Introduction
Nodular goiter is a prevalent thyroid disease.
According to the study by Carlé et al (1) (2014), more than one-tenth of the
world's population is to some degree affected by goiters and most
of these individuals harbour nodules (1). Ablation therapy or systematic
follow-up monitoring is the standard therapeutic approach for small
nodular goiters localized within the cervical region (2). However, retrosternal goiters or those
presenting with compressive symptoms typically necessitate surgical
intervention (2-4).
Large or deeply invasive mediastinal thyroid tumors typically
require combined cervicothoracic surgical intervention, which
increases surgical trauma outcomes and elevates operative risks
(2-4).
Selective arterial embolization has emerged as a key
therapeutic modality in clinical medicine. It is extensively
employed in the management of vascular anomalies, life-threatening
hemorrhages as well as benign and malignant neoplasms (5-7).
In the management of both neoplasms, selective arterial
embolization precisely occludes targeted blood vessels to induce
tumor ischemia and decrease the tumor volume, establishing itself
as an indispensable element of holistic management for neoplastic
diseases (5,8).
However, current literature on thyroid artery
embolization as a preoperative therapeutic approach for thyroid
disorders remains limited. Graves' disease is an autoimmune thyroid
disease and the most common cause of hyperthyroidism in clinical
practice. Medication, surgery and radioactive iodine therapy are
the main treatment methods (9). A
number of clinical studies have documented the application of
thyroid artery embolization in the management of Graves' disease,
demonstrating its efficacy in restoring the thyroid function of
patients to normative levels (10-12).
