Introduction
The radiological appearance is one of the most
impart properties of the sealers used in endodontic treatments
(1). An ideal sealer should be
tacky when the two components are mixed (paste-paste or
powder-liquid), to ensure good adhesion between the gutta-percha
cone and the dentin, ensuring a good hermetic root canal seal.
Moreover, it must also be radiopaque so that it can be visualized
on radiographs. The sealer should be bacteriostatic or at least it
should not promote bacterial growth. Furthermore, the sealer should
slowly harden with a slow grip, be insoluble in body fluids and
well tolerated by periapical tissues, and must be soluble in
ordinary solvents if reprocessing is required (1).
The possibility of pushing sealers into the
periapical tissue has increased with the diversification of sealing
techniques. Since root filling extrusion cannot be completely
prevented, there is a chance that the subsequent foreign body
reaction will result in persistent apical periodontitis (2). In a previous study, cytotoxicity and
cytokine production were measured to determine the amount of
debris, and extruded material was found to be the source of higher
levels of both (3).
Economides et al (4) conducted the first study on the impact
of endodontic sealers on ions concentration in major organs. The
authors measured the concentration of zinc and calcium in the brain
and kidneys in mice which were implanted with Ah Plus Jet sealer,
observing an increase in zinc concentration. Khalil and Eid
(5) also observed an increased
inflammatory response in the liver in white albino rats after
exposure to ProRoot MTA and DiaRoot BioAggregate. The effects could
be tracked up to 30 days after exposure.
Other studies showed increased concentrations of
chromium, a known carcinogen, when using materials such as
Biodentine, Micro Mega MTA and BioAggregate (6); however, metal concentrations remained
below safe limits. It is the opinion of the present authors that
overextensions with sealers should be avoided as much as possible
or kept to a minimum (6).
Moreover, meta-analysis studies showed that sealer overextension
negatively affected the healing of periapical lesions (7).
Postoperative radiography remains the easiest method
through which the correctness of the treatment can be assessed,
especially in terms of the amount of sealer that passes into the
periapical tissues (8).
The radiopacity of endodontic materials was
evaluated by several studies (8,9). In
recent years, a new category of sealers has been introduced, which
promises superior results over traditional sealers. The evaluation
of this new category of sealants was performed starting from the
properties of an ideal sealer, meaning that it should possess a
perfect combination of sealing ability and biocompatibility
(10,11). When these materials were positioned
adjacent to periapical bone defects or extruded over the root apex,
the premixed bioceramic sealers released biologically relevant ions
(such as Ca2+ and OH), which may give potential benefits
(12).
Moreover, the radiopacity of the sealers must be
comparable to a 3-mm aluminum standard, according to the ISO
6876:2001 specification.
Evaluation of sealers should be performed both in
vitro and in vivo using postoperative radiographs.
Radiation doses during exposure decreased with the introduction of
digital radiology, possibly leading to a weaker radiological image;
digital software is routinely used to compensate for this
shortcoming.
Materials and methods
Study design
The present study was performed on 52 patients who
were treated for orthodontic lesions at the Endodontic Clinic of
the Faculty of Dental Medicine Craiova from 2020-2022. All patients
provided written informed consent to participate. The study was
approved by the University and Scientific Ethics and Deontology
Commission of the University of Medicine and Pharmacy in Craiova
and patients' information was anonymized.
Among the patients, 36 presented with different
diagnoses of inflammatory pulpal diseases and acute and chronic
apical periodontitis and these patients were selected for inclusion
in the present study. The patients underwent clinical and
retro-alveolar radiological examinations. General data were
collected and recorded on an observational chart, including
socio-demographic data (age group, sex, environment origin, level
of education) and medical history (general clinical examination
data-objectification of the clinical signs related to postoperative
radiological changes, dental examination data and identification of
risk factors for complications and iatrogenesis).
The same endodontic treatment protocol was followed
for all patients included in the study. Patients were subjected to
standard clinical practices and the materials used were not
experimental but intended and commercialized for dental treatment.
The patients received standard endodontic treatments.
Inclusion criteria were defined as adult patients
(>18 years of age) with inflammatory pulpal diseases and acute
and chronic apical periodontitis. The statistical analysis was
performed starting from the analysis of data related to the
patient's age, sex, environment of origin, level of education and
post-operative radiological changes.
Exclusion criteria were defined as follows: patients
≤18 years of age; pregnancy; mental illnesses; breastfeeding;
malignant diseases; and osteoporosis.
In the present study, 36 postoperative radiographs
were used, divided into four groups. Bioceramic-based sealers were
used in three groups, namely Total Fill (FKG Dentaire SA), Bioroot
RCS and Biodentine (both purchased from Septodont, Ltd.), while
patients treated with resin-based AH Plus Jet sealer
(Dentsply-DeTrey; Dentsply Sirona) were used as controls.
