Introduction
Periodontal disease causes chronic inflammation of
the supporting tissues around teeth. Some reports (1-3)
have demonstrated that periodontal disease and cardiovascular
disease (CVD) are closely related. However, the mechanism of their
occurrence is still unclear. Periodontal disease is associated with
the development of early atherosclerotic carotid lesions (4). In addition, low-grade chronic
inflammation plays an important role as a pathogenetic determinant
of atherosclerosis (AS) in the development of CVD (5). Vascular calcification is a universal
clinical sign of AS and is also a special expression of soft tissue
calcification induced by chronic inflammatory factors (6). We believe that periodontitis can
promote vascular calcification. Previous animal experiments have
demonstrated that periodontitis promotes vascular calcification
(7); however, the mechanism is
still unclear.
Osteoprotegerin (OPG)/receptor activator of nuclear
factor-κB (RANK)/receptor activator of nuclear factor-κB ligand
(RANKL) are new members of the tumor necrosis factor (TNF) family,
serving as crucial regulators of osteoclastogenesis and bone
resorption, with a key role in periodontitis (8-11).
They also play an essential role in vascular calcification
(12-15).
Compared to periodontal health, RANKL is upregulated, while OPG is
downregulated in periodontitis, increasing the RANKL/OPG ratio
(16). Recent research has also
shown that OPG/RANK/RANKL are key molecules in the vascular system
that inhibit vascular calcification and protect vascular
endothelial cells (15). In
addition, increased plasma levels of OPG in atherosclerotic
subjects indicated that OPG might be involved in the development of
AS (14). However, the potential
role of OPG/RANK/RANKL in periodontitis-associated vascular
calcification remains unknown.
The rat is an ideal choice for the preparation of a
vascular calcification model, because the anatomical structure of
alveolar bone and periodontal membrane are similar to that of
human. Rats were selected as animal models in this study (17,18).
In the present study, periodontitis and vascular calcification
animal models were established to explore the expression of the
OPG/RANK/RANKL system in vascular tissues of rats, and to identify
the potential role of this system in the effect of periodontitis on
vascular calcification.
Materials and methods
Establishment of the animal
models
Male Wistar rats, aged 8 weeks and weighing 200±20
g, were purchased from the Animal Center of Affiliated Hospital of
Qingdao University (Qingdao, China) [license number: SCXK
(lu)20090007]. All the animals were given humane care, conforming
to the Animal Management Rule of the Ministry of Health (Beijing,
China). After one week of adaptation, 36 male Wistar rats were
randomly assigned to four groups (n=9): the sham group (group C),
vascular calcification group (group VDN), periodontitis group
(group CP), and test group (group CP+VDN). The rats in each group
underwent treatments similar to previous studies to establish the
animal models (7). The rats in
group VDN received vitamin D3 plus nicotine as follows (19). The rats were given vitamin D3
[300,000 IU/kg in peanut oil (i.m.) and nicotine (25 mg/kg in 5 ml
of peanut oil, p.o.)] (Sigma-Adrich; Merck KGaA) at 9:00 on the
first day. The nicotine administration was repeated at 18:00 on the
same day. Rats were placed in a supine position and anesthetized by
intraperitoneal injection of 10% chloral hydrate at a dose of 300
mg/kg. Group CP was treated with silk ligation and local
inoculation of periodontal mixed pathogen. Subgingival plaque of
periodontitis patients was scraped and placed in a centrifuge tube
containing PBS solution. The plaque was dispersed by whirlpool
oscillator and cultured in BHI liquid medium for 5 days. The left
and right maxillary second molar were ligated with 4-0 silk thread
and placed in gingival sulcus as far as possible. Meanwhile,
periodontal pathogens were inoculated locally (17,18,20).
The treatment in the VDN+CP group consisted of silk-ligaturing and
simultaneous treatment with vitamin D3 (300,000 IU/kg, i.m.) plus
nicotine (25 mg/kg in 5 ml, p.o.). Group C was administered an
intramuscular injection of normal saline solution and gavages of
pure peanut oil to replace the vitamin D3 and nicotine treatments,
respectively.
After 3 months, the periodontal tissue and vascular
tissue of rats in each group were detected. The probing depth and
gingival sulcus bleeding index of maxillary second molars were
recorded.
Before euthanasia, all rats were fasted for 12 h and
anesthetized by intraperitoneal injection of 10% chloral hydrate
(300 mg/kg). No peritonitis was observed in the rats. Finally, the
rats were sacrificed by cervical dislocation.
Vascular calcification examination
Hematoxylin and eosin (H&E) staining, calcium deposition in the
aortas, and alkaline phosphatase (ALP) activity assay
The aorta was observed by H&E staining. Image
Pro Plus 6.0 medical image analysis software (Media Cybernetics,
Inc.) was used for semi-quantitative analysis of the
immunohistochemical results. All slides were analyzed at the same
magnification (x40) and light intensity. Measurement index: Average
optical density (AOD)=IG225-iga, where A represents the measured
gray value. A calcium assay kit (Nanjing Jiancheng Bioengineering
Institute) was used to detect calcium in the cardiovascular
tissues. The supernatants were assayed for ALP activity according
to the manufacturer's instructions (21).
