Introduction
Adrenal myelolipoma (AML) is a rare,
non-functioning, benign tumor originating from adrenal tissue.
Composed primarily of mature adipose and hematopoietic tissue, it
was first described by Gierke in 1905 (1,2).
AMLs are usually asymptomatic due to their benign nature and lack
of hormonal activity, unless they grow large enough to compress
surrounding structures or cause spontaneous hemorrhage. Symptoms,
when present, may include nonspecific abdominal or flank pain,
hypertension, nausea, vomiting or hematuria (3). AMLs are most commonly detected
incidentally during imaging for unrelated conditions or routine
health checkups. Giant AMLs are uncommon in clinical practice and
bilateral cases are exceptionally rare, often presenting
significant therapeutic challenges because of the large tumor size,
increased risk of hemorrhage and complex anatomical relationships
with adjacent organs (4). At
present, treatment options for AMLs primarily include observation
or surgical intervention. While open adrenalectomy remains the gold
standard for giant AMLs, laparoscopic techniques have been
increasingly adopted for unilateral cases. However, there is a
paucity of literature on the laparoscopic management of bilateral
giant AMLs. The present study reported on a rare case of bilateral
giant AML resected via transabdominal and retroperitoneal
laparoscopic adrenalectomy, offering clinical insights into
surgical strategy and approach selection.
Case report
A 60-year-old man with no clinical symptoms was
referred to Zhejiang Provincial Hospital of Chinese Medicine
(Hangzhou, China) in July 2022, after bilateral adrenal masses were
detected incidentally on B-ultrasound examination. The patient had
a 2-year history of hypertension (up to 170/110 mmHg) but was not
on any regular antihypertensive therapy. Physical examination on
