Introduction
Coma induced by severe brain injury is a
self-limiting state that typically resolves within 2 weeks
(1). Severe and diffuse lesions of
the cortex or underlying white matter, bilateral thalamic damage
and brainstem injury account for the primary reasons of comas
(1). After two weeks, comas are
classified into disorders of consciousness (DOC), which can be
divided into 2 subgroups: Vegetative state (VS) and minimally
conscious state (MCS) (1). VS is a
condition of a wakeful unconscious state. In VS, patients can
spontaneously open their eyes, but without repetitive behavioral
responses to verbal comprehension, verbal or gestural
communication, and purposeful situations of visual, auditory,
tactile and harmful stimuli (1,2). MCS
is a condition of severely altered consciousness characterized by
functional communication or functional use of objects (1,2).
Patients with MCS showed a range of behavioral signs of
inconsistent awareness and reliable communication (1,2). The
use of multiple treatments for DOC recovery in different stages is
necessary, including invasive and non-invasive treatments. Invasive
methods, including deep brain and spinal cord stimulation, have
ethical and procedural limitations (3,4) and
are not suitable for early DOC. A report of non-invasive measures
using electrical and magnetic stimulation of the brain, spinal cord
and roots was endorsed by the first International Federation of
Clinical Neuroelectrophysiology (IFCN) 30 years ago. Among
developed neurostimulation techniques, non-invasive measures,
including transcranial magnetic stimulation and transcranial direct
current stimulation, may be promising for early DOC therapeutic
intervention (5). However, there
are still no sufficient evidence-based methods to treat DOC to
date. During the past decade, several studies and clinical trials
have demonstrated potential therapeutic applications of
non-invasive brain stimulation, particularly for transcranial
magnetic stimulation (TMS), which is non-invasive, safe, painless
and effective in treating DOC (6-8).
A magnetic stimulating coil placed on the human
scalp can generate a strong magnetic field by a rapid pulse
current, which can penetrate the skull, causing secondary induction
current at adjacent nerve tissues (9). The current acts on the cell membrane
of cerebral cortical neurons, generating excitatory or inhibitory
postsynaptic potentials to stimulate neurons that lead to altered
cortical function (10,11). TMS can be applied one stimulus at a
time (single-pulse TMS), in pairs of stimuli separated by a
variable interval (paired-pulse TMS) or in trains repetitive TMS
(rTMS) (3,11). rTMS focuses on a particular cortical
site to improve neurophysiological functions and has been proven to
have a neuromodulatory effect (3,7,11).
Furthermore, its repetitive effect has been proven to be more
effective than single-pulse and paired-pulse TMS in the treatment
of DOC (12-16).
rTMS is currently used for the treatment of several diseases such
as depression, psychiatric illness, epilepsy, Parkinson's disease
and cognitive dysfunction, and achieves satisfactory curative
effects (16-20).
However, studies using rTMS to treat DOC have shown
conflicting results. Louise-Bender Pape et al (6) reported a trend toward significant
neurobehavioral gains by rTMS to stimulate the right dorsolateral
prefrontal cortex (DLPFC) in a traumatic patient with
VS/unresponsive wakefulness syndrome. Xie and Zhang (8) reported that rTMS treatment could
improve consciousness disturbance in 10 patients with stroke as
detected by quantitative electroencephalography spectral power
analysis. Naro et al (21)
found that a single session of 10 Hz rTMS over the right DLPFC may
improve consciousness and partially restore the connectivity within
several cortical areas, but no clinical effects were observed
between the test and control groups. Liu et al (22) reported no behavioral improvement
following one session of primary motor cortex (M1) 20 Hz rTMS for
10 min in 10 patients with DOC. However, hemodynamic functions were
improved in the MCS group but not in the unresponsive wakefulness
syndrome group. Bai et al (23) reported that an increased Coma
Recovery Scale-Revised (CRS-R) score was observed in a female with
intracranial hemorrhage for 9 months prior to receiving rTMS 30
times. No effect of rTMS on the DOC was reported in another study.
Cincotta et al (24)
reported a double-blinded randomized controlled trial comprising 74
patients with DOC. No behavioral improvements were found following
five repeated sessions at 20 Hz applied over the M1 for 10 min in
11 patients with unresponsive wakefulness syndrome. For the
diagnosis of a consciousness disorder, the target of rTMS
stimulation may impact the efficacy of rTMS on DOC. The present
study hypothesized that high-frequency rTMS stimulation on patients
in VS could improve the consciousness state (CS) and CRS-R scores.
The aim of the present study was to investigate the efficacy of
rTMS on VS patients who received 10 Hz rTMS on the right DLPFC.
