Introduction
Myositis ossificans (MO) is a rare, benign ossifying
lesion characterized by focal formation of heterotopic bone and
cartilage in extraskeletal soft-tissue, typically affected areas
being the flexor muscles of the arm and the extensor muscles of the
thigh (1).
MO most commonly occurs in young adults, with both
males and females being affected equally (2). The etiology of MO is variable; in most
cases, no causative factor can be identified. However, ~60-70% of
cases occur as a result of a repetitive minor mechanical trauma and
other possible causative factors include ischemia, inflammation,
infections, burns, neuromuscular disorders, hemophilia or drug
abuse (1).
The MO localized form is usually a
well-circumscribed lesion that frequently complicates hematoma
formation of the muscles after sports trauma with contusions. The
widespread form of MO occurs in progressive fibrodysplasia
ossificans, a rare autosomal dominant mutation disease with ectopic
calcifications in several muscles beginning in childhood (3).
The main differential diagnosis of MO is conducted
with malignant tumors, such as osteosarcoma, soft-tissue sarcoma
(4) or periarticular ossifications
that usually occur in a context of central neurological pathologies
(5).
The diagnosis of MO is usually based on the
patient's history of trauma, clinical symptoms, on radiological
findings and histological examination, while laboratory test
results are usually normal (6).
Risk factors include male gender, past history of
having formed heterotopic bone, hypertrophic osteoarthritis,
ankylosing spondylitis, and diffuse idiopathic skeletal
hyperostosis (7).
The typical clinical presentation of MO is as a
significant inflammatory, rapidly growing, and painful muscular
tumor that within a few weeks, becomes a firm and often painful
mass which ossifies and becomes painless over 6-12 months.
When X-rays are performed two to three weeks after
MO onset and sometimes even later, the ossifications are often
missed because standard X-rays do not disclose any anomaly within
the early stages of MO (8). A
computerized tomography (CT) scan examination is more sensitive
than X-ray for ossification diagnosis and may also show a central
fatty metaplastic area (9).
Magnetic resonance imaging (MRI) is the preferred diagnostic tool
in the evaluation of a soft-tissue mass although the final
diagnosis is always histological (10). Ultrasonography may be a sensitive
imaging modality to early depict the acute phase in MO (10).
Case report
A 40-year-old man was admitted in the Emergency
County Hospital Craiova, Romania, Department of Physical and
Rehabilitation Medicine, suffering from weakness in motion of the
left fingers with a decrease in prehension for more than three
weeks, with no history of a specific acute injury, or
exercise-related trauma of the forearm. On physical examination, we
palpated a single tumor, slightly tender, hard, not
well-circumscribed, poorly mobile, painless lump on the volar side
of the left distal forearm. The patient's significant medical
history was negative and he reported no weight loss, malaise,
anorexia or fever. The usual laboratory findings were normal.
Written informed consent was obtained for patient participation and
the publication of all associated data and images.
The T2-weighted MRI showed a hyperintense area with
surrounding hypointense rim as a well-defined, inhomogeneous soft
tissue mass, surrounded by a frame of lower signal intensity,
signifying cortical calcification within the muscles of the flexor
compartment in the distal and volar part of the left forearm.
The patient underwent a surgical procedure during
which the tumor was extirpated completely and the specimen was sent
to histopathological examination. The patient had no neurological
deficits after surgical treatment and was discharged on the fifth
day after the surgery in good condition with the recommendation to
begin a rehabilitation program.
