Introduction
The global burden associated with liver cancer is
substantial. In 2020, worldwide, 905,700 new liver cancer cases and
830,200 liver cancer deaths were estimated (1). In 90 countries, liver cancer is among
the top 5 causes of cancer death, and in 46 countries it is among
the top 3 causes of cancer death (2). Furthermore, with the growth and aging
of the world population, the number of liver cancer cases is
expected to increase with a predicted 1.3 million liver cancer
deaths in 2040(2). Thus, liver
cancer, and specifically hepatocellular carcinoma (HCC), which
constitutes the majority of liver cancer cases (75-80%), presents a
significant global health problem (1).
Considerations in HCC treatment include not only the
disease stage, tumor characteristics, and patient's comorbidities
but also liver function and the potential hepatotoxicity of the
treatment, as the benefits of the treatment should be weighed
against a potential deterioration in hepatic function (3,4).
Liver function is often categorized by the Child-Pugh (CP) scoring
system, which integrates multiple laboratory and clinical criteria.
The system classifies patients into 3 categories: Child-Pugh A
(CPA; good hepatic function), Child-Pugh B (CPB; moderately
impaired hepatic function), and Child-Pugh C (CPC; advanced hepatic
dysfunction) (5). For CPB HCC
patients, the only curative option includes downstaging followed by
liver transplantation. However, this approach is appropriate for
only a small proportion of patients and is also limited by the
scarcity of livers available for transplantation (6). Thus, CPB HCC patients are often
treated with the multi-kinase inhibitor sorafenib, which is
approved by the US Food and Drug Administration (FDA) for all
advanced HCC patients, irrespective of liver function (7). Notably, all the clinical trials that
investigated first-line treatments for advanced HCC focused on
patients with CPA cirrhosis (8).
Likewise, second-line treatments (following treatment with
sorafenib) are also primarily geared toward CPA patients. CPB
patients are typically excluded from clinical studies as their
prognosis is poor and their expected response rate is low (9). Thus, presently, established
treatments for advanced HCC patients with CPB cirrhosis are
lacking.
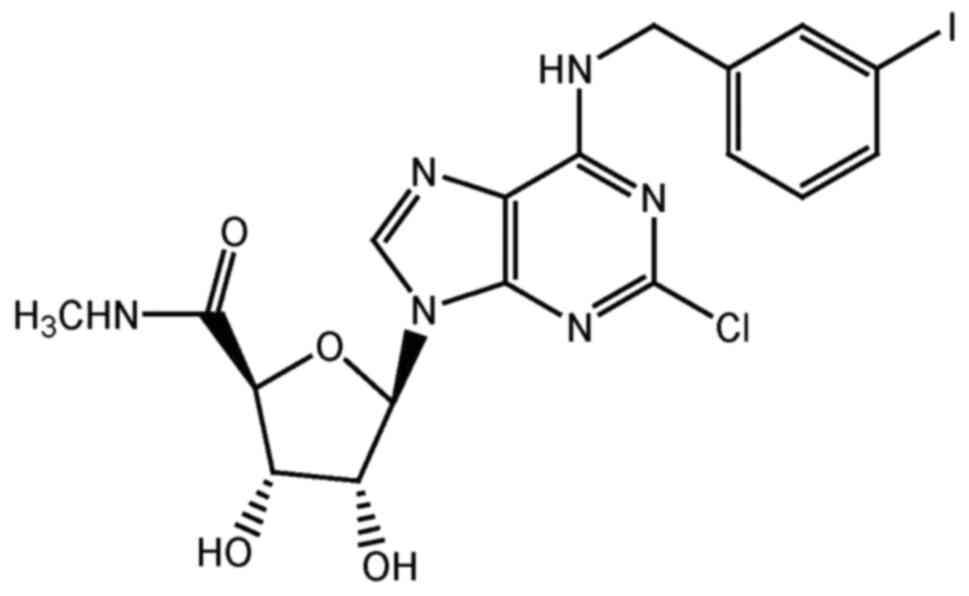
Namodenoson (CF102, also known as Cl-IB-MECA; CAS
registry number, 163042-96-4) is an orally available, small
molecule, which is a highly selective A3 adenosine receptor (A3AR)
agonist. The molecular formula of namodenoson is
C18H18ClIN6O4
(molecular weight, 544.73 Da) (Fig.
