Introduction
The testes occasionally fail to completely descend
along the normal path or may deviate from it. The former condition
is called undescended testis and is present in ~4.5% of newborns,
with its incidence being higher in preterm babies (1), whereas the latter is known as
testicular ectopia (TE). TE is a rare anomaly characterized by the
testes lying outside the normal descent route (retroperitoneum to
the scrotum). There are several variants of TE, including perineal
ectopic testis (PET), femoral and penile ectopic testis, transverse
TE (TTE) and preperitoneal and anterior abdominal wall ectopic
testis (2). PET is the most common
variant (3); in this case, the
testis is located in the perineal region, with its final position
often being further from the groin than a scrotal testis, and is
covered by a perineal fat pad rather than being within the
low-temperature environment of the scrotum. Although it is the most
common type, PET accounts for <1% of abnormal testicular
migration cases, and may be as rare as <1/10,000 cases (4). TTE, also known as crossed TE, is an
extremely rare anomaly of testicular descent, during which
bilateral gonads migrate along the same inguinal canal toward the
scrotum, and it is commonly associated with an inguinal hernia. To
the best of our knowledge, <100 cases have been reported in the
literature worldwide (5). An
accurate preoperative diagnosis is challenging because it is easy
to diagnose simple undescended testis in the majority of the
reported cases. However, with the improvement of medicine,
diagnostic advancements continue to be made. Laparoscopy surgery is
the main treatment (6).
Laparoscopy is commonly used in the diagnosis and treatment of TTE.
The early diagnosis and surgical treatment of ectopic testes
facilitate normal development of the genitourinary system and
prevent complications. Ultrasonography, laparoscopy and magnetic
resonance imaging (MRI) have been used for the diagnosis of this
condition (2).
Case report
Case 1
A 4-month-old male patient was admitted to the
Department of Pediatric Surgery (The Affiliated Hospital of Jining
Medical University, Jining, China) presenting with bilateral
absence of the testes. The patient was treated with human chorionic
gonadotropin (HCG; each ampoule contains 5,000 IU of HCG injection
powder; Nanjing Organon Pharmaceutical Co., Ltd.) 1,000 IU via
intramuscular injection twice a week for 5 weeks. The right
testicle reached the bottom of the scrotum 8 months later, but the
left scrotum remained empty. At 1 year and 2 months of age, the
parents of the patient identified an oval mass (diameter, 1.0 cm)
in the right inguinal region, which was painless, retractable and
gradually increased in size. The ultrasound examination (ZS3 Exp;
Zonare) showed the echo of two testes; the epididymis was detected
at the right scrotum and external inguinal ring, and no testicular
echo was identified in the left inguinal or scrotum. A transverse
incision of the right inguinal region identified a testis in the
right inguinal canal. Bilateral spermatic cords and vessels were
carefully dissected, and no fused abnormality or remnant of
Mullerian structure was identified. Since the left spermatic cord
was long enough to reach the left hemiscrotum, the scrotal septum
was opened through subcutaneous tunneling and the left testis was
fixed at the bottom of the left scrotum (transseptal orchidopexy).
Next, the hernia sac was transected and ligated at a high level. No
testicular abnormalities were observed following ultrasonography
(ZS3 Exp; Zonare) of the scrotum during the 2-year follow-up.
