Introduction
Carbohydrate antigen 19-9 (CA19-9) is a highly
glycosylated mucin-type tumor biomarker identified by the
monoclonal antibody 1116-NS-19-9. It serves as a key diagnostic and
prognostic monitoring tool primarily for pancreaticobiliary and
gastrointestinal malignancies (1).
Its physiological basis stems from Lewis blood group
antigen-related glycan structures expressed in normal epithelia of
the pancreatobiliary ducts, gastrointestinal tract, endometrium and
fallopian tubes. However, CA19-9 has well-documented limited
specificity. Elevated levels are increasingly recognized in various
benign conditions because of mechanisms such as
inflammation-induced disruption of epithelial barriers facilitating
antigen leakage into the circulation or excessive production by
metaplastic or hyperplastic mucinous epithelia (1-3).
Common benign conditions include acute cholangitis, liver
cirrhosis, pelvic inflammatory disease and notably, gynecological
cysts such as ovarian endometriomas and uterine adenomyotic cysts
(1-3).
Bartholin's gland cysts are among the most common
benign vulvar lesions, typically resulting from ductal obstruction
leading to mucus retention and account for ~2% of vulvar masses in
women (4). To the best of our
knowledge, no prior studies have reported an association between
Bartholin's gland cysts and markedly elevated CA19-9.
Notably, similarly high CA19-9 levels (>1,000
U/ml) in benign gynecological conditions are rare. Documented cases
are rare and predominantly involve uterine
adenomyotic/endometriotic cysts, such as, Zheng et al
(5) reported a case with CA19-9
>1,000 U/ml (alongside elevated CA125); Imaoka et al
(6) reported levels of 846 U/m in
cystic adenomyosis. Ovarian endometriomas: While mild elevations
(<200 U/ml) occur in ~30% of endometriosis cases, values
exceeding 1,000 U/ml are reported in <2% of cases and are often
associated with cyst rupture (2,7).
Other benign entities: Moderate elevations have been noted in
conditions such as hydrosalpinx and cervical mucinous cysts
(3,8), but levels persistently >1,000 U/ml
remain rare and necessitate thorough investigation to exclude
occult malignancy.
The present case report presents the first
documented case of a Bartholin's gland cyst accompanied by a
notably elevated CA19-9 level (>1,000 U/ml). This striking
finding challenges the conventional clinical tenet that ‘CA19-9
>1,000 U/ml is pathognomonic for malignancy’. This finding
underscores the need to reevaluate the interpretation of tumor
markers within the context of benign mucin-producing cysts and
highlights the risk of misdiagnosis, leading to unnecessary anxiety
or aggressive interventions.
Through detailed analysis of diagnostic pathway of
this case, therapeutic intervention (marsupialization) and rapid
biomarker dynamics, the present case report aims to provide
evidence-based insights that can be used to improve differential
diagnostic strategies. The aim is to equip clinicians with the
ability to distinguish such benign yet biomarker-alarm
presentations from true malignancies, thereby preventing
unnecessary interventions.
Case report
Admission
A 43-year-old woman was admitted to the Department
of Gynecology of the Second Affiliated Hospital of Tianjin
University of Traditional Chinese Medicine (Tianjin, China) in
January 2025, with a chief complaint of a palpable mass in the
vulva for 4 days accompanied by pain for 1 day.
Medical history
This patient had a regular menstrual history with a
cycle of 28-30 days and moderate flow, without dysmenorrhea. The
last menstrual period of the patient was 19 days before admission.
The patient had undergone laparoscopic ovarian cystectomy and
cesarean section in 2003, both of which yielded benign pathology
results. There was no history of chronic diseases such as diabetes,
hypertension or coronary heart disease, as well as infectious
diseases such as hepatitis, tuberculosis, typhoid fever or malaria.
There was also no other surgical history, trauma or blood
transfusion, and the patient had received routine vaccinations.