Reverse transcription-qPCR
Total RNA was extracted from rat aortic tissue by
using Trizol reagent, and reversely transcribed into cDNA using the
PrimeScipt RT reagent kit (Takara Biotechnology Co., Ltd.) as
previously described (7). Gene
primers were ordered from Sangon Biotech Co., Ltd.. The forward and
reverse PCR primers (rat) included: GAPDH forward,
5'-ACCACCAACTGCTTAGCCCC-3' and reverse,
5'-CATGGACTGTGGTCATGAGCC-3'; OPG forward,
5'-AAGTGGCTGTGCTGTGCACTC-3' and reverse, 5'-CGGTTTCTGGGTCATAATGC
AA-3'; and RANKL forward, 5'-AGCCTTTCAAGGGGCCGTGC-3' and reverse,
5'-GGGCCACATCGAGCCACGAA-3'. The PCR cycling conditions were as
follows: one cycle at 95˚C for 5 min, 39 cycles at 95˚C for 30 sec,
60˚C for 30 sec and 72˚C for 30 sec, and final extension at 72˚C
for 6 min. SYBR Premix Ex Taq II (Takara Biotechnology Co., Ltd.)
was used to obtain the RT-qPCR product according to the
manufacturer's instructions. Lightcycler 480 (Roche, Switzerland)
was detected by qPCR using the 2-ΔΔCq method (22). Gene expression results were
normalized by internal control GAPDH. Each sample was tested in
triplicate and then averaged for the final analysis.
Immunohistochemistry
Immunohistochemistry of tissue slides was performed
as described previously (23,24).
The EnVision™ immunohistochemistry system was used to detect the
expression of OPG and RANKL in aortic tissues. After conventional
dewaxing, EDTA antigen retrieval was performed for 2 min, followed
by adding 3% H2O2 to each slice for 10 min.
After blocking, the slides were incubated with a primary anti-OPG
antibody (dilution 1:100; cat. no. orb247239; Biorbyt) or a primary
anti-RANKL antibody (dilution 1:100; cat. no. orb11190; Biorbyt) at
37˚C for 1 h. Then the slices were rinsed with PBS three times for
5 min. The goat anti-rabbit secondary antibody (cat. no. DS-0004;
Beijing Zhongshan Golden Bridge Biotechnology Co., Ltd.) was added
to slices at 37˚C for 30 min. Finally, the visualization signal was
developed with a diamino-benzidine-(DAB-)peroxidase substrate for 1
min. The sections were counterstained with hematoxylin, dehydrated,
made transparent, and finally sealed with neutral gum.
Western blot analysis
Aortic tissue samples were homogenized on ice using
lysis buffer and centrifuged at 13,000 x g for 15 min at 4˚C. The
BCA assay was applied to determine protein concentrations. All the
samples were prepared to the same concentration with loading buffer
(5X) and, boiled for 5 min. Protein (30 µg) was separated by 12%
SDS-PAGE and transferred to PVDF membranes. Next, the membranes
were incubated with primary antibodies of OPG and RANKL (cat. nos.
orb247239 and orb11190; Biorbyt) diluted 1:300 in 5% skimmed milk
in TBST overnight at 4˚C. Horseradish peroxidase-conjugated
anti-rabbit IgG (cat. no. ZB-2306) was used to detect the bound
antibody. After the membranes were rinsed, a Bio-Rad image analysis
system (Quantity One, Bio-Rad Laboratories, Inc.) was used to
quantify the band intensities by densitometry. The results were
normalized against the β-actin protein purchased from Santa Cruz
Biotechnology, Inc. Each experiment was repeated three times with
each animal.
Measurement of serum OPG and RANKL
concentration
Sandwich enzyme-linked immune-sorbent assay (ELISA)
(DuoSet ELISA, R&D Systems, Inc.) was used to determine serum
concentrations of OPG and RANKL in the collected serum samples. All
the samples were tested in duplicate, and then average values were
calculated. The detection limit of OPG was 0.07 pmol/l. The
intra-assay and inter-assay precision were ≤3 and ≤5%,
respectively. The limit of detection for RANKL was 0.01 pmol/l. The
intra-assay and inter-assay precision were ≤5 and ≤3%,
respectively.
Statistical analysis
The data conformed to normal and the variance was
uniform. The data are expressed as means ± standard deviation (mean
± SD). All the statistical analyses were carried out using SPSS
19.0 (IBM Corp.). One-way analysis of variance (ANOVA) and Tukey's
multiple comparison method were used to compare the groups.
Statistical significance was defined at P<0.05 for all
tests.
Results
Periodontal and vascular tissues
H&E staining, calcium assay and ALP assay
results were examined in our previous study (7). Calcium content in group VDN and group
CP+VDN were significantly higher than that in group C and group CP
(P<0.05), and the calcium content in group CP+VDN was higher
than that in group VDN, and the difference was statistically
significant (P<0.05). The alkaline phosphatase activity of group
CP, group VDN and group CP+VDN were higher than that of group C;
the difference was statistically significant (P<0.05), and the
difference was statistically significant (P<0.05) between CP+VDN
group and CP and VDN group.
Expression of OPG/RANKL
The expression of OPG/RANKL in vascular tissues was
detected by real-time qPCR, immunohistochemistry, and western blot
analysis, from mRNA to protein, from quantification to
location.