1). Namodenoson is undergoing clinical development for multiple
indications, including HCC, as A3AR was found to be overexpressed
in HCC cells and peripheral blood mononuclear cells (PBMC) derived
from patients with HCC, but not in healthy tissues (10). The mechanism of action of
namodenoson includes direct and indirect effects. The direct effect
involves de-regulation of 2 signaling pathways (NF-κB, Wnt), which
results in increased levels of pro-apoptotic proteins and
Fas-ligand, leading to inhibition of tumor growth (10,11).
The indirect effect involves PBMC and specifically, natural killer
(NK) cells, as namodenoson was found to activate NK cells and
induce IL-2 production, resulting in tumor growth inhibition
(12).
Following encouraging results in an open-label phase
1/2 study that investigated namodenoson in advanced HCC (13), a randomized, placebo-controlled,
multicenter phase 2 clinical trial was initiated to investigate
namodenoson as a second-line treatment for advanced HCC patients
with CPB cirrhosis (clinicaltrials.gov identifier: NCT02128958). The
findings from this phase 2 trial have been published (14). This trial, which included a total
of 78 patients (50 in the namodenoson arm who received 25 mg, BID,
and 28 in the placebo arm), demonstrated that namodenoson has a
favorable safety profile. No patients withdrew due to adverse
events, and no deaths were noted (14). The study did not meet its primary
endpoint, which was overall survival (OS). The median OS was 4.1
months in the namodenoson arm vs. 4.3 months in the placebo arm
(hazard ratio, 0.82; 95% confidence interval, 0.49-1.38; P=0.46).
However, analysis of the subgroup of patients with the least severe
cirrhosis in the CPB category (i.e., patients with a CP score of
7), which included 34 patients in the namodenoson arm and 22 in the
placebo arm, revealed a statistically significant better 12-month
OS in the namodenoson arm vs. placebo (44% vs. 18%, P=0.028)
(14).
The current case report presents a patient who
participated in this phase 2 study of namodenoson vs. placebo in
HCC with CPB cirrhosis, was assigned to the namodenoson arm and
received namodenoson throughout the blinded study, and who, upon
unblinding, continued treatment with open-label namodenoson for a
total treatment of more than 6 years through the extension
program.
Case presentation
The current case involves a patient with advanced
HCC and a history of hepatitis B-related cirrhosis, who met the
inclusion criteria of the randomized placebo-controlled phase 2
clinical trial investigating namodenoson for the treatment of HCC
with CPB cirrhosis (14). This
phase 2 study was approved by the relevant local Institution Review
Boards (IRBs). For the site in which the patient described herein
participated, the study was approved by the National Bioethics
Committee for Medicine and Medical Devices in Bucharest Romania
(approval date, Oct 29, 2014; approval code, 116S).
The patient enrolled to the study on Nov 28, 2016,
and was treated at the S.C. Pelican Impex S.R.L.-Oncology
Department in Oradea, Romania. This patient, who was 61 years old
at enrollment, was a Caucasian woman with metastatic HCC that was
histology-confirmed (data not shown) and had received 5 cycles of
sorafenib therapy as first-line treatment for her disease. The
patient was categorized as having CPB cirrhosis with a CP score of
7: She had ascites but no encephalitis, her total bilirubin level
was 0.23 mg/dl (normal range: 0.3-1.0 mg/dl), her albumin level was
3.2 g/dl (normal range: 3.5-5.5 g/dl), and her international
normalized ratio (INR) was 1.0 (normal range: 0.9-1.2). Also at
enrollment, the patient had Barcelona Clinic Liver Cancer (BCLC)
stage C, and Eastern Cooperative Oncology Group (ECOG) performance
status of 1.
Computed tomography (CT) scans demonstrated that at
baseline, the patient had 2 HCC lesions in the liver. The larger
lesion was observed in the right lobe (segments VI and VII) and its
longest diameter was 91 mm. A smaller liver lesion was observed in
segment VI of the right lobe and its longest diameter was 55 mm. In
addition, 2 lesions were noted in the abdominal wall (a pelvic
peritoneal nodule with a longest diameter of 20 mm, and a
subumbilical peritoneal nodule with a longest diameter of 18 mm),
and another nodule was noted in the interaortocaval lymph node
(longest diameter, 16 mm). The sum of the longest diameters of all
target lesions at baseline was 200 mm. In addition, peritoneal
carcinomatosis was noted.
