Introduction
Nowdays, more and more people (particularly the
young) suffer from sudden sensorineural hearing loss (SSNHL)
(1,2). The disease has unknown causes and is
characterized by continuous decline of two or more hearing
frequencies, rapid progression and short time of onset (3,4). A
previous study has shown that most patients with SSNHL experience
hearing loss accompanied by vestibular trauma, which seriously
damages hearing and significantly affects prognoses (5). The factors causing SSNHL are unclear,
and the disease cannot be treated with specific regimens. The
current standard treatment for sudden hearing loss is a tapered
course of oral high-dose corticosteroids to increase circulation to
the inner ear (6). In the present
study, alprostadil and the combination of alprostadil and HBO were
investigated as treatments for SSNHL.
Alprostadil regulates the activities of adenylate
cyclase and phosphodiesterase in vascular smooth muscle cells,
increases the cellular concentration of cyclic adenosine
monophosphate and significantly relaxes vascular smooth muscles. It
also reduces platelet activity and blood viscosity to inhibit blood
aggregation, and eliminates oxygen free radicals, thus improving
vascular function in inner ear microcirculation disorders and
promoting blood circulation in the ears (7,8). As a
naturopathy that fuses oxygen and blood through high-concentration
air pressure in a chamber, hyperbaric oxygen (HBO) improves tissue
hypoxia and inner ear circulation disorders in the supportive
treatment of SSNHL (9,10). A previous study reported that, while
medicines alone are limited in treating the disease, a combination
of medicines with HBO increases partial pressure of blood oxygen in
the body and improves inner ear ischemia, hypoxia and edema with
positive therapeutic effects (11).
Currently, SSNHL is commonly treated with alprostadil and HBO, and
the value of this treatment has gradually increased in recent
years.
In the present study, the therapeutic value of
alprostadil combined with HBO are discussed in detail, and the
effects of this combination on hearing recovery and hemorheology
are assessed. The possible influencing factors of treatment
efficacy for SSNHL are comprehensively analyzed to improve the
overall therapeutic effect.
Materials and methods
General information
A total of 104 patients with SSNHL admitted from
January 2015 to July 2018 were enrolled in the randomized
controlled trial. Group A (n=52) received alprostadil treatment and
Group B (n=52) was treated with HBO plus alprostadil. Of the total
patients, 55 and 49 were males and females, respectively, with a
mean age of 44.62±11.45 years (age range, 20-59 years) and average
body mass index (BMI) of 21.63±3.35 kg/m2. The time of
onset ranged from 2 to 14 days with an average of 8.34±4.62 days.
The patients experienced flat descending SSNHL (n=26),
low-frequency descending SSNHL (n=33) and high-frequency descending
SSNHL (n=45).
Inclusion and exclusion criteria
The inclusion criteria were as follows: i) Patients
with hearing loss of >30 dB, affecting three or more frequencies
and arising over <3 days; ii) patients with unilateral deafness
accompanied by vertigo, vestibular dysfunction, aural fullness,
tinnitus and with normal cranial nerve examination results; and
iii) patients not allergic to alprostadil.
The exclusion criteria were as follows: i) Patients
who had recently taken ear medicines or undergone surgical
treatment; ii) patients with other pathological deafness; iii)
patients with ear trauma and critical strikes; iv) patients with
cognitive or communication disorders; and v) patients with poor
compliance. All patients and their families agreed to participate
in this study and signed an informed consent form. The present
study was approved by the Medical Ethics Committee of Zibo Central
Hospital (Zibo, China).
Experimental reagents and
materials
Alprostadil was purchased from Hagaoke White Swan
Pharmaceutical Group Co., Ltd. (State Food and Drug Administration;
approval no. H23023072). A HBO chamber was purchased from Ningbo
KQD Plastic Tech Co., Ltd. A non-invasive hemorheometer was
purchased from Beckman Coulter, Inc. A fully automated coagulation
analyzer was purchased from Jiangsu Horner Medical Instrument Co.,
Ltd.
Experimental methods
Patients in Group A were treated with alprostadil.
Alprostadil (10 µg) was dissolved and diluted in 0.9% NaCl solution
(200 ml) and administered via intravenous drip. The standard scheme
was once per day, and one course of treatment was completed in 10
days. The patients were treated for two courses and the interval
between courses was 3 days.
