Introduction
Lower back pain (LBP) is a common clinical problem
that affects 70~85% of the population worldwide. Chronic pain
seriously affects the quality of life and mental state of patients,
which in turn incurs a substantial social burden (1). LBP is commonly caused by lumbar disc
herniation (LDH) (2).
Anatomically, the intervertebral disc (IVD) is a complex tissue
composed of three parts: the central nucleus pulposus (NP), the
peripheral annulus fibrosus (AF), and two cartilage endplates
(CEPs) (3,4). During IVD formation, NP tissue is
captured by the surrounding AF and CEPs to isolate the NP from the
immune system. Traditionally, the intervertebral disc is identified
as an immune-privileged organ (5).
Degeneration or trauma of the intervertebral disc can lead to the
exposure of antigen components to circulating blood, resulting in
an abnormal autoimmune response and chronic inflammation,
accompanied by low back pain and sciatica (6,7).
Therefore, intervertebral disc degeneration (IVDD) is an autoimmune
disease and is accompanied by the inflammatory response that
constantly exacerbates the process of degeneration (8). Furthermore, when the body is under
pathological conditions, such as autoimmune diseases, tumors,
inflammation or infections, these factors not only can block the
normal differentiation of immature myeloid cells (IMCs), but also
induce them to become a bone marrow-derived inhibitor
myeloid-derived suppressor cells (MDSCs), which are massively
recruited and activated in the peripheral blood, bone marrow or
tumor tissue (9). Therefore, this
study seeks to explore the specific changes in MDSCs in LDH.
MDSCs are immunoregulatory cells, and they prevent
uncontrolled inflammation and maintain homeostasis of immune
response in the early tissue damage (10). However, in chronic inflammation and
extensive tissue damage caused by severe trauma or chronic virus
infection, the normal differentiation of MDSCs is interrupted by
pathological processes, resulting in their prolonged expansion and
enhanced immunosuppressive function (11). Under these conditions, MDSCs become
chronic inflammatory cells that impair protective immune responses,
which lead to an inability to clear infection, increased tissue
damage from autoimmune responses, and a failure to restore tissue
homeostasis and regulate tissue repair (12). Therefore, MDSCs play a dual role in
autoimmunity. On the one hand, these differences can be explained
by the different autoimmune models and phenotypes used in various
studies and strategies for identifying MDSCs (13). On the other hand, these
contradictory findings may also indicate that the dual contribution
to protecting and worsening the disease depends on the severity and
stage of the disease.
MDSCs are characterized by a lack of lineage markers
(B cells, T cells, and natural killer cells), low or negative
expression of HLA-DR, and expression of monocytes and the myeloid
marker CD33(14). According to the
different surface markers, MDSCs can be divided into granulocyte
MDSCs, or polymorphonuclear MDSCs (G-MDSCs: HLA-DR-
Lin- CD33+ CD15+
CD14-), and mononuclear MDSCs (M-MDSCs:
HLA-DR-/low CD14+). In addition, there is
also a group of phenotypically immature MDSCs called known as early
MDSCs (eMDSCs: HLA-DR- Lin- CD33+
CD14- CD15-) in human peripheral blood
mononuclear cells. The frequency of MDSCs in patients with LDH, the
MDSC subpopulations, and their clinical relevance remain unclear to
date.
At present, the gold standard for the diagnosis of
LDH is magnetic resonance imaging (MRI) followed by surgery, and
conservative treatment, such as bed rest, functional exercise, and
physical therapy, is the primary therapeutic option (15). Both these treatments are aimed at
individual symptom relief and supportive treatment, not radical
recovery of LDH. The main problems with using MRI for diagnosis are
that the procedure is time-consuming, results in potential
radiation exposure, lacks predictive capability and is not
cost-effective.
This study aims to find an immune marker that is a
potential target for the treatment of LDH. We have undertaken a
comprehensive flow cytometry-based study to investigate the
phenotype of circulating MDSCs in patients with LDH. We hope to
identify potential subtypes that could serve as an auxiliary
examination item for LDH and therapeutic targets to prevent the
progression of IVDD.
Materials and methods
Study population
This study was approved by the Institutional Review
Board (Ethical batch number: PJ 2022-02-16). From June 2021 to June
2022, 40 patients with LDH (Pfirrmann classification) with complete
clinical data were recruited at the First Affiliated Hospital of
Anhui Medical University, China (Table
I). Fifteen healthy donors (HD) were used as controls, and they
also underwent MRI to rule out LDH. Written informed consent was
obtained before blood sampling.
 | Table IBreakdown of demographics between
patients with stages I-IV LDH. |
Table I
Breakdown of demographics between
patients with stages I-IV LDH.
| Pfirrmann
stage | n | Age (years) | Sex
(male/female) |
|---|
| Stage I | 15 | 43.53±19.26 | 7/8 |
| Stage II | 14 | 44.43±16.73 | 6/8 |
| Stage III | 15 | 46.60±16.13 | 8/7 |
| Stage IV | 11 | 46.73±16.26 | 5/6 |
|
F/χ2 | - | 0.832 | 0.347 |
| P-value | - | 0.483 | 0.951 |
LDH was confirmed in these patients using MRI. All
subjects had no history of underlying diseases such as infections,
tumors, and chronic inflammation known to affect the level of
MDSCs. It is worth mentioning that all the samples were collected
at patient's first visit. Because of the persistence of the
intervertebral disc injury, we could not study the effect of the
length of LDH history on MDSCs. Our inclusion criteria were as
follows:(1) patients who were
hospitalized and diagnosed with lumbar disc herniation in the First
Affiliated Hospital of Anhui Medical University; (2) peripheral blood samples for all
patients obtained at their initial visit; (3) patients with low back pain or lower
limb pain and numbness as the main clinical symptoms; (4) magnetic resonance imaging showing
degenerative changes in lumbar intervertebral discs; (5) no conditions affecting the structure
of the spine; and (6) no previous
lumbar spine surgery or other treatments that would deform the
lumbar spine.
Furthermore, our study used the following strict
exclusion criteria: (1) patients
with severe scoliosis; (2)
patients with a recent history of lumbar spine trauma or fracture;
(3) patients with nondegenerative
or chronic infectious diseases of the lumbar spine; (4) patients with diseases of the
autoimmune system or metabolic diseases; (5) patients who had previously or were
currently on immunoadaxis; (6)
patients who had used glucocorticoids in the last 3 months; and
(7) patients who had used NSAIDs
within the last 2 weeks.