However, the literature provides limited reports on the application
of thyroid artery embolization in the management of large thyroid
masses (3,4). These studies demonstrate that
preoperative thyroid artery embolization not only reduces
intraoperative hemorrhage risk but also serves as a palliative
intervention for surgically ineligible patients (3,4,8). The
present report outlines the clinical case of a patient diagnosed
with a giant retrosternal goiter, who successfully underwent
preoperative thyroid artery embolization prior to
thyroidectomy.
Case report
A 70-year-old female patient presented with a goiter
that had persisted for 40 years without intervention. Over the past
2 years, the patient had observed an increase in goiter size and
experienced dyspnoea while at rest. The patient self-administered
Spica Prunellae oral liquid, which was ineffective and was
subsequently admitted to the Department of Thyroid Surgery at
Weifang People's Hospital (Shandong, China) in March 2025. The
patient's arterial oxygen saturation was 92%. Physical examination
revealed a well-defined and mobile 5x10 cm mass in the left thyroid
gland. It exhibited a smooth surface and showed synchronous
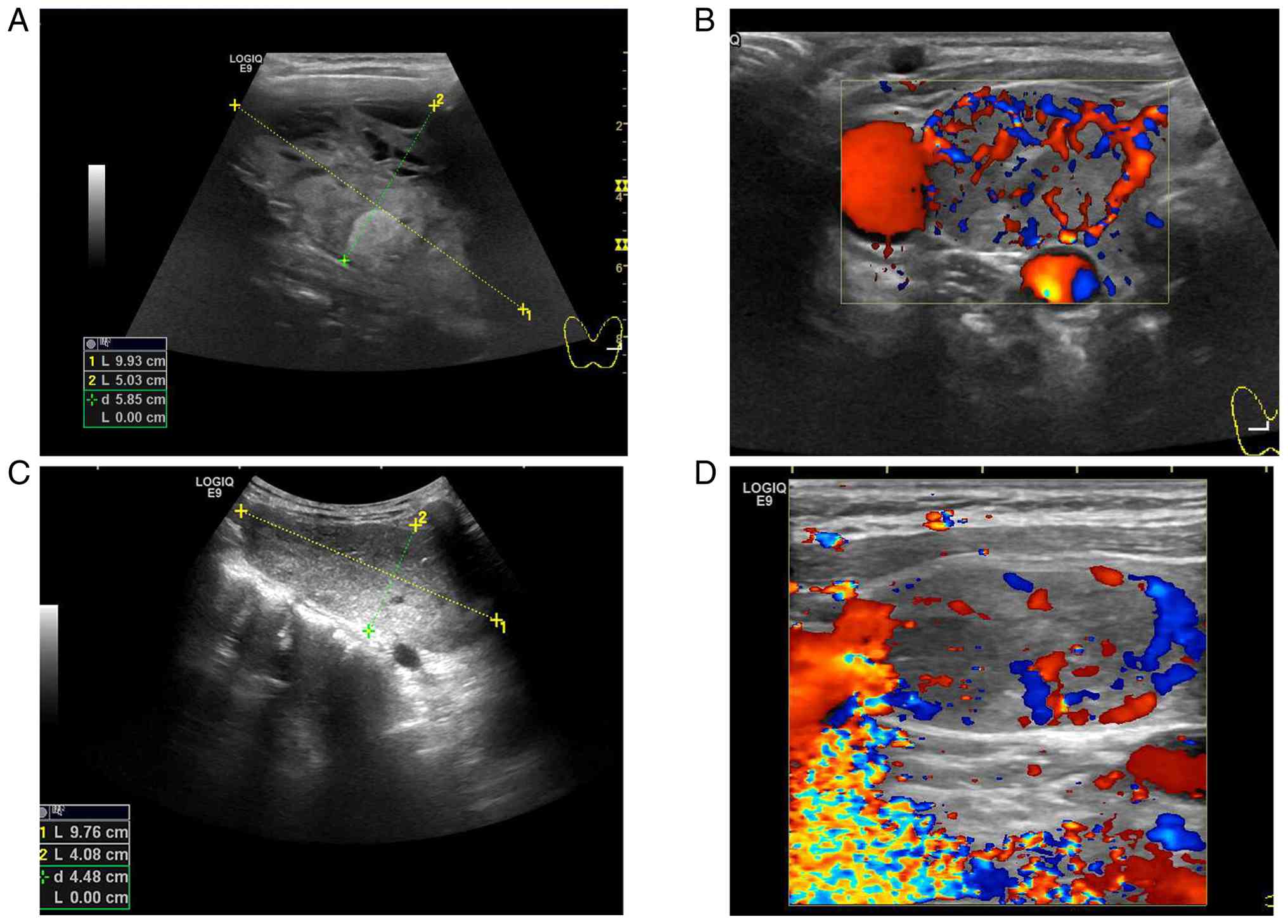
movement during swallowing. B-mode ultrasonography identified a
complex cystic-solid nodule in the parenchyma of the left thyroid
lobe, measuring 99.3x87.3x50.3 mm (Fig. 1A). Color doppler flow imaging
revealed extensive vascularization within the lesion (Fig. 1B). CT imaging of the neck and
thoracic region demonstrated notable enlargement of the left
thyroid lobe, measuring ~7.7x13.0x9.3 cm, with inferior extension
into the anterior mediastinum. The mass volume was estimated using
the ellipsoid volume formula (V=0.52 x length x width x height),