Case 2
A 2-year and 10-month-old male was admitted to
Department of Pediatric Surgery in the Affiliated Hospital of
Jining Medical University with a left inguinal mass. On physical
examination, an egg-sized mass was felt in the left inguinal groin
area after the increase in abdominal pressure, which then retracted
automatically with the lack of pressure. The left testis was felt
at the bottom of the scrotum, while a testicular substance was
found at the level of the left external inguinal ring. No
testicular substance was felt in the right hypoplastic scrotum and
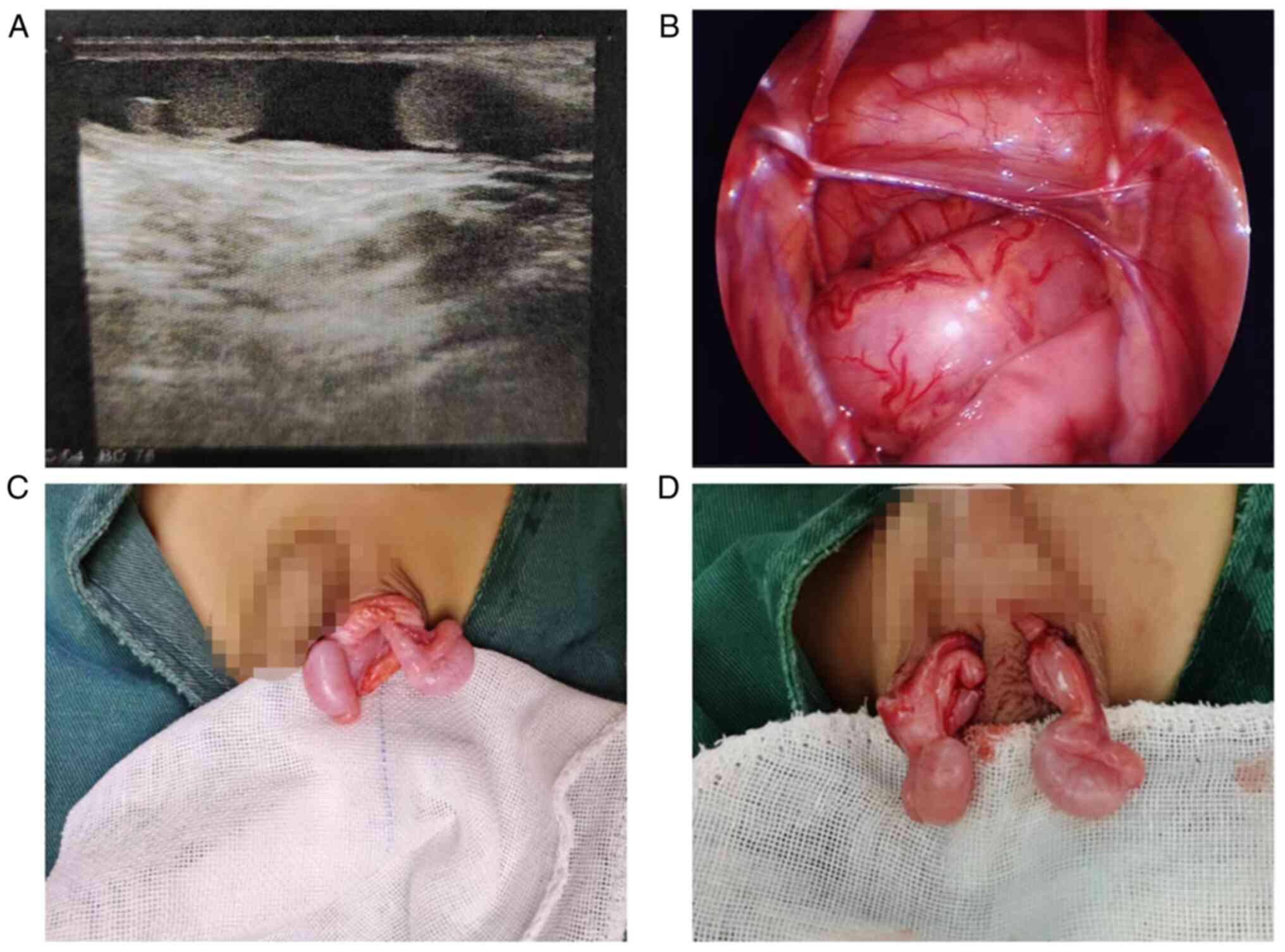
groin area. The ultrasound indicated that the right scrotum was
empty, while the echo of two testes and epididymis were detected at
the left scrotum and external inguinal ring (Fig. 1A). During laparoscopic exploration,
it was observed that the right spermatic cord and vessels travelled
upwards above the bladder and entered the left inguinal canal
together with the left ones (Fig.
1B). Laparoscopic (German Wolf) exploration was employed to
pull the two testicles down to the scrotum to avoid an incision in
the inguinal area, identify the laterality of the two testicles
directly and avoid confusing the laterality of the testes during
fixation. Remnant Mullerian duct structures and other fused
anomalies were not discovered (Fig.