GEO database analysis
The Gene Expression Omnibus (GEO), a publicly
available NCBI genomics database of high-throughput gene expression
data, was thoroughly queried for all datasets involving studies of
MDSCs. The eligibility criteria for analysis were as follows:
(1) studies with IVDD tissue
samples; (2) studies with
information on the technology and platform utilized; and (3) studies that included normal groups as
controls. Based on these criteria, two datasets for G-MDSCs were
downloaded from the repository; no dataset for M-MDSCs was found.
Principal component analysis (PCA) was performed on the datasets
for dimensionality reduction and quality control. If the quality of
a particular sample was insufficient, it was excluded from
subsequent analysis.
MRI classification
MRI has proven to be an extremely valuable tool in
the assessment of normal and pathological spinal anatomy. It is
commonly used to assess the containment of discal material by the
outer fibers of the AF and posterior longitudinal ligaments. The
German Siemens 3.0T MRI scanner was used to perform lumbar
intervertebral disc MRI examinations on the subjects. Patients were
placed in the conventional supine position, and the scan sequences
included fat-suppressed T1, T2 and DW I transverse coronal and
sagittal three-dimensional scan sequences. All scanned images were
processed and transferred to the PACS image reading system, and two
deputy chief physicians of the Department of Orthopedics used the
Pfirrmann grading system (10,16)
to classify the lumbar intervertebral disc degeneration based on
the lumbar MRI images. The degree of LDH was evaluated according to
the morphologic structure of the responsible disc and assigned one
of five stages (I-V) (criteria presented in Table II). The control group was
identified as stage I.
| Table IIPfirrmann grading scale standard. |
Table II
Pfirrmann grading scale standard.
| Pfirrmann
scale | Structure | Margin between
nucleus and annular | Signal
intensity | Height of disc |
|---|
| I | Homogenius,
white | Clear | High signal | Normal |
| II | Inhomogenius or
gray horizontal line | Clear | High signal | Normal |
| III | Inhomogenius,
gray | Unclear | Medial signal | Normal to slightly
decreased |
| IV | Inhomogenius, gray
to dark | Vanish | Low signal | Normal to obviously
decreased |
| V | Inhomogenius,
dark | Vanish | Low signal | Collapse |
Whole blood staining and MDSC
immunophenotyping
Peripheral blood (2-3 ml) was collected from
patients and processed within 6 h. For lysing of the red blood
cells (RBCs), 10x RBC lysis buffer was diluted to 1x working
concentration with deionized water. The 1x solution was then warmed
to 25˚C before use. Then, 50.0 ml 1x RBC lysis buffer was added to
each 50 ml centrifuge tube containing up to 2.5 ml whole blood.
Each tube was gently vortexed immediately after adding the lysate,
before incubation at 25˚C in the dark for 10-15 min. Thereafter,
the tubes were centrifuged at 350 x g for 5 min, and the
supernatant was aspirated without disturbing the precipitate. The
pellet was resuspended in an appropriate amount of PBS buffer and
washed once. For antibody labelling, the live cells were counted
and resuspended in PBS buffer at a concentration of
5-10x106 cells/ml, and then 100 µl cell suspension was
dispensed into respective 2 ml Eppendorf tubes.
To determine the frequency and phenotype of MDSCs in
fresh whole blood, five surface markers were combined, including
the lineage-specific mixtures (CD3/CD19/CD56/CD14/CD20/CD16)-APC
(Biolegend, Cat: 348803, 20 µl/test), HLA-DR-APC-Cy7 (Biolegend,
Cat: 307617, 5 µl/test), CD33-PerCP-Cy5.5 (Biolegend, Cat: 303413,
5 µl/test), CD15-FITC (Biolegend, Cat: 323003, 5 µl/test) and
CD14-PE (Biolegend, Cat: 301805, 5 µl/test). Incubation with
recommended concentration of fluorescent primary antibodies were
performed for 15-20 min on ice in the dark. Then, the solution was
