Introduction
Depression is the most common disease of affective
disorders, which is part of the field of psychiatry. Depression is
defined more as a mood disorder than as a thinking disorder,
limiting the normal functioning of individuals, and ranging from an
extremely mild to a severe form (1).
This negative emotional state can persist for a
short period of time or for a longer period, with mild, moderate or
severe intensity, which can seriously damage one's health (2). Globally, depression is a leading cause
of premature death, along with cardiovascular disease and cancer,
limiting the individual from activity, and with a significant risk
of suicide (3). Almost 800,000
individuals die each year from suicide (4). Depression is found in 5% of Europeans
and 25% are likely to experience a depressive episode at least once
in their lives (5). By 2030, it is
estimated that depression will become one of the most significant
mental and behavioral disorders, as it currently occupies a second
place in the ranking of diseases worldwide, following
cardiovascular diseases (6).
Approximately 80% of individuals who suffer from a
mental disease do not receive treatment, especially in poorly
developed countries (7). The most
common treatments used in depression are pharmacological medication
with antidepressants, or their combination with psychotherapy or
psychotherapy as singular treatment. Each employed treatment was
found to be useful, but for patients with severe depression, a high
dropout rate and low remission were found, and clinically
significant differences were observed between antidepressants and
placebo. Consequently, patients having mild or moderate depression
seek alternative treatments (1).
Bioresonance therapy has been successfully used as
an alternative therapy since 1970 in various ailments, by many
practitioners worldwide. This type of therapy was presented by
physicist Franz Morell and electrical engineering technician Erich
Rasche as a result of medical tests in electroacupuncture. Several
clinical, physical and organic studies have been completed by
global research groups that demonstrate the effectiveness of the
bioresonance approach in situations such as allergies, rheumatic
diseases, respiratory diseases and many painful syndromes (8). In the present study, the aim was to
determine whether this new method of therapy is a viable
alternative to antidepressants from the selective serotonin
reuptake inhibitor class for patients diagnosed with recurrent
moderate or mild depressive disorder by decreasing the level of
depression quantified with the Hamilton Scale. In addition, the aim
was to verify the null hypothesis (H0), which holds that the
applied bioresonance therapy does not accelerate the healing
process in patients with recurrent moderate and mild depressive
disorder, compared with antidepressant medication from the
selective serotonin reuptake inhibitor class. The alternative
hypothesis (H1) held that the applied therapy accelerates the
healing process in patients with recurrent moderate and mild
depressive disorder compared with antidepressant medication from
the selective serotonin reuptake inhibitor class.
Patients and methods
General
The present study included patients with recurrent
mild and moderate depressive disorder as per the criteria listed in
the Diagnostic Manual of Mental Disorders Five (DSMV) (2).
The patients were selected from the Mureș County
Clinical Hospital, Psychiatry Clinic I, in Targu-Mures, Romania and
in the specialized outpatient clinic and in the Terapia Ultramed
Bioresonance Therapy Practice within the Terapia Ultramed Clinic of
Targu-Mures. The retrospective study was conducted from October
2017 to 2018. Participants received an explanation on how the
research would be carried out, its duration, benefits, stages,
implications, data confidentiality and the possibility to exit the
study at any point. Participation in the study was based on
volunteering. Subjects received an informed consent form regarding
their participation in the study, which was knowingly signed by
those who agreed. The members of the Ethics Committee of the Mureș
County Clinical Hospital approved the study favorably (no.
16462/16.10.2017). The patients who were treated only with
bioresonance therapy did not undergo pharmacological treatment with
antidepressants.
Patient groups
The analyzed group comprised women and men, from
different social backgrounds, aged between 18 and 89 years (mean 49
years/SD 17.16 years). Patients that had undergone suicidal
attempts in their medical history, patients with pacemakers and
pregnant women were excluded.