Materials and methods
Patients
In the present retrospective cohort study, all
patients were recruited from the Departments of Neurosurgery and
Coma Recovery (Central Hospital of Jinzhou, Jinzhou, China) and
between May 2017 to November 2018. The Coma Recovery Department of
Jinzhou Central Hospital is the first standard coma recovery and
rehabilitation ward in northeast China. The inclusion criteria were
as follows: i) Accepted coma treatments 2 weeks after admission;
ii) aged 18-75 years; iii) vital signs were stable; iv) their CRS-R
score was assessed by international criteria and they fulfilled the
diagnostic criteria of VS (1); v)
had no seizures or brain edema; vi) received no sedatives and
anti-epilepsy drugs within the last 7 days; vii) informed consent
was signed by patients of their legally authorized representative
to participate in the present study. The exclusion criteria were as
follows: i) No motor evoked potentials (MEP) were elicited; ii)
severe dysfunction of heart, liver or kidney; iii) extreme
complications, such as pneumonia and deep venous thrombosis; iv)
seizures or skull scalp injury during treatment; v) craniotomy or
metallic implantation on the right side of the head; vi) previous
neurological or psychiatric disorders; vii) no 20 consecutive rTMS
treatments in the rTMS group. There were two groups in the present
study. The patients whose legally authorized representatives
accepted rTMS treatment were allocated into the rTMS group and
those who refused rTMS treatment were allocated into the control
group. Finally, patient data was collected from 15 patients from
the rTMS group and 17 patients from the control group. All patients
received similar routine medication and rehabilitation course in
our coma recovery ward.
Study design and stimulation
protocol
The effect of rTMS is dependent on its frequency.
Low-frequency rTMS (<1 Hz) can reduce neuronal excitability,
local metabolism levels and cerebral blood flow, and inhibit
cortical activity (13,25), whereas high-frequency rTMS (5-20 Hz)
exerts the opposite effects. In addition, rTMS can affect the
transmission of monoamine neurotransmitters and genetic expression
of neuronal excitability in the brain (11,26).
The patients in the rTMS group received active 10 Hz rTMS on the
right DLPFC once per day over 20 consecutive days. TMS pulses were
delivered using a Yiruide CCY-IA stimulator and a circular coil
(Wuhan Yiruide Medical Equipment New Technology Co., Ltd.), which
can produce a pulse stimulation frequency of 0.01-100 Hz and a
2.0-T maximum magnetic field strength. The circular coil had a
diameter of 10 cm, where stimulation is most effective under the
coil. The minimal stimulation is in the center of the ring
(15). The consciousness is
dependent on the function of the cerebral cortex, which affects
high-level central neural system function and bilateral hemisphere
functional cortices that compete and suppress together, and the
ascending reticular activating system that affects regular
awakening (27,28). The key point for rTMS is the site of
stimulation, which has been discussed in several studies. The DLPFC
(6-8)
and M1 (24,29,30)
are the most common stimulation sites of choice. Several studies
have chosen the left (7) or right
(8) DLPFC as the site of
stimulation, with positive outcomes. The right DLPFC is closely
linked to the brain network structure, with the ascending reticular
activating system connecting to the DLPFC and even the entire
cortex, via the thalamic relay and raphe nuclei, which are the most