centrifuged at 350 x g for 5 min and washed 2x with at least
2 ml of PBS buffer. Afterwards, the cell pellet was resuspended in
0.5 ml of cell staining buffer. As the sample was fresh peripheral
blood, no viability staining solution was added to exclude dead
cells. Finally, flow cytometry analysis was performed on a CytoFLEX
flow cytometer (Beckman Coulter, Brea, CA, USA), and FlowJo v10.7.2
(TreeStar, Ashland, OR, USA) was used to analyze the data.
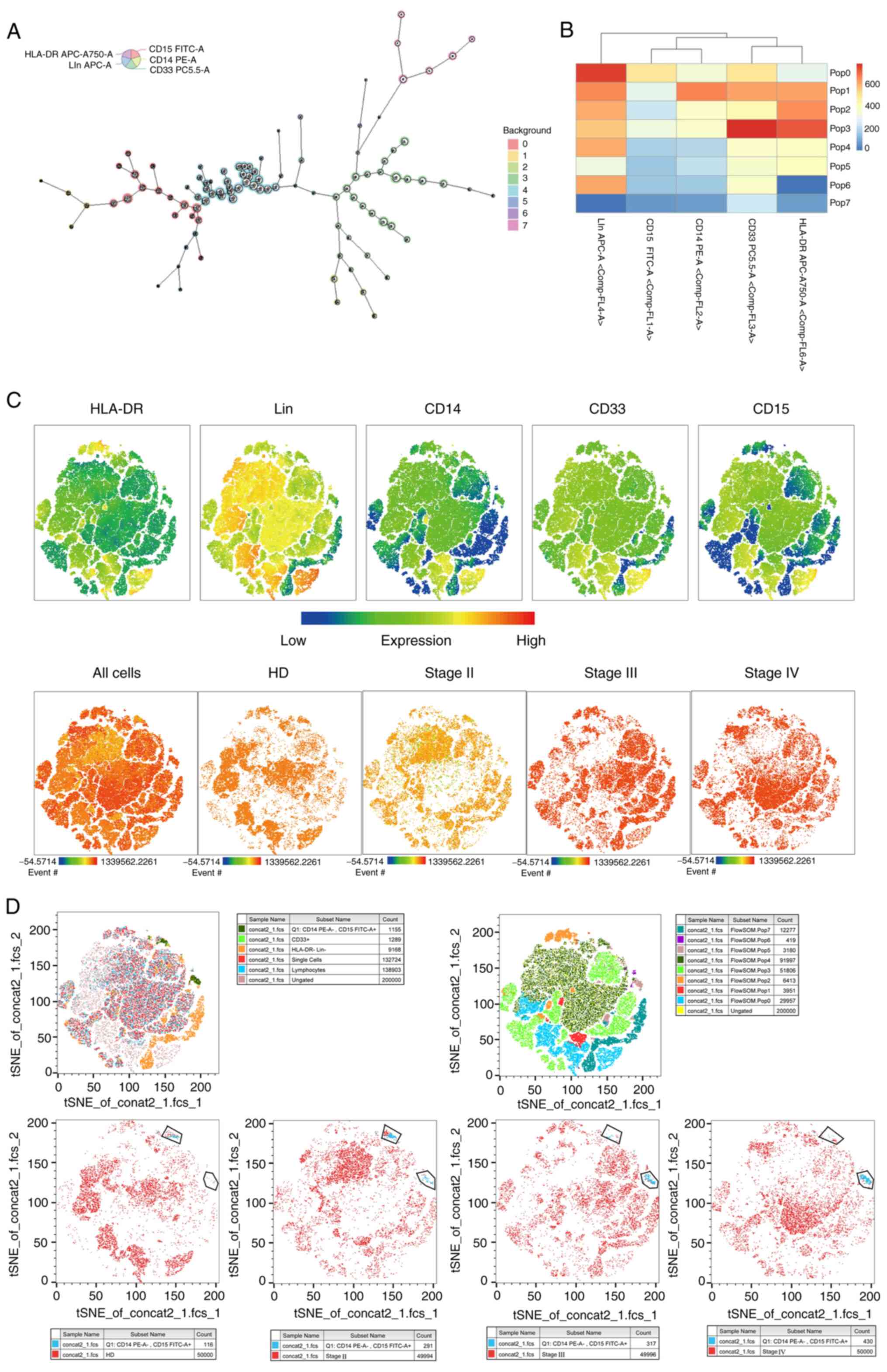
Data analysis. Cytometry data
auxiliary analysis of G-MDSCs
We used manual gating and automated cluster analysis
methods for exploratory analysis. Data analysis of flow cytometry
is traditionally performed through manual gating, which includes a
visual inspection of two-dimensional scatterplots to identify known
cell populations. However, this technique suffers from several
major limitations, including subjectivity, operator bias,
difficulty in detecting unknown cell populations, and difficulty in
reproducibility. Therefore, we additionally used clustering and
dimensionality reduction as an algorithmic method to reduce
subjectivity and bias. The dimensionality reduction algorithm,
t-distributed stochastic neighborhood embedding (t-SNE) was used to
visualize the high-dimensional single cell data. Furthermore,
FlowSOM was used as an automatic analysis method to perform cluster
analysis on single biological samples, multiple samples based on
each sample, or combined data from multiple samples. The detected
clusters (cell populations) were then analyzed individually or
compared between samples.
We obtained consistent results with the manual
gating by performing the computer algorithm. The Barnes-Hut
implementation of t-SNE by the ‘tsne’ package of R with 1,000
iterations, a perplexity parameter of 30, a trade-off θ of 0.5, and
the ‘FlowSOM’ package of R with 8 meta clusters were used to
perform the dimensionality reduction algorithm. Each island
represents a group of similar cells, and from the results, we can
see directly that the number of G-MDSCs increased with the
increasing clinical LDH stage.
Statistics
Distribution analysis was performed by the
D'Agostino-Pearson test on Prism v8.0.2 (GraphPad, San Diego, CA,
USA). Unpaired parametric student's t-test was used to determine
the statistical significance between observations and groups.
Assuming that the number of MDSCs did not follow a normal
distribution, comparisons between different groups were made using
the Mann-Whitney U test. Spearman's test was used to assess the
correlation between circulating MDSCs and lumbar disc herniation
stage. The diagnostic accuracy of biomarkers was determined by
receiver operating characteristic (ROC) curve analysis, using
GraphPad Prism v8.0.2. Statistical analyses were performed on Prism
v8.0.2 (GraphPad, San Diego, CA, USA) and SPSS version 13.0 for
Windows (SPSS Inc., Chicago, IL, USA). Differences were considered
statistically significant at two-tailed P<0.05.
Results
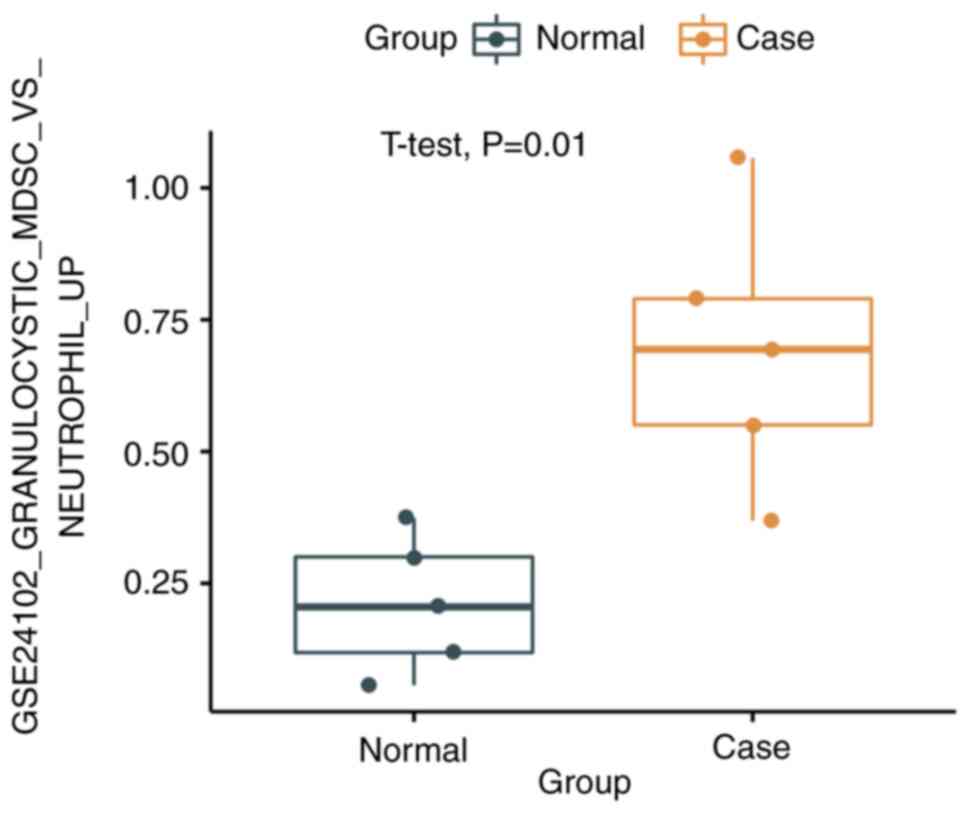
GSE database predicts changes in the
proportion of MDSC subtypes
The gene expression sequencing results of the
GSE56081 dataset were collected from the public platform GEO of the
NCBI, including the NP of 5 patients with lumbar disc degeneration
and 5 control NP tissues. In addition, referring to the
GSE24102_GRANULOCYSTIC_MDSC_VS_NEUTROPHIL_UP differential gene set
(using a series of up-regulated genes in G-MDSCs as a reference),
we used the ssGSEA method to score 10 patients in the GSE56081
cohort to obtain the infiltration of G-MDSCs in the NP according to
the condition of each patient. The corresponding sequencing data of
M-MDSCs were not found. We demonstrated that compared with the NP
of normal patients, the G-MDSCs infiltration score of patients with
lumbar disc degeneration was significantly higher (0.692 vs. 0.211,
P=0.01) (Fig. 1).
