Introduction
The prevalence of kidney stones has been increasing
worldwide over the past few decades. In Asia, the prevalence is
1-19% (1,2), which represents a considerable burden
for public healthcare systems. According to the European
Association of Urology (EAU) Guidelines, ‘high burden stones’
comprise single or multiple large calculi (a total surface area
>300 mm2, or with the largest diameter measuring
>20 mm, for urolithiasis) and staghorn calculi. A series of
complications are associated with high burden stones, including
renal deterioration, pyonephrosis, obstruction, flank pain and
life-threatening sepsis. Percutaneous nephrolithotomy (PCNL) is the
preferred first-line treatment for high burden urolithiasis.
However, it has the disadvantage of there being more than one
access site that may be required in order to bring about a complete
clearance. To achieve a one-stage clearance of the stones, other
novel combined techniques have been explored, such as combinations
of PCNL and extracorporeal shock wave lithotripsy (ESWL; so-called
‘sandwich’ therapies) and endoscopic combined intrarenal surgery
(ECIRS). ECIRS involves a combination of PCNL and ureteroscopy to
investigate the renal cavities (3). Laparoscopic ureterolithotomy has the
benefits of being a minimally invasive technique with short
hospital stays, as well as the advantage of one-time removal of
calculi, which is usually the case with open surgery (4). Furthermore, it is a viable option in
difficult stone situations and in cases where there is an abnormal
anatomy of the urinary system. To eliminate the high burden stones
from solitary kidney patients (born with one kidney), we have
devised a novel type of surgery combining laparoscopy and
endoscopy. The latter comprised a flexible ureteroscope, a rigid
ureteroscope and ureteroscope pneumatic lithotripsy. Laparoscopy
and endoscopy cooperative surgery have previously been introduced
as a minimally invasive technique for the resection of
gastrointestinal subepithelial tumors (5). At the present time, cooperative
surgery is not routinely used as a technique in urology, although
there are a few clinical studies that have been published on it
(6,7). The experience of clinical treatment
in the present case study could provide much guidance for the
future treatment of high burden stones. Note that the following
case is presented in accordance with the CARE reporting
checklist.
