Introduction
Although it has previously been established that
coronaviruses infect humans and generate mild respiratory
infections (1), severe acute
respiratory syndrome coronavirus 2 (SARS-CoV-2), the newly
identified member of the betacoronaviruses, is responsible for the
most significant pandemic since the Spanish flu pandemic of
1918-1920(2).
SARS-CoV-2 has a large RNA genome and a complex
antigenic profile (3). Due to its
genetic profile, the large number of infected patients and the
immunological pressure, the virus exhibits the ability to mutate
and novel variants can elude the natural or vaccine-generated
antibody response (3,4). The onset of the current pandemic
occurred with great speed; since 2019, >363 million cases have
been confirmed worldwide, with ~2 million in Romania. Despite the
fact the lethality of the disease is currently <2% worldwide and
2.87% in Romania (5), in specific
patient categories (6), for
example patients within an ageing population or with comorbidities,
patients with an absence of previous immunization, or those in
overwhelmed public health systems, this figure may be much higher.
In addition, patients who recover from this disease may present
with long-term complications [long coronavirus disease 2019
(COVID-19)] (7). Notably, despite
quarantine mechanisms in place, the virus remains and continues to
pose a serious threat to public health.
COVID-19 exhibits a wide array of clinical
manifestations. Originating in China as a predominantly respiratory
disease (8), at present it is
regarded a disease involving almost any organ or system. Symptoms
vary according to individual factors, including age, genetic
background, comorbidities and the viral subtype involved (9-11).
The evolution of certain diseases is often difficult to predict.
However, numerous early risk factors for the development of a
severe form of disease had been proposed (10) and may help to promote the correct
management of the patient.
Despite ethical barriers for investigation in human
subjects (12), research has been
dedicated to the development of safe vaccines (13,14)
and effective antiviral therapies to target this disease (15,16).
The interactions between SARS-CoV-2 and the immune
system remain a key focus of current research, to improve
understanding of the pathogenesis and effect that COVID-19 may have
on patients. Antibody responses serve a primary role in protecting
individuals against SARS-CoV-2, particularly by the activity of
neutralizing antibodies that can block viral infection (17). Specific immune response to viral
antigens involves the action of lymphocytes, including B cells and
T cells, chemokines, cytokines and antigen-neutralizing
immunoglobulin (Ig)A (18). The
potency of IgA is highlighted in various sites of the body,
including the saliva, blood or bronchoalveolar lavage in the first
stage of COVID-19 disease. Thus, the presence of SARS-CoV-2
neutralization in the first weeks following symptom onset is more
closely associated with IgA, than IgM or IgG antibodies (19). Elevated titers of IgG antibodies
are essential for developing immune memory in order to prevent
reinfection. The specific type of IgG against SARS-CoV-2 following
infection remains undetermined; however, results of a previous
study highlighted a decrease in IgG antibodies in week 5-7 after
infection, that only continued for 1-2 weeks (20).
The present study aimed to evaluate the presence of
IgA and IgG SARS-CoV-2 antibodies in patients with COVID-19 that
had been confirmed using reverse transcription-quantitative (RT-q)
PCR. The main purpose of the present study was to analyse
SARS-CoV-2-specific IgA detection and associate it to the clinical
course of COVID-19 and the inflammatory response of patients.
Materials and methods
Study population
A cross-sectional study involving 75 consecutive
patients was conducted. A total of 40 (53.33%) males and 35
(46.67%) females that were hospitalized during October 2020 in
Sfanta Parascheva Infectious Diseases Hospital of Iași, Romania
were included. Demographic data, including age, sex, occupation and
residential region of each participant, were collected. All
patients were confirmed positive for COVID-19 via SARS-CoV-2
detection in nasopharyngeal swabs using RT-qPCR.
Detection of SARS-CoV-2
antibodies
After obtaining written informed consent from all
patients, serum samples were collected (between 7 and 28 days
post-onset of symptoms) and ELISA kits were used for the detection
of anti-SARS-CoV-2 (cat. nos. EI 2606-9601 A and EI 2606-9601 G;
EUROIMMUN AG), in order to provide semi-quantitative in
vitro determination of IgA and IgG against SARS-CoV-2. Each kit
contained microplate strip wells coated with a recombinant
structural protein of SARS-CoV-2: S1 domain of spike protein
expressed in the human embryonic kidney cell line (293 cells).
Semi-quantitative evaluation of the results was calculated using
the following formula: Optical density (OD) ratio of the extinction
of the control or patient sample over the extinction of the
calibrator. The result was interpreted as recommended by the
manufacturer: <0.8 for negative samples; ≥0.8 to <1.0 as
borderline and >1.1 for positive samples. Diagnostic sensitivity
of the ELISA kit to anti-SARS-CoV-2 IgA in samples taken between
day 10 and 20 following symptom onset was determined by the
manufacturer and amounted to 91.7%. In samples taken after >20
days, the sensitivity of the ELISA kit amounted to 100%. The
specificity of the ELISA kit to anti-SARS-CoV-2 IgA amounted to
88.2 and 82.4% during the aforementioned timeframes, respectively.