1C). Next, the internal ring was ligated at the extraperitoneal
area and transseptal orchidopexy was performed (Fig. 1D). No testicular abnormalities were
observed in the ultrasonography of the scrotum following the
surgery.
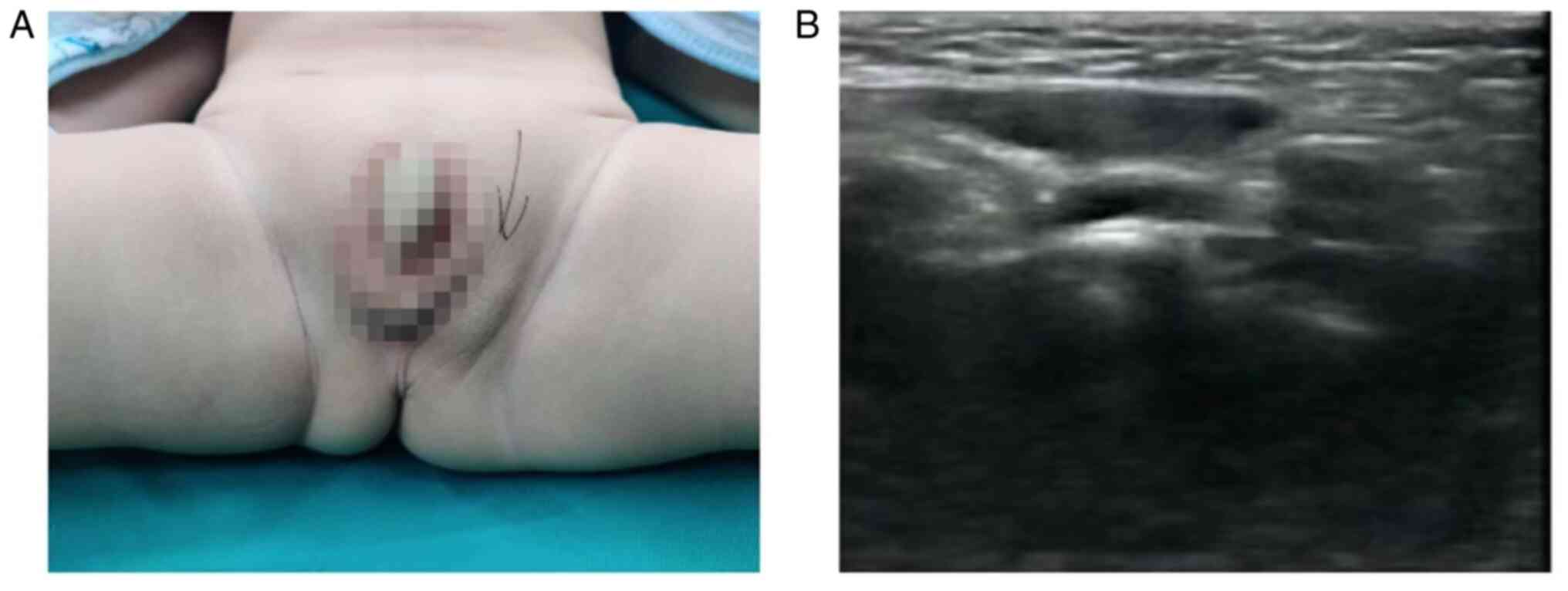
Case 3
A male patient aged 1 year and 3 months came to the
Department of Pediatric Surgery with the right testis missing and a
left perineal mass. On physical examination, the bilateral scrotum
was hypoplastic, the right testis was felt in the ipsilateral
inguinal region and the left was in the ipsilateral perineum
(Fig. 2A). Ultrasound confirmed
the results of the aforementioned examination (Fig. 2B). The left testis was easily
discovered in the subcutaneous tunnel and limited dissection of the
spermatic cord and blood vessels was adequate to perform
orchidopexy. No testicular anomalies were observed via
ultrasonography of the scrotum during routine follow-ups (10
months). Differences between the three cases are presented in
Table I.