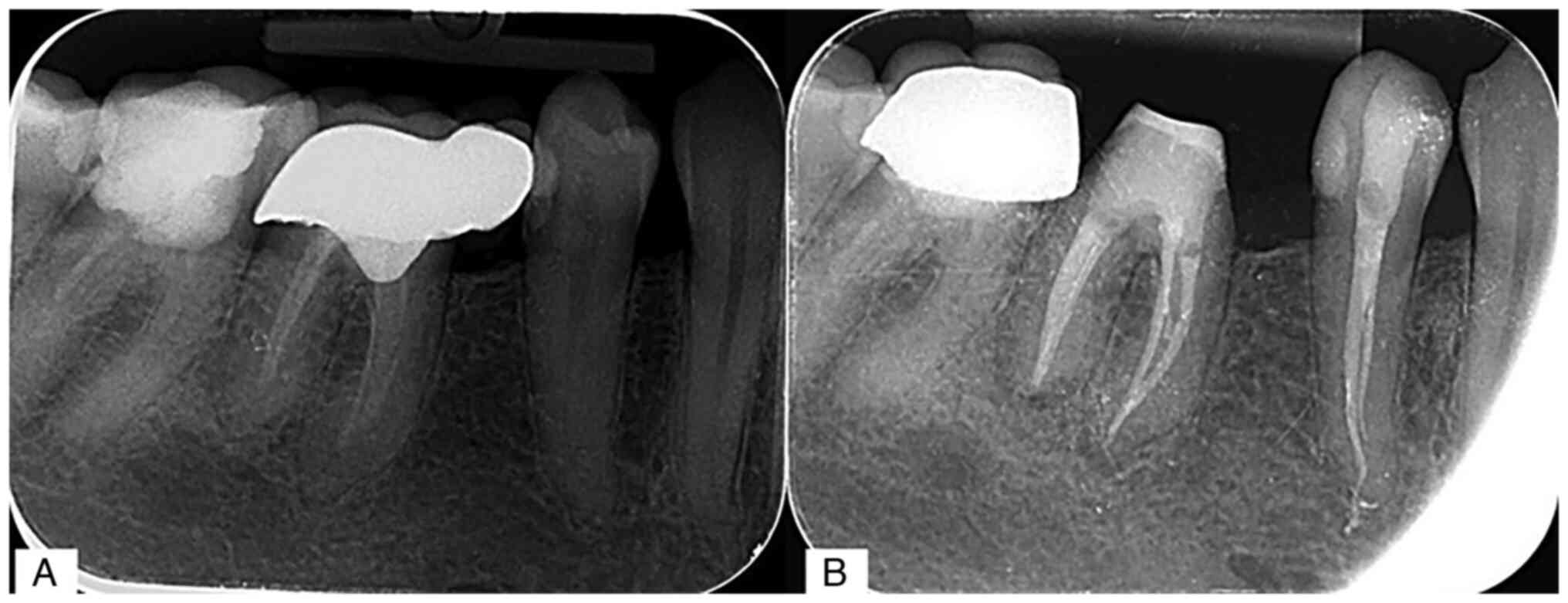
Total Fill is a hydrophilic sealer that chemically
binds to dentine to generate hydroxyapatite. Because of its
extremely alkaline pH, unlike conventional sealers with a low
contraction, it exerts an anti-bacterial while it is setting.
(Fig. 1).
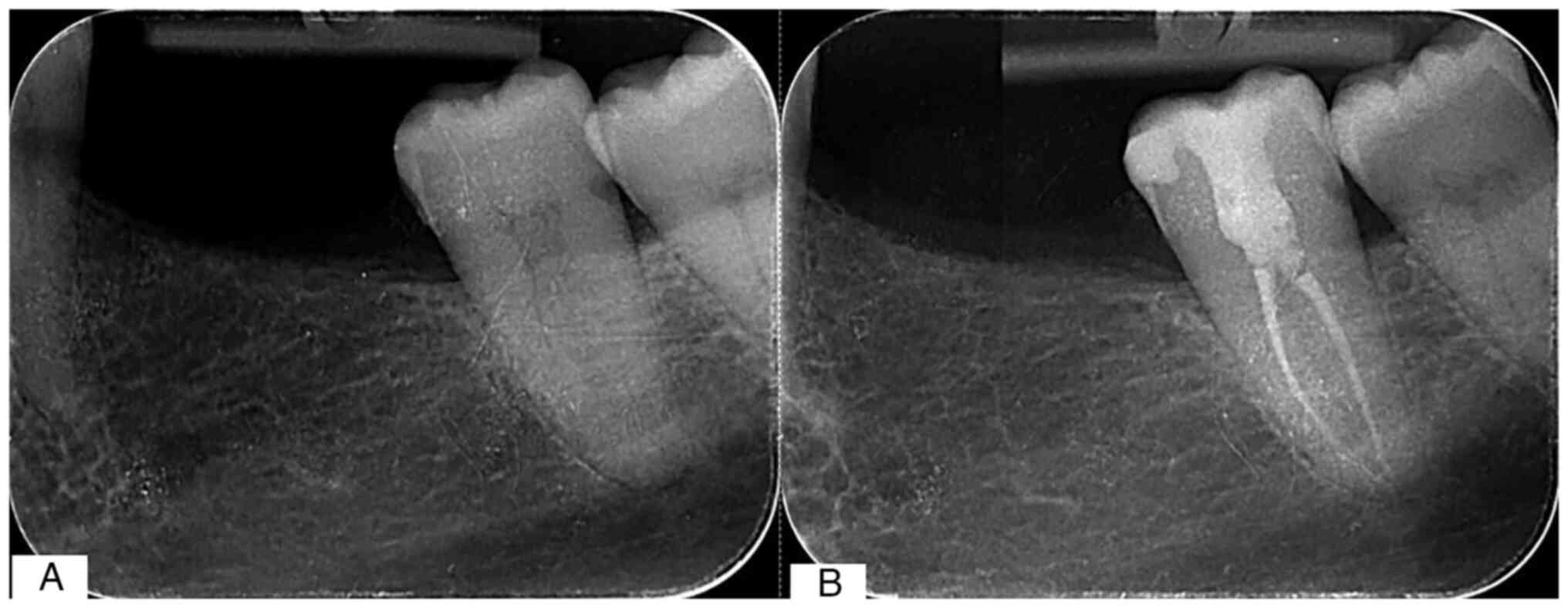
BioRoot RCS is a bioactive mineral root canal sealer
recommended for use with Gutta-Percha (13) (Fig.
2). Gutta-percha is a widely used ‘gold-standard’ endodontic
filling material with praiseworthy qualities of non-toxicity and
biocompatibility (14).