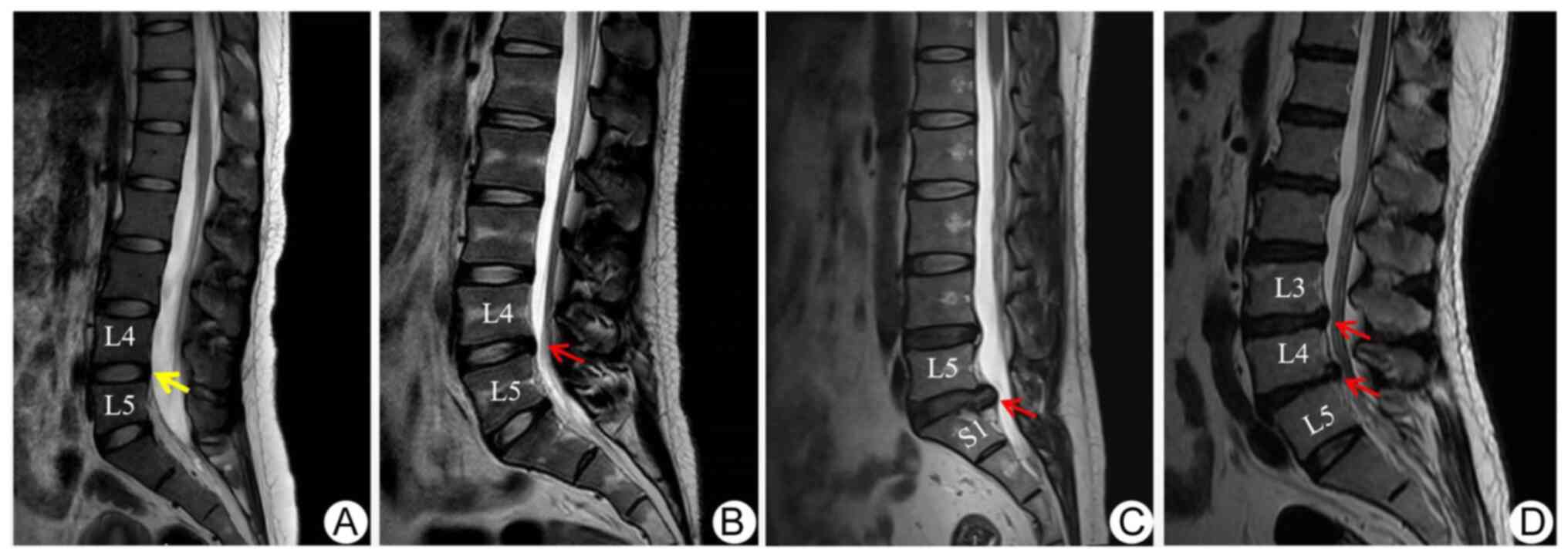
The gating of different MDSC subtypes
in blood from patients
Using five-color flow cytometric analysis, we aimed
to explore all three subsets of circulating MDSCs:
HLA-DR- Lin- CD33+
CD14- CD15- immature MDSCs (a),
HLA-DR- Lin- CD33+
CD15+ CD14- G-MDSCs (b), and
HLA-DR-/low CD14+ M-MDSCs (c) in whole blood
from patients with LDH and age-matched healthy controls. IVDDs were
divided into stages I-IV (Fig. 2),
while no stage V cases-the most severe condition-were observed in
our samples. The frequency of circulating MDSCs was calculated as a
percentage of single-cells. Representative flow cytometric data of
a healthy donor and a patient with stage IV is shown in Fig. 3A-B.