important for DOC recovery (6). The
maintenance of sustained arousal and attention are also cardinal
functions of the right DLPFC (6).
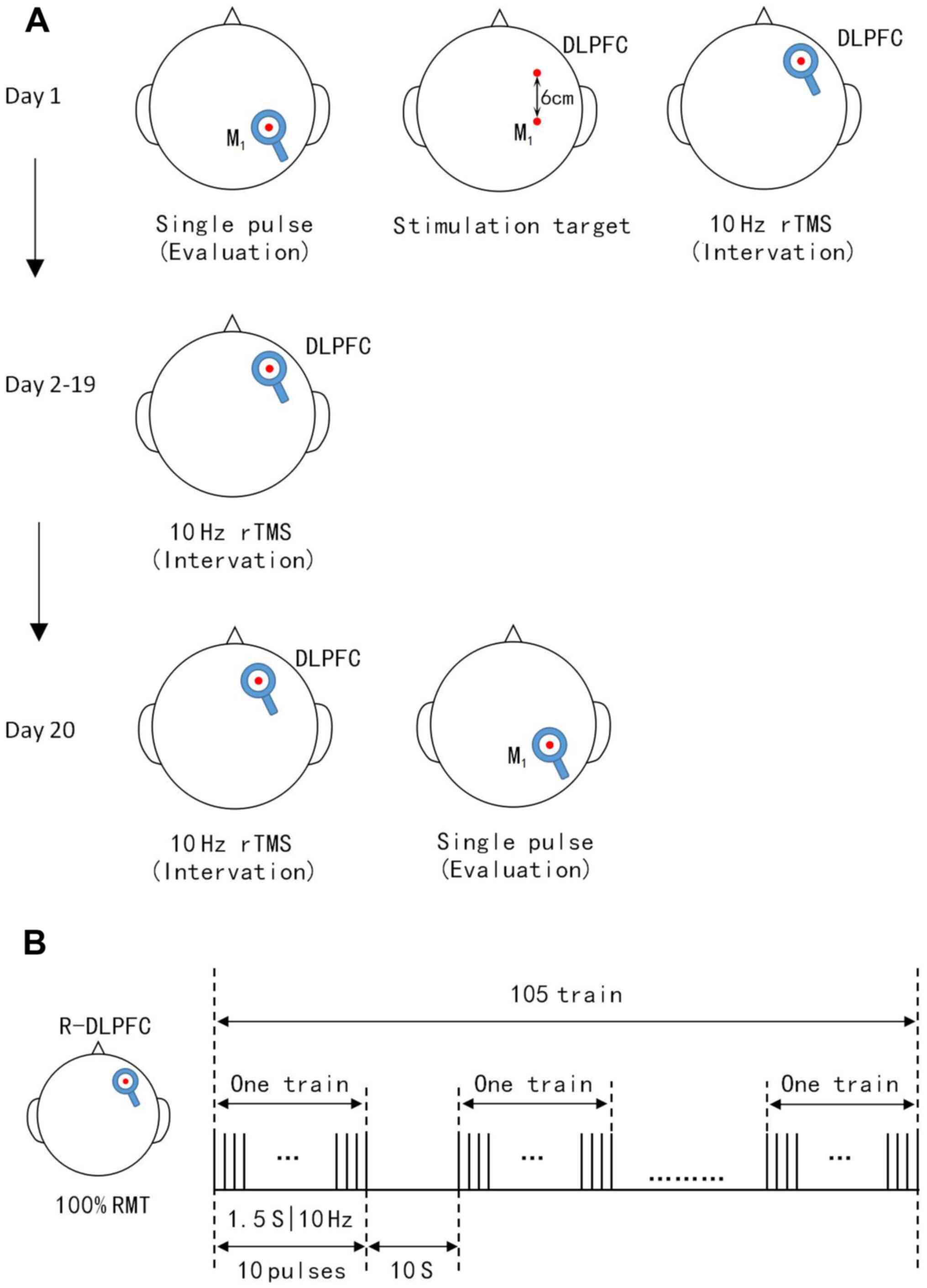
Based on these reasons, the right DLPFC was selected as the
stimulation site in the present study. The stimulation target is
the most important parameter for rTMS treatment (27-30).
The right hemisphere motor cortex was determined by MEP and the 5+1
cm prefrontal cortex in front of the right M1 was chosen as the
right DLPFC (Fig. 1A) (31). The coil was placed tangentially
toward the scalp over the right DLPFC for stimulation. Stimulation
intensity is the second most important parameter for each patient
and was determined based on the resting motor threshold (RMT). The
stimulation intensity of RMT is also undefined. Xia et al
(7) administered 90% RMT to
patients with chronic DOC. Xie and Zhang (8) used 100% RMT to treat patients with DOC
with stroke. However, high levels of intensity and frequency could
trigger seizures. Cavinato et al (32) reported that 20 Hz rTMS treatment
could trigger frequent seizures. Most rTMS studies used 10 Hz and
100% RMT and had a lower risk of epilepsy (5,6,8). Based
on the above consideration, 10 Hz and 100% RMT were chosen as the
treatment parameters in the present study. According to the IFCN
Committee recommendations (15),
RMT was defined as the lowest TMS intensity to evoke at least 5/10
electromyogram with an amplitude of >50 µV peak-to-peak in the
relaxed first dorsal interosseous muscle of the right hand
(7,15). During RMT measurement, earplugs were
inserted into the ears of patients, which continuously played a
masking noise to prevent the interference of auditory potentials
with TMS discharge. When the total number of pulses per treatment
was >1,000 and the stimulation intensity was ≥100% RMT, the cure
rate of patients was significantly increased. A single treatment of
1,000-2,000 pulses is safe and effective according to TMS
guidelines (15). A single daily
session of stimulation consisted of 1,575 pulses (10 Hz trains for
1.5 sec; repeated 105 times with an inter-train interval of 10 sec;
total session, 20 min and 8 sec) at an intensity of 100% RMT
(Fig. 1B) was applied in the
present study. Meanwhile, patient routine medication and
rehabilitation courses continued as usual during rTMS
treatment.
Outcome evaluation
All patients received CRS-R scores and MEP latency
and central motor conduction time (CMCT) measurements prior to the
first treatment and after 20 days of treatment, which was the end
of the study.
Statistical analysis
All statistical analysis was performed using
GraphPad Prism 7.0 (GraphPad Software, Inc.). The Mann-Whitney U
test, Wilcoxon matched pairs signed rank test, paired t-test,
unpaired t-test and Fisher's exact probability tests were used for
comparison between groups, as appropriate. Normally distributed
data are expressed as the mean ± SD. Skewed distributed data are
expressed as the median with interquartile range. P<0.05 was
considered to indicate a statistically significant difference.
Results
Patient data in rTMS and control
groups
All patients remained in a stable clinical state
during routine medication and rehabilitation course. There were no
focal lesions in the right DLPFC in all patients, as evidenced by
their brain scans. Detailed clinical characteristics of
participants are shown in Tables I
and II. The mean age of the
patients was 60.5±1.8 (range, 49-70) years in the rTMS group and
59.7±2.1 (range, 39-72) years in the control group (P>0.05).