BioRoot RCS benefits from proprietary Active
BioSilicate Technology and has several bioactive qualities such as
biocompatibility, hydroxyapatite production, mineralization of
dentinal structure and alkaline pH (13).
Biodentine is an endodontic sealer composed of
calcium silicate, primarily tricalcium silicate, with certain
additives and a zirconium oxide radiopacifier. It is specifically
designed to be utilized as a dentine replacement material and has
undergone extensive scientific engineering (15).
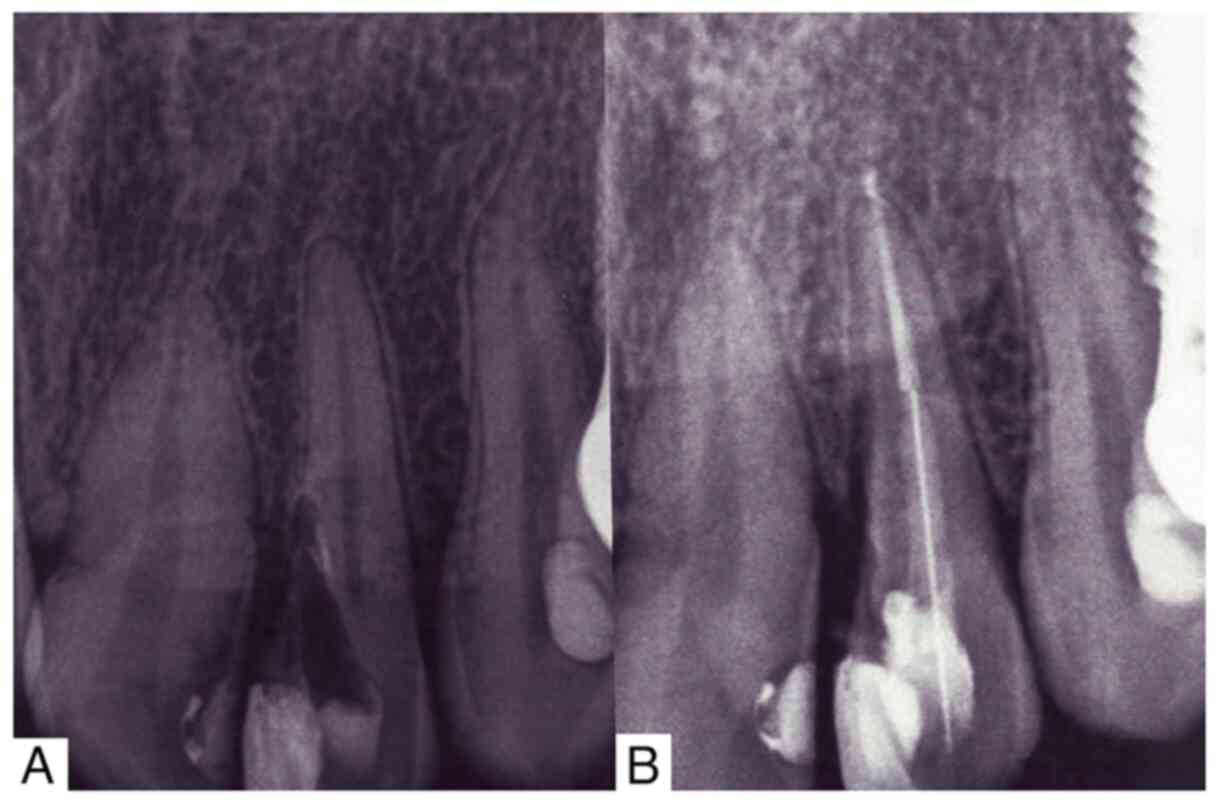
Ah Plus Jet (Fig.