Case report
The current study presented the case of surgical
treatment of a patient with one solitary kidney and ureter with
multiple calculus. Laparoscopy, flexible ureteroscopy and rigid
ureteroscopy were used in the one-stage surgery. A 68-year-old male
patient with a history of kidney and ureter calculus for 18 years
and bilateral necrosis femoral heads for 15 years was admitted to
Shandong Provincial Hospital with the complaint of intermittent
left-flank pain for 10 days and anuria for 3 days. A physical
examination showed limited movement of both lower limbs and
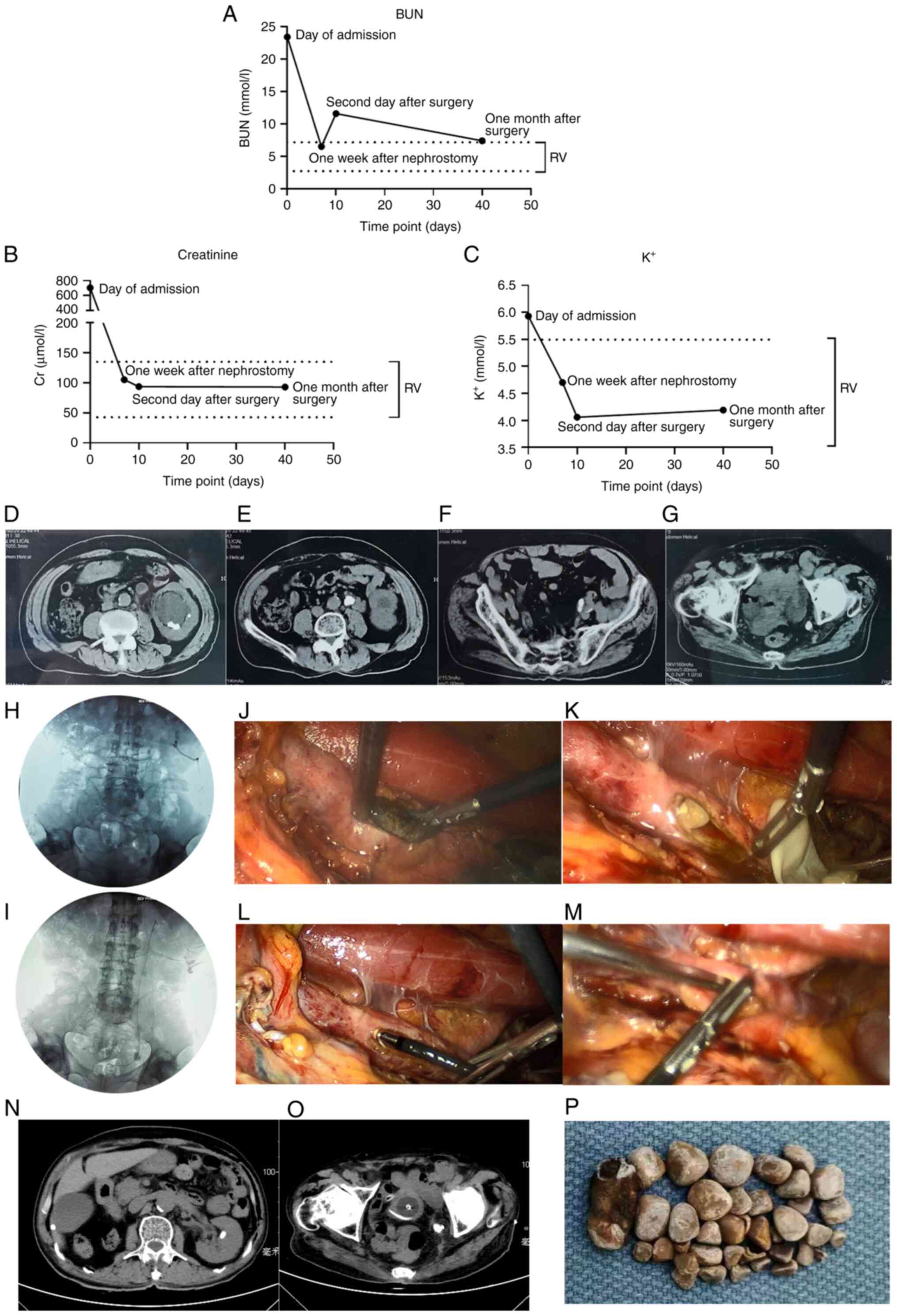
percussion tenderness in the left kidney region. Laboratory
examination revealed levels of blood urea nitrogen (BUN) of 23.4
mmol/l (normal range: 2.8-7.14 mmol/l), creatinine (Cr) of 706.21
µmol/l (normal range: 40-135 µmol/l) and potassium of 5.93 mmol/l
(normal range: 3.5-5.3 mmol/l) (Fig.
1A-C). The patient had been treated with antibiotics prior to
attending hospital. Neither sepsis nor coagulation disorders were
detected in the patient; neither were bacteria cultured in his
urine. The white blood cells were not increased and the C-reactive
protein was increased a small amount on the day of admission.
Urinary ultrasound revealed a dilation of the left renal pelvis of
~4.3 cm anteroposterior (AP) diameter [Society of Fetal Urology
(SFU)-III (one of the grading systems of hydronephrosis)] (8) and several stones were detected in the
left kidney. The maximum renal stone was ~2.7x0.8 cm. No kidney was
detected in the right renal area. A stone of 2.9x0.9 cm size was
found in the left upper ureter. Stones of diameter >2 cm were
also detected in the pelvic part of the left ureter. Abdominal
computed tomography (CT) showed left renal and ureteral calculus
with hydronephrosis, whereas the right kidney was absent (Fig. 1D-G). On the day of admission,
percutaneous nephrostomy (PCN) was performed on the left kidney. On
the second day after PCN, a second ultrasound showed that the AP
diameter of the left hydronephrosis had decreased from 4.3 to 1.4
cm [SFU-IIb] (8). One week after
PCN, the renal function was reviewed: BUN was found to be present
at a concentration of 6.5 mmol/l, Cr was 105.22 µmol/l and
potassium was 4.7 mmol/l (Fig.
1A-C). Kidney, ureter and bladder plain film radiography was
subsequently performed to locate the calculi again immediately
prior to the surgery (Fig.
1H).