There were eight males and seven females in the rTMS group,
including seven with ICH and eight with TBI and 10 males and seven
females in the control group, including nine with ICH and eight
with TBI. The admission time was 4.6±0.8 h in the rTMS group and
4.4±0.7 h in the control group (P>0.05). The mean CRS-R score
was 3.7±0.7 (3-5)
in the rTMS group and 3.8±0.8 (3-5)
in the control group (P>0.05). The mean MEP prior to treatment
was 29.87±0.96 msec in the rTMS group and 30.02±0.98 msec in the
control group (P>0.05). The mean CMCT before treatment was
11.04±0.24 msec in the rTMS group and 11.14±0.23 msec in the
control group (P>0.05). Baseline data, including age, sex,
etiology, admission time, admission Glasgow Coma Scale score, CRS-R
score, MEP and CMCT prior to treatment were not significantly
different between the rTMS and control groups (Fig. 2).
 | Figure 2Baseline data for the rTMS and
control groups. (A) Etiology, (B) sex, (C) sex distribution in the
rTMS group, (D) sex distribution in the control group, (E) number
of males in the rTMS and control groups, (F) number of females in
the rTMS and control groups, (G) age, (H) admission time, (I)
admission GCS score, (J) CRS-R score, (K) MEP and (L) CMCT prior to
treatment were not significantly different between rTMS and control
groups. CRS-R, JFK Coma Recovery Scale-Revised; MEP, motor evoked
potentials; CMCT, central motor conduction time; rTMS, repetitive
transcranial magnetic stimulation; pre, prior to treatment; ICH,
intracerebral hemorrhage; TBI, traumatic brain injury; GCS, Glasgow
Coma Scale. |
 | Table IClinical data of the repetitive
transcranial magnetic stimulation group. |
Table I
Clinical data of the repetitive
transcranial magnetic stimulation group.
| | | | | | | CRS-R | MEP latency,
msec | CMCT, msec | CS |
|---|
| Patient | Age years | Sex | Etiology | Admission time,
h | Admission GCS | Day 1 | Day 20 | Day 1 | Day 20 | Day 1 | Day 20 | Day 20 |
|---|
| 1 | 65 | M | ICH | 4 | 4 | 3 | 5 | 31.04 | 27.96 | 12.45 | 12.03 | VS |
| 2 | 55 | M | TBI | 3 | 5 | 4 | 8 | 29.81 | 29.44 | 11.09 | 10.21 | MCS- |
| 3 | 58 | F | ICH | 4 | 4 | 3 | 6 | 30.83 | 27.15 | 11.97 | 11.12 | MCS- |
| 4 | 62 | F | TBI | 2 | 5 | 4 | 7 | 29.13 | 28.13 | 10.54 | 9.86 | MCS- |
| 5 | 49 | M | TBI | 3 | 4 | 3 | 7 | 30.56 | 29.84 | 11.23 | 10.14 | MCS- |
| 6 | 52 | M | TBI | 2 | 4 | 3 | 6 | 31.27 | 27.45 | 12.37 | 11.84 | MCS- |
| 7 | 68 | F | TBI | 4 | 4 | 4 | 6 | 28.97 | 29.21 | 10.21 | 9.75 | MCS- |
| 8 | 50 | F | ICH | 4 | 4 | 3 | 7 | 30.07 | 27.46 | 11.08 | 10.26 | MCS- |
| 9 | 70 | M | ICH | 5 | 6 | 5 | 8 | 28.75 | 30.01 | 10.11 | 9.84 | MCS- |
| 10 | 65 | F | TBI | 3 | 4 | 3 | 5 | 31.66 | 27.48 | 12.58 | 11.46 | VS |
| 11 | 57 | M | ICH | 6 | 6 | 5 | 9 | 28.97 | 28.04 | 9.75 | 9.43 | MCS- |
| 12 | 60 | F | TBI | 3 | 4 | 4 | 8 | 29.11 | 28.96 | 10.87 | 10.22 | MCS- |
| 13 | 63 | M | ICH | 5 | 5 | 4 | 7 | 29.35 | 27.26 | 10.34 | 9.94 | MCS- |
| 14 | 65 | F | ICH | 4 | 5 | 4 | 9 | 29.45 | 27.88 | 10.89 | 9.75 | MCS- |
| 15 | 69 | M | TBI | 3 | 5 | 4 | 8 | 29.14 | 27.88 | 10.11 | 10.03 | MCS- |
| Table IIClinical data of the control
group. |
Table II
Clinical data of the control
group.