The patient was randomized to the namodenoson arm of
the study, and thus received 25 mg namodenoson BID for the duration
of study. Her treatment started on Dec 7, 2016 (approximately 6
weeks after discontinuing sorafenib) and participation in the
blinded study, where she had a follow up every 2 weeks, continued
until March 29, 2019. Upon unblinding of the treatment assignments
in the phase 2 study, the patient continued treatment with
open-label namodenoson at the same dose for a total of more than 6
years under an extension program (treatment is ongoing).
After 2 treatment cycles (e.g., approximately 7
weeks) the CT scans revealed a smaller tumor mass, consistent with
a partial response. Within 4 years of treatment, the tumors, as
well as ascites, and peritoneal carcinomatosis disappeared,
consistent with a complete response by RECIST 1.1 and mRECIST
(Fig. 2). This complete response
is ongoing.
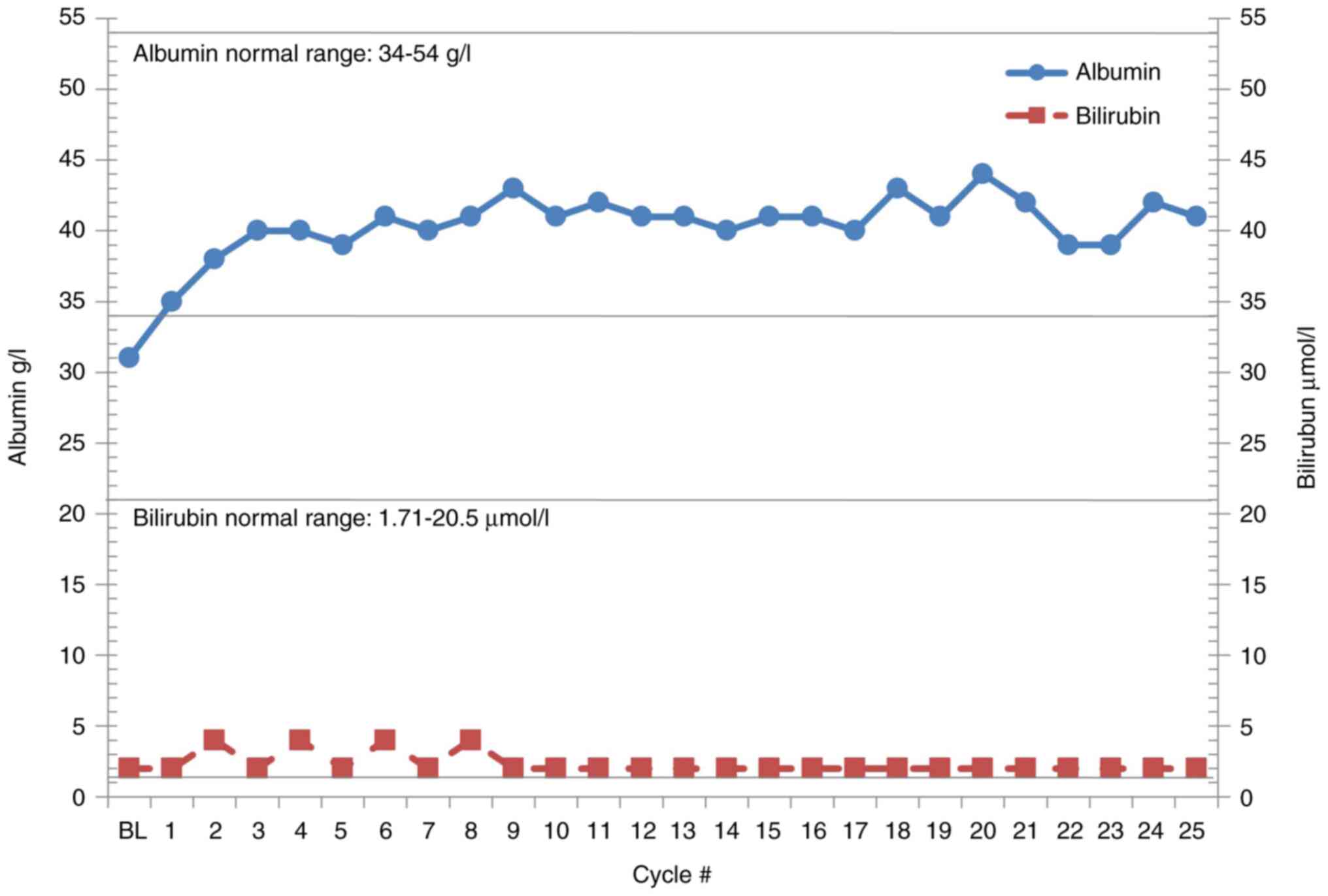
A secondary objective of the study was an evaluation
of liver function. At baseline, albumin levels were lower than
normal and normalized within 1 treatment cycle (4 weeks) (Fig. 3). Bilirubin levels were within the
normal range at baseline and remained within this range throughout
(Fig. 3).