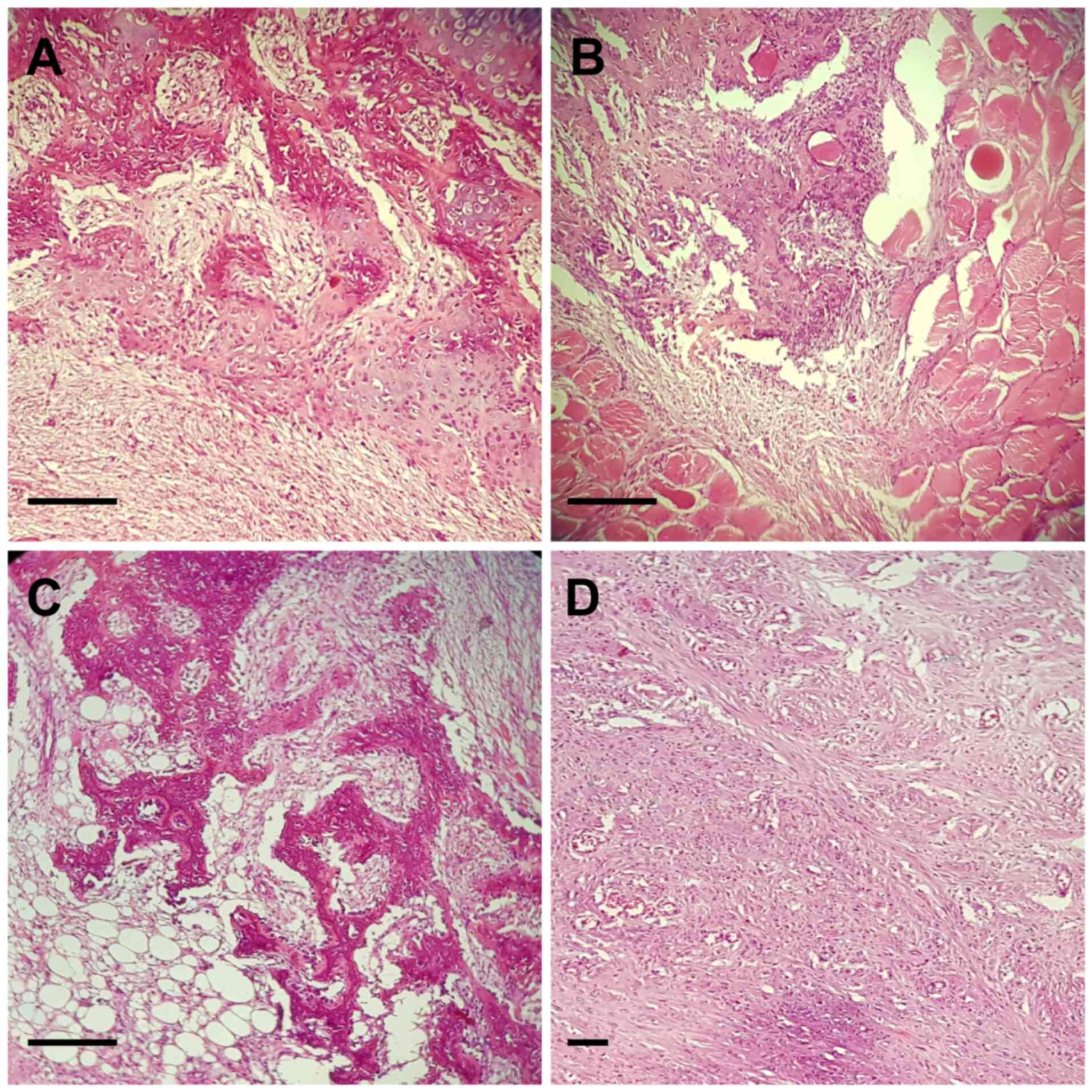
Tissue fragments were characterized by adipose
tissue and striated muscle fibers dissociated by irregular,
infiltrative area proliferating with a zonal pattern; the
intermediate zone with osteoblasts including immature osteoid
formations, surrounded by myxoid fibrous tissue; areas with
fusiform cells with fasciculated growing pattern; richly
vascularized areas; peripheral zone characterized of mature
cartilage. No necrotic areas were noted.
The histological and pathological findings suggested
the diagnosis of MO (Fig. 1A-D).
Immunohistochemistry (IHC) tests were recommended. Upon IHC
testing, cluster of differentiation (CD)34 was positive in vessels.