3) is a root canal-bonding epoxy-bisphenol resin sealer that
also contains adamantine. Being an epoxy resin-based sealer, AH
Plus has stronger penetration into the micro-irregularities due to
its creep capacity and long setting time, which improves the
mechanical interlocking between the sealer and root dentin. This
may also explain the increased adherence of AH Plus Jet to the root
dentin (16).
Each tooth was prepared using the Twisted Files
Adaptative system (SybronEndo Corporation) using up to a 6% taper
file. The endodontic system obturation was performed using the
monocone and sealer technique. In each case, the master cone had a
taper of 4% and the gutta-percha cones (Meta Biomed) used were of
4% taper. All accessed cavities were restored using composite
restoration material VisCalor bulk (VOCO GmbH) or Ceram X (Dentsply
Sirona) if the use of fiber post was recommended. Angelus Reforpost
(Angelus Dental Solutions) was used because of the metal wire that
makes them easier to identify radiologically. Fiber posts were
bonded using dual cure bonding (All Bond 2 Dental Adhesive; BISCO,
Inc.) and core build material (Build-it™ FR Core Material; Pentron
Corporation).
Biodentine was used for teeth that were indicated
for its use, i.e. teeth that had large apical diameters,
perforations or that received direct caping or pulpotomies.
Postoperative radiography was performed using a
CS2100 Kodak tube and CS7200 phosphor plates (Kodak). For the
radiography, the Kerr (Kerr Dental Suisse) holder for the phosphor
plate and the parallelism technique were used (Fig. 1).
Because of their similar radiological appearance,
the present study compared the radiodensities of Biodentine and
dentin by measuring their radiolucency values (Fig. 4). Table I reports the values obtained by
measuring the radiolucency of dentin and Biodentine.
 | Table ISealers' radiopacities and their
comparisons at 3-, 6- and 9-mm RA levels. |
Table I
Sealers' radiopacities and their
comparisons at 3-, 6- and 9-mm RA levels.
| | Radiodensity at
different RA levels |
|---|
| Sealer | 3-mm RA (n=9) | 6-mm RA (n=9) | 9-mm RA (n=9) |
|---|
| BioRoot RCS | 102.11±7.39 | 117.22±2.39 | 128.44±10.33 |
| Totalfill | 116.33±5.59 | 132.78±6.83 | 151.78±4.09 |
| Ah Plus Jet | 120.78±7.61 | 143.00±8.28 | 158.22±10.52 |
|
P-valuea | 0.00001781 | 0.00000004 | 0.00000049 |
| Biodentine | - | - | 113.22±10.64 |
| Dentine | - | - | 115.44±10.74 |
|
P-valueb | - | - | 0.64971325 |
For Biodentine, the location of the measurement was
chosen using preoperative radiography where the position of the
canal/perforation to be obturated could be located precisely.
Subsequently, the same location was used on postoperative
radiography to measure the radiolucency, although the radiolucency
corresponding to the canal/perforation was no longer visible due to
the same radiolucency.
Biodentine and dentin have similar radiodensity,
which makes them difficult to differentiate radiologically
(Fig. 4).
Postoperative radiography was performed using CS
2200 Kodak tube-intraoral x-rays system and CS7200 phosphor plates
(Carestream Health). The x-rays were analyzed using the Kodak 2200
Carestream CS7200 3D Imaging Version 3.8.7 (Carestream Health).
This software uses standard units of measurement in dental medicine
to measure radiopacity, which is the density of the radiographic
material compared to soft tissues. Radiopacity is expressed in
Hounsfield units (HU), which is a measure of the apparent density
of a radiographic material. In the case of this software, HU values
are used to measure the level of radiopacity of dental structures
and other materials used in dental treatment. Radiodensity was
measured at three distances from the radiological apex (RA) as
follows: Apical third (3-mm RA); medium (6-mm RA); and coronary
(9-mm RA).
Statistical analysis
Data distribution for each material and any of the
three distances from the RA was analyzed using the Anderson-Darling
normality test and all datasets conformed to the Gaussian
distribution; therefore, the parametric unpaired Student's t-test
or one-way ANOVA followed by Tukey's post hoc test were used to
compare two or multiple groups, respectively. The comparison was
made between the radiodensity values under the effect of the 4
sealers and the corresponding values of dentine. Statistical
analysis of clinical and paraclinical data was performed in
Microsoft Excel 2019 with the XLSTAT 2019.6 data analysis add-on
for Excel (Microsoft Corporation).
