Introduction
Glioma is the most common tumor type in the central
nervous system, and glioblastoma multiforme (GBM; grade IV
according to the the 2016 WHO Classification of Glioma) is the most
lethal, with a median survival of 14.6 months (1-4).
The median recurrence period of GBM is 6-12 months, and that of
anaplastic glioma (grade III) is 18-36 months (5). Studies have shown that the malignancy
and invasiveness of glioma is increased after recurrence (4,6).
Considering that the recurrence and prognosis of malignant gliomas
largely depends on the extent of invasion of tumors into normal
brain parenchyma, brain radiotherapy with enlarged field is the
recommended treatment to target the maximum number of tumor cells
possible. However, clinical studies show that, even if patients
with glioma received extended resection and field radiotherapy,
~80% of malignant glioma recurrence is located within 2-3 cm of the
resected margin (7,8).
In addition to residual tumor cells and
radioresistance, the tumor microenvironment also plays an important
role in tumor recurrence (9). There
are numerous different stromal cells aside from tumor cells in the
tumor lesions, including include endothelial cells as well as
inflammatory cells, that constitute tumor microenvironment
(10). Recently, more and more
studies have revealed that the tumor microenvironment plays an
important role in the process of tumorigenesis, tumor development,
chemo- and radio-resistance and tumor recurrence (11-15).
However, until now, the underlying mechanisms for these processes
in glioma were unclear.
The C-C motif chemokine ligand (CCL)2, one of the
most important members of the chemokine family of proteins, was the
first C family chemokine to be cloned and identified (16). CCL2 is highly expressed in several
human central nervous system tumors, such as glioma, meningioma and
Schwannoma (17-19).
Production of CCL2 in tumor microenvironments can be stimulated by
IL-1β and TNF-α (17). In normal
brain tissues, CCL2 is primarily secreted by endothelial cells,
fibroblasts, microglia, astrocytes and monocytes and its expression
is relatively low (17). CCL2
functions by binding to the CC receptor (R)2, leading to
accelerated Ca2+ influx, cAMP inhibition, and
phospholipase C and phosphoinositol-3 kinase activation (20). The activation of CCL2/CCR2 signaling
recruits monocytes from the bloodstream through the vascular
endothelium and regulates the routine immunological surveillance of
brain tissues (21).
Several studies have revealed that CCL2/CCR2
signaling is a promising target in patients with tumors and
inflammation (16,22-24).
However, little is known on the role of CCL2/CCR2 in tumor
recurrence, especially after radiotherapy. Our previous study
proposed that after radiotherapy, irradiated brain tissues promote
the ability of tumor cells to invade and metastasize by secreting
cytokines and proteases, which may partly result in the recurrence
and progression of glioma (25).
The present study investigated the expression of CCL2 and CCR2 in
primary and recurrent glioma and analyzed the association with
glioma relapse. The difference in the expression of CCL2/CCR2
between post-radiation and non-radiation recurrent glioma was also
compared.
Materials and methods
Patients and tissue specimens
The records of 80 patients with glioma who underwent
two glioma resections in Qilu Hospital of Shandong University
(Jinan, China) between January 1995 and December 2015 were
analyzed. The tissue specimens were evaluated by two pathologists
experienced in glioma pathology. All specimens were collected
retrospectively from primary tumors and their corresponding
recurrent tumors. All patients were treated according to the
guidelines used in our institutions. The present study complied
with national regulations, and was approved by The Institutional
Ethics and Investigation Committee of Qilu Hospital, Shandong
University [approval no. KYLL-2015(KS)-068].
The inclusion criteria were as follows: i) All the
cases were solitary lesions and pathologically diagnosed as glioma
(2016 WHO classification of tumors of the central nervous system
(3)); ii) both the first and second
operations were performed in Qilu Hospital; iii) cranial MRI was
performed after the first operation with detection of enhanced new
lesions, or >25% larger than before, iv) the expected survival
time was >8 weeks and v) the Karnofsky score (KPS) was
>60(26). Patients with
irradiation necrosis were excluded. According to whether the
patients received radiotherapy after the first operation, they were
divided into two groups: Post-radiation group (first operation,
radiotherapy, recurrence, second operation) and non-radiation group
(first operation, recurrence, second operation). 33 cases of
primary (de novo) and 24 cases of secondary GBM (progressed
from low-grade or anaplastic glioma) were included in this study.
In addition, 10 non-tumor brain specimens were collected from
patients with brain trauma who underwent partial resection of
normal brain as decompression treatment for severe head injuries
(Qilu Hospital of Shandong University) between January 2013 and
December 2015. The clinicopathological characteristics of patients
are listed in Table SI. Informed
consent was provided by all individual participants included in the
study (consent of patients <18 years old was provided by their
guardians). Follow-up was performed over the phone and the deadline
was April 2019. The time between surgery and disease recurrence was
defined as the disease-free interval (DFI). The overall survival
(OS) time of the primary tumors was calculated from the date of the
operation following primary diagnosis to the date of death or last
follow-up.