The participants were divided into two groups as
follows: Group 1 included 40 patients (31 women and 9 men), with 17
females having recurrent mild depressive episodes, and 14 females
recurrent moderate depressive episodes. Within the male category, 4
men suffered from a recurrent moderate depressive episode and 5 men
from a recurrent mild depressive episode. They received
bioresonance therapy solely. Group 2 included 40 patients (19 were
women and 21 men). All study participants in this group were
previously diagnosed with recurrent moderate depressive episodes.
They received a monotherapy treatment with antidepressants from the
selective serotonin reuptake inhibitor class. The detailed
demographic structure of the two groups is detailed in Table I.
 | Table IDemographic aspects of the studied
groups. |
Table I
Demographic aspects of the studied
groups.
| Variable | Group 1
Bioresonance | Group 2 SSRI |
|---|
| Sex (female) | 77.50% | 47.50% |
|
Age
(years) | | |
|
Mean ±
SD | 43.85±12.58 | 55±17.16 |
| Marital status
(%) | | |
|
Married | 50.00 | 55.00 |
|
Divorced | 30.00 | 7.50 |
|
Single | 20.00 | 20.00 |
|
Widower | 0.00 | 17.50 |
| Educational level
(%) | | |
|
Primary | 0.00 | 12.50 |
|
Gymnasium | 0.00 | 17.50 |
|
High
school | 30.00 | 30.00 |
|
Secondary | 12.50 | 0.00 |
|
Vocational
school | 5.00 | 20.00 |
|
Higher
education | 52.50 | 20.00 |
| Environment (%) | | |
|
Rural | 35.00 | 37.50 |
|
Urban | 65.00 | 62.50 |
Method
For all patients, the decrease in the level of
depression, within a period of maximum 2 months, from the first to
the fifth session, was monitored.
The bioresonance treatment consisted of 20 min and
was conducted using a Mora Nova bioresonance device (Med-Tronik
GmbH, Germany). The bioresonance device automatically displays on
the screen of the device the 16 values of the energy field, eight
at the beginning and eight at the end of each bioresonance session.
When commencing with the therapy, the conductance between the hands
and feet is automatically measured and displayed. The principle of
basic bioresonance therapy with the Mora Nora device includes
endogenous therapy, by means of hand and foot electrodes, on the
palms and fingers and soles, respectively, where the reflexogenic
areas of the organs are provided, being considered the fundamental
principle of therapy with physical bioresonance. Through these
measurements the specific reaction of the patient to the applied
therapy was evaluated, showing the mental state in which the
patient was before and at the end of each treatment session
(9).
The Mora Nova device is an electromagnetic
transceiver, with a frequency between 0.1 and 480,000 Hz insured
with a frequency filter from 1 up to 500,000 Hz, which works
through connection to a source of electricity (10).
The basic principle of coupled electric oscillators
is to consider the cells as complex systems of layers, or as
charged structures, respectively, all biomolecules being highly
charged ions or even multipoles. Cellular systems are regarded as
numerous different distributions of charges and currents, induced
by the transfer of charge through hydrogen bonds or other molecular
deformations. The advanced technique of the Mora device, through
the biorhythm program, separated the oscillating information of the
molecules that stress the body from the oscillation information
that is conducive to the body's health. The human body incorporates
similar discrete frequencies of molecular oscillations, given by
the power of intermolecular forces (11). When connecting the patient to the
bioresonance device, no mechanical devices such as a smartphone,
jewellery, clips or any other electronic device should be present.
Before and after each treatment session, the electrodes are cleaned
with 700 alcohol (12).
The therapy was individualized according to the
biorhythm of the patient and incorporated high and low potencies.
Through biorhythm, the therapeutic program selected from the device
software regulated and controlled the patient's own oscillating
information, as well as their ability to adjust, in order to
initiate precisely target healing processes (13).