Also, at baseline, elevated alanine transaminase
(ALT) and aspartate aminotransferase (AST) levels were reported (68
U/l and 44 U/l, respectively). Within 1 treatment cycle (4 weeks),
both ALT and AST levels normalized and were stable for more than 6
years (Fig. 4). Also, the serum
α-fetoprotein level, which was elevated at baseline (47 ng/ml)
normalized after 5 cycles of treatment (20 weeks) and was 1.3 ng/ml
at time of complete response. The patient experienced no
treatment-emergent adverse events. At the time of reporting this
case (more than 6 years from namodenoson treatment initiation), the
patient is alive, on namodenoson treatment (25 mg BID), and her
response is ongoing as manifested by imaging studies and liver
function evaluation.
Discussion
This report of a patient who participated in the
phase 2 study of namodenoson in advanced HCC with CPB cirrhosis
demonstrates that namodenoson treatment is safe and well tolerated
and can result in a long-term complete response and improved liver
function in HCC with CPB cirrhosis and a CP score of 7. The
improvement in liver function is notable, as it is consistent with
the hepatoprotective properties of namodenoson [reviewed in
(15)]. In contrast, sorafenib
(the first-line therapy received by the patient), similar to some
of the other tyrosine-kinase inhibitors, is associated with
hepatotoxicity (16).
The current case report provides only a low level of
evidence (LOE) for the clinical utility of namodenoson, with
respect to both its efficacy and safety, as it is limited by the
inherent characteristics of the design (i.e., a sample size of one
patient, lack of generalizability, lack of comparison). It is,
though, an example of a long-term response to namodenoson in one
patient that represents a population for whom no effective
treatments are available. This example could be used to complement
findings from prospective randomized trials that, by nature,
provide a higher LOE. The results of the phase 2 clinical trial
which included the patient described in the current case report
have been published (beyond the current case report, the data from
the open-label extension program do not merit publication)
(14).
The encouraging results of this phase 2 study
(14), particularly in the
subgroup of patients with a CP score of 7 prompted the initiation
of a pivotal phase 3 clinical study (LIVERATION) investigating
namodenoson (25 mg BID) in HCC and CPB cirrhosis with a CP score of
7, which is currently recruiting patients (ClinicalTrials.gov identifier: NCT05201404) (17). The patient described in the current
case report is not enrolled in the phase 3 study and will continue
to receive namodenoson as part of the phase 2 extension program
until disease progression or unaccepted toxicity. Data from the
phase 3 trial which will include a total of 471 patients will be
reported once the study is concluded and the data become
available.
Acknowledgements
Not applicable.
Funding
Funding: The Phase 2 study was sponsored by Can-Fite BioPharma
Ltd.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
PF, SMS, MF, ZH, AB-S, and MHS conceived and
designed the manuscript. IAC and RL performed data acquisition.
AB-S and PF wrote the manuscript. All authors read and approved the
final manuscript. PF, IAC, and MF confirm the authenticity of all
the raw data.
Ethics approval and consent to
participate
The phase 2 study in which the case described
therein participated was approved by all relevant national
regulatory authorities and local Ethics Committees/Institutional
Review Boards, was conducted in accordance with the Declaration of
Helsinki, and a written informed consent was obtained from all
patients [as described in Stemmer et al (14)]. For the site in which the patient
described herein participated, the study was approved by the
National Bioethics Committee for Medicine and Medical Devices in
Bucharest Romania (approval date, Oct 29, 2014; approval no.
116S).
Patient consent for publication
Written informed consent for publication was
obtained from the patient.
Competing interests
MF, ZH, MHS, and PF are Can-Fite BioPharma, Ltd
employees. SMS received research grant and stock options from
Can-Fite BioPharma Ltd. AB-S is a consultant for Can-Fite BioPharma
Ltd. The remaining authors declare no competing interests. Can-Fite
BioPharma sponsored the phase 2 study; however, this sponsorship
had no bearing on the results of the study or their scientific
interpretation.
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249.