Immunohistochemistry
Paraffin sections (4 µm) were deparaffinized with
xylene and ethanol gradient (100, 95 and 80%) methods at 65˚C for
30 h and treated with 3% hydrogen peroxide for 10 min to block the
endogenous peroxidase, and then microwaved (98˚C) in 10 mM sodium
citrate buffer (pH 6.0) to unmask the epitopes. After being blocked
with goat serum (Beyotime Institute of Biotechnology) for 30 min at
37˚C, the sections were incubated with the rabbit anti-CCL2
antibody [1:100 in buffer (1% BSA, 99% PBS, pH 7.4); cat. no.
ab73680] and the rabbit anti-CCR2 antibody [1:250 in buffer (0.75%
glycine, 1.21% Tris, 10% glycerol) cat. no. ab155321] (both Abcam,)
overnight at 4˚C. At the same time, the controls were treated
similarly, except the primary antibody was replaced by PBS. After
being washed three times with PBS, the sections were developed with
DAB for ~1 min and counterstained with hematoxylin for 30 sec at
room temperature. At last, the sections were examined and images
were captured using a light microscope equipped with a digital
camera (DM2000; Leica Microsystems GmbH) and stained cells were
manually counted in five randomly selected fields of vision
(original magnification, x400). Immunostaining intensity higher
compared with the average background could be observed in the
cytoplasmic staining. The mean number of cells expressing CCL2 and
CCR2 was recorded. Immunohistochemically staining results were
interpreted independently by two pathologists who were blinded to
the clinical parameters of the individual cases. The scoring method
used was described by Li et al (27) to determine positive CCL2 and CCR2
staining, The score of staining intensity of absent, low, medium
and high was quantified as 0, 1, 2 and 3, respectively. The score
of extent of staining (0, ≤25, ≤50 and ≤100%) was also classified
as 0, 1, 2 and 3, respectively. The product of staining intensity
and extent of staining was multiplied as the immunoreactive score
(IRS), which ranged from 0 to 9. Then, the scores were divided into
four groups: 0, 1-2, 3-5 and 6-9, corresponding to the absent, low,
medium and high scores, respectively. Based on IRS, slides with
scores of ≥3 were classified as positive expression, while slides
with scores <3 were classified as absent expression.
Statistical analysis
The independent Student's t-test was used to analyze
the continuous variables. The inconsistency rate for CCL2 is
(21+4)/80=31.25%, and inconsistency rate for CCR2 is
(26+6)/80=40.00%. Qualitative data were analyzed using
χ2 tests, including grade and location, and Fisher's
exact test was used when n<5 as appropriate. McNemar's test was
used to compare changes in grade and protein expression between
primary diagnosis and recurrence. Spearman's rank correlation
method was used for correlation analysis. The total survival curve
was drawn by Kaplan-Meier survival function, and log rank tests
were used for statistical analysis. When there was cross-over of
survival curves, a weighted test, such as ABS permutation, was used
instead. In addition, Cox multivariate regression analysis was
performed to determine independent prognostic factors. P<0.05
was considered to indicate a statistically significant difference.
All calculations were performed using SPSS version 17.0 (SPSS
Inc.).
Results
Patient distribution, survival and
recurrent status
To explore the expression pattern of CCL2/CCR2 in
glioma, protein expression was analyzed and clinical data were
obtained. In total, 80 patients with glioma were included in the
present study. Overall, two patients were lost during follow-up and
no patients were still alive on the last day of follow-up. The
status of these patients with respect to age, sex, adjuvant
radiotherapy, histological grade, location of tumors, DFI and OS is
listed in Table SI. The average
age was 42.90 years (range, 9-77 years). Mean DFI and OS time were
30.16 months (range, 2.10-105.80) and 60.19 months (range,
6.00-169.20), respectively. There was a significant difference in
tumor grade (P=1.097x10-5) when between primary and
recurrent gliomas (Table I), which
showed increased malignancy after tumor relapse. Among the 49
patients with high tumor grade in the first operation phase, only
one patient (2.04%) developed low grade recurrent tumors. Non-brain
tumor specimens from 10 patients with brain trauma were used as
control, the characteristics of whom are presented in Table SII.
 | Table IInconsistency rate of tumor grade and
protein expressions of CCL2/CCR2 between primary and recurrent
astrocytoma. |
Table I
Inconsistency rate of tumor grade and
protein expressions of CCL2/CCR2 between primary and recurrent
astrocytoma.
