Introduction
Cervical cancer (CC) ranks as the fourth most common
cancer and the fourth leading cause of cancer-related mortality
among women globally (1). For
high-grade squamous intraepithelial lesions of the cervix, cold
knife conization, laser conization or loop electrosurgical excision
procedures are standard treatment methods, while for elderly
patients unsuitable for cervical conization, a total hysterectomy
with bilateral salpingectomy serves as an alternative approach
(2). According to the National
Comprehensive Cancer Network guidelines (NCCN) guidelines (3), patients with stage IA1 cervical
cancer who do not require fertility preservation may undergo a
total hysterectomy, while those with fertility preservation needs
may undergo cervical conization. The subsequent treatment plan is
determined based on the presence or absence of lymphovascular space
invasion in the postoperative pathology. For cervical carcinoma in
situ, the 5-year survival rate after standard treatment reaches
93%, and for stage I CC confined to the cervix, it's 80% (4). However, superficial spreading
cervical squamous cell carcinoma (SCC) is a form of cervical SCC
that superficially extends to the inner surface of the uterus,
replacing the endometrium and the epithelium fallopian tubes, and
spreads to the ovarian surface. Due to its low incidence,
information on the diagnosis, treatment and prognosis of
superficial spreading cervical SCC is incomplete. In the present
case report, a case of superficial spreading cervical SCC with
microinvasion (#x003C;1 mm) extending to the endometrium and
interstitial portions of the fallopian tubes is presented, along
with a review of the relevant literature.
Case report
A 76-year-old patient was admitted to West China
Second Hospital (Chengdu, China) in September 2024 with lower
abdominal pain lasting for >1 month. At 2 weeks prior to
admission, the patient underwent an ultrasound examination at
another hospital, which revealed pyometra in the uterine cavity.
After undergoing antibiotic treatment (ceftriaxone + tinidazole) at
that hospital, the condition of the patient improved. A cervical
ThinPrep cytologic test was conducted, which revealed high-grade
squamous intraepithelial lesion with human papillomavirus (HPV)16
positivity. Subsequently, a cervical biopsy was performed, and the
pathological report results were sent to West China Second Hospital
for consultation. The consultation results indicated: At the 3 and