In samples obtained between day 10 and 20 after symptom onset, the
sensitivity of the ELISA kit to anti-SARS-CoV-2 IgG declared by the
manufacturer amounted to 75 and 99% for specificity.
Following serological testing, the patients were
split into two groups; namely, group 1: Positive for IgA
anti-SARS-CoV-2 (n=54) and group 2: negative for IgA
anti-SARS-CoV-2 (n=21). Blood collection was performed between the
7 and 14th day following disease onset, in order to evaluate the
presence of IgA anti SARS-CoV-2. Results revealed 77.8% in group 1,
compared with 85.7% in group 2 (Table
I).
 | Table IEvaluation of the presence of IgA anti
SARS-CoV-2 and the stage of the infection. |
Table I
Evaluation of the presence of IgA anti
SARS-CoV-2 and the stage of the infection.
| | Between 7-14 day of
evolution | After the 14 days of
evolution |
|---|
| Group | No. of patients | % | Mean | No. of patients | % | Mean |
|---|
| Group 1 (anti
SARS-CoV-2 IgA positive) | 42 | 77.8 | 10 | 12 | 22.2 | 16 |
| Group 2 (anti
SARS-CoV-2 IgA negative) | 18 | 85.7 | 9 | 3 | 14.3 | 15 |
Other laboratory/imagistic tests
All patients included in the study were also
examined using an imaging system, such as computerized tomography
scans or chest radiography and evaluated for blood inflammatory
markers, liver transaminase levels (RX Imola analyzer) and
hematological parameters (fully automated bidirectionally analyzer
fluorescence & flow cytometry-Sysmex xn550). These included the
mean leukocyte count, percentage of neutrophils, mean neutrophil
count and mean platelet count.
Statistical analysis
Statistical analysis was performed using Analyse-it
Add-on for Microsoft Excel (Analyse-it Software, Ltd.). Descriptive
data are presented as absolute values, percentages and means.
Differences between groups were tested for statistical significance
using unpaired T-Student and χ2 square tests. P<0.05
was considered to indicate a statistically significant
difference.
Results
Demographic and clinical
characteristics of the patients
The comparative demographic and clinical
characteristics of the patients from the two groups are displayed
in Table II.
| Table IIPatient clinical and demographic
characteristics. |
Table II
Patient clinical and demographic
characteristics.
| Characteristic | Group 1 (positive for
IgA anti SARS-CoV-2) | Group 2 (negative for
IgA anti SARS-CoV-2) | P-value |
|---|
| Median age
(years) | 63 | 67 | 0.59 |
| Sex ratio
(M/F) | 0.75 | 1.08 | 0.66 |
| Hospitalization
period (days) | 11.1 | 10.5 | 0.49 |
| Fever (>38˚C,
%) | 81.1 | 83.4 | 0.72 |
| Cough (%) | 90.5 | 93.4 | 0.61 |
| Anosmia/Ageusia
(%) | 33.3 | 38.4 | 0.51 |
| Pneumonia (%) | 85.2 | 90.3 | 0.46 |
The age of IgA anti-SARS-CoV-2 positive patients
ranged from 40-88 years, with a median age of 63 years. Among the
patients with detectable antibodies, 42.6% were >65 years old.
Group 2 (negative for IgA anti SARS-CoV-2) included hospitalized
patients aged between 23-101 years old, with a median age of 67
years. Among the patients who did not present with SARS-CoV-2
detectable antibodies, 66.7% were >65 years of age. Analysis of
sex distribution indicated that males were dominant over females in
group 2 [male (M)/female (F), 1.08], compared with a higher number
of female patients in group 1 (M/F, 0.75), but the difference was
not statistically significant. In addition, almost no differences
were noted regarding the frequency of the main clinical
manifestations of the disease; namely, fever, cough, anosmia or
ageusia between the two groups (Table
II). Radiologically detectable pneumonia was present in most
patients in both groups (85.2 vs. 90.3%) and the hospitalization
period of both groups of patients was comparable (11 vs. 10
days).
In order to further evaluate the presence of IgA
anti-SARS-CoV-2, all patients included in the study were evaluated
for existing comorbidities (Table
III). Infections are often associated with comorbidities that
increase the risk of certain medical conditions; thus, leading to a
higher severity of the disease.
| Table IIIComorbidities in patients with
COVID-19. |
Table III
Comorbidities in patients with
COVID-19.
| | Group 1 (positive
for anti-SARS-CoV-2 IgA) | Group 2 (negative
for anti-SARS-CoV-2 IgA) | |
|---|
| Characteristic | No. of
patients | % | No. of
patients | % | P-value |
|---|
| Without
comorbidities | 11 | 20.4 | 2 | 9.5 | P=0.26 |
| With
comorbidities | 43 | 79.6 | 19 | 90.5 | |
Hematological and biochemical
characteristics of the patients
Disturbance of the immune system in patients with
COVID-19 has been considered as one of the distinctive features of
SARS-CoV-2 infection, particularly lymphopenia (21). Results of a previous study
demonstrated that SARS-CoV-2 infection is not only a pulmonary
disease, but also a systemic inflammatory illness (7). Key laboratory parameters of the
patients included in the present study are detailed in Table IV.