| | Recurrent
tumor |
|---|
| | Grade | CCL2 | CCR2 |
|---|
| Primary tumor | Low | High | Negative | Positive | Negative | Positive |
|---|
| Low/Negative, n
(%) | 10 (12.50) | 21 (26.25) | 8 (10.00) | 21 (26.25) | 15 (18.75) | 26 (32.50) |
| High/Positive, n
(%) | 1 (1.25) | 48 (60.00) | 4 (5.00) | 47 (58.75) | 6 (7.50) | 33 (41.25) |
| Total change, n
(%) | 22 (27.50) | | 25 (31.25) | | 32 (40.00) | |
| P-value |
1.097x10-5 | | 0.001 | | 0.001 | |
Inconsistency rate of protein
expression of CCL2/CCR2 between primary and recurrent gliomas
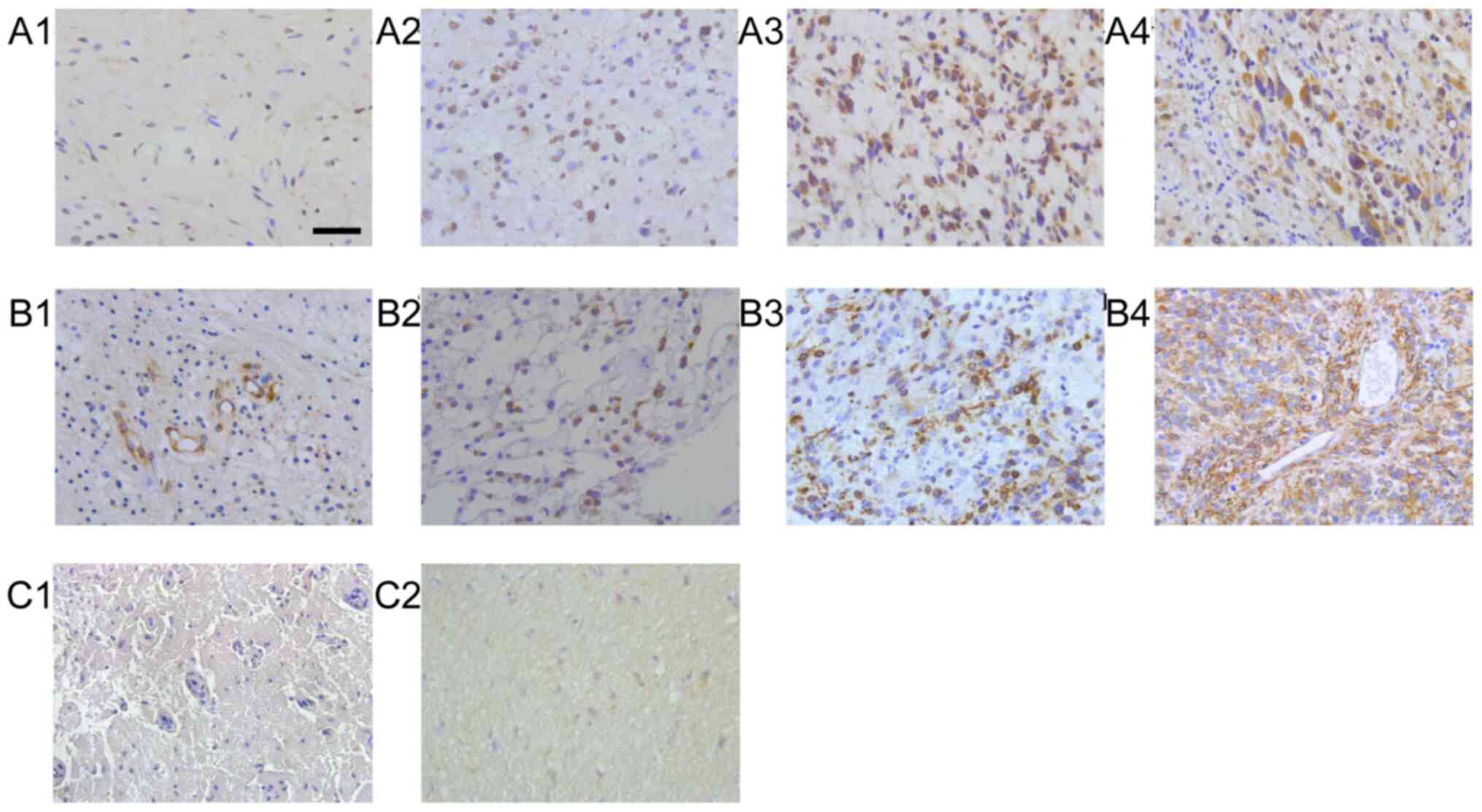
Protein expression of CCL2 and CCR2 in patients with
glioma and brain trauma are presented in Fig. 1. The immunoreactivity of all
proteins studied was mainly localized in tumor cells, but a
considerable proportion of cases were localized in stromal cells.
The inconsistency rate of CCL2/CCR2 between primary and recurrent
tumors was 31.25 and 40.00%, respectively (Table I). The frequency of CCL2 and CCR2
expression was higher in the recurrent gliomas (85.00 vs. 63.75%
for CCL2, P=0.001; 73.7% vs. 48.75% for CCR, P=0.001) compared with
in the primary group (Table I).
Correlation between tumor grade and
protein expression of CCL2/CCR2
CCL2 and CCR2 showed significant positive
correlations with tumor grade in the recurrent tumors
(P=4.014x10-5 and P=9.763x10-5,
respectively), as well as in the primary tumors (P=0.006 and
P=0.019, respectively; Table
SIII).