first admission revealed normal vital signs, with no palpable
abdominal wall mass or tenderness, and no relevant family history
of genetic diseases. Laboratory tests, including adrenal hormones
(catecholamines, aldosterone, adrenocorticotropic hormone, etc.),
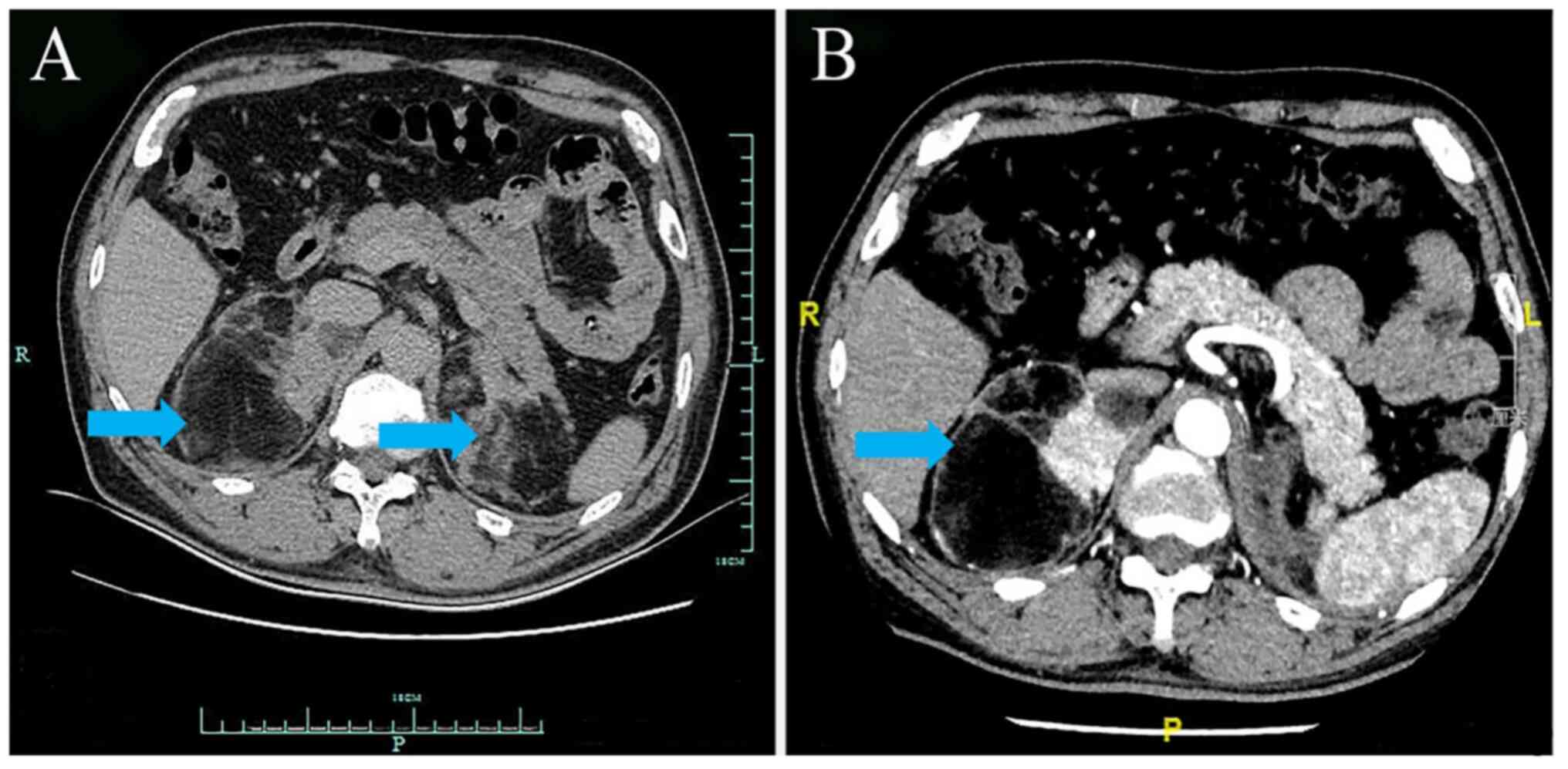
were within normal limits. Adrenal contrast-enhanced computed
tomography (CT) revealed bilateral giant adrenal masses-100x87x63
mm on the right and 75x52x33 mm on the left-with smooth margins and
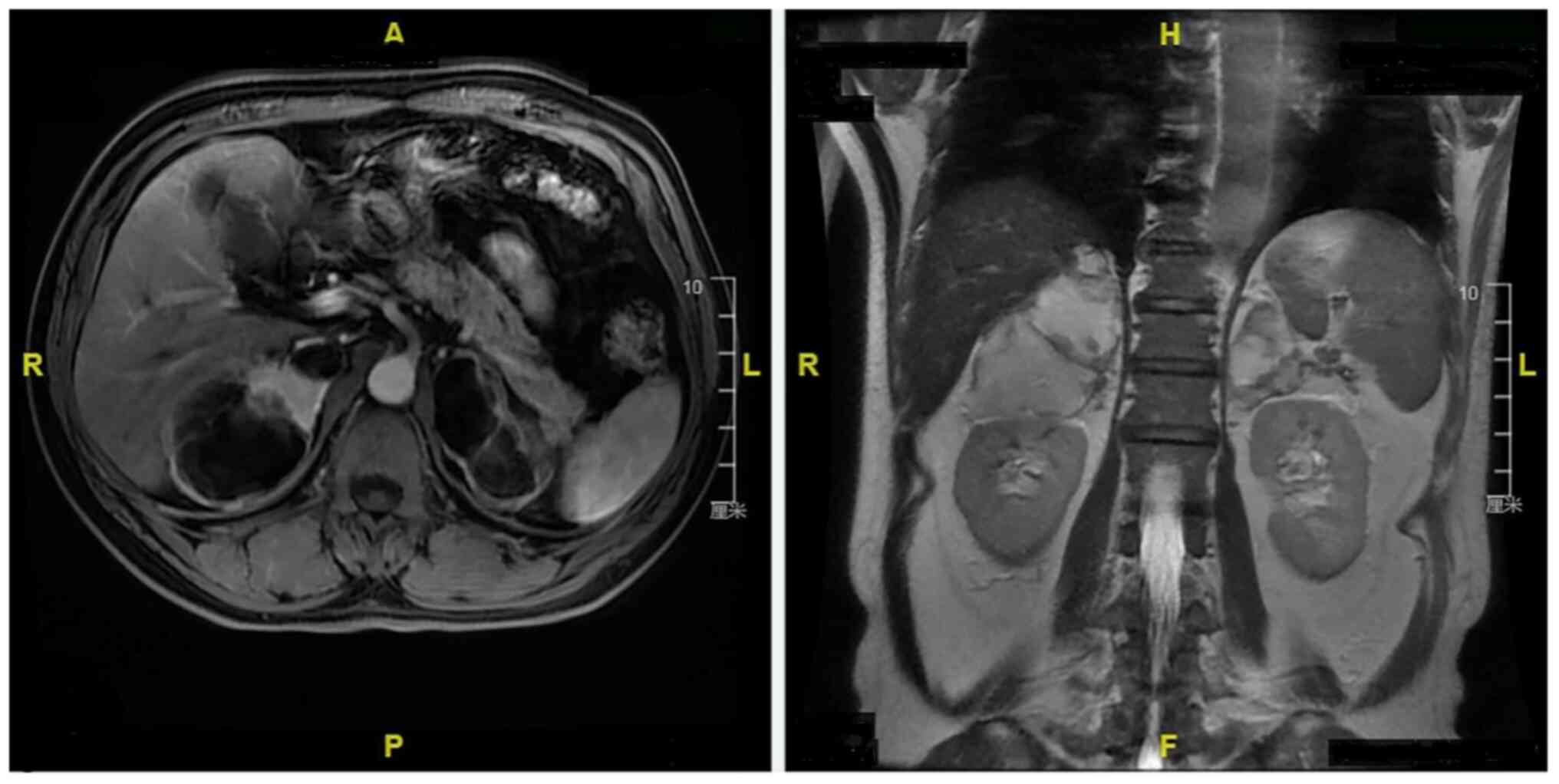
heterogeneous density (-35 to 44 HU) (Fig. 1). Adrenal contrast-enhanced
magnetic resonance imaging (MRI) further confirmed the CT findings
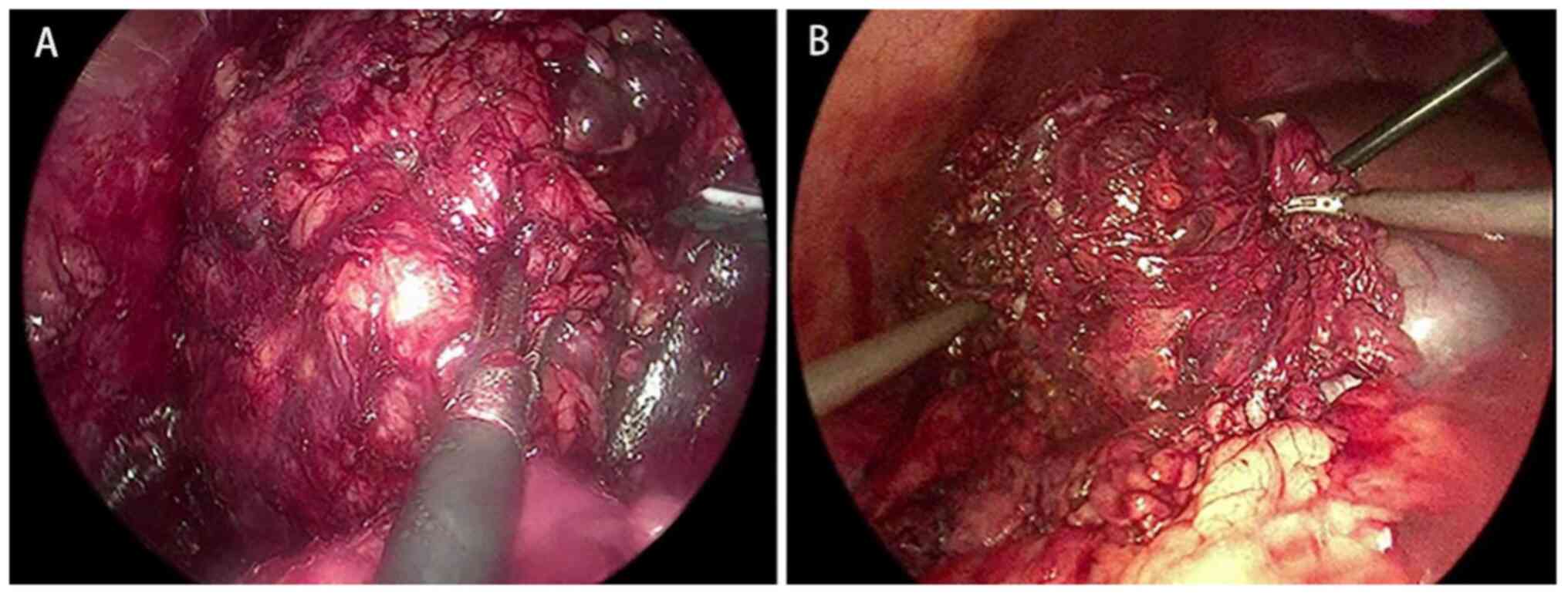
(Fig. 2). The patient first
underwent retroperitoneal laparoscopic left adrenalectomy (Fig. 3A), followed by transperitoneal
laparoscopic right adrenalectomy 1 month later (Fig. 3B). Due to liver and intestinal