Physical examination
On admission, the vital signs of the patient were
stable, with a temperature of 36.5˚C, a pulse rate of 90 beats per
min, a respiratory rate of 18 breaths per min and a blood pressure
of 130/85 mmHg. Cardiopulmonary examination revealed no notable
abnormalities. Abdominal examination revealed a soft abdomen
without hepatosplenomegaly or lower limb edema. Gynecological
examination revealed a 4-cm cystic mass in the left Bartholin's
gland with tenderness and fluctuation, a patent vagina, a smooth
cervix, a normal-sized anteverted uterus and no notable
abnormalities in the adnexa.
Laboratory and imaging
Most of the laboratory tests, including the tests
for coagulation profile (six items), complete blood count,
hepatitis B surface antigen/antibody, hepatitis C antibody,
syphilis antibody, and HIV antibody were within normal limits.
However, laboratory tests revealed elevated levels of CA19-9
(>1,000 U/ml; normal range, 0-27 U/ml), which were measured via
an electrochemiluminescence immunoassay on a Roche Cobas e 801
analyzer (Roche Diagnostics). Pelvic ultrasound revealed multiple
uterine fibroids (the largest measuring 3.9x4.4x3.6 cm) and pelvic
effusion. Abdominal and pelvic CT scans revealed a full uterus with
an irregular shape and a cyst in the upper pole of the left
kidney.
Diagnosis and treatment
Patient was diagnosed with a Bartholin's gland cyst.
The clinical presentation was typical for a Bartholin's gland cyst.
An abdominal examination revealed a soft abdomen without
hepatosplenomegaly or lower limb edema. Gynecological examination
revealed a 4-cm cystic mass in the left Bartholin's gland with
tenderness and fluctuation, a patent vagina, a smooth cervix, a
normal-sized anteverted uterus and no notable abnormalities in the
adnexa. The attending physician proceeded with surgical drainage
under local anesthesia on the day of admission. The procedure
involved making a longitudinal incision over the cyst, with
transparent fluid drainage and placement of Vaseline gauze for
drainage. Postoperatively, the patient was managed with routine
gynecological care, including daily wound dressing changes. The
medication used included one subcutaneous injection of 0.1 g
lidocaine and one intravenous infusion of 500 ml 0.5% glucose.
Follow-up
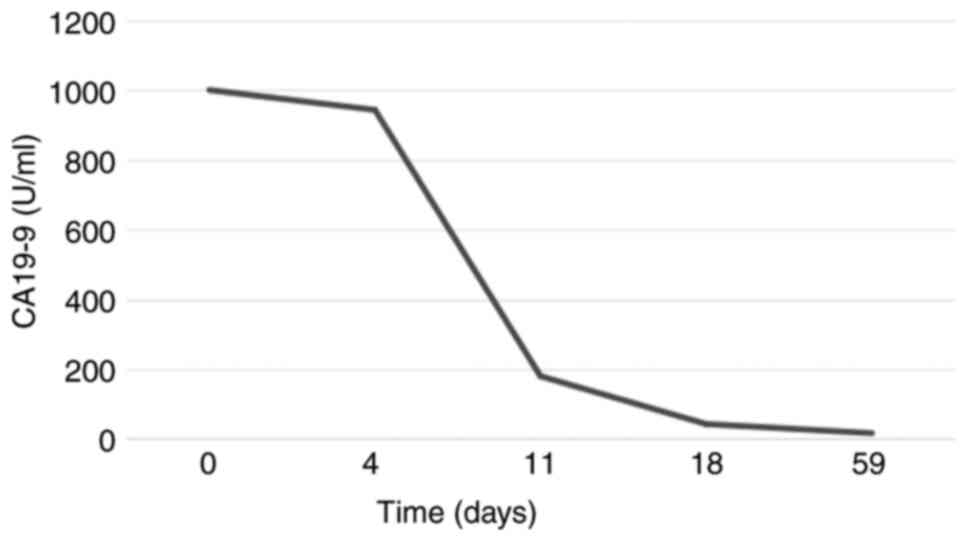
Changes in CA19-9 levels are shown in Fig. 1. The postoperative course of the
patient was uneventful, with no signs of infection or
complications. The elevated CA19-9 levels prompted further
evaluation via an abdominal and pelvic CT scan, which revealed
reduced enhancement in the tail of the pancreas. Gastrointestinal
endoscopy revealed mild gastritis. CA19-9 results were obtained
postoperatively, which led to retrospective monitoring of tumor
markers (including tests for α-fetoprotein, carcinoembryonic
antigen, CA125, squamous cell carcinoma antigen, human epididymis
protein 4 and human chorionic gonadotropin) and imaging studies
(pelvic ultrasound, and abdominal and pelvic CT). While monitoring
the patient for 2 months, no new diseases were observed, and other
possible diseases that could cause elevated CA19-9 levels were
successfully ruled out. It was ultimately confirmed that the
increase in this indicator was only related to the Bartholin's
cyst.
