.57%
bilateral, 30% unilateral); in small children, this was reported by
the parents, or educators. Other local symptoms included ear
fullness with autophony (20%), mild otalgia (33%), tinnitus (2.85%)
and mild dizziness (15.7%) (Fig.
3).
Recorded symptoms associated with SOM were nasal
obstruction with oral breathing (44.2%), rhinorrhea (8.5%),
dysphagia (4.3%), cough (2.85%) and hyponasality (15.7%) (data not
shown).
Physical examinations
Through the physical examination of the children,
retrostilian, submandibular and laterocervical adenopathies were
observed. The nodes were elastic, painless and mobile with an
average diameter of 3x1cm. Other patients had nasal pyramid
dysmorphism.
The otoscopic diagnosis (in 97.15% of cases, the
aspect of the tympanic membrane was modified) was more evident in
adults than in children. In adults, the presence of liquid with or
without air bubbles was most often observed behind a slightly
retracted eardrum (10% of cases). In children, the observation of
fluid level was exceptional.
Audiometric testing was performed on children >5
years of age. Audiometric results showed bilateral conductive HL in
34.37% of patients, unilateral conductive HL in 37.53% of patients,
24% showed bilateral mixed HL and 4.1% showed unilateral mixed HL
and conductive HL in the contralateral ear. HL was greater at low
frequencies, in most cases around 30-40 dB.
Treatment methods
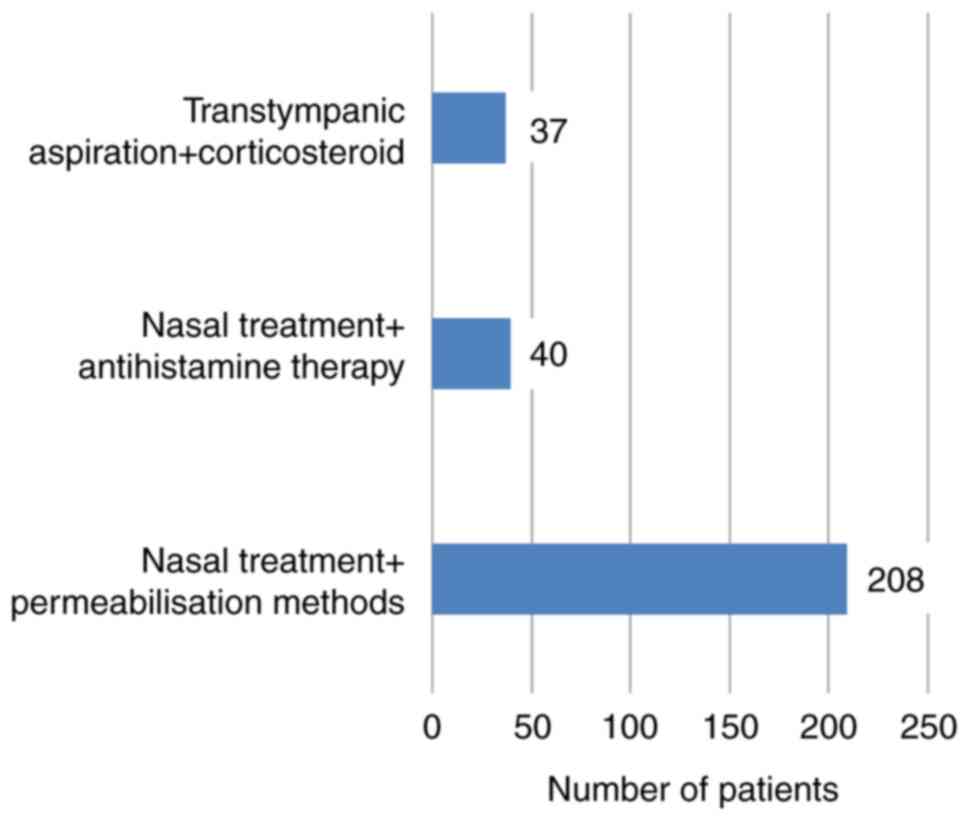
In 208 patients (73%), SOM healed within 3 months,
with just local nasal treatment and ET permeabilization methods: ET
anemizations, mechanical exercises (positive pressure in the
rhinopharynx). In 40 cases (14%), nasal decongestant and
disinfectant drops were accompanied by antihistaminic short-time
treatment (loratadine, levocetirizine) and mucolytic (active
substance acetylcysteine) treatment (Fig. 4).