interference, two additional optical trocars were inserted during
the right-side transperitoneal approach. The operation time for the
two operations was 110 min (left) and 85 min (right), and estimated
blood loss was 170 ml (left) and 150 ml (right). The two operations
in succession were completed with no perioperative complications.
Prophylactic steroid replacement therapy was administered after the
second surgery, consisting of intravenous hydrocortisone 200 mg/day
for 48 h, followed by tapering and transition to long-term oral
maintenance therapy with hydrocortisone 20 mg/day and
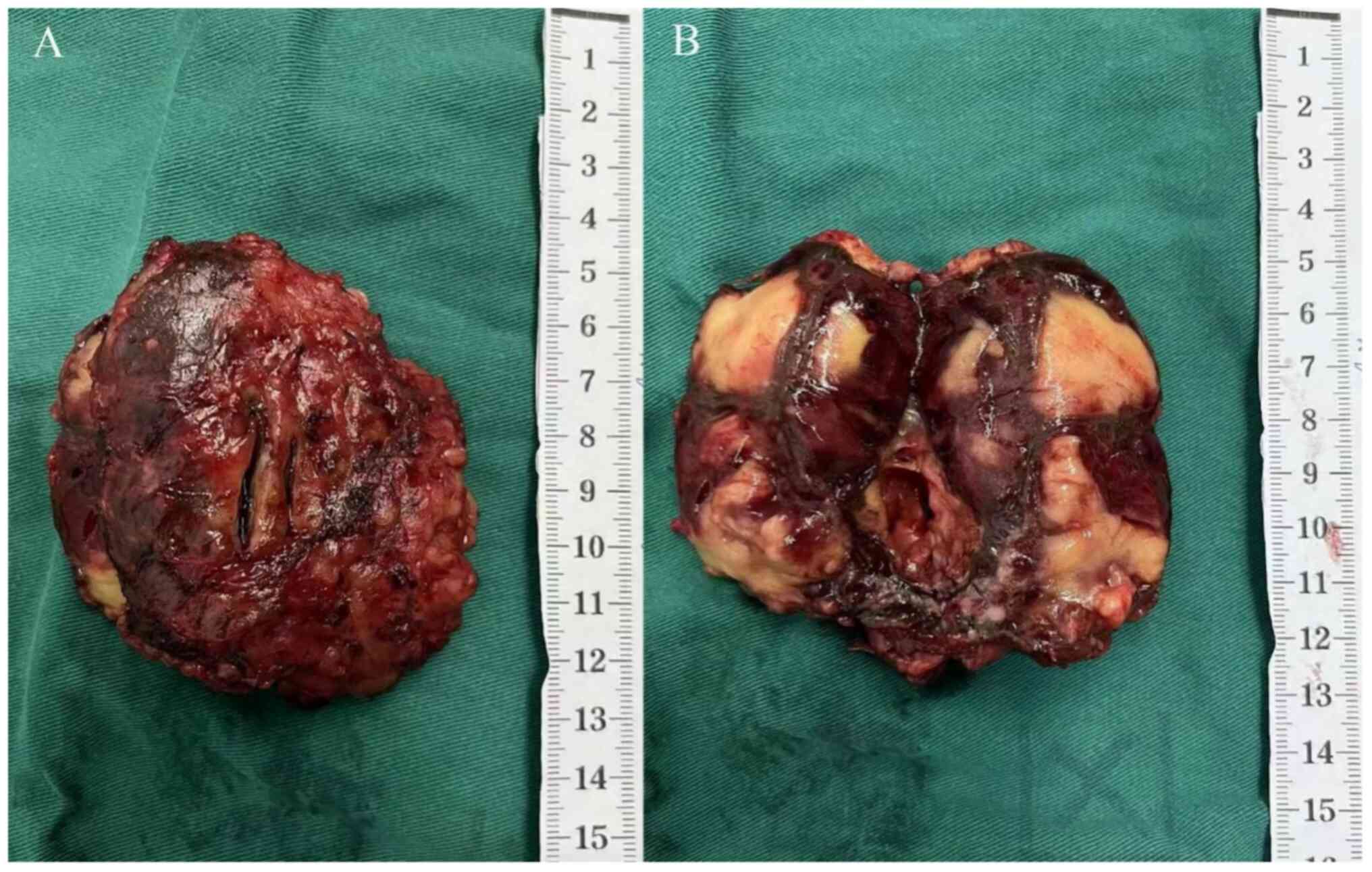
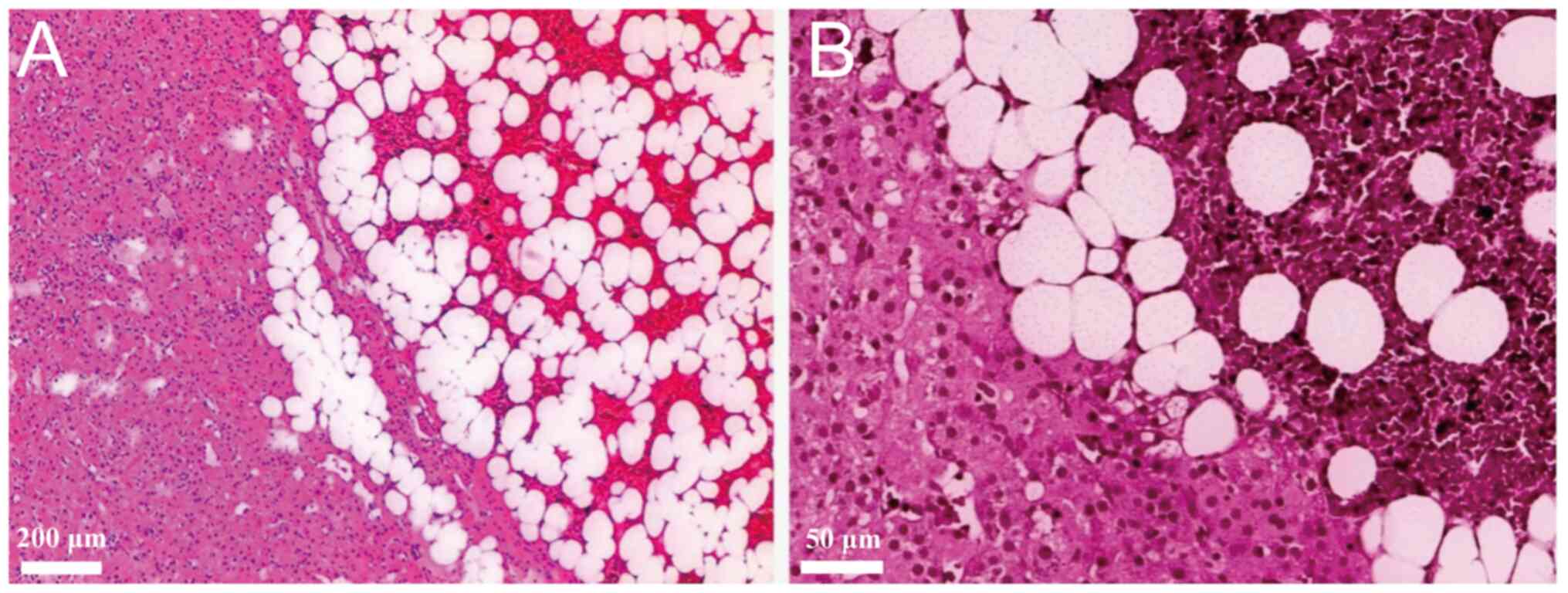
fludrocortisone 0.1 mg/day. Gross examination revealed
well-encapsulated masses composed of yellow adipose and brown
hematopoietic tissue (Figs. 4A and
B and 5). Postoperative histopathology (H&E
staining) performed according to standard procedures confirmed AML
in both adrenal glands (Fig. 6).
