Introduction
Exposure to high altitude or normobaric hypoxia is a
characteristic reason behind pulmonary vasoconstriction and
pulmonary hypertension (1-6).
Initially, pulmonary vasoconstriction is a physiological adaptation
to maintain the ventilation/perfusion ratio as a response to
hypoxia. This leads to a decline in arterial oxygen saturation
(SaO2), causing pulmonary vasoconstriction and enhanced
pulmonary artery systolic pressure (PASP). This can be observed
after exposure to hypoxia for only 2 h (7), despite being more pronounced for
several days or weeks (5). One of
the response mechanisms is the reduction of nitric oxide (NO)
production in pulmonary artery smooth muscle cells (8). cGMP is a potent vasodilator
synthesized by NO-activated soluble guanylate cyclase.
Sildenafil, a phosphodiesterase type-5 (PDE-5)
inhibitor, induces vasodilation by inhibiting the hydrolytic
breakdown of cGMP (9) with
approved indications as pulmonary arterial hypertension treatment
(10). Indeed, a recent
meta-analysis revealed that PDE-5 inhibitors effectively attenuated
high-altitude pulmonary hypertension (11).
Studies have been conducted on the clinical efficacy
of Sildenafil during altitude-induced hypoxemia (2,12,13).
Short-term Sildenafil treatment can attenuate the altitude-induced
high pulmonary systolic arterial pressure without significant
beneficial effects on arterial oxygen saturation, heart rate and
acute mountain sickness (14).
However, there are conflicting views (2,15,16).
Several meta-analyses have assessed the efficacy of Sildenafil in
treating high altitude-induced hypoxia (11,14).
However, the effects of Sildenafil on hypoxia have been
inconsistent during rest and exercise. Some studies of Sildenafil
on endurance performance in hypoxia show beneficial effects
(2,3), while others show no significant
effect (17). The degree and
duration of hypoxia affect associated parameters, such as pulmonary
artery pressure (PAP), SaO2 and arterial oxygen content
(CaO2) (18-20).
Whether different altitudes influence the outcomes significantly
remains to be elucidated. The efficacy of Sildenafil may be
different at varying altitudes for most of the population (16). Therefore, the present study aimed
to review systematically the efficacy of Sildenafil on
hypoxia-related parameters and endurance performance in healthy
humans based on the exercise state and different altitudes using
meta-analysis.
Materials and methods
Inclusion Criteria
Eligible articles were independently identified with
the following inclusion criteria: i) The target population was
healthy unacclimatized lowlanders; ii) studies were randomized
controlled trials (RCT) in which the experimental group was treated
with Sildenafil and the control group was given a placebo or other
drugs; iii) hypoxia was induced in either simulated high altitude
or natural high altitude environments; iv) the principal evaluation
indicator included at least one parameter of echocardiography or
hemodynamics. The exclusion criteria were: i) Subjects with
pre-existing high-altitude cerebral edema and/or high-altitude
pulmonary edema; ii) Studies related to Sildenafil usage combined
with the treatment; and iii) incomplete, unavailable or
inaccessible data.
Literature search
A systematic search for clinical trials of sildenafil
was performed using the PubMed (https://pubmed.ncbi.nlm.nih.gov/), Embase (https://www.embase.com) and Cochrane (https://www.cochrane.org/) to databases. The following
terms: ‘Sildenafil OR Sildenafil citrate OR phosphodi-esterase type
5 inhibitor OR PDE-5 inhibitor’ AND ‘high altitude OR hypoxia OR
plateau’ with applicable filter limit to ‘randomized controlled
clinical trials (RCTs)’ were searched. The period of searching the
online databases was between 1998 and Dec 2022.
Quality assessment
The selected studies were assessed for quality by
estimating the risk of bias, using the Cochrane risk of bias
assessment tool (21), which tests
for randomization, blinding, reporting of withdrawal, generation of
random numbers and allocation concealment.
Data extraction
The data was extracted from the studies included in
the review by two reviewers independently. The following
information was collected: Year of publication, number of included
participants, demographic characteristics, the duration of
follow-up, the altitude or simulated altitude and dose of
Sildenafil.
Statistical analysis
Data were analyzed using RevMan 5.4 (The Cochrane
Collaboration) and Stata15 software (version 15.0; Stata Corp LP).
Variability between studies in a systematic review may be termed
heterogeneity, commonly evaluated using a chi-squared test
(χ2) in which an I2 statistic >50% or
P<0.10 are considered indicators (22). A fixed effects model helped analyze
the data where no significant heterogeneity was observed between
studies (P>0.10; I2≤50%). Conversely, a random
effects model was used where heterogeneity was identified. Standard
deviation is calculated by the simple formula: SD=SEx√sample size
(23). Means and standard variance
from the median were derived using range and sample size (24). For graphical data, the authors were
contacted for statistical values. If the authors did not respond,
the data were estimated from the graphs.
Results
Study characteristics
A total of 2,998 articles were identified using the
pre-defined search strategy. Among these studies, 37 satisfied the
primary inclusion criteria after reading titles and abstracts.
After carefully reading the full text, 20 studies were excluded due
to pharmacokinetics trials in healthy volunteers (n=6),
non-randomized controlled studies (n=14) and pulmonary arterial
hypertension (n=1). One randomized controlled trial (RCT) was
reported twice (13,25) and the data were extracted from a
study by Snyder et al (25). Eventually, 16 RCTs were included in
the current meta-analysis (Fig.
1).