6 o'clock positions of the cervix, it was determined that chronic
inflammation, cervical intraepithelial neoplasia (CIN) I and CIN II
were present. At the 9 and 12 o'clock positions, chronic cervicitis
with focal CIN I and CIN II was diagnosed. Free squamous epithelia
in the cervical canal showed moderate to severe atypical
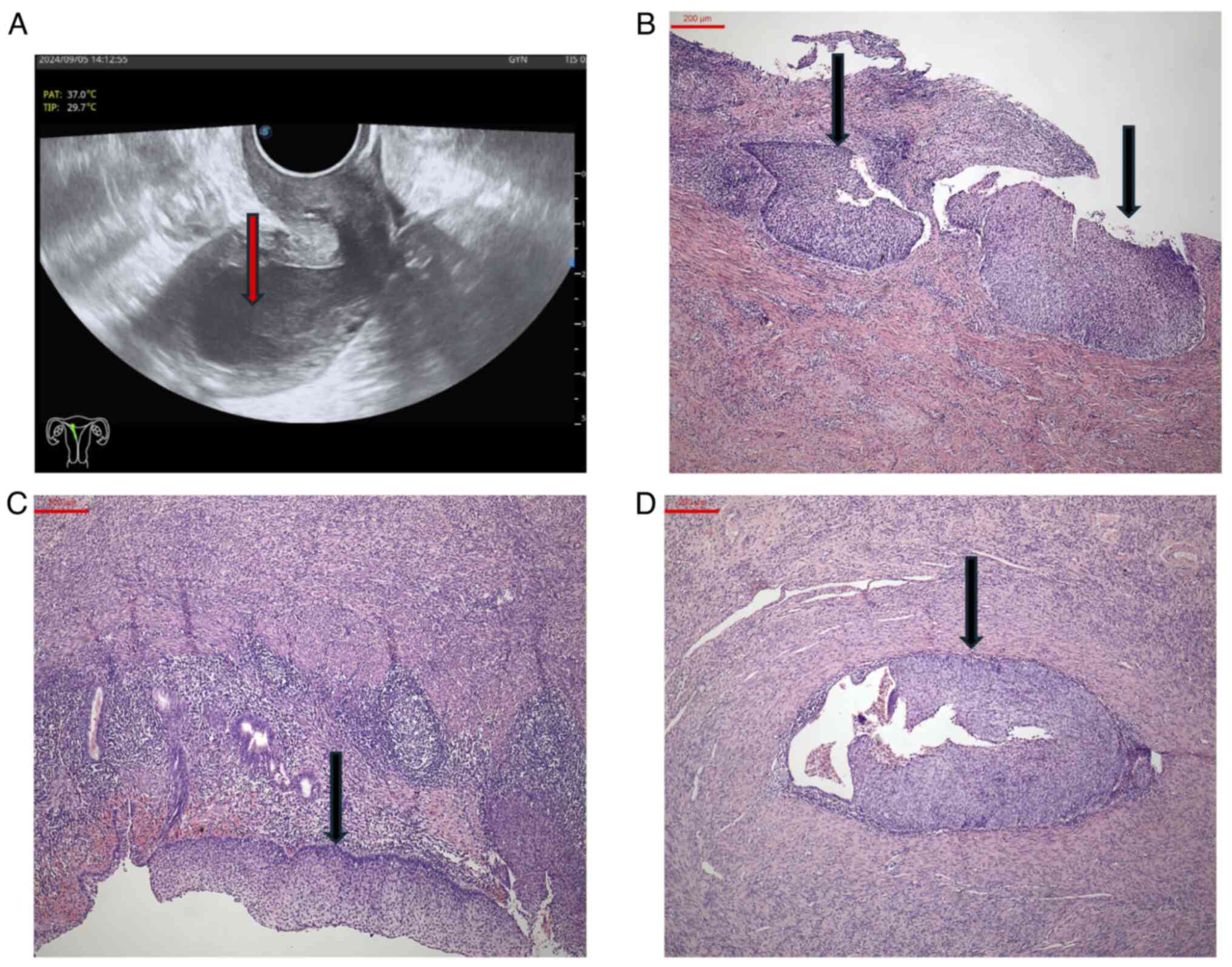
hyperplasia. The B-scan ultrasonography results upon admission
revealed the following (Fig. 1A):
The endometrial monolayer measured ~0.1 cm in thickness, with a
uterine cavity separation of 0.3 cm, within which multiple
flocculent hypoechoic areas were observed, thus indicating pyometra
of the uterine cavity. As the preoperative cervical biopsy did not
indicate invasive carcinoma, no magnetic resonance imaging (MRI)
examination was performed. Subsequently, an experienced professor
of gynecology conducted a triple examination on the patient, and no
parametrial infiltration was palpated. Due to severe cervical
atrophy in the patient, it was not possible to perform a cervical
cone biopsy and instead the patient directly underwent a
laparoscopic total hysterectomy with bilateral
salpingo-oophorectomy. Upon postoperative examination of the
uterus, pyometra was observed in the uterine cavity, but no obvious
masses were seen in the cervix or endometrium. Pathological
examinations were performed on the resected specimens, including
hematoxylin and eosin (H&E) staining and immunohistochemical
(IHC) testing. The uterine and bilateral salpingo-oophorectomy
tissue samples were fixed in 10% neutral-buffered formalin at room
temperature (~22˚C) for 24 h. The fixed tissues were then processed
and embedded in paraffin. Sections were cut at a 4-µm thickness
using a microtome. Conventional H&E staining was performed at
room temperature with hematoxylin for 5 min and eosin for 2 min. As
for IHC testing, the paraffin sections were dewaxed by placing them
in a 67˚C oven for 2 h and then removing the glass. The sections
were dehydrated with graded ethanol (95, 85 and 75%). The antigens
were repaired twice using antigen retrieval solution (0.01M sodium
citrate buffer, pH 6.0) and washed three times with PBS. The
sections were then immunolabeled with anti-p16 (cat. no. MAB-0673;
Fuzhou Maixin Biotechnology Development Co., Ltd.) and anti-Ki-67
(cat. no. RMA-0542; Fuzhou Maixin Biotechnology Development Co.,
Ltd.) antibodies overnight at 4˚C. After thoroughly washing with
PBS, the sections were incubated with secondary antibody (cat. no.