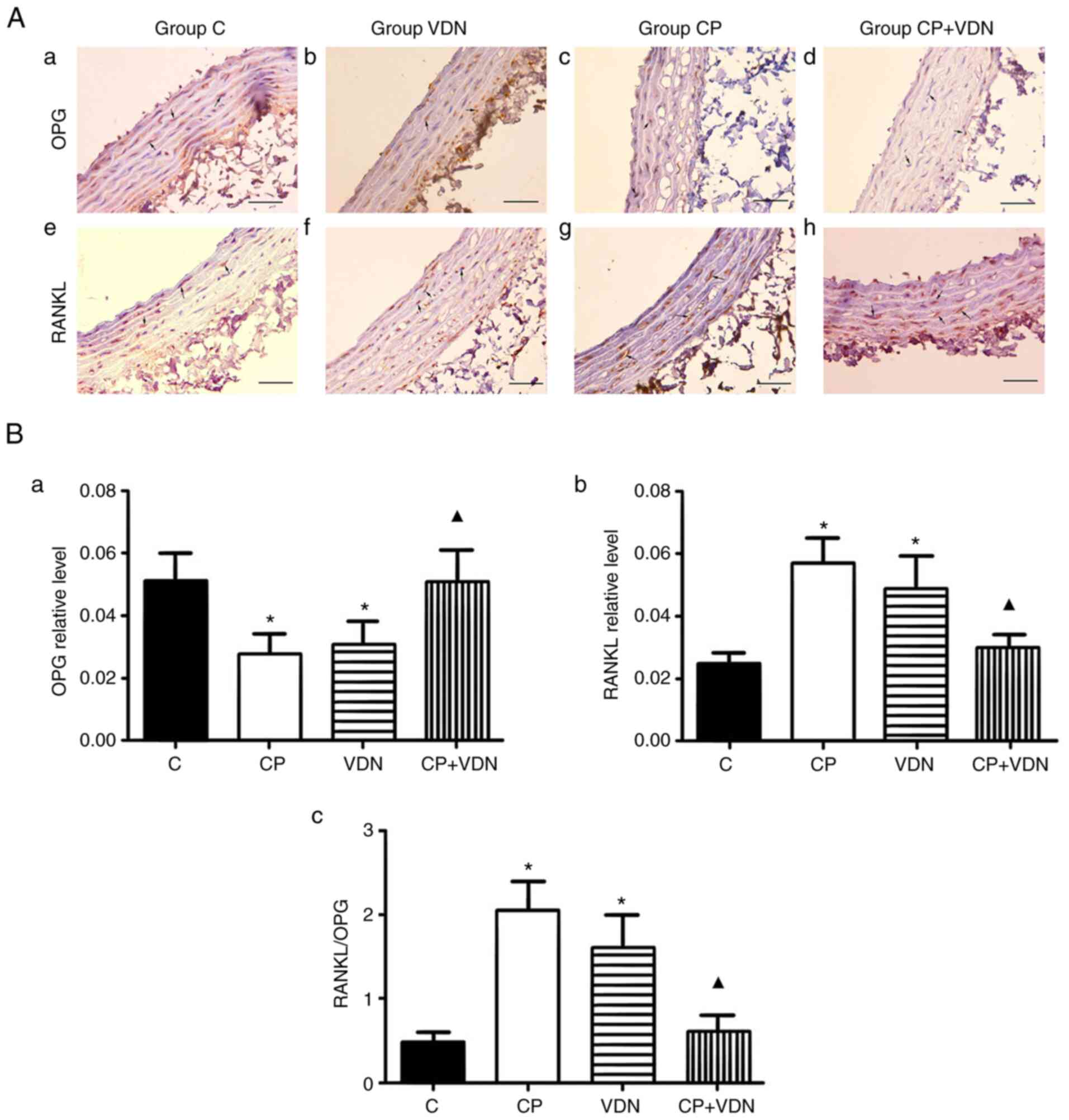
Immunohistochemistry
OPG and RANKL were both expressed in the vascular
tissues of the four groups with different degrees. OPG expression
was stronger in group C than in groups CP and VDN; however, it was
similar to that in group CP+VDN (Fig.
1Aa-d). Instead, RANKL expression was different from OPG, which
was stronger in groups VDN and CP than in groups C and CP+VDN
(Fig. 1Aa-h). IOD/area value of
OPG and RANKL were calculated with Image-Pro Plus software (Media
Cybernetics, Inc.; Fig. 1Ba and
b); the OPG/RANKL value is
presented in Fig. 1Bc. The value
of RANKL/OPG in the CP and VDN groups was higher than that in the C
and CP+VDN groups, indicating that both periodontitis and vascular
calcification could affect OPG/RANK/RANKL expression; however, when
periodontitis was tested with vascular calcification, the effect
was not simply superimposed.