Discussion
As a key tumor marker, CA19-9 is secreted by various
epithelial cells under normal physiological conditions and is
mainly distributed in tissues such as the biliary tract, pancreatic
duct epithelium, endometrium, fallopian tubes, endocervix and
bronchial gland epithelium (9).
CA19-9 is a substance similar to monosialylated Lewis blood group
antigen and its synthesis involves the catalytic action of
glycosyltransferases (such as β3GALT5 and FUT3). In malignant tumor
cells, the increase in glycosyltransferase activity leads to the
overproduction of CA19-9. In patients with digestive system forms
of cancer, the level of CA19-9 is markedly elevated, with the
incidence of elevated CA19-9 levels in patients with malignant
tumors being markedly increased compared with that in patients with
benign lesions and healthy individuals. The most common type of
cancer is pancreatic cancer (62.04%), followed by liver cancer
(44.25%), gastric cancer (26.40%) and colorectal cancer (26.32%)
(10). Luo et al (11) revealed that the level of CA19-9 in
patients with pancreatic cancer is considerably increased compared
with that in healthy individuals or patients with benign pancreatic
diseases (such as pancreatitis), with a diagnostic sensitivity of
~70%, and it is positively associated with pathological stage: the
later the stage, the higher the levels of CA19-9.
The liver, as the main organ for clearing CA19-9,
carries out a key role in its metabolism. In hepatobiliary
diseases, biliary obstruction (due to stones or tumor compression)
can lead to impaired excretion of CA19-9, whereas secondary biliary
tract inflammation or infection can stimulate the overproduction of
CA19-9 by biliary epithelial cells (12).
The level of CA19-9 in patients with
cholangiocarcinoma is markedly increased compared with that in
patients with benign biliary diseases. In the diagnosis of
colorectal cancer with liver metastasis, the diagnostic sensitivity
of CA19-9 is 72.3% (13,14). Zhang et al (15) confirmed that a CA19-9 level >309
µg/l is a specific threshold for diagnosing malignant biliary
obstruction (89%), whereas a CA19-9 level >1,000 U/ml indicates
a poor prognosis for patients with liver metastasis (with a median
survival of only 8 months). In gastric cancer, CA19-9 levels are
highly consistent with tumor cell proliferation activity and are
markedly elevated in advanced-stage patients. It is often necessary
to combine CA19-9 with other markers, such as CEA, CA72-4 and
CA125, to enhance diagnostic efficacy (16,17).
There are also reports revealing that CA19-9 is elevated to varying
degrees in ovarian malignant tumors, especially in the middle and
late stages of ovarian cancer, where its level can rise notably
(18).
However, elevated CA19-9 is not a specific
manifestation of malignant tumors. Among the healthy population
undergoing physical examinations, 97.9% of individuals with
elevated CA19-9 levels have non-malignant causes of increased
CA19-9 levels (19). The main
mechanisms involve inflammation-induced epithelial hyperplasia
(such as increased ductal secretion caused by chronic pancreatitis)
and oversecretion by cystic lesions. For example, Zurli et
al (20) reported a case of a
large atypical hepatic cyst in which the CA19-9 level of a patient
reached 638 U/ml. Subsequent detection of CA72.4 in the cystic
fluid confirmed that the lesion was benign (21). Moreover, although a CA19-9 level
>1,000 U/ml usually raises concerns regarding malignant tumors,
certain benign gynecological conditions can also demonstrate
detectable expression of this marker (22-24).