A4416; MilliporeSigma). The staining was visualized using the
peroxide substrate solution diaminobenzidine and counterstaining
with haematoxylin. Observation was conducted under a light
microscope (Olympus BX53; Olympus Corporation). The postoperative
pathological results indicated superficial spreading cervical SCC
in situ (Fig. 1B),
extensively involving the endometrium (Fig. 1C) and the mucosa of the
interstitial portions of both fallopian tubes (Fig. 1D). The carcinoma demonstrated
multiple foci of vertical infiltration in the cervix and uterine
body on the basis of extensive horizontal spread, with infiltration
depths all #x003C;1 mm. No cancer involvement was observed in the
bilateral parametria, bilateral pelvic sidewall resection margins
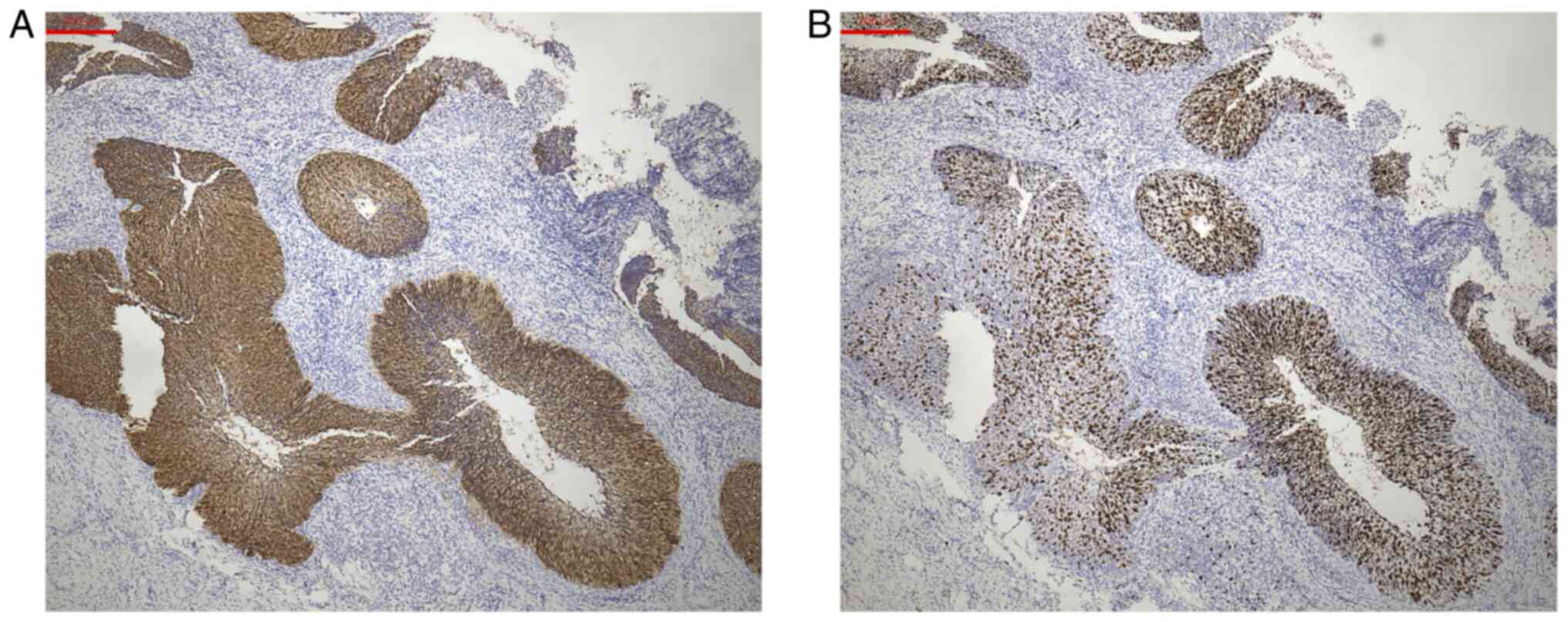
or bilateral ovaries. The immunohistochemistry results demonstrated
p16+++ (Fig. 2A), with Ki-67+
consistent with the range of p16 positivity (Fig. 2B).