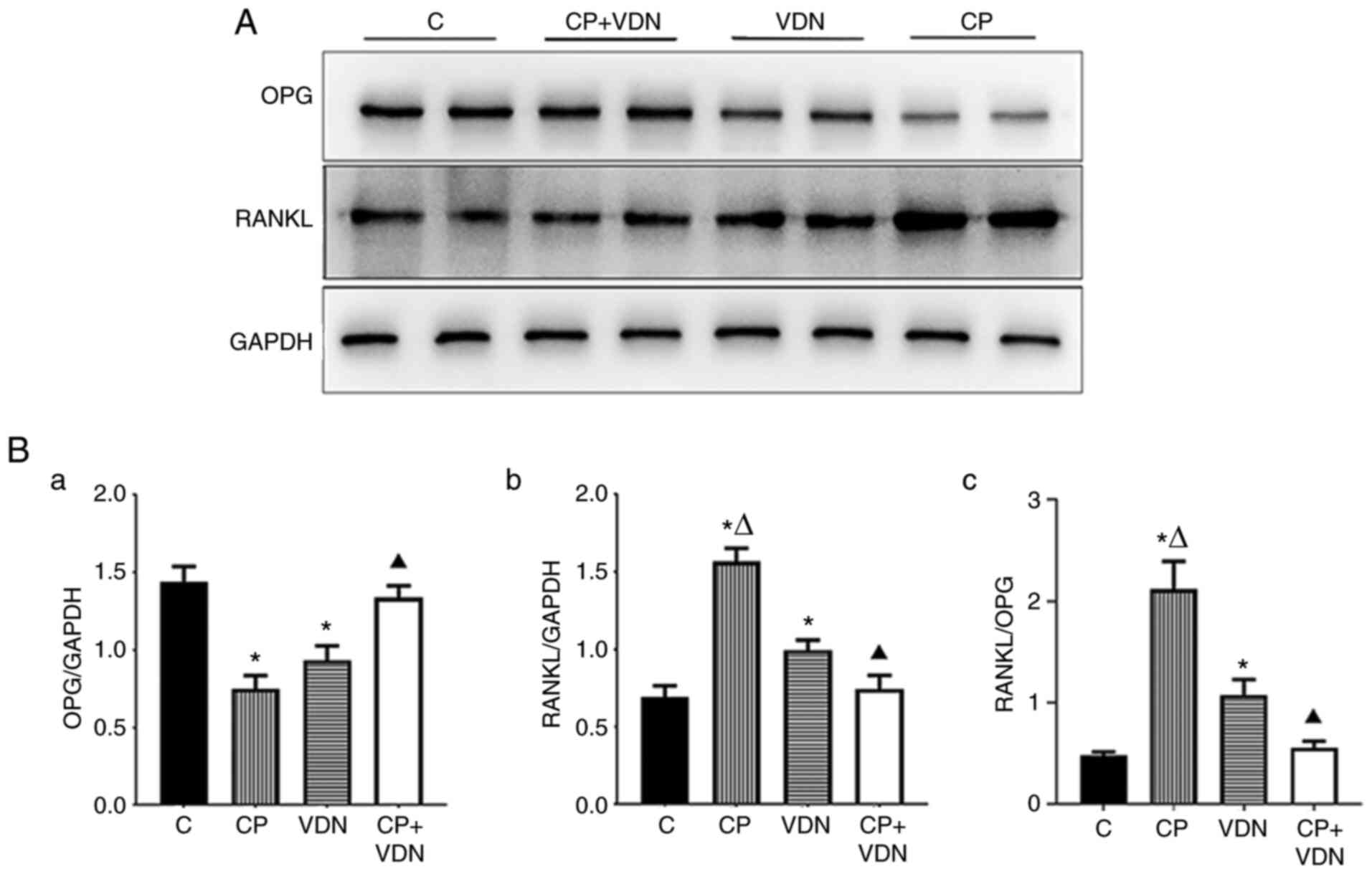
Western blot analysis
OPG protein gray values in the C and CP+VDN groups
were higher than that in the other groups (Fig. 2A and Ba). RANKL protein gray value and the
value of RANKL/OPG (Fig. 2A and
Bb and c) showed the contrast tendency compared
to OPG. Comparisons between the four groups showed statistically
significant differences.
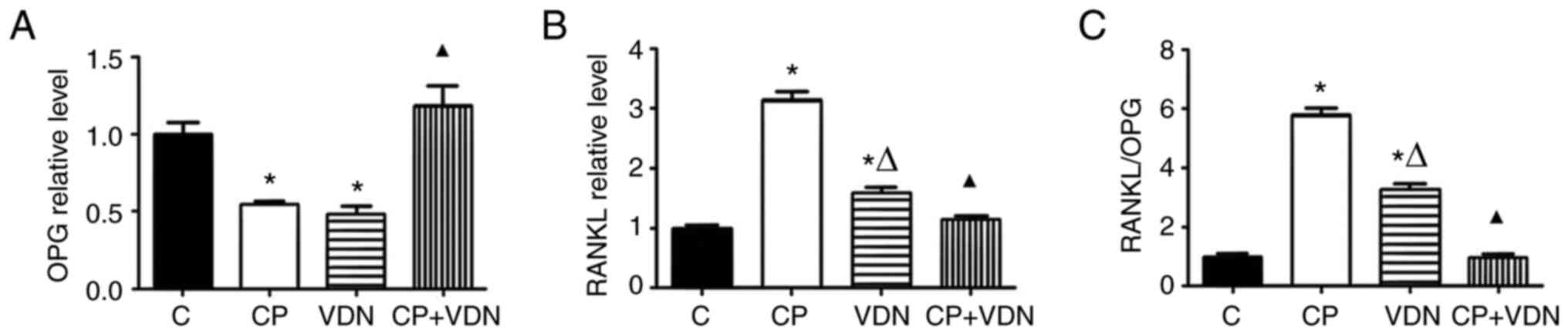
Reverse transcription-qPCR
OPG expression in the C and CP+VDN groups was higher
than that in the CP and VDN groups. However, OPG expression in the
CP+VDN group was similar to that in the C group (Fig. 3A). The quantitative analysis
revealed a significant decrease in RANKL expression levels in the
aorta of groups C and CP+VDN compared with groups CP and VDN, with
the highest expression in the CP group (Fig. 3B). The RANKL/OPG ratio was the
highest in the CP group, with no significant difference between the
C and CP+VDN groups (P>0.05) (Fig.
