The lung is a complex organ composed of a system of
tubes. It is involved in various important physiological
activities, including gaseous exchanges and immune responses.
Respiratory diseases occur frequently, seriously endanger public
health and are a major cause of concern. For example, the overall
prevalence of asthma from 2012 to 2015 in China was 4.2%, which
represents 45.7 million adults (1). The increasing rate of incidence of
respiratory diseases has imposed a huge burden on society (2,3).
Although several advances have been made in the understanding of
the epidemiology and pathophysiology, only a few effective drug
treatment options are available for patients with pulmonary
diseases, especially those associated with higher mortality rates.
Since pulmonary transplant is the only choice for patients with
advanced diseases (4-7),
there is an urgent need to identify novel and more effective
treatment regimens for pulmonary diseases.
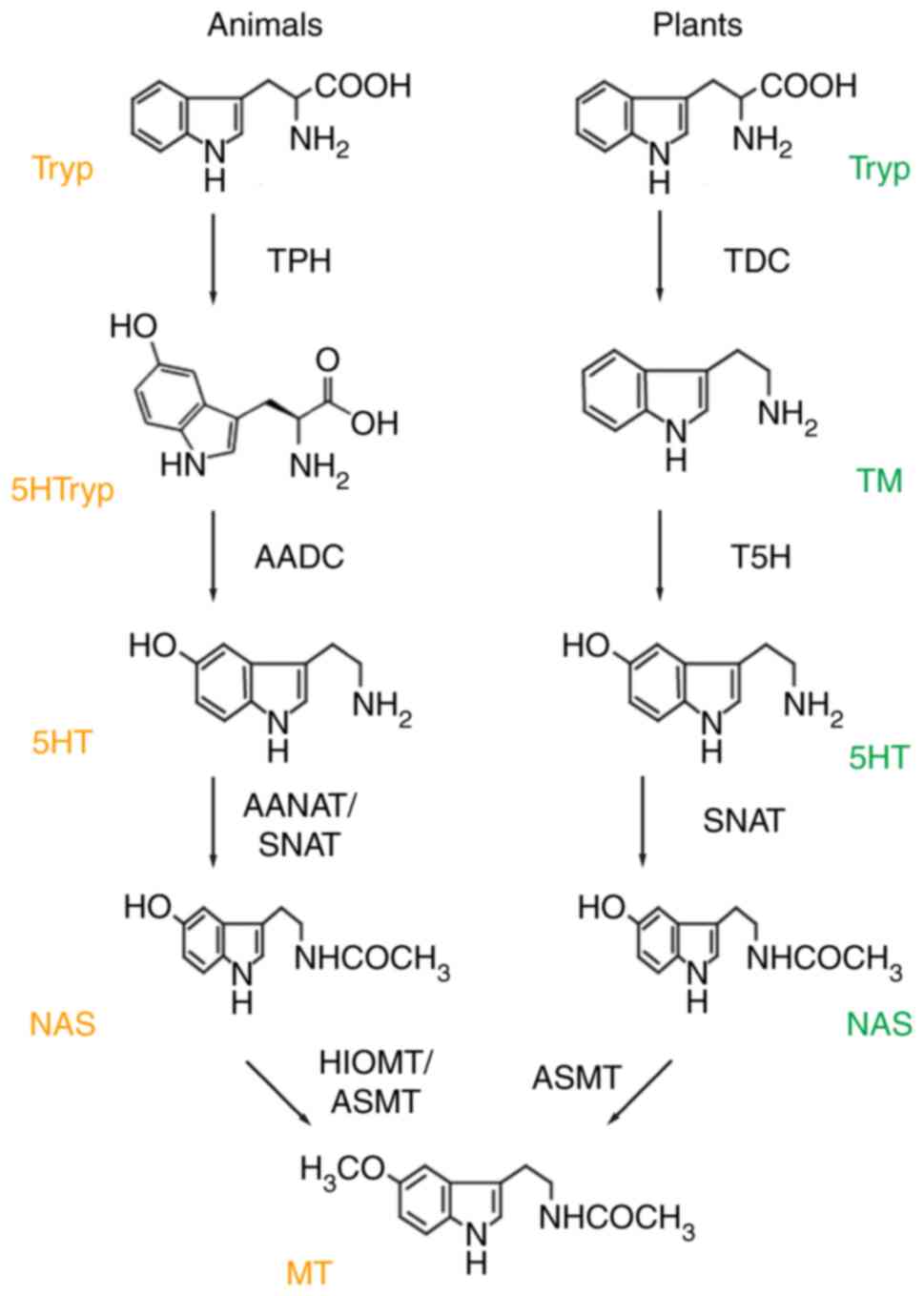
Chemically, N-acetyl-5-methoxytryptamine, also known
as melatonin, is an indoleamine synthesized from tryptophan
(8). Starting from tryptophan,
melatonin biosynthesis comprises four enzymatic steps in all
organisms (Fig. 1). First,
tryptophan is converted into serotonin through decarboxylation and
hydroxylation. The biosynthetic pathway of serotonin in vertebrates
differs from that in microorganisms and plants, resulting in the
production of melatonin specific for different taxa (9). In plants, tryptophan decarboxylase,
decarboxylates tryptophan into tryptamine and tryptamine
5-hydroxylase then catalyzes the synthesis of serotonin (10). However, tryptophan decarboxylation
is not the first step in serotonin production. In animals,
tryptophan hydroxylase hydroxylates tryptophan and produces
5-hydroxytryptophan and then aromatic amino acid decarboxylase
decarboxylates 5-hydroxytryptophan, resulting in the production of
serotonin (11-13).
Finally, serotonin is either acetylated to N-acetylserotonin or
methylated to form 5-methoxytryptamine. Through corresponding
methylation or acetylation processes, these products finally
produce melatonin (14-19).
Melatonin exerts regulatory physiological effects on the central
nervous system, immune system, endocrine system, cardiovascular
system, reproductive system and metabolism (20-28).
In addition to its direct action, melatonin can also function
indirectly through the melatonin receptors. Melatonin has three
receptors, namely melatonin receptor-1 (MT1), melatonin receptor-2
(MT2) and melatonin receptor-3 (MT3). MT1 is characterized as a
receptor linked to a pertussis toxin-sensitive guanine
nucleotide-binding protein (G-protein), which mediates the
inhibition of adenyly lcyclase in native tissues (29,30).
MT2 was cloned just 1 year after the MT1 receptor was cloned. It is
362 amino acids long with a molecular weight of 40,188 Da and it
shares 60% homology with MT1 (31-34).
MT3 is an enzyme belonging to the reductase group, which is
involved in the prevention of oxidative stress by inhibiting the
electron transfer reactions of quinones (35,36).
As a popular natural food supplement, melatonin is famous for its
minimal side effects, although there are few studies on its
long-term safety. The acute toxicity of melatonin is extremely low
in both animal and human studies (22,24).
Melatonin has been reported to exhibit strong clinical efficacy in
a number of diseases (21);
however, the recent findings on melatonin functions in the field of
pulmonary disorders, such as its beneficial effects of decreasing
thrombosis and sepsis in COVID-19 patients (37,38),
have not received much attention. The present review mainly
summarizes and discusses the roles of melatonin in pulmonary
disorders.
Inflammation is a basic pathological process,
wherein the body is stimulated by some injury factors, such as
trauma and infection. Inflammatory cells, including leukocytes,
macrophages, mast cells and endothelial cells, are involved in the
repair processes of inflammatory tissues (39). Inhibition of the inflammatory
processes is essential in antagonizing chronic or acute
inflammatory diseases (40,41).
The main mechanism of action of the commonly used nonsteroidal
anti-inflammatory drugs in clinical settings is the inhibition of
the activity of cyclooxygenase and the reduction in synthesis of
prostaglandin with a high risk of adverse reactions, such as
gastrointestinal and skin reactions as well as liver damage.