Patients in Group B were treated with HBO combined
with alprostadil. The pressure of the HBO chamber was adjusted to
0.2 MPa and then boosted for 20 min. The patients inhaled pure
oxygen for 1 h. The standard scheme was performed once per day, and
one course of treatment was completed in 10 days. The patients were
treated for two courses and the interval between courses was 3
days.
Outcome measures
The outcomes measured were as follows: i) Total
effective rate of treatment: The therapeutic effect was divided
into cured (symptoms completely disappeared), markedly effective
(symptoms basically disappeared and hearing threshold increased by
30 dB), effective (symptoms were significantly relieved and hearing
threshold increased by 15-30 dB) and ineffective (symptoms were
still significant and hearing threshold increased by <15 dB).
The total effective rate of treatment=(curative + markedly
effective + effective cases)/total number of cases x100% (12); ii) hearing recovery: Improvements of
tinnitus, aural fullness and vertigo in the two groups were
observed by clinicians and recorded as disappearance, alleviation,
or ineffectiveness. Hearing recovery rate=(disappearance +
alleviation cases)/total number of cases x100% (13); iii) Hemorheological index changes: A
non-invasive hemorheometer was used to detect and assess changes in
low-, middle- and high-shear whole blood viscosity as well as whole
blood viscosity before and after treatment; iv) Coagulation
function: A fully automated coagulation analyzer was used to
detect, record and assess changes in fibrinogen (FIB), platelet
factor (PF), prothrombin time (PT) and activated partial thrombin
time (APTT); and v) Analysis of related influencing factors:
According to the efficacy of HBO combined with alprostadil, the
patients were divided into effective and ineffective groups.
Multivariate logistic regression was used to analyze the factors
influencing the efficacy of treatment for SSNHL.
Statistical methods
SPSS 20.0 (IBM Corp.) was used for statistical
analysis. Measurement data were analyzed by the χ2 test
and expressed as the mean ± SD. Multiple comparisons were performed
using a mixed ANOVA followed by an appropriate post hoc test
(Bonferroni's correction) in order to compare indicators before and
after treatment. Multivariate logistic regression was used to
analyze factors influencing the efficacy of treatment for SSNHL.
Differences with P<0.05 were statistically significant.
Results
Comparison of general information
No significant differences were observed between
Group A and B with regards to sex, age, BMI and time or site of
onset (P>0.05; Table I).
 | Table IComparison of baseline characteristics
between patient groups. |
Table I
Comparison of baseline characteristics
between patient groups.
| Groups | Group A (n=52) | Group B (n=52) |
χ2-value/t | P-value |
|---|
| Sex | | | 0.347 | 0.556 |
|
Male | 26 (50.00) | 29 (55.77) | | |
|
Female | 26 (50.00) | 23 (44.23) | | |
| Age, years | 44.74±11.26 | 43.95±11.64 | 0.352 | 0.726 |
| BMI,
kg/m2 | 21.57±3.45 | 21.73±3.23 | 0.244 | 0.808 |
| Time of onset,
days | 8.87±3.37 | 8.25±3.58 | 0.706 | 0.482 |
| Site of onset | | | 0.040 | 0.842 |
|
Left
ear | 31 (59.62) | 30 (57.69) | | |
|
Right
ear | 21 (40.38) | 22 (42.31) | | |
| Hearing threshold,
dB | 67.35±7.93 | 68.25±8.01 | 0.576 | 0.566 |
| Classification of
deafness | | | 0.206 | 0.902 |
|
Flat
descent | 12 (23.08) | 14 (26.92) | | |
|
Low
frequency descent | 17 (32.69) | 16 (30.77) | | |
|
High
frequency descent | 23 (44.23) | 22 (42.31) | | |
Comparison of total effective rate of
treatment
The total effective rate of treatment in Group A was
lower compared with that in Group B (P<0.05; Table II).
| Table IIComparison of total effective rate of
treatment. |
Table II
Comparison of total effective rate of
treatment.
| Groups | Group A (n=52) | Group B (n=52) |
χ2-value | P-value |
|---|
| Curative | 12 (23.08) | 18 (34.62) | - | - |
| Markedly
effective | 11 (21.15) | 13 (25.00) | - | - |
| Effective | 13 (25.00) | 14 (26.92) | - | - |
| Ineffective | 16 (20.77) | 7 (13.46) | - | - |
| Total effective rate
of treatment | 36 (69.23) | 45 (86.54) | 4.522 | 0.034 |
Comparison of hearing recovery
Tinnitus, ear tightness and vertigo or vestibular
dysfunction improved in the two groups following treatment.