3C).
ELISA
OPG expression in the C and CP+VDN groups was higher
than that in CP and VDN groups, while its expression in the CP+VDN
group was similar to that in group C (Fig. 4A). However, compared to the other
two groups, RANKL expression level in groups C and CP+VDN was
significantly lower, with the highest level in group CP (Fig. 4B). The RANKL/OPG ratio had a
tendency similar to the expression of RANKL (Fig. 4C).
Discussion
Periodontal disease and cardiovascular disease (CVD)
are closely related, but the mechanism is still unclear. Many
studies have demonstrated that vascular calcification, a common
occurrence in CVD, results in increased cardiovascular mortality
(25). We previously found in
animal experiments that periodontitis promotes vascular
calcification (7). However, the
mechanism is still unclear.
The present study investigated the relationship and
mechanism between periodontitis and vascular calcification by
establishing rat models of periodontitis and vascular
calcification. There are different types of experimental
periodontitis models. One of the most commonly used models is the
rat model of periodontitis induced by ligation, which results in
continuous accumulation of calculus and plaque at the ligation site
(26,27). Periodontal probing depth (PD),
sulcus bleeding index (SBI), and hematoxylin and eosin (H&E)
staining of periodontal tissue serve as indicators of periodontal
disease. Periodontitis models were successfully established.
Vitamin D3 combined with nicotine-induced vascular calcification in
rats has the advantages of simple operation, high survival rate,
and good reproducibility (19,28).
The calcium assay and alkaline phosphatase (ALP) can serve as
indicators of vascular calcification. The rat vascular
calcification models were successfully established by the higher
levels of calcium and ALP. As for the group CP+VDN, the symptoms of
both periodontitis and vascular calcification were found which were
more severe than any other group, indicating an interaction between
periodontitis and vascular calcification.
Osteoprotegerin (OPG), a member of the tumor
necrosis factor receptor family, is a soluble decoy receptor of
receptor activator of nuclear factor-κB ligand (RANKL), which is
usually expressed by osteoblasts and inhibits bone resorption by
binding to RANKL, thereby preventing RANKL from binding to RANK
(29). The bone tissue destruction
that occurs in periodontitis is regulated by the balance between
OPG and RANKL levels (30). The
expression of RANKL increases significantly in patients with
chronic periodontitis compared to healthy individuals (31,32).
There are also reports that OPG and RANKL have been detected in
mice, consistent with the present study that RANKL-positive cells
are present in healthy gingival tissue samples (33). These all indicate that RANKL and
OPG play a key role in periodontitis.
The RANKL/RANK/OPG system has been extensively
explored in vascular biology, which is an essential factor in
balancing bone metabolism, in regulating the immune system, and in
participating in vascular calcification (34). RANKL and OPG perform vital
functions in osteogenic modulation of the vascular system. OPG can
be produced by various tissues, including cardiovascular tissue,
and is found in high concentrations in renal and aortic arteries.
In contrast to OPG, RANKL is not usually detectable in the normal
vascular system (14). By
immunohistochemical staining, Kaden et al (35) found that the expression of OPG in
the local calcified area was decreased, while the expression of
RANKL was increased in the vascular tissue of atherosclerosis and
calcified aortic valve stenosis. Bucay et al (36) found significant calcification in
the renal artery and aortic media in OPG-knockout mice, indicating
that OPG plays an important role in protecting the media of large
vessels from calcification. Similar to the former research, OPG
protein and RNA were strongly expressed in the normal vasculature
and weakly in vascular calcification. As for RANKL, which is also
found at a low level in the normal vasculature, it was upregulated
in vascular calcification. This also indirectly showed that OPG had
a protective effect on blood vessels and an inhibitory effect on
arterial calcification. In the vascular system of the periodontitis
group, similar results were achieved as that in the vascular
calcification group, suggesting that perhaps periodontitis affects
the vascular system by OPG/RANK/RANKL, which might be the same as
vascular calcification.
As to serum OPG and RANKL levels, the results were
complex and even controversial. As shown in previous studies, high
levels of serum OPG are associated with age, end-stage renal
disease, high cardiovascular mortality, diabetes, coronary artery
disease, and acute cerebral infarction (37-39).
There are many reports that serum OPG is elevated in the supportive
condition of AS (14,15,40).
It has been suggested that the serum concentration of RANKL is the
highest in ischemic cerebrovascular disease, acute myocardial
infarction, and other acute vascular syndromes (41). The RANKL/OPG ratio was positively
correlated with total coronary artery calcification, while OPG was
negatively correlated with total coronary artery calcification.
There was no significant correlation between RANKL serum
concentration and the degree of coronary artery calcification
(42). However, in this research,
serum OPG and RANKL levels differed from other studies, with the
same tendency to be expressed in the vessel, i.e., the OPG level
was lower in CP and VDN groups, while the level of RANKL was
higher.