Melatonin has great potential as a therapeutic drug
for preventing inflammation and regulating the sleep cycle in
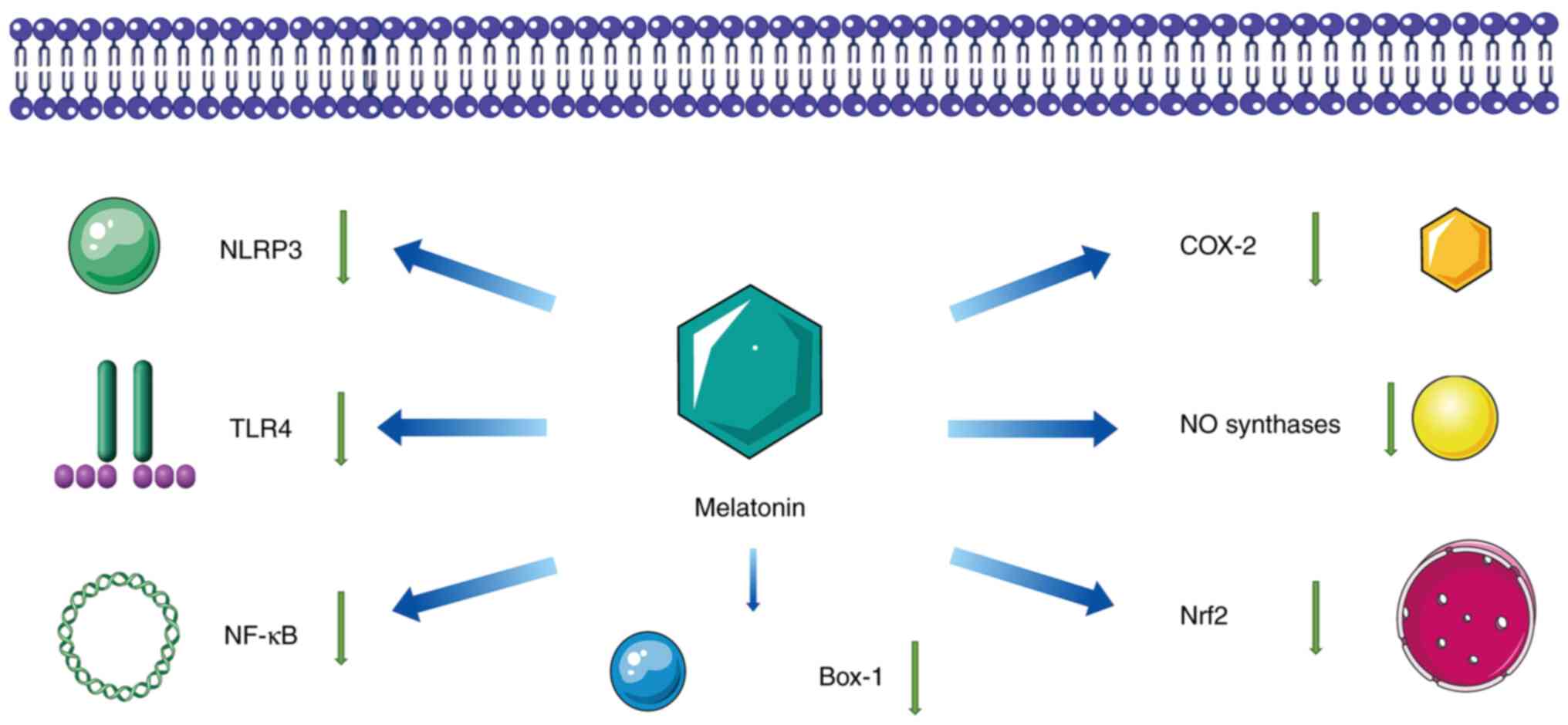
patients admitted to intensive care units (42). The mechanisms of anti-inflammatory
effects are variable and consist of several pathways. These include
downregulation of the activities of neuronal nitric oxide (NO)
synthases, downregulation of nuclear factor erythroid 2-related
factor 2 (Nrf2) and cyclooxygenase-2, and inhibition of
high-mobility group box-1 signaling, inflammasome NLR-family pyrin
domain containing protein 3 (NLRP3), NF-κB and toll-like receptor-4
(43-45)
(Fig. 2). These effects are
exerted via the downregulation of pro-inflammatory factors and
concomitant upregulation of anti-inflammatory cytokines (46). Pro-inflammatory effects of
amyloid-β peptides are reduced upon increasing the activity of
α-secretase and inhibiting those of β- and γ-secretases (47-49).
Particularly, the role of melatonin may be associated with the
upregulation of sirtuin-1, which affects signaling through mTOR and
Notch pathways (50,51).
In the processes of energy metabolism, free radicals
of oxygen are inevitably produced by aerobic metabolism, and
without an adequate defense system for their removal, excess free
radicals of oxygen can lead to cell damage (52,53).
In 1993, melatonin was identified as a potent and efficient
endogenous radical scavenger (8).
Compared with conventional antioxidants (vitamins C and E,
mannitol, and glutathione), melatonin has substantially powerful
antioxidant potential (39). It is
a strong endogenous free radical scavenger whose basic function is
to participate in the antioxidant system and prevent oxidative
damage to cells (54,55). Melatonin can eliminate several
oxygen-derived reactants, including neutralizing superoxide anion,
hydroxyl radical, hydrogen peroxide, singlet oxygen and
hypochlorous acid. In addition, it has been reported that melatonin
can detoxify NO, peroxynitrite anion and/or peroxynitrous acid
(56,57). After scavenging these free
radicals, melatonin is transformed into metabolites, such as cyclic
3-hydroxmelatonin, N1-acetyl-N2-formyl-5-methoxykynuramine and
N1-acetyl-5-methoxykynuramine; these also exert potent
antioxidative actions (58).
Furthermore, melatonin indirectly increases the activities of
antioxidant enzymes [superoxide dismutase (SOD) and glutathione
peroxidase]. Through MT1 or MT2, the activities and the mRNA
expression of the antioxidant enzymes increase substantially
(57).
Melatonin exerts protective effects against several
cancer types, including ovarian, prostate, colon and breast cancer
(26,28). In a randomized study, after 31
months, relative to the ‘no treatment’ group, the percentage of
disease-free survival in patients with melanoma who received oral
adjuvant therapy of melatonin daily, was higher and the curve was
substantially longer, suggesting that the adjuvant therapy with
melatonin is effective in preventing tumor progression (59). Studies in animal models are
consistent with these clinical findings; melatonin has anticancer
effects in vivo at different stages of tumor development,
where it is critical in inhibiting the mitogenic signaling
molecule, linoleic acid and its metabolism to
13-hydroxyoctadecadienoic acid (60). Similarly, a reduction in melatonin
secretion caused upon increasing exposure to nocturnal light is
associated with the elevation in incidence rates of breast,
endometrial and colorectal cancer (61,62).
Additionally, melatonin suppresses chromium and X-ray-induced DNA
damage, and reduces safrole-induced DNA-adduct formation and
genetic damage caused by cis-platinum (63,64).
Notably, melatonin administration inhibits endothelin-1 synthesis
by suppressing the activity of endothelin converting enzyme, which
is critical in suppressing tumor angiogenesis (65,66).
Apoptosis is a spontaneous and ordered cell death
process controlled by genes to maintain the stability of the
internal environment (67). It
involves the activation, expression and regulation of several
genes. It is not a phenomenon of self-injury under pathological
conditions, but a death process that actively strives for improved
adaptation to the living environment (68). Amyloid β (Aβ)-treated cells show
several apoptotic characteristics, while cells pre-treated with
melatonin prior to Aβ exposure show a decrease in apoptotic
characteristics due to decreased intracellular reactive oxygen
species (ROS) production, attenuation of NF-κB activation and
decreased activity of the caspase-3 enzyme (69). Melatonin also prevented NO levels
and apoptosis induced upon ischemic stroke through the upregulation
of the expression of the anti-apoptotic protein, BCL-2, in the
pineal gland tumor-β immortalized cell line (70). Several studies have confirmed that
melatonin reduces cancer cell proliferation and promotes their
apoptosis (71,72).