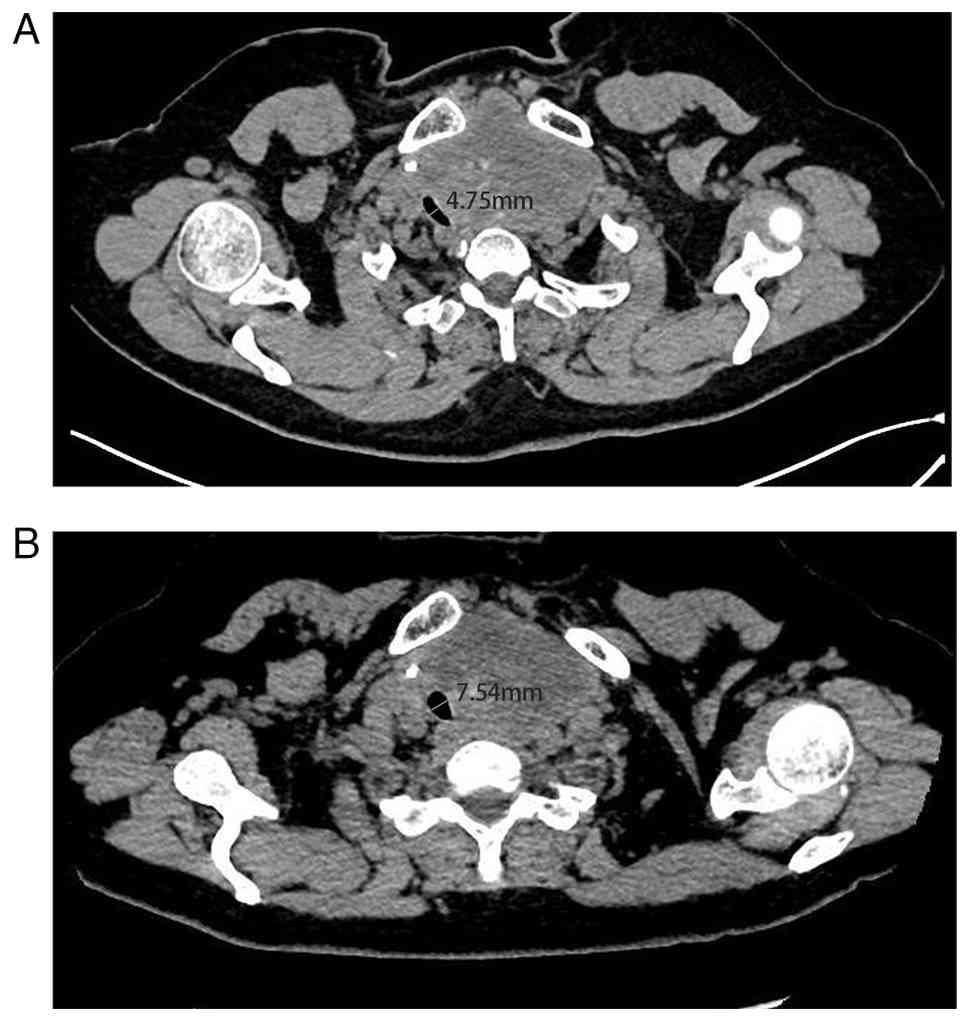
resulting in a value of 484.1 cm3. Imaging findings
indicated that tracheal compression leads to a rightward
displacement and flattening of the trachea. Quantitative assessment
indicated severe tracheal stenosis with a luminal diameter of 4.75
mm (Fig. 2A). Furthermore, the
tracheal softening test showed that the trachea moved to the right
and was compressed. The inner diameter of the trachea in the
Miller's test was 6.06 mm, and the inner diameter of the trachea in
the Valsalva test was 11.50 mm (13). (Negative reference value for
tracheal softening test: Cross-sectional diameter of the trachea in
the ward >7 mm; difference in inner diameter between the
Miller's and Valsalva experimental wards <2-3 mm).
Laboratory investigations revealed endocrine
dysfunction, which was indicated by elevated free triiodothyronine
(FT3) levels at 6.48 pmol/l (reference range: 2.77-6.31 pmol/l),
reduced free thyroxine (FT4) levels at 7.19 pmol/l (reference
range: 10.44-24.38 pmol/l) and thyroid-stimulating hormone (TSH)
levels at 3.089 µIU/ml (reference range: 0.380-4.340 µIU/ml). A
comprehensive reassessment of the thyroid profile of the patient
was conducted 72 h post-admission due to the abnormal thyroid
function indices. The laboratory results indicated an FT3 level of
5.98 pmol/l, an FT4 level of 12.25 pmol/l and an FSH level of 2.496
µIU/ml. Subsequent re-evaluations suggested that the initially
observed abnormal thyroid function in the patient may have resulted
from various confounding factors, such as inaccuracies in
laboratory testing. Parathyroid hormone (PTH) levels were notably
elevated at 69.10 pg/ml, exceeding the reference range of 15-65
pg/ml. Serum calcium levels were normal at 2.39 mmol/l (reference
range: 2.11-2.58 mmol/l).