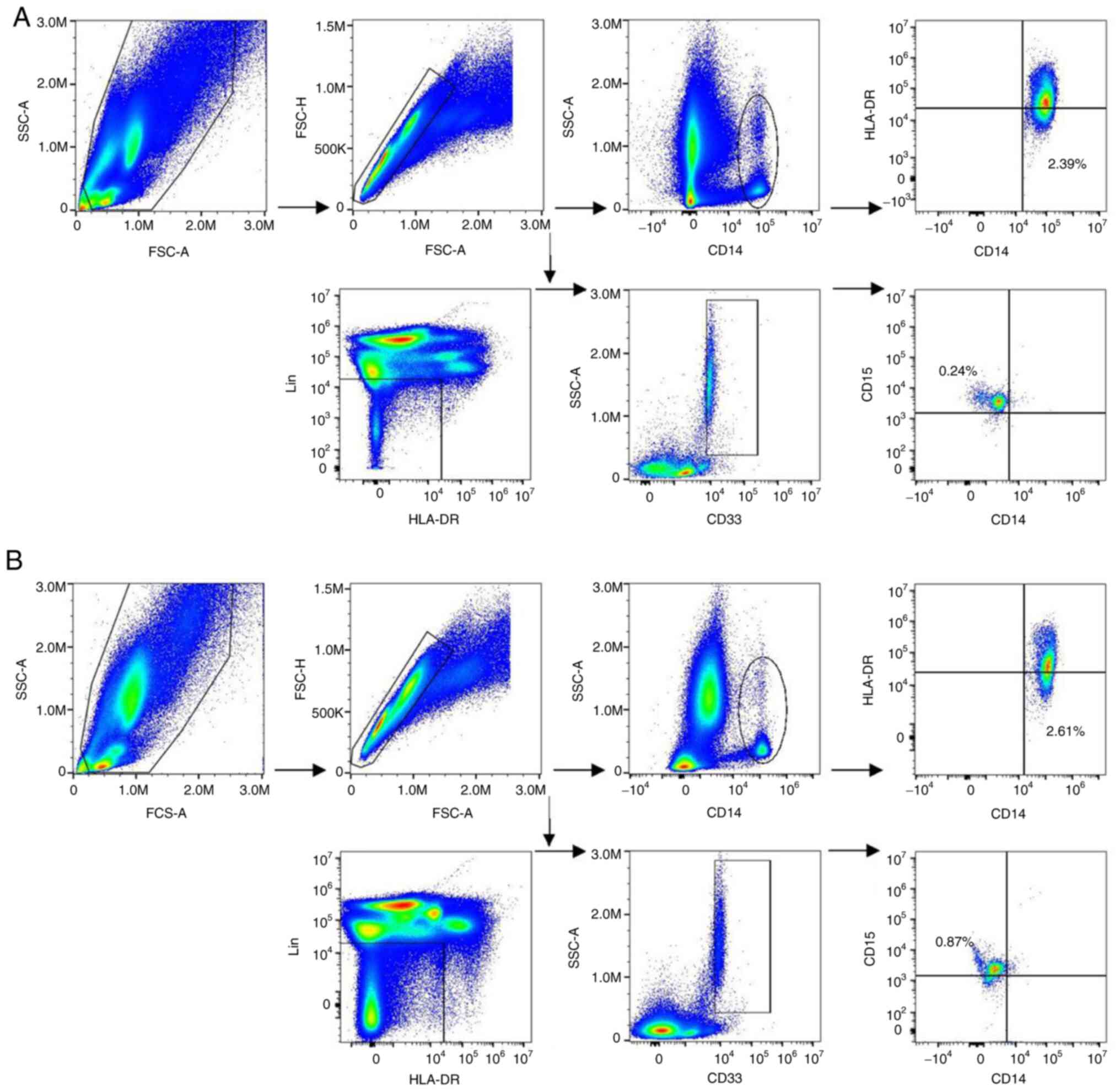 | Figure 3Identification and characterization
of different MDSC subtypes in blood from patients with LDH. (A)
Frequency of G-MDSCs and M-MDSCs were 0.24 and 2.39%, respectively,
in a healthy donor. Gating strategy for MDSCs: For immature MDSCs
and G-MDSCs, the acquired cells were first gated on the
non-expression of Lin and HLA-DR. Within this population, the
fraction of cells expressing both CD33 and SSC was determined. The
expression of CD15 was further explored in this fraction. For
M-MDSCs, SSC vs. CD14 was first gated to isolate the monocytes cell
populations, and then HLA-DR vs. CD14 was plotted for M-MDSCs. (B)
Frequency of G-MDSCs and M-MDSCs were 0.87 and 2.61%, respectively,
in a patient with stage IV LDH. MDSC, myeloid-derived suppressor
cells; LDH, lumbar disc herniation; G-MDSC, granulocyte MDSCs. |
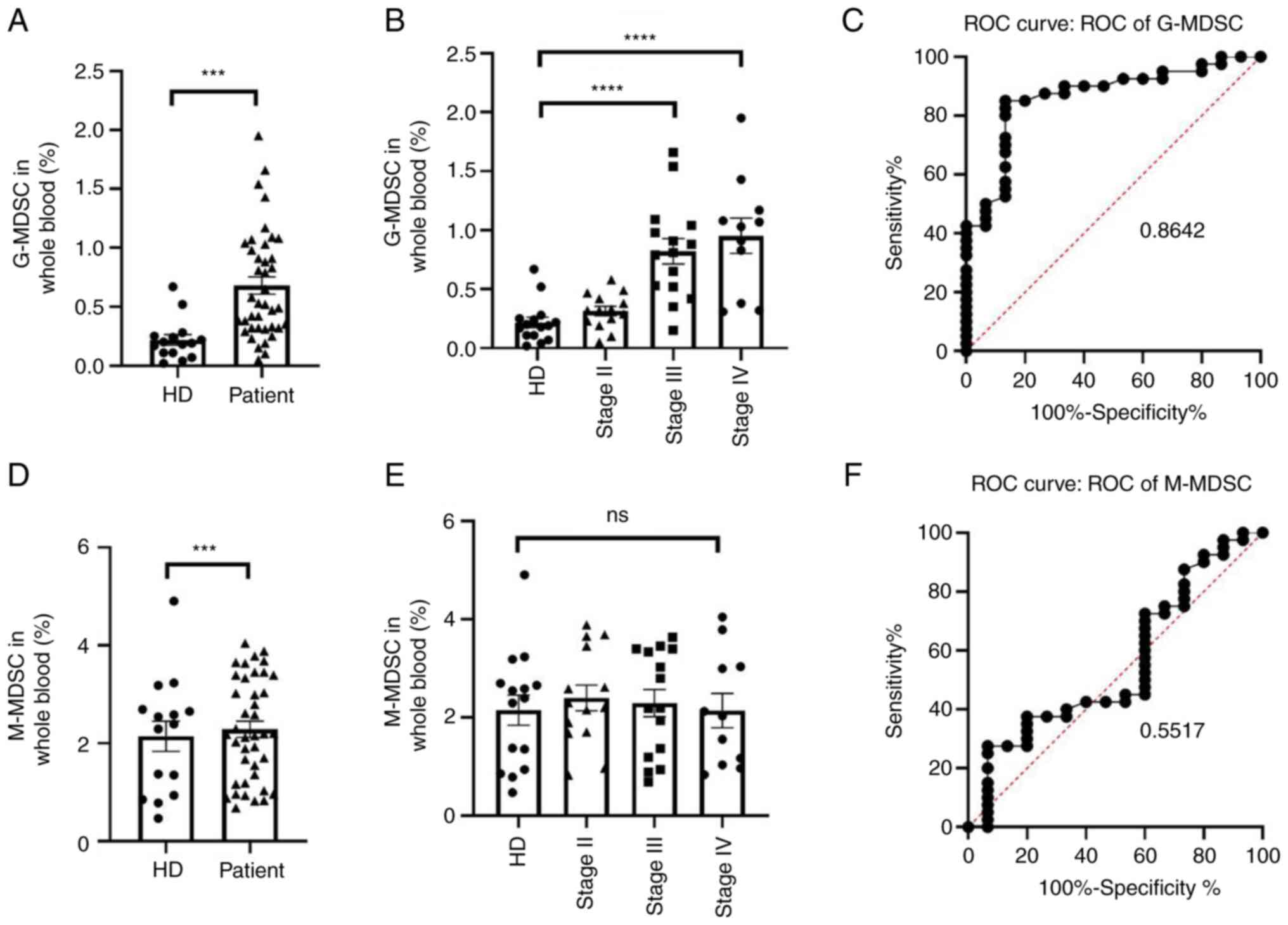
The frequency of G-MDSCs increased in
the blood of patients with stage III and IV
A significantly higher level of circulating G-MDSCs
was observed in patients with LDH that in controls (mean 0.6805 vs.