However, after treatment, the overall recovery rate of hearing in
Group B was higher than that in Group A (P<0.05; Table III).
| Table IIIComparison of hearing recovery
[n(%)]. |
Table III
Comparison of hearing recovery
[n(%)].
| Groups | Group A (n=52) | Group B (n=52) |
χ2-value | P-value |
|---|
| Tinnitus | | | 4.981 | 0.026 |
|
Disappearance | 24 (46.15) | 26 (50.00) | - | - |
|
Improved | 19 (36.54) | 24 (46.15) | - | - |
|
Ineffective | 9 (17.31) | 2 (3.85) | - | - |
|
Overall
recovery rate | 43 (82.69) | 50 (96.15) | - | - |
| Aural Fullness | | | 4.308 | 0.038 |
|
Disappearance | 25 (48.08) | 29 (55.77) | - | - |
|
Improved | 17 (32.69) | 20 (38.46) | - | - |
|
Ineffective | 10 (19.23) | 3 (5.77) | - | - |
|
Overall
recovery rate | 42 (80.77) | 49 (94.23) | - | - |
| Vertigo | | | 4.727 | 0.030 |
|
Disappearance | 22 (42.31) | 26 (50.00) | - | - |
|
Improved | 18 (34.62) | 22 (42.31) | - | - |
|
Ineffective | 12 (23.08) | 4 (7.69) | - | - |
|
Overall
recovery rate | 40 (76.92) | 48 (92.31) | - | - |
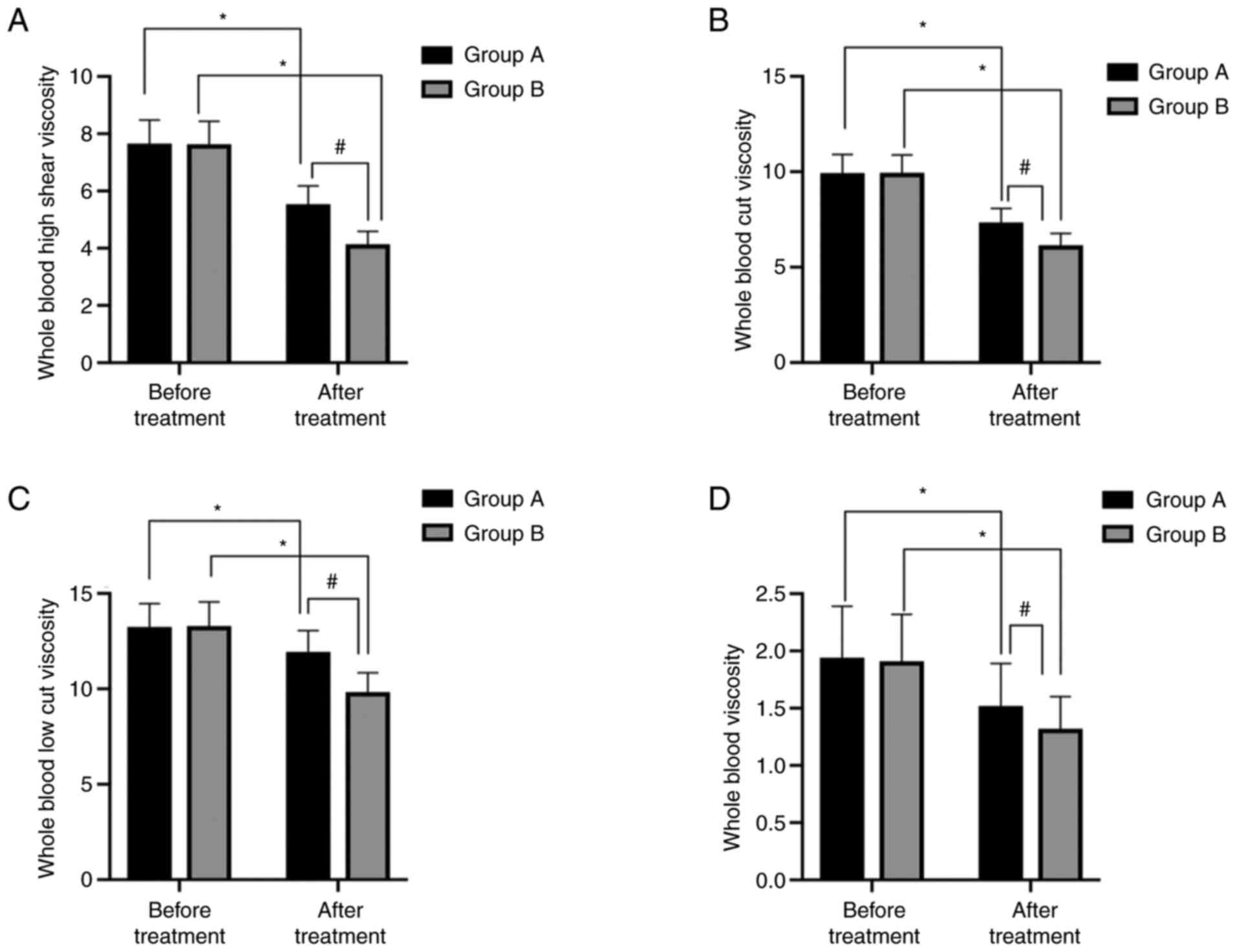
Comparison of hemorheological index
changes
Before treatment, there were no significant
differences between Group A and B in hemorheological indices
(P>0.05). After treatment, low-, middle- and high-shear whole
blood viscosity decreased in the two groups, and these
hemorheological indices in Group B were lower than those in Group A
(P<0.05; Fig. 1).
Comparison of coagulation
function
Before treatment, no significant differences were
noted between Group A and B in PF, FIB, PT and APTT (P>0.05).
After treatment, PF and FIB levels in the two groups decreased