Severe acute respiratory syndrome coronavirus 2
(SARS-CoV-2) is a novel and highly pathogenic virus, and caused the
recent pandemic, as declared by the World Health Organization in
March 2020. Coronaviruses are linear single-stranded RNA viruses
with a set of envelopes that are a naturally occurring huge family
of viruses. The diameter of the coronavirus is 80-120 nm (73). The 5 ‘end of the genome has a
methylated cap structure, while the 3’ end has a poly-(A) tail. The
entire length of the complete genome is 27-32 kb, which is the
largest among all known RNA viruses (74). The coronavirus disease-2019
(COVID-19) is a highly pathogenic infection caused by SARS-CoV-2
and transmitted primarily through respiratory droplets. Patients
with COVID-19 present various symptoms, including fever, cough,
myalgia, fatigue and diarrhea. However, severe progression of
COVID-19 leads to acute lung injury or acute respiratory distress
syndrome, which is associated with high mortality rates among the
elderly and those with previous underlying medical conditions
(75). As SARS-CoV-2 attaches to
the angiotensin-converting enzyme 2 receptor on the airway
epithelial cell surfaces, it triggers a pro-inflammatory response,
often leading to a cytokine storm and acute respiratory distress
syndrome. Another pro-oxidation reaction leads to alveolar damage
mediated by ROS. Therefore, to avoid severe development, treatment
should be started immediately after confirmation of the infection
(76-78).
Melatonin treatment for COVID-19 has been reported
to exhibit satisfactory results with an expected reduction in
symptom severity and possibly immunopathology (79-81).
In addition, the combination of melatonin and antiviral drugs (such
as ribavirin and acyclovir) has been found to be more effective
than antiviral drugs alone (82,83).
By inhibiting calmodulin and chymotrypsin-like protease, melatonin
reduces the viral entry and viral replication in the host.
Meanwhile, melatonin reduces systemic inflammation and acute
respiratory distress syndrome by increasing sirtuin 1 activity, and
simultaneously inhibiting the NLR family pyrin domain-containing 3
(NRLP3) inflammasome, toll-like receptor 4, nuclear factor kappa B
(NF-κB) signaling, expression of cyclooxygenase-2 and inducible NO
synthase (80). Melatonin also
protects the lungs by inhibiting angiotensin II and promoting
angiotensin 1-7 activity (82). In
order to reduce SARS-CoV-2-induced oxidative stress, melatonin can
eliminate reactive nitrogen species, and increase the activities of
SOD, glutathione peroxidase and catalase activity (84-86).
Overall, the beneficial role of melatonin in improving the symptoms
of COVID-19 is attributed to its multi-faceted roles as an
antioxidant, anti-inflammatory and immunomodulatory agent.
At present, the COVID-19 virus has mutated and
become more contagious; the number of infected individuals is on
the rise. The challenge of suppressing the COVID-19 pandemic is
further complicated by the emergence of several SARS-COV-2
variants, such as the B.1.1.7 (Alpha), B.1.351 (Beta), P1 (Gamma)
and B.1.617.2 (Delta) variants, showing increased transmissibility
and resistance to vaccines and treatments (87,88).
These variants are characterized by multiple mutations in the viral
spike protein, the target of neutralizing antibodies elicited in
response to infection or vaccine immunization (89). Thus, safe, effective and
inexpensive drugs for the prevention of infection spread are
warranted; melatonin is a strong candidate and further studies
should verify its effect on these variants. Furthermore, viruses
have always been a threat to humanity, which is reaffirmed by the
SARS spread in 2003, and at present, they threaten human health due
to multiple lung complications and disorders of the immune system.
Melatonin may be a secret weapon against these viruses.
COPD, which can further develop into pulmonary heart
disease and respiratory failure, is a type of chronic bronchitis
and/or emphysema characterized by airflow obstruction (90). It is related to the abnormal
inflammatory reaction of harmful gases and harmful particles. It is
associated with high rates of disability and fatality (91). Its global incidence rate in
patients over 40 years old has reached 9-10% (92). The underlying pathogenic factors
can be divided into two categories: External factors (environmental
factors) and internal factors (individual-specific factors for
susceptibility). External causes include smoking, inhalation of
dust and chemicals, air pollution, respiratory infections, and
lower socioeconomic status (possibly related to indoor and outdoor
air pollution, crowded rooms, poor nutrition, and other factors
associated with lower socioeconomic status). Internal causes
include genetic factors, increased reactivity with the airway, and
individuals with impaired lung development or growth attributed to
different reasons during pregnancy, and in neonates, infants and
children (93-95).
Preclinical data suggest that increased TGF-β1,
brain-derived neurotrophic factor, NLRP3, oxidant and mucus
production, as well as reduced sirtuin-1 and antioxidant levels,
suboptimal mitochondrial activity and dysfunction in the
endoplasmic reticulum are important in COPD (96). All of them may be substantially
improved by melatonin therapy. The protective effect of melatonin
on COPD relies on targeting MT1 or MT2 (97,98)
Melatonin improves the necroptosis by altering the LPS-induced
disordered pathways of alanine, aspartate and glutamate metabolism
(99-101).
In addition, it may also be associated with the PI3K/AKT signaling
pathway and neuroregulation of α7 nicotinic acetylcholine receptor
activity (102,103).
Lung cancer is a commonly occurring malignant tumor.
According to the International Agency for Research on Cancer,
almost one million new cases of lung cancer are registered
worldwide each year, and 60% of patients with lung cancer succumb
to the disease (104). The cause
of lung cancer is still not completely clear, a large amount of
data suggest that long-term smoking and lung cancer have a close
relationship (105,106). There are two types of lung
cancer: Small-cell lung cancer and NSCLC. NSCLC accounts for ~80%
of all lung cancer cases, and ~75% of these patients are first
diagnosed in the advanced stages, thereby having low 5-year
survival rates (104). The usual
treatment strategy is surgical resection along with adjuvant
platinum chemotherapy. However, chemotherapy, a proven therapy for
NSCLC, is often associated with toxicity, reducing its therapeutic
potential (107,108). Thus, it is essential to find
alternative and complementary treatment regimens with fewer adverse
effects and enhanced therapeutic properties. In a double-blind
randomized controlled trial, 100 patients with consecutively
untreated metastatic NSCLC were divided into chemotherapy only
[cisplatin, 20 mg/m/day, intravenous (i.v.); and etoposide, 100
mg/m/day, i.v.] or chemotherapy and melatonin (daily oral
administration for 7 consecutive days before chemotherapy; 20 mg
per day in the evening) groups. The results demonstrated that in
terms of the toxicity of treatment, patients treated with melatonin
could tolerate chemotherapy and the percentage of 5-year survival
(6%) was higher in patients who received melatonin treatment
compared with those (0%) receiving chemotherapy alone (109).
Melatonin restrains tumor cell proliferation by
suppressing the activating enhancer-binding protein-2β/human
telomerase reverse transcriptase signaling pathway and tumor growth
by regulating EGFR (110-114);
it exerts anti-metastatic roles by inhibiting the JNK/MAPK
signaling pathway, and induces its apoptotic properties through
regulating the balance of Bcl-2/Bax (114-116).
Possible mechanisms related to the anticancer effects of melatonin
are summarized in Table I
(110-120).
Pulmonary fibrosis is a terminal change in several
lung diseases, which is characterized by the proliferation of
fibroblasts and aggregation of the extracellular matrix (ECM), and
is accompanied by inflammation injury and destruction of tissue
structure. The normal alveolar tissue is damaged and failure to
properly repair leads to structural abnormalities (scar formation).
Fibrotic changes in different organ systems comprise four phases.
First is the onset of response, driven by the primary injury to
organs or tissues. Second is the activation of effector cells and
third is the elaboration of the ECM. The fourth phase is the
dynamic deposition (and insufficient resorption) of ECM, which
ultimately ends in end-organ failure (121-125).
To date, there is no effective treatment for this condition.
It has been reported that melatonin may serve a role
in pulmonary fibrosis by inhibiting fibrotic processes caused by
growth factors because of the important role of vascular
endothelial growth factor, fibroblast growth factor and
platelet-derived growth factor signaling pathways in pulmonary
fibrosis and inhibitory effects of these growth factors caused by
melatonin (131-134).
Endothelin, which is not only found in vascular endothelium but
also in various tissues and cells, is an important factor that
regulates cardiovascular function and serves an important role in
maintaining basic vascular tension and in the homeostasis of the
cardiovascular system (135).
Produced by endothelial cells, ET-1 is effective in constricting
blood vessels and bronchus and regulating inflammation and mitotic
activity (136). ET-1 regulates
signal transduction through two different G-protein-coupled
receptors, endothelin A and endothelin B. Melatonin can inhibit
ET-1 expression in focal cerebral ischemia (137). Melatonin reduces ischemic injury
by stabilizing vascular function with a strong inhibition of
endothelin converting enzyme-1, a zinc-dependent metalloprotease
involved in proteolysis of endothelin precursor to maturation of
ET-1(65). In addition, melatonin
also downregulates the expression and secretion of ET-1 through
inactivating FoxO1 and NF-κB transcription factors in colorectal
cancer cells and inhibits angiotensin II-induced secretion of
pro-inflammatory cytokines and oxidative stress caused by
mitochondrial dysfunction (66).