The key characteristics of the 16 trials are
demonstrated in Table I. A total
of 314 healthy volunteers were enrolled in the 16 RCTs, of which
150 were in the Sildenafil treatment group and 164 in the placebo
group. A total of six studies evaluated participants at a naturally
high altitude, and 10 studies investigated hypoxia by the
simulation of high altitude in laboratory conditions. The
participants in the study performed by Lalande et al
(26) were randomly receiving
Sildenafil and acetazolamide or a placebo. The data was extracted
from Sildenafil and placebo groups. The participants in the study
performed by Olfert et al (27) randomly received Sildenafil or
bosentan group. Thus, data was extracted from the bosentan group as
the control group.
 | Table IStudy characteristics. |
Table I
Study characteristics.
| First author,
year | N | M/F | Median age | Median weight,
kg | Altitude or
simulated altitude | Sildenafil dose,
mg | (Ref.) |
|---|
| Ghofrani et
al, 2004 | 14 | 12/2 | 36.5 | 72.3 | Mount Everest
(altitude: 5,245 m) | 50 | (2) |
| Ricart et
al, 2005 | 14 | 14/0 | 33.1±7.2 | 76.3±7.2 | Hypobaric chamber:
PB=405 mmHg, PO2=85 mmHg, (simulated
altitude: 5,000 m) | 100 | (4) |
| Richalet et
al, 2004 | 12 | 12/0 | 29±6 | 79±11 | Observatoire Vallot
Altitude (altitude: 4.350 m) | 40 | (5) |
| Hsu et al,
2006 | 10 | 10/0 | 31±4 | 76.83±9.5 | Breathing hypoxic
gas (12.8% oxygen simulated altitude: 3,874 m) | 50, 100 | (3) |
| Faoro et al,
2007 | 14 | 8/6 | 36 | 67±10 | Mount Chimborazo
(altitude: 5,000 m) | 50 | (17) |
| Reichenberger et
al, 2007 | 14 | 12/12 | 37 | - | Inspiration of gas
containing 10% O2 (simulated altitude: 4,500 m);
Himalaya region (altitude: 3,440 m) Mount Everest (altitude: 5,245
m) | 50 | (20) |
| Snyder et
al, 2008 | 14 | 13 | 33±11 | 85±14 | Low-oxygen tent,
12.5% O2 (simulated altitude: 4,300 m) | 100 | (25) |
| Lalande et
al, 2009 | 15 | 7/8 | 34.8±2.4 | 73.8±3.7 | Low-oxygen tent,
12.5% O2 (simulated altitude: 4,300 m) | 40 | (26) |
| Rodway et
al, 2016 | 12 | 8/4 | 66.5 | 67.2 | Hypobaric chamber
(simulated altitude: 2,750 m) | 50 | (41) |
| Bates et al,
2011 | 62 | 36/26 | 21 | SI: 65.1±7.5 pla:
69.5±11.8 | Chacaltaya
laboratory (altitude: 5,200 m) | 50 | (42) |
| Zhao et al,
2001 | 10 | 10/0 | - | - | Breathing 11%
O2 (simulated altitude: 5,350 m) | 100 | (15) |
| Cornolo et
al, 2004 | 12 | 12/0 | 29±6 | 79±11 | Observatoire Vallot
Altitude in France (altitude: 4,350 m) | 40 | (30) |
| Toro-Salinas et
al, 2016 | 11 | 6/5 | 26.8±4.2 | 66±7.3 | Hypobaric chamber
(simulated altitude: 4,000 m) | 100 | (28) |
| Olfert et
al, 2011 | 16 | 8/8 | SI: 25±3 BS:
28±7 | 175±7 | Hypoxic chamber,
11% O2 (simulated altitude: 5,350 m) | 50 | (27) |
| Kressler et
al, 2011 | 21 | 11/10 | M: 25±2 F:
27±2 | M: 72.1±1.2 F:
60.8±2.1 | Breathed hypoxic
gas (12.8% FiO2; simulated altitude: 3,900 m) | 50 | (16) |
| Jacobs et
al, 2011 | 35 | | M: 26.3±1.2 F:
25.5±1.4 | M: 176.8±1.4 F:
166.8±1.4 | Breathed hypoxic
gas (12.8% FiO2; simulated altitude: 3,900 m) | 50 | (29) |
Data quality
The selected studies were also assessed using
Cochrane's recommended tool to assess the risk of bias. There was a
low risk of bias in >50% of studies in terms of random sequence
generation, blinding of the participants and trial personnel,
incomplete outcome data and selective reporting. (Fig. 2). All the studies except for Hsu
et al (3), Toro-Salinas
et al (28) and Lalande
et al (26) described the
randomization process (Fig.
3).