The patient began radiotherapy 6 weeks after
surgery, consisting of 6 weeks of external beam pelvic radiotherapy
[with a dosage of clinical target volume (CTV) 1.8 Gy per fraction
for 25 fractions, and gross tumor volume 2.2 Gy per fraction for 25
fractions]. After external beam pelvic radiotherapy, the patient
received two sessions of three-dimensional intracavitary
brachytherapy within 3 days (with a dosage of CTV 6.0 Gy per
fraction for 2 fractions). During the follow-up period extending up
to 10 months after the surgery, the patient had multiple physical
examinations, along with pelvic enhanced MRI and serum SCC antigen
tests, none of which indicated recurrence or metastasis.
Discussion
CC is a common gynecological tumor, with the mode of
metastasis often involving direct extension and lymphatic spread
(5). SCC of the cervix with
superficial spread to the endometrium, fallopian tubes or even
ovaries is relatively rare (6).
Symptoms in elderly patients with cervical lesions are often
atypical. In the present case, the primary symptoms were lower
abdominal pain and pyometra, underscoring that cervical cancer
screening is necessary for elderly women presenting with lower
abdominal pain or pyometra, regardless of whether cervical lesions
are visually detectable.
In 1967, Hallgrímsson (7) first reported a case of SCC in
situ simultaneously affecting the cervix, endometrium and
fallopian tubes; however, the author was unable to determine
whether the lesion originated from the cervix or the endometrium.
In 1969, Salm (8) first proposed
that cervical carcinoma in situ could superficially spread
to the endometrium. A 44-year-old woman underwent a total
hysterectomy due to a preoperative diagnosis of CIN. Postoperative
pathology revealed that the cervical SCC in situ extended
upwards, replacing part of the endometrium. Additionally, part of
the endometrium exhibited a bilayer appearance, with a lower layer
of normal endometrium and an upper layer of SCC in situ.
PubMed (https://pubmed.ncbi.nlm.nih.gov/) was searched for all
reports of superficial spreading cervical SCC published after 1967
and excluded those where the primary cervical lesion was an
invasive cancer, as CC above stage IA1 exhibits significantly
increased lymphatic metastasis rates, potentially spreading to the
endometrium and other organs via lymphatic routes or other
mechanisms (9,10). The case reports with follow-up data
are listed in Table I (11-19),
it was determined that all patients with superficial spreading
cervical SCC were postmenopausal women. The most common symptoms
were pyometra and vaginal discharge, and half of the patients had
undergone conization due to CIN3/carcinoma in situ. All
patients were diagnosed with superficial spreading cervical SCC
postoperatively, and 90% of them did not undergo pelvic lymph node
dissection. None of the cervical lesions showed vascular
infiltration. In the retrieved case series, over one-half of
patients with superficial spreading cervical SCC presented with
pyometra, indicating that cervical conization alone may lead to
underdiagnosis of endometrial lesions in postmenopausal women with
cervical squamous cell carcinoma in situ who exhibit
pyometra or abnormal vaginal discharge. The overall prognosis for
patients with this type of CC was relatively good. Four patients
did not receive additional treatment after surgery and had no
recurrence during the 6-24 months of follow-up; three patients
received supplementary radiotherapy and had no recurrence during
the 12-72 months of follow-up; one patient received supplementary
chemotherapy and had no recurrence after 40 months of follow-up.
For the remaining two patients, it was not mentioned whether they
received supplementary radiotherapy or chemotherapy, but they also
had no recurrence during the 30-54 months of follow-up. Since
radiotherapy is the preferred adjuvant treatment for cervical SCC,
in order to avoid recurrence, adjuvant radiotherapy was
administered in the present case. A recently published article
reported that for intermediate-risk CC, adding chemotherapy to
radiotherapy does not improve overall survival (20); therefore, radiotherapy alone may be
sufficient for such patients. Thus far, after 10 months of
follow-up, there has been no evidence of metastasis or recurrence
for the present patient.
 | Table IReported cases of squamous cell
carcinoma in the literature. |
Table I
Reported cases of squamous cell
carcinoma in the literature.