The patient underwent left laparoscopic
ureterolithotomy combined with flexible ureteroscopy and rigid
ureteroscopy and ureteroscope pneumatic lithotripsy on the 9th day
after admission to hospital and nearly 40 stones and fragments were
removed (Fig. 1P). Under general
anesthesia, a urethral catheter was introduced retrograde into the
bladder and 150 ml 0.8% methylene blue [diluted in normal saline
(NS)] was irrigated into bladder. The catheter was then clamped.
The patient was placed in an approx. 70˚ lateral position. Once a
pneumoperitoneum was established, a 10 mm trocar was placed at the
umbilicus for the camera and 5-, 10- and 12-mm ports were inserted,
respectively. First, the colon was reflected to provide adequate
visualization of the anterior surface of the psoas tendon.
Secondly, the ureter was dissected. After carefully examining the
region of the upper ureter, it was found to have become coarse and
edematous. Unipolar electrocoagulation was used to cut the ureter
longitudinally at the beginning of the ureterectasia and several
pieces of stone were found to exist in the ureteral lumen, the
largest one of them being 1 cm in length and cylindrical, with a
yellow-brown color. The stone was removed using a vascular clamp
(Fig. 1J). An F8 catheter was
inserted into the trocar and upper side of the cut and NS was
irrigated into the kidney. With a rapid withdrawal of the catheter,
several stones were flushed out. More stones were flushed out as a
result of NS being irrigated through the nephrostomy tube (Fig. 1K). Thirdly, a flexible ureteroscope
was inserted through the trocar under the laparoscopic view and the
ureteral incision was used to explore the renal pelvis (Fig. 1L). No further kidney stones were
observed. Subsequently, the flexible ureteroscope was used to
continue to explore the lower part of the ureter. A large number of
calculi were in the pelvic part of the ureter, although they could
not be removed by the flexible ureteroscope. Fourthly, the rigid
ureteroscope combined with forceps were introduced through the
trocar to remove the middle and lower urinary calculi. The residual
calculi (i.e., >10 large calculi of diameter >1 cm) were
crushed using ureteroscope pneumatic lithotripsy and pushed into
the bladder (Fig. 1M). The
methylene blue finally flowed out from the lower ureteral incision.
A double J tube was placed in the left ureter. One end of the
double J tube was in the renal pelvis, while the other end was in
the bladder and the ureteral incision was ligated using sutures,
with repeated washing of the wound using the internally located
drainage peritoneal tube.
On the second day after surgery, renal function was
analyzed once again and the concentrations of the biochemical
markers were as follows: BUN, 11.6 mmol/l; creatinine, 93.73
µmol/l; and potassium, 4.06 mmol/l. The thyroid function series
were subsequently tested and there were no signs of
hyperparathyroidism. At 5 days post-operation, the drainage was
suppressed. The catheter was then removed 7 days post-operation,
although the nephrostomy tube was kept to maintain the renal
function. The patient recovered well and was discharged on the
eighth day post-operation. One month after the operation, the
patient's BUN level was 7.4 mmol/l, the creatinine concentration
was 93.10 µmol/l and the potassium level was 4.19 mmol/l. Two
stones of diameter ~1 cm remained, one in the left kidney and the
other in the left ureter (Fig. 1I,
N and O) and ESWL was performed 43 days
post-operation. The ESWL was performed using a lithotripter with up
to 3,500 shock waves at 11-14 kV. The total energy used was 95.32
J. Thereafter, the patient was not subjected to any further
examinations or treatment.
All procedures performed in the present study were
in accordance with the ethical standards of the institutional
and/or national research committee(s) and with the Helsinki
Declaration (as revised in 2013). The present study was approved by
the Ethics Committee of Shandong Provincial Hospital Affiliated to
Shandong First Medical University (Jinan, China; approval no. SWYX:
No. 2021-370). The subject signed an informed consent form and had
complete clinical data.
Discussion
The patient in the present study was an elderly male
with a solitary kidney and ureter, which meant the renal function
of his only kidney assumed a greater importance. He had had a
history of calculi for 18 years. The accompanying bilateral
necrosis femoral heads led to his limitation of movement, which
also contributed to the formation of multiple stones in the left
kidney and ureter. The maximum diameters of the stones were 2.7 cm
in the kidney and 2.9 cm in the ureter. All the features described
above contributed towards the complexity of the present case. On
the day of admission, the first aim was not surgery, but to resolve
the anuria and to save the patient's life. PCN was performed
immediately, serving as the critical step in the whole treatment.