| Table IVResults of blood tests obtained from
all evaluated patients. |
Table IV
Results of blood tests obtained from
all evaluated patients.
| Variable | Group 1 (positive
for anti-SARS-CoV-2 IgA) | Group 2 (negative
for anti-SARS-CoV-2 IgA) | P-value |
|---|
| Mean leukocyte
count (/mm3) | 6,390 | 6,050 | 0.7 |
| Percent of
neutrophils | 72.4 | 73.5 | 0.76 |
| Mean neutrophils
count (/mm3) | 4726.8 | 4848.0 | 0.87 |
| Mean platelet count
(/mm3) | 216,157.6 | 184,907.1 | 0.22 |
| Mean ALT
(UI/l) | 37.6 | 39.8 | 0.79 |
| Mean CRP
(mg/l) | 68.2 | 55.2 | 0.48 |
IgA, IgG anti SARS-COV-2 antibodies
and clinical severity
The illness severity among symptomatic infections
varied widely, from mild cases to critical ones with respiratory
failure, or dysfunction of multiple other organ systems. In the
present study, the association between the presence of IgA
anti-SARS-CoV-2 antibodies and disease severity revealed
significant differences between the two groups (Table V).
| Table VClinical evaluation of patients with
COVID-19 and the presence of IgA anti-SARS-CoV-2. |
Table V
Clinical evaluation of patients with
COVID-19 and the presence of IgA anti-SARS-CoV-2.
| | Group 1 (positive
for anti-SARS-CoV-2 IgA) | Group 2 (negative
for anti-SARS-CoV-2 IgA) | |
|---|
| Disease
severity | No. of
patients | % | No. of
patients | % | P-value |
|---|
| Mild | 7 | 12.9 | 0 | 0 | 0.037 |
| Moderate | 30 | 55.6 | 18 | 85.7 | |
| Severe | 17 | 31.5 | 3 | 14.3 | |
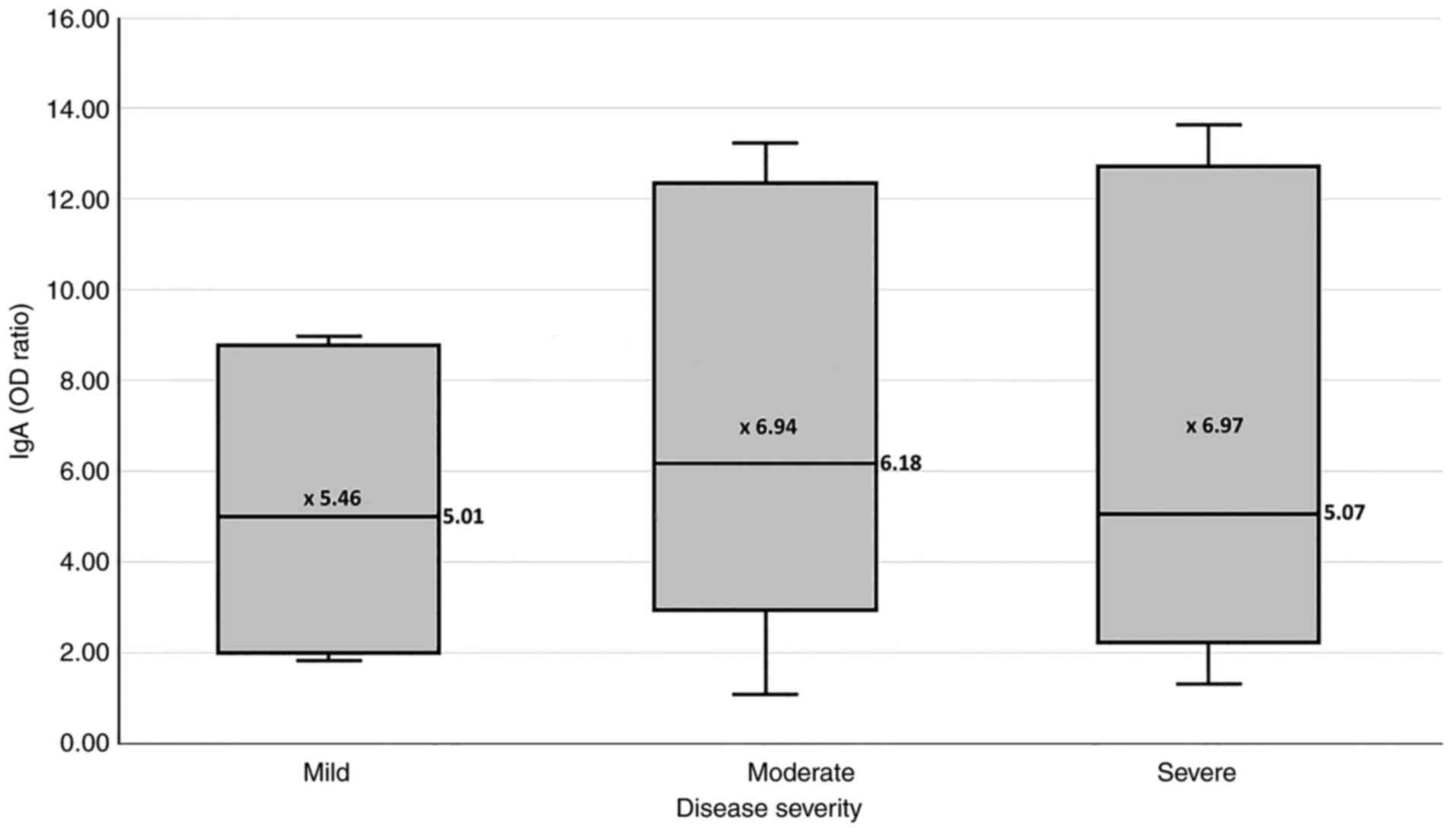
No significant differences were determined between
the ODs for IgA anti SARS-CoV-2 of the patient samples and disease
severity. Notably, mild forms were established at 5.45, compared
with medium forms at 6.94 and severe forms at 6.97 (P=0.98;
Fig. 1).