0.2180%, P=0.0004) (Fig. 4A). When
patients were further divided by the Pfirrmann stage, a direct
correlation between the LDH stage and percentage of circulating
G-MDSCs was noted (Spearman's r=0.718, P<0.001). There
was a significant difference in the level of G-MDSCs between
patients with stage IV LDH and controls (P<0.0001), as well as
stage III and controls (P<0.0001) but there was no
significant difference between stage II and controls (P=0.1156)
(Figs. 4B and 5). The receiver operating characteristic
(ROC) curve (area=0.8642, P<0.0001) also suggested that G-MDSCs
had clinical diagnostic potential (Fig. 4C).
No difference in the frequency of
circulating M-MDSCs between patients and HD
The frequency of circulating M-MDSCs was not
significantly different between patients with IVDD and controls
(mean 2.147 vs. 2.286%, P=0.6755) (Fig. 4D). The level of M-MDSCs appeared to
increase but was not significant between stage II and HD
(P=0.5468), between stages III and IV (P=0.7347), and between stage
III and controls (P=0.7326) (Fig.
4E). The ROC curve (area=0.5517, P=0.5580) of M-MDSCs
did not show clinical diagnostic potential (Fig. 4F).
For immature MDSCs, the analysis showed that these
HLA-DR- Lin- CD33+ cells in
peripheral blood samples almost all expressed CD15+.
Therefore, in the peripheral blood of patients with LDH, the
phenotype of immature MDSCs was virtually non-existent.
Discussion
Due to the acceleration of population aging, IVDD
will become a topic of interest in the future. LDH mainly manifests
as LBP and nerve root pain, which is related to the rupture of AF,
NP, and nerve fiber stimulation, affecting ~9% of the global
population (11). Intervertebral
disc degeneration is a complex pathological phenomenon caused by
heredity, aging, malnutrition, loading history and autoimmunity,
but the mechanism has not yet been clarified (17,18).
Gertzbein et al (19)
identified a potential role for autoimmunity in IVDD, pointing to
components such as proteoglycans in the NP as a major cause of
chronic inflammatory responses. Bobechko et al's (20) research also supported the role of
autoimmunity in IVDD by implanting autologous NP into the ears of
rabbits, resulting in local lymphadenopathy, which is proved that
NP has a self-antigen function. Starkweather et al (21) demonstrated that herniated NP tissue
or disc fragments in the epidural space activated the neuroimmune
system, inducing the release of a high number of inflammatory
cells, including macrophages, T cells, and a few monocytes from the
degenerating disc (22). Wang
et al (23) also discovered
that when the human immune system is exposed to intervertebral disc
tissue, macrophage infiltration and the release of IL-6,
interleukin 1β (IL-1β), and TNF are related to the subsequent
autoimmune response. In addition, monocyte chemoattractant protein
1 (MCP-1) released from the intervertebral disc is able to amplify
macrophage infiltration and inflammatory responses, which indicates
that the immune response is involved in the pathogenesis of IVDD
(24).
Although some patients can be relieved by
conservative treatment, persistent and severe pain often
necessitates surgery. The first case of spontaneous resorption of
the lumbar IVD in myelography was demonstrated in 1945 by Key et
al (25). Since then,
increasing reports have confirmed that LDH may spontaneously
disappear with time without surgery (26,27),
which should be considered by patients who choose not to have
surgery. The mechanism of phagocytosis is also the most supported
by clinical research. Previous studies also showed that
neovascularization and macrophage infiltration were required for
spontaneous absorption of herniated discs (28,29).
Takada et al (30) observed
that mechanical hyperalgesia in a rat intervertebral disc model was
substantially correlated with macrophage infiltration and the
up-regulation of TNF-α, IL-6, IL-8, and COX-2. Arai et al
(31) proposed that the
spontaneous absorption of IVDs might be a consequence of the
phagocytic activity of T cells and macrophages. These studies show
that macrophages and T cells seem to play an important role in this
pathological process. Furthermore, the inflammatory signal from
macrophages as well as T cells can mature and activate MDSCs
(32). MDSCs in turn inhibit the T
cell cycle and immune checkpoints, down-regulate T cell receptors,
and recruit regulatory T cells. They also suppress the activity of
other immune cells through the production of ROS, RNS, degradation
of L-arginine, and the production of anti-inflammatory factors,
such as TGF-β and IL-10 (25,33).
These factors further hinder the reabsorption process.
In our study, we provided a new basis for the
conservative treatment of patients with LDH. We analyzed and
correlated the proportion of MDSCs in the peripheral blood of
patients to determine the MDSC subgroup distribution in the
different stages of LDH. We were unable to collect patients with
stage V, because the stage is so severe that it's rare. We showed
that the proportion of G-MDSCs increased with LDH progression, but
no correlation was found with early-stage II. This may be on the
one hand because stage II patients were hospitalized rarely, and we
did not collect enough samples; on the other hand, this likely
indicated that the proportion of G-MDSCs is not obvious during
early IVD injury. It may be that AF integrity is still retained
during this stage, and the effect of tearing is either non-existent
or negligible. This also confirms that the proportion of MDSCs
increases after trauma. For M-MDSCs, although their proportion of
it increased to a certain extent, it was not statistically
significant. Related researches have shown that extensive tissue
damage caused by trauma or surgery can lead to the release of bone
marrow-derived cells, including MDSCs (34). Interestingly, MDSCs could play a
repair role in the early stage of trauma and aggravate the disease
in the later stage of chronic inflammation (35). This suggests that MDSCs may play a
different role in the progression of the disease. However, trauma
can stimulate the expression of T-helper 2 (Th2)
lymphocytes. Th2 cytokines can boost the expression of
arginase-1 in MDSCs and lead to arginine deficiency, which further
inhibits the function of lymphocytes, such as T cells, macrophages,
and natural killer cells (36,37),
in turn hindering the progress of NP reabsorption. In this study,
the G-MDSCs obtained by our subtyping analysis were from phenotype
CD33+. A study by Fultang et al (38) showed that the CD33 humanized
monoclonal antibody gemtuzumab ozogamicin has made clinical
progress in human trials, which could be used to target and reduce
the inhibitory effect of MDSCs on cellular immunity. It may promote
NP reabsorption. Therefore, the use of this drug may aid in the
treatment of LDH in the future.