| First author,
year | Age, years | Clinical
presentation | HPV | Cervical lesion | Extension of
lesion | Adjuvant therapy | Follow-up period,
months | Outcome after
follow-up | (Refs.) |
|---|
| Razquin et al,
1993 | 52 | Cervical stenosis and
pyometra | NA | In situ | Endometrium (in
situ), right fallopian tube (in situ) | Radiotherapy | 72 | Disease free | (11) |
| Pins et al,
1997 | 55 | Abnormal cervical
smear | 16+ | In situ | Endometrium (in
situ), bilateral fallopian tubes (in situ), bilateral
ovaries (invasive) | Radiotherapy | 42 | Disease free | (12) |
| Kushima et al,
2001 | 68 | Excessive vaginal
discharge | NA | In situ | Endometrium
(microinvasive), left fallopian tube (invasive), left ovary
(invasive) | NA | 54 | Disease free | (13) |
| | 72 | Hematometra | NA | In situ | Endometrium (in
situ) | NA | 30 | Disease free | |
| Tan et al,
2004 | 70 | Vaginal
discharge | NA | Microinvasive | Endometrium
(microinvasive) | - | 6 | Disease free | (14) |
| Anthuenis et
al, 2016 | 72 | Distended
abdomen | NA | Microinvasive | Endometrium (in
situ) | - | 24 | Disease free | (15) |
| Nakajima et
al, 2019 | 67 | Pain in the lower
abdomen | + | In situ | Endometrium (in
situ, focal myometrial involvement) bilateral tubes and ovaries
(in situ), omentum (invasive), transverse colon
(invasive) | Chemotherapy | 40 | Disease free | (16) |
| Wang et al,
2021 | 53 | Pyometra | + | In situ | Endometrium (in
situ) | - | 6 | Disease free | (17) |
| Martín-Vallejo et
al, 2022 | 61 | Pyometra and vaginal
discharge | 16+ | Microinvasive | Endometrium (in
situ) | - | 12 | Disease free | (18) |
| Shu et al,
2022 | 57 | Pyometra | 16+ | In situ | Endometrium (in
situ) | Radiotherapy | 12 | Disease free | (19) |
Regarding the etiology of superficial spreading
cervical SCC, Ishida and Okabe (21) analyzed two cases of superficial
spreading CC and found that the intraepithelial component of the
cervical invasive cancer and the endometrial component were
strongly positive for CD138, while the invasive component beyond
the epithelium had minimal expression of CD138, suggesting that
high expression of CD138 may be associated with the direct spread
of SCC to the endometrium. Kushima et al (13) conducted a preliminary analysis of
chromosomal heterogeneity in patients and suggested that
superficial spreading cervical SCC undergo a single clonal process
with frequent loss of heterozygosity on chromosomes 6p, 6q, 11p and
11q. Due to the rarity of cases, the metastatic mechanism of
superficial spreading cervical SCC has not been thoroughly studied
at present.
The upregulation of p16 is typically associated with
HPV infection, whereas high expression of Ki-67 reflects the
proliferative activity of tumors. In the present case, the
expression pattern of p16 was consistent with that of Ki-67,
suggesting that HPV infection may be associated with this type of
CC. It was reported in 1993 by Pins et al (12) that this type of CC may be
associated with HPV infection. More recently, Zhang et al
(22) reported a case of SCC of
the cervix with superficial spread to the endometrium, fallopian
tubes and ovaries, in which all lesions tested positive for HPV.
The association between HPV and endometrial malignancies has been
reported previously; a large-scale observational clinical trial
among Taiwanese women conducted by Wu et al (23) found that HPV infection increases
the incidence of endometrial cancer among women (HR 1.88, 95% CI
1.335-1.888). Darre et al (24) also reported a case of SCC of the
endometrium that was positive for HPV16/18. Jiang et al
(25) reported 15 cases of CC
involving the endometrium, all of which were positive for HPV16.
The findings in the present case suggest that HPV16 may be
associated with superficial spreading CC.
In clinical practice, the staging and treatment of
CC are often based on the International Federation of Gynecology
and Obstetrics (FIGO) staging system, which focuses on the depth of
invasion of the cancer lesion, its size and the local extent of
involvement. For patients with cervical invasive carcinoma where
the lesion has spread to the endometrium, the decision to
administer adjuvant chemoradiotherapy postoperatively can be made
according to the FIGO guidelines or NCCN guidelines (3,26).