At the 3- and 6-month follow-ups, no signs of recurrence were
observed via ultrasound and the patient recovered well and remained
symptom-free over a 3-year postoperative period.
Discussion
AML is a rare, benign, hormonally inactive adrenal
tumor, accounting for 3.3-6.5% of all adrenal masses (1). Approximately 85-90% of AMLs are
detected incidentally (5,6). While AMLs are typically unilateral,
~12% are bilateral (7). According
to statistics, AMLs are three times more common on the right
adrenal gland than on the left (3). A long-term longitudinal follow-up
study suggested that larger AMLs (>6 cm) are more often
associated with bilateral involvement (6). The prevalence of AML has been
reported to be 0.24% in patients undergoing CT (8), and ~0.32% in the general population
at around 40 years of age (9),
whereas patients with congenital adrenal hyperplasia (CAH)
demonstrate a much higher rate (10.1%) (9). Additionally, bilateral or giant AMLs
are more frequently observed in patients with CAH (10) and may even serve as an early sign
of CAH (7). In a recent
epidemiological survey, AML was detected in 4-10% of patients with
adrenalectomy (9). Diagnosis of
benign adrenal tumors, such as AML, is gradually becoming more
accurate. Certain scholars have reported cases of adrenalectomy due
to misdiagnosis (11). In most
histopathological reports, the pathological features of bilateral
AMLs are the same (7,12,13).
Yet, the possibility of varying histopathological types of AML in
the left and right adrenal glands cannot be clinically excluded to
reduce the probability of misdiagnosis. The present case is a
bilateral AML with the same pathological type without abnormal and
correlated laboratory indicators and a disease history of CAH.
AML usually results from the differentiation of
adrenal medulla or cortical cells into adipose tissue and
extramedullary hematopoietic tissue. Chronic stress, infection,
tissue ischemia, necrosis, trauma and fat metabolism disorders are
known to cause this disease (14,15).
Studies have suggested links between the adrenocorticotropic
hormone, erythropoietin and AML development (6,9).
Scholars have discovered the first AML-associated somatic genetic
aberration in the early stage, balanced translocation between
chromosomes 3q25 and 21p11, thus offering the earliest genetic
evidence for tumor origin (16).
Later, cytogenetic studies found that AML is a clonal tumor based
on non-random X chromosome inactivation; such inactivation in
hematopoietic cells and adipocytes may be of clonal origin
(17). Hypotheses regarding AML
pathogenesis are as follows: i) AML may be caused by an ectopic
proliferation of bone marrow cells in the embryonic adrenal gland.
It may originate from fetal bone marrow residues, bone marrow cell
embolism and ectopic reticulocyte proliferation (11); ii) adipocytes develop from
mesenchymal stem cells in the endothelium (18); iii) microRNA profiles unique to AML
have been determined, distinguishing it from other adrenocortical
tumors (19); and iv) scholars
have found a non-pathogenic ARMC5 allelic variation in a patient
with AML with a co-existing adrenal cortical adenoma. However,
ARMC5 mutation is typically associated with the pathogenesis of
primary bilateral macronodular hyperplasia and its correlation with
myelolipoma or mixed tumors remains unelucidated (11). Bilateral AMLs may involve more
complex pathogenic mechanisms than unilateral ones.
In recent years, the AML detection rate has
significantly increased, largely due to the widespread use and
advancement of imaging modalities such as B-ultrasound and CT.
B-ultrasound, being non-invasive and radiation-free, is ideal for
initial screening and follow-up monitoring of AML. However, CT
remains the most accurate tool for identifying and characterizing
AML, with its hallmark features being low-density fat and iso- to
hyperdense marrow-like components (20). On CT, AML typically appears as a
round or ovoid mass with a well-defined margin in the adrenal
region. The tumor was demonstrated to have heterogeneous density,
containing areas of mature fat (CT value <-30 HU) interspersed
with fine reticular, cord-like or lamellar hematopoietic tissue of
slightly higher density (21).
Multiplanar CT reconstruction is particularly valuable in
localizing lesions and evaluating their relationship with adjacent
structures such as the liver and kidneys. On unenhanced MRI, AMLs
with a high fat content show high signal intensity on both T1- and
T2-weighted images (21).