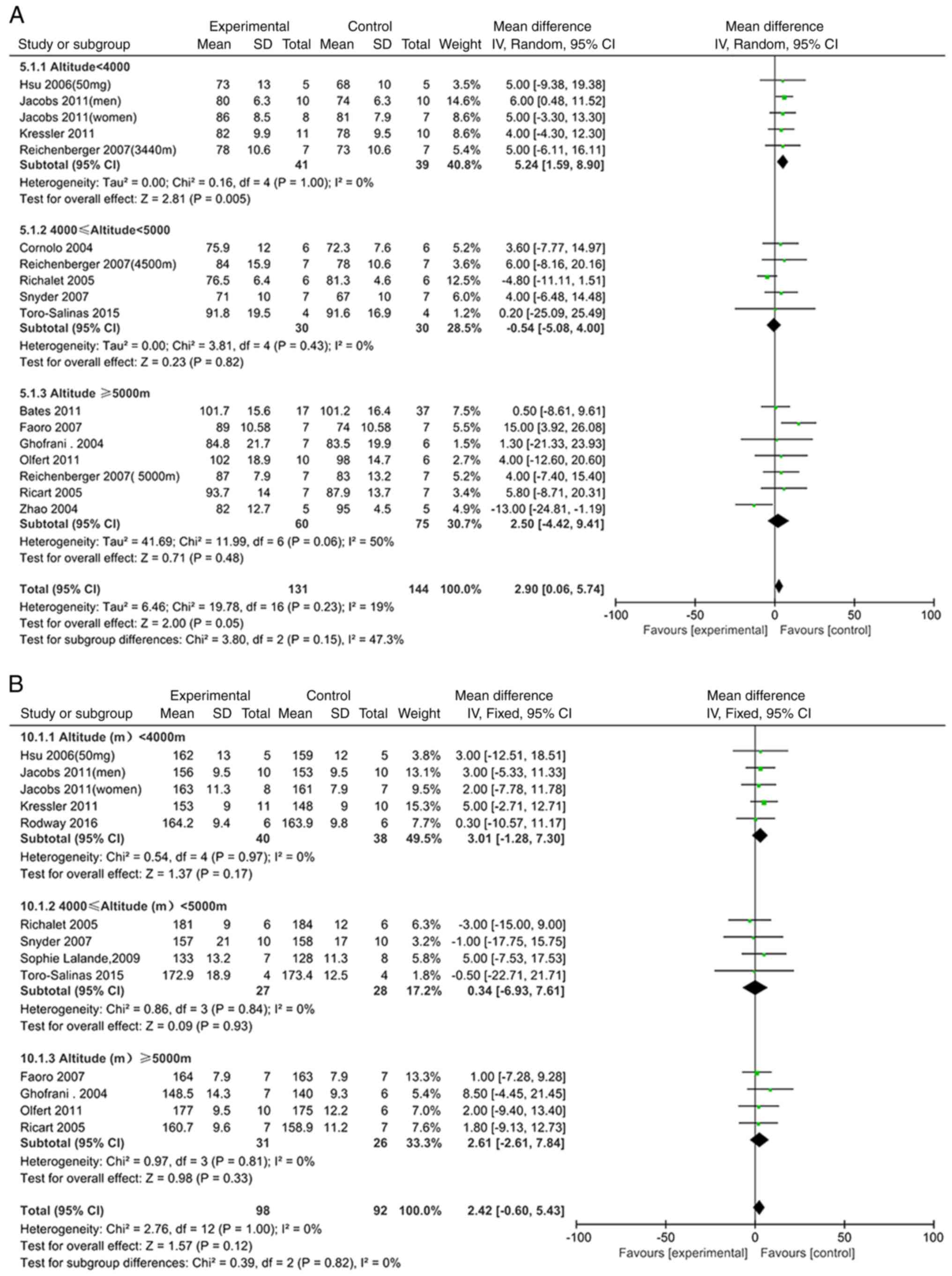
A total of 14 studies reported the mean resting
heart rate while 12 studies reported the exercising heart rate.
Only two of the 14 studies indicated a statistically significant
elevation in resting heart rate (16,29).
Meta-analysis of the data indicated that Sildenafil increased heart
rate, without significance, except at altitude <4,000 meters.
The mean increase in the resting heart rate of participants
allocated to the Sildenafil treatment group was 5.24 (95% CI
1.59-8.90; P<0.01; Fig.
4A) compared with the control group at <4,000 meters,
without significant heterogeneity (I2=0%;
P>0.1). There was also no significant difference in the
resting heart rate between both groups above 4,000 meters, with no
heterogeneity evidence (I2≤50%). During exercise, no
change in heart rate was associated with Sildenafil treatment
across different altitudes (P>0.05; Fig. 4B). I2 value of
heterogeneity was 50% among studies above 5,000 meters, natural
hypoxia and simulated hypoxia were used for subgroup analysis. A
total of three studies (4,15,27)
simulated hypoxia and others simulated natural hypoxia. Subgroup
analysis results show that no significant difference in heart rate
was observed between the two groups whether at naturally high