However, for patients whose cervix shows only carcinoma in
situ or microinvasive carcinoma with the lesion extending to
the endometrium, there are currently no corresponding guidelines
available. Nakajima et al (16) reported a case of a patient with
cervical carcinoma in situ, in which the tumor superficially
disseminated to the endometrium, the surfaces of both fallopian
tubes, both ovaries, transverse colon and implanted on the greater
omentum, forming an invasive carcinoma. After undergoing a radical
hysterectomy, bilateral salpingo-oophorectomy, omentectomy and
transverse colectomy, the patient received six cycles of
chemotherapy with paclitaxel and carboplatin. Following a 40-month
follow-up period the patient showed no signs of recurrence. This
report indicates that supplementary chemotherapy may be beneficial
to the prognosis of CC with superficial dissemination to the
ovaries. Nevertheless, due to the scarcity of cases, large-scale
controlled trials cannot be conducted, and it remains uncertain
whether postoperative adjuvant chemoradiotherapy is beneficial for
prognosis.
In conclusion, superficial spreading SCC of the
cervix currently lacks standardized diagnostic and treatment
methods. It was the aim of the present report to highlight that for
elderly patients with pyometra whose cervical cytology only
indicates CIN and does not suggest cervical invasive carcinoma,
merely administering anti-infective treatment or performing a
cervical conization might lead to a missed diagnosis of superficial
spreading cervical SCC. For such patients, fractional curettage
should minimally be performed concurrent with cervical conization.
Due to the limited number of cases, conducting molecular or
histopathological studies at present would not yield statistically
significant results; therefore, more cases of superficial spreading
cervical SCC should be collected to investigate the molecular
mechanisms underlying its pathogenesis, particularly the role of
specific HPV genotypes in its development. Additionally, these
patients should be followed up over a prolonged period to assess
their prognosis and explore whether adjuvant chemoradiotherapy is
beneficial for improving outcomes.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
XH conceived the case report. SS and HZ collected
and analyzed the data. SS and HZ wrote and revised the manuscript.
XH and SS confirm the authenticity of all the raw data. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was provided by the patient
for the case report to be published.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Global Burden of Disease Cancer
Collaboration. Fitzmaurice C, Akinyemiju TF, Al Lami FH, Alam T,
Alizadeh-Navaei R, Allen C, Alsharif U, Alvis-Guzman N, Amini E, et
al: Global, regional, and national cancer incidence, mortality,
years of life lost, years lived with disability, and
disability-adjusted life-years for 29 cancer groups, 1990 to 2016:
A systematic analysis for the global burden of disease study. JAMA
Oncol. 4:1553–1568. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Martin-Hirsch PP, Paraskevaidis E, Bryant
A, Dickinson HO and Keep SL: Surgery for cervical intraepithelial
neoplasia. Cochrane Database Syst Rev: CD001318, 2010.
|
|
3
|
National Comprehensive Cancer Network
(NCCN): NCCN Clinical Practice Guidelines in Oncology: Cervical
Cancer (Version 1.2025). NCCN, Plymouth Meeting, PA, 2024.
|
|
4
|
Siegel RL, Miller KD, Fuchs HE and Jemal
A: Cancer statistics, 2021. CA Cancer J Clin. 71:7–33.
2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Lifshitz SG and Buchsbaum HJ: Spread of
cervical carcinoma. Obstet Gynecol Annu. 6:341–354. 1977.PubMed/NCBI
|
|
6
|
Rangankar V, Bokil S and Deshmukh S:
Superficial spread of nonkeratinizing squamous cell carcinoma of
the cervix to the endometrium: A case report. Cureus.
16(e63931)2024.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Hallgrímsson JT: Carcinoma in situ of the
endocervix, corpus uteri and both oviducts. Acta Obstet Gynecol
Scand. 46:268–272. 1967.PubMed/NCBI
|
|
8
|
Salm R: Superficial intra-uterine spread
of intra-epithelial cervical carcinoma. J Pathol. 97:719–723.
1969.PubMed/NCBI View Article : Google Scholar
|
|
9
|
van Meurs H, Visser O, Buist MR, Ten Kate
FJW and van der Velden J: Frequency of pelvic lymph node metastases
and parametrial involvement in stage IA2 cervical cancer: A
population-based study and literature review. Int J Gynecol Cancer.