Effect of radiotherapy on CCL2/CCR2
protein expression
There was no significant difference in the baseline
of clinical characteristics between glioma with and without
radiotherapy after the first operation (Table II). No difference was observed
between irradiation and histological grade, location of tumor or
CCL2 protein expression during the second operation (P=0.433,
P=0.302 and P=0.108, respectively; Table III). However, irradiation was
significantly associated with CCR2 expression in recurrent glioma
(P=0.020; Table III). It was
suggested that irradiation-induced expression of CCL2 is transient,
while irradiation-induced expression of CCR2 is lasting.
| Table IIBaseline of clinical characteristics
between patients with glioma with and without radiotherapy during
the first operation. |
Table II
Baseline of clinical characteristics
between patients with glioma with and without radiotherapy during
the first operation.
| | Radiotherapy | |
|---|
|
Characteristics | No | Yes | P-value |
|---|
| Mean age ± SD,
years | 42.76±13.80 | 42.98±13.22 | 0.944 |
| Sex, n (%) | | | 0.227 |
|
Male | 13 (16.25) | 30 (37.50) | |
|
Female | 16 (20.00) | 21 (26.25) | |
| Location of tumor
[n (%)] | | | 0.216a |
|
Frontal
lobe | 15 (18.75) | 29 (36.25) | |
|
Temporal
lobe | 4 (5.00) | 13 (16.25) | |
|
Parietal
lobe | 4 (5.00) | 4 (5.00) | |
|
Occipital
lobe | 1 (1.25) | 3 (3.75) | |
|
Others | 5 (6.25) | 2 (2.50) | |
| Grade [n (%)] | | | 0.148a |
|
I | 3 (3.75) | 4 (5.00) | |
|
II | 13 (16.25) | 11 (13.75) | |
|
III | 4 (5.00) | 12 (15.00) | |
|
IV | 9 (11.25) | 24 (30.00) | |
| Expression of CCL2,
n (%) | | | 0.472 |
|
Negative | 12 (15.00) | 17 (21.25) | |
|
Positive | 17 (21.25) | 34 (42.50) | |
| Expression of CCR2,
n (%) | | | |
|
Negative | 13 (16.25) | 28 (35.00) | 0.386 |
|
Positive | 16 (20.00) | 23 (28.75) | |
| Table IIIEffect of radiotherapy on markers of
recurrent astrocytoma. |
Table III
Effect of radiotherapy on markers of
recurrent astrocytoma.
| | Radiotherapy | |
|---|
|
Characteristics | No | Yes | χ2 | P-value |
|---|
| Histological grade,
n (%)a | | | 2.750 | 0.433 |
|
I | 1 (1.25) | 1 (1.25) | | |
|
II | 5 (6.25) | 4 (5.00) | | |
|
III | 4 (5.00) | 12 (15.00) | | |
|
IV | 19 (23.75) | 34 (42.50) | | |
| Location of tumor,
n (%)a | | | 4.747 | 0.302 |
|
Frontal
lobe | 17 (21.25) | 29 (36.25) | | |
|
Temporal
lobe | 4 (5.00) | 13 (16.25) | | |
|
Parietal
lobe | 3 (3.75) | 1 (1.25) | | |
|
Occipital
lobe | 1 (1.25) | 4 (5.00) | | |
|
Others | 4 (5.00) | 4 (5.00) | | |
| Expression of CCL2,
n (%)a | | | - | 0.108 |
|
Negative | 7 (8.75) | 5 (6.25) | | |
|
Positive | 22 (27.50) | 46 (57.50) | | |
| Expression of CCR2,
n (%) | | | 5.379 | 0.020F |
|
Negative | 12 (15.00) | 9 (11.25) | | |
|
Positive | 17 (21.25) | 42 (52.50) | | |
Difference of CCL2/CCR2 protein
expression between primary and secondary GBM
GBM can be divided into de novo (primary GBM)
or progression from low-grade or anaplastic glioma (secondary GBM)
(3). Hence, the present study
investigated the difference of CCL2/CCR2 protein expression between
33 cases of primary and 24 cases of secondary GBM. There was no
significant difference in the baseline of clinical characteristics
between primary GBM during the first operation and secondary GBM
during the second operation (Table
IV). In addition, no significant difference was observed for
the protein expression of CCL2 and CCR2 between primary and
secondary GBM (P=0.214 and P=0.346, respectively).
| Table IVDifference of CCL2/CCR2 expression
between primary and secondary glioblastoma. |
Table IV
Difference of CCL2/CCR2 expression
between primary and secondary glioblastoma.