(P<0.05), and PT and APTT were prolonged (P<0.05). The
improvement of these coagulation function parameters in Group B
were significantly greater than that in Group A (P<0.05;
Fig. 2).
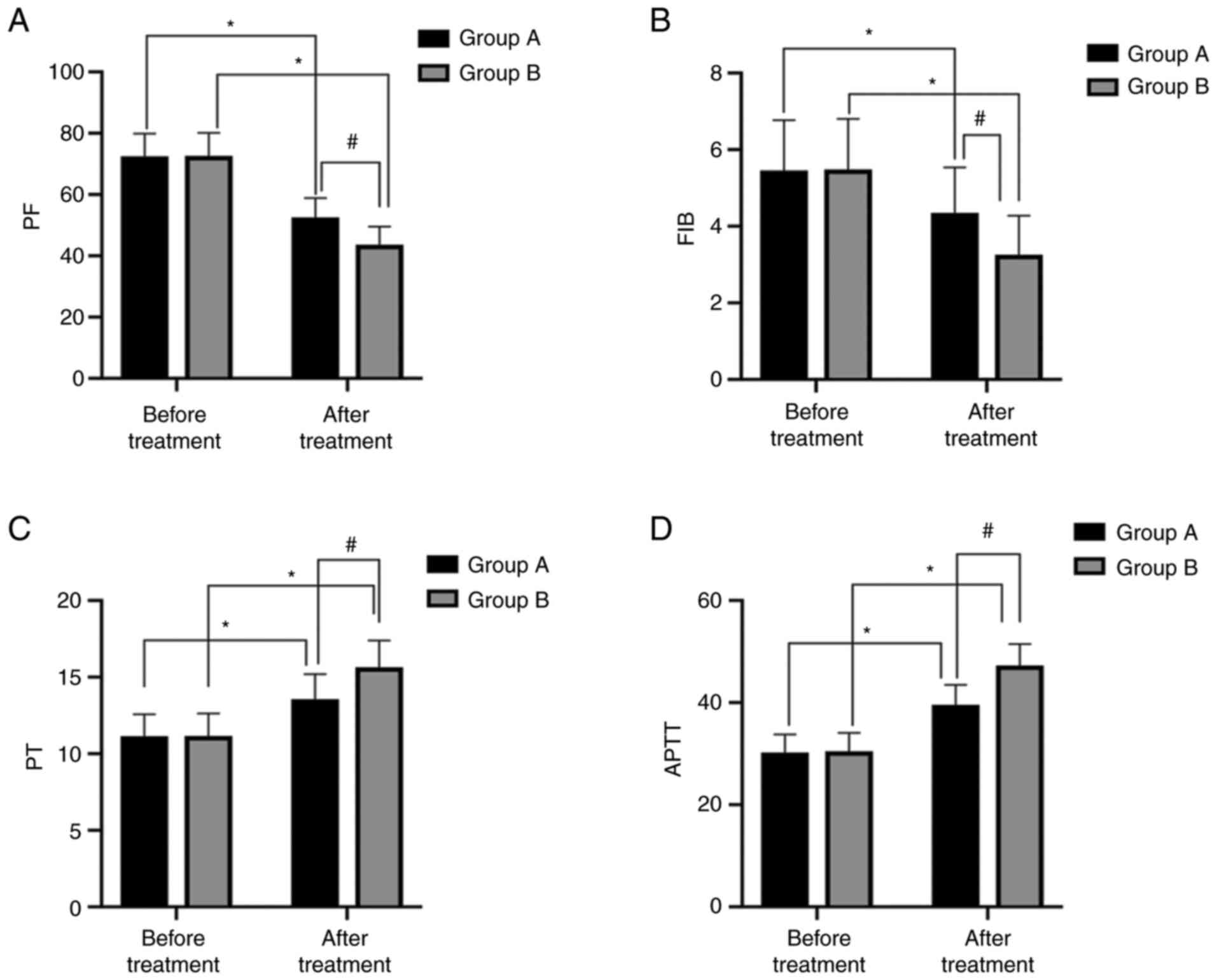 | Figure 2Comparison of parameters of
coagulation function. (A) After treatment, PF levels in both groups
significantly decreased, and were significantly lower in Group B
than in Group A. (B) After treatment, FIB levels in both groups
significantly decreased, and were significantly lower in Group B
than in Group A. (C) After treatment, PT in both groups was
significantly shortened, and was significantly shorter in Group B
than in Group A. (D) After treatment, APTT in both groups was
significantly shortened, and was significantly shorter in Group B
than in Group A. *P<0.05 vs. pre-treatment;
#P<0.05 vs. Group A. PF, platelet factor; FIB,
fibrinogen; PT, prothrombin time; APTT, activated partial thrombin
time. |
Univariate logistic regression
analysis
According to the efficacy of HBO combined with
alprostadil, patients were divided into effective (n=45) and
ineffective (n=7) groups. Univariate analysis of the clinical data
showed that there were significant differences between the two
groups in age, time of onset, hearing threshold, presence or
absence of tinnitus, plasma viscosity and C-reactive protein (CRP)
level. Changes in plasma viscosity have a huge impact on the degree
of deafness (P<0.05) whereas gender, and differences in the site
of onset, types of hearing curves, and presence or absence of
vertigo do not (P>0.05; Table
IV).
| Table IVUnivariate logistic regression
analysis. |
Table IV