CD68 was positive in intralesional rare macrophages. Anti-α-smooth
muscle actin (α-SMA) antibodies were positive in intralesional area
and vessels. Anti-desmin antibodies were positive in striated
muscle tissue. The activity of Ki67 proliferative index was
positive in 1-3% of cells.
The patient started a program at the Physical
Medicine and Rehabilitation Outpatient Clinic. He followed a 30-min
exercise program performed five times/week, once daily, which
involved active range-of-motion, hand and finger flexion and
extension and ball resistance excercises. After 4 weeks of
supervised program, he began an unsupervised home exercise program,
15 min, twice a day, after he received detailed instructions
concerning the type of exercises, repetitions, intensity, training,
rest phases and demonstrations. After 12 weeks of rehabilitative
treatment, we assessed the wrist flexion and extension with a
goniometer and the Patient-Rated Wrist Evaluation (PRWE) a 15-item
questionnaire designed to measure wrist pain and disability in
activities of daily living (11).
Extension increased to 62.7% and flexion achieved 63.2%. Physical
therapy also increased hand function with better results to 12-week
PRWE.
Discussion
In the event a patient has no history of traumatic
injury, it is difficult to diagnose MO. In some cases, we must ask
the patient concerning such minor injuries such as strenuous
physical activity, heavy manual labor or weight lifting.
Most commonly MO affects the largest skeletal
muscles of the body, typically after a trauma, but the exact
pathophysiology is still poorly understand. We searched various MO
cases of different localizations and different traumatic and
nontraumatic etiology reported in the literature (Table I).
 | Table ILiterature review of myositis
ossificans: localization and etiology. |
Table I
Literature review of myositis
ossificans: localization and etiology.
| Author, year
(ref.) | Case no. | Age (years)/sex | Etiology | Localization |
|---|
| Goto et al,
1998(12) | 1 | 18/F | Repetitive minor
trauma | Tip of the thumb |
| Onen et al,
2019(13) | 1 | 5/M | Nontrauma | Lumbar region |
| Jayade et al,
2013(14) | 1 | 25/F | Nontrauma | Medial, lateral
pterygoid, and contralateral temporalis muscles |
| Wei et al,
2015(15) | 1 | 29/F | Long-term nape
massage | Serratus
anterior |
| Akahane et al,
2015(16) | 1 | 15/F | Nontrauma | Thenar region |
| Simmonds et
al, 2016(17) | 1 | 5 months/F | Nontrauma, nongenetic
mutation | Posterior
triangle |
| Lee et al,
2013(18) | 1 | 26/F | Acupuncture | Paraspinal muscles of
the neck |
| Raudenbush et
al, 2017(19) | 1 | 30/M | Upper cervical spine
fracture | Longus coli
muscle |
| Abdallah et
al, 2014(20) | 1 | 31/M | Nontrauma | Lumbar spine |
| Bultheel et
al, 2016(21) | 1 | 21/M | Nontrauma | Superior
anterolateral thigh |
| Yunus et al,
2016(22) | 1 | 36/F | Nontrauma | Hip |
| Dubuisson et
al, 2019(23) | 1 | 5 years, 6
months/M | Nontrauma | Neck region |
In 1998, Goto et al described a case of MO in
a 18-year-old woman in the tip of the left thumb after repetitive
minor trauma. The lesion arose in the subcutaneous fatty tissue in
the distal portion of the thumb and had a typical zonal pattern
(12). A 5-year-old pediatric
patient who developed scoliosis associated with nontraumatic MO in
the lumbar region was described by Onen et al (13). There has been no report of scoliosis
associated with myositis ossificans. Jayade et al (14) described a rare case of MO in medial
and lateral pterygoid and contralateral temporalis muscles in a
25-year-old woman without any obvious etiology, with no history of
trauma, tooth extraction, or infection.
In 2015, Wei et al (15) presented the case of a 29-year-old
woman with a rare form of MO of the serratus anterior that
developed due to long-term aggressive nape massage. The symptoms
disappeared after surgery. In addition, in 2015, the case of a
15-year-old Japanese girl with a 2-month history of a painful mass
in the right thenar region without previous trauma was presented by
Akahane et al. The diagnosis of MO was made on incisional
biopsy (16).
