Introduction
Primary cardiac tumors are uncommon, with a
prevalence ranging from 0.17-0.19% worldwide (1). Cardiac lipoma is a rare benign tumor
that accounts for 8.4% of worldwide primary cardiac tumors
(2). The symptoms of cardiac
lipomas are based on their locations in the heart, although most
cardiac lipomas are asymptomatic and detected incidentally
(3). Cardiac lipomas originate
from the subendocardium, subepicardium or myocardium, with
proportions of 50, 25 and 25%, respectively (4). Moreover, they always occur in the
right atrium and left ventricle (5). Studies have found that the clinical
presentation of cardiac lipoma varies, ranging from mild chest
discomfort to sudden death (6,7).
Thus, the diagnosis and early management of cardiac lipomas are
particularly important for improving the prognosis of patients.
Currently, non-invasive imaging approaches are
widely used to diagnose cardiac lipomas, including computed
tomography (CT), echocardiography, magnetic resonance imaging (MRI)
and CT angiography (CTA) (8).
Non-invasive imaging methods can also modify the treatment of
cardiac lipomas. However, the diagnosis and management of cardiac
lipomas are still in the exploratory stage in clinical practice,
lacking a unified standard. The current study describes a cardiac
lipoma that was present in the left ventricular intermuscular
region using non-invasive imaging methods. In the present case, the
cardiac lipoma was removed under general anesthesia intubation and
cryogenic cardiopulmonary bypass, and a mechanical mitral valve
replacement was performed.
Case report
A 22-year-old woman without history of pregnancy was
admitted to Suining Central Hospital (Suining, China) because of
left chest pain for >6 months, with further aggravation over 2
days. The patient presented with left chest pain without obvious
inducement, and the symptoms were alleviated by rest. The patient
did not have a history of headache, syncope, cyanosis, finger
clubbing or squatting phenomenon, and no paroxysmal dyspnea or
upright breathing occurred at night. The patient visited Suining
Central Hospital (Suining, China) for treatment because the left
chest pain worsened and continued without relief.
Physical examination after admission was as follows:
Body temperature, 36.3˚C; heart rate, 96 bpm; respiration, 20
breaths/min; blood pressure, 118/88 mmHg; height, 157 cm; body
weight, 80 kg; and oxygen saturation, 99%. The thorax was normal
with no tenderness in the sternum. Bilateral respiratory movement
was normal, and no widening of the intercostal space was
identified. In addition, bilateral tactile fremitus is normal, no
pleural friction sensation, clear percussion sound on both lungs,
clear breath sounds (bilateral), no dry or wet rales, and no
pleural friction sound. The shape of the breasts were normal and