Post-contrast MRI typically shows no significant signal change due
to the fat-rich nature of the tumor. The drop in the fat
suppression sequence signal is characteristic of this disease and
aids in diagnosis. MRI is able to more accurately display cystic
changes in the tumor. Due to its multiplanar capabilities, MRI
serves as a useful complement to CT in assessing tumor location and
its spatial relationships with nearby organs, particularly in
retroperitoneal lesions (22).
When AMLs are large, intratumoral hemorrhage may occur and CT is
particularly sensitive for detecting such bleeding events (23). CT is also more effective than other
modalities in revealing the presence of bone marrow tissue and
calcifications within the mass (24). Despite the utility of imaging,
preoperative fine-needle aspiration or biopsy guided by ultrasound
or CT is not generally recommended due to its invasiveness and
associated risks, including tumor rupture, bleeding, infection or
tumor implantation. It is therefore not recommended for widespread
use. Therefore, the gold standard for AML diagnosis remains
postoperative histopathological examination.
Historically, AMLs larger than 6 cm in diameter were
considered contraindications for laparoscopic surgery and managed
with open adrenalectomy (25).
However, with the advancement of endoscopic equipment and the
refinement of laparoscopic and robotic surgical techniques,
minimally invasive approaches have increasingly replaced open
surgery even in large tumors (26-28).
Growing experience and technological improvements have expanded the
indications for laparoscopic management. Several studies have
demonstrated the safety and feasibility of laparoscopic resection
in giant AMLs (29). Laparoscopic
adrenalectomy can be performed via transperitoneal or
retroperitoneal approaches. The transperitoneal approach is often
preferred for larger tumors requiring extensive exposure,
particularly in obese patients or when tumors are located near
critical structures such as the inferior vena cava, liver or other
abdominal organs (30). This
approach provides superior visualization and operative space,
enabling safe, precise tumor resection while minimizing damage to
vital vessels and organs, thereby reducing the risk of
intraoperative and postoperative complications (31). By contrast, the retroperitoneal
approach offers easier and direct access to the adrenal glands
without transgressing the peritoneal cavity. This minimizes
interference from intra-abdominal organs and facilitates quicker
postoperative bowel function recovery and shorter hospital stays.
Because it avoids major vascular structures and organs, this
approach is generally associated with reduced intraoperative
bleeding, shorter operative time and lower rates of postoperative
complications such as postoperative adhesions and infections
(32). Our clinical experience
also suggests that the retroperitoneal approach typically requires
fewer trocars, further contributing to faster postoperative
recovery. This approach is particularly suitable for relatively
small tumors in favorable anatomical positions or in patients with
a history of prior abdominal surgeries. A review of the literature
shows that most unilateral AMLs are managed via laparoscopic
adrenalectomy-predominantly through the transperitoneal approach,
although the retroperitoneal route has also been successfully
employed in selected cases (32).
Bilateral AML is rare. When clinically appropriate, surgeons
typically prioritize resection of the larger or symptomatic mass
first, preserving the contralateral adrenal gland to maintain
adrenal function, with periodic monitoring of the remaining lesion
(33). The surgical strategy for
unilateral resection in bilateral AML cases is similar to that for
unilateral AML. However, when AML tumors are extensively adherent
to major vessels or organs, when imaging or intraoperative findings
raise suspicion of malignancy, or in cases of tumor rupture with
acute hemorrhage, open surgery remains the recommended safer option
for both unilateral and bilateral cases (14). Furthermore, in rare instances of
bilateral giant AML where both tumors are large or high-risk,
existing case reports predominantly describe bilateral
adrenalectomy performed via transperitoneal laparoscopy or open
surgery, with no cases performed via a retroperitoneal approach,
and these patients require lifelong steroid replacement therapy
postoperatively (34-36).
No prior reports have documented bilateral adrenalectomy using both
laparoscopic approaches (retroperitoneal and transperitoneal) in
the same patient. Furthermore, comparative data between these two
laparoscopic methods in the context of giant AML are currently
lacking, to the best of our knowledge. In this case, after thorough
preoperative evaluation, both retroperitoneal and transperitoneal
laparoscopic approaches were employed in the same patient to resect
bilateral giant AMLs. The perioperative data for both surgical
approaches were also summarized in Table SI/Appendix. Consistent with existing
literature, laparoscopic adrenalectomy was associated with several
advantages, including reduced blood loss, less postoperative pain,
low complication rates, faster recovery and shorter hospital stays
(37,38). The present findings confirmed these
benefits in both procedures. Based on perioperative comparisons and
clinical experience at our hospital, it may be suggested that the
retroperitoneal approach may offer certain advantages in selected
cases. Although this report of a single case and lacks sufficient
credibility with extensive data and a large sample size, it
contributes valuable clinical insight into the surgical management
of rare bilateral giant AMLs.
Furthermore, several factors may be considered to be
crucial for achieving optimal outcomes in the laparoscopic
resection of giant AMLs. First, during perioperative management,
blood pressure, heart rate, serum potassium and adrenal hormone
levels should be routinely monitored to detect and prevent
potential functional lesions. Second, because AMLs often have a
delicate capsule, dissection should be carried out carefully along
the extracapsular plane to preserve its integrity, thereby reducing
the risk of rupture that could obscure the operative field. Leaving
a thin layer of pericapsular fatty connective tissue may further
minimize the chance of capsule disruption caused by direct
traction. Third, when the tumor is situated on the right side and
lies close to the inferior vena cava, the surgeon must have a
detailed understanding of the local anatomy and proceed with
particular caution to avoid vascular injury. Finally, in bilateral
AML resections, the risk of adrenal crisis is greater than in
unilateral cases, making postoperative prophylactic hormone
replacement therapy advisable.