Endogenous therapy
Endogenous therapy is included in the principle of
basic bioresonance therapy with the Mora Nova device and is
considered the fundamental principle of bioresonance therapy at the
physical level. This type of therapy involves the destructive
inference or the so-called ‘overlapping extinction’ of rigid,
isolated vibrations, considered pathological vibrations in
themselves. In this way, they seem to be integrated into the
flexible vibrational composition of patients through the processes
of self-regulation. The physiological blockages correlated with the
‘rigid’ vibrations later dissolve. According to these hypotheses,
‘pathological vibrations’ are correlated with the disease on an
electromagnetic plane. A weak electromagnetic interaction has a
physiological consequence, due to the informative catalytic effect,
because they are weak interactions, in an initially fragile
situation. The energy needed to carry out the program must be
provided by the living system itself, through the acupressure
points of the lower and upper limbs. Bioresonance therapy also
promotes the individual's potential for self-healing (12).
Monotherapy
The second group received monotherapy with selective
serotonin reuptake inhibitors (SSRIs) as indicated in Table II. SSRIs are part of one of the
most widely used classes of antidepressants, with lower toxicity
and much higher safety compared to first-generation
antidepressants, which include monoamine oxidase inhibitors and
tricyclic antidepressants. Regarding the mechanism of action, SSRIs
inhibit serotonin reuptake, leading to an increase in the amount of
time serotonin stays in the synaptic cleft, resulting in longer
receptor stimulation, leading to greater accumulation of serotonin
in the synaptic cleft and increased signalling between synapses.
SSRI treatment stimulates 5HT1A and 5HT7
receptors on cell bodies in the nucleus of the raffia and
5HT1D receptors on serotonergic terminals, reducing 5HT
synthesis and release. With repeated administration of an SSRI,
there is a gradual decrease and desensitization of these
self-receptor mechanisms. Downward regulation of 5HT2A
postsynaptic receptors may contribute either to direct
antidepressant efficacy or by influencing noradrenergic function
and other serotonergic receptors. Other postsynaptic 5HT receptors
remain receptive to increased synaptic concentrations of 5HT and
contribute to the therapeutic effects of SSRIs. The subsequent
effects of SSRI treatment may also be important in mediating the
final responses of the therapy (14,15).
| Table IISSRI medication description. |
Table II
SSRI medication description.
| Medication | Dosage | No. of patients |
|---|
| Escitalopram | 10 mg Once per
day | 2 |
| Mirtazapine | 30 mg Once per
day | 17 |
| Mirtazapine | 30 mg Half per
day | 2 |
| Sertraline | 50 mg Once per
day | 2 |
| Sertraline | 50 mg Twice per
day | 16 |
| Sertraline | 50 mg Once and a half
per day | 1 |
Hamilton Scale
In order to assess the therapeutic outcome, the
Hamilton Scale was used to assess depression composed of 17 items
(Ham-D: 17). The Hamilton Scale measures individual depressive
symptoms and their general severity, reflected by a final score,
which indicates the degree of depression. The minimum score is 0
points and the maximum, 52 points. Symptoms are described as anchor
points comprising between 3 and 5 possible responses to each item,
with increasing severity. The score between 0 and 7 points
indicates the state of normalcy, the score between 8 and 17 points
represents a slight level of depression, between 18 and 24 points a
moderate level of depression, and a score above 24 means a severe
level of depression (16). The
change in depressive symptoms from the first to the last session of
therapy was assessed and bioresonance therapy was applied once a
week. For the second group, the change in depressive symptoms was
assessed after five weeks on antidepressant medication. The
Hamilton score analysis is presented in Table III.
| Table IIIHamilton Scale score between the
initial and the final sessions for each group. |
Table III
Hamilton Scale score between the
initial and the final sessions for each group.
| Group 1
Bioresonance | Hamilton score
Initial | Hamilton score
Outcome | Hamilton score
Difference |
|---|
| Mean | 16.9 | 13.8 | 3.1 |
| SD | 3.23 | 3.19 | 1.28 |
| No. of values | 40 | 40 | 40 |
| Outlier detected | No | No | No |
| Significance
level | | | P<0.0001 |
| Group 2 | Hamilton score | Hamilton score | Hamilton score |
| SSRI | Initial | Outcome | Difference |
| Mean | 22.8 | 20.6 | 2.2 |
| SD | 0.79 | 1.13 | 0.61 |
| No. of values | 40 | 40 | 40 |
| Outlier
detected | No | No | No |
| Significance
level | | | P<0.0001 |
Statistical analysis
For statistical calculations, Graph Pad 3.6
(GraphPad Software, Inc.) was used. The Student's t-test was used
to assess the differences between the means of continuous variables
(expressed as mean ± SD), while differences between nonparametric
variables (expressed as median, range) were compared using the
Mann-Whitney test. We interpreted all tests against a P=0.05
significance threshold and statistical significance was considered
for P-values below the significance threshold.