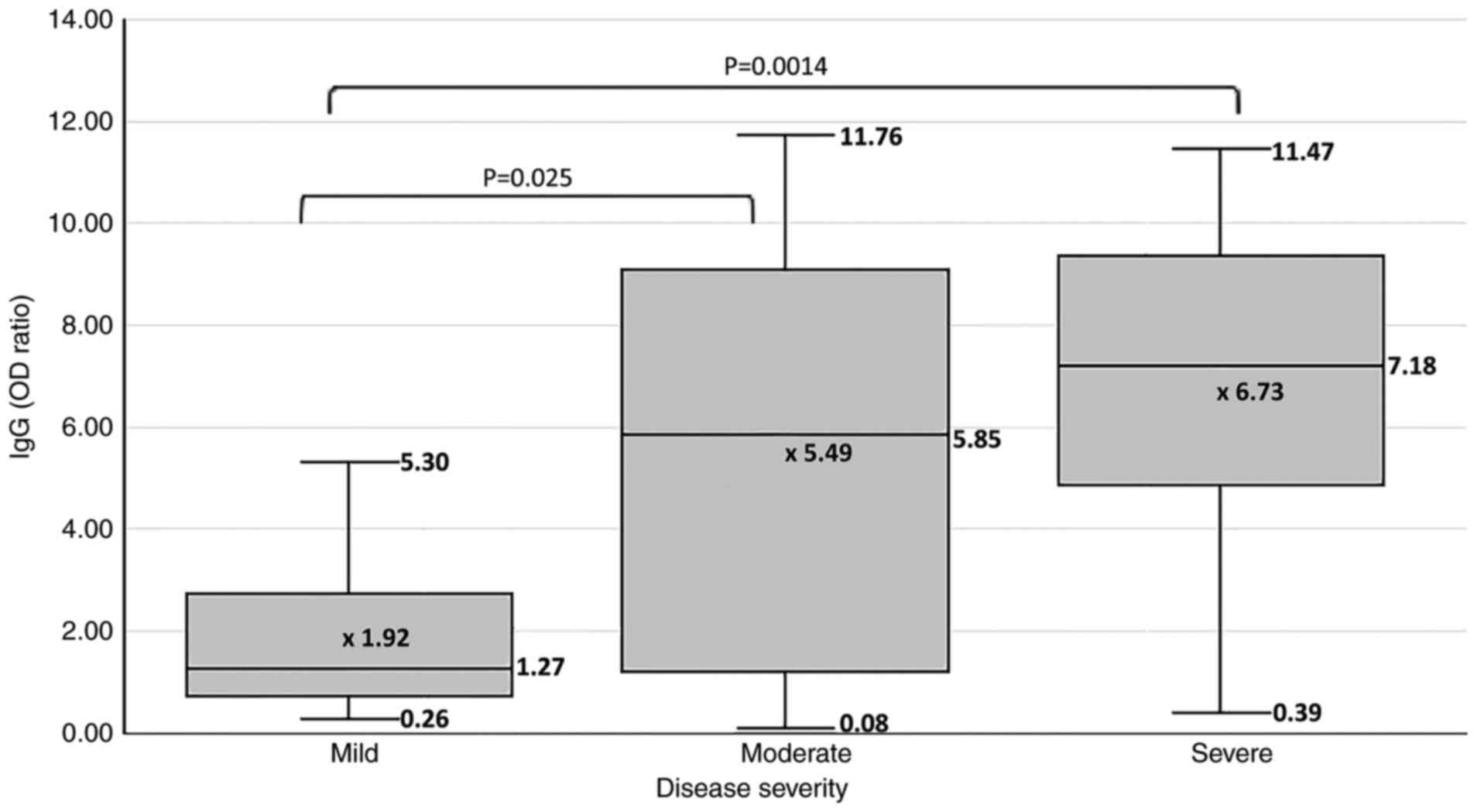
Patients who developed moderate to severe disease
exhibited significantly higher ODs for anti-SARS-CoV-2 IgG
antibodies than those with mild disease (1.27 vs. 5.49 vs. 6.73;
Fig. 2).