|
Characteristics | Primary
glioblastoma | Secondary
glioblastoma | P-value |
|---|
| Mean age ± SD,
yearsa | 46.21±15.03 | 45.13±8.54 | 0.731 |
| Sex, n (%) | | | 0.157 |
|
Male | 20 (60.61) | 10 (41.67) | |
|
Female | 13 (39.39) | 14 (58.33) | |
| Location of tumor,
n (%)b | | | 0.196 |
|
Frontal
lobe | 16 (48.49) | 15 (62.50) | |
|
Temporal
lobe | 6 (18.18) | 6 (25.00) | |
|
Parietal
lobe | 5 (15.15) | 2 (8.33) | |
|
Occipital
lobe | 3 (9.09) | 0 (0.00) | |
|
Others | 3 (9.09) | 1 (4.17) | |
| Expression of CCL2,
nb | | | 0.214 |
|
Negative | 4 (12.12) | 0 (0.00) | |
|
Positive | 29 (87.88) | 24 (100.00) | |
| Expression of CCR2,
nb | | | |
|
Negative | 9 (27.27) | 4 (16.67) | 0.346 |
|
Positive | 24 (72.73) | 20 (83.33) | |
Impact of CCL2/CCR2 protein expression
on patient survival
Kaplan-Meier analysis and results of analyses for
DFI are shown in Table V. It was
revealed that age, tumor grade and the protein expression of
CCL2/CCR2 were significant prognostic factors in gliomas using
Kaplan-Meier analysis (Fig. S1).
To exclude possible confounding factors, multivariate Cox analysis
was used to predict DFI considering multiple variables
simultaneously. After adjusting for sex, radiotherapy and location
of tumors, the significant prognostic factors for DFI were age
[hazard ratio (HR) =1.846; 95% confidence interval (CI),
1.046-3.257; P=0.034), tumor grade (HR =2.247; 95% CI, 1.301-3.882;
P=0.004) and expression of CCL2 (HR=1.663; 95% CI, 1.012-2.731;
P=0.045) (Table V).
| Table VPrognostic values of the
clinicopathological parameters and markers. |
Table V
Prognostic values of the
clinicopathological parameters and markers.
| | DFI |
|---|
| | Mann-Whitney U | Cox |
|---|
|
Characteristics | Survival analysis
P-value | Z | P-value | HR | 95% CI | P-value |
|---|
| Age, years |
4.186x10-4a | -2.739 | 0.006 | 1.846 | 1.046-3.257 | 0.034 |
|
<50 | | | | | | |
|
≥50 | | | | | | |
| Sex | 0.594a | | | | | |
|
Male | | | | | | |
|
Female | | | | | | |
| Radiotherapy | 0.526a | | | | | |
|
Yes | | | | | | |
|
No | | | | | | |
| Grade |
7.263x10-6a | -4.079 |
4.500x10-5 | 2.247 | 1.301-3.882 | 0.004 |
|
I-II | | | | | | |
|
III-IV | | | | | | |
| Location | 0.359a | | | | | |
|
Frontal | | | | | | |
|
Temporal | | | | | | |
|
Parietal | | | | | | |
|
Occipital | | | | | | |
|
Others | | | | | | |
| CCL2 | 0.001a | -3.898 |
9.700x10-5 | 1.663 | 1.012-2.731 | 0.045 |
|
Negative | | | | | | |
|
Positive | | | | | | |
| CCR2 | 0.026b | -2.224 | 0.026 | 1.133 | 0.694-1.849 | 0.618 |
|
Negative | | | | | | |
|
Positive | | | | | | |
Using the Kaplan-Meier survival analysis model, it
was demonstrated that age, tumor grade and protein expression of
CCL2/CCR2 were significant prognostic factors for OS in gliomas
(Fig. S2 and Table SIV). In Cox multivariate modeling,
after adjusting for sex, radiotherapy and location of tumors,
expression of CCL2 and CCR2 remained significant prognostic factors
for OS (HR=1.879; 95% CI, 1.092-3.236; P=0.023 and HR =1.744; 95%
CI, 1.033-2.945, P=0.037, respectively; Table SIV), as well as age and tumor grade
(Table SIV).
Discussion
As one of the most important methods in the
treatment of glioma, radiotherapy has been used in the clinic for
over a century (28). But
recurrence still occurs, even after whole brain radiotherapy. An
increasing number of studies have shown that irradiation promotes
malignant behaviors, including increased proliferation, invasion
and migration (4,29).
Recently, the tumor microenvironment has attracted
more and more attention regarding research into tumorigenesis,
tumor development, antitumor resistance and tumor relapse (11-13).
Morganti et al reported that single high-dose (10 Gy) γ-ray
irradiation altered the microenvironment of brain tissue and
induced increased infiltration of peripheral CCR2+
macrophages (30). A further study
showed that CCL2 secreted by glioma cells induced microglia to
infiltrate into tumor tissues, while microglia also secreted CCL2,
which resulted in an amplifying effect for the recruitment of
microglia (31). CCL2 is
upregulated at both the mRNA and protein levels in the serum and
tumor tissues of patients with glioma (21).
CCR2, the main receptor of CCL2, is overexpressed in
most malignant glioma cells (20).