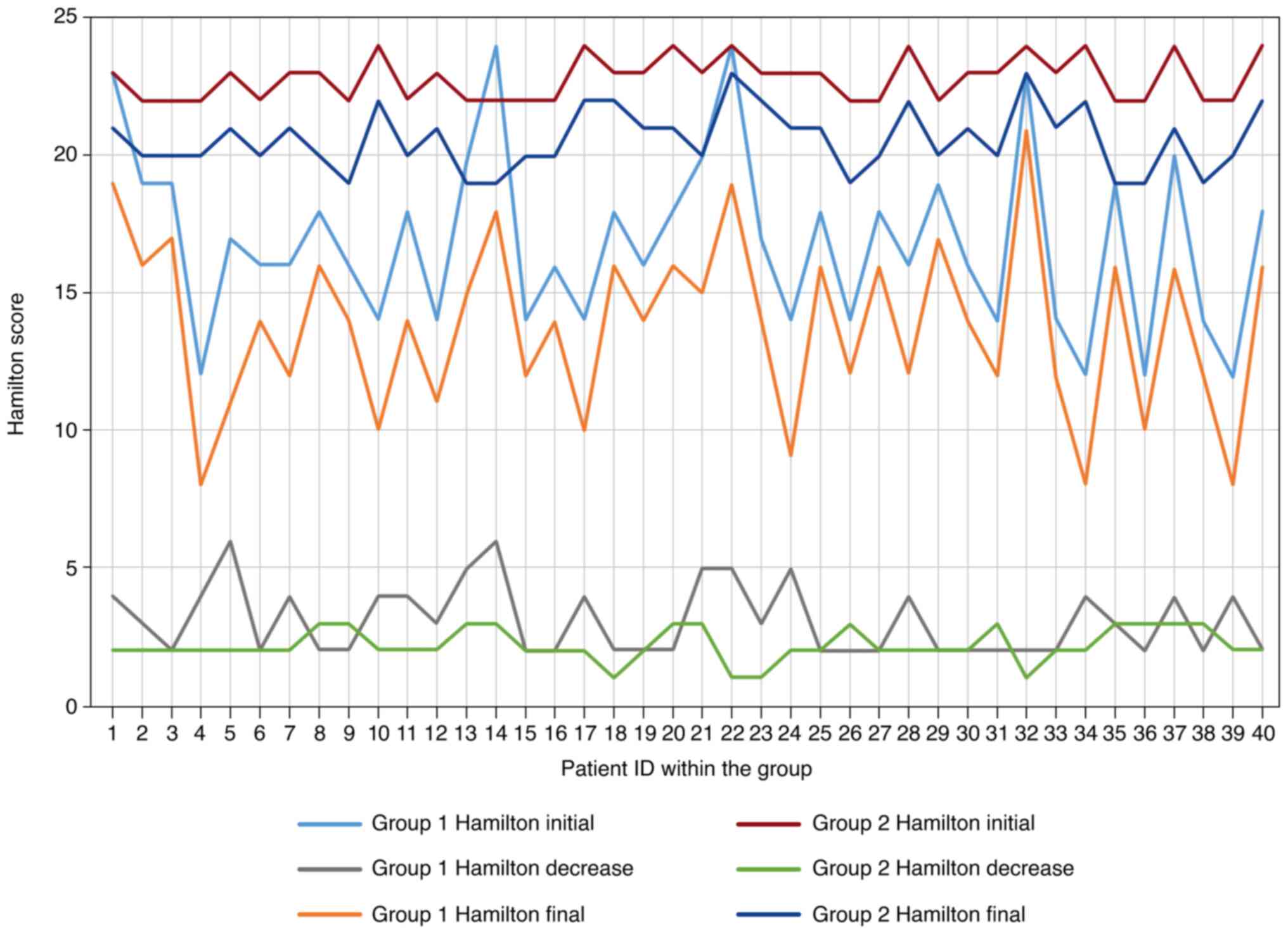
Results
The first group included 40 patients, having a
baseline score between 12 and 24 (mean 16.9, standard deviation
(SD) 3.23) on Hamilton Depression Rating Scale, with 17 items
(Table III). The patients of the
first group received only bioresonance therapy for five weeks,
without any other type of treatment.