Antibody detection was comparable in most cases; in
the IgA positive group, 79.7% of patients presented with both types
of antibodies and in the IgA negative group, 80.9% of patients were
also IgG negative (Table VI).
| Table VISummary of SARS CoV-2 RNA-positive
hospitalized patients (n=75) blood test results and clinical forms
of the disease. |
Table VI
Summary of SARS CoV-2 RNA-positive
hospitalized patients (n=75) blood test results and clinical forms
of the disease.
| A, SARS CoV-2
IgA-positive patients (n=54) |
|---|
| Parameter | No. of
patients |
|---|
| Disease
severity | |
|
Mild
disease | 7 |
|
Moderate
disease | 30 |
|
Severe
disease | 17 |
| SARS CoV-2 IgG
status | |
|
IgG-positive | 43 |
|
IgG-negative | 11 |
| B, SARS CoV-2
IgA-negative patients (n=21) |
| Parameter | No. of
patients |
| Disease
severity | |
|
Mild
disease | 0 |
|
Moderate
disease | 18 |
|
Severe
disease | 3 |
| SARS CoV-2 IgG
status | |
|
IgG-positive | 4 |
|
IgG-negative | 17 |
Discussion
The clinical manifestations following SARS-CoV-2
infection vary in severity, from asymptomatic, to mild, moderate or
severe respiratory disease and multi-organ failure requiring
intensive care. The course of infection depends mainly on the
individual immune responses and is therefore difficult to predict.
The main objective of the present study was to evaluate the
association between IgA anti SARS-Cov-2 antibodies and the severity
of disease in early COVID-19 infection. In addition, the
association of age, sex, laboratory variables and duration of
symptoms with the presence of IgA antibodies were investigated.
Coronaviruses are recognized as having the largest
RNA genomes, which are transcribed by 14 different lengths of open
reading frames (1). This aspect
increases the chance of mutagenesis and the efficacy of viral
replication and decreases the possibility of being eliminated by
the immune system (22,23). The spike glycoprotein is a fusion
protein responsible for initiating SARS-CoV-2 entry into
susceptible cells by binding to cell receptors. The spike comprises
two functional subunits that enable viral attachment to the surface
of host cells (S1 subunit) and the fusion of the viral envelope and
cellular membranes (S2 subunit). Once inside the cell, the virus
replicates its RNA genome using the replicase gene (24). Coronavirus recombination serves an
important role in viral evolution, favoring the appearance of novel
strains with unpredictable consequences for animals and humans.
These viruses have an extensive range of natural origins and can
cause respiratory, hepatic, enteric and neurologic diseases
(25).
IgA antibody constitutes 15-20% of the total
immunoglobulins circulating in human serum. IgA is present in blood
and mucous secretions. The essential biological function is to
protect the body against molecular antigens that could be absorbed,
mainly by endocytosis. This immunoglobulin constitutes the first
line of defense against infection by blocking viral adhesion to
epithelial cell receptors (26).
IgA is also involved in pathogen or antigen elimination through an
IgA-mediated excretory pathway, characterized by the development of
a poly-immunoglobulin receptor-mediated transport of immune
complexes (27). The specific
humoral responses against SARS-CoV-2 spike-1 receptor-binding
domain (RBD) and nucleocapsid proteins indicate that in a
significant number of patients, neutralizing IgG and IgA antibodies
were detected within 2-3 weeks from the initial onset of symptoms.
Subsequently, the levels of neutralizing anti-RBD IgG increased
until the fourth week following symptom onset after a plateau,
whereas IgA levels decreased by day 28(28).
Antibodies targeting various virus-encoded proteins
are central players in conveying protective immunity against viral
infections such as SARS-CoV-2. Antibody detectability has broadly
been associated with COVID-19 severity (29); thus, IgA and IgG antibody detection
following seroconversion provides data for further understanding
the dynamics of the immune response to infection. Accurate
interpretation of serology tests depends on antigen specificity. In
the present study, anti-spike antibody assays were used,
demonstrating high-fidelity performance characteristics. These data
can be used to guide epidemiology and seroprevalence studies;
however, the specific length of time for which these antibodies
stay detectable and in what specific populations remains to be
fully elucidated. Although the diagnostic uses of serological
testing in the acute phase of illness is limited, it may be useful
for identifying symptomatic patients suspected of suffering with
long COVID-19. In addition, detection of IgA and IgG antibodies
against SARS-CoV-2 spike protein may be a useful tool for
evaluating SARS-CoV-2 infection in patients with PCR-positive
COVID-19, mainly in asymptomatic cases and in patients with a low
viral load (30). In addition,
immunoassays are useful in post-infection immunity evaluation and
also in analyzing the efficacy of vaccines. In patients with
PCR-confirmed SARS-CoV-2 infection in the present study, 28%
presented as IgA negative at the time of sampling (>7 days after
the onset of symptoms) and these patients presented with an
increased age and an increased number of comorbidities. Yu et
al (31) detected IgA
seroconversion on day 2 and IgM/IgG on day 5 following the onset of
symptoms.