Results
Regarding the patient's characteristics, such as
age, sex, background and level of education (Table SI), no statistically significant
differences were found. Instead, statistically significant
differences were found regarding the radiotransparency of different
root canal obturation materials.
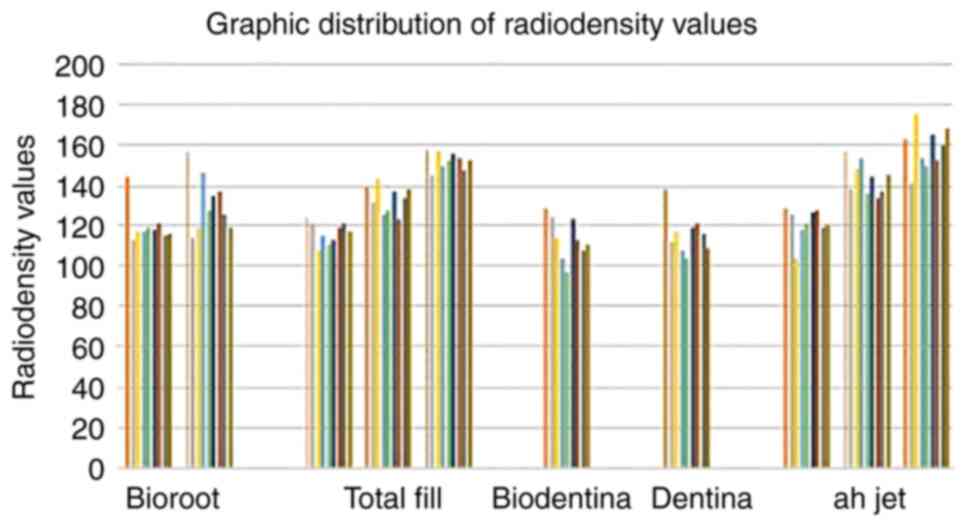
Radiological images were used to compare the
radiodensity of dentine with that of Biodentine sealer (Table SII). Moreover, radiodensity values
were measured for each of the other three sealers at the
aforementioned three RA levels (Table
SIII; Fig. 5). All sealers had
good radiopacity and could be easily detected radiologically.
The statistical analysis of the average radiodensity
values for the three materials showed that at the 3-mm RA level,
there was a highly significant difference between BioRoot RCS and
AhPlus Jet and Total Fill; subsequent post hoc analysis revealed
statistically significant differences in radiodensity values
between BioRoot RCS and the other two materials, but not between
any other group combination, even if Ah Plus Jet radiodensities
were numerically higher than Total Fill radiodensities. At a 6-mm
RA level, the radiodensity of the three materials was significantly
different; Tukey's post hoc analysis revealed that the increase
from BioRoot RCS to Total Fill was statistically significant, as
well as the increase from Total Fill to Ah plus Jet, but no other
group differences were statistically significant. At the 9-mm RA
level, there was also a statistically significant difference
between the radiodensities of BioRoot RCS and those of Ah Plus Jet
or Total Fill. Although the average radiodensities of Ah Plus Jet
or Total Fill were not significantly different, the former was
numerically higher. The radiodensities of Biodentine and dentin did
not differ significantly (P=0.649) (Table I).
Although Ah Plus Jet, a sealer recognized for good
radiopacity, showed higher radiodensity values, Bioceramic sealers
offer good radiopacity comparable to the other fillers, with
TotalFill offering the best values (Table I).
The present results indicated that there were
significant differences in radiopacity between sealers, at certain
levels of obturation. Radiodensity values increased from the apical
to coronary location because the volume of sealer and gutta-percha
was larger at the coronary.
Discussion
Traditional sealers give good obturation combined
with gutta-percha, especially when used in warm techniques
(17). The development of the
bioceramic sealer introduced a new material with high
biocompatibility (18). Sealers
based on bioceramics are a group of sealers that contain calcium
silicate or calcium phosphate. Calcium phosphate enhances the
setting properties of bioceramic sealers, resulting in a
crystalline structure similar to hydroxyapatite that improves the
sealer adhesion to the dentin (19).
The method of obturation of the root canals with
bioceramic materials is important since it has a prognostic value
on the postoperative healing potential, especially after the
iatrogenesis that follows the endodontic treatment, the
effectiveness of the treatment and the maintenance of the results
over time. Moreover, it allows for the identification of structural
changes in the endodontic space, but also periapical, which is
associated with the prediction of post-iatrogenic healing, provides
a complex picture of the pulp pathology (10).
The present study aimed to assess the radiopacity of
bioceramic sealers compared with a common sealer, Ah Plus Jet canal
sealer. The success of endodontic treatment depends on microbial
control, cleaning, shaping and obturating the root canal, using
gutta-percha associated with a fluid sealer to provide hermetic
sealing in all dimensions (20,21).