Overall, by inhibiting the Janus kinase/STAT signaling pathway and
angiotensin II-induced oxidative stress, melatonin may serve as an
ideal drug for treating pulmonary fibrosis in the future (138-142).
The present review discussed the beneficial effects
of melatonin in COVID-19, COPD, NSCLC and pulmonary fibrosis. A
growing body of evidence has already demonstrated that melatonin
has great potential in the treatment of pulmonary diseases.
Numerous animal and human studies have demonstrated that short-term
melatonin use is safe, even at extreme dosages (81,95).
To date, to the best of our knowledge, no study has reported any
serious side effects of exogenous melatonin administration
(143). Relative to a placebo
treatment, a randomized clinical study demonstrated that long-term
administration of melatonin induced only mild adverse effects
(144). These findings indicate
that melatonin is beneficial for patients with pulmonary diseases
if administered within the limits of a safe dosage (a single dose
of 1-10 mg). Therefore, studies should be designed to elucidate the
mechanisms of action of melatonin in pulmonary diseases.
Not applicable.
Funding: No funding was received.
Not applicable.
LL and XGo reviewed literature and wrote the
manuscript. XGa and JW reviewed and revised the manuscript. XGo
gave final approval for publication. All authors read and approved
the final version of the manuscript. Data authentication is not
applicable.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Huang K, Yang T, Xu J, Yang L, Zhao J,
Zhang X, Bai C, Kang J, Ran P, Shen H, et al: Prevalence, risk
factors, and management of asthma in China: A national
cross-sectional study. Lancet. 394:407–418. 2019.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Yach D, Hawkes C, Gould CL and Hofman KJ:
The global burden of chronic diseases: Overcoming impediments to
prevention and control. JAMA. 291:2616–2622. 2004.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Heron M, Hoyert DL, Murphy SL, Xu J,
Kochanek KD and Tejada-Vera B: Deaths: Final data for 2006. Natl
Vital Stat Rep. 57:1–134. 2009.PubMed/NCBI
|
|
4
|
Orens JB, Shearon TH, Freudenberger RS,
Conte JV, Bhorade SM and Ardehali A: Thoracic organ transplantation
in the United States, 1995-2004. Am J Transplant. 6 (5 Pt
2):1188–1197. 2006.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Trulock EP, Christie JD, Edwards LB,
Boucek MM, Aurora P, Taylor DO, Dobbels F, Rahmel AO, Keck BM and
Hertz MI: Registry of the International Society for Heart and Lung
Transplantation: Twenty-fourth official adult lung and heart-lung
transplantation report-2007. J Heart Lung Transplant. 26:782–795.
2007.PubMed/NCBI View Article : Google Scholar
|
|
6
|
O'Beirne S, Counihan IP and Keane MP:
Interstitial lung disease and lung transplantation. Semin Respir
Crit Care Med. 31:139–146. 2010.PubMed/NCBI View Article : Google Scholar
|
|
7
|
King TE Jr, Pardo A and Selman M:
Idiopathic pulmonary fibrosis. Lancet. 378:1949–1961.
2011.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Zhao D, Yu Y, Shen Y, Liu Q, Zhao Z,
Sharma R and Reiter RJ: Melatonin synthesis and function:
Evolutionary history in animals and plants. Front Endocrinol
(Lausanne). 10(249)2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Back K, Tan DX and Reiter RJ: Melatonin
biosynthesis in plants: Multiple pathways catalyze tryptophan to
melatonin in the cytoplasm or chloroplasts. J Pineal Res.
61:426–437. 2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Manchester LC, Coto-Montes A, Boga JA,
Andersen LP, Zhou Z, Galano A, Vriend J, Tan DX and Reiter RJ:
Melatonin: An ancient molecule that makes oxygen metabolically
tolerable. J Pineal Res. 59:403–419. 2015.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Hardeland R: Melatonin, hormone of
darkness and more: Occurrence, control mechanisms, actions and
bioactive metabolites. Cell Mol Life Sci. 65:2001–2018.
2008.PubMed/NCBI View Article : Google Scholar
|
|
12
|
De Luca V, Marineau C and Brisson N:
Molecular cloning and analysis of cDNA encoding a plant tryptophan
decarboxylase: Comparison with animal dopa decarboxylases. Proc
Natl Acad Sci USA. 86:2582–2586. 1989.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Park M, Kang K, Park S and Back K:
Conversion of 5-hydroxytryptophan into serotonin by tryptophan
decarboxylase in plants, Escherichia coli, and yeast. Biosci
Biotechnol Biochem. 72:2456–2458. 2008.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Tan DX, Manchester LC, Esteban-Zubero E,
Zhou Z and Reiter RJ: Melatonin as a potent and inducible
endogenous antioxidant: Synthesis and Metabolism. Molecules.
20:18886–18906. 2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Axelrod J and Weissbach H: Enzymatic
O-methylation of N-acetylserotonin to melatonin. Science.
131(1312)1960.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Kang K, Lee K, Park S, Byeon Y and Back K:
Molecular cloning of rice serotonin N-acetyltransferase, the
penultimate gene in plant melatonin biosynthesis. J Pineal Res.
55:7–13. 2013.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Byeon Y, Choi GH, Lee HY and Back K:
Melatonin biosynthesis requires N-acetylserotonin methyltransferase
activity of caffeic acid O-methyltransferase in rice. J Exp Bot.
66:6917–6925. 2015.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Byeon Y, Lee HJ, Lee HY and Back K:
Cloning and functional characterization of the Arabidopsis
N-acetylserotonin O-methyltransferase responsible for melatonin
synthesis. J Pineal Res. 60:65–73. 2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Klein DC: Arylalkylamine
N-acetyltransferase: ‘The Timezyme’. J Biol Chem. 282:4233–4237.
2007.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Favero G, Moretti E, Bonomini F, Reiter
RJ, Rodella LF and Rezzani R: Promising antineoplastic actions of
melatonin. Front Pharmacol. 9(1086)2018.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Reiter RJ, Rosales-Corral SA, Tan DX,
Acuna-Castroviejo D, Qin L, Yang SF and Xu K: Melatonin, a full
service anti-cancer agent: Inhibition of initiation, progression
and metastasis. Int J Mol Sci. 18(843)2017.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Sanchez-Barcelo EJ, Rueda N, Mediavilla
MD, Martinez-Cue C and Reiter RJ: Clinical uses of melatonin in
neurological diseases and mental and behavioural disorders. Curr
Med Chem. 24:3851–3878. 2017.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Cipolla-Neto J, Amaral FG, Afeche SC, Tan
DX and Reiter RJ: Melatonin, energy metabolism, and obesity: A
review. J Pineal Res. 56:371–381. 2014.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Favero G, Franceschetti L, Bonomini F,
Rodella LF and Rezzani R: Melatonin as an Anti-Inflammatory agent
modulating inflammasome activation. Int J Endocrinol.
2017(1835195)2017.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Ma N, Zhang J, Reiter RJ and Ma X:
Melatonin mediates mucosal immune cells, microbial metabolism, and
rhythm crosstalk: A therapeutic target to reduce intestinal
inflammation. Med Res Rev. 40:606–632. 2020.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Moradkhani F, Moloudizargari M, Fallah M,
Asghari N, Heidari Khoei H and Asghari MH: Immunoregulatory role of
melatonin in cancer. J Cell Physiol. 235:745–757. 2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Alghamdi BS: The neuroprotective role of
melatonin in neurological disorders. J Neurosci Res. 96:1136–1149.
2018.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Ji G, Zhou W, Li X, Du J, Li X and Hao H:
Melatonin inhibits proliferation and viability and promotes
apoptosis in colorectal cancer cells via upregulation of the
microRNA-34a/449a cluster. Mol Med Rep. 23(187)2021.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Al-Ghoul WM, Herman MD and Dubocovich ML:
Melatonin receptor subtype expression in human cerebellum.