Univariate logistic regression
analysis.
| Groups | Effective group
(n=45) | Ineffective group
(n=7) |
χ2-value/t | P-value |
|---|
| Sex | | | 0.006 | 0.937 |
|
Male | 25 (55.56) | 4 (57.14) | | |
|
Female | 20 (44.44) | 3 (42.86) | | |
| Age, years | 41.34±9.26 | 49.93±10.25 | 2.253 | 0.029 |
| Time of onset,
days | 7.51±3.25 | 11.25±3.54 | 2.148 | 0.037 |
| Site of onset | | | 0.001 | 0.975 |
|
Left
ear | 26 (57.78) | 4 (57.14) | | |
|
Right
ear | 19 (42.22) | 3 (42.86) | | |
| Hearing threshold,
dB | 64.55±8.25 | 73.44±8.41 | 2.646 | 0.011 |
| Types of hearing
curves | | | 0.625 | 0.429 |
|
Low-frequency
or flat descent | 20 (44.44) | 2 (28.57) | | |
|
High-frequency
descent or total deafness | 25 (55.56) | 5 (71.43) | | |
| Tinnitus | | | 4.127 | 0.042 |
|
Yes | 20 (44.44) | 6 (85.71) | | |
|
No | 25 (55.56) | 1 (14.29) | | |
| Vertigo | | | 1.486 | 0.223 |
|
Yes | 21 (46.67) | 5 (71.43) | | |
|
No | 24 (53.33) | 2 (28.57) | | |
| Whole blood
viscosity, MPa.s | 1.24±0.21 | 1.63±0.26 | 4.431 | <0.001 |
| Serum CRP level,
µmol/l | 21.23±3.57 | 28.23±3.63 | 4.816 | <0.001 |
Multivariate logistic regression
analysis
Multivariate logistic regression analysis was
conducted using efficacy of HBO combined with alprostadil in
treating SSNHL as a dependent variable, and differences between the
groups identified in the univariate analysis as independent
variables (Table V). The results
show that age, time of onset, hearing threshold, presence or
absence of tinnitus, plasma viscosity, and serum CRP level were the
influencing factors of the efficacy of HBO combined with
alprostadil for SSNHL (P<0.05; Table VI).