According to Shah et al (22), the materials used to seal the
endodontic system must differ radiologically from adjacent tissues
as well as from dentin. For the physician, the evaluation of the
quality of the filling is necessary to assess the correctness of
the endodontic treatment performed. A correctly completed filling
contributes significantly to the success of endodontic treatment
(23,24) The methods by which the doctor can
assess the quality of the filling are represented by postoperative
radiography or cone beam CT (CBCT). Because CBCT brings a high dose
of radiation to the patient, compared with classic X-ray, and due
to its high financial cost, RIO radiography remains the most common
method for assessing the quality of treatment.
To the best of our knowledge, there are only a few
reports evaluating the clinical radiological features. Most
previous studies were performed using 1-mm thick sealer discs
compared with a 3-mm thick aluminum disc. If we consider that the
thickness of a lateral canal is often <1 mm, several studies
suggested that a 4-mm thick aluminum disc should be used as
standard (25). It should also be
taken into account that the tooth is surrounded by tissues with
different radiopacities that overlap over the filling, for this
reason, the clinical radiological features may differ from in
vitro studies. As the recommended technique for bioceramic
sealers, physicians most frequently use the monocone technique
(26). It is known that bioceramic
changes when it is used with a technique that uses
thermoplasticized gutta-percha. The monocone technique was shown to
allow a large amount of sealer next to the cone, but still, third
its amount decreased in the apical making it much harder to be
identified (27).
Manufacturers use various opacifying compounds. For
example, Biodentine and Totall Fill contain zirconium oxide while
BioRoot RCS contains zirconium oxide and povidone, which provide a
much more intense radiopacity (28).
The reason for such a difference might be due to
some study results which showed that zirconium oxide possesses
biocompatible characteristics and is indicated as a bioinert
material with favorable mechanical properties and resistance to
corrosion (28).
A highly radiopaque sealer will provide images that
can confuse the doctor in evaluating the filling with a very
homogeneous appearance, while a highly radiolucent sealer might
give the impression that the filling is incomplete, which is the
case with Biodentine. This drawback originated from the first
indication of Biodentine as a dentine replacement material. In this
situation, the same radiopacity could be an advantage (29). In a different situation, like with
retrograde filling material, large amounts of materials could be
left in the bone or simply confuse different clinicians on the
presence of the filling (30).
Dammaschke et al (31), in the evaluation of the
radiological aspect, concluded that dentine was difficult to
differentiate from Biodentine, a result that was also confirmed by
Tanalp et al (32). In an
in vitro study, the Biodentine filler showed a greater
radiopacity than a 3-mm thickness aluminum standard (33), which was also confirmed by
Camilleri et al (34).
Nonetheless, Coaguila-Llerena et al (35) showed that Biodentine failed to
exceed the 3-mm aluminum standard. These results should be
interpreted carefully as conditions of experimentation, storage and
other factors may influence the results of radiopacity studies.
Dželetović et al (36) performed in vitro study
comparing Ah Plus Jet with several bioceramic sealers and concluded
that Ah Plus Jet had a radiopacity higher than that of BioRoot RCS.
Prüllage et al (30) also
found no statistical differences between Ah Plus Jet and BioRoot
RCS in vitro.
Hrab et al (37) performed in vitro studies to
determine that Total fill had radiopacity above 3 mm aluminum
(38). Thus, all the sealers
studied fall within the ISO standard (38,39).
An interesting correlation was found by Miyashita et al
(40) who showed that in the case
of sealers that presented a good radiopacity in two dimensions, the
probability that they presented artifacts during the CBCT
evaluation increased. Therefore, a sealer with a lower radiopacity
could be favored in the future, as the frequency of CBCT use
increases.
Although in the present study, the Ah Plus Jet
sealer still had higher values in terms of radiodensity,
statistically all sealers behaved the same and offered a possibly
good radiological evaluation, which was confirmed by other studies
as well.
Unlike previous in vitro studies, the present
study was performed in vivo, emphasizing the importance of a
good radiological evaluation of fillings made with bioceramic
materials, well tolerated by the periapical tissues, which
decreased the number of endodontic treatment failures.
In conclusion, Biodentine-based sealants showed a
radiodensity close to that of dentin, which made it quite difficult
for the physician to assess radiologically the correctness of the
canal filling. The results of the current study showed that there
were statistical differences between the Ah jet sealer, a
resin-based sealer recognized for good radiopacity, and
bioceramic-based sealers, which offer very good radiopacity close
to that offered by Ah Plus Jet. The current study provided
important insights that could facilitate the implementation,
validation and continuous improvement of the materials used in
canal obturation.
Supplementary Material
Distribution of patients according to
sex, demographic, level of education and clinicopathological
information.
Radiodensity values in Hounsfield
units for Biodentine and dentin.