there was no abnormal uplift of the anterior heart area or
enlargement of the heart boundary. The apical area was located in
the fifth intercostal area of the left midclavicular line. The
cardiac rhythm was consistent, and no pathological murmurs were
heard in the auscultation area of each valve.
Electrocardiography indicated sinus tachycardia, and
a chest CT scan showed a low-density shadow in the left ventricle
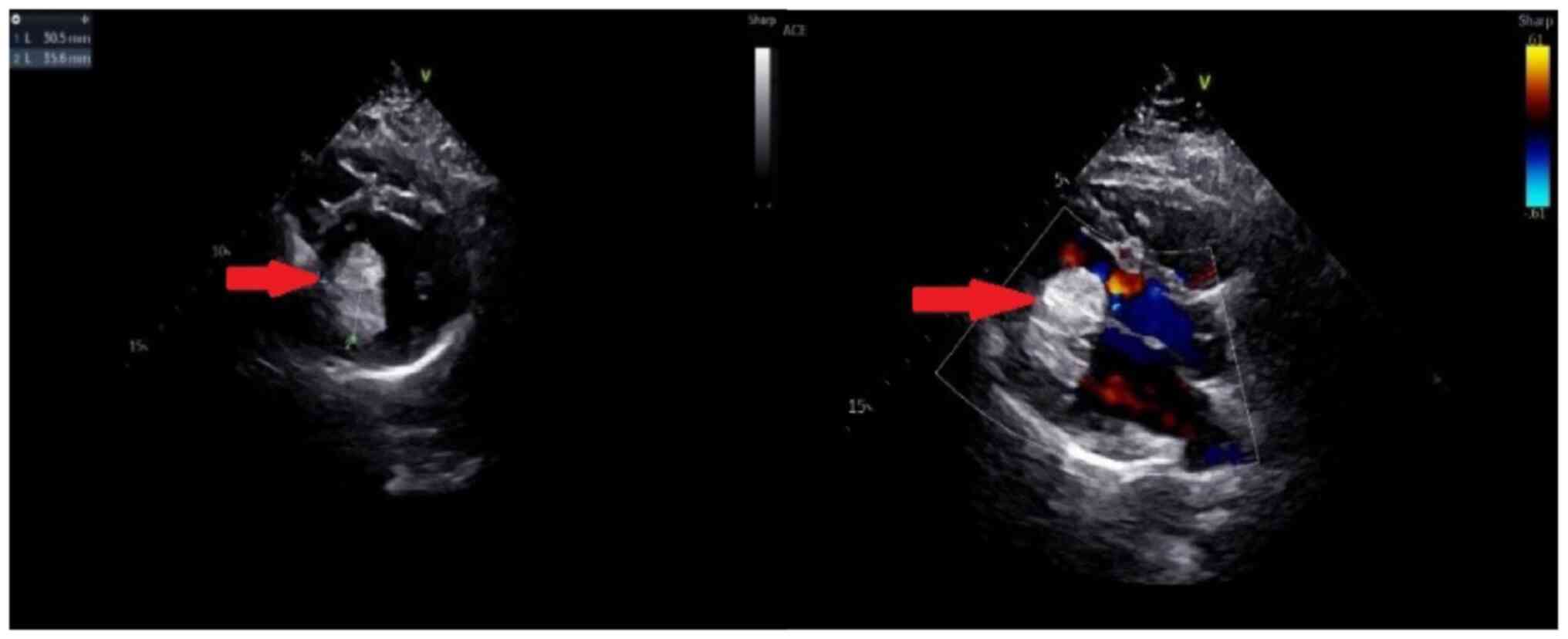
(Fig. 1). Echocardiography also
revealed a slightly stronger echo cluster in the left ventricle,
with a range of ~29x30x35 mm, which was closely related to the
lower wall and part of the posterior wall of the left ventricle
(Fig. 2). Moreover, the
preoperative ejection fraction was 60%, while the pulmonary valve
velocity was 106 cm/sec. Contrast-enhanced ultrasound (CEUS) showed
that the left ventricular mass was enhanced in a circular and
dot-line shape, with left ventricular solid occupation and rich
blood supply (Fig. 3). Moreover,
CTA showed a nodule of left ventricular lipid density that was
27x27x24 mm in size (Fig. 4).
Laboratory examination showed that the aspartate aminotransferase
level was 45.7 U/l, while myocardial enzyme profile (creatine
kinase-MB, 104.67 ng/ml; troponin I, 42433.7 pg/ml; myoglobin,
404.66 ng/ml), ESR (11 mm/h), humoral and cellular immunity
(rheumatoid factors, <20.0 IU/ml; immunoglobulin G, 9.43 g/l;
immunoglobulin A, 0.94 g/l; immunoglobulin M, 1.77 g/l; complement
C3, 1.3 g/l; complement C4, 0.27 g/l; C-reactive protein, 5.84
mg/l) were considered normal.
The heart mass was removed under general anesthesia,
intubation and cryogenic cardiopulmonary bypass after preoperative
preparation. An irregular grey and white mass was found in the left
ventricle during the operation with a size of 30x22x17 mm,
occupying ~1/3 of the space of the left ventricle. The anterior
chordinae tendinae surrounding the mitral valve and the papillary
muscle showed infiltrating growth. The tumor pedicle was wide and
attached to the posterior inferior wall of the left ventricle, and
both anterior and posterior mitral valves were normal. Considering
that the nature of the mass was unknown and that the left anterior
chordae tendinae and papillary muscle infiltrated and grew,
complete resection of the mass could not preserve the chordae
tendinae and papillary muscle. Thus, mechanical mitral valve
replacement was performed simultaneously. After transition to the
intensive care unit, the patient was transferred to the general
ward and received routine anticoagulant treatment. All risks
associated with mechanical valves, anticoagulation and pregnancy
were explained to the patient prior to the procedure. Postoperative
chest CT indicated that the mechanical valve was in place, and no
residual tumor was identified (Fig.