 | Table IClinical characteristics of the three
cases. |
Table I
Clinical characteristics of the three
cases.
| Age at diagnosis | Type of ectopic
testis | Location of
testes | Presentation | Location of testes
(US) | Types of
operation | Follow-up/ testicular
abnormalities |
|---|
| 1 Y, 2 M | TTE | R scrotum L
inguinal | R inguinal hernia L
undescended testis | R scrotum L
inguinal | Transseptal
orchidopexy | 2 Y/N |
| 2 Y, 10 M | TTE | R inguinal L external
inguinal ring | Left inguinal hernia
Right undescended testis | R external inguinal
ring L scrotum | Laparoscopy- assisted
transseptal orchidopexy | 1 Y, 4 M/N |
| 1 Y, 3 M | Perineum ectopic | R inguinal L
perineum | R undescended testis
L perineum ectopic | R: inguinal L
perineum | Orchidopexy | 10 M/N |
Discussion
The descent of the testes is hypothesized to occur
in two phases: Intra-abdominal and inguinal migration. The ectopic
testis completes inguinal migration normally but is misdirected
outside the normal path of descent below the external ring
(7). TE can be an abnormality of
testicular development and is caused by several factors, such as
persistent Müllerian duct syndrome, androgen disorder, true
hermaphroditism and mixed gonadal dysgenesis (8). It can also be an abnormality caused
by descent and migration processes, including anomalous insertion
of the distal gubernaculum testis (9). It has been hypothesized to result
from abnormal fixation or movement of the peritoneum during
testicular descent (4). There are
several variants of TE, including PET, femoral and penile ectopic
testis and TTE.PET is the most common variant of TE where the
testis was found in the perineal region (10-12).
In perineal ectopia, the testis is not truly undescended, but
exhibits malformed cryptorchidism as the testis is not located in
the scrotum, its final position is often further from the groin and
it is covered by a perineal fat pad, where it benefits from the
specialized, low temperature environment (3). There are numerous theories for the
pathogenesis of PET, including congenital obstruction of the
secondary external inguinal ring and the subsequent migration of
the testis to the perineal pouch (12), abnormal interplay between androgen
and calcitonin gene-related peptide release from the genitofemoral
nerve (10) and aberrant
gubernacular stabilization caused by an anomaly at the distal
extremity of the gubernaculum (11). These factors may also lead to the
occurrence of femoral and penile ectopic testis (2,13).
The cases reported in the present study were admitted to the
hospital due to an abnormal perineal mass and were diagnosed with
PET following preoperative examination. However, the specific cause
of the disease was not defined because the hormone and gene levels
were not determined.
TTE is an extremely rare congenital anomaly
characterized by the presence of two testes in the same hemiscrotum
or the descent or migration of two testes along the same inguinal
canal (14). TTE is frequently
associated with congenital inguinal hernia and less frequently with
additional genitourinary anomalies, including hypospadias, seminal
vesicle cyst, renal agenesis and persistent Müllerian duct
(15). The persistence of
Müllerian duct structures has been reported in 20-49% of patients
with TTE and is hypothesized to be due to inadequate anti-Mullerian
hormone or because the target organ is not sensitive to this
hormone (16,17). However, the Müllerian duct
structures were not found in either of the TTE cases in the present
study. At present, the pathogenesis of TTE is not clear; the
mainstream views on its pathogenesis are as follows: Both testes
being derived from the same germinal ridge; mechanical effect of
persistent Müllerian duct structures preventing testicular descent
or causing both testicles to descend toward the same hemiscrotum
and defective gubernacular formation (3). No single theory explains the
pathogenesis. Due to the high cost, the long duration of genetic
testing and the refusal of the parents of the children, gene
testing and hormone evaluation are not routinely carried out in
clinical treatment. Therefore, regardless of the type of ectopic
testis, clarifying its specific pathogenesis is difficult.