Neuroreport. 9:4063–4068. 1998.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Klosen P, Lapmanee S, Schuster C,
Guardiola B, Hicks D, Pevet P and Felder-Schmittbuhl MP: MT1 and
MT2 melatonin receptors are expressed in nonoverlapping neuronal
populations. J Pineal Res. 67(e12575)2019.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Meléndez J, Maldonado V and Ortega A:
Effect of melatonin on beta-tubulin and MAP2 expression in NIE-115
cells. Neurochem Res. 21:653–658. 1996.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Lacoste B, Angeloni D, Dominguez-Lopez S,
Calderoni S, Mauro A, Fraschini F, Descarries L and Gobbi G:
Anatomical and cellular localization of melatonin MT1 and MT2
receptors in the adult rat brain. J Pineal Res. 58:397–417.
2015.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Ng KY, Leong MK, Liang H and Paxinos G:
Melatonin receptors: distribution in mammalian brain and their
respective putative functions. Brain Struct Funct. 222:2921–2939.
2017.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Gerbier R, Ndiaye-Lobry D, Martinez de
Morentin PB, Cecon E, Heisler LK, Delagrange P, Gbahou F and
Jockers R: Pharmacological evidence for transactivation within
melatonin MT2 and serotonin 5-HT2C receptor
heteromers in mouse brain. FASEB J. 35(e21161)2021.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Nosjean O, Ferro M, Coge F, Beauverger P,
Henlin JM, Lefoulon F, Fauchere JL, Delagrange P, Canet E and
Boutin JA: Identification of the melatonin-binding site MT3 as the
quinone reductase 2. J Biol Chem. 275:31311–31317. 2000.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Boutin JA and Ferry G: Is there sufficient
evidence that the melatonin binding site MT3 Is quinone
reductase 2? J Pharmacol Exp Ther. 368:59–65. 2019.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Hasan ZT, Atrakji DMQYMAA and Mehuaiden
DAK: The effect of melatonin on thrombosis, sepsis and mortality
rate in COVID-19 Patients. Int J Infect Dis. 114:79–84.
2022.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Ziaei A, Davoodian P, Dadvand H, Safa O,
Hassanipour S, Omidi M, Masjedi M, Mahmoudikia F, Rafiee B and
Fathalipour M: Evaluation of the efficacy and safety of Melatonin
in moderately ill patients with COVID-19: A structured summary of a
study protocol for a randomized controlled trial. Trials.
21(882)2020.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Medzhitov R: Origin and physiological
roles of inflammation. Nature. 454:428–435. 2008.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Kuprash DV and Nedospasov SA: Molecular
and cellular mechanisms of inflammation. Biochemistry (Mosc).
81:1237–1239. 2016.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Zarrin AA, Bao K, Lupardus P and Vucic D:
Kinase inhibition in autoimmunity and inflammation. Nat Rev Drug
Discov. 20:39–63. 2021.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Wang W and Gao J: Effects of melatonin on
protecting against lung injury (Review). Exp Ther Med.
21(228)2021.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Hardeland R: Melatonin and
inflammation-Story of a double-edged blade. J Pineal Res.
65(e12525)2018.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Mańka S and Majewska E: Immunoregulatory
action of melatonin. The mechanism of action and the effect on
inflammatory cells. Postepy Hig Med Dosw (Online). 70:1059–1067.
2016.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Hardeland R, Cardinali DP, Brown GM and
Pandi-Perumal SR: Melatonin and brain inflammaging. Prog Neurobiol.
127:–128. 46–63. 2015.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Steinhilber D, Brungs M, Werz O,
Wiesenberg I, Danielsson C, Kahlen JP, Nayeri S, Schräder M and
Carlberg C: The nuclear receptor for melatonin represses
5-lipoxygenase gene expression in human B lymphocytes. J Biol Chem.
270:7037–7040. 1995.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Garcia-Mauriño S, Gonzalez-Haba MG, Calvo
JR, Goberna R and Guerrero JM: Involvement of nuclear binding sites
for melatonin in the regulation of IL-2 and IL-6 production by
human blood mononuclear cells. J Neuroimmunol. 92:76–84.
1998.PubMed/NCBI View Article : Google Scholar
|
|
48
|
García-Mauriño S, Pozo D, Calvo JR and
Guerrero JM: Correlation between nuclear melatonin receptor
expression and enhanced cytokine production in human lymphocytic
and monocytic cell lines. J Pineal Res. 29:129–137. 2000.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Carrillo-Vico A, García-Mauriño S, Calvo
JR and Guerrero JM: Melatonin counteracts the inhibitory effect of
PGE2 on IL-2 production in human lymphocytes via its mt1 membrane
receptor. FASEB J. 17:755–757. 2003.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Lardone PJ, Carrillo-Vico A, Naranjo MC,
De Felipe B, Vallejo A, Karasek M and Guerrero JM: Melatonin
synthesized by Jurkat human leukemic T cell line is implicated in
IL-2 production. J Cell Physiol. 206:273–279. 2006.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Kuklina EM, Glebezdina NS and Nekrasova
IV: Role of melatonin in the regulation of differentiation of T
cells producing interleukin-17 (Th17). Bull Exp Biol Med.
160:656–658. 2016.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Kühlwein E and Irwin M: Melatonin
modulation of lymphocyte proliferation and Th1/Th2 cytokine
expression. J Neuroimmunol. 117:51–57. 2001.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Hardeland R, Reiter RJ, Poeggeler B and
Tan DX: The significance of the metabolism of the neurohormone
melatonin: Antioxidative protection and formation of bioactive
substances. Neurosci Biobehav Rev. 17:347–357. 1993.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Poeggeler B, Reiter RJ, Tan DX, Chen LD
and Manchester LC: Melatonin, hydroxyl radical-mediated oxidative
damage, and aging: A hypothesis. J Pineal Res. 14:151–168.
1993.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Reiter RJ: Functional pleiotropy of the
neurohormone melatonin: Antioxidant protection and neuroendocrine
regulation. Front Neuroendocrinol. 16:383–415. 1995.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Reiter RJ, Tan DX, Manchester LC,
Lopez-Burillo S, Sainz RM and Mayo JC: Melatonin: Detoxification of
oxygen and nitrogen-based toxic reactants. Adv Exp Med Biol.
527:539–548. 2003.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Tamura H, Jozaki M, Tanabe M, Shirafuta Y,
Mihara Y, Shinagawa M, Tamura I, Maekawa R, Sato S, Taketani T, et
al: Importance of melatonin in assisted reproductive technology and
ovarian aging. Int J Mol Sci. 21(1135)2020.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Moniruzzaman M, Ghosal I, Das D and
Chakraborty SB: Melatonin ameliorates
H2O2-induced oxidative stress through
modulation of Erk/Akt/NFkB pathway. Biol Res. 51(17)2018.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Lissoni P, Brivio O, Brivio F, Barni S,
Tancini G, Crippa D and Meregalli S: Adjuvant therapy with the
pineal hormone melatonin in patients with lymph node relapse due to
malignant melanoma. J Pineal Res. 21:239–242. 1996.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Blask DE, Sauer LA, Dauchy RT, Holowachuk
EW, Ruhoff MS and Kopff HS: Melatonin inhibition of cancer growth
in vivo involves suppression of tumor fatty acid metabolism via
melatonin receptor-mediated signal transduction events. Cancer Res.
59:4693–4701. 1999.PubMed/NCBI
|
|
61
|
Blask DE, Dauchy RT, Brainard GC and
Hanifin JP: Circadian stage-dependent inhibition of human breast
cancer metabolism and growth by the nocturnal melatonin signal:
Consequences of its disruption by light at night in rats and women.