The second group, the SSRI group, included 40
patients having a baseline score on the Hamilton Depression Rating
Scale, with 17 items between 22 and 24 (mean 22.8, SD 0.79)
(Table III). The second group
received either newly introduced or on-going pharmacological
treatment with selective serotonin reuptake inhibitors in
monotherapy for five weeks. After the applied treatment, an outcome
measurement of the illness severity was performed. The evolution in
Hamilton scores is presented in Fig.
1.
The differences were calculated for each patient.
Group 1 obtained a higher decrease in the Hamilton score. The
difference between the two data series was statistically different,
based on the Student's t-test (P<0.0001).
Discussion
The current study aimed to identify whether the
bioresonance therapy has quantifiable results in the treatment of
patients with recurrent mild or moderate depressive disorder. In
addition, it aimed to compare the therapy outcome with a group
treated with selective serotonin reuptake inhibitors.
As a strength, all the patients were diagnosed with
depression based on the DSMV criteria, assessed by a limited number
of psychiatrists. Strict exclusion criteria were applied. The
Hamilton questionnaires were applied by the same interview team to
all the patients, in order to minimize, as much as possible, a
subjective interpretation.
The use of alternative and complementary medicine
has increased among patients with psychiatric disorders, as it has
in the general population (17).
Therefore, there is a need to inquire about and analyze the way the
alternative solutions are functioning, if they are useful and what
risks and benefits they may involve. However, evidence-based
information is limited.
In the current model of mental illness care, widely
used treatments include pharmacological medication,
psychotherapeutic techniques such as psychotherapy,
cognitive-behavioral therapy and also electroconvulsive therapy and
transcranial magnetic stimulation (18,19).
Further research is needed to help identify cost-effective
alternative therapies for the treatment of depression, especially
for patients who refuse or no longer wish to continue
pharmacological treatment with antidepressants (16,20).
Specialized literature presents several studies in
which bioresonance therapy is successfully used in the case of
various pathologies (8) To the best
of our knowledge, no study thus far has conducted an objective
evaluation for the effectiveness of bioresonance therapy as an
alternative form of therapy in the treatment of depression.
A controlled clinical study was performed in Russia
in 2018 on 60 patients, who were high-performance athletes affected
by excessive physical exertion and addressed the regulation of
systolic blood pressure, heart rate, as well as the reduction of
stress by restoring the psycho-emotional balance. The non-placebo
group had more favorable results (21).
Bioresonance therapy can significantly improve
gastrointestinal disorders, as identified in a randomized
controlled study performed in Germany on 20 individuals with
psychosomatic diseases and gastrointestinal disorders, respectively
(22).
An observational pilot study carried out in 8
patients with lymphedema and lower limb lipedema demonstrated that
bioresonance therapy in lymphedema and lipedema was effective,
leading to reduced edema, relieved symptoms and improved lymphatic
drainage, without side effects (19,23).
A German prospective controlled clinical study
performed on 190 smokers has proven that Mora bioresonance therapy
was effective in discontinuing smoking and presented no side
effects (8,20).
A study conducted in Russia analyzed the synthesis
of proteins by lymphocytes from patients with rheumatoid arthritis
who received bioresonance therapy. This form of therapy is used to
correct energy disorders in the body's meridian system, with
electromagnetic waves at a frequency range of 10-500,000 Hz. It was
identified that, after bioresonance therapy, the intensity of
protein synthesis in the resting lymphocytes of the patients
returned to normal (21,24).