In 2016, Simmonds et al presented a case of a
5-month-old infant with a posterior neck mass suspicious for
neoplasia, which was treated with surgical resection and found to
be a non-traumatic, non-genetic form of MO (17). In 2013, Lee et al (18) reported a case of a 26-year-old woman
with MO in the paraspinal muscle of the neck after acupuncture. The
patient was conservatively treated through rest and analgesics and
the neck pain and swelling improved following several months.
Raudenbush et al (19) reported a case in 2017 of a
30-year-old male with upper cervical spine fracture occurring due
to high-energy trauma that resulted in MO of the longus coli
muscle. The patient was treated non-operatively for neck rotation
and MO with gradual improvement of symptoms. Abdallah et al
(20) presented the rare case of a
31-year-old Turkish man with MO not associated with trauma, with
severe low back pain and restriction of low back motion. A biopsy
was necessary to confirm diagnosis and the mass was surgically
excised from the patient.
An atypical presentation of MO in the superior
anterolateral thigh of a 21-year-old male is presented by Bultheel
et al (21) in 2016. This
case demonstrates that the diagnosis of MO can be more challenging
in the absence of a history of trauma. In 2016, Yunus et al
(22) presented a hip case of MO
without any trauma occurring in a 36-year-old female. Nontraumatic
MO is very rare in the literature. Dubuisson et al (23) in 2019 described a case of a 5 years
and 6 months old boy with a cervical tumor causing torticollis and
high suspicion of malignancy. The lesion was completely resected
and the biopsy established the diagnosis of MO.
Involvement of the forearm is very rare and only a
few cases have been reported to date. Say et al reported a
rare case of MO on the forearm in a 10-year-old girl (24) and Grebić et al reported a
case of MO in the forearm of a 48-year-old woman presenting
clinically as a mesenchymal tumor (25).
Early in the disease, the lesion is soft and
painful, and within a few weeks, the lesion becomes firm; and over
12 months it ossifies and becomes painless. Significant functional
deficits result in only 10-20% of patients (26).
MO passes through three characteristic phases. The
acute phase (first week) is when the proliferation is composed of
mesenchymal cells secreting a myxoid matrix, as well as fibroblasts
exhibiting numerous mitoses, which gives the mass a
pseudo-fibrosarcomatous appearance. The subacute phase (next two
weeks) is when histologically fibroblasts differentiate into
osteoblasts and secrete an osteoid matrix at the periphery of the
initial myxoid zone, giving it a pseudo-osteosarcomatous
appearance. Finally, the maturation phase (2-5 weeks) is when a
histological diagnosis can accurately be carried out (27).
Due to the presence of bone formation as well as a
similar epidemiology, osteosarcoma needs to be excluded. It is very
important to identify the early stage of MO using imaging. However,
early in the disease course, radiographs are often negative and a
biopsy conducted at the early stage of MO may lead to a wrong
diagnosis of sarcoma. On the other hand, when biopsy is delayed, a
true sarcoma may be missed. Computerized axial tomography optimally
identifies the typical patterns of this disease, including the
separation of the mass from the adjacent cortex and the decreased
attenuation of the center of the mass (9).
MRI is the elected investigation for evaluating
soft-tissue lesions with the classic finding for MO, a peripheral
rim enhancement that correlates with calcification and ossification
(28). MO can disappear
spontaneously, the treatment is usually reserved for symptomatic
lesions: Rest, ice, compression, nonsteroidal anti-inflammatory
drug (NSAID) therapy could be initiated leading to clinical
improvement and concomitant decrease of the soft tissue swelling.
The specialty literature recognized that NSAIDs may stop the
evolutionary process of MO (29).