The present case also adds new evidence to the
elevation in benign mucinous cysts: Zheng et al (5) reported that CA19-9 levels in a
uterine adenomyotic cyst were >1,000 U/ml, which returned to
normal 6 weeks after resection; Imaoka et al (6) reported a level of 846 U/ml in cystic
adenomyosis, attributing it to mucinous exudation; Takemori and
Sugimura (7) and Rokhgireh et
al (2) reported that although
30% of endometriosis cases showed mild elevation of CA19-9 (<200
U/ml), values exceeding 1,000 U/ml occurred in <2% of cases,
usually accompanied by cyst rupture; other benign diseases, such as
hydrosalpinx and cervical mucinous cysts, may show moderate
elevation of CA19-9 (3,8), but levels exceeding 1,000 U/ml are
still considered abnormal.
The patient in this case was a 43-year-old woman who
presented with a palpable vulvar mass. After examination, the
patient was ultimately diagnosed with a Bartholin's gland cyst. The
attending physician carried out surgery for the Bartholin's gland
cyst following the examination. The patient received routine
postoperative care and did not develop any infections or other
complications. However, the CA19-9 level of the patient exceeded
the normal range (peak >1,000 U/ml). A series of tests were then
conducted and malignancy was ruled out. Unexpectedly, the present
case report confirmed that the elevation of the CA19-9 levels of
the patient was likely associated with the Bartholin's cyst. This
case is the first to show that a Bartholin gland cyst may cause a
considerable increase in the serum CA19-9 concentration, which may
be associated with the following factors: First, active secretion
by the mucinous epithelium can occur. It has been confirmed that
numerous patients with benign cysts (such as hepatic, renal and
ovarian cysts) have a certain probability of experiencing elevated
CA19-9 levels (21). We reasonably
suspect that Bartholin's cysts may also fall into this category.
Moreover, research by Yan et al (21) revealed that the serum CA19-9
positivity rate in patients with benign mucinous cystic diseases
was 19.8%, which also supports the conclusion in the present case
that the elevation of CA19-9 is likely due to the Bartholin's cyst.
Second, multiple studies have demonstrated that key inflammatory
factors in this disease, such as IL-6 and tumor necrosis factor-α
(TNF-α), are associated with tumor markers (25-27).
These factors may be the main cause of the sharp increase in the
CA19-9 levels of the patient in the present case report. The fact
that the CA19-9 level in this case decreased rapidly within 7 days
(postoperative days 4-11) further indirectly demonstrates that the
elevation was driven by inflammation. Third, regarding the physical
characteristics of the cyst, Yan et al (21) revealed that in patients with benign
cystic lesions, the CA19-9 level is positively associated with the
cyst diameter (21,28).
For patients with elevated CA19-9 levels, a rational
differential diagnosis pathway is key. On the basis of this case
and the literature (5,6,29),
the present case report proposes a strategy that includes dynamic
monitoring, imaging and the combined use of multiple tumor markers
for diagnosis. First, it is necessary to rule out false positives
caused by detection interference (such as heterophilic antibodies
or hemolysis) (30). The dynamic
changes in CA19-9 can also be valuable for differentiating benign
and malignant diseases and for monitoring therapeutic effects.
CA19-9 should be retested at short intervals: If the level is
>1,000 U/ml, retesting within 24-48 h is recommended. A rapid
decline (a decrease of >50% within 24 h) strongly supports a
benign lesion. In the case of tumor recurrence, CA19-9 may rise
again and this may occur before imaging diagnosis. Therefore, it
can also be used to monitor tumor recurrence (31). It is also recommended to combine
the detection of tumor markers to improve the accuracy and
effectiveness of disease identification (18,32).