5). Histopathological examination of the excised mass revealed
intramuscular lipoma (Fig. 6).
After 6 months, symptoms such as chest tightness had disappeared,
blood coagulation function was normal and there was no evidence of
tumor recurrence in the ventricle.
Discussion
The present study reported the case of a patient
with invasive cardiac lipoma in the left ventricular intermuscular
region with their main symptoms including persistent left chest
pain and sudden aggravation. Cardiac lipoma was diagnosed using
non-invasive imaging techniques, including CT, echocardiography,
CEUS and CTA. The cardiac lipoma involved the left anterior chordae
tendinae and papillary muscle, and while the mass in the chordae
tendinae and papillary muscle was resected, a mechanical mitral
valve replacement was performed. The symptoms disappeared after the
procedure, and no residual tumor was observed in the heart. To the
best of our knowledge, the present study is the first to report
cardiac lipoma involving the left anterior chordae tendinae and
papillary muscle.
Cardiac lipomas at various locations have been
reported in numerous studies; their characteristics are presented
in Table I (2,4,9-39).
These studies include 16 male and 17 female patients, and they have
no obvious difference in sex. Moreover, the ages of the included
patients ranged from 0.1-77.0 years, while the majority of patients
(25/33) were aged ≥30.0 years. Most cardiac lipomas are
asymptomatic and have a good prognosis; however, some giant cardiac
lipomas can cause left ventricular inflow or outflow disturbances,
left ventricular dysfunction or conduction system invasion
(30,40). These conditions can induce dyspnea,
presyncope, syncope or palpitations (30,40);
however, the present study reported on a patient that presented
with no etiologic chest pain, which could be considered as cardiac
lipoma in clinical practice. Cardiac lipomas can be located in any
part of the heart and typically originate from the epicardial fat
or pericardial fat. They are surrounded by fibrous tissue and
contain a small amount of myocardial tissue, as well as components
of connective tissue (31).
Lipomas located in the myocardium are usually small with a complete
capsule, and occasionally grow on the mitral or tricuspid valve
(31). The most common location is
the atrial septum, followed by the endocardium of the right atrium
and left ventricle (41), while in
a few cases the lipomas are located in the myocardium,
subepicardium and pericardium (29). In the present study, an invasive
cardiac lipoma was observed in the left ventricular intermuscular
region.
 | Table ISummary results for patients with
cardiac lipoma. |
Table I
Summary results for patients with
cardiac lipoma.
| First author/s,
year | Age, years | Sex | Diagnostic tool | Tumor location | (Refs.) |
|---|
| Kamiya et al,
1990 | 45.0 | Male | Echocardiography, CT,
MRI, CTA | Interventricular
septum | (9) |
| Morikami et
al, 1994 | 38.0 | Male | Echocardiography,
CT, MRI | Inferior wall of
the left ventricle near the apex | (10) |
| Fukushima et
al, 1999 | 22.0 | Male | Echocardiography,
MRI | Left ventricle
beneath the mitral valve | (11) |
| Schrepfer et
al, 2003 | 31.0 | Female | Echocardiography,
CT, MRI, CTA | Right
ventricular | (12) |
| Agacdiken et
al, 2005 | 18.0 | Female | Chest X-ray,
echocardiography, CT, MRI | Interventricular
septum | (13) |
| Friedberg et
al, 2006 | 13.0 | Male | Chest X-ray,
echocardiography, MRI | Lateral mitral
annulus | (14) |
| Ozaki et al,
2006 | 74.0 | Female | Chest X-ray,
echocardiography, CT, MRI | Interventricular
septum | (15) |
| Arslan et