Integr Cancer Ther. 8:347–353. 2009.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Blask DE, Hill SM, Dauchy RT, Xiang S,
Yuan L, Duplessis T, Mao L, Dauchy E and Sauer LA: Circadian
regulation of molecular, dietary, and metabolic signaling
mechanisms of human breast cancer growth by the nocturnal melatonin
signal and the consequences of its disruption by light at night. J
Pineal Res. 51:259–269. 2011.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Susa N, Ueno S, Furukawa Y, Ueda J and
Sugiyama M: Potent protective effect of melatonin on
chromium(VI)-induced DNA single-strand breaks, cytotoxicity, and
lipid peroxidation in primary cultures of rat hepatocytes. Toxicol
Appl Pharmacol. 144:377–384. 1997.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Tan DX, Pöeggeler B, Reiter RJ, Chen LD,
Chen S, Manchester LC and Barlow-Walden LR: The pineal hormone
melatonin inhibits DNA-adduct formation induced by the chemical
carcinogen safrole in vivo. Cancer Lett. 70:65–71. 1993.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Kilic E, Kilic U, Reiter RJ, Bassetti CL
and Hermann DM: Prophylactic use of melatonin protects against
focal cerebral ischemia in mice: Role of endothelin converting
enzyme-1. J Pineal Res. 37:247–251. 2004.PubMed/NCBI View Article : Google Scholar
|
|
66
|
León J, Casado J, Jiménez Ruiz SM, Zurita
MS, González-Puga C, Rejón JD, Gila A, Muñoz de Rueda P, Pavón EJ,
Reiter RJ, et al: Melatonin reduces endothelin-1 expression and
secretion in colon cancer cells through the inactivation of FoxO-1
and NF-κβ. J Pineal Res. 56:415–426. 2014.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Elmore S: Apoptosis: A review of
programmed cell death. Toxicol Pathol. 35:495–516. 2007.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Obeng E: Apoptosis (programmed cell death)
and its signals-A review. Braz J Biol. 81:1133–1143.
2021.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Jang MH, Jung SB, Lee MH, Kim CJ, Oh YT,
Kang I, Kim J and Kim EH: Melatonin attenuates amyloid
beta25-35-induced apoptosis in mouse microglial BV2 cells. Neurosci
Lett. 380:26–31. 2005.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Yoo YM, Yim SV, Kim SS, Jang HY, Lea HZ,
Hwang GC, Kim JW, Kim SA, Lee HJ, Kim CJ, et al: Melatonin
suppresses NO-induced apoptosis via induction of Bcl-2 expression
in PGT-beta immortalized pineal cells. J Pineal Res. 33:146–150.
2002.PubMed/NCBI View Article : Google Scholar
|
|
71
|
Joo SS and Yoo YM: Melatonin induces
apoptotic death in LNCaP cells via p38 and JNK pathways:
Therapeutic implications for prostate cancer. J Pineal Res.
47:8–14. 2009.PubMed/NCBI View Article : Google Scholar
|
|
72
|
Mayo JC, Sainz RM, Uría H, Antolín I,
Estéban MM and Rodríguez : Inhibition of cell proliferation:
A mechanism likely to mediate the prevention of neuronal cell death
by melatonin. J Pineal Res. 25:12–18. 1998.PubMed/NCBI View Article : Google Scholar
|
|
73
|
Han Z, Battaglia F and Terlecky SR:
Discharged COVID-19 patients testing positive again for SARS-CoV-2
RNA: A minireview of published studies from China. J Med Virol.
93:262–274. 2021.PubMed/NCBI View Article : Google Scholar
|
|
74
|
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu
Y, Zhang L, Fan G, Xu J, Gu X, et al: Clinical features of patients
infected with 2019 novel coronavirus in Wuhan, China. Lancet.
395:497–506. 2020.PubMed/NCBI View Article : Google Scholar
|
|
75
|
Salehi S, Abedi A, Balakrishnan S and
Gholamrezanezhad A: Coronavirus disease 2019 (COVID-19): A
systematic review of imaging findings in 919 patients. AJR Am J
Roentgenol. 215:87–93. 2020.PubMed/NCBI View Article : Google Scholar
|
|
76
|
Simko F, Hrenak J, Dominguez-Rodriguez A
and Reiter RJ: Melatonin as a putative protection against
myocardial injury in COVID-19 infection. Expert Rev Clin Pharmacol.
13:921–924. 2020.PubMed/NCBI View Article : Google Scholar
|
|
77
|
Tan DX and Hardeland R: Targeting host
defense system and rescuing compromised mitochondria to increase
tolerance against pathogens by melatonin may impact outcome of
deadly virus infection pertinent to COVID-19. Molecules.
25(4410)2020.PubMed/NCBI View Article : Google Scholar
|
|
78
|
Cross KM, Landis DM, Sehgal L and Payne
JD: Melatonin in early treatment for COVID-19: A narrative review
of current evidence and possible efficacy. Endocr Pract.
27:850–855. 2021.PubMed/NCBI View Article : Google Scholar
|
|
79
|
Zhou Y, Hou Y, Shen J, Mehra R, Kallianpur
A, Culver DA, Gack MU, Farha S, Zein J, Comhair S, et al: A network
medicine approach to investigation and population-based validation
of disease manifestations and drug repurposing for COVID-19. PLoS
Biol. 18(e3000970)2020.PubMed/NCBI View Article : Google Scholar
|
|
80
|
Reiter RJ, Abreu-Gonzalez P, Marik PE and
Dominguez-Rodriguez A: Therapeutic algorithm for use of melatonin
in patients with COVID-19. Front Med (Lausanne).
7(226)2020.PubMed/NCBI View Article : Google Scholar
|
|
81
|
Zhang R, Wang X, Ni L, Di X, Ma B, Niu S,
Liu C and Reiter RJ: COVID-19: Melatonin as a potential adjuvant
treatment. Life Sci. 250(117583)2020.PubMed/NCBI View Article : Google Scholar
|
|
82
|
Cardinali DP, Brown GM, Reiter RJ and
Pandi-Perumal SR: Elderly as a high-risk group during COVID-19
pandemic: Effect of circadian misalignment, sleep dysregulation and
melatonin administration. Sleep Vigil. 1–7. 2020.PubMed/NCBI View Article : Google Scholar : (Epub ahead of
print).
|
|
83
|
Huang SH, Cao XJ, Liu W, Shi XY and Wei W:
Inhibitory effect of melatonin on lung oxidative stress induced by
respiratory syncytial virus infection in mice. J Pineal Res.
48:109–116. 2010.PubMed/NCBI View Article : Google Scholar
|
|
84
|
Shneider A, Kudriavtsev A and Vakhrusheva
A: Can melatonin reduce the severity of COVID-19 pandemic? Int Rev
Immunol. 39:153–162. 2020.PubMed/NCBI View Article : Google Scholar
|
|
85
|
Campos LA, Cipolla-Neto J, Amaral FG,
Michelini LC, Bader M and Baltatu OC: The Angiotensin-melatonin
axis. Int J Hypertens. 2013(521783)2013.PubMed/NCBI View Article : Google Scholar
|
|
86
|
Zhang HM and Zhang Y: Melatonin: A
well-documented antioxidant with conditional pro-oxidant actions. J
Pineal Res. 57:131–146. 2014.PubMed/NCBI View Article : Google Scholar
|
|
87
|
Wang R, Hozumi Y, Yin C and Wei GW:
Mutations on COVID-19 diagnostic targets. Genomics. 112:5204–5213.
2020.PubMed/NCBI View Article : Google Scholar
|
|
88
|
Jia Z and Gong W: Will mutations in the
spike protein of SARS-CoV-2 lead to the failure of COVID-19
Vaccines? J Korean Med Sci. 36(e124)2021.PubMed/NCBI View Article : Google Scholar
|
|
89
|
Samudrala PK, Kumar P, Choudhary K, Thakur
N, Wadekar GS, Dayaramani R, Agrawal M and Alexander A: Virology,
pathogenesis, diagnosis and in-line treatment of COVID-19. Eur J
Pharmacol. 883(173375)2020.PubMed/NCBI View Article : Google Scholar
|
|
90
|
Raherison C and Girodet PO: Epidemiology
of COPD. Eur Respir Rev. 18:213–221. 2009.PubMed/NCBI View Article : Google Scholar
|
|
91
|
Negewo NA, Gibson PG and McDonald VM: COPD
and its comorbidities: Impact, measurement and mechanisms.
Respirology. 20:1160–1171. 2015.PubMed/NCBI View Article : Google Scholar
|
|
92
|
Vestbo J, Hurd SS, Agustí AG, Jones PW,
Vogelmeier C, Anzueto A, Barnes PJ, Fabbri LM, Martinez FJ,
Nishimura M, et al: Global strategy for the diagnosis, management,
and prevention of chronic obstructive pulmonary disease: GOLD
executive summary. Am J Respir Crit Care Med. 187:347–365.