A careful physical examination reveals an empty,
sagging scrotum. For all children with scrotal cavitation,
regardless of the type of ectopic testis, careful clinical
examination along the descent path and all potential ectopic testis
sites is important. These include the perineum, femoral canal, base
of the penis, intraperitoneal cavity, contralateral pouch, inguinal
canal and deep ring (13). Imaging
models can be used for the diagnosis of TE in cases where physical
examination is inconclusive or in children who are uncooperative or
who have had a genitourinary surgery. Ultrasound is especially used
extensively in diagnostic procedures to avoid ionizing radiation
(18). If physical examination and
ultrasound cannot confirm this, CT and MRI may be considered to
locate the testis before surgery. CT has a relatively high success
rate in locating ectopic testes. However, the pediatric population
is unique as there is a risk of developing a malignancy due to
ionizing radiation; therefore, CT is not routinely used in
diagnosis and localization of ectopic testes (19). MRI is an option, as it has an
accuracy similar to CT without ionizing radiation exposure, but it
is expensive, may not be readily accessible and typically involves
a form of sedation or anesthesia (20). Diagnosing PET based on an empty
scrotum and swollen perineum is easier (21). However, the preoperative diagnosis
of TTE is difficult; the diagnosis of the first TTE case in the
present study was determined intraoperatively. Due to this
complexity, TTE is often misdiagnosed as simple cryptorchidism,
testicular tumor and single testis deformity. The presence of
ectopic masses can be detected by imaging diagnostic techniques,
but the specific nature of the masses cannot be clearly defined in
most cases (2). Therefore, the
diagnosis of TTE is often made intraoperatively during inguinal
hernia repair (22). The first
case in the present study began with HCG therapy as simple
cryptorchidism; although the most recent guidelines recommend the
surgical management of a congenital undescended testis, HCG
hormone, has been widely used for the treatment of congenital
undescended testes since 1930 (23,24),
but the treatment of congenital undescended testes with HCG hormone
has low success rates; it may, however, be effective in high
scrotal testes (25). Since the
present case was not a simple cryptorchidism, a complete cure was
not achieved.
TE is associated with complications, such as trauma,
torsion and bilateral infertility (26). Therefore, surgical treatment is
necessary and early surgical intervention is important for
long-term prognosis. The aim of treatment is the fixation of the
testes into the respective hemiscrotum (27) to restore optimal development
environment, improve the later development potential and decrease
incidence of malignant transformation. Surgical correction is
recommended at 1 year of age, as cryptorchidism may show definite
histological changes (28). It is
reported that it is not reasonable to expect TTE to have a natural
recovery, so it is very important for surgical treatment to be
performed as soon as possible following the detection of TTE
(29,30). The optimal time of surgery is at
1-2 years of age, and the age of operation tends to decrease
continuously. The treatment principles of TTE are to preserve
fertility, decrease risk of testicular neoplasia and repair
congenital anomalies, hernia and orchidopexy (6,31).
Common surgical methods for TTE treatment include transseptal,
extraperitoneal orchidopexy, testicular anatomical reduction,
Fowler-Stephens primary or Stage descent orchidopexy and in
situ orchidopexy, testicular transplantation or orchiectomy
(32). Both TTE cases in the
present study underwent transseptal orchidopexy. For PET,
orchiopexy is recommended and surgical intervention should be
performed early, regardless of the existence of an inguinal hernia,
as there is no clear benefit to delaying the procedure until the
child is ≥6 months old (33).
Orchidopexy is an option for children <2 years old. The PET
cases in the present study were treated using simple orchidopexy;
however, if atrophic testes were identified, orchiectomy should be
performed, which may effectively reduce the occurrence of long-term
testicular malignancies (34).
Orchidopexy, which is suitable for PET and femoral and penile
ectopic testis, is usually easy to perform, as long as it is the
length of the testicular vessels and vas deferens is adequate
(35). The traditional method of
testicular fixation via scrotal incision is no longer recommended
for the treatment of ectopic testes alone due to limitations such
as testicular position, spermatic cord length and inability to
observe other abdominal malformations (4). The minimally invasive laparoscopic
technique achieves great visual assessment of the abnormal
testicular development situation, spermatic cord length, vas
deferens and ectopic spermatic cord, presence of Müllerian tube
residues and deformity of other abdominal organs.