The present study showed that there was significant positive
correlation between CCL2/CCR2 and tumor grade in primary and
recurrent glioma. CCL2 attracted microglia/macrophages, T
lymphocytes, basophils, NK cells and hematopoietic progenitor cells
to migrate and infiltrate into tumor tissues, all of which
participate in a variety of tumor pathological processes, such as
stimulating tumor proliferation and migration (32). CCL2 induces microglia/macrophages
migration into glioma and indirectly induces the invasion and
migration by secreting cytokines (33). An in vitro co-culture study
showed that high expression of CCR2 in tumor cells directly
promotes perineural invasion, a phenomenon in which cancer cells,
especially prostate cancer, invaded the nerves and then reached
other sites via the nervous system (34). Zhu et al reported that
intraperitoneal injection of monoclonal antibodies against CCL2
significantly prolonged the survival of glioma xenograft mice
(35). Therefore, CCL2/CCR2
signaling is closely associated with the progression of glioma.
GBM, the most lethal type of glioma, is classified
into primary and secondary GBM (3).
The two subgroups are histologically indistinguishable; however,
more and more studies have distinguished between these using
genetic, epigenetic, and molecular profiles (36,37).
Telomerase reverse transcriptase promoter mutation, PTEN tumor
suppressor gene mutation and high-level gene amplification of EGFR
are hallmarks in primary GBMs, while mutations of isocitrate
dehydrogenase, mitochondrial 1/2, TP53 and transcriptional
regulator ATRX are more common in secondary GBMs (38). However, until now, little was known
about the difference of chemokines in primary and secondary GBM.
The present study analyzed the expression of CCL2/CCR2 in primary
and secondary GBM. However, the results revealed that there was no
significant difference.
Targeting CCL2/CCR2 has been shown to be effective
in tumor chemosensitization [18], but whether it has a
radiosensitizing effect is largely unknown. Recently, more and more
studies reported that CCL2/CCR2 is involved in irradiation-induced
damage of brain tissues and irradiation-induced malignant
behaviors, such as increased migration and invasion (39-41).
Therefore, the combination of radiotherapy and inhibition of
CCL2/CCR2 may be promising to improve the prognosis of patients
with glioma.
Overall, the present study revealed a significant
correlation between CCL2 and CCR2 expression and glioma tumor
grade. Furthermore, irradiation affected the expression of CCR2,
but not CCL2. Hence, CCL2/CCR2 has potential as therapeutic target
for patients with glioma.
Supplementary Material
Kaplan-Meier analysis of correlation
between DFI and the clinicopathological parameters and markers. (A)
age, (B) tumor grade, (C) positive expression of CCL2 and (D)
positive expression of CCR2. DFI, disease-free interval; Cum,
cumulative survival; C-C motif chemokine ligand; CCR, C-C motif
receptor.
Kaplan-Meier analysis of correlation
between OS and the clinicopathological parameters and markers. (A)
age, (B) tumor grade, (C) positive expression of CCL2 and (D)
positive expression of CCR2. OS overall survival; Cum, cumulative
survival; C-C motif chemokine ligand; CCR, C-C motif receptor.
Baseline characteristics of 80
patients with astrocytoma.
Clinical characteristics of the
control group.
Correlation between tumor grade and
CCL2/CCR2.
Prognostic values of the
clinicopathological parameters and markers.
Acknowledgements
The authors would like to thank Mr. Jian Wang, Mr.
Bin Huang and Mrs. Anjing Chen (Brain Science Research Institute,
Key Laboratory of Brain Functional Remodeling, Shandong University,
Jinan, Shandong, P.R. China) for their excellent technical
assistance.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
WZ and ZJ conceived the study and designed most of
the experiments. WZ and XZ interpreted the data and wrote the
manuscript. QY performed most of the statistical analyses and
generated all graphs and tables. JZ had primary responsibility for
patient characterization and management. JZ, LM and WZ performed
the immunohistological analysis. All authors discussed the results
and approved the final submitted version. All authors read and
approved the final manuscript. WZ and QY confirmed the authenticity
of all the raw data.
Ethics approval and consent to
participate
All procedures performed were in accordance with the
Declaration of Helsinki and the study was approved by The
Institutional Ethics and Investigation Committee of Qilu Hospital,
Shandong University [approval no. KYLL-2015(KS) -068]. All patients
provided informed written consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Touat M, Idbaih A, Sanson M and Ligon KL:
Glioblastoma targeted therapy: Updated approaches from recent
biological insights. Ann Oncol. 28:1457–1472. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Gao M, Lin Y, Liu X, Li Y, Zhang C, Wang
Z, Wang Z, Wang Y and Guo Z: ISG20 promotes local tumor immunity
and contributes to poor survival in human glioma. Oncoimmunology.
8(e1534038)2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Louis DN, Perry A, Reifenberger G, von
Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD,
Kleihues P and Ellison DW: The 2016 World Health Organization
Classification of tumors of the central nervous system: A summary.
Acta Neuropathol. 131:803–820. 2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Zhang X, Wang X, Xu R, Ji J, Xu Y, Han M,
Wei Y, Huang B, Chen A, Zhang Q, et al: YM155 decreases
radiation-induced invasion and reverses epithelial-mesenchymal
transition by targeting STAT3 in glioblastoma. J Transl Med.