altitude or simulation of high altitude
(Psimulated=0.77, Pnatural=0.12), with no
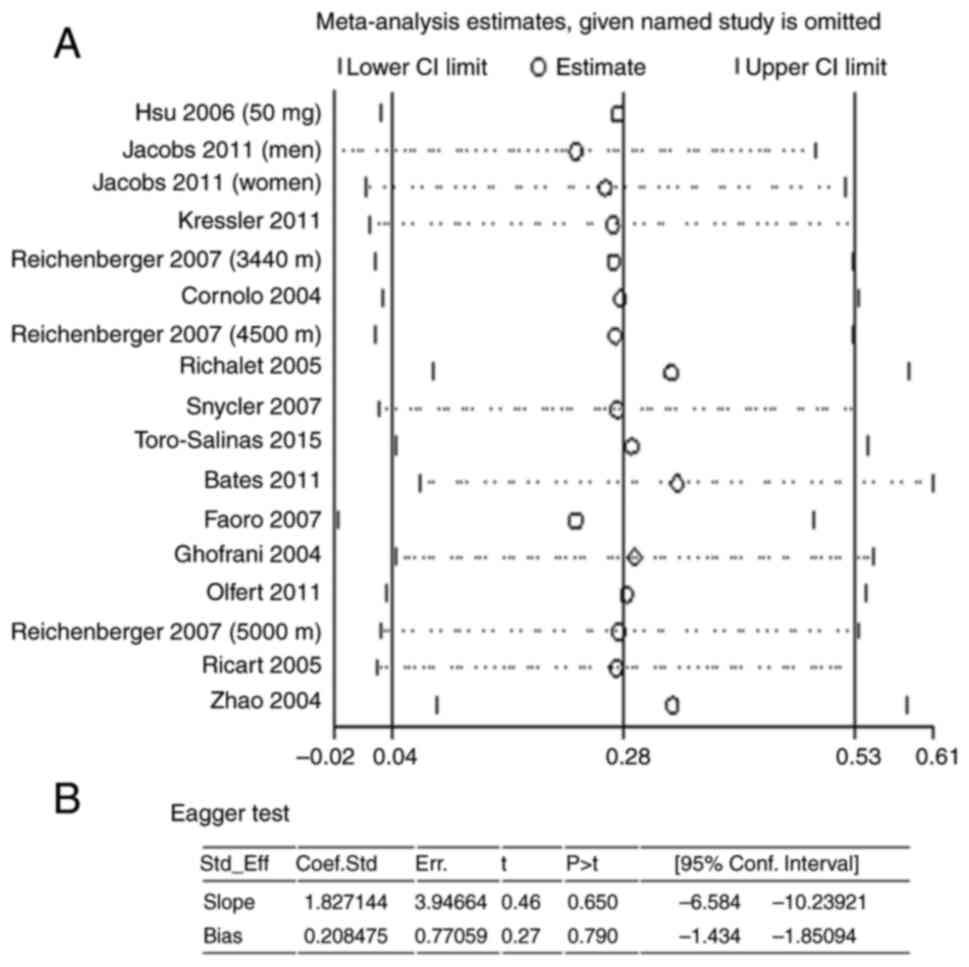
evidence of heterogeneity (I2=0%). Moreover, the results
of performing a leave-one-out sensitivity analysis remained
consistent with those of the overall analysis (Fig. 5A). Publication bias using Egger's
test showed no publication bias (P>0.05; Fig. 5B)
A total of nine studies reported data on cardiac
output at rest (2,3,5,16,17,25,28-30).
Meta-analysis of the data indicated that Sildenafil did not elevate
cardiac output below 5,000 meters. However, cardiac output did
increase at rest compared with the placebo group when exposed to
altitudes above 5,000 meters (MD, 1.14; 95% CI, 0.44, 1.84;
P<0.01; Fig. 6A).
Although there was a trend of increased cardiac output during
exercise at different altitudes, the difference was not significant
(P>0.05; Fig. 6B).
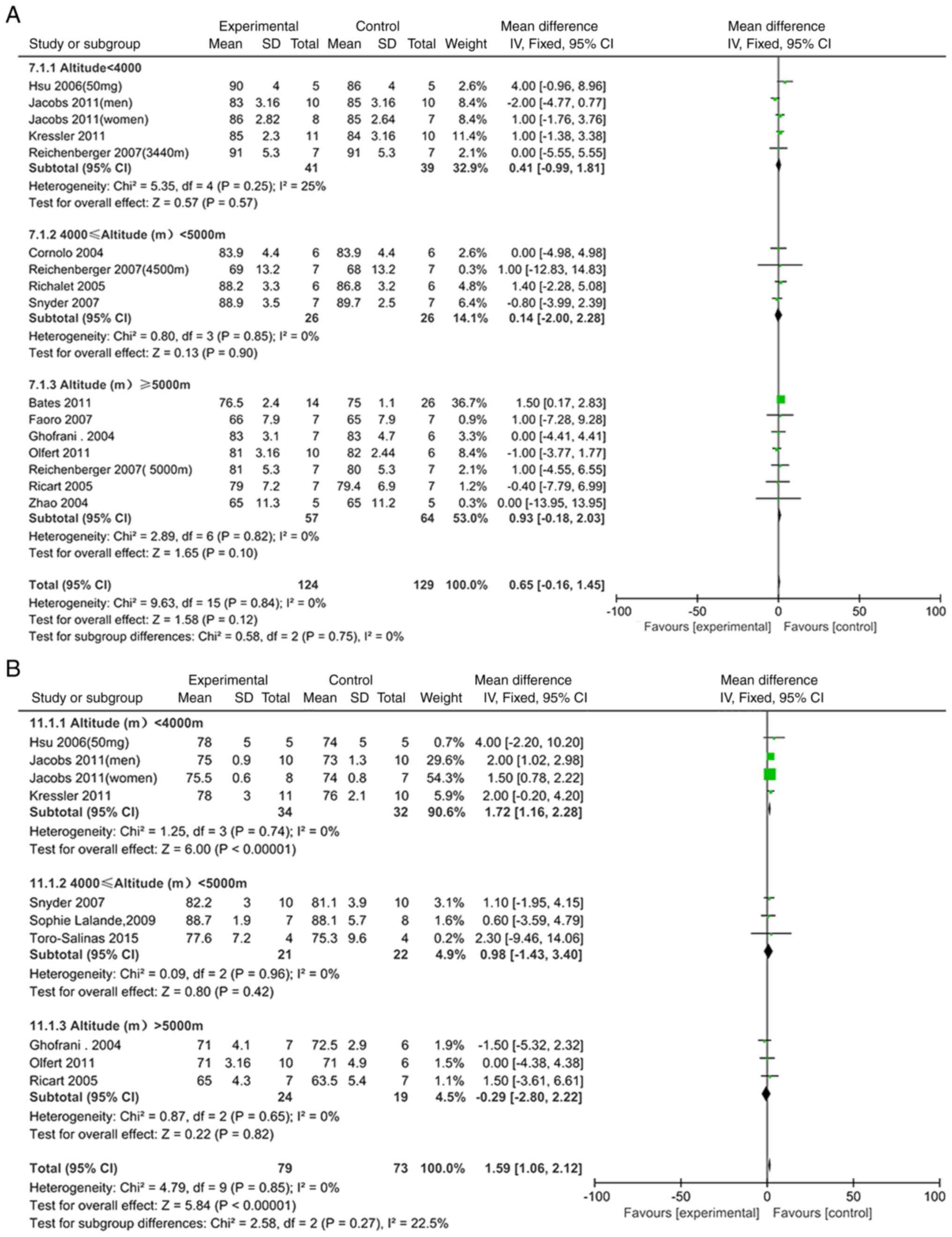
A total of 13 studies reported data at rest and nine
during exercise for SaO2. Meta-analysis indicated that
the administration of Sildenafil did not increase SaO2
at rest after exposure to high altitudes (P>0.05) with no
apparent heterogeneity (I2=0%; P>0.1) detected
among studies (Fig. 7A).