However, no studies are available on the potential
role of OPG and RANKL in the effect of periodontitis on vascular
calcification. In addition, the mechanism of interaction between
vascular calcification and periodontitis is unclear.
Immunohistochemistry, western blot analysis, quantitative real-time
qPCR, and ELISA were used to analyze OPG and RANKL in vascular
tissues and serum of different groups to investigate whether
OPG/RANK/RANKL is involved in the effect of periodontitis on
vascular calcification. The RANKL/OPG ratio has also been studied.
Although OPG/RANK/RANKL plays a key role in both periodontitis and
vascular calcification, periodontitis promotes vascular
calcification. The expression levels of RANKL and OPG were slightly
different from the previous speculation. The OPG level in the group
CP+VDN was not lower than that in the groups CP and VND, but the
same as the sham group. RANKL in the CP+VDN group was not more
highly expressed than that in group CP or VDN, but it was the same
as that in the sham group. The same tendency was observed in
vascular tissues and serum by four methods, and the RANKL/OPG ratio
was the same.
The results were surprising and far different from
the previous speculation, which may be related to several aspects.
Firstly, vascular calcification is actively regulated by a variety
of networks, including negative and positive regulators, activation
of modulators or temporal expression, and multiple amplification or
suppression of feedback loops that coordinate function, cell
recruitment, survival, differentiation, and interactions with other
cells or matrix molecules (43-45).
OPG/RANK/RANKL may participate in several aspects of the above
processes that govern vascular calcification. Secondly, the
expression of RANKL and OPG might be affected by many factors, such
as inflammatory cytokines. High levels of OPG are associated with
insulin resistance and HbA1c level, as well as with high
inflammatory markers, such as fibrinogen, interleukin-6, and CRP
(46). Periodontitis is a chronic
infection with high inflammatory cytokine levels. Finally, in the
VDN+CP group, the effect of periodontitis and vascular
calcification on OPG/RANKL/RANK might be contrary and considerable,
leading to the expression of OPG and RANKL, which was similar to
the sham group. Although OPG has attracted much attention as a
connecting molecule between the vascular system and bone, there is
controversy concerning the role the OPG/RANK/RANKL system plays in
cardiovascular diseases, and the mechanism of OPG/RANK/RANKL in the
process of vascular calcification remains unclear. There is yet no
consensus in opinion unifying the dichotomy of OPG in animal models
and human studies (47). In
atherosclerotic lesions, the elevated OPG level might be a response
to the damage of blood vessels and persistent inflammatory
processes. It is believed that the increased level of OPG might be
a self-defensive and compensatory response against AS
progression.
OPG/RANK/RANKL has been involved in the progression
of vascular calcification. However, it is only one aspect of the
complicated network and is regulated by many other factors. When
periodontitis is involved, the progression is more complex.
In conclusion, taken together, RANKL/RANK/OPG may
have important functions in the process in which periodontitis
could promote vascular calcification. However, if periodontitis and
vascular calcification co-exist, the expression levels of RANKL and
OPG are not simply superimposed. If OPG or RANKL is used as a
marker to indicate one disease, the effect of the other disease
should be considered.
Acknowledgements
No applicable.
Funding
Funding: The present study was supported by the National Natural
Science Foundation of China (NSFC; grant no. 81100755) and the
Health Department of Shandong Province (grant no. 2016WS0252).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
MJ and PZ contributed to the design and
implementation of the experiment and the writing of the paper. XY
and ML contributed to the design of the experiment. PS, YQ and KP
put forward valuable suggestions on the design of the experiment
and the revision of the paper, and supervised the implementation of
the experiment. PZ and KP contributed to the data collection and
guaranteed the authenticity of the data. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Medical Ethics
Committee of the Affiliated Hospital of Qingdao University
(approval no. AHQU20140425). The study is consistent with the 1964
Declaration of Helsinki and its subsequent amendments or similar
ethical standards.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Almeida APCPSC, Fagundes NCF, Maia LC and
Lima RR: Is there an association between periodontitis and
atherosclerosis in adults? A systematic review. Curr Vasc
Pharmacol. 16:569–582. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Naderi S and Merchant AT: The association
between periodontitis and cardiovascular disease: An update. Curr
Atheroscler Rep. 22(52)2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Sanz M, Marco Del Castillo A, Jepsen S,
Gonzalez-Juanatey JR, D'Aiuto F, Bouchard P, Chapple I, Dietrich T,
Gotsman I, Graziani F, et al: Periodontitis and cardiovascular
diseases: Consensus report. J Clin Periodontol. 47:268–288.
2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Schenkein HA, Papapanou PN, Genco R and
Sanz M: Mechanisms underlying the association between periodontitis
and atherosclerotic disease. Periodontol 2000. 83:90–106.
2020.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Raggi P, Genest J, Giles JT, Rayner KJ,
Dwivedi G, Beanlands RS and Gupta M: Role of inflammation in the
pathogenesis of atherosclerosis and therapeutic interventions.
Atherosclerosis. 276:98–108. 2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
López-Mejías R and González-Gay MA: IL-6:
Linking chronic inflammation and vascular calcification. Nat Rev
Rheumatol. 15:457–459. 2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Li H, Pan K, Meng Y, Deng J, Zhang P, Song
W and Li S: Mutual promotions between periodontitis and vascular
calcification by rat animal model. J Periodontal Res. 55:810–820.