19:21–26. 2009.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Costa S, Marra E, Martinelli GN, Santini
D, Casadio P, Formelli G, Pelusi C, Ghi T, Syrjänen K and Pelusi G:
Outcome of conservatively treated microinvasive squamous cell
carcinoma of the uterine cervix during a 10-year follow-up. Int J
Gynecol Cancer. 19:33–38. 2009.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Razquin S, Mayayo E, Antón E and Alvira R:
Squamous cell carcinoma in situ of the endometrium as superficial
extension of cervical carcinoma. Gynecol Obstet Invest.
35:190–1902. 1993.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Pins MR, Young RH, Crum CP, Leach IH and
Scully RE: Cervical squamous cell carcinoma in situ with
intraepithelial extension to the upper genital tract and invasion
of tubes and ovaries: Report of a case with human papilloma virus
analysis. Int J Gynecol Pathol. 16:272–278. 1997.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Kushima M, Fujii H, Murakami K, Ota H,
Matsumoto T, Motoyama T, Kiyokawa T and Ishikura H: Simultaneous
squamous cell carcinomas of the uterine cervix and upper genital
tract: Loss of heterozygosity analysis demonstrates clonal
neoplasms of cervical origin. Int J Gynecol Pathol. 20:353–358.
2001.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Tan GC, Isa MR, Ng SP and Jamil YMA:
Unusual form of superficial spreading microinvasive squamous cell
carcinoma of uterine cervix involving the endometrium of uterus. J
Obstet Gynaecol Res. 30:363–367. 2004.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Anthuenis J, Baekelandt J, Bourgain C and
De Rop C: Squamous cell carcinoma in situ lining the uterine
cavity. Eur J Gynaecol Oncol. 37:135–138. 2016.PubMed/NCBI
|
|
16
|
Nakajima T, Hatta H, Nishida T, Minamisaka
T, Miwa S, Terahata S and Imura J: Superficial spread of cervical
squamous cell carcinoma to the upper genital tract and
dissemination to the omentum. Pathol Int. 69:119–121.
2019.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Wang W and Zhou F: Cervical HSIL involving
the endometrium and adenomyosis: A case report and literature
review. J Coll Physicians Surg Pak. 31:337–339. 2021.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Martín-Vallejo J, Laforga JB,
Molina-Bellido P and Clemente-Pérez PA: Superficial spreading
cervical squamous cell carcinoma in situ involving the endometrium:
A case report and review of the literature. J Med Case Rep.
16(196)2022.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Shu XY, Dai Z, Zhang S, Yang HX and Bi H:
Endometrial squamous cell carcinoma originating from the cervix: A
case report. World J Clin Cases. 10:8782–8787. 2022.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Agusti N, Viveros-Carreño D, Wu CF, Wilke
RN, Kanbergs A, Barajas K, Zamorano AS, Pareja R, Melamed A and
Rauh-Hain JA: Adjuvant chemoradiotherapy vs radiotherapy alone for
patients with intermediate-risk cervical cancer. JAMA Oncol.
11:511–518. 2025.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Ishida M and Okabe H: Superficial
spreading squamous cell carcinoma of the uterine cervix involving
the endometrium: Report of two cases with emphasis on the likely
molecular mechanism. Oncol Lett. 5:31–34. 2013.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Zhang Y, Zhang X, Wang H and Shen D: Stage
IA1 HPV-associated cervical squamous cell carcinoma metastasizing
to ovary by special pathway: A case report and literature review. J
Ovarian Res. 15(21)2022.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Wu PJ, Tsai SCS, Huang JY, Lee MS, Wang PH
and Lin FCF: From infection to malignancy: Tracing the impact of
human papillomavirus on uterine endometrial cancer in a nationwide
population-based cohort study. Viruses. 15(2314)2023.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Darré T, Aboubakari AS, Sonhaye L,
Douaguibe B, Bassowa A and Napo-Koura G: Primary squamous cell
carcinoma of the endometrium associated with human papilloma virus
in a young woman: A case report. J Med Case Rep.
13(167)2019.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Jiang X, Han Z, Chun Z, Wen B and Chen T:
An unusual pattern of endometrial involvement: Superficial
spreading squamous cell carcinoma of the cervix. Front Oncol.
14(1456297)2024.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Bhatla N and Denny L: FIGO cancer report
2018. Int J Gynaecol Obstet. 143 (Suppl 2):S2–S3. 2018.PubMed/NCBI View Article : Google Scholar
|