| Table VVariable assignment in logistic
regression analysis. |
Table V
Variable assignment in logistic
regression analysis.
| Factors | Assignment |
|---|
| Age | A continuous
variable analyzed by initial data |
| Time of onset | A continuous
variable analyzed by initial data |
| Hearing
threshold | A continuous
variable analyzed by initial data |
| Tinnitus | Yes=1, no=0 |
| Plasma
viscosity | A continuous
variable analyzed by initial data |
| Serum CRP
level | A continuous
variable analyzed by initial data |
| Table VIMultivariate logistic regression
analysis. |
Table VI
Multivariate logistic regression
analysis.
| | 95% C.I. for
EXP(B) |
|---|
| Factors | B | S.E, | Wals | Sig. | Exp (B) | Lower | Upper |
|---|
| Age | 0.040 | 0.-47 | 0.721 | 0.021 | 1.435 | 0.949 | 1.142 |
| Time of onset | -1.160 | 0.146 | 1.201 | 0.011 | 0.833 | 0.120 | 1.135 |
| Hearing
threshold | 0.003 | 0.060 | 0.002 | 0.022 | 1.003 | 0.118 | 1.127 |
| Tinnitus | 0.778 | 1.070 | 0.530 | 0.001 | 1.078 | 1.033 | 17.727 |
| Plasma
viscosity | -7.14 | 0.561 | 0.061 | 0.002 | 0.490 | 0.265 | 35.945 |
| Serum CRP
level | 0.042 | 0.432 | 0.031 | 0.014 | 1.403 | 0.117 | 1.457 |
Discussion
SSNHL is a disease with clinical symptoms including
tinnitus and vertigo. Its specific pathogenesis remains unclear,
although it may be related to viral infection, inner ear
microcirculation disorders and eardrum rupture (14,15).
Studies have shown that viral infection and hemodynamic changes in
patients with the disease result in lacunar obstruction after edema
and damaged functional structure of the cochlea due to insufficient
blood oxygen supply. This results in hearing loss and destruction
of the inner ear, which affects maintenance of body balance and
transmission of sound information. Deafness and tinnitus occur in
severe cases. Therefore, to treat SSNHL, blood oxygen supply in the
inner ear should be restored to normal levels (16,17).
Alprostadil, with a high bioavailability, delivers prostaglandin E1
to the lesion site, thereby improving its therapeutic stability
(18). HBO increases the partial
pressure and content of blood oxygen in patients, increases oxygen
diffusion, and improves tissue hypoxia and blood supply,
facilitating hair cell repair (19). It also increases blood flow,
improves the blood supply capacity of the vertebrobasilar artery in
the inner ear and improves the endothelial permeability of inner
ear capillaries. This results in greatly improved repair efficiency
of hair cells and vestibular nerve fibers (20). Few studies have investigated the
combined effects of alprostadil and HBO on hearing recovery and
hemorheology in patients with SSNHL. Therefore, the present study
explored the efficacy and influencing factors of combining
alprostadil with HBO in treating SSNHL.
In the current study, patients in Group B (treated
with combined alprostadil and HBO) had: i) Higher total effective
rate of treatment and overall recovery rate of hearing (P<0.05);
ii) lower blood viscosity after treatment (P<0.05); and iii)
greater improvement of coagulation function parameters after
treatment (P<0.05) relative to those treated with alprostadil
only (Group A). Previous studies have shown that alprostadil
significantly relieves pathological symptoms and promotes hearing
recovery in patients with SSNHL (21). The combination of alprostadil and
HBO leads to improvement of peripheral vascular resistance in terms
of antiplatelet aggregation by increasing the activity of
intracellular cyclic adenosine monophosphate. Moreover, it
accelerates the absorption of extravascular tissue fluid to correct
local edema, ensures ear blood supply and reduces the effects of
immune response damage on the body (22,23).
These results are consistent with the present findings, which
suggest that a combination of alprostadil and HBO (with wider and
more effective clinical value) can improve the therapeutic
efficiency of alprostadil and promote hearing recovery.