SaO2 of the treatment group was significantly higher
during exercise than the control group below 4,000 meters (MD=1.72;
95% CI: 1.16, 2.28; P<0.0001), with no significant
heterogeneity observed (I2=0%; P>0.1). No
significant difference and heterogeneity were observed between the
Sildenafil and placebo groups (P>0.05) above 4,000 meters
(I2=0%) (Fig. 7B).
A total of seven studies reported PASP at rest and
five studies revealed that Sildenafil significantly attenuated
PASP. According to the meta-analysis, a significant PASP reduction
was observed due to treatment with Sildenafil by a mean of 4.07
mmHg (95% CI: -7.36, -0.78; P=0.02) at an altitude of 4,000-5,000
meters and 5.67 mmHg (95% CI: -7.32, -4.01; P<0.0001)
above 5,000 meters, without significant heterogeneity
(I2<50%; P>0.1) (Fig. 8A). Two studies reported PASP during
exercise at an altitude of 5,000 meters. Compared with the placebo
group, the mean reduction was 6.10 mmHg (95% CI: -8.34, -3.86;
P<0.0001) in the Sildenafil group (Fig. 8B).
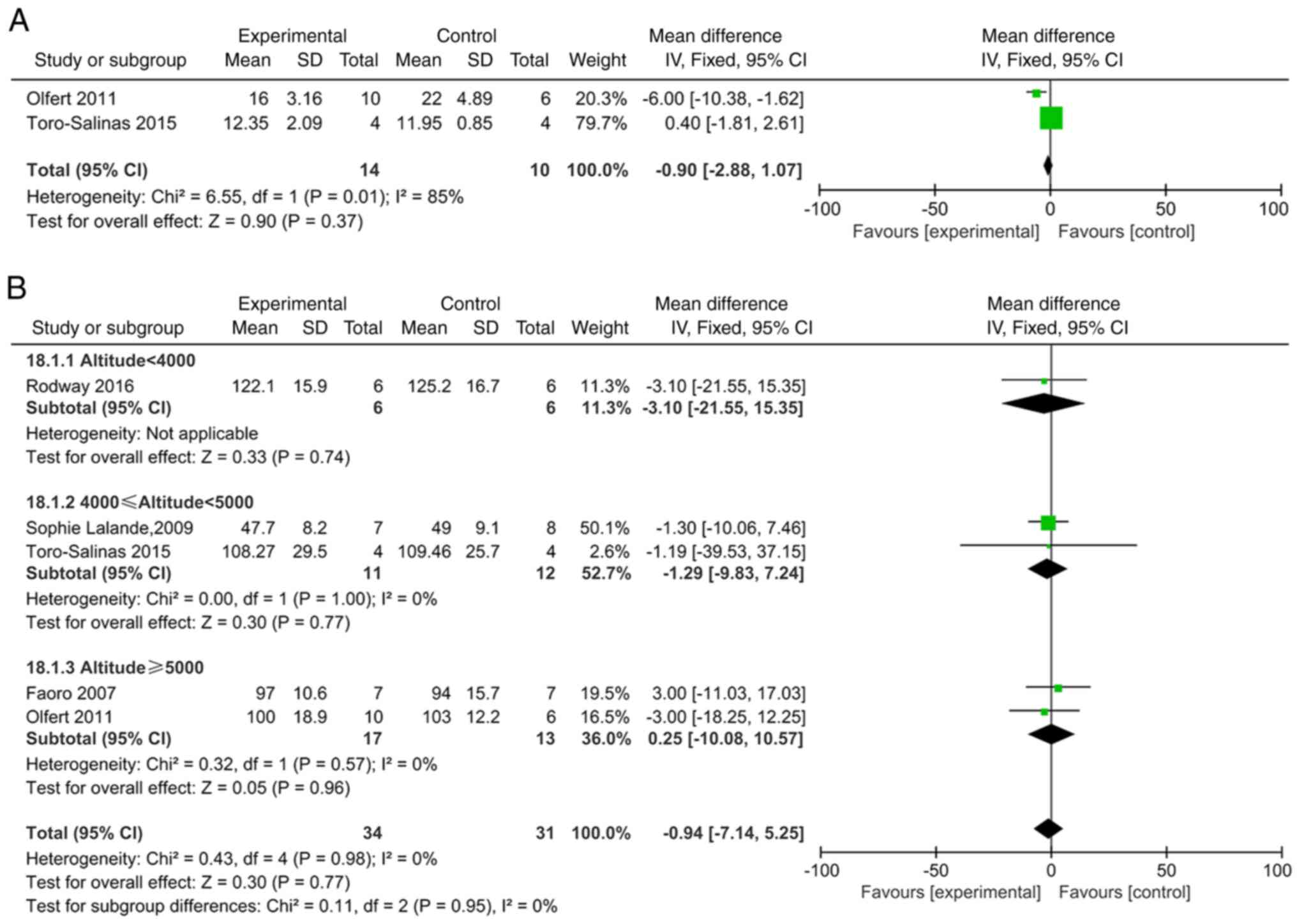
A total of two studies reported minute ventilation
(VE) at rest and five during exercise. No differences
were identified for VE either rest or during exercise
(P>0.05) in Sildenafil group compared with the control
group after exposure to high altitudes (Fig. 9).