Second, for patients with confirmed elevated CA19-9 and no abnormal
liver or kidney function, imaging should be carried out on the
basis of symptoms: Pelvic MRI to rule out deep adenomyotic cysts
(7) and if CA19-9 levels continue
to rise, CT or PET-CT should be carried out to rule out
pancreaticobiliary malignancy (33). In addition, cyst fluid analysis is
also important. In future cases, CA19-9 in the drainage fluid
should be quantified (a concentration much higher compared with
that in serum suggests local secretion) and combined with markers
such as CA72-4 and CEA to confirm local production.
However, the present study also has certain
limitations. First, the tracking of inflammatory factors such as
IL-6 and TNF-α could be increased to assess their potential impact
on tumor markers. In addition, the present case report has a
single-case design and lacks analysis of cyst fluid biomarkers.
Future studies should include immunohistochemical analysis of
CA19-9 in the cyst epithelium (5),
tracking the relationship between inflammatory cytokines (such as
IL-6 and CRP) and CA19-9, and establishing a multicenter registry
for rare CA19-9 elevations.
This case highlights the importance of a
comprehensive approach for managing patients with elevated tumor
marker levels and benign gynecological conditions. This underscores
the need for clinicians to consider benign conditions when
interpreting elevated tumor marker levels, potentially reducing
unnecessary anxiety or aggressive interventions.
Acknowledgements
Not applicable.
Funding
Funding: The present study is supported by the Talent
Development Program of the Second Affiliated Hospital of Tianjin
University of Traditional Chinese Medicine (grant no.
YC-ZY202404).
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
All authors contributed to the data collection and
discussed the final version of the paper. WZ and TZ made
substantial contributions to the conception or design of the work,
acquisition, analysis and interpretation of the work, drafting the
work or critically revising it for important intellectual content.
All authors have read and approved the final manuscript. WZ and TZ
confirm the authenticity of all the raw data. All authors agree to
be accountable for all aspects of the work in ensuring that
questions related to the accuracy or integrity of any part of the
work are appropriately investigated and resolved.
Ethics approval and consent to
participate
The research complied with all the relevant national
regulations, institutional policies and was in accordance with the
tenets of the Helsinki Declaration, ethics approval was waived by
the medical ethics review board of the Second Affiliated Hospital
of Tianjin University of Traditional Chinese Medicine (waiver no.
EfE2024/003/01). Informed consent for participation and publication
was obtained from the patient prior to the start of the study.
Patient consent for publication
Written informed consent for publication was
obtained from the patient.
Competing interests
The authors declare that they have no competing
interests.
Use of artificial intelligence tools
During the preparation of this work, artificial
intelligence tools (https://china.aje.com/cn/rubriq) were used to improve
the readability and language of the manuscript, and subsequently,
the authors revised and edited the content produced by the
artificial intelligence tools as necessary, taking full
responsibility for the ultimate content of the present
manuscript.
References
|
1
|
Lee T, Teng TZJ and Shelat VG:
Carbohydrate antigen 19-9 - tumor marker: Past, present, and
future. World J Gastrointest Surg. 12:468–490. 2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Rokhgireh S, Mehdizadeh Kashi A, Chaichian
S, Delbandi AA, Allahqoli L, Ahmadi-Pishkuhi M, Khodaverdi S and
Alkatout I: The diagnostic accuracy of combined Enolase/Cr, CA125,
and CA19-9 in the detection of endometriosis. Biomed Res Int.