First, it led to a rapid reduction in the concentrations of BUN, Cr
and potassium, which provide a suitable precondition for subsequent
treatment; secondly, in the combined surgery, the renal fistula act
as another channel for irrigation of NS, which also helped to flush
the stones out.
For the surgical treatment of high burden stones,
there are a series of surgery management strategies available.
Laparoscopic ureterolithotomy has the advantage of one-time removal
of large stones. Although certain large ureter stones may be
squeezed out from the incision, the removal of kidney stones and
stones in the pelvic region of ureter cannot be achieved and a
larger incision is required. Retrograde intrarenal surgery (RIRS)
has the advantages of minimal invasion and wide scope of vision,
although for stones >2 cm in diameter, the duration of the
surgery is usually longer compared with laparoscopy and one-stage
clearance is very difficult to accomplish (9). Even if the stones are finally
cleared, the formation of a ureteric steinstrasse is quite commonly
seen as a side effect (9,10). To dispose of the steinstrasse, much
more work is required, such as ESWL or RIRS once again (11). PCNL is the first-line choice for
high burden stones in the upper urinary tract, but not for stones
in the ureter. Furthermore, the injury caused to the kidney is
clearly larger compared with RIRS (10). There are a series of complications
in PCNL, including intraoperative complications: Hydrothorax,
bleeding, pelvic perforation and postoperative events, in addition
to fever, urinary tract infections, low back pain, hematuria
(12). In the present case, a
larger number of stones were detected in the ureter compared with
in the kidney (Fig. 1D-G and
H) and so the clearance of ureter
stones >2 cm was the top priority and PCNL was not considered.
To make good use of the advantages of laparoscopy and ureteroscopy,
laparoscope-flexible, ureteroscope-rigid, ureteroscope-pneumatic
lithotripsy combined surgery was performed, which, to the best of
the authors' knowledge, has yet to be reported as a standard
solution for high burden stones according to any guidelines. It
should be noted that a similar surgery was performed in the
treatment of ureteropelvic junction (UPJ) obstruction combined with
renal stones (6). In addition,
Salvado et al (7) presented
a case series on the application of laparoscopy combined with
flexible endoscopy for the treatment of large pelvic stones, UPJ
obstruction, or a poorly functioning kidney. Pyelotomy was
necessary for the removal of large kidney stones. In the present
case, this combined surgery satisfied the requirements of removing
large upper ureter stones (by laparoscopic ureterolithotomy) and
kidney stones and pelvic ureter stones (by RIRS), while remaining
minimally invasive. The use of high-pressure NS irrigation also
assisted in the clearance of kidney stones. The position between
operations was not changed, although the trocar and the ureter
incision was used as the pathway for the ureteroscope. This helped
to both shorten the operation duration and decrease the number of
access sites.
Combining PCNL with RIRS, a new combined surgery
(ECIRS) has been developed in recent years. ECIRS allows the
combined use of all the rigid and flexible items of endourological
equipment. It is usually performed in the Galdakao-modified supine
Valdivia (GMSV) position. The stone-free rates (SFRs) of ECIRS have
been determined to lie in the range 86.7-87.4% (3,13).
The ECIRS method has the advantages of limited exposure of the
surgeon's hands to X-rays (14)
and more patient comfort (in terms of obviating the need for
intraoperative repositioning). Certain of these advantages were
also featured in our combined surgery. RIRS is a necessary step in
GMSV for the management of ureter stones. The overall complication
rate of ECIRS is 38.6% (3) and the
commonest complications are identified as transient fever, urinary
leakages and hematoma and hematuria. Our surgical method omitted
PCNL, which greatly reduced the complications that are usually seen
following PCNL.
Another sandwich surgery, combining PCNL with ESWL,
has been reported previously (15,16).
The approach began with PCNL through one or two tracts and ESWL was
performed either the next day (15) or 2 weeks later (17). However, a PCNL tract is a trauma
for the renal parenchyma, performing ESWL within 24 h adds another
trauma that could lead to renal rupture a severe hemorrhage.