al, 2007 | 45.0 | Male | Echocardiography,
CT | Interventricular
septum | (16) |
| Ganame et
al, 2008 | 62.0 | Male | Echocardiography,
MRI | Endocardial surface
of the mid-anterior septum | (17) |
| Hayashi et
al, 2008 | 55.0 | Male | Echocardiography,
CT | Left ventricular
myocardium | (18) |
| Gan et al,
2008 | 0.1 | Male | Echocardiography,
CT | Right atrium | (19) |
| Kawarai et
al, 2010 | 57.0 | Male | Echocardiography,
CT, MRI | Left
ventricular | (20) |
| Song et al,
2010 | 56.0 | Female | Chest X-ray,
echocardiography, CT, CTA | Aneurysmal right
ventricle | (21) |
| Domoto et
al, 2010 | 70.0 | Male | Echocardiography,
CT, MRI | Left ventricular
apex | (22) |
| Frank et al,
2012 | 36.0 | Female |
Echocardiography | Anterior wall | (23) |
| Schiettecatte et
al, 2012 | 68.0 | Female | Echocardiography,
MRI | Intracardiac | (24) |
| Singh et al,
2013 | 26.0 | Female | Echocardiography,
MRI | Mimicking atrial
myxoma | (25) |
| Tanaka et
al, 2015 | 77.0 | Female | Echocardiography,
CT, MRI | Left ventricular
apex | (26) |
| Li et al,
2015 | 65.0 | Male | Echocardiography,
CT, MRI | Interventricular
septum | (2) |
| Shenthar et
al, 2015 | 25.0 | Male | Echocardiography,
CT, MRI | Right
ventricle | (27) |
| Zhang et al,
2016 | 49.0 | Female | Echocardiography,
MRI | Right
ventricular | (28) |
| Fang et al,
2016 | 48.0 | Female | Echocardiography,
MRI | Right
ventricle | (29) |
| D'Souza et
al, 2017 | 33.0 | Male | Echocardiography,
MRI | Right atrium | (4) |
| Sun et al,
2018 | 70.0 | Female | Echocardiography,
MRI | Left
ventricular | (30) |
| Karangelis et
al, 2019 | 72.0 | Female | Echocardiography,
MRI | Right
ventricle | (31) |
| Shamsi et
al, 2020 | 57.0 | Male | Echocardiography,
MRI | Left
ventricular | (32) |
| Elenizi et
al, 2020 | 17.0 | Female | Echocardiography,
CT, MRI | Right
ventricular | (33) |
| Abdelradi et
al, 2020 | 51.0 | Male | Echocardiography,
CT, MRI | Left
ventricular | (34) |
| Bai et al,
2021 | 25.0 | Female | Echocardiography,
CT, MRI | Right atrium | (35) |
| Younes et
al, 2021 | 49.0 | Female | Echocardiography,
MRI | Left
ventricular | (36) |
| Nepal et al,
2022 | 50.0 | Female | Echocardiography,
CT, MRI | Interventricular
septum | (37) |
| Watanabe et
al, 2022 | 51.0 | Female | Echocardiography,
CT, MRI | Posterior surface
of the heart | (38) |
| Bajdechi et
al, 2022 | 30.0 | Male | Echocardiography,
MRI | Right atrium | (39) |
Echocardiography is the initial choice for the
diagnosis of cardiac lipomas, but it cannot detect smaller tumors
(30). Moreover, echocardiography
cannot provide clear information regarding lipomas and other
primary cardiac tumors (42).
Thus, CT and MRI should be performed to provide useful information
on tissue characteristics and the degree of myocardial infiltration
(30,41). Especially for MRI, which is
considered to be the most accurate diagnostic tool owing to their
distinctive fatty characteristics, they can be easily identified as
masses (41). A previous study has
demonstrated that lipomas show up clearly in T1- and T2-weighted
images, accompanied with complete suppression on fat-saturated
sequences (43). In the present
study, the patient had repeated chest tightness, chest pain and
discomfort, accompanied by palpitations, which might be related to
outflow tract obstruction caused by a left ventricular tumor or
paroxysmal ventricular tachycardia caused by conduction tissue
compression; this was not discovered until B-mode ultrasound was
performed. Furthermore, CT indicated the presence of dense lipid
nodules, which supported evidence of a lipoma, further suggesting
that CT imaging can be used to differentiate the properties of a
tumor.