Discussion
High altitudes are among the most inhospitable
locations on earth. The atmospheric pressure decreases gradually as
altitude increases. Research in a hypobaric hypoxic environment
indicates that altitude differences and the rate of increase affect
humans physiologically (31-34).
However, to the best of our knowledge, almost no hypoxic effects
below 2,500 meters have been reported (31). Humans can be affected by hypoxia at
an altitude of >3,000 meters (31). Individuals unaccustomed to high
altitudes will be affected at >4,000 meters without
environmental adaptation (31).
High altitude hypoxia leads to altitude sickness, due to decreased
barometric pressure when ascending from low to high altitudes,
thereby reducing the pressure of inspired oxygen (35,36).
Sildenafil helped to reduce pulmonary vascular resistance in
different forms of precapillary pulmonary hypertension (37-39)
and mimicked the features of a selective pulmonary vasodilator.
However, a threshold altitude may limit the usefulness of
Sildenafil at lower altitudes while providing greater benefits
above the threshold (16). The
hypoxic pulmonary vasoconstriction (HPV) response does not elevate
cardiac output sufficiently for Sildenafil to impart a recognizable
improvement below 3,000 meters (16). Researchers have also considered
several other factors modulating the effectiveness of Sildenafil
(16,29,40).
This includes the possibility of responders and non-responders, the
influence of central regulation on exercise and sex difference.
Encouraged by the previous research, the present
study considered the effect of sildenafil on healthy humans in
plateau environment according to different altitude and exercise
state. Unlike previous meta-analyses involving the impact of
Sildenafil on high altitude hypoxia and its complications, the
present meta-analysis focused on the potential clinical efficacy of
Sildenafil at different high altitudes among healthy individuals
while exercising and resting.
The present study revealed that Sildenafil therapy
increases resting heart rate at <4,000 meters and decreases PASP
at other altitudes. Cardiac output could be significantly elevated
above 5,000 meters. During exercise, Sildenafil increased
SaO2 <4,000 meters and reduced PASP above 5,000
meters.
The meta-analysis data revealed that the resting
heart rate was significantly elevated after Sildenafil treatment
below 4,000 meters, inconsistent with previous research. A total of
two studies found an increase in resting heart rate at above 5,000
meters due to Sildenafil (4,27),
but it was found to decrease in the present review (15). There are possible adverse effects
of Sildenafil treatment at altitudes <4,000 meters in
individuals with an elevated response to this drug (28). These data suggest that treating
healthy individuals with Sildenafil is not likely to be beneficial
for every person. An explanation for this differential response is
worthy of further research. Sildenafil has a moderate effect on
increasing SaO2 during exercise (40), but another study provided
non-significant benefits (11).
The present meta-analysis showed that Sildenafil considerably
increased SaO2 during exercise, but only at altitudes
<4,000 meters. The beneficial effect was not apparent at other
altitudes, either during exercise or at rest. Therefore, the
beneficial impact of Sildenafil on SaO2 is associated
with altitude, rest, or exercise.
Sildenafil reduces PASP at rest and during exercise
and the effect was observed at any altitude. The effect of
Sildenafil on PAP leads to increased cardiac output, mostly above
5,000 meters. The pooled data analysis revealed that the effect on
PAP moderately increases cardiac output at rest.
The aforementioned results in the present study
demonstrated that the efficacy of Sildenafil in healthy humans with
high-altitude hypoxia was associated with altitude and rest or
exercise.
Throughout the current analysis, two studies
depicted an elevated effect of Sildenafil on heart rate without any
significant methodological heterogeneity (16,29).
When the study by Jacobs et al was removed, the effect on
heart rate decreased (29). This
study stratified the effects of Sildenafil in men and women and is
an outlying data point and its effect on the outcome requires
careful consideration. The possible lack of published negative
research will bias the aggregate effect towards the positive effect
of Sildenafil. This will significantly affect the rational guidance
of medication for people rushing into the plateau or altitude
hypoxia, in sports medicine, or altitude acclimatization and combat
ability of officers and men at altitude.
There were several limitations to the present study.
In recognition of the differences between hypoxia simulated at high
altitudes in laboratory conditions and natural high altitudes,
subgroup analysis would have enhanced the findings of the present
review. However, the lack of available studies prevented such an
analysis. There were different designs of experiments. A total of
six included studies were cross-over trials, all with small sample
sizes. Although the research was conducted based on altitude, other
outcomes, such as exercise intensity and different dose, were not
classified due to a lack of data.
Therefore, the present review provided novel
insights while interpreting the efficacy of Sildenafil on
echocardiographic and hemodynamic parameters in healthy humans in
high-altitude hypoxia. The efficacy depended on whether the subject
is exercising or at rest but also on altitude.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the Natural Science
Foundation of China (grant no. 82260333), basic research project of
Qinghai province (grant no. 2023-ZJ-769) and Kunlun Talents
High-end Innovation and Entrepreneurial Talents project in Qinghai
province.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from PubMed (https://pubmed.ncbi.nlm.nih.gov/), Embase (https://www.embase.com) and Cochrane (https://www.cochrane.org/) website. The datasets used
and/or analyzed in the present study are available from the
corresponding author on reasonable request.