| | | | | | | CRS-R | MEP latency,
msec | CMCT, msec | CS |
|---|
| Patient | Age years | Sex | Etiology | Admission time,
h | Admission GCS | Day 1 | Day 20 | Day 1 | Day 20 | Day 1 | Day 20 | Day 20 |
|---|
| 1 | 68 | F | ICH | 4 | 4 | 3 | 3 | 31.84 | 31.55 | 12.67 | 12.58 | VS |
| 2 | 65 | M | ICH | 5 | 4 | 3 | 4 | 30.95 | 31.01 | 12.14 | 11.99 | VS |
| 3 | 52 | M | TBI | 3 | 5 | 4 | 5 | 30.13 | 30.05 | 11.75 | 11.37 | VS |
| 4 | 63 | F | ICH | 5 | 4 | 4 | 5 | 29.45 | 29.34 | 10.98 | 10.56 | VS |
| 5 | 59 | F | TBI | 3 | 5 | 4 | 6 | 29.63 | 29.55 | 11.04 | 10.88 | MCS- |
| 6 | 39 | M | ICH | 3 | 6 | 4 | 7 | 29.97 | 28.88 | 11.34 | 10.01 | MCS- |
| 7 | 56 | F | TBI | 2 | 5 | 5 | 7 | 28.74 | 28.05 | 10.13 | 9.59 | MCS- |
| 8 | 57 | M | TBI | 3 | 4 | 4 | 6 | 29.03 | 28.93 | 10.21 | 10.09 | MCS- |
| 9 | 69 | M | ICH | 5 | 4 | 3 | 4 | 31.37 | 32.01 | 12.45 | 12.56 | VS |
| 10 | 71 | F | ICH | 4 | 3 | 3 | 3 | 30.87 | 32.54 | 11.97 | 12.01 | VS |
| 11 | 62 | M | TBI | 4 | 4 | 3 | 4 | 31.41 | 30.61 | 12.47 | 12.06 | VS |
| 12 | 72 | M | ICH | 6 | 5 | 5 | 5 | 28.87 | 28.64 | 10.11 | 10.13 | VS |
| 13 | 49 | F | TBI | 4 | 4 | 3 | 6 | 30.21 | 29.15 | 10.87 | 10.22 | MCS- |
| 14 | 60 | M | TBI | 4 | 4 | 3 | 4 | 29.95 | 29.74 | 10.54 | 10.45 | VS |
| 15 | 54 | M | ICH | 4 | 5 | 4 | 5 | 29.87 | 28.93 | 10.89 | 10.57 | VS |
| 16 | 56 | F | ICH | 5 | 4 | 5 | 3 | 28.98 | 29.88 | 9.89 | 10.51 | VS |
| 17 | 62 | M | TBI | 3 | 4 | 5 | 3 | 29.01 | 30.13 | 9.97 | 11.06 | VS |
Effects of the 10 Hz rTMS treatment
protocol as determined by CRS-R scores on day 20
A total of 15 patients in the rTMS group and 17
patients in the control group completed the treatment (Tables I and II), with no specific side effects
recorded. There were no statistical differences between the two
groups prior to treatment (Fig. 2).
A significant increase in the CRS-R scores (Fig. 3A; P<0.001) in the rTMS group was
observed 20 days later compared with those at pretreatment. An
increase in the CRS-R scores (Fig.
3B; P=0.035) in the control group was also observed compared
with those at pretreatment. The CRS-R scores were increased in all
patients in the rTMS group. A total of seven patients showed
improved CRS-R scores by >4 points in the rTMS group. Only two
patients in the control group improved their CRS-R scores by 3
points; however, no significant increase was observed in most
patients. The median CRS-R score change in the rTMS group improved
by 3 points, whereas the control group improved by 1 point
(Fig. 3C; P<0.001). Significant
differences were observed in the improvement of the CS rate. In the
rTMS group, 13 VS patients (86.7%) turned MCS-, with only five
patients (29.4%) in the control group (P=0.0016). In the rTMS
group, the changes in CRS-R scores of seven patients were ≥4 points
at day 20 (Table III).
| Table IIIChanges of ≥4 points in CRS-R scores
at day 20 in the rTMS group. |
Table III
Changes of ≥4 points in CRS-R scores
at day 20 in the rTMS group.
| | CRS-R | |
|---|
| Patient no. | Day | Auditory | Visual | Motor | Oro-motor | Comm | Arousal | Total | CS |
|---|
| 2 | 1 | 1 | 1 | 2 | 0 | 0 | 0 | 4 | VS |
| | 20 | 1 | 1 | 3 | 1 | 0 | 2 | 8 | MCS- |
| 5 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 3 | VS |
| | 20 | 1 | 1 | 3 | 0 | 0 | 2 | 7 | MCS- |
| 8 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 3 | VS |
| | 20 | 1 | 1 | 3 | 0 | 0 | 2 | 7 | MCS- |
| 11 | 1 | 1 | 1 | 2 | 0 | 0 | 1 | 5 | VS |
| | 20 | 2 | 1 | 3 | 1 | 0 | 2 | 9 | MCS- |
| 12 | 1 | 1 | 1 | 2 | 0 | 0 | 0 | 4 | VS |
| | 20 | 1 | 1 | 3 | 1 | 0 | 2 | 8 | MCS- |
| 14 | 1 | 1 | 1 | 2 | 0 | 0 | 0 | 4 | VS |
| | 20 | 2 | 1 | 3 | 1 | 0 | 2 | 9 | MCS- |
| 15 | 1 | 1 | 1 | 2 | 0 | 0 | 0 | 4 | VS |
| | 20 | 1 | 1 | 3 | 1 | 0 | 2 | 8 | MCS- |
Effects of the 10 Hz rTMS treatment
protocol as determined by MEP latency and CMCT measurements
The two groups of patients were examined using
magnetic stimulation evoked potentials, the main indicators of
which were MEP and CMCT. There were no statistical differences
between the two groups prior to treatment (Fig. 2K; P=0.662; Fig. 2L; P=0.758). A significant decrease
in the MEP and CMCT in the rTMS group were observed 20 days later
compared with those at pretreatment (Fig. 3D; P<0.001; Fig. 3G; P<0.001), with no significant
decrease in the control group (Fig.