To avoid the partial loss of G-MDSCs in the PBMCs
during the Ficoll density gradient separation process and a
deviation in MDSC subgroup analysis (39), we lyzed red blood cells in the
whole blood to obtain and analyze the percentage of circulating
MDSCs in this study. In addition, we used the cocktail lineage
(CD3/CD19/CD56/CD14/CD20/CD16) to exclude the non-specific staining
of a large number of neutrophils in the whole blood. Negative
selection of CD16 antibody can filter mature neturophils out.
CD3/CD19/CD56 antibodies negatively select mature lymphocytes and
CD14 antibody negatively selects mononuclear cells. These technical
points make our research results more accurate. Furthermore, we
were not able to obtain many samples because we used strict
criteria to ensure that the patient only had LDH. Finally, it is
worth mentioning that because intervertebral disc degeneration is a
long-term and complex process, the current animal models of
intervertebral disc degeneration are mostly caused by mechanical
damage (40), and there is no
model that is very consistent with the upright characteristics of
the human spine, our research has not yet involved animal-level
verification. However, we believe that exciting models will be
developed in the near future.
In conclusion, the peripheral blood MDSC subset
changes significantly after lumbar disc degeneration, and our
findings provide new clinical evidence for the autoimmune and
inflammatory theory of disc degeneration. Our study shows that an
increasing proportion of circulating G-MDSCs is associated with
stage III or IV in patients with LDH. The detection of peripheral
blood MDSC subpopulation can be used as an auxiliary examination
project for lumbar disc degenerative diseases. This study has
several limitations that need to be emphasized, such as the limited
number of samples, the absence of authoritative animal model and
control tissue of normal IVD, and a lack of pathological
examination. There is also a lack of detailed research on MDSC
function, and further in-depth researches are needed. Lumbar disc
degeneration is a multi-factor co-operation, continuous progression
of chronic inflammatory process, and autoimmunity plays an
important role in its pathogenesis and symptom development. By
elucidating the mechanism of IVDD, the development of drugs for the
immune system may be a new idea for the treatment of low back pain.
New discoveries to further promote the autoimmune research on IVDD
will have great benefits to society.
Acknowledgements
Not applicable.
Funding
Funding: This work was supported by grants from the National
Natural Science Foundation of China (grant nos. 31701162,
8197102295 and U1732157).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Author's contributions
BS, WH and JD contributed to the conception, design
and interpretation of the study. HZ and CL performed the
experiments and wrote the manuscript. HZ, CS and FH were
responsible for the tissue preservation collection, statistical
analysis and bioinformatics analysis in preparation of figures and
tables. HZ and CL confirm the authenticity of all the raw data. All
the authors participated in revision of the manuscript. All authors
have read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by The Committee on
Medical Ethics of The First Affiliated Hospital of Anhui Medical
University and a waiver of informed consent was granted (approval
no. PJ 2022-02-16).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Katz JN: Lumbar disc disorders and
low-back pain: Socioeconomic factors and consequences. J Bone Joint
Surg Am. 88:21–24. 2006.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Wang P, Chen C, Zhang QH, Sun GD, Wang CA
and Li W: Retraction of lumbar disc herniation achieved by
noninvasive techniques: A case report. World J Clin Cases.
27:8082–8089. 2021.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Lakstins K, Arnold L, Gunsch G, Flanigan
D, Khan S, Gadde N, Jones B, Agarwal G and Purmessur D:
Characterization of the human intervertebral disc cartilage
endplate at the molecular, cell, and tissue levels. J Orthop Res.
9:1898–1907. 2021.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Roberts S, Evans H, Trivedi J and Menage
J: Histology and pathology of the human intervertebral disc. J Bone
Joint Surg Am. 88:10–14. 2006.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Tsuru M, Nagata K, Ueno T, Jimi A, Irie K,
Yamada A, Nishida T and Sata M: Electron microscopic observation of
established chondrocytes derived from human intervertebral disc
hernia (KTN-1) and role of macrophages in spontaneous regression of
degenerated tissues. Spine J. 1:422–431. 2001.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Gruber HE and Hanley EN Jr: Analysis of
aging and degeneration of the human intervertebral disc: Comparison
of surgical specimens with normal controls. Spine (Phila Pa 1976).
23:751–757. 1998.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Liu SR, Ren D, Wu HT, Yao SQ, Song ZH,
Geng LD and Wang PC: Reparative effects of chronic intermittent
hypobaric hypoxia pre treatment on intervertebral disc degeneration
in rats. Mol Med Rep. 5(173)2022.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Tapia-Pérez H: Intervertebral disc
pathologies from an immunological perspective. Rev Neurol.
46:751–757. 2008.PubMed/NCBI(In Spanish).
|
|
9
|
Varikuti S, Singh B, Volpedo G, Ahirwar
DK, Jha BK, Saljoughian N, Viana AG, Verma C, Hamza O, Halsey G, et
al: Ibrutinib treatment inhibits breast cancer progression and
metastasis by inducing conversion of myeloid-derived suppressor
cells to dendritic cells. Br J Cancer. 7:1005–1013. 2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Rade M, Määttä JH, Freidin MB, Airaksinen
O, Karppinen J and Williams FMK: Vertebral endplate defect as
initiating factor in intervertebral disc degeneration: Strong
association between endplate defect and disc degeneration in the
general population. Spine (Phila Pa 1976). 43:412–419.
2018.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Hoy D, March L, Brooks P, Blyth F, Woolf
A, Bain C, Williams G, Smith E, Vos T, Barendregt J, et al: The
global burden of low back pain: Estimates from the global burden of
disease 2010 study. Ann Rheum Dis. 73:968–974. 2014.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Di Mitri D, Toso A, Chen JJ, Sarti M,
Pinton S, Jost TR, D'Antuono R, Montani E, Garcia-Escudero R,
Guccini I, et al: Tumour-infiltrating Gr-1+ myeloid cells
antagonize senescence in cancer. Nature. 515:134–137.
2014.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Amodio G, Cichy J, Conde P, Matteoli G,
Moreau A, Ochando J, Oral BH, Pekarova M, Ryan EJ, Roth J, et al:
Role of myeloid regulatory cells (MRCs) in maintaining tissue
homeostasis and promoting tolerance in autoimmunity, inflammatory
disease and transplantation. Cancer Immunol Immunother. 68:661–672.