Considering that sudden death risk has already been
reported in patients with cardiac lipomas, surgical resection
should be performed irrespective of the symptoms of cardiac lipomas
(44). The surgical method of
cardiac lipoma resection is usually performed through a median
sternum incision under complete cardiopulmonary bypass (44). Cardiac lipomas are always
encapsulated, rarely invade the heart muscles and are easy to
remove (44). Additionally, early
surgical resection of small lipomas can preserve heart function
(44); however, conduction
dysfunction caused by lipoma invasion of the heart muscle can lead
to arrhythmias, which is the most common complication after
surgical removal of cardiac tumors (45). In the present case, the lipoma
infiltrated the anterior chordae tendinae surrounding the mitral
valve and papillary muscle, and the scope of infiltration growth
was small. Heart integrity might not be affected after complete
resection of the tumor (44);
thus, complete resection was selected to prevent postoperative
recurrence risk. Simultaneous mitral valve replacement may be a
viable surgical option for patients with complete resection of the
mass and no retention of the chordae tendinae or papillary
muscle.
Left ventricular infiltrating lipoma is a rare
disease; however, owing to the size and location of the tumor,
corresponding obstruction symptoms or conduction disorders caused
by invasion of the myocardium may lead to arrhythmias (7). Furthermore, the myocardial tissue in
the corresponding section becomes thinner. Therefore, in
asymptomatic young patients presenting with the aforementioned
electrocardiographic manifestations, echocardiography should be
performed to avoid misdiagnosis. Surgical treatment is the
preferred treatment for cardiac lipoma, and complete resection is
still a viable treatment option when the lesion scope is small for
invasive lipomas. If the lesion involves the valve, chordae
tendinae, papillary muscle or other tissues, heart valve
replacement should be performed.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JX, JPL, WH, JG, YHZ, LC and XZZ performed
acquisition of data, analysis and interpretation of data, drafting
the article and final approval. XHC and QZ performed conception and
design of the study, critical revision and final approval. YHZ and
QZ confirm the authenticity of all the raw data. All authors read
and approved the final version of the manuscript.
Ethics approval and consent to
participate
The protocol, design and study performed were
approved by The Ethics Committee of Suining Central Hospital
(Suining, China; approval no. LLSLH20220124) in accordance with the
Declaration of Helsinki. All treatment in this case followed normal
protocols of Suining Central Hospital.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of this study.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Wu S, Teng P, Zhou Y and Ni Y: A rare case
report of giant epicardial lipoma compressing the right atrium with
septal enhancement. J Cardiothoracic Surg. 10(150)2015.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Li D, Wang W, Zhu Z, Wang Y, Xu R and Liu
K: Cardiac lipoma in the interventricular septum: A case report. J
Cardiothoracic Surg. 10(69)2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
McAllister HAJ, Fenoglio JJJ and Fine G:
Tumors of the cardiovascular system. (Atlas of tumor pathology,
second series, Fascicle 15.) New York: Armed Force Institute of
Pathology, pp44-46, 1978.
|
|
4
|
D'Souza J, Shah R, Abbass A, Burt JR, Goud
A and Dahagam C: Invasive cardiac lipoma: A case report and review
of literature. BMC Cardiovasc Disord. 17(28)2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Ismail I, Al-Khafaji K, Mutyala M,
Aggarwal S, Cotter W, Hakim H, Khosla S and Arora R: Cardiac
lipoma. J Community Hosp Intern Med Perspect.
5(28449)2015.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Puvaneswary M, Edwards JR, Bastian BC and
Khatri SK: Pericardial lipoma: Ultrasound, computed tomography and
magnetic resonance imaging findings. Australas Radiol. 44:321–324.
2000.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Li J, Ho SY, Becker AE and Jones H:
Multiple cardiac lipomas and sudden death: A case report and
literature review. Cardiovasc Pathol. 7:51–55. 1998.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Monti L, Scardino C, Nardi B and Balzarini
L: Lipoma of the interventricular septum. Eur Heart J.
36(3073)2015.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Kamiya H, Ohno M, Iwata H, Ohsugi S,
Sawada K, Koike A, Ogawa K, Yano Y, Hayase S and Horiba M: Cardiac
lipoma in the interventricular septum: Evaluation by computed
tomography and magnetic resonance imaging. Am Heart J.