3E; P=0.693; Fig. 3H; P=0.070).
The changes in MEP and CMCT between the two groups were
statistically significant (Fig. 3F;
P<0.00; Fig. 3I; P<0.01).
Discussion
The aim of the present study was to investigate the
effects of 10 Hz rTMS at the right DLPFC in patients with VS. The
present results demonstrated that 10 Hz rTMS at the right DLPFC
could improve CS from VS to MCS-, increase the CRS-R score and
decrease MEP and CMCT.
CS was the main factor that could affect the outcome
evaluation, since VS and MCS were fundamentally different in DOC
(1,22,33).
Functional neuroimaging has previously verified that MCS+ patients
preserve greater metabolic activity and resting state functional
connectivity in the language network (33,34).
It is important to distinguish VS form MCS, as misdiagnosis can
affect the outcome of a study (35). It was confirmed that functional
outcome was significantly more favorable for patients in MCS
relative to those in VS, especially for traumatic brain injury
(36,37). All participants were in VS, as
determined by their CRS-R (measured three times), in our
departments. The CRS-R score was the highest score assessed by
three trained physicians. Patients who had recently used
antiepileptics and sedatives were excluded from the current study,
as these drugs can have a significant impact on the accurate
scoring of patients. After 20 days of treatment, an increase in the
CRS-R scores in the control group was also observed compared with
the pretreatments cores that may be caused by an insufficient
number of cases and insufficient self-recovery following brain
injury in certain patients. However, the change in CRS-R scores was
significantly different between the two groups. Patient no. 14 from
the rTMS group was used as a sample. Prior to treatment, she had an
occasional response to sound and a startle response when the
physician's finger approached her eyeballs. Flexing was observed
when her upper limbs were stimulated; however, she could not open
her eyes. Her CRS-R scores for auditory, motor and oro-motor
function had increased by 1 point 20 days after treatment. Her
arousal score increased by 2 points. She could open her eyes
spontaneously, locate sound and respond to pain in her upper limbs.
She was also occasionally able to put the surface of her tongue
between her lips. Her behavior had improved and the increased CRS-R
score was 5. Behavioral improvements were also observed in 13 VS
patients from in the rTMS group. Auditory and motor functions and
arousal are major aspects of behavioral improvement (8). The findings of the present study were
similar to those in the reports of Louise-Bender Pape et al
(6) and Xie and Zhang (8). The choice of DLPFC as the stimulating
target might be the reason for the significant increase in arousal.
It was shown that 10 Hz rTMS of the right DLPFC in early VS is
feasible and efficient.
MEP latency and amplitude, as well as CMCT, were
used as evaluation indicators by Barker et al (9) in 1985. Cakar et al (38) reported that MEP latency and
amplitude, as well as CMCT, exhibited a correlation with clinical
parameters and daily life functionality in 22 chronic post-stroke
patients. Shorter MEP latency and faster CMCT were positively
correlated with improved clinical measurements. The data of the
present study, which demonstrated that rTMS treatment could
increase the conduction velocity of the central nervous system.
Additionally, treatment enhanced the excitability of central
neurons and the function of the cerebral cortex to activate the
ascending reticular activating system, which affects regular
awakening, were similar to the results obtained by Cakar et
al (38). The present study
focused on recovery outcomes of early VS patients, which is rarely
reported in current studies. Early functional recovery could
enhance the confidence of doctors and family members to continue
treatment, avoiding abandonment of treatment for some VS patients
who might recover. The present study was not, however, without its
limitations. The present study had a relatively small sample size
and was a monocentric retrospective cohort study, lacking
randomization and a sham group. It lacked measures of the patient
long term outcome as many factors affected long term prognosis
after treatment including family, economy and follow-up treatment
levels. The data for 3- and 6-month follow-ups were incomplete for
various reasons. A multicenter, randomized and sham treatment study
should be conducted in the future.
In conclusion, 10 Hz rTMS at the right DLPFC in
early DOC is feasible and efficient. rTMS treatment could
significantly improve patient state of awareness and accelerate
their recovery in early VS.
Acknowledgements
Not applicable.
Funding
The current study was supported by the Scientific
Technology Research Projects of Jinzhou (grant no. 16B1G37).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
XG designed the study. XG, YZ and XL drafted the
manuscript. YZ, TX and XL collected and statistically analyzed
data. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of the Central Hospital of Jinzhou (Jinzhou, China).