The present case demonstrates that both
retroperitoneal and transperitoneal laparoscopic approaches are
safe and effective for the resection of giant AMLs. The
retroperitoneal approach may offer advantages in selected cases,
particularly when tumor location and size are favorable.
Ultimately, the choice of surgical approach should be based on
tumor size, location, relationship with surrounding organs, and the
surgeon's experience and expertise.
Supplementary Material
Evaluation Scores of the surgical
approach by the attending surgeon.
Comparison of the two surgical
approaches
Acknowledgements
Not applicable.
Funding
Funding: This study was supported by the 2025 Provincial Medical
and Health Technology Program of Zhejiang Province (grant no.
2025KY967).
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
XL and JY were the patient's attending physicians.
JY performed the surgery. JW, WZ, YC and JL were involved in the
collection of clinical and imaging data, preliminary analysis and
figure preparation, and contributed to drafting the original
version of the manuscript. YL was responsible for long-term patient
follow-up and contributed to critical revision and editing of the
manuscript. JW and JY confirm the authenticity of all the raw data.
All authors have read and approved the final manuscript for
submission.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report and any accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Calissendorff J, Juhlin CC, Sundin A,
Bancos I and Falhammar H: Adrenal myelolipomas. Lancet Diabetes
Endocrinol. 9:767–775. 2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Gierke E: Über Knochenmarksgewebe in der
Nebenniere. Zeiglers Beitr Pathol Anat. 7 (Suppl 1):S311–S324.
1905.
|
|
3
|
Decmann Á, Perge P, Tóth M and Igaz P:
Adrenal myelolipoma: A comprehensive review. Endocrine. 59:7–15.
2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Yang Q, Zhu Q, You Y, Li M and Zhang K:
Incidentally findings of bilateral giant adrenal myelolipoma: Case
report. Int J Surg Case Rep. 122(110045)2024.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Ebbehoj A, Li D, Kaur RJ, Zhang C, Singh
S, Li T, Atkinson E, Achenbach S, Khosla S, Arlt W, et al:
Epidemiology of adrenal tumours in Olmsted County, Minnesota, USA:
A population-based cohort study. Lancet Diabetes Endocrinol.
8:894–902. 2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Hamidi O, Raman R, Lazik N, Iniguez-Ariza
N, McKenzie TJ, Lyden ML, Thompson GB, Dy BM, Young WF Jr and
Bancos I: Clinical course of adrenal myelolipoma: A long-term
longitudinal follow-up study. Clin Endocrinol (Oxf). 93:11–18.
2020.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Gupta P, Mondal S, Datta C and Pal DK:
Bilateral giant adrenal myelolipoma: A rare scenario. Indian J
Pathol Microbiol. 65:689–691. 2022.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Campbell MJ, Obasi M, Wu B, Corwin MT and
Fananapazir G: The radiographically diagnosed adrenal myelolipoma:
What do we really know? Endocrine. 58:289–294. 2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Nermoen I and Falhammar H: Prevalence and
characteristics of adrenal tumors and myelolipomas in congenital
adrenal hyperplasia: A systematic review and meta-analysis. Endocr
Pract. 26:1351–1365. 2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Aveiro-Lavrador M, De Sousa Lages A,
Barros L and Paiva I: Late diagnosis of classic congenital adrenal
hyperplasia: Long-term consequences during adulthood. Endocrinol
Diabetes Metab Case Rep. 2021:21–0032. 2021.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Naser N, Nava V, Khosla S and Nylen E:
Allelic variant of armadillo repeat containing protein 5 (ARMC5) in
myelolipoma mimicking pheochromocytoma: A case report. Cureus.
15(e34454)2023.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Posses SP, Prado BC, Bechara GR, Puppim
AR, Carli CRS and Miranda MML: Giant bilateral adrenal myelolipoma:
Case presentation and a brief literature review. Urol Case Rep.
18:67–69. 2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Piskinpasa H, Ciftci Dogansen S, Kusku
Cabuk F, Guzey D, Sahbaz NA, Akdeniz YS and Mert M: Bilateral
adrenal and testicular mass in a patient with congenital adrenal
hyperplasia. Acta Endocrinol (Buchar). 5:113–117. 2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Shenoy VG, Thota A, Shankar R and Desai
MG: Adrenal myelolipoma: Controversies in its management. Indian J
Urol. 31:94–101. 2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Cochetti G, Paladini A, Boni A, Silvi E,
Tiezzi A, De Vermandois JAR and Mearini E: Robotic treatment of
giant adrenal myelolipoma: A case report and review of the
literature. Mol Clin Oncol. 10:492–496. 2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Chang KC, Chen PI, Huang ZH, Lin YM and
Kuo PL: Adrenal myelolipoma with translocation (3;21)(q25;p11).