Occasionally, rigid and flexible nephroscopy may be employed to
achieve an improved SFR. The associated SFR is of the order of
67-70% and its main complications were found to be bleeding and
fever. The sandwich surgery mainly focuses on the treatment of
kidney stones, albeit without decreasing the risk of PCNL. The ESWL
was usually applied to stones >2 cm, although this type of
sandwich management is not often used now. For the treatment of
high burden stones in the pelvic kidney or other renal anomalies
(16), there have also been
reports on the use of laparoscopy-assisted PCNL (LA-PNL) (18-20).
The SFR of this method was found to be in the range 75-91% and no
complications were reported.
Based on the literature and our experiences, PCNL is
no doubt the first choice for the treatment of high burden kidney
stones. In our case, however, the most urgent problem to be
resolved was the ureter stones and so PCNL was not employed;
rather, a combination of laparoscopy with rigid and flexible
endourological equipment was used. This has seldom been reported
previously and has enabled us to achieve an ideal SFR with the
protection of kidney function. Using one-stage combined surgery,
the side effects of multi-stage operations on isolated renal
function can be largely avoided. However, the present case also had
certain limitations. For example, for the high burden urolithiasis,
placement of the gauze under the ureter incision prior to cutting
would help to hold the stones that emerge from the urinary tract,
thereby negating the need to search unnecessarily for stones that
might otherwise fall into the abdomen. Furthermore, when flexible
ureteroscopy is used, laser lithotripsy becomes technically
practicable and the introduction of lasers might simplify the
one-stage combined surgery by a further step. We did not perform
more examination such as 24-h urinalysis or spectroscopic analysis
of stones, which is also a limitation to our study.
In the present case, the patient came to our
hospital with the compliant of both stones and, most important,
anuria. The treatment successfully solved the problem of
obstruction, saved the function of solitary kidney and avoided the
possible renal failure. Even if a combined surgery was performed on
the patient, the laboratory examination showed an acceptable
injury. At least, we can try to prolong the duration before his
next admission. This is the value of the therapeutic approach. For
further surveillance measures, we recommend the urine white blood
cell, urine electrolytes and evaluation of hydronephrosis.
Prophylaxis or metaphylaxis measures may yet be adopted. In order
to avoid the antibiotic resistance, antibiotics will be added when
urinary tract infection is diagnosed.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the Shandong
Provincial Natural Science Foundation (grant no.
ZR2021QH313),Academic Promotion Programme by Shandong First Medical
University (grant no. 2020LI001) and the Scientific Research
Incubation Fund of Shandong Provincial Hospital Affiliated to
Shandong First Medical University (grant no. 2020FY041).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding authors on reasonable
request.
Authors' contributions
SD proposed the concept and designed the manuscript.
KZ and SD confirm the authenticity of all the raw data and provided
administrative support. KZ, YC and YG collected and assembled the
data. KZ, YC and DZ analyzed and interpreted the data. SD, YG and
KZ contributed to the minimally invasive surgery. All authors
contributed to the writing of the manuscript and have read and
approved the final manuscript.
Ethics approval and consent to
participate
All procedures performed in this study were in
accordance with the ethical standards of the institutional and/or
national research committee(s) and with the Helsinki Declaration
(as revised in 2013). The present study was approved by the Ethics
Committee of Shandong Provincial Hospital Affiliated to Shandong
First Medical University (Jinan, China; approval no. SWYX: No.
2021-370). The subject signed an informed consent form and had
complete clinical data.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report and accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Liu Y, Chen Y, Liao B, Luo D, Wang K, Li H
and Zeng G: Epidemiology of urolithiasis in Asia. Asian J Urol.
5:205–214. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Sorokin I, Mamoulakis C, Miyazawa K,
Rodgers A, Talati J and Lotan Y: Epidemiology of stone disease
across the world. World J Urol. 35:1301–1320. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Scoffone CM, Cracco CM, Cossu M, Grande S,
Poggio M and Scarpa RM: Endoscopic combined intrarenal surgery in
Galdakao-modified supine Valdivia position: A new standard for
percutaneous nephrolithotomy? Eur Urol. 54:1393–1403.
2008.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Turk C, Petrik A, Sarica K, Seitz C,
Skolarikos A, Straub M and Knoll T: EAU guidelines on
interventional treatment for Urolithiasis. Eur Urol. 69:475–482.