Surgical excision is generally reserved for
symptomatic MO lesions. However, since recurrence has been
reported, excision with clear resection margins is recommended
(30). When symptoms are not
associated with trauma, the diagnosis of MO is challenging. The MRI
findings may suggest the mesenchymal tumor like malignant fibrous
histiocytoma.
Finally, diagnosis is always established by
histopathological examination. It may be difficult with
histological evidence alone to differentiate an MO from a sarcoma;
therefore, correlation of the clinical and radiological findings is
important in such cases. There is no need for further therapy once
the diagnosis of MO has been established by excision. MO is a rare
clinical entity and understanding its etiology and pathophysiology
can save the patient from the anxiety of a suspected neoplasm.
In conclusion, particularities of our case report is
the diagnosis of MO in middle aged patients, which is very rare, as
MO commonly occurs in young males. Our patient had no history of
acute injury or repetitive minor trauma of the forearm, thus the
aetiology still remains unclear. In addition, involvement of the
forearm muscles is rare. We found in our literature search only a
few cases reported. Treatment is usually conservative but, due to
the limited strength and range of motion of the left hand, the
tumor was extirpated and the diagnosis of MO was made by biopsy. In
future research, the molecular mechanisms of this rare disease must
be discovered and gene therapy may be used in the early stages as a
treatment strategy.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Further information regarding the case and the
review may be requested from the corresponding author upon
reasonable request.
Authors' contributions
DR performed the surgical procedure. SP, VP, RRM,
RP, and DM carried out the patient investigation and SP, VP, RP,
and MB data curation. SP, VP, DR, and DM carried out the writing
and original draft preparation. VP, RRM, RP, DM and SP performed
the literature data review and SP and VP finally reviewed the
manuscript. All authors have read and agreed to the published
version of the manuscript.
Ethics approval and consent to
participate
The case report was approved by the local
institutional Ethics Committee of the University of Medicine and
Pharmacy of Craiova.
Patient consent for publication
Written informed consent was obtained for patient
participation and the publication of all associated data and
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Walczak BE, Johnson CN and Howe BM:
Myositis ossificans. J Am Acad Orthop Surg. 23:612–622.
2015.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Li PF, Lin ZL and Pang ZH: Non-traumatic
myositis ossificans circumscripta at elbow joint in a 9-year old
child. Chin J Traumatol. 19:122–124. 2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Bridges AJ, Hsu KC, Singh A, Churchill R
and Miles J: Fibrodysplasia (myositis) ossificans progressiva.
Semin Arthritis Rheum. 24:155–164. 1994.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Mahale YJ, Vyawahare CS, Dravid NV, Upase
A and Rathi R: A rare case of non traumatic myositis ossificans
circumscripta. J Orthop Case Rep. 5:15–17. 2015.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Olsen KM and Chew FS: Tumoral calcinosis:
Pearls, polemics, and alternative possibilities. Radiographics.
26:871–885. 2006.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Man SC, Schnell CN, Fufezan O and Mihut G:
Myositis ossificans traumatica of the neck-a pediatric case.
Maedica (Buchar). 6:128–131. 2011.PubMed/NCBI
|
|
7
|
Aneiros-Fernandez J, Caba-Molina M,
Arias-Santiago S, Ovalle F, Hernandez-Cortes P and Aneiros-Cachaza
J: Myositis ossificans circumscripta without history of trauma. J
Clin Med Res. 2:142–144. 2010.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Goldman AB: Myositis ossificans
circumscripta: A benign lesion with a malignant differential
diagnosis. AJR Am J Roentgenol. 126:32–40. 1976.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Amendola MA, Glazer GM, Agha FP, Francis
IR, Weatherbee L and Martel W: Myositis ossificans circumscripta:
Computed tomographic diagnosis. Radiology. 149:775–779.
1983.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Wang H, Nie P, Li Y, Hou F, Dong C, Huang
Y and Hao D: MRI findings of early myositis ossificans without
calcification or ossification. Biomed Res Int.