2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Sojod B, Chateau D, Mueller CG, Babajko S,
Berdal A, Lézot F and Castaneda B: RANK/RANKL/OPG signalization
implication in periodontitis: New evidence from a RANK transgenic
mouse model. Front physiol. 8(338)2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Crotti TN, Dharmapatni AA, Alias E and
Haynes DR: Osteoimmunology: Major and costimulatory pathway
expression associated with chronic inflammatory induced bone loss.
J immunol Res. 2015(281287)2015.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Borges CD, Ricoldi MS, Messora MR, Palioto
DB, Souza SLS, Novaes Júnior AB and Taba M*Jr: Clinical attachment
loss and molecular profile of inflamed sites before treatment. J
Appl Oral Sci. 27(e20180671)2019.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Gibertoni F, Sommer MEL, Esquisatto MAM,
Amaral MECD, Oliveira CA, Andrade TAM, Mendonça FAS, Santamaria M
Jr and Felonato M: Evolution of periodontal disease: Immune
response and RANK/RANKL/OPG system. Braz Dent J. 28:679–687.
2017.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Kang YH, Jin JS and Son SM: Long Term
effect of high glucose and phosphate levels on the
OPG/RANK/RANKL/TRAIL system in the progression of vascular
calcification in rat aortic smooth muscle cells. Korean J Physiol
Pharmacol. 19:111–118. 2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Krajewska-Włodarczyk M and Stompór T:
Osteoporosis and vascular calcification in rheumatoid arthritis-the
role of osteoprotegerin and sclerostin. Pol Merkur Lekarski.
43:41–47. 2017.PubMed/NCBI(In Polish).
|
|
14
|
Oštrić M, Kukuljan M, Markić D, Gršković
A, Ivančić A, Bobinac D, Španjol J, Maroević J, Šoša I and Ćelić T:
Expression of bone-related proteins in vascular calcification and
its serum correlations with coronary artery calcification score. J
Biol Regul Homeost Agents. 33:29–38. 2019.PubMed/NCBI
|
|
15
|
Rochette L, Meloux A, Rigal E, Zeller M,
Malka G, Cottin Y and Vergely C: The role of osteoprotegerin in
vascular calcification and bone metabolism: The basis for
developing new therapeutics. Calcif Tissue Int. 105:239–251.
2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Teodorescu AC, Martu I, Teslaru S,
Kappenberg-Nitescu DC, Goriuc A, Luchian I, Martu MA, Solomon SM
and Mârțu S: Assessment of salivary levels of RANKL and OPG in
aggressive versus chronic periodontitis. J Immunol Res.
2019(6195258)2019.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Ekuni D, Tomofuji T, Sanbe T, Irie K,
Azuma T, Maruyama T, Tamaki N, Murakami J, Kokeguchi S and Yamamoto
T: Vitamin C intake attenuates the degree of experimental
atherosclerosis induced by periodontitis in the rat by decreasing
oxidative stress. Arch Oral Biol. 54:495–502. 2009.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Zhou R, Shen L, Yang C, Wang L, Guo H,
Yang P and Song A: Periodontitis may restrain the mandibular bone
healing via disturbing osteogenic and osteoclastic balance.
Inflammation. 41:972–983. 2018.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Niederhoffer N, Bobryshev YV,
Lartaud-Idjouadiene I, Giummelly P and Atkinson J: Aortic
calcification produced by vitamin D3 plus nicotine. J Vase Res.
34:386–398. 1997.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Jain A, Batista EL Jr, Serhan C, Stahl GL
and Van*Dyke TE: Role for periodontitis in the progression of lipid
deposition in an animal model. Infect Immun. 71:6012–6018.
2003.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Bessey OA, Lowry OH and Brock MJ: A method
for the rapid determination of alkaline phosphates with five cubic
millimeters of serum. J Biol Chem. 164:321–329. 1946.PubMed/NCBI
|
|
22
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408.
2001.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Ma HB, Wang R, Yu KZ and Yu C: Dynamic
changes of early-stage aortic lipid deposition in chronic renal
failure rats and effects of decorin gene therapy. Expl Ther Med.
9:591–597. 2015.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Li K, He W, Lin N, Wang X and Fan QX:
N-cadherin knock-down decreases invasiveness of esophageal squamous
cell carcinoma in vitro. World J Gastroenterol. 15:697–704.
2009.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Gungor O, Kocyigit I, Yilmaz MI and Sezer
S: Role of vascular calcification inhibitors in preventing vascular
dysfunction and mortality in hemodialysis patients. Semin Dial.
31:72–81. 2018.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Lee DH, Lee H, Kim MH and Yang WM: The
effects of gardenia jasminoides on periodontitis in
ligature-induced rat model. Oral Health Prev Dent. 18:799–806.
2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Yu X, Gong Z, Lin Q, Wang W, Liu S and Li
S: Denervation effectively aggravates rat experimental
periodontitis. J Periodontal Res. 52:1011–1020. 2017.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Niederhoffer N, Lartaud-Idjouadiene I,
Giummelly P, Duvivier C, Peslin R and Atkinson J: Calcification of
medial elastic fibers and aortic elasticity. Hypertension.