2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Cassetta L, Baekkevold ES, Brandau S,
Bujko A, Cassatella MA, Dorhoi A, Krieg C, Lin A, Loré K, Marini O,
et al: Deciphering myeloid-derived suppressor cells: Isolation and
markers in humans, mice and non-human primates. Cancer Immunol
Immunother. 68:687–697. 2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Kim JH, Park YS, Oh KJ and Choi HS:
Surgical treatment of severe osteoporosis including new concept of
advanced severe osteoporosis. Osteoporos Sarcopenia. 4:164–169.
2017.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Kettler A and Wilke HJ: Review of existing
grading systems for cervical or lumbar disc and facet joint
degeneration. Eur Spine J. 15:705–718. 2006.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Jin L, Balian G and Li XJ: Animal models
for disc degeneration-an update. Histol Histopathol. 33:543–554.
2018.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Jin X, Wang J and Ge L: Identification of
immune-related biomarkers for sciatica in peripheral blood. Front
Genet. 12(781945)2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Gertzbein SD, Tile M, Gross A and Falk R:
Autoimmunity in degenerative disc disease of the lumbar spine.
Orthop Clin North Am. 6:67–73. 1957.PubMed/NCBI
|
|
20
|
Bobechko WP and Hirsch C: Auto-immune
response to nucleus pulposus in the rabbit. J Bone Joint Surg Br.
47:574–580. 1965.PubMed/NCBI
|
|
21
|
Starkweather A, Witek-Janusek L and
Mathews HL: Neural-immune interactions: Implications for pain
management in patients with low-back pain and sciatica. Biol Res
Nurs. 6:196–206. 2005.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Risbud MV and Shapiro IM: Role of
cytokines in intervertebral disc degeneration: Pain and disc
content. Nat Rev Rheumatol. 1:44–56. 2014.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Wang L, He T, Liu J, Tai J, Wang B, Zhang
L and Quan Z: Revealing the immune infiltration landscape and
identifying diagnostic biomarkers for lumbar disc herniation. Front
Immunol. 12(666355)2021.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Miyagi M, Uchida K, Takano S, Nakawaki M,
Sekiguchi H, Nakazawa T, Imura T, Saito W, Shirasawa E, Kawakubo A,
et al: Role of CD14-positive cells in inflammatory cytokine and
pain-related molecule expression in human degenerated
intervertebral discs. J Orthop Res. 8:1755–1762. 2021.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Key JA: Intervertebral disk lesions are
the most common cause of low back pain with or without sciatica.
Ann Surg. 121:534–539. 1945.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Kaliya-Perumal AK and Yoong-Leong JO:
Spontaneous total resolution of severe lumbar disc herniation.
Chonnam Med J. 56:77–78. 2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Ma Z, Yu P, Jiang H, Li X, Qian X, Yu Z,
Zhu Y and Liu J: Conservative treatment for giant lumbar disc
herniation: Clinical study in 409 cases. Pain Physician.
5:E639–E648. 2021.PubMed/NCBI
|
|
28
|
Haro H, Kato T, Komori H, Osada M and
Shinomiya K: Vascular endothelial growth factor (VEGF)-induced
angiogenesis in herniated disc resorption. J Orthop Res. 3:409–415.
2002.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Haro H, Komori H, Kato T, Hara Y, Tagawa
M, Shinomiya K and Spengler DM: Experimental studies on the effects
of recombinant human matrix metalloproteinases on herniated disc
tissues-how to facilitate the natural resorption process of
herniated discs. J Orthop Res. 2:412–419. 2005.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Takada T, Nishida K, Maeno K, Kakutani K,
Yurube T, Doita M and Kurosaka M: Intervertebral disc and
macrophage interaction induces mechanical hyperalgesia and cytokine
production in a herniated disc model in rats. Arthritis Rheum.
8:2601–2610. 2012.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Arai Y, Yasuma T, Shitoto K, Yamauchi Y
and Suzuki F: Immunohistological study of intervertebral disc
herniation of lumbar spine. J Orthop Sci. 3:229–231.
2000.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Schrijver IT, Théroude C and Roger T:
Myeloid-derived suppressor cells in sepsis. Front Immunol.
10(327)2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Bryk JA, Popovic PJ, Zenati MZ, Munera V,
Pribis JP and Ochoa JB: Nature of myeloid cells expressing arginase
1 in peripheral blood after trauma. J Trauma. 68:843–852.
2010.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Sanchez-Pino MD, Dean MJ and Ochoa AC:
Myeloid-derived suppressor cells (MDSC): When good intentions go
awry. Cell Immunol. 362(104302)2021.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Schwacha MG, Scroggins SR, Montgomery RK,
Nicholson SE and Cap AP: Burn injury is associated with an
infiltration of the wound site with myeloid-derived suppressor
cells. Cell Immunol. 338:21–26. 2019.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Ochoa JB, Bernard AC, O'Brien WE, Griffen
MM, Maley ME, Rockich AK, Tsuei BJ, Boulanger BR, Kearney PA and
Morris SM Jr: Arginase I expression and activity in human
mononuclear cells after injury. Ann Surg. 233:393–399.
2001.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Li X, Liu J, Xing Z, Tang J, Sun H, Zhang
X, Lv S, Chen Z, Shi M, Chen M, et al: Polymorphonuclear
myeloid-derived suppressor cells link inflammation and damage
response after trauma. J Leukoc Biol. 6:1143–1161. 2021.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Fultang L, Panetti S, Ng M, Collins P,
Graef S, Rizkalla N, Booth S, Lenton R, Noyvert B, Shannon-Lowe C,
et al: MDSC targeting with Gemtuzumab ozogamicin restores T cell
immunity and immunotherapy against cancers. EBioMedicine.
47:235–246. 2019.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Grützner E, Stirner R, Arenz L,
Athanasoulia AP, Schrödl K, Berking C, Bogner JR and Draenert R:
Kinetics of human myeloid-derived suppressor cells after blood
draw. J Transl Med. 14(2)2016.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Zhu P, Kong F, Wu X, Dong Z, Du J, Mao Y,
Zhou H, Liu Y, Mao H, Gu Y, et al: A minimally invasive annulus
fibrosus needle puncture model of intervertebral disc degeneration
in rats. World Neurosurg. 169:e1–e8. 2023.PubMed/NCBI View Article : Google Scholar
|