2018(4186324)2018.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Kleinlugtenbelt YV, Krol RG, Bhandari M,
Goslings JC, Poolman RW and Scholtes VA: Are the patient-rated
wrist evaluation (PRWE) and the disabilities of the arm, shoulder
and hand (DASH) questionnaire used in distal radial fractures truly
valid and reliable? Bone Joint Res. 7:36–45. 2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Goto H, Hatori M, Kokubun S and Makino M:
Myositis Ossificans in the tip of the thumb: A case report. Tohoku
J Exp Med. 184:67–72. 1998.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Onen MR, Varol E, Tosun MI and Naderi S:
Nontraumatic myositis ossificans as an uncommon cause of scoliosis:
Case report and review of the literature. World Neurosurg.
123:208–211. 2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Jayade B, Adirajaiah S, Vadera H,
Kundalaswamy G, Sattur AP and Kalkur C: Myositis ossificans in
medial, lateral pterygoid, and contralateral temporalis muscles: A
rare case report. Oral Surg Oral Med Oral Pathol Oral Radiol.
116:E261–E266. 2013.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Wei J, Jia Y and Liang B: Myositis
ossificans of the serratus anterior as a rare complication of
massage: A case report. J Med Case Rep. 9(143)2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Akahane T, Mori N and Nakatsuchi Y:
Myositis ossificans occupying the thenar region: A case report. J
Med Case Rep. 9(105)2015.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Simmonds J, Taki N, Chilton I and
Vecchiotti M: A rare case of pediatric nontraumatic myositis
ossificans in the posterior triangle. Int J Pediatr
Otorhinolaryngol. 84:116–118. 2016.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Lee DG, Lee SH, Hwanga SW, Kim ES and Eoh
W: Myositis ossificans in the paraspinal muscles of the neck after
acupuncture: A case report. Spine J. 13:e9–e12. 2013.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Raudenbush BL, McCalla D, Mesfin A and
Rubery PT: Myositis ossificans of the longus coli muscle following
cervical spine fracture-dislocation. J Spinal Cord Med. 40:372–376.
2017.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Abdallah A, Gokcedag A, Ofluoglu AE and
Emel E: Non-traumatic myositis ossificans in the lumbar Spine. Am J
Case Rep. 15:421–425. 2014.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Bultheel M, Kirby JH, Viljoen JT and
Viviers PL: An atypical presentation of myositis ossificans. SA J
Sports Med. 28:33–34. 2016.
|
|
22
|
Yunus O, Ozcan MS, Sezer HB, Kilinc BE and
Eren OT: Nontraumatic myositis ossificans of hip: A case
presentation. Case Rep Orthop. 2016(1982656)2016.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Dubuisson A, Lombard A and Otto B:
Pseudomalignant myositis ossificans of the neck in a child: Case
report and review of the literature. World Neurosurg. 130:95–97.
2019.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Say F, Coskun S, Buelbuel M and Alici O:
Myositis ossificans on the forearm in a 10-year-old girl. J Pediatr
Orthop B. 24:223–225. 2015.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Grebić D, Pozderac I, Milas I and Eljuga
D: A sporadic case of myositis ossificans of the forearm presenting
clinically as mesenchimal tumor. Medicina fluminensis. 53:225–230.
2017.
|
|
26
|
Rothwell AG: Quadriceps hematoma: A
prospective clinical study. Clin Orthop Relat Res. 97–103.
1982.PubMed/NCBI
|
|
27
|
McCarthy EF and Sundaram M: Heterotopic
ossification: A review. Skeletal Radiol. 34:609–619.
2005.PubMed/NCBI View Article : Google Scholar
|
|
28
|
De Smet AA, Norris MA and Fisher DR:
Magnetic resonance imaging of myositis ossificans: Analysis of
seven cases. Skeletal Radiol. 21:503–507. 1992.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Mann D and McCormack B: Commentary:
Myositis ossificans. CJEM. 1(199)1999.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Mavrogenis AF, Soucacos PN and
Papagelopoulos PJ: Heterotopic ossification revisited. Orthopedics.
34(177)2011.PubMed/NCBI View Article : Google Scholar
|