Multivariate logistic regression analysis revealed
that age, time of onset, hearing threshold, presence or absence of
tinnitus, plasma viscosity and serum CRP level are factors that
influence the efficacy of alprostadil and HBO in treating SSNHL
(P<0.05). A similar study suggested that age growth combined
with complications results in slow blood circulation and
deterioration of hearing function, which may affect the onset of
SSNHL (24). Slow blood flow in the
inner ear may cause stasis and, subsequently, hypoxia-induced hair
cell damage; however, timely treatment can improve microcirculation
to obtain a better outcome. Hearing threshold is affected by hair
cell damage and reflects hearing function and the therapeutic
effect of treatment on the inner ear (25). The presence of tinnitus symptoms
indicates that the lesion has reached the vestibular labyrinth,
which increases the difficulty of treatment and rehabilitation.
Serum CRP level is a common inflammatory response index, and
changes in its expression level affect the development and
progression of SSNHL. High plasma viscosity indicates poor blood
circulation. Therefore, monitoring plasma viscosity may be of great
significance for efficacy evaluation of certain treatments
(26). The aforementioned studies
further verify the findings of the current study that the
therapeutic effect of the treatment was poor if the corresponding
pathological factors were present.
In summary, alprostadil combined with HBO was an
effective treatment for SSNHL. However, certain shortcomings need
to be explored in future studies. For example, the efficacy of
SSNHL treatment is different among different hearing loss types and
detailed analysis is yet to be completed. Additionally, the
population size used in this study was relatively small. Other
important influencing factors for the prognosis of SSNHL (such as
the levels of serum lipids) will be examined in future studies.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
TF, QZ, JW, XW and YG conceived and designed the
research and interpreted the results of experiments. QZ, JW and XW
contributed to the design of the study and interpretation of
experimental results. TF and YG performed experiments, analyzed
data, prepared figures, and drafted the manuscript. TF and YG
edited and revised the manuscript. All authors read and approved
the final version of the manuscript.
Ethics approval and consent to
participate
All patients and their families agreed to
participate in this study and signed an informed consent form. This
study was approved by the Medical Ethics Committee of Zibo Central
Hospital.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Furuhashi A, Matsuda K, Asahi K and
Nakashima T: Sudden deafness: Long-term follow-up and recurrence.
Clin Otolaryngol Allied Sci. 27:458–463. 2002.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Research on deafness. Doctoral
dissertations. Am Ann Deaf. 147:230–233. 2002.PubMed/NCBI
|
|
3
|
Hirayama M, Shitara T, Okamoto M and Sano
H: Idiopathic bilateral sensorineural hearing loss: Its clinical
study in cases with rapidly progressed deafness. Acta Otolaryngol
Suppl. 534:39–42. 1996.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Qiu L, Zheng X, Xie F, Zhang M, Zhang J,
Yuan SB and Zeng GZ: Clinical observation on the different
frequency hearing damages in sudden deafness treated by
electroacupuncture combined with western medicine comprehensive
therapy. World J Acupunct Moxibustion. 22:22–27. 2012.
|
|
5
|
Inagaki T, Cureoglu S, Morita N, Terao K,
Sato T, Suzuki M and Paparella MM: Vestibular system changes in
sudden deafness with and without vertigo: A human temporal bone
study. Otol Neurotol. 33:1151–1155. 2012.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Ersoy Callioglu E, Tuzuner A, Demirci S,
Cengiz C and Caylan R: Comparison of simultaneous systemic steroid
and hyperbaric oxygen treatment versus only steroid in idiopathic
sudden sensorineural hearing loss. Int J Clin Exp Med. 8:9876–9682.
2015.PubMed/NCBI
|
|
7
|
Augustin AJ, Diehm C, Grieger F and Bentz
J: Alprostadil infusion in patients with dry age related macular
degeneration: A randomized controlled clinical trial. Expert Opin
Investig Drugs. 22:803–812. 2013.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Güneysu E, Koçman AE, Özatik O, Ovali C,
Can B, Alataş İÖ and Sevin MB: The effects of iloprost and
alprostadil on ischemia-reperfusion injury in preventing
inflammation, tissue degeneration, and apoptosis in rat skeletal
muscle. Turk J Med Sci. 47:1028–1036. 2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
de Pont AC, de Jonge E and Vroom MB:
Hyperbaric oxygen for acute carbon monoxide poisoning. N Engl J
Med. 348:557–560. 2003.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Li J, Shi Q, Wei Q and Han P: Re: Efficacy
and safety of mirodenafil for patients with erectile dysfunction: A
meta-analysis of three multicenter, randomized, double-blind,
placebo-controlled clinical trials. Aging Male.