Results of a previous study demonstrated that
sensitivity and specificity of the commercially available
SARS-CoV-2 immunoassays is adequate, ranging between 80-90%,
highlighting a suitable diagnostic performance (32).
Carnicelli et al (33) demonstrated that IgA and IgG
antibody responses are connected, although IgA seroconversion
begins at an earlier point. Results of this previous study
demonstrated that both IgA and IgG responses are detected in
patients with severe COVID-19. Results of the present study
demonstrated that disease severity led to significant differences
between the two groups of patients. Notably, in the positive IgA
anti SARS-CoV-2 group, more patients exhibited a severe form of the
disease (31.5%), compared with the IgA negative group (14.3%). As
IgA detection was associated with disease severity, this may be
attributed to higher immune responsiveness of the respiratory
system facing a severe respiratory infection.
In contrast with the findings by Korte et al
(34), no significant differences
were found regarding the presence of IgA antibodies between the two
sexes.
Ma et al (35), Carnicelli et al (33) and Zervouz (36) report that patients with severe
COVID-19 present high levels of the IgA antibody. These finding
could not be confirmed in the present study, where only the IgG
antibody levels were increased in severe COVID-19 cases. The stage
and severity of COVID-19 infection are important factors associated
with the presence of IgA, but the development of immune complexes,
the immune system and genetic characteristics of the patient may
interfere with the humoral response against SARS-CoV-2.
The evaluation of hematological and other laboratory
parameters is essential in understanding how the immune system
works following infection with SARS-CoV-2. Neutrophils account for
>50% of the total white blood cell count, being the most
important white blood cells that fight viral infection (32). The analysis of the blood tests
results revealed no significant differences in the number of
leukocytes or neutrophils (percentage or absolute) between positive
and negative IgA SARS-CoV-2 groups. Platelet count values were
increased in patients in group 1, but the difference was not
statistically significant. The mean alanine aminotransferase level
was above normal in both groups, without significant variation. The
mean C-reactive protein values detected in IgA SARS-CoV-2 positive
patients was also increased (68.2 vs. 55.2 mg/l).
Analysis of comorbidities and IgA anti-SARS-CoV-2
revealed that more patients (82.7%) that identified with
comorbidities were included in the second group of patients (79.6
vs. 90.5%), including those that were positive for SARS-CoV-2 RNA,
but negative for IgA anti SARS-CoV-2. Nonetheless, each patient
should be considered as a unique model, where COVID-19 clinical
evolution depends on other comorbidities.
Results of a previous study noted that SARS-CoV-2
infection elicits strong humoral immune responses, represented by
the production of IgA, IgM and IgG virus-specific antibodies
(16). A total of 4 patients in
the IgA negative group presented with anti-SARS CoV2 IgG
antibodies. These patients, 3 males and 1 female, exhibited
advanced ages (89, 67, 101 and 67 years) and multiple
comorbidities; all of them developed moderate forms of the disease,
without identifying with other clinical features or the laboratory
variables analyzed.
The present study has some limitations, including
the relatively low number of patients included and the large
sampling interval (relative to onset of symptoms) for IgA; however,
it provides a basis for future sampled research.
In conclusion, results of the present study
suggested that the detection of IgA antibodies against SARS-CoV-2
early in the course of the disease may be associated with severe
disease development, but further research is required. Their
presence may be influenced by several individual factors, such as
age, comorbidities or the time of sampling in association with the
onset of symptoms. In addition, data obtained during the present
study suggested that patients with severe infection may also
present a stronger IgG response. Further studies should focus on
increasing the sample number and expanding the median age of the
patients evaluated.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
AV and AA designed the study. DA and AV performed
the experiments and analyzed the data. CDM, FMR, IFM and DA were
responsible for the analysis and discussion of the data. AA and AV
drafted the manuscript. CML, GS and AV critically revised the
manuscript for important intellectual content and made substantial
contributions to the interpretation of data. AV and DA confirm the
authenticity of all the raw data. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
The study was conducted with fully adherence to the
international norms of medical ethics, as set out in the Helsinki
Declaration. The patients gave their informed written consent for
enrollment in the study. The study was approved by the Sfanta
Parascheva Infectious Diseases Hospital of Iași Ethics Committee
(approval no. 14/04.12.2020).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Docea AO, Tsatsakis A, Albulescu D,
Cristea O, Zlatian O, Vinceti M, Moschos SA, Tsoukalas D, Goumenou
M, Drakoulis N, et al: A new threat from an old enemy: Re-emergence
of coronavirus (Review). Int J Mol Med. 45:1631–1643.