Authors' contributions
ZCD and ZZZ contributed to study conception and
design, drafted the submitted manuscript and revised it critically
for important intellectual content. ZQY and GMD independently
appraised the study quality of the included trials and contributed
to the analysis and interpretation of data. LDJ processed and
beautified the pictures in the manuscript. ZCD and ZZZ contributed
to acquisition, analysis and interpretation of data and drafted the
manuscript. ZCD and ZQY contributed to the literature search and
extracted data. SL contributed to sensitivity analyses and
publication bias. All authors read and approved the final
manuscript. Data authentication is not applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Rubin LJ: Primary pulmonary hypertension.
N Engl J Med. 336:111–117. 1997.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Ghofrani HA, Reichenberger F, Kohstall MG,
Mrosek EH, Seeger T, Olschewski H, Seeger W and Grimminger F:
Sildenafil increased exercise capacity during hypoxia at low
altitudes and at Mount Everest base camp: A randomized,
double-blind, placebo-controlled crossover trial. Ann Intern Med.
141:169–177. 2004.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Hsu AR, Barnholt KE, Grundmann NK, Lin JH,
McCallum SW and Friedlander AL: Sildenafil improves cardiac output
and exercise performance during acute hypoxia, but not normoxia. J
Appl Physiol (1985). 100:2031–2040. 2006.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Ricart A, Maristany J, Fort N, Leal C,
Pagés T and Viscor G: Effects of sildenafil on the human response
to acute hypoxia and exercise. High Alt Med Biol. 6:43–49.
2005.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Richalet JP, Gratadour P, Robach P, Pham
I, Déchaux M, Joncquiert-Latarjet A, Mollard P, Brugniaux J and
Cornolo J: Sildenafil inhibits altitude-induced hypoxemia and
pulmonary hypertension. Am J Respir Crit Care Med. 171:275–281.
2005.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Weitzenblum E: Chronic cor pulmonale.
Heart. 89:225–230. 2003.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Dorrington KL, Clar C, Young JD, Jonas M,
Tansley JG and Robbins PA: Time course of the human pulmonary
vascular response to 8 hours of isocapnic hypoxia. Am J Physiol.
273:H1126–H1134. 1997.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Scherrer U, Allemann Y, Rexhaj E, Rimoldi
SF and Sartori C: Mechanisms and drug therapy of pulmonary
hypertension at high altitude. High Alt Med Biol. 14:126–133.
2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Humbert M, Morrell NW, Archer SL, Stenmark
KR, MacLean MR, Lang IM, Christman BW, Weir EK, Eickelberg O,
Voelkel NF and Rabinovitch M: Cellular and molecular pathobiology
of pulmonary arterial hypertension. J Am Coll Cardiol 43(12 Suppl
S). 43:S13–S24. 2004.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Andersson KE: PDE5 inhibitors-pharmacology
and clinical applications 20 years after sildenafil discovery. Br J
Pharmacol. 175:2554–2565. 2018.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Jin B, Luo XP, Ni HC and Shi HM:
Phosphodiesterase type 5 inhibitors for high-altitude pulmonary
hypertension: A meta-analysis. Clin Drug Investig. 30:259–265.
2010.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Barst RJ, Ivy DD, Gaitan G, Szatmari A,
Rudzinski A, Garcia AE, Sastry BK, Pulido T, Layton GR,
Serdarevic-Pehar M and Wessel DL: A randomized, double-blind,
placebo-controlled, dose-ranging study of oral sildenafil citrate
in treatment-naive children with pulmonary arterial hypertension.
Circulation. 125:324–334. 2012.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Kjaergaard J, Snyder EM, Hassager C, Olson
TP, Oh JK, Johnson BD and Frantz RP: Right ventricular function
with hypoxic exercise: Effects of sildenafil. Eur J Appl Physiol.
102:87–95. 2007.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Xu Y, Liu Y, Liu J and Qian G:
Meta-analysis of clinical efficacy of sildenafil, a
phosphodiesterase type-5 inhibitor on high altitude hypoxia and its
complications. High Alt Med Biol. 15:46–51. 2014.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Zhao L, Mason NA, Morrell NW, Kojonazarov
B, Sadykov A, Maripov A, Mirrakhimov MM, Aldashev A and Wilkins MR:
Sildenafil inhibits hypoxia-induced pulmonary hypertension.
Circulation. 104:424–428. 2001.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Kressler J, Stoutenberg M, Roos BA,
Friedlander AL, Perry AC, Signorile JF and Jacobs KA: Sildenafil
does not improve steady state cardiovascular hemodynamics, peak
power, or 15-km time trial cycling performance at simulated
moderate or high altitudes in men and women. Eur J Appl Physiol.
111:3031–3040. 2011.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Faoro V, Lamotte M, Deboeck G, Pavelescu
A, Huez S, Guenard H, Martinot JB and Naeije R: Effects of
sildenafil on exercise capacity in hypoxic normal subjects. High
Alt Med Biol. 8:155–163. 2007.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Calbet JA, Boushel R, Rådegran G,
Søndergaard H, Wagner PD and Saltin B: Determinants of maximal
oxygen uptake in severe acute hypoxia. Am J Physiol Regul Integr
Comp Physio. 284:R291–R303. 2003.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Fulco CS, Rock PB and Cymerman A: Maximal
and submaximal exercise performance at altitude. Aviat Space
Environ Med. 69:793–801. 1998.PubMed/NCBI
|
|
20
|
Reichenberger F, Kohstall MG, Seeger T,
Olschewski H, Grimminger F, Seeger W and Ghofrani HA: Effect of
sildenafil on hypoxia-induced changes in pulmonary circulation and
right ventricular function. Respir Physiol Neurobiol. 159:196–201.