In 37 cases (13%), SOM did not resolve unless
transtympanic aspiration of the sero-mucous fluid was performed
under sedation and corticosteroid medication (DXM) was placed in
the tympanic cavity (Fig. 4).
Tympanic membrane perforation usually healed
primarily between 5 and 10 days. There were no cases of persistent
tympanic membrane perforation, and audiometric testing at 1 month
showed improvement of hearing thresholds. Follow-up was performed
at one and three years. Most of the patients showed full recovery,
however, a group of 23 patients (8%) showed recurrent SOM and
needed further treatment.
Discussion
The study followed the frequency of SOM by age
groups in parallel with its possible etiopathogenesis. Regarding
children (aged <14 years), there was an increased frequency of
52% in younger children (2-6 years of age) and only 25.2% in older
children (7-14 years of age).
Data from literature confirm this fact. It is
reported that 90% of children have severe serous otitis before
school age (5). The frequency of
common SOM episodes is particularly high, averaging about four
episodes per year (6).
In the first year of life, >50% of children have
SOM which can reach >60% by the age of 2(7). One out of eight children aged five to
six, in preschool, have fluid in one or both ears (8).
Most episodes of SOM heal spontaneously within 3
months, but 30-40% of children have repeated episodes and 5-10%
have SOM lasting over a year or more (1,5,9).
The etiopathogenic factors, according to the medical
files of the patients (anamnesis and personal medical history),
most commonly incriminated in the age group 2-14 years were acute
and chronic adeno-amygdalitis 83.18% (183 out of 220 patients),
acute and chronic rhinosinusitis 51.81% (114 patients out of 220),
septal deviations and inferior turbinate hypertrophy 32.72% (72 out
of 220 patients).
Most factors for the 15- to 30-year age group were:
acute and chronic adeno-amygdalitis 77.35% (41 out of 53 patients),
acute and chronic rhinosinusitis 69.81% (37 out of 53 patients),
septal deviations and turbinate hypertrophy, especially posteriorly
73.58% (39 out of 53 patients).
Patients in the latter age group presented septum
deviation and chronic hypertrophic rhinitis 83.33% (10 out of 12
patients), rhinosinusitis allergy 33.33% (4 out of 12 patients),
chronic otitis media 25% (3 out of 12 patients), acute untreated
rhinopharyngitis 25% (3 out of 12 patients) and rhinopharyngeal
carcinoma 16.66% (2 out of 12 patients).
An increased frequency in symptomatology was
observed during the spring period (40% of cases) and the months
with increased incidence of SOM were March, April, May, September
and October. An explanation can be the increased frequency of viral
rhinopharyngeal inflammation, considerable temperature variations
and sudden changes in atmospheric pressure.
Patient origin was recorded and a higher percentage
of SOM was observed in socio-economically deprived urban
neighborhoods (42.45%, 121 patients), compared to rural areas
(26.66%, 76 patients) and 30.87% in urban areas. This could be
explained by a lower medical addressability, crowded dwellings and
increased exposure to risk factors, such as passive smoking.
According to literature, the average duration of a
SOM episode is 17 days (6). Common
symptomatology is discrete and minimal eardrum changes were
observed (10).
If the SOM persists for >3 months (present in 25%
of cases), symptoms such as HL, vestibular dysfunction, poor school
performance and ear fullness or behavioral changes may occur
(11). SOM can transform into acute
suppurated otitis, which needs antibiotic treatment in order to
avoid further complications (12,13).
Patients included in the study had associated
symptoms as well, such as nasal obstruction with oral breathing,
rhinorrhea, dysphagia, cough, hyponasality, increased frequency of
retrostilian, submandibular, laterocervical adenopathy and
sometimes nasal pyramid dysmorphism. For a correct diagnosis, an
audiometric examination was essential and could be performed on
children after the age of 5.
The audiometric examination should be completed with
tympanometry. This technique has the advantage of objectifying the
variations of acoustic impedance. Tympanometry is a non-invasive
technique that can be achieved in young children and usually a B-
or C-type curve is recorded in SOM.
This examination is especially useful in young
children, where otoscopy is often difficult or inconclusive.