In the present study, among the patients in the
first group, after applying five bioresonance therapy sessions, 4
men and 10 women improved from a moderate depressive status to a
mild depressive stage. Among the study participants in the second
group, both women and men remained in a moderate depressive
status.
The limitations of the study are imposed by the
current state of knowledge in the field of bioresonance which is
less known in Romania and less studied in the world not having
enough studies. In addition, the bioresonance therapy in the
present study was applied with only one type of bioresonance
device, but the Mora Nova device in our opinion, is one of the most
powerful and complex currently available on the market. Also, the
patient monitoring period was relatively short at five weeks.
Surpassing the limitations of the present study can be achieved by
monitoring patients for a longer period of time, using other types
of bioresonance devices.
In conclusion, the study results confirmed that
bioresonance therapy could improve, independently of the level of
depression assessed with the Hamilton Depression Rating Scale
comprising 17 items, the status of patients suffering from mild and
moderate recurrent depression, who did not opt to use
pharmacological treatment.
Nevertheless, more rigorous and larger studies are
recommended. At present, based on the analysis in the current
study, bioresonance therapy appears promising and deserves further
study.
Acknowledgements
Professional editing, linguistic and technical
assistance performed by Irina Radu, Individual Service Provider
(credentials: E0048/2014, Medicine-Pharmacy).
Funding
Funding: No funding was received.
Availability of data and materials
All data and materials supporting the results of the
present study are available in the published article.
Authors' contributions
DM and IGG contributed to the design and conception
of the study. DM, SV and CRB wrote the original draft. DM, AS and
IGG participated in the data acquisition. SV and CRB contributed to
statistical analysis and interpretation of the data. DM, IGG and AS
worked on the part of the study related to patients. SV, AS, CRB
and IGG contributed to manuscript drafting or critical revisions to
the intellectual content. All authors approved the final manuscript
version and agreed to be accountable for all aspects of the work.
DM and IGG confirm the authenticity of all the raw data. All
authors have read and approved the final manuscript.
Ethics approval and consent to
participate
All patients gave their informed consent for
inclusion before they participated in the study. The study was
conducted in accordance with the Declaration of Helsinki and the
protocol was approved by the Ethics Committee of the Mures County
Hospital from Targu Mures, no. 16462/16.10.2017.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Haller H, Anheyer D, Cramer H and Dobos G:
Complementary therapies for clinical depression: An overview of
systematic reviews. BMJ Open. 9(e028527)2019.PubMed/NCBI View Article : Google Scholar
|
|
2
|
American Psychiatric Association:
Diagnostic and statistical manual of mental disorders. 5th edition.
American Psychiatric Association Press, Arlington, VA, pp155-188,
2013.
|
|
3
|
Rang HP, Dale MM, Ritter JM, Flower RJ and
Henderson G: Rang and Dale's pharmacology. 7th edition.
International Edition. British Library Cataloguing in Publication
Data. Elsevier Inc., Edinburgh, pp553-583, 2012.
|
|
4
|
James SL, Abate D, Abate KH, Abay SM,
Abbafati C, Abbasi N, Abbastabar H, Abd-Allah F, Abdela J,
Abdelalim A, et al: Global, regional, and national incidence,
prevalence, and years lived with disability for 354 diseases and
injuries for 195 countries and territories, 1990-2017: A systematic
analysis for the global burden of disease study 2017. Lancet.
392:1789–1858. 2018.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Wittchen HU, Jacobi F, Rehm J, Gustavsson
A, Svensson M, Jönsson B, Olese J, Allgulander C, Alonso J,
Faravelli C, et al: The size and burden of mental disorders and
other disorders of the brain in Europe 2010. Eur
Neuropsychopharmacol. 21:655–679. 2011.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Malhi GS and Mann JJ: Depression. Lancet.