Cancer Genet Cytogenet. 134:77–80. 2002.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Yildiz L, Akpolat I, Erzurumlu K, Aydin O
and Kandemir B: Giant adrenal myelolipoma: Case report and review
of the literature. Pathol Int. 50:502–504. 2000.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Bokhari MR, Zulfiqar H, Leslie SW and
Garla VV: Adrenal myelolipoma. In: StatPearls. StatPearls
Publishing LLC, Treasure Island, FL, 2025.
|
|
19
|
Decmann A, Perge P, Nyíro G, Darvasi O,
Likó I, Borka K, Micsik T, Tóth Z, Bancos I, Pezzani R, et al:
MicroRNA expression profiling in adrenal myelolipoma. J Clin
Endocrinol Metab. 103:3522–3530. 2018.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Wale DJ, Wong KK, Viglianti BL, Rubello D
and Gross MD: Contemporary imaging of incidentally discovered
adrenal masses. Biomed Pharmacother. 87:256–262. 2017.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Cyran KM, Kenney PJ, Memel DS and Yacoub
I: Adrenal myelolipoma. AJR Am J Roentgenol. 166:395–400.
1996.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Krebs TL and Wagner BJ: MR imaging of the
adrenal gland: Radiologic-pathologic correlation. Radiographics.
18:1425–1440. 1998.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Emekli E and Gündoğdu E: Computed
tomography findings in wunderlich syndrome. Hong Kong J Radiol.
25:136–142. 2022.
|
|
24
|
Kenney PJ, Wagner BJ, Rao P and Heffess
CS: Myelolipoma: CT and pathologic features. Radiology. 208:87–95.
1998.PubMed/NCBI View Article : Google Scholar
|
|
25
|
MacGillivray DC, Shichman SJ, Ferrer FA
and Malchoff CD: A comparison of open vs laparoscopic
adrenalectomy. Surg Endosc. 10:987–990. 1996.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Katsimantas A, Filippou D, Melloy A,
Paparidis S and Ferakis N: Macroscopic appearance of giant adrenal
myelolipoma during laparoscopy: An adjunct in differential
diagnosis. Cureus. 12(e6582)2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Tinozzi FP, Morone G, Calì B, Rebba A,
Osman N, Albertario S, Abbiati F and Ruggiero R: Laparoscopic
adrenalectomy for a giant adrenal myelolipoma: A case report. Int J
Surg Case Rep. 90(106678)2022.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Dogrul AB, Cennet O and Dincer AH:
Minimally invasive techniques in benign and malignant adrenal
tumors. World J Clin Cases. 10:12812–12821. 2022.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Vemula BR, Olajide OB and Adepoju Y:
Bilateral adrenal myelolipomas in a female patient with undiagnosed
non-classic congenital adrenal hyperplasia. Cureus.
15(e35017)2023.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Kermansaravi M, Masoudpour H, Nikeghbalian
S and Ghaffaripour S: Successful laparoscopic right adrenalectomy
in a morbidly obese patient with a large liver: A case report. Int
J Clin Med. 6:589–593. 2015.
|
|
31
|
Mohammadi-Fallah MR, Mehdizadeh A,
Badalzadeh A, Izadseresht B, Dadkhah N, Barbod A, Babaie M and
Hamedanchi S: Comparison of transperitoneal versus retroperitoneal
laparoscopic adrenalectomy in a prospective randomized study. J
Laparoendosc Adv Surg Tech A. 23:362–366. 2013.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Arezzo A, Bullano A, Cochetti G, Cirocchi
R, Randolph J, Mearini E, Evangelista A, Ciccone G, Bonjer HJ and
Morino M: Transperitoneal versus retroperitoneal laparoscopic
adrenalectomy for adrenal tumours in adults. Cochrane Database Syst
Rev. 12(Cd011668)2018.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Zattoni D, Balzarotti R and Rosso R: The
management of bilateral myelolipoma: Case report and review of the
literature. Int J Surg Case Rep. 12:31–36. 2015.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Yang Y, Ye LY, Yu B, Guo JX, Liu Q and
Chen Y: Two case reports of bilateral adrenal myelolipomas. World J
Clin Cases. 3:853–860. 2015.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Roger BR, Dhali A, Ramesh RS and Dsouza C:
Giant bilateral adrenal myelolipoma: Case report. Indian J
Endocrinol Metab. 24:551–553. 2020.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Purohit A and Rappaport M: Management of
giant bilateral adrenal myelolipomas in congenital adrenal
hyperplasia. JCEM Case Rep. 3(luaf169)2025.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Li Z, Li H, Lv P, Peng X, Wu C, Ren J and
Wang P: Prospective multicenter study on the incidence of surgical
site infection after emergency abdominal surgery in China. Sci Rep.
11(7794)2021.PubMed/NCBI View Article : Google Scholar
|
|
38
|
de Vermandois JAR, Cochetti G, Zingaro MD,
Santoro A, Panciarola M, Boni A, Marsico M, Gaudio G, Paladini A,
Guiggi P, et al: Evaluation of surgical site infection in
mini-invasive urological surgery. Open Med (Wars). 14:711–718.
2019.PubMed/NCBI View Article : Google Scholar
|