Another advantage of tympanometry is the possibility of observing
the dynamic of middle ear pathology. Performed routinely,
tympanometry would allow a greater detection of SOM.
Targeted treatment is needed for rhinopharyngeal
disobliteration and ET permeabilization in order to establish
normal anatomic and physiologic conditions, hearing improvement and
the prevention of recurrences and development of chronic condition
of the middle ear (chronic SOM, atelectatic ear,
cholesteatoma).
Vasoconstrictor and nasal disinfectants, such as
Phenylephrine and Colloidal Silver, were used after nasal
secretions were aspirated or eliminated by correct nose blowing.
Most of the patients that presented with fresh symptomatology onset
benefited from decongestant substances at the rhinopharyngeal tubal
orifices applied by cotton swabs (34% of cases).
Nasal mucosa hypertrophy is influenced by local
anatomical mechanical obstruction and inflammation, air quality and
allergic terrain of the child. Although studies show a limited
efficacy of antihistaminic medication in ET function prognosis
(14,15), in some cases it may be effective in
nasal decongestion and ET permeabilization (especially in patients
with allergic conditions) (16). In
select cases, before initiating transtympanic function treatment
protocol (performed under sedation during continuous
hospitalization), antihistaminic drugs were used 5-7 days with some
favorable results (6% of cases).
Second-generation H (1)-antihistamines (loratadine or
levocetirizine) have high selectivity for H (1)-receptors with improved efficacy and
minimal side effects compared to first-generation molecules and can
provide improvement of ET mechanics (16).
After ITD, some of the patients complained about ear
fullness 26.31% (75 patients), sometimes light dizziness 10.87% (31
patients) and discrete ear discharge 19.65% (56 patients). Symptoms
can persist several hours and are related to the presence of the
liquid in the middle ear. Myringotomy healed in all patients.
DXM has been used due to good local dispersion with
the ability to inhibit inflammation and reduce edema, satisfactory
absorption in the middle ear and no side effects locally and
generally. Previous findings also found DXM to be effective in the
reduction of granulation tissue, more than antibiotic therapy alone
(17). Mucosal hypertrophy
reduction and possible permeabilization improvement through ET is
expected.
SOM is a disorder found more commonly in childhood,
with recurrent episodes and a higher frequency of viral
rhinopharyngeal infections.
Most frequent etiopathogenic factors were found to
be ET dysfunction, infection, and allergy.
SOM can be relatively asymptomatic with uni- and
even bilateral conductive HL. An audiometric examination is
indispensable in adults and children.
Surgical interventions for associated diseases can
indirectly treat SOM and the inherent ear affliction. The General
Practitioner is familiar with SOM, as well as its treatment. SOM is
especially frequent in school-aged children. If not treated, it can
lead to repeated episodes of SOM and other complications in
time.
Upper respiratory tract mucosa inflammation and
edema should be addressed by complex medical treatment
(vasoconstrictor, disinfectant, corticosteroid, mucolytic,
antihistaminic), although sometimes SOM has to be addressed by
myringotomy. The placement of DXM in the middle ear is an effective
method for localized corticosteroid drug delivery with minimal
local and general side effects.
Acknowledgements
Professional editing, linguistic and technical
assistance were performed by Irina Radu, Individual Service
Provider.
Funding
Funding: No funding was received.
Availability of data and materials
All data and materials supporting the results of the
present study are available in the published article.
Authors' contributions
All authors contributed to the acquisition of the
data and critical revision of manuscript for important intellectual
content. CM contributed to the design of the study, data analysis
and edited the manuscript. SC contributed to the design of the
study and data acquisition. BC analyzed and interpreted the data.
DV designed the study, provided archive data and wrote the main
manuscript text. CB contributed to the data analysis and to the
design of the study. DB contributed to the data acquisition and
data interpretation. AC provided archive data, contributed to data
acquisition and edited the manuscript. LR contributed to the data
analysis, data interpretation and edited the manuscript. All
authors read and approved the final version of the manuscript. CM
and BC are responsible for confirming the authenticity of raw
data.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
‘Grigore T. Popa’ University of Medicine and Pharmacy (Iasi,
Romania)- Nr.4/13.09.21. Written informed consent was obtained from
all the patients and/or guardians prior to publication.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kocygit M, Ortekin SG, Cakabay T, Ozkaya
G, Bezgin SU and Adali MK: Frequency of serous otitis media in
children without otolaryngological symptoms. Int Arch
Otorhinolaryngol. 21:161–164. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Stool SE, Berg AO, Berman S, Carney CJ,
Cooley JR, Culpepper L, Eavey RD, Feagans LV, Finitzo T, Friedman
E, et al: Managing otitis media with effusion in young children.