2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Hiki N, Yamamoto Y, Fukunaga T, Yamaguchi
T, Nunobe S, Tokunaga M, Miki A, Ohyama S and Seto Y: Laparoscopic
and endoscopic cooperative surgery for gastrointestinal stromal
tumor dissection. Surg Endosc. 22:1729–1735. 2008.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Fu W, Chen H, Ren C and Zhao J:
Transabdominal laparoscopy and ureteroscopy one-stage surgery in
the treatment of bilateral ureteropelvic junction obstruction
combined with bilateral renal stones: A case report. Exp Ther Med.
24(450)2022.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Salvado JA, Guzman S, Trucco CA and Parra
CA: Laparoscopic pyelolithotomy: Optimizing surgical technique. J
Endourol. 23:575–578. 2009.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Onen A: Grading of hydronephrosis: An
ongoing challenge. Front Pediatr. 8(458)2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Hyams ES, Munver R, Bird VG, Uberoi J and
Shah O: Flexible ureterorenoscopy and holmium laser lithotripsy for
the management of renal stone burdens that measure 2 to 3 cm: A
multi-institutional experience. J Endourol. 24:1583–1588.
2010.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Jiang K, Zhang P, Xu B, Luo G, Hu J, Zhu J
and Sun F: Percutaneous nephrolithotomy vs. retrograde intrarenal
surgery for renal stones larger than 2 cm in patients with a
solitary kidney: A systematic review and a meta-analysis. Urol J.
17:442–448. 2020.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Birowo P, Rasyid N, Atmoko W and Sutojo B:
Case report: An occurrence of steinstrasse in retrograde intra
renal surgery (RIRS) for large staghorn kidney stone: A difficult
experience in managing surgical outcomes. F1000Res.
9(184)2020.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Grosso AA, Sessa F, Campi R, Viola L,
Polverino P, Crisci A, Salvi M, Liatsikos E, Feu OA, Maida FD, et
al: Intraoperative and postoperative surgical complications after
ureteroscopy, retrograde intrarenal surgery, and percutaneous
nephrolithotomy: A systematic review. Minerva Urol Nephrol.
73:309–332. 2021.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Hamamoto S, Yasui T, Okada A, Taguchi K,
Kawai N, Ando R, Mizuno K, Kubota Y, Kamiya H, Tozawa K and Kohri
K: Endoscopic combined intrarenal surgery for large calculi:
Simultaneous use of flexible ureteroscopy and mini-percutaneous
nephrolithotomy overcomes the disadvantageous of percutaneous
nephrolithotomy monotherapy. J Endourol. 28:28–33. 2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Ibarluzea G, Scoffone CM, Cracco CM,
Poggio M, Porpiglia F, Terrone C, Astobieta A, Camargo I, Gamarra
M, Tempia A, et al: Supine Valdivia and modified lithotomy position
for simultaneous anterograde and retrograde endourological access.
BJU Int. 100:233–236. 2007.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Streem SB and Geisinger MA: Combination
therapy for staghorn calculi in solitary kidneys: Functional
results with long-term followup. J Urol. 149:449–452.
1993.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Diri A and Diri B: Management of staghorn
renal stones. Ren Fail. 40:357–362. 2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Merhej S, Jabbour M, Samaha E, Chalouhi E,
Moukarzel M, Khour R and Chaiban R: Treatment of staghorn calculi
by percutaneous nephrolithotomy and SWL: The hotel Dieu de France
experience. J Endourol. 12:5–8. 1998.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Soylemez H, Penbegul N, Utangac MM, Dede
O, Çakmakçı S and Hatipoglu NK: Laparoscopy assisted percutaneous
stone surgery can be performed in multiple ways for pelvic ectopic
kidneys. Urolithiasis. 44:345–352. 2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Haghighi R, Razi A, Haghighi A,
Ebrahimipour N and Teimouri A: Laparoscopy-assisted transperitoneal
percutaneous nephrolithotomy for the treatment of renal stones in a
horseshoe kidney. Res Rep Urol. 12:49–52. 2020.PubMed/NCBI View Article : Google Scholar
|
|
20
|
El-Kappany HA, El-Nahas AR, Shoma AM,
El-Tabey NA, Eraky I and El-Kenawy MR: Combination of laparoscopy
and nephroscopy for treatment of stones in pelvic ectopic kidneys.
J Endourol. 21:1131–1136. 2007.PubMed/NCBI View Article : Google Scholar
|