2007.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Moher D, Pham B, Jones A, Cook DJ, Jadad
AR, Moher M, Tugwell P and Klassen TP: Does quality of reports of
randomised trials affect estimates of intervention efficacy
reported in meta-analyses? Lancet. 352:609–613. 1998.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Higgins JP, Thompson SG, Deeks JJ and
Altman DG: Measuring inconsistency in meta-analyses. BMJ.
327:557–560. 2003.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Altman DG and Bland JM: Standard
deviations and standard errors. BMJ. 331(903)2005.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Hozo SP, Djulbegovic B and Hozo I:
Estimating the mean and variance from the median, range, and the
size of a sample. BMC Med Res Methodol. 5(13)2005.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Snyder EM, Olson TP, Johnson BD and Frantz
RP: Influence of sildenafil on lung diffusion during exposure to
acute hypoxia at rest and during exercise in healthy humans. Eur J
Appl Physiol. 103:421–430. 2008.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Lalande S, Snyder EM, Olson TP, Hulsebus
ML, Orban M, Somers VK, Johnson BD and Frantz RP: The effects of
sildenafil and acetazolamide on breathing efficiency and
ventilatory control during hypoxic exercise. Eur J Appl Physiol.
106:509–515. 2009.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Olfert IM, Loeckinger A, Treml B,
Faulhaber M, Flatz M, Burtscher M, Truebsbach S and Kleinsasser A:
Sildenafil and bosentan improve arterial oxygenation during acute
hypoxic exercise: A controlled laboratory trial. Wilderness Environ
Med. 22:211–221. 2011.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Toro-Salinas AH, Fort N, Torrella JR,
Pagès T, Javierre C and Viscor G: Sildenafil does not improve
exercise capacity under acute hypoxia exposure. Int J Sports Med.
37:785–791. 2016.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Jacobs KA, Kressler J, Stoutenberg M, Roos
BA and Friedlander AL: Sildenafil has little influence on
cardiovascular hemodynamics or 6-km time trial performance in
trained men and women at simulated high altitude. High Alt Med
Biol. 12:215–222. 2011.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Cornolo J, Mollard P, Brugniaux JV, Robach
P and Richalet JP: Autonomic control of the cardiovascular system
during acclimatization to high altitude: Effects of sildenafil. J
Appl Physiol. 97:935–940. 2004.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Hainsworth R, Drinkhill MJ and
Rivera-Chira M: The autonomic nervous system at high altitude. Clin
Auton Res. 17:13–19. 2007.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Vogel JA, Hansen JE and Harris CW:
Cardiovascular responses in man during exhaustive work at sea level
and high altitude. J Appl Physiol. 23:531–539. 1967.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Vogel JA and Harris CW: Cardiopulmonary
responses of resting man during early exposure to high altitude. J
Appl Physiol. 22:1124–1128. 1967.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Coppel J, Hennis P, Gilbert-Kawai E and
Grocott MP: The physiological effects of hypobaric hypoxia versus
normobaric hypoxia: A systematic review of crossover trials. Extrem
Physiol Med. 4(2)2015.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Netzer N, Strohl K, Faulhaber M, Gatterer
H and Burtscher M: Hypoxia-related altitude illnesses. J Travel
Med. 20:247–255. 2013.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Swenson ER: Hypoxic pulmonary
vasoconstriction. High Alt Med Biol. 14:101–110. 2013.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Ghofrani HA, Wiedemann R, Rose F,
Olschewski H, Schermuly RT, Weissmann N, Seeger W and Grimminger F:
Combination therapy with oral sildenafil and inhaled iloprost for
severe pulmonary hypertension. Ann Intern Med. 136:515–522.
2002.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Wilkens H, Guth A, König J, Forestier N,
Cremers B, Hennen B, Böhm M and Sybrecht GW: Effect of inhaled
iloprost plus oral sildenafil in patients with primary pulmonary
hypertension. Circulation. 104:1218–1222. 2001.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Sastry BK, Narasimhan C, Reddy NK, Anand
B, Prakash GS, Raju PR and Kumar DN: A study of clinical efficacy
of sildenafil in patients with primary pulmonary hypertension.
Indian Heart J. 54:410–414. 2002.PubMed/NCBI
|
|
40
|
Carter EA, Lohse K, Sheel W and Koehle M:
Sildenafil does not reliably improve exercise performance in
hypoxia: A systematic review. BMJ Open Sport Exerc Med.
5(e000526)2019.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Rodway GW, Lovelace AJ, Lanspa MJ,
McIntosh SE, Bell J, Briggs B, Weaver LK, Yanowitz F and Grissom
CK: Sildenafil and exercise capacity in the elderly at moderate
altitude. Wilderness Environ Med. 27:307–315. 2016.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Bates MG, Thompson AA, Baillie JK,
Sutherland AI, Irving JB, Hirani N and Webb DJ: Sildenafil citrate
for the prevention of high altitude hypoxic pulmonary hypertension:
double blind, randomized, placebo-controlled trial. High Alt Med
Biol. 12:207–214. 2011.PubMed/NCBI View Article : Google Scholar
|