2020(5208279)2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Kim S, Park BK, Seo JH, Choi J, Choi JW,
Lee CK, Chung JB, Park Y and Kim DW: Carbohydrate antigen 19-9
elevation without evidence of malignant or pancreatobiliary
diseases. Sci Rep. 10(8820)2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Omole F, Simmons BJ and Hacker Y:
Management of Bartholin's duct cyst and gland abscess. Am Fam
Physician. 68:135–140. 2003.PubMed/NCBI
|
|
5
|
Zheng L, Shan L and Cai F: Uterine
adenomyotic cyst with markedly elevated serum CA19-9 and CA125
levels: A case report. Exp Ther Med. 24(665)2022.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Imaoka I, Kaji Y, Kobashi Y, Wada A, Honjo
G, Hayashi M, Yoshida M and Matsuo M: Cystic adenomyosis with
florid glandular differentiation mimicking ovarian malignancy. Br J
Radiol. 78:558–561. 2005.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Takemori M and Sugimura K: Ovarian
chocolate cyst with markedly elevated serum CA19-9 level: A case
report. Eur J Obstet Gynecol Reprod Biol. 42:241–244.
1991.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Sato H, Borsari R, Yajima EK, Ninomiya T,
Saito CS and Kumagai CA: Adenomyoma associated with high level of
CA 125 and CA 19-9: Case report. Eur J Gynaecol Oncol. 32:455–456.
2011.PubMed/NCBI
|
|
9
|
Wang L, Wang D, Zheng G, Yang Y, Du L,
Dong Z, Zhang X and Wang C: Clinical evaluation and therapeutic
monitoring value of serum tumor markers in lung cancer. Int J Biol
Markers. 31:e80–e87. 2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Xiang DK, Xie JY, Luo W, Zou H and Wang D:
Systematic Analysis of Carbohydrate Antigen (CA19-9) within Serum
Multiple Tumor Markers Chip and its Clinical Significance in Cancer
Diagnosis. Practical Journal of Cancer. 27:147–152. 2012.(In
Chinese).
|
|
11
|
Luo XZ, Yang X and Fu WL: Evaluation of
the diagnostic value of CA19-9 combined with routine blood and
liver function indicators for pancreatic cancer. Inter J Laborat
Med. 43:1434–1439. 2022.(In Chinese).
|
|
12
|
Zhang K, Zhang LF, Zheng LX, et al:
Clinical predictive value of different serological indexes for
acute cholangitis secondary to choledocholithiasis. J Region
Anatomy Operat Surg. 31:512–515. 2022.(In Chinese).
|
|
13
|
Li X, Yan J, Meng WB, Zhang L, Zhou W, Zhu
K, Zhu X, He W and Bai Z: Department of General Surgery, the First
Hospital of Lanzhou University. Clinical value of serum
carbohydrate antigen 19-9 in the differential diagnosis of benign
and malignant biliary system diseases. Chin J Hepatic Surg
(Electronic Edition). 3:226–230. 2014.(In Chinese).
|
|
14
|
Sun W, Wang Q, Liu J, et al: Application
of serum tumor markers in the diagnosis of colorectal cancer. Chin
J Laborat Med. 23:10–12. 2000.(In Chinese).
|
|
15
|
Zhang XD, Ge XL, Liu SC, Zheng WQ and Shen
T: The prognostic and predictive value of serum CA199 and CEA in
colorectal cancer metastasis. Chin J Disease Control Prevent.
22:57–61. 2018.(In Chinese).
|
|
16
|
Wu AJ and Zhang ZX: Value of preoperative
multi-slice spiral CT enhancement scanning in determining TNM stage
of gastric cancer and its relationship with tumor markers and
proliferation molecule expression. J Hainan Med Univ. 22:2928–2931.
2016.(In Chinese).
|
|
17
|
Wang H and Yin Y: The expression
difference of CEA, CA19-9, CA72-4 and CA125 in patients with
different staging of gastric cancer and the relationship with
metastasis and recurrence. Biomed Res. 28:9769–9772. 2017.
|
|
18
|
Yue LJ, Hou XL, Xue L, Zhu H-C, Zhang J-J
and Wang Y: Department of Oncology, Hanzhong Central Hospital.