American Academy of Pediatrics the Otitis Media Guideline Panel.
Pediatrics. 94:766–773. 1994.PubMed/NCBI
|
|
3
|
Shekelle P, Takata G, Chan LS,
Mangione-Smith R, Corley PM, Morphew T and Morton S: Diagnosis,
natural history, and late effects of otitis media with effusion.
Evid Rep Technol Assess (Summ). 55:1–5. 2002.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Gates GA, Avery CA, Prihoda TJ and Cooper
JC Jr: Effectiveness of adenoidectomy and tympanostomy tubes in the
treatment of chronic otitis media with effusion. N Engl J Med.
317:1444–1451. 1987.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Tos M: Epidemiology and natural history of
secretory otitis. Am J Otol. 5:459–62. 1984.PubMed/NCBI
|
|
6
|
Mandel EM, Doyle WJ, Winther B and Alper
CM: The incidence, prevalence and burden of OM in unselected
children aged 1-8 years followed by weekly otoscopy through the
‘common cold’ season. Int J Pediatr Otorhinolaryngol. 72:491–499.
2008.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Casselbrant M and Mandel EM: Epidemiology.
In: Rosenfeld RM, Bluestone CD, Eds: Evdence-based otitis media, cd
2, Hamilton, Ontario, BC Decker, 147-162, 2003.
|
|
8
|
Martines F, Bentivegna D, Di Piazza F,
Martinciglio G, Sciacca V and Martines E: The point prevalence of
otitis media with effusion among primary school children in Western
Sicily. Eur Arch Otorhinolaryngol. 267:709–714. 2010.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Williamson IG, Dunleavey J, Bain J and
Robinson D: The natural history of otitis media with effusion--a
three-year study of the incidence and prevalence of abnormal
tympanograms in four South West Hampshire infant and first schools.
J Laryngol Otol. 108:930–934. 1994.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Bhutta MF, Thornton RB, Kirkham LS,
Kerschner JE and Cheeseman MT: Understanding the aetiology and
resolution of chronic otitis media from animal and human studies.
Dis Model Mech. 10:1289–1300. 2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Rosenfeld RM, Schwartz SR, Cannon CR,
Roland PS, Simon GR, Kumar KA, Huang WW, Haskell HW and Robertson
PJ: Clinical practice guideline: Acute otitis externa. Otolaryngol
Head Neck Surg. 150 (Suppl 1):S1–S24. 2014.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Butnaru C, Serban R, Martu C, Lungu A,
Doroftei EA, Cobzeanu B and Cozma S: Otitis media complications
proceedings of national Ent. Head and Neck Surgery Conference.
102–106. 2019.
|
|
13
|
Serban R, Butnaru C, Stefanescu H, Martu
C, Cozma S and Radulescu L: Complications of otomastoiditis in
children. Conference: National ENT, head and neck surgery national
ent. Head And Neck Surgery Conference. 312–315. 2017.
|
|
14
|
Vanneste P and Page C: Otitis media with
effusion in children: Pathophysiology, diagnosis, and treatment. A
review. J Otol. 14:33–39. 2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Norman G, Llewellyn A, Harden M,
Coatesworth A, Kimberling D, Schilder A and McDaid C: Systematic
review of the limited evidence base for treatments of Eustachian
tube dysfunction: A health technology assessment. Clin Otolaryngol.
39:6–21. 2014.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ma Y, Liang M, Tian P, Liu X, Dang H, Chen
Q, Zou H and Zheng Y: Eustachian tube dysfunction in patients with
house dust mite-allergic rhinitis. Clin Transl Allergy.
10(30)2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Paksoy M, Altin G, Eken M and Hardal U:
Effectiveness of intratympanic dexamethasone in otitis media with
effusion resistant to conventional therapy. Indian J Otolaryngol
Head Neck Surg. 65 (Suppl 3):S461–S467. 2013.PubMed/NCBI View Article : Google Scholar
|