392:2299–2312. 2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Wang PS, Aguilar-Gaxiola S, Alonso J,
Angermeyer MC, Borges G, Bromet EJ, Bruffaerts R, de Girolamo G, de
Graaf R, Gureje O, et al: Use of mental health services for
anxiety, mood, and substance disorders in 17 countries in the WHO
world mental health surveys. Lancet. 370:841–850. 2007.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Pihtili A, Galle M, Cuhadaroglu C,
Kilicaslan Z, Issever H, Erkan F, Cagatay T and Gulbaran Z:
Evidence for the efficacy of a bioresonance method in smoking
cessation: A pilot study. Forsch Komplementmed. 21:239–245.
2014.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Gottfried C: The new diagnostic system by
Dr. Cornelissen. IMZ Akademie, pp157-171, 2007.
|
|
10
|
Med-Tronik GmbH: Manual of instructions.
Version 3.1.3. Med-Tronik GmbH, pp72, 2020.
|
|
11
|
Muresan D, Salcudean A, Sabau CD, Bodo CR
and Gabos Grecu I: Bioresonance therapy may treat depression. J Med
Life. 14:238–242. 2021.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Med-Tronik GmbH: Nova MED
Training&Therapy Manual, medical technology in the 21st
century. Med-Tronik GmbH, pp16-37, 2014.
|
|
13
|
Muresan D, Salcudean A, Barbu BV, Bodo CR
and Gabos GI: Evaluation of an alternative depression therapy using
bioresonance. J Interdiscip Med. 6:82–86. 2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
O’Donnell JM, Bies RR and Shelton RC: Drug
therapy of depression and anxiety disorders. Chapter 15. In:
Goodman and Gilman’s pharmacological basis of therapeutics, 13th
edition. Brunton LL, Hilal-Dandan R, Knollmann BC (eds).
McGraw-Hill, New York, ΝΥ, pp267-277, 2001.
|
|
15
|
Stahl SM: Selectivity of SSRIs:
Individualising patient care through rational treatment choices.
Int J Psychiatry Clin Pract. 8 (Suppl 1):S3–S10. 2004.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Zimmerman M, Martinez HJ, Young D,
Chelminski I and Dalrymple K: Severity classification on the
Hamilton depression rating scale. J Affect Disord. 150:384–388.
2013.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Freeman MP: Complementary and alternative
medicine (CAM): Considerations for the treatment of major
depressive disorder. J Clin Psychiatry. 70 (Suppl 5):S4–S6.
2009.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Lake J and Turner MS: Urgent need for
improved mental health care and more collaborative model of care.
Perm J. 21:17–024. 2017.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Trifu S, Sevcenco A, Stănescu M, Drăgoi AM
and Cristea BM: Efficacy of electroconvulsive therapy as a
potential first-choice treatment in treatment-resistant depression
(Review). Exp Ther Med. 22(1281)2021.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Nguyen J: A literature review of
alternative therapies for postpartum depression. Nurs Womens
Health. 21:348–359. 2017.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Badtieva VA, Pavlov VI, Khokhlova MN and
Pachina AV: The application of bioresonance therapy for the
correction of the overtrained athlete syndrome. Vopr Kurortol
Fizioter Lech Fiz Kult. 95:51–57. 2018.PubMed/NCBI View Article : Google Scholar : (In Russian).
|
|
22
|
Nienhaus J and Galle M: Placebo-controlled
study of the effects of a standardized MORA bioresonance therapy on
functional gastrointestinal complaints. Forsch Komplementmed.
13:28–34. 2006.PubMed/NCBI View Article : Google Scholar : (In German).
|
|
23
|
Elio C, Guaitolini E, Paccasassi S, Rosati
N and Cavezzi : Application of microcurrents of bioresonance
and transdermal delivery of active principles in lymphedema and
lipedema of the lower limbs: A pilot study. G Ital Dermatol
Venereol. 149:643–647. 2014.PubMed/NCBI
|
|
24
|
Islamov BI, Funtikov VA, Bobrovskiĭ RV and
Gotovskiĭ YV: Bioresonance therapy in rheumatoid arthritis and heat
shock proteins. Bull Eksp Biol Med. 128:525–528. 1999.PubMed/NCBI(In Russian).
|