16(79)2018.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Ostrom QT, Gittleman H, Liao P,
Vecchione-Koval T, Wolinsky Y, Kruchko C and Barnholtz-Sloan JS:
CBTRUS statistical report: Primary brain and other central nervous
system tumors diagnosed in the United States in 2010-2014. Neuro
Oncol. 19 (Suppl 5):v1–v88. 2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Fleischmann DF, Jenn J, Corradini S, Ruf
V, Herms J, Forbrig R, Unterrainer M, Thon N, Kreth FW, Belka C and
Niyazi M: Bevacizumab reduces toxicity of reirradiation in
recurrent high-grade glioma. Radiother Oncol. 138:99–105.
2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Lara-Velazquez M, Al-Kharboosh R,
Jeanneret S, Vazquez-Ramos C, Mahato D, Tavanaiepour D, Rahmathulla
G and Quinones-Hinojosa A: Advances in brain tumor surgery for
glioblastoma in adults. Brain Sci. 7(166)2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Gaspar LE, Fisher BJ, Macdonald DR, LeBer
DV, Halperin EC, Schold SC Jr and Cairncross JG: Supratentorial
malignant glioma: Patterns of recurrence and implications for
external beam local treatment. Int J Radiat Oncol Biol Phys.
24:55–57. 1992.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Zhang X, Ding K, Wang J, Li X and Zhao P:
Chemoresistance caused by the microenvironment of glioblastoma and
the corresponding solutions. Biomed Pharmacother. 109:39–46.
2019.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Zhang M, Wang X, Chen X, Zhang Q and Hong
J: Novel immune-related gene signature for risk stratification and
prognosis of survival in lower-grade glioma. Front Genet.
11(363)2020.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Au-Yeung CL, Yeung TL, Achreja A, Zhao H,
Yip KP, Kwan SY, Onstad M, Sheng J, Zhu Y, Baluya DL, et al: ITLN1
modulates invasive potential and metabolic reprogramming of ovarian
cancer cells in omental microenvironment. Nat Commun.
11(3546)2020.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Erin N, Grahovac J, Brozovic A and Efferth
T: Tumor microenvironment and epithelial mesenchymal transition as
targets to overcome tumor multidrug resistance. Drug Resist Updat.
53(100715)2020.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Uttam S, Stern AM, Sevinsky CJ, Furman S,
Pullara F, Spagnolo D, Nguyen L, Gough A, Ginty F, Lansing Taylor D
and Chakra Chennubhotla S: Spatial domain analysis predicts risk of
colorectal cancer recurrence and infers associated tumor
microenvironment networks. Nat Commun. 11(3515)2020.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Yang W, Yang S, Zhang F, Cheng F, Wang X
and Rao J: Influence of the Hippo-YAP signalling pathway on tumor
associated macrophages (TAMs) and its implications on cancer
immunosuppressive microenvironment. Ann Transl Med.
8(399)2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Schiffer D, Annovazzi L, Casalone C,
Corona C and Mellai M: Glioblastoma: Microenvironment and Niche
Concept. Cancers (Basel). 11(5)2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Hao Q, Vadgama JV and Wang P: CCL2/CCR2
signaling in cancer pathogenesis. Cell Commun Signal.
18(82)2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Desbaillets I, Tada M, de Tribolet N,
Diserens AC, Hamou MF and Van Meir EG: Human astrocytomas and
glioblastomas express monocyte chemoattractant protein-1 (MCP-1) in
vivo and in vitro. Int J Cancer. 58:240–247. 1994.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Nalla AK, Gogineni VR, Gupta R, Dinh DH
and Rao JS: Suppression of uPA and uPAR blocks radiation-induced
MCP-1 mediated recruitment of endothelial cells in meningioma. Cell
Signal. 23:1299–1310. 2011.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Fischer S, Weishaupt A, Troppmair J and
Martini R: Increase of MCP-1 (CCL2) in myelin mutant Schwann cells
is mediated by MEK-ERK signaling pathway. Glia. 56:836–843.
2008.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Yoshimura T: The production of monocyte
chemoattractant protein-1 (MCP-1)/CCL2 in tumor microenvironments.
Cytokine. 98:71–78. 2017.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Vakilian A, Khorramdelazad H, Heidari P,
Sheikh Rezaei Z and Hassanshahi G: CCL2/CCR2 signaling pathway in
glioblastoma multiforme. Neurochem Int. 103:1–7. 2017.PubMed/NCBI View Article : Google Scholar
|
|
22
|
He M, Yu W, Chang C, Miyamoto H, Liu X,
Jiang K and Yeh S: Estrogen receptor α promotes lung cancer cell
invasion via increase of and cross-talk with infiltrated
macrophages through the CCL2/CCR2/MMP9 and CXCL12/CXCR4 signaling
pathways. Mol Oncol. 14:1779–1799. 2020.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Lubos N, van der Gaag S, Gercek M, Kant S,
Leube RE and Krusche CA: Inflammation shapes pathogenesis of murine
arrhythmogenic cardiomyopathy. Basic Res Cardiol.