119:1215–1217. 1990.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Morikami Y, Higashi T, Isomura T, Hirano
A, Tanaka K, Hisatomi K and Ohishi K: Cardiac lipoma with changes
of ST segment and T wave on electrocardiogram. Jpn Circ J.
58:733–736. 1994.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Fukushima KK, Mitani T, Hashimoto K,
Hosogi S, Emori T, Morita H, Fujimoto Y, Nakamura K, Yamanari H and
Ohe T: Ventricular tachycardia in a patient with cardiac lipoma. J
Cardiovasc Electrophysiol. 10(1161)1999.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Schrepfer S, Deuse T, Detter C, Treede H,
Koops A, Boehm DH, Willems S, Lacour-Gayet F and Reichenspurner H:
Successful resection of a symptomatic right ventricular lipoma. Ann
Thorac Surg. 76:1305–1307. 2003.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Agacdiken A, Gurbuz Y, Ciftci E, Omay O,
Vural A and Ural D: Cardiac lipoma in a patient with proven
arrhythmogenic right ventricular dysplasia: A case report. A huge
intramyocardial lipoma. Int J Cardiovasc Imaging. 21:463–467.
2005.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Friedberg MK, Chang IL, Silverman NH,
Ramamoorthy C and Chan FP: Images in cardiovascular medicine. Near
sudden death from cardiac lipoma in an adolescent. Circulation.
113:e778–e779. 2006.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Ozaki N, Mukohara N, Yoshida M and Shida
T: Cardiac lipoma in the ventricular septum-a case report. Thorac
Cardiovasc Surg. 54:356–357. 2006.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Arslan S, Gundogdu F, Acikel M and
Kantarci AM: Asymptomatic cardiac lipoma originating from the
interventricular septum diagnosed by multi-slice computed
tomography. Int J Cardiovasc Imaging. 23:277–279. 2007.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Ganame J, Wright J and Bogaert J: Cardiac
lipoma diagnosed by cardiac magnetic resonance imaging. Eur Heart
J. 29(697)2008.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Hayashi H, Hidaka F, Kiriyama T, Sato H,
Takagi R and Kumita S: A left ventricular lipoma diagnosed on
three-dimensional electrocardiogram-gated cardiac computed
tomography. Heart Vessels. 23:366–369. 2008.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Gan C, An Q, Tao K, Tang H and Li W: An
asymptomatic lipoma of the right atrium in a neonate. J Pediatr
Surg. 43:1920–1922. 2008.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kawarai S, Yaginuma GY, Abe K, Hamasaki A,
Ishikawa K and Tanaka D: Left ventricular lipoma with
pseudoaneurysm-like appearance. Gen Thorac Cardiovasc Surg.
58:279–282. 2010.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Song Y, Hickey W, Nabi F and Chang SM:
Extensive cardiac lipoma with aneurysmal right ventricle. Interact
Cardiovasc Thorac Surg. 11:691–692. 2010.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Domoto S, Nakano K, Kodera K, Sasaki A,
Asano R, Ikeda M and Kataoka G: Cardiac lipoma originating from the
left ventricular apex diagnosed using the magnetic resonance
imaging fat suppression technique: Report of a case. Surg Today.
40:871–873. 2010.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Frank S, Pochmalicki G, Achor A, Debauchez
M and Ha DE: Successful resection of an intra-cardiac lipoma during
the first trimester of pregnancy, coming to term normally. Eur J
Obstet Gynecol Reprod Biol. 160:236–237. 2012.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Schiettecatte A, Verdries D, de Mey J, De
Maeseneer M and Dujardin M: Magnetic resonance imaging findings in
cardiac lipoma. JBR-BTR. 95:300–301. 2012.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Singh B, Bhairappa S, Shankar SK, Prasad
NM and Manjunath CN: Cardiac lipoma at unusual location-mimicking
atrial myxoma. Echocardiography. 30:E72–E74. 2013.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Tanaka Y, Yoshimuta T, Yamagishi M and
Sakata K: Video-assisted transmitral resection of primary cardiac
lipoma originated from the left ventricular apex. Eur Heart J
Cardiovasc Imaging. 16(401)2015.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Shenthar J, Sharma R, Rai MK and Simha P:
Infiltrating cardiac lipoma presenting as ventricular tachycardia
in a young adult. Indian Heart J. 67:359–361. 2015.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Zhang HW, Zhong MH, Meng W, Zhang EY, Gu J
and Hu J: Intramuscular lipoma as an unusual cause of right
ventricular outflow tract obstruction. Echocardiography.