Clinical value of combined detection of multiple tumor markers in
diagnosis of the recurrence of ovarian cancer. Chin J Clin Oncol
Rehab. 27:20–22. 2020.(In Chinese).
|
|
19
|
Han XD, Ying S and Chen ZY: Analysis of
serum CA19-9 test results in healthy physical examination
population. Shanghai J Prevent Med. 25:109–110. 2013.(In
Chinese).
|
|
20
|
Zurli L, Decker J, Robles B and Regimbeau
JM: Atypic large hepatic cyst with persistent elevated CA19.9 serum
value: utility of intracystic CA72.4 dosage for a mini-invasive
management. Clin J Gastroenterol. 14:258–262. 2021.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Yan XQ, Huang QL and He YH: Correlation
research of serum CA1 9-9 with benign cystic diseases. Guizhou Med
J. 47:176–177. 2023.(In Chinese).
|
|
22
|
Liu YH, Liu YQ and Qiu YH: Expression and
clinical value of vascular endothelial growth factor, carbohydrate
antigen 125, and carbohydrate antigen 19-9 in cervical cancer.
Oncology Progress. 20:712–715. 2022.
|
|
23
|
Chen YE, Wu XM and Wen YH: Expression of
serum HE4, CA125 and CA19-9 in patients with endometrial carcinoma
and its relationship with clinicopathological features. Chin J
Gerontol. 37:3787–3789. 2017.(In Chinese).
|
|
24
|
Fan CM, Luo X and Wen F: Clinical Value of
Serum CA125 and CA19-9 Detection for the Diagnosis of Epithelial
Ovarian Cancer and Endometriosis. J Chin Med Univ. 38:376–378.
2009.(In Chinese).
|
|
25
|
Zhang Q and Jin X: Relationship of
dyscrasia formation and the concentration of tumor necrosis
factor-α (TNF-α) and interleukin-6 (IL-6) of patients with advanced
gastrointestinal cancer. Chin Modern Doctor. 52:129–131. 2014.(In
Chinese).
|
|
26
|
Agca S and Kir S: The role of
interleukin-6 family cytokines in cancer cachexia. FEBS J.
291:4009–4023. 2024.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Hannan CJ, Lewis D, O'Leary C, Donofrio
CA, Evans DG, Stapleton E, Freeman SR, Lloyd SK, Rutherford SA,
Hammerbeck-Ward C, et al: Beyond antoni: A surgeon's guide to the
vestibular schwannoma microenvironment. J Neurol Surg B Skull Base.
83:1–10. 2020.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Cho HY, Kim K, Jeon YT, Kim YB and No JH:
CA19-9 elevation in ovarian mature cystic teratoma: Discrimination
from ovarian cancer - CA19-9 level in teratoma. Med Sci Monit.
19:230–235. 2013.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Pontrelli G, Bounous VE, Scarperi S,
Minelli L, Di Spiezio Sardo A and Florio P: Rare case of giant
cystic adenomyoma mimicking a uterine malformation, diagnosed and
treated by hysteroscopy. J Obstet Gynaecol Res. 41:1300–1304.
2015.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Trapé J, Fernández-Galán E, Auge JM,
Carbonell-Prat M, Filella X, Miró-Cañís S and González-Fernández C:
Oncology biomarkers section of the catalan association of clinical
laboratory science. Factors influencing blood tumor marker
concentrations in the absence of neoplasia. Tumour Biol.
46(s1):S35–S63. 2024.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Yu L: Common tumor markers and their
clinical detection applications. Medical Information. 24:3494–3495.
2011.
|
|
32
|
Han M, Ma MJ and Lian J: Clinical value of
combined detection of serum AFP,CEA,CA199,CA125 and HE4 in
diagnosis of ovarian cancer. Hebei Med J. 44:76–78, 82. 2022.(In
Chinese).
|
|
33
|
Wu HJ, He NA, Xie L, et al: Application of
contrast-enhanced ultrasound combined with serum CA19-9 in the
differential diagnosis of cholangiocarcinoma and hepatocellular
carcinoma. J Practical Hepatol. 24:903–906. 2021.(In Chinese).
|