115(42)2020.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Gong X, Duan Y, Zheng J, Ye Z and Hei TK:
Tetramethylpyrazine prevents contrast-induced nephropathy via
modulating tubular cell mitophagy and suppressing mitochondrial
fragmentation, CCL2/CCR2-mediated inflammation, and intestinal
injury. Oxid Med Cell Longev. 2019(7096912)2019.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Zhou W, Jiang Z, Xu YY and Li XG:
Attention to normal brain volumes in glioblastoma radiotherapy:
Potential role in tumor invasion and vasculogenesis. Med
Hypotheses. 80:501–504. 2013.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Mistry AM, Mummareddy N, Salwi S, Davis LT
and Ihrie RA: Glioblastoma distance from the subventricular neural
stem cell niche does not correlate with survival. Front Oncol.
10(564889)2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Li N, Li Y, Li Z, Huang C, Yang Y, Lang M,
Cao J, Jiang W, Xu Y, Dong J and Ren H: Hypoxia inducible factor 1
(HIF-1) recruits macrophage to activate pancreatic stellate cells
in pancreatic ductal adenocarcinoma. Int J Mol Sci.
17(799)2016.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Zhang X, Wang J, Li X and Wang D:
Lysosomes contribute to radioresistance in cancer. Cancer Lett.
439:39–46. 2018.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Cui YH, Suh Y, Lee HJ, Yoo KC, Uddin N,
Jeong YJ, Lee JS, Hwang SG, Nam SY, Kim MJ and Lee SJ: Radiation
promotes invasiveness of non-small-cell lung cancer cells through
granulocyte-colony-stimulating factor. Oncogene. 34:5372–5382.
2015.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Morganti JM, Jopson TD, Liu S, Gupta N and
Rosi S: Cranial irradiation alters the brain's microenvironment and
permits CCR2+ macrophage infiltration. PLoS One.
9(e93650)2014.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Cherry JD, Meng G, Daley S, Xia W, Svirsky
S, Alvarez VE, Nicks R, Pothast M, Kelley H, Huber B, et al: CCL2
is associated with microglia and macrophage recruitment in chronic
traumatic encephalopathy. J Neuroinflammation.
17(370)2020.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Yoshimura T: The chemokine MCP-1 (CCL2) in
the host interaction with cancer: A foe or ally? Cell Mol Immunol.
15:335–345. 2018.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Chen Z, Feng X, Herting CJ, Garcia VA, Nie
K, Pong WW, Rasmussen R, Dwivedi B, Seby S, Wolf SA, et al:
Cellular and molecular identity of tumor-associated macrophages in
glioblastoma. Cancer Res. 77:2266–2278. 2017.PubMed/NCBI View Article : Google Scholar
|
|
34
|
He S, He S, Chen CH, Deborde S, Bakst RL,
Chernichenko N, McNamara WF, Lee SY, Barajas F, Yu Z, et al: The
chemokine (CCL2-CCR2) signaling axis mediates perineural invasion.
Mol Cancer Res. 13:380–390. 2015.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Zhu X, Fujita M, Snyder LA and Okada H:
Systemic delivery of neutralizing antibody targeting CCL2 for
glioma therapy. J Neurooncol. 104:83–92. 2011.PubMed/NCBI View Article : Google Scholar
|
|
36
|
D'Alessio A, Proietti G, Sica G and
Scicchitano BM: Pathological and molecular features of glioblastoma
and its peritumoral tissue. Cancers (Basel). 11(469)2019.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Seifert M, Schackert G, Temme A, Schröck
E, Deutsch A and Klink B: Molecular characterization of astrocytoma
progression towards secondary glioblastomas utilizing
patient-matched tumor pairs. Cancers (Basel).
12(1696)2020.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Aldape K, Zadeh G, Mansouri S,
Reifenberger G and von Deimling A: Glioblastoma: Pathology,
molecular mechanisms and markers. Acta Neuropathol. 129:829–848.
2015.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Kalbasi A, Komar C, Tooker GM, Liu M, Lee
JW, Gladney WL, Ben-Josef E and Beatty GL: Tumor-derived CCL2
mediates resistance to radiotherapy in pancreatic ductal
adenocarcinoma. Clin Cancer Res. 23:137–148. 2017.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Thomas JG, Parker Kerrigan BC, Hossain A,
Gumin J, Shinojima N, Nwajei F, Ezhilarasan R, Love P, Sulman EP
and Lang FF: Ionizing radiation augments glioma tropism of
mesenchymal stem cells. J Neurosurg. 128:287–295. 2018.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Flores-Toro JA, Luo D, Gopinath A,
Sarkisian MR, Campbell JJ, Charo IF, Singh R, Schall TJ, Datta M,
Jain RK, et al: CCR2 inhibition reduces tumor myeloid cells and
unmasks a checkpoint inhibitor effect to slow progression of
resistant murine gliomas. Proc Natl Acad Sci USA. 117:1129–1138.
2020.PubMed/NCBI View Article : Google Scholar
|