29:999–1006. 1997.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Liu C, Zhang Y, Kong X, Zhu L, Pang J, Xu
Y, Chen W, Zhan H, Lu A and Lin N: Triptolide prevents bone
destruction in the collagen-induced arthritis model of rheumatoid
arthritis by targeting RANKL/RANK/OPG signal pathway. Evid Based
Complement Alternat Med. 2013(626038)2013.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Sağlam M, Köseoğlu S, Hatipoğlu M, Esen HH
and Köksal E: Effect of sumac extract on serum oxidative status,
RANKL/OPG system and alveolar bone loss in experimental
periodontitis in rats. J Appl Oral Sci. 23:33–41. 2015.PubMed/NCBI View Article : Google Scholar
|
|
31
|
López Roldán A, García Giménez JL and
Alpiste*Illueca F: Impact of periodontal treatment on the RANKL/OPG
ratio in crevicular fluid. PLoS One. 15(e0227757)2020.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Balci Yuce H, Gokturk O, Aydemir Turkal H,
Inanir A, Benli I and Demir O: Assessment of local and systemic
25-hydroxy-vitamin D, RANKL, OPG, and TNF levels in patients with
rheumatoid arthritis and periodontitis. J Oral Sci. 59:397–404.
2017.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Bi CS, Sun LJ, Qu HL, Chen F, Tian BM and
Chen FM: The relationship between T-helper cell polarization and
the RANKL/OPG ratio in gingival tissues from chronic periodontitis
patients. Clin Exp Dent Res. 5:377–388. 2019.PubMed/NCBI View
Article : Google Scholar
|
|
34
|
Bargnoux AS, Morena M, Aenaud J, Cavalier
É, Zaoui P, Delanaye P and Cristol JP: Groupe de Travail Mixte SFBC
SN Biomarqueurs des Calcifications Vasculaires Au Cours de
L'insuffisance Rénale Chronique. Biomarkers of vascular
calcifications: The osteoprotegerin/RANK/RANK L axis. Ann Biol Clin
(Paris). 73:289–298. 2015.PubMed/NCBI View Article : Google Scholar : (In French).
|
|
35
|
Kaden JJ, Bickelhaupt S, Grobholz R, Haase
KK, Sarikoç A, Kiliç R, Brueckmann M, Lang S, Zahn I, Vahl C, et
al: Receptor activator of nuclear factor kappaB ligand and
osteoprotegerin regulate aortic valve calcification. J Mol Cell
Cardiol. 36:57–66. 2004.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Bucay N, Sarosi I, Dunstan CR, Morony S,
Tarpley J, Capparelli C, Scully S, Tan HL, Xu W, Lacey DL, et al:
Osteoprotegerin-deficient mice develop early onset osteoporosis and
arterial calcification. Genes Dev. 12:1260–1268. 1998.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Bernardi S, Toffoli B, Bossi F, Candido R,
Stenner E, Carretta R, Barbone F and Fabris B: Circulating
osteoprotegerin is associated with chronic kidney disease in
hypertensive patients. BMC Nephrol. 18(219)2017.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Morisawa T, Nakagomi A, Kohashi K, Kusama
Y and Shimizu W: Serum tartrate-resistant acid phosphatase-5b
levels are associated with the severity and extent of coronary
atherosclerosis in patients with coronary artery disease. J
Atheroscler Thromb. 24:1058–1068. 2017.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Li Y, Terauchi M, Vikulina T, Roser-Page S
and Weitzmann MN: B cell production of both OPG and RANKL is
significantly increased in aged mice. Open Bone J. 6:8–17.
2014.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Rochette L, Meloux A, Rigal E, Zeller M,
Cottin Y and Vergely C: The role of osteoprotegerin and its ligands
in vascular function. Int J Mol Sci. 20(705)2019.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Abbas AAH, Naji AA and Hashem RB: RANKL
and OPG serum levels in acute coronary syndrome. J Natural Sci Res.
5:105–110. 2015.
|
|
42
|
Mohammadpour AH, Shamsara J, Nazemi S,
Ghadirzadeh S, Shahsavand S and Ramezani M: Evaluation of RANKL/OPG
serum concentration ratio as a new biomarker for coronary artery
calcification: A pilot study. Thrombosis.
2012(306263)2012.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Durham AL, Speer MY, Scatena M, Giachelli
CM and Shanahan CM: Role of smooth muscle cells in vascular
calcification: Implications in atherosclerosis and arterial
stiffness. Cardiovasc Res. 114:590–600. 2018.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Kurabayashi M: Molecular mechanism of
vascular calcification. Clin Calcium. 29:157–163. 2019.PubMed/NCBI View Article : Google Scholar : (In Japanese).
|
|
45
|
Chang X, Zhang B, Li L and Feng Z: T3
inhibits the calcification of vascular smooth muscle cells and the
potential mechanism. Am J Transl Res. 8:4694–4704. 2016.PubMed/NCBI
|
|
46
|
Bilgir O, Yavuz M, Bilgir F, Akan OY,
Bayindir AG, Calan M, Bozkaya G and Yuksel A: Relationship between
insulin resistance, hs-CRP, and body fat and serum
osteoprotegerin/RANKL in prediabetic patients. Minerva Endocrinol.
43:19–26. 2018.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Makarović S, Makarović Z, Steiner R,
Mihaljević I and Milas-Ahić J: Osteoprotegerin and vascular
calcification: Clinical and prognostic relevance. Coll Antropol.
39:461–468. 2015.PubMed/NCBI
|