In conclusion, TE is a rare abnormality and its
etiology remains unclear. It is characterized by the testes being
outside the normal descent path. There are several variants of TE,
including PET and TTE. PET is the most common variant and can be
detected by physical examination. However, preoperative diagnosis
of TTE is difficult and is usually achieved using imaging or
intraoperatively. Ectopic testes should be treated surgically at an
early stage, often with orchidopexy or transseptal orchidopexy, to
ensure good postoperative recovery; however, the overall management
of ectopic testes, long-term follow-up and possible complications
need further study.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the Doctoral Startup
Foundation of the Affiliated Hospital of Jining Medical University
(grant no. 2016-BS-014).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JC and MG collected data and drafted the manuscript.
HL, LS, NH and CZ performed data analysis. LS, JS, CH and NH
performed minimally invasive surgery. CH, JC, MG and LS confirm the
authenticity of all the raw data. All authors have read and
approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of the Affiliated Hospital of Jining Medical University
(approval no. 2023-01-C015).
Patient consent for publication
The parents or legal guardians of all the children
involved in the present study provided written informed consent for
publication.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Khatwa UA and Menon PS: Management of
undescended testis. Indian J Pediatr. 67:449–454. 2000.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Iliodromiti Z, Karapati E, Sokou R,
Boutsikou T, Iacovidou N and Salakos C: Bilateral ectopic femoral
testes: A rare cause of empty scrotum. Urol Case Rep.
33(101348)2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Punwani VV, Wong JSY, Lai CYH, Chia JCY
and Hutson JM: Testicular ectopia: Why does it happen and what do
we do? J Pediatr Surg. 52:1842–1847. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Priam A, Chabani N, Klein C and Haraux E:
Scrotal orchidopexy for perineal ectopic testis. Arch Pediatr.
29:404–406. 2022.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Oludiran OO and Sakpa CL: Crossed ectopic
testis: A case report and review of the literature. Pediatr Surg
Int. 21:672–673. 2005.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Zhou G, Yin J, Jiang M, Yang Z and Li S:
Clinical characteristics, ultrasonographic findings, and treatment
of pediatric transverse testicular ectopia: A 10-year retrospective
review. Urology. 154:249–254. 2021.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Koc G, Sural YS, Filiz ND and Yilmaz Y:
Perineal ectopic testis. Urol J. 9:433–435. 2012.PubMed/NCBI
|
|
8
|
Clarnette TD, Sugita Y and Hutson JM:
Genital anomalies in human and animal models reveal the mechanisms
and hormones governing testicular descent. Br J Urol. 79:99–112.
1997.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Favorito LA, Klojda CA, Costa WS and
Sampaio FJ: Is there a relationship with anomalous insertions of
the distal gubernaculum testis and testicular ectopia? Analysis in
human fetuses and patients with cryptorchidism. J Urol. 170 (2 Pt
1):554–557. 2003.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Hadziselimović F: Mechanism of testicular
descent. Urol Res. 12:155–157. 1984.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Redman JF: Observations on course of
cremasteric muscle in perineal testes with commentary on
gubernaculum. Urology. 41:462–465. 1993.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Mirilas P and Mentessidou A: The secondary
external inguinal ring and associated fascial planes: Surgical
anatomy, embryology, applications. Hernia. 17:379–389.
2013.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Ramareddy RS, Alladi A and Siddappa OS:
Ectopic testis in children: Experience with seven cases. J Pediatr
Surg. 48:538–541. 2013.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Bchini F, Boughdir M, Daib A, Tlili S,
Hellal Y and Kaabar N: Type 2 transverse testicular ectopia: A case
report. Urol Case Rep. 40(101909)2021.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Yıldız A, Yiğiter M, Oral A and Bakan V:
Transverse testicular ectopia. Pediatr Int. 56:102–105.
2014.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Sipani M, Bhat A and Prabhakar G:
Transverse testicular ectopia: A report of five cases and review of
literature. J Indian Assoc Pediatr Surg. 25:404–407.
2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Tasian GE, Copp HL and Baskin LS:
Diagnostic imaging in cryptorchidism: Utility, indications, and
effectiveness. J Pediatr Surg. 46:2406–2413. 2011.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Gkekas C, Symeonidis EN, Tsifountoudis I,
Georgiadis C, Kalyvas V, Malioris A and Papathanasiou M: A rare
variation of transverse testicular ectopia (TTE) in a young adult
as an incidental finding during investigation for testicular pain.