2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Lu H, Stratton CW and Tang YW: Outbreak of
pneumonia of unknown etiology in Wuhan, China: The mystery and the
miracle. J Med Virol. 92:401–402. 2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Neagu M, Calina D, Docea AO, Constantin C,
Filippini T, Vinceti M, Drakoulis N, Poulas K, Nikolouzakis TK,
Spandidos DA and Tsatsakis A: Back to basics in COVID-19: Antigens
and antibodies-completing the puzzle. J Cell Mol Med. 25:4523–4533.
2021.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Islam MT, Quispe C, Herrera-Bravo J, Khan
IN, Bawazeer SS, Kumar M, Cruz-Martins N, Martorell M, Docea AO,
Sharifi-Rad J, et al: Possible mutation pathways in SARS-Cov-2.
Farmacia. 69:1001–1017. 2021.
|
|
5
|
Ritchie H, Mathieu E, Rodés-Guirao L,
Appel C, Giattino C, Ortiz-Ospina E, Hasell J, Macdonald B,
Beltekian D and Roser M: Coronavirus Pandemic (COVID-19), 2020.
Available from https://ourworldindata.org/coronavirus=.
|
|
6
|
Calina D, Hartung T, Mardare I, Mitroi M,
Poulas K, Tsatsakis A, Rogoveanu I and Docea AO: COVID-19 pandemic
and alcohol consumption: Impacts and interconnections. Toxicol Rep.
8:529–535. 2021.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Michelen M, Manoharan L, Elkheir N, Cheng
V, Dagens A, Hastie C, O'Hara M, Suett J, Dahmash D, Bugaeva P, et
al: Characterising long COVID: A living systematic review. BMJ Glob
Health. 6(e005427)2021.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He
JX, Liu L, Shan H, Lei CL, Hui DSC, et al: Clinical characteristics
of coronavirus disease 2019 in China. N Engl J Med. 382:1708–1720.
2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Goumenou M, Sarigiannis D, Tsatsakis A,
Anesti O, Docea AO, Petrakis D, Tsoukalas D, Kostoff R, Rakitskii
V, Spandidos DA, et al: COVID-19 in Northern Italy: An integrative
overview of factors possibly influencing the sharp increase of the
outbreak (Review). Mol Med Rep. 22:20–32. 2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Popov GT, Baymakova M, Vaseva V,
Kundurzhiev T and Mutafchiyski V: Clinical characteristics of
hospitalized patients with COVID-19 in Sofia, Bulgaria. Vector
Borne Zoonotic Dis. 20:910–915. 2020.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Lechien JR, Chiesa-Estomba CM, Place S,
Van Laethem Y, Cabaraux P, Mat Q, Huet K, Plzak J, Horoi M, Hans S,
et al: Clinical and epidemiological characteristics of 1420
European patients with mild-to-moderate coronavirus disease 2019. J
Intern Med. 288:335–344. 2020.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Calina D, Hartung T, Docea AO, Spandidos
DA, Egorov AM, Shtilman MI, Carvalho F and Tsatsakis A: COVID-19
vaccines: Ethical framework concerning human challenge studies.
Daru. 28:807–812. 2020.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Calina D, Hernández AF, Hartung T, Egorov
AM, Izotov BN, Nikolouzakis TK, Tsatsakis A, Vlachoyiannopoulos PG
and Docea AO: Challenges and scientific prospects of the newest
generation of mRNA-based vaccines against SARS-CoV-2. Life (Basel).
11(907)2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Calina D, Docea AO, Petrakis D, Egorov AM,
Ishmukhametov AA, Gabibov AG, Shtilman MI, Kostoff R, Carvalho F,
Vinceti M, et al: Towards effective COVID-19 vaccines: Updates,
perspectives and challenges (Review). Int J Mol Med. 46:3–16.
2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Sidiropoulou P, Docea AO, Nikolaou V,
Katsarou MS, Spandidos DA, Tsatsakis A, Calina D and Drakoulis N:
Unraveling the roles of vitamin D status and melanin during
Covid-19 (Review). Int J Mol Med. 47:92–100. 2021.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Islam MT, Quispe C, Martorell M, Docea AO,
Salehi B, Calina D, Reiner Ž and Sharifi-Rad J: Dietary
supplements, vitamins and minerals as potential interventions
against viruses: Perspectives for COVID-19. Int J Vitam Nutr Res.
92:49–66. 2022.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Pang NY, Pang AS, Chow VT and Wang DY:
Understanding neutralising antibodies against SARS-CoV-2 and their
implications in clinical practice. Mil Med Res.
8(47)2021.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Garcia-Beltran WF, Lam EC, Astudillo MG,
Yang D, Miller TE, Feldman J, Hauser BM, Caradonna TM, Clayton KL,
Nitido AD, et al: COVID-19-neutralizing antibodies predict disease
severity and survival. Cell. 184:476–488.e11. 2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Guo L, Ren L, Yang S, Xiao M, Chang D,
Yang F, Dela Cruz CS, Wang Y, Wu C, Xiao Y, et al: Profiling early
humoral response to diagnose novel coronavirus disease (COVID-19).