Written informed consent was obtained from each patient's legally
authorized representative.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Giacino JT, Fins JJ, Laureys S and Schiff
ND: Disorders of consciousness after acquired brain injury: The
state of the science. Nat Rev Neurol. 10:99–114. 2014.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Wu DY, Cai G, Yuan Y, Liu L, Li GQ, Song
WQ and Wang MB: Application of nonlinear dynamics analysis in
assessing unconsciousness: A preliminary study. Clin Neurophysiol.
122:490–498. 2011.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Guerra A, Costantini EM, Maatta S, Ponzo D
and Ferreri F: Disorders of consciousness and electrophysiological
treatment strategies: A review of the literature and new
perspectives. Curr Pharm Des. 20:4248–4267. 2014.PubMed/NCBI
|
|
4
|
Shin SS, Dixon CE, Okonkwo DO and
Richardson RM: Neurostimulation for traumatic brain injury. J
Neurosurg. 121:1219–1231. 2014.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Rossini PM, Barker AT, Berardelli A,
Caramia MD, Caruso G, Cracco RQ, Dimitrijević MR, Hallett M,
Katayama Y, Lücking CH, et al: Noninvasive electrical and magnetic
stimulation of the brain, spinal cord and roots: Basic principles
and procedures for routine clinical application Report of an IFCN
committee. Electroencephalogr Clin Neurophysiol. 91:79–92.
1994.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Louise-Bender Pape T, Rosenow J, Lewis G,
Ahmed G, Walker M, Guernon A, Roth H and Patil V: Repetitive
transcranial magnetic stimulation-associated neurobehavioral gains
during coma recovery. Brain Stimul. 2:22–35. 2009.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Xia X, Bai Y, Zhou Y, Yang Y, Xu R, Gao X,
Li X and He J: Effects of 10 Hz repetitive transcranial magnetic
stimulation of the left dorsolateral prefrontal cortex in disorders
of consciousness. Front Neurol. 8(182)2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Xie Y and Zhang T: Repetitive transcranial
Magnetic Stimulation improves Consciousness disturbance in stroke
patients: A quantitative electroencephalography spectral power
analysis. Neural Regen Res. 7:2465–2472. 2012.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Barker AT, Jalinous R and Freeston IL:
Non-invasive magnetic stimulation of human motor cortex. Lancet.
1:1106–1107. 1985.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Di Lazzaro V, Oliviero A, Pilato F,
Saturno E, Dileone M, Mazzone P, Insola A, Tonali PA and Rothwell
JC: The physiological basis of transcranial motor cortex
stimulation in conscious humans. Clin Neurophysiol. 115:255–266.
2004.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Chervyakov AV, Chernyavsky AY, Sinitsyn DO
and Piradov MA: Possoble mechanisms underlying the therapeutic
effects of transcranial magnetic stimulation. Front Hum Neurosci.
9(303)2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Maeda F, Keenan JP, Tormos JM, Topka H and
Pascual-Leone A: Modulation of corticospinal excitability by
repetitive transcranial magnetic stimulation. Clin Neurophysiol.
111:800–805. 2000.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Klomjai W, Lackmy-Vallée A, Roche N,
Pradat-Diehl P, Marchand-Pauvert V and Katz R: Repetitive
transcranial magnetic stimulation and transcranial direct current
stimulation in motor rehabilitation after stroke: An update. Ann
Phys Rehabil Med. 58:220–224. 2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Lefaucheur JP, André-Obadia N, Antal A,
Ayache SS, Baeken C, Benninger DH, Cantello RM, Cincotta M, de
Carvalho M, De Ridder D, et al: Evidence-based guidelines on the
therapeutic use of repetitive transcranial magnetic stimulation
(rTMS). Clin Neurophysiol. 125:2150–2206. 2014.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Rossini PM, Burke D, Chen R, Cohen LG,
Daskalakis Z, Di Iorio R, Di Lazzaro V, Ferreri F, Fitzgerald PB,
George MS, et al: Non-invasive electrical and magnetic stimulation
of the brain, spinal cord, roots and peripheral nerves: Basic
principles and procedures for routine clinical and research
application An updated report from an I.F.C.N. Committee. Clin
Neurophysiol. 126:1071–1107. 2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Phillips AL, Burr RL and Dunner DL: rTMS
effects in patients with co-morbid somatic pain and depressive mood
disorders. J Affect Disord. 241:411–416. 2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Kozel FA: Clinical repetitive transcranial
magnetic stimulation for posttraumatic stress disorder, generalized
anxiety disorder, and bipolar disorder. Psychiatr Clin North Am.
41:433–446. 2018.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Kimiskidis VK, Valentin A and Kälviäinen
R: Transcranial magnetic stimulation for thediagnosis and treatment
of epilepsy. Curr Opin Neurol. 27:236–241. 2014.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Randver R: Repetitive transcranial
magnetic stimulation of the dorsolateral prefrontal cortex to
alleviate depression and cognitive impairment associated with
Parkinson's disease: A review and clinical implications. J Neurol
Sci. 393:88–99. 2018.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Nardone R, Tezzon F, Höller Y, Golaszewski
S, Trinka E and Brigo F: Transcranial magnetic stimulation
(TMS)/repetitive TMS in mild cognitive impairment and Alzheimer's
disease. Acta Neurol Scand. 129:351–366. 2014.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Naro A, Russo M, Leo A, Bramanti P,
Quartarone A and Calabrò RS: A single session of repetitive
transcranial magnetic stimulation over the dorsolateral prefrontal
cortex in patients with unresponsive wakefulness syndrome:
Preliminary results. Neurorehabil Neural Repair. 29:603–613.