2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Rumgay H, Arnold M, Ferlay J, Lesi O,
Cabasag CJ, Vignat J, Laversanne M, McGlynn KA and Soerjomataram I:
Global burden of primary liver cancer in 2020 and predictions to
2040. J Hepatol. 77:1598–1606. 2022.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ramadori G, Schleyer E and Armbrust T:
Safety of imatinib in patients with liver cirrhosis and
hepatocellular carcinoma. J Clin Oncol. 22:4244. 2004.
|
|
4
|
Shannon AH, Ruff SM and Pawlik TM: Expert
insights on current treatments for hepatocellular carcinoma:
Clinical and molecular approaches and bottlenecks to progress. J
Hepatocell Carcinoma. 9:1247–1261. 2022.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Tsoris A and Marlar CA: Use of the child
Pugh score in liver disease. In: StatPearls. Treasure Island (FL),
2021.
|
|
6
|
Granito A and Bolondi L: Non-transplant
therapies for patients with hepatocellular carcinoma and
Child-Pugh-Turcotte class B cirrhosis. Lancet Oncol. 18:e101–e112.
2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Sorafenib (package insert). Whippany, NJ:
Bayer Health Care Pharmaceuticals Inc; 2017.
|
|
8
|
Llovet JM, Ricci S, Mazzaferro V, Hilgard
P, Gane E, Blanc JF, de Oliveira AC, Santoro A, Raoul JL, Forner A,
et al: Sorafenib in advanced hepatocellular carcinoma. N Engl J
Med. 359:378–390. 2008.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Llovet JM, Di Bisceglie AM, Bruix J,
Kramer BS, Lencioni R, Zhu AX, Sherman M, Schwartz M, Lotze M,
Talwalkar J, et al: Design and endpoints of clinical trials in
hepatocellular carcinoma. J Natl Cancer Inst. 100:698–711.
2008.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Bar-Yehuda S, Stemmer SM, Madi L, Castel
D, Ochaion A, Cohen S, Barer F, Zabutti A, Perez-Liz G, Del Valle L
and Fishman P: The A3 adenosine receptor agonist CF102 induces
apoptosis of hepatocellular carcinoma via de-regulation of the Wnt
and NF-kappaB signal transduction pathways. Int J Oncol.
33:287–295. 2008.PubMed/NCBI
|
|
11
|
Cohen S, Stemmer SM, Zozulya G, Ochaion A,
Patoka R, Barer F, Bar-Yehuda S, Rath-Wolfson L, Jacobson KA and
Fishman P: CF102 an A3 adenosine receptor agonist mediates
anti-tumor and anti-inflammatory effects in the liver. J Cell
Physiol. 226:2438–2447. 2011.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Harish A, Hohana G, Fishman P, Arnon O and
Bar-Yehuda S: A3 adenosine receptor agonist potentiates natural
killer cell activity. Int J Oncol. 23:1245–1249. 2003.PubMed/NCBI
|
|
13
|
Stemmer SM, Benjaminov O, Medalia G,
Ciuraru NB, Silverman MH, Bar-Yehuda S, Fishman S, Harpaz Z,
Farbstein M, Cohen S, et al: CF102 for the treatment of
hepatocellular carcinoma: A phase I/II, open-label, dose-escalation
study. Oncologist. 18:25–26. 2013.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Stemmer SM, Manojlovic NS, Marinca MV,
Petrov P, Cherciu N, Ganea D, Ciuleanu TE, Pusca IA, Beg MS,
Purcell WT, et al: Namodenoson in advanced hepatocellular carcinoma
and Child-Pugh B cirrhosis: Randomized placebo-controlled clinical
trial. Cancers (Basel). 13(187)2021.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Fishman P, Stemmer SM, Bareket-Samish A,
Silverman MH and Kerns WD: Targeting the A3 adenosine receptor to
treat hepatocellular carcinoma: Anti-cancer and hepatoprotective
effects. Purinergic Signal. 19:513–522. 2023.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Shah RR, Morganroth J and Shah DR:
Hepatotoxicity of tyrosine kinase inhibitors: Clinical and
regulatory perspectives. Drug Saf. 36:491–503. 2013.PubMed/NCBI View Article : Google Scholar
|
|
17
|
National Library of Medicine (NLM):
Description of the ‘Namodenoson in the treatment of advanced
hepatocellular carcinoma in patients with Child-Pugh Class B7
cirrhosis (LIVERATION)’ study (NCT05201404). Clinical
Trials.gov ID, NCT05201404. NLM, Bethesda, MD, 2023. https://clinicaltrials.gov/study/NCT05201404?intr=namodenoson&rank=2&tab=table.
Accessed February 20, 2024.
|