Clin Infect Dis. 71:778–785. 2020.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Mazzini L, Martinuzzi D, Hyseni I,
Benincasa L, Molesti E, Casa E, Lapini G, Piu P, Trombetta CM,
Marchi S, et al: Comparative analyses of SARS-CoV-2 binding (IgG,
IgM, IgA) and neutralizing antibodies from human serum samples. J
Immunol Methods. 489(112937)2021.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Lee J, Park SS, Kim TY, Lee DG and Kim DW:
Lymphopenia as a biological predictor of outcomes in COVID-19
patients: A nationwide cohort study. Cancers (Basel).
13(471)2021.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Wang R, Luo X, Liu F and Luo S:
Confronting the threat of SARS-CoV-2: Realities, challenges and
therapeutic strategies (Review). Exp Ther Med.
21(155)2021.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Ursu RG, Luca CM, Luca AS, Toader E,
Simion L and Iancu LS: Laboratory diagnosis for optimize therapy of
B hepatitis virus infection by using biochemical and molecular
biology methods. Rev Chim (Bucharest). 67:2614–2617. 2016.
|
|
24
|
Ortega MA, Fraile-Martínez O,
García-Montero C, García-Gallego S, Sánchez-Trujillo L,
Torres-Carranza D, Álvarez-Mon MÁ, Pekarek L, García-Honduvilla N,
Bujan J, et al: An integrative look at SARS-CoV-2 (Review). Int J
Mol Med. 47:415–434. 2021.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Woof JM and Kerr MA: The function of
immunoglobulin A in immunity. J Pathol. 208:270–282.
2006.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Dietzen DJ: Amino acids, peptides, and
proteins. In: Principles and Applications of Molecular Diagnostics.
Rifai N, Horvath AR and Wittwer CT (eds). Elsevier, Amsterdam,
pp345-380, 2018.
|
|
27
|
Stancioiu F, Papadakis GZ, Kteniadakis S,
Izotov BN, Coleman MD, Spandidos DA and Tsatsakis A: A dissection
of SARS-CoV2 with clinical implications (Review). Int J Mol Med.
46:489–508. 2020.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Chvatal-Medina M, Mendez-Cortina Y, Patiño
PJ, Velilla PA and Rugeles MT: Antibody responses in COVID-19: A
review. Front Immunol. 12(633184)2021.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Sterlin D, Mathian A, Miyara M, Mohr A,
Anna F, Claër L, Quentric P, Fadlallah J, Devilliers H, Ghillani P,
et al: IgA dominates the early neutralizing antibody response to
SARS-CoV-2. Sci Transl Med. 13(eabd2223)2021.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Meinberger D, Koch M, Roth A, Hermes G,
Stemler J, Cornely OA, Streichert T and Klatt AR: Analysis of IgM,
IgA, and IgG isotype antibodies directed against SARS-CoV-2 spike
glycoprotein and ORF8 in the course of COVID-19. Sci Rep.
11(8920)2021.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Yu HQ, Sun BQ, Fang ZF, Zhao JC, Liu XY,
Li YM, Sun XZ, Liang HF, Zhong B, Huang ZF, et al: Distinct
features of SARS-CoV-2-specific IgA response in COVID-19 patients.
Eur Respir J. 56(2001526)2020.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Okba NMA, Müller MA, Li W, Wang C,
GeurtsvanKessel CH, Corman VM, Lamers MM, Sikkema RS, de Bruin E,
Chandler FD, et al: Severe acute respiratory syndrome coronavirus
2-specific antibody responses in coronavirus disease patients.
Emerg Infect Dis. 26:1478–1488. 2020.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Carnicelli A, Fiori B, Ricci R, Piano A,
Bonadia N, Taddei E, Fantoni M, Murri R, Cingolani A, Barillaro C,
et al: Characteristic of IgA and IgG antibody response to
SARS-CoV-2 infection in an Italian referral COVID-19 hospital.
Intern Emerg Med. 17:53–64. 2022.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Korte W, Buljan M, Rösslein M, Wick P,
Golubov V, Jentsch J, Reut M, Peier K, Nohynek B, Fischer A, et al:
SARS-CoV-2 IgG and IgA antibody response is gender dependent; and
IgG antibodies rapidly decline early on. J Infect. 82:e11–e14.
2021.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Ma H, Zeng W, He H, Zhao D, Jiang D, Zhou
P, Cheng L, Li Y, Ma X and Jin T: Serum IgA, IgM, and IgG responses
in COVID-19. Cell Mol Immunol. 17:773–775. 2020.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Zervou FN, Louie P, Stachel A,
Zacharioudakis IM, Ortiz-Mendez Y, Thomas K and Aguero-Rosenfeld
ME: SARS-CoV-2 antibodies: IgA correlates with severity of disease
in early COVID-19 infection. J Med Virol. 93:5409–5415.
2021.PubMed/NCBI View Article : Google Scholar
|