Radiodensity values in Hounsfield
units, by sealer groups, for Bioroot RCS, Totalfill and Ah Plus at
different root levels.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CA, MT and CP conceived the study. LG and CA
designed the study. CC and AGN confirm the authenticity of all the
raw data. CP, OD and AGN provided resources. MT, OD and CA were
responsible for data curation. CC and CP drafted and wrote the
manuscript. CP, CA and LG wrote, edited and reviewed the
manuscript. CA acquired the radiographic images. AGN, MJT, OAD, LG
and CA made substantial contributions to the acquisition, analysis,
and interpretation of data for the research. HM supervised the
study. MT managed the project. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
The study was conducted according to the guidelines
of the Declaration of Helsinki and approved by the Ethics Committee
of the University of Medicine and Pharmacy of Craiova (approval
reference no. 26/20.05.2022). Written informed consent was obtained
from the subjects involved in the study.
Patient consent for publication
The patients involved in the study provided written
consent for the publication of their radiographic images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Grossman L (ed): Obturation of root canal.
In: Endodontic Practice. 10th edition. Lea and Febiger,
Philadelphia, PA, p297, 1982.
|
|
2
|
Kum KY, Kim EC, Yoo YJ, Zhu Q, Safavi K,
Bae KS and Chang SW: Trace metal contents of three tricalcium
silicate materials: MTA Angelus: Micro Mega MTA and Bioaggregate.
Int Endod J. 47:704–710. 2014.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Silva EJ, Brito ME, Ferreira VD,
Belladonna FG, Neves AA, Senna PM and De-Deus G: Cytotoxic effect
of the debris apically extruded during three different retreatment
procedures. J Oral Sci. 58:211–217. 2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Economides N, Kotsaki-Kovatsi VP,
Poulopoulos A, Kolokuris I, Rozos G and Shore R: Experimental study
of the biocompatibility of four root canal sealers and their
influence on the zinc and calcium content of several tissues. J
Endod. 21:122–127. 1995.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Khalil WA and Eid NF: Biocompatibility of
bioaggregate and mineral trioxide aggregate on the liver and
kidney. Int Endod J. 46:730–737. 2013.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Simsek N, Bulut ET, Ahmetoğlu F and Alan
H: Determination of trace elements in rat organs implanted with
endodontic repair materials by ICP-MS. J Mater Sci Mater Med.
27(46)2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Aminoshariae A and Kulild JC: The impact
of sealer extrusion on endodontic outcome: A systematic review with
meta-analysis. Aust Endod J. 46:123–129. 2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Malka VB, Hochscheidt GL, Larentis NL,
Grecca FS, Fontanella VR and Kopper PM: A new in vitro method to
evaluate radio-opacity of endodontic sealers. Dentomaxillofac
Radiol. 44(20140422)2015.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Gu S, Rasimick BJ, Deutsch AS and Musikant
BL: Radiopacity of dental materials using a digital X-ray system.
Dent Mater. 22:765–770. 2006.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Pontoriero DIK, Ferrari Cagidiaco E,
Maccagnola V, Manfredini D and Ferrari M: Outcomes of
endodontic-treated teeth obturated with bioceramic sealers in
combination with warm gutta-percha obturation techniques: A
Prospective Clinical Study. J Clin Med. 12(2867)2023.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Rekha R, Kavitha R, Venkitachalam R,
Prabath SV, Deepthy S and Krishnan V: Comparison of the sealing
ability of bioceramic sealer against epoxy resin based sealer: A
systematic review & meta-analysis. J Oral Biol Craniofac Res.
13:28–35. 2023.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Zamparini F, Prati C, Taddei P, Spinelli
A, Di Foggia M and Gandolfi MG: Chemical-physical properties and
bioactivity of new premixed calcium silicate-bioceramic root canal
sealers. Int J Mol Sci. 23(13914)2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Retana-Lobo C, Tanomaru-Filho M,
Guerreiro-Tanomaru JM, Benavides-García M, Hernández-Meza E and
Reyes-Carmona J: Push-Out bond strength, characterization, and ion
release of premixed and powder-liquid bioceramic sealers with or
without gutta-percha. Scanning. 2021(6617930)2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Hargreaves KM and Berman LH (eds):
(Editor): Cohen's pathways of the pulp. Elsevier, St. Louis, MO,
2016.
|
|
15
|
Rebolledo S, Alcántara-Dufeu R, Luengo
Machuca L, Ferrada L and Sánchez-Sanhueza GA: Real-time evaluation
of the biocompatibility of calcium silicate-based endodontic
cements: An in vitro study. Clin Exp Dent Res. 9:322–331.
2023.PubMed/NCBI View
Article : Google Scholar
|
|
16
|
Souza LC, Neves GST, Kirkpatrick T, Letra
A and Silva R: Physicochemical and biological properties of AH plus
bioceramic. J Endod. 49:69–76. 2023.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Akhtar H, Naz F, Hasan A, Tanwir A,
Shahnawaz D, Wahid U, Irfan F, Ahmed MA, Almadi KH, Alkahtany MF,
et al: Exploring the most effective apical seal for contemporary
bioceramic and conventional endodontic sealers using three
obturation techniques. Medicina (Kaunas). 59(567)2023.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Cirstea AC, Gheorghiță L, Diaconu OA,
Bataiosu M, Georgescu RV, Dascălu IT, Amza OE, Nicola AG, Raescu M
and Tuculina MJ: Bioceramic-based root canal sealers: A review.