2015.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Liu P, Gao J, Pan S, Meng F, Pan G, Li J
and Luo B: Effects of High-frequency repetitive transcranial
magnetic stimulation on cerebral hemodynamics inpatients with
disorders of consciousness: A Sham-controlled study. Eur Neurol.
76:1–7. 2016.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Bai Y, Xia X, Kang J, Yin X, Yang Y, He J
and Li X: Evaluating the effect of repetitive transcranial magnetic
stimulation on disorders of consciousness by using TMS-EEG. Front
Neurosci. 10(473)2016.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Cincotta M, Giovannelli F, Chiaramonti R,
Bianco G, Godone M, Battista D, Cardinali C, Borgheresi A,
Sighinolfi A, D'Avanzo AM, et al: No effects of 20 Hz-rTMS of the
primary motor cortex in vegetative state: A randomised,
sham-controlled study. Cortex. 71:368–3676. 2015.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Hosono Y, Urushihara R, Harada M, Morita
N, Murase N, Kunikane Y, Shimazu H, Asanuma K, Uguisu H and Kaji R:
Comparison of monophasic versus biphasic stimulation in rTMS over
premotor cortex: SEP and SPECT studies. Clin Neurophysiol.
119:2538–2545. 2008.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Johnson KA, Baig M, Ramsey D, Lisanby SH,
Avery D, McDonald WM, Li X, Bernhardt ER, Haynor DR, Holtzheimer PE
III, et al: Prefrontal rTMS for treating depression: Location and
intensity results from the OPT-TMS Multi-site clinical trial. Brain
Stimul. 6:108–117. 2013.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Laureys S, Owen AM and Schiff ND: Brain
function in coma, vegetative state, and related disorders. Lancet
Neurol. 3:537–546. 2004.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Terao Y and Ugawa Y: Basic mechanisms of
TMS. J Clin Neurophysiol. 19:322–343. 2002.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Piccione F, Cavinato M, Manganotti P,
Formaggio E, Storti SF, Battistin L, Cagnin A, Tonin P and Dam M:
Behavioral and neurophysiological effects of repetitive
transcranial magnetic stimulation on the minimally conscious state:
A case study. Neurorehabil Neural Repair. 25:98–102.
2011.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Manganotti P, Formaggio E, Storti SF,
Fiaschi A, Battistin L, Tonin P, Piccione F and Cavinato M: Effect
of high-frequency repetitive transcranial magnetic stimulation on
brain excitability in severely Brain-injured patients in minimally
conscious or vegetative state. Brain Stimul. 6:913–921.
2013.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Wassermann EM and Lisanby SH: Therapeutic
application of repetitive transcranial magnetic stimulation: A
review. Clin Neurophysiol. 112:1367–1377. 2001.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Cavinato M, Iaia V and Piccione F:
Repeated sessions of Sub-threshold 20-Hz rTMS. Potential cumulative
effects in a Brain-injured patient. Clin Neurophysiol.
123:1893–1895. 2012.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Thibaut A, Bodien YG, Laureys S and
Giacino JT: Minimally conscious state ‘plus’: Diagnostic criteria
and relation to functional recovery. J Neurol. 267:1245–1254.
2020.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Bruno MA, Majerus S, Boly M,
Vanhaudenhuyse A, Schnakers C, Gosseries O, Boveroux P, Kirsch M,
Demertzi A, Bernard C, et al: Functional neuroanatomy underlying
the clinical subcategorization of minimally conscious state
patients. J Neurol. 259:1087–1098. 2012.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Annen J, Filippini MM, Bonin E, Cassol H,
Aubinet C, Carrière M, Gosseries O, Thibaut A, Barra A, Wolff A, et
al: Diagnostic accuracy of the CRS-R index in patients with
disorders of consciousness. Brain Inj. 33:1409–1412.
2019.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Lammi MH, Smith VH, Tate RL and Taylor CM:
The minimally conscious state and recovery potential: A follow-up
study 2 to 5 years after traumatic brain injury. Arch Phys Med
Rehabil. 86:746–754. 2005.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Bodien YG, Carlowicz CA, Chatelle C and
Giacino JT: Sensitivity and specificity of the coma recovery
Scale-revised total score in detection of conscious awareness. Arch
Phys Med Rehabil. 97:490–492.e1. 2016.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Cakar E, Akyuz G, Durmus O, Bayman L,
Yagci I, Karadag-Saygi E and Gunduz OH: The relationships of
Motor-evoked potentials to hand dexterity, motor function, and
spasticity in chronic stroke patients: A transcranial magnetic
stimulation study. Acta Neurol Belg. 116:481–487. 2016.PubMed/NCBI View Article : Google Scholar
|