2013.PubMed/NCBI View Article : Google Scholar
|
|
93
|
Buist AS, McBurnie MA, Vollmer WM,
Gillespie S, Burney P, Mannino DM, Menezes AM, Sullivan SD, Lee TA,
Weiss KB, et al: International variation in the prevalence of COPD
(the BOLD Study): A population-based prevalence study. Lancet.
370:741–750. 2007.PubMed/NCBI View Article : Google Scholar
|
|
94
|
Menn P, Heinrich J, Huber RM, Jörres RA,
John J, Karrasch S, Peters A, Schulz H and Holle R: KORA Study
Group. Direct medical costs of COPD-an excess cost approach based
on two population-based studies. Respir Med. 106:540–548.
2012.PubMed/NCBI View Article : Google Scholar
|
|
95
|
Yong W, Ma H, Na M, Gao T, Zhang Y, Hao L,
Yu H, Yang H and Deng X: Roles of melatonin in the field of
reproductive medicine. Biomed Pharmacother.
144(112001)2021.PubMed/NCBI View Article : Google Scholar
|
|
96
|
Mao K, Luo P, Geng W, Xu J, Liao Y, Zhong
H, Ma P, Tan Q, Xia H, Duan L, et al: An integrative transcriptomic
and metabolomic study revealed that melatonin plays a protective
role in chronic lung inflammation by reducing necroptosis. Front
Immunol. 12(668002)2021.PubMed/NCBI View Article : Google Scholar
|
|
97
|
Shin NR, Ko JW, Kim JC, Park G, Kim SH,
Kim MS, Kim JS and Shin IS: Role of melatonin as an SIRT1 enhancer
in chronic obstructive pulmonary disease induced by cigarette
smoke. J Cell Mol Med. 24:1151–1156. 2020.PubMed/NCBI View Article : Google Scholar
|
|
98
|
Shin NR, Park JW, Lee IC, Ko JW, Park SH,
Kim JS, Kim JC, Ahn KS and Shin IS: Melatonin suppresses fibrotic
responses induced by cigarette smoke via downregulation of TGF-β1.
Oncotarget. 8:95692–95703. 2017.PubMed/NCBI View Article : Google Scholar
|
|
99
|
Mahalanobish S, Dutta S, Saha S and Sil
PC: Melatonin induced suppression of ER stress and mitochondrial
dysfunction inhibited NLRP3 inflammasome activation in COPD mice.
Food Chem Toxicol. 144(111588)2020.PubMed/NCBI View Article : Google Scholar
|
|
100
|
Shin IS, Shin NR, Park JW, Jeon CM, Hong
JM, Kwon OK, Kim JS, Lee IC, Kim JC, Oh SR and Ahn KS: Melatonin
attenuates neutrophil inflammation and mucus secretion in cigarette
smoke-induced chronic obstructive pulmonary diseases via the
suppression of Erk-Sp1 signaling. J Pineal Res. 58:50–60.
2015.PubMed/NCBI View Article : Google Scholar
|
|
101
|
Hung MW, Yeung HM, Lau CF, Poon AMS, Tipoe
GL and Fung ML: Melatonin attenuates pulmonary hypertension in
chronically hypoxic rats. Int J Mol Sci. 18(1125)2017.PubMed/NCBI View Article : Google Scholar
|
|
102
|
Kim GD, Lee SE, Kim TH, Jin YH, Park YS
and Park CS: Melatonin suppresses acrolein-induced IL-8 production
in human pulmonary fibroblasts. J Pineal Res. 52:356–364.
2012.PubMed/NCBI View Article : Google Scholar
|
|
103
|
Pieper MP: The non-neuronal cholinergic
system as novel drug target in the airways. Life Sci. 91:1113–1118.
2012.PubMed/NCBI View Article : Google Scholar
|
|
104
|
Ferlay J, Colombet M, Soerjomataram I,
Parkin DM, Piñeros M, Znaor A and Bray F: Cancer statistics for the
year 2020: An overview. Int J Cancer. 2021.PubMed/NCBI View Article : Google Scholar : (Epub ahead of
print).
|
|
105
|
Carter-Harris L, Ceppa DP, Hanna N and
Rawl SM: Lung cancer screening: What do long-term smokers know and
believe? Health Expect. 20:59–68. 2017.PubMed/NCBI View Article : Google Scholar
|
|
106
|
Pinsky P and Gierada DS: Long-term cancer
risk associated with lung nodules observed on low-dose screening CT
scans. Lung Cancer. 139:179–184. 2020.PubMed/NCBI View Article : Google Scholar
|
|
107
|
Lemjabbar-Alaoui H, Hassan OU, Yang YW and
Buchanan P: Lung cancer: Biology and treatment options. Biochim
Biophys Acta. 1856:189–210. 2015.PubMed/NCBI View Article : Google Scholar
|
|
108
|
Vinod SK and Hau E: Radiotherapy treatment
for lung cancer: Current status and future directions. Respirology.
25 (Suppl 2):S61–S71. 2020.PubMed/NCBI View Article : Google Scholar
|
|
109
|
Lissoni P, Chilelli M, Villa S, Cerizza L
and Tancini G: Five years survival in metastatic non-small cell
lung cancer patients treated with chemotherapy alone or
chemotherapy and melatonin: A randomized trial. J Pineal Res.
35:12–15. 2003.PubMed/NCBI View Article : Google Scholar
|
|
110
|
García-Navarro A, González-Puga C, Escames
G, López LC, López A, López-Cantarero M, Camacho E, Espinosa A,
Gallo MA and Acuña-Castroviejo D: Cellular mechanisms involved in
the melatonin inhibition of HT-29 human colon cancer cell
proliferation in culture. J Pineal Res. 43:195–205. 2007.PubMed/NCBI View Article : Google Scholar
|
|
111
|
Tam CW, Mo CW, Yao KM and Shiu SY:
Signaling mechanisms of melatonin in antiproliferation of
hormone-refractory 22Rv1 human prostate cancer cells: Implications
for prostate cancer chemoprevention. J Pineal Res. 42:191–202.
2007.PubMed/NCBI View Article : Google Scholar
|
|
112
|
Benítez-King G, Soto-Vega E and
Ramírez-Rodriguez G: Melatonin modulates microfilament phenotypes
in epithelial cells: Implications for adhesion and inhibition of
cancer cell migration. Histol Histopathol. 24:789–799.
2009.PubMed/NCBI View Article : Google Scholar
|
|
113
|
Mediavilla MD, Cos S and Sánchez-Barceló
EJ: Melatonin increases p53 and p21WAF1 expression in MCF-7 human
breast cancer cells in vitro. Life Sci. 65:415–420. 1999.PubMed/NCBI View Article : Google Scholar
|
|
114
|
Zhou Q, Gui S, Zhou Q and Wang Y:
Melatonin inhibits the migration of human lung adenocarcinoma A549
cell lines involving JNK/MAPK pathway. PloS One.
9(e101132)2014.PubMed/NCBI View Article : Google Scholar
|
|
115
|
Haus E, Dumitriu L, Nicolau GY, Bologa S
and Sackett-Lundeen L: Circadian rhythms of basic fibroblast growth
factor (bFGF), epidermal growth factor (EGF), insulin-like growth
factor-1 (IGF-1), insulin-like growth factor binding protein-3
(IGFBP-3), cortisol, and melatonin in women with breast cancer.
Chronobiol Int. 18:709–727. 2001.PubMed/NCBI View Article : Google Scholar
|
|
116
|
Fan C, Pan Y, Yang Y, Di S, Jiang S, Ma Z,
Li T, Zhang Z, Li W, Li X, et al: HDAC1 inhibition by melatonin
leads to suppression of lung adenocarcinoma cells via induction of
oxidative stress and activation of apoptotic pathways. J Pineal
Res. 59:321–333. 2015.PubMed/NCBI View Article : Google Scholar
|
|
117
|
Wang J, Xiao X, Zhang Y, Shi D, Chen W, Fu
L, Liu L, Xie F, Kang T, Huang W and Deng W: Simultaneous
modulation of COX-2, p300, Akt, and Apaf-1 signaling by melatonin
to inhibit proliferation and induce apoptosis in breast cancer
cells. J Pineal Res. 53:77–90. 2012.PubMed/NCBI View Article : Google Scholar
|
|
118
|
Lu JJ, Fu L, Tang Z, Zhang C, Qin L, Wang
J, Yu Z, Shi D, Xiao X, Xie F, et al: Melatonin inhibits
AP-2β/hTERT, NF-κB/COX-2 and Akt/ERK and activates caspase/Cyto C
signaling to enhance the antitumor activity of berberine in lung
cancer cells. Oncotarget. 7:2985–3001. 2016.PubMed/NCBI View Article : Google Scholar
|
|
119
|
Carrillo-Vico A, Calvo JR, Abreu P,
Lardone PJ, García-Mauriño S, Reiter RJ and Guerrero JM: Evidence
of melatonin synthesis by human lymphocytes and its physiological
significance: possible role as intracrine, autocrine, and/or
paracrine substance. FASEB J. 18:537–539. 2004.PubMed/NCBI View Article : Google Scholar
|
|
120
|
Reiter RJ, Tan DX, Sainz RM, Mayo JC and
Lopez-Burillo S: Melatonin: Reducing the toxicity and increasing
the efficacy of drugs. J Pharm Pharmacol. 54:1299–1321.