Romanian J Oral Rehab. 12:48–54. 2020.
|
|
19
|
Mendes AT, Silva PBD, Só BB, Hashizume LN,
Vivan RR, Rosa RAD, Duarte MAH and Só MVR: Evaluation of
physicochemical properties of new calcium silicate-based sealer.
Braz Dent J. 29:536–540. 2018.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Guerreiro-Tanomaru JM, Duarte MA,
Gonçalves M and Tanomaru-Filho M: Radiopacity evaluation of root
canal sealers containing calcium hydroxide and MTA. Braz Oral Res.
23:119–123. 2009.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Schilder H: Filing root canals in three
dimensions. 1967. J Endod. 32:281–290. 2006.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Shah PM, Chong BS, Sidhu SK and Ford TR:
Radiopacity of potential root-end filling materials. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod. 81:476–479. 1996.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Al-Haddad A and Che Ab Aziz ZA:
Bioceramic-based root canal sealers: A review. Int J Biomater.
2016(9753210)2016.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Hommez GM, Coppens CR and De Moor RJ:
Periapical health related to the quality of coronal restorations
and root fillings. Int Endod J. 35:680–689. 2002.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Ng YL, Mann V and Gulabivala K: A:
Prospective study of the factors affecting outcomes of non-surgical
root canal treatment: Part 2: tooth survival, Int Endod. J.
44:610–625. 2011.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Piconi C and Maccauro G: Zirconia as a
ceramic biomaterial. Biomaterials. 20:1–25. 1999.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Jainaen A, Palamara JE and Messer HH:
Push-out bond strengths of the dentine-sealer interface with and
without a main cone. Int Endod J. 40:882–890. 2007.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Reszka P, Grocholewicz K, Droździk A and
Lipski M: Evaluation of the radiopacity of selected
calcium-silicate root canal sealers. Pomeranian J Life Sci.
65:17–24. 2019.
|
|
29
|
Malkondu Ö, Karapinar Kazandağ M and
Kazazoğlu E: A review on biodentine, a contemporary dentine
replacement and repair material. Biomed Res Int.
2014(160951)2014.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Caron G, Azérad J, Faure MO, Machtou P and
Boucher Y: Use of a new retrograde filling material (Biodentine)
for endodontic surgery: Two case reports. Int J Oral Sci.
6:250–253. 2014.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Kaup M, Schäfer E and Dammaschke T: An in
vitro study of different material properties of Biodentine compared
to ProRoot MTA. Head Face Med. 11(16)2015.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Tanalp J, Karapınar-Kazandağ M, Dölekoğlu
S and Kayahan MB: Comparison of the radiopacities of different
root-end filling and repair materials. ScientificWorldJournal.
2013(594950)2013.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Grech L, Mallia B and Camilleri J:
Investigation of the physical properties of tricalcium silicate
cement-based root-end filling materials. Dent Mater. 29:e20–e28.
2013.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Camilleri J, Sorrentino F and Damidot D:
Investigation of the hydration and bioactivity of radiopacified
tricalcium silicate cement, Biodentine and MTA Angelus. Dent Mater.
29:580–593. 2013.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Coaguila-Llerena H, Ochoa-Rodríguez VM,
Castro-Núñez GM, Faria G, Guerreiro-Tanomaru JM and Tanomaru-Filho
M: Physicochemical properties of a bioceramic repair material-
BioMTA. Braz Dent J. 31:511–515. 2020.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Dželetović B, Milanović I, Antonijević Đ,
Badnjar J, Petrov Z, Antić S and Ležaja-Zebić M: Radiopacity of
premixed and two-component Calcium silicate-based Root Canal
sealers. Balk J Dent Med. 26:161–166. 2022.
|
|
37
|
Prüllage RK, Urban K, Schäfer E and
Dammaschke T: Material properties of a tricalcium
silicate-containing, a mineral trioxide aggregate-containing, and
an epoxy resin-based root canal sealer. J Endod. 42:1784–1788.
2016.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Hrab D, Chisnoiu AM, Badea ME, Moldovan M
and Chisnoiu RM: Comparative radiographic assessment of a new
bioceramic-based root canal sealer. Clujul Med. 90:226–230.
2017.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Aminoshariae A, Primus C and Kulild JC:
Tricalcium silicate cement sealers: Do the potential benefits of
bioactivity justify the drawbacks? J Am Dent Assoc. 153:750–760.
2022.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Miyashita H, Asaumi R, Sakamoto A, Kawai T
and Igarashi M: Root canal sealers affect artifacts on cone-beam
computed tomography images. Odontology. 109:679–686.
2021.PubMed/NCBI View Article : Google Scholar
|