Case Rep Urol. 2018(6919387)2018.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Smith-Bindman R, Lipson J, Marcus R, Kim
KP, Mahesh M, Gould R, Berrington de González A and Miglioretti DL:
Radiation dose associated with common computed tomography
examinations and the associated lifetime attributable risk of
cancer. Arch Intern Med. 169:2078–2086. 2009.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Budianto IR, Tan HL, Kinoshita Y, Tamba
RP, Leiri S and Taguchi T: Role of laparoscopy and ultrasound in
the management of ‘impalpable testis’ in children. Asian J Surg.
37:200–204. 2014.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Ulubay M: Perineal ectopic testis: A rare
congenital anomaly. Urol Case Rep. 24(100853)2019.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Shah M, Odugoudar A, Chawla A and Hameed
ZB: Transverse testicular ectopia: Two rare adult cases and a
review of literature. BMJ Case Rep. 13(e232240)2020.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Ellerkamp V, Schmid A, Blumenstock G,
Hrivatakis G, Astfalk W, Loff S, Fuchs JJ and Zundel S: Guideline
implementation for the treatment of undescended testes: Still room
for improvement. J Pediatr Surg. 53:2219–2224. 2018.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Abacı A, Çatlı G, Anık A and Böber E:
Epidemiology, classification and management of undescended testes:
Does medication have value in its treatment? J Clin Res Pediatr
Endocrinol. 5:65–72. 2013.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Elsherbeny MS and Abdelhay S: Human
chorionic gonadotrophin hormone for treatment of congenital
undescended testis: Anatomical barriers to its success. J Pediatr
Surg. 54:2413–2415. 2019.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Jlidi S, Echaieb A, Ghorbel S, Khemakhem
R, Ben Khalifa S and Chaouachi B: Perineal ectopic testis: Report
of four paediatric cases. Prog Urol. 14:532–533. 2004.PubMed/NCBI(In French).
|
|
27
|
Higgins M, Smith DE, Gao D, Wilcox D, Cost
NG and Saltzman AF: The impact of age at orchiopexy on testicular
cancer outcomes. World J Urol. 38:2531–2536. 2020.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Lugg JA, Penson DF, Sadeghi F, Petrie B,
Freedman AL, Gonzalez-Cadavid NF, Hikim AS and Rajfer J: Prevention
of seminiferous tubular atrophy in a naturally cryptorchid rat
model by early surgical intervention. J Androl. 17:726–732.
1996.PubMed/NCBI
|
|
29
|
Boyle TA, Perez EA, Diez R, Sola JE, Sanz
EE, Garcia A and Fuentes EJ: Transverse testicular ectopia
discovered following reduction of an inguinal hernia. J Pediatr
Surg. 54:608–611. 2019.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Saleem M, Ather U, Mirza B, Iqbal S,
Sheikh A, Shaukat M, Sheikh MT, Ahmad F and Rehan T: Persistent
mullerian duct syndrome: A 24-year experience. J Pediatr Surg.
51:1721–1724. 2016.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Abdullayev T and Korkmaz M: Transvers
testicular ectopia: A case report and literature review. Int J Surg
Case Rep. 65:361–364. 2019.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Picard JY, Cate RL, Racine C and Josso N:
The persistent müllerian duct syndrome: An update based upon a
personal experience of 157 cases. Sex Dev. 11:109–125.
2017.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Stoykov B, Kolev N, Dunev V and Genov P:
Torsion of the testis with perineal ectopy. Urol Case Rep.
29(101087)2020.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Kuyumcuoglu U, Erol D, Matay E and Ozen H:
Bilateral perineal ectopic testes. Int Urol Nephrol. 22:271–273.
1990.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Nouira F, Ben Ahmed Y, Jlidi S, Sarrai N,
Chariag A, Ghorbel S, Khemakhem R and Chaouachi B: Management of
perineal ectopic testes. Tunis Med. 89:47–49. 2011.PubMed/NCBI
|