18(71)2015.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Wei KU, Liu Y, Jing WU, Wang Q, Tong B and
Duan M: Meta-analysis of the clinical efficacy of treatment of
sudden deafness using hyperbaric oxygen combined with drug in
China. Chin J Otol. 12:93–98. 2014.
|
|
12
|
Arndt S, Laszig R, Aschendorff A,
Hassepass F, Beck R and Wesarg T: Cochlear implant treatment of
patients with single-sided deafness or asymmetric hearing loss.
German version. HNO. 65:586–598. 2017.PubMed/NCBI View Article : Google Scholar : (In German).
|
|
13
|
Weiss D, Böcker AJ, Koopmann M, Savvas E,
Borowski M and Rudack C: Predictors of hearing recovery in patients
with severe sudden sensorineural hearing loss. J Otolaryngol Head
Neck Surg. 46(27)2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Zhai S, Ning Y, Guiliang Z, Yuhua Z and He
Q: Effect of retreatment on the end-stage sudden deafness. Cell
Biochem Biophys. 62:403–406. 2012.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Merchant SN, Durand ML and Adams JC:
Sudden deafness: Is it viral? ORL J Otorhinolaryngol Relat Spec.
70:52–62. 2008.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ban JH, Hong SJ, Lee SY, Lee KC and Kim
CG: A clinical analysis of psychogenic hearing loss presenting as
sudden deafness. Korean J Otolaryngol Head Neck Surg. 48:572–576.
2005.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Domachevsky L, Keynan Y, Shupak A and Adir
Y: Hyperbaric oxygen in the treatment of sudden deafness. Eur Arch
Otorhinolaryngol. 264:951–953. 2007.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Kornberg A: Letter: Prostaglandin E1
therapy with alprostadil and risk reduction of early hepatic
cellular carcinoma after liver transplantation-authors' reply.
Aliment Pharmacol Ther. 43:173–174. 2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Liu Y, Sun D, Shao S, Jiang W, Sun Z and
Li Z: The effect of hyperbaric oxygen therapy to different degree
of hearing loss and types of threshold curve in sudden deafness
patients. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi.
24:890–894. 2010.PubMed/NCBI(In Chinese).
|
|
20
|
Tatar S, Orhan N, Yilmaz CU, Arican N,
Ahishali B, Kucuk M, Elmas I, Kaya M and Toklu AS: Hyperbaric
oxygen therapy for five days increases blood-brain barrier
permeability. Undersea Hyperb Med. 44:345–355. 2017.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Jiang J, Wang S and Tong K: Synergic
effect of alprostadil injection and ginaton in treating sudden
deafness. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi.
25:597–599. 2011.PubMed/NCBI(In Chinese).
|
|
22
|
Xin W, Wen HL, Zhao Q and Zhao ZW: Blood
dilution, hyperbaric oxygen, anticoagulation treatment for acute
carbon monoxide poisoning 115 patients. Chinese Journal of
Medicinal Guide. 45–47. 2008.
|
|
23
|
Hernández-Tejedor A, Cabré-Pericas L,
Martín-Delgado MC, Leal-Micharet AM and Algora-Weber A: EPIPUSE
study group. Evolution and prognosis of long intensive care unit
stay patients suffering a deterioration: A multicenter study. J
Crit Care. 30:654.e1–e7. 2015.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Ren J and Lu Y: Sudden deafness in the
elderly. Lin Chuang Er Bi Yan Hou Ke Za Zhi. 12:257–259.
1998.PubMed/NCBI(In Chinese).
|
|
25
|
Liberman MC: Noise-induced hearing loss:
Permanent versus temporary threshold shifts and the effects of hair
cell versus neuronal degeneration. Adv Exp Med Biol. 875:1–7.
2016.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Gao D, Shao J, Jin W, Xia X and Qu Y:
Correlations of serum cystatin C and hs-CRP with vascular
endothelial cell injury in patients with systemic lupus
erythematosus. Panminerva Med. 60:151–155. 2018.PubMed/NCBI View Article : Google Scholar
|