33:328–329. 2016.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Fang L, He L, Chen Y, Xie M and Wang J:
Infiltrating lipoma of the right ventricle involving the
interventricular septum and tricuspid valve: Report of a rare case
and literature review. Medicine (Baltimore).
95(e2561)2016.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Sun X, Liu G, Kim H and Sun W: Left
ventricular lipoma resected using thoracoscope-assisted limited
sternotomy: A case report and literature review. Medicine
(Baltimore). 97(e11436)2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Karangelis D, Palios J, Tzertzemelis D,
Economidou S and Panagiotou M: Surgical resection of a cardiac
lipoma of the right ventricle. Ann Card Anaesth. 22:452–454.
2019.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Shamsi F, Bajwa G and Ghalib H: ‘Left
ventricular lipoma….. a rare case’, case report. J Cardiothorac
Surg. 15(85)2020.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Elenizi K, Matta A, Alharthi R,
Campelo-Parada F, Lhermusier T, Bouisset F, Elbaz M, Carrié D and
Roncalli J: Incidental discovery of right ventricular lipoma in a
young female associated with ventricular hyperexcitability: An
imaging multimodality approach. World J Cardiol. 12:220–227.
2020.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Abdelradi A and Yekta A: A case of
asymptomatic cardiac lipoma and literature review. CJC Open.
3:207–209. 2020.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Bai R, Zhang Y, Wang H, Yang J and Sun D:
Invasive cardiac lipoma diagnosis based on echocardiography: Case
report and literature review. J Clin Ultrasound. 49:408–412.
2021.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Younes A, Ahmad S, Yousaf A and Marcu CB:
A rare presentation of cardiac lipoma as an acute coronary
syndrome: A case report and review of literature. Cureus.
13(e15503)2021.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Nepal S, Deshmane SB, Donovan K, May A and
Chaudhuri D: Invasive lipoma of the interventricular septum, a rare
benign cardiac mass with atypical presentation and management. J
Investig Med High Impact Case Rep.
10(23247096221104469)2022.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Watanabe S, Ichihara Y, Morita K, Saito S
and Niinami H: Successful removal of a posterior cardiac lipoma by
transection of the ascending aorta and main pulmonary artery. Case
Rep Cardiol. 2022(3813369)2022.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Bajdechi M, Onciul S, Costache V, Brici S
and Gurghean A: Right atrial lipoma: A case report and literature
review. Exp Ther Med. 24(697)2022.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Lin HD, Hsu PF, Wu MH, Leu HB and Hsu TL:
Images in cardiology: Subaortic stenosis caused by left ventricular
outflow tract lipoma. Clin Cardiol. 29(421)2006.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Rocha RV, Butany J and Cusimano RJ:
Adipose tumors of the heart. J Card Surg. 33:432–437.
2018.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Barbuto L, Ponsiglione A, Del Vecchio W,
Altiero M, Rossi G, De Rosa D, Pisani A and Imbriaco M: Humongous
right atrial lipoma: A correlative CT and MR case report. Quant
Imaging Med Surg. 5:774–777. 2015.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Hoey ET, Mankad K, Puppala S, Gopalan D
and Sivananthan MU: MRI and CT appearances of cardiac tumours in
adults. Clin Radiol. 64:1214–1230. 2009.PubMed/NCBI View Article : Google Scholar
|
|
44
|
D'Errico S, Mazzanti A, Frati P and
Fineschi V: Conduction disorder and primary cardiac tumor: A fatal
case of multiple lipomas of the right atrium. J Geriatr Cardiol.
16:431–433. 2019.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Li S and Gao C: Surgical experience of
primary cardiac tumor: Single-institution 23-year report. Med Sci
Monit. 23:2111–2117. 2017.PubMed/NCBI View Article : Google Scholar
|