2002.PubMed/NCBI View Article : Google Scholar
|
|
121
|
Rockey DC, Bell PD and Hill JA: Fibrosis-a
common pathway to organ injury and failure. N Engl J Med.
372:1138–1149. 2015.PubMed/NCBI View Article : Google Scholar
|
|
122
|
Birbrair A, Zhang T, Wang ZM, Messi ML,
Mintz A and Delbono O: Type-1 pericytes participate in fibrous
tissue deposition in aged skeletal muscle. Am J Physiol Cell
Physiol. 305:C1098–C1113. 2013.PubMed/NCBI View Article : Google Scholar
|
|
123
|
Drobnik J, Karbownik-Lewińska M,
Szczepanowska A, Słotwińska D, Olczak S, Jakubowski L and Dabrowski
R: Regulatory influence of melatonin on collagen accumulation in
the infarcted heart scar. J Pineal Res. 45:285–290. 2008.PubMed/NCBI View Article : Google Scholar
|
|
124
|
Di Lullo GA, Sweeney SM, Korkko J,
Ala-Kokko L and San Antonio JD: Mapping the ligand-binding sites
and disease-associated mutations on the most abundant protein in
the human, type I collagen. J Biol Chem. 277:4223–4231.
2002.PubMed/NCBI View Article : Google Scholar
|
|
125
|
Pugazhenthi K, Kapoor M, Clarkson AN, Hall
I and Appleton I: Melatonin accelerates the process of wound repair
in full-thickness incisional wounds. J Pineal Res. 44:387–396.
2008.PubMed/NCBI View Article : Google Scholar
|
|
126
|
Ding Z, Wu X, Wang Y, Ji S, Zhang W, Kang
J, Li J and Fei G: Melatonin prevents LPS-induced
epithelial-mesenchymal transition in human alveolar epithelial
cells via the GSK-3β/Nrf2 pathway. Biomed Pharmacother.
132(110827)2020.PubMed/NCBI View Article : Google Scholar
|
|
127
|
Yildirim Z, Kotuk M, Erdogan H, Iraz M,
Yagmurca M, Kuku I and Fadillioglu E: Preventive effect of
melatonin on bleomycin-induced lung fibrosis in rats. J Pineal Res.
40:27–33. 2006.PubMed/NCBI View Article : Google Scholar
|
|
128
|
Genovese T, Di Paola R, Mazzon E, Muià C,
Caputi AP and Cuzzocrea S: Melatonin limits lung injury in
bleomycin treated mice. J Pineal Res. 39:105–112. 2005.PubMed/NCBI View Article : Google Scholar
|
|
129
|
Karimfar MH, Rostami S, Haghani K,
Bakhtiyari S and Noori-Zadeh A: Melatonin alleviates
bleomycin-induced pulmonary fibrosis in mice. J Biol Regul Homeost
Agents. 29:327–334. 2015.PubMed/NCBI
|
|
130
|
Hosseinzadeh A, Javad-Moosavi SA, Reiter
RJ, Hemati K, Ghaznavi H and Mehrzadi S: Idiopathic pulmonary
fibrosis (IPF) signaling pathways and protective roles of
melatonin. Life Sci. 201:17–29. 2018.PubMed/NCBI View Article : Google Scholar
|
|
131
|
Alvarez-García V, González A,
Alonso-González C, Martínez-Campa C and Cos S: Antiangiogenic
effects of melatonin in endothelial cell cultures. Microvasc Res.
87:25–33. 2013.PubMed/NCBI View Article : Google Scholar
|
|
132
|
Alvarez-García V, González A,
Alonso-González C, Martínez-Campa C and Cos S: Regulation of
vascular endothelial growth factor by melatonin in human breast
cancer cells. J Pineal Res. 54:373–380. 2013.PubMed/NCBI View Article : Google Scholar
|
|
133
|
Song J, Kang SM, Lee WT, Park KA, Lee KM
and Lee JE: The beneficial effect of melatonin in brain endothelial
cells against oxygen-glucose deprivation followed by
reperfusion-induced injury. Oxid Med Cell Longev.
2014(639531)2014.PubMed/NCBI View Article : Google Scholar
|
|
134
|
Crespo I, San-Miguel B, Fernández A, Ortiz
de Urbina J, González-Gallego J and Tuñón MJ: Melatonin limits the
expression of profibrogenic genes and ameliorates the progression
of hepatic fibrosis in mice. Transl Res. 165:346–357.
2015.PubMed/NCBI View Article : Google Scholar
|
|
135
|
Czechowska G, Celinski K, Korolczuk A,
Wojcicka G, Dudka J, Bojarska A and Reiter RJ: Protective effects
of melatonin against thioacetamide-induced liver fibrosis in rats.
J Physiol Pharmacol. 66:567–579. 2015.PubMed/NCBI
|
|
136
|
Yip HK, Chang YC, Wallace CG, Chang LT,
Tsai TH, Chen YL, Chang HW, Leu S, Zhen YY, Tsai CY, et al:
Melatonin treatment improves adipose-derived mesenchymal stem cell
therapy for acute lung ischemia-reperfusion injury. J Pineal Res.
54:207–221. 2013.PubMed/NCBI View Article : Google Scholar
|
|
137
|
Finsnes F, Skjønsberg OH, Lyberg T and
Christensen G: Endothelin-1 production is associated with
eosinophilic rather than neutrophilic airway inflammation. Eur
Respir J. 15:743–750. 2000.PubMed/NCBI View Article : Google Scholar
|
|
138
|
Ji ZZ and Xu YC: Melatonin protects
podocytes from angiotensin II-induced injury in an in vitro
diabetic nephropathy model. Mol Med Rep. 14:920–926.
2016.PubMed/NCBI View Article : Google Scholar
|
|
139
|
Montero P, Milara J, Roger I and Cortijo
J: Role of JAK/STAT in interstitial lung diseases; Molecular and
cellular mechanisms. Int J Mol Sci. 22(6211)2021.PubMed/NCBI View Article : Google Scholar
|
|
140
|
Wang J, Chen L, Chen B, Meliton A, Liu SQ,
Shi Y, Liu T, Deb DK, Solway J and Li YC: Chronic activation of the
renin-angiotensin system induces lung fibrosis. Sci Rep.
5(15561)2015.PubMed/NCBI View Article : Google Scholar
|
|
141
|
Li X, Molina-Molina M, Abdul-Hafez A,
Ramirez J, Serrano-Mollar A, Xaubet A and Uhal BD: Extravascular
sources of lung angiotensin peptide synthesis in idiopathic
pulmonary fibrosis. Am J Physiol Lung Cell Mol Physiol.
291:L887–L895. 2006.PubMed/NCBI View Article : Google Scholar
|
|
142
|
Uhal BD, Dang MT, Li X and Abdul-Hafez A:
Angiotensinogen gene transcription in pulmonary fibrosis. Int J
Pept. 2012(875910)2012.PubMed/NCBI View Article : Google Scholar
|
|
143
|
Andersen LP, Gögenur I, Rosenberg J and
Reiter RJ: The safety of melatonin in humans. Clin Drug Investig.
36:169–175. 2016.PubMed/NCBI View Article : Google Scholar
|
|
144
|
Habtemariam S, Daglia M, Sureda A,
Selamoglu Z, Gulhan MF and Nabavi SM: Melatonin and respiratory
diseases: A review. Curr Top Med Chem. 17:467–488. 2017.PubMed/NCBI View Article : Google Scholar
|