The patient possessed a 20-year history of
hypertension and had been consistently administered telmisartan
orally. The advanced age of the patient and compromised oxygen
saturation levels considerably increased the risk associated with
the administration of general anesthesia. The thyroid mass
exhibited a notable size with mediastinal extension, potentially
requiring a combined cervicothoracic surgical approach for
effective management. A thoracotomy, due to the condition of the
patient, represented a highly invasive procedure with marked
associated risks, including potential intraoperative hemorrhage and
iatrogenic injury, as well as adjacent major vascular and neural
structures (14). Accordingly, a
strategic therapeutic approach was developed, whereby initial
thyroid artery embolization was conducted, followed by subsequent
surgical intervention.
Radiologists from Weifang People's Hospital
conducted the angiography procedure with the Seldinger technique
for bilateral carotid and subclavian artery angiography (2). The imaging results demonstrated
multiple abnormal feeding vessels (superior and inferior thyroid
arteries) supplying the neck mass with notable staining.
Embolization was performed using a combination of 500-700 µm
microspheres and gelatin sponge particles measuring 560-710 or
710-1,000 µm. Post-embolization angiography demonstrated a lack of
abnormal staining. A final slow angiography demonstrated total
obstruction of the aberrant vessels, indicating the successful
outcomes of the embolization procedure (data not shown).
Post-embolization, the patient reported cervicalgia
and was prescribed a therapeutic regimen that included nalbuphine
hydrochloride solution (20 mg) through intravenous infusion for
analgesia across 3 days, oral nifedipine sustained-release tablets
(20 mg) twice a day for hypertension, dexamethasone sodium
phosphate injection (5 mg) administered intravenously for
anti-inflammatory treatment across 3 days and oral cefixime (50 mg)
twice a day for prophylactic antibiotic therapy across 3 days.
The patient underwent comprehensive clinical
assessment 3 days after embolization, which included symptomatic
evaluation, physical examination and diagnostic imaging analysis.
The patient exhibited a notable enhancement in respiratory
function, indicating a marked decrease in dyspnoea. Subsequent
measurements of oxygen saturation indicated a stable reading of
98%, demonstrating the restoration of normal pulmonary oxygenation
status. B-mode ultrasonography revealed a mass in the left thyroid
lobe parenchyma (Fig. 1C),
measuring 97.6x40.8x87.3 mm in maximal dimensions. The mass
exhibited minimal vascularity, indicated by the lack of
considerable blood flow signals on Doppler imaging (Fig. 1D). A CT scan of the cervical region
indicated that the mass measured 7.6x12.5x9.6 cm, with stable
thyroid morphological changes and no notable progression compared
with prior imaging studies. The diameter of the trachea at the
corresponding anatomical level was measured at 7.54 mm (Fig. 2B). The mass volume was estimated
using the ellipsoid volume formula (V=0.52 x length x width x
height), resulting in a value of 474.2 cm3. At 1-week
post-embolization, the patient underwent a left thyroidectomy. In
the surgical procedure, the trachea was carefully suspended on the
sternocleidomastoid muscle and anterior cervical muscles to avert
the risk of postoperative tracheal collapse. Postoperative
monitoring indicated notable enhancement in the symptoms of
dyspnoea and choking initially presented by the patient. No
instances of hoarseness were observed during the postoperative
period. Subsequent laboratory analyses indicated serum calcium
levels of 2.25 mmol/l and PTH levels of 64.37 pg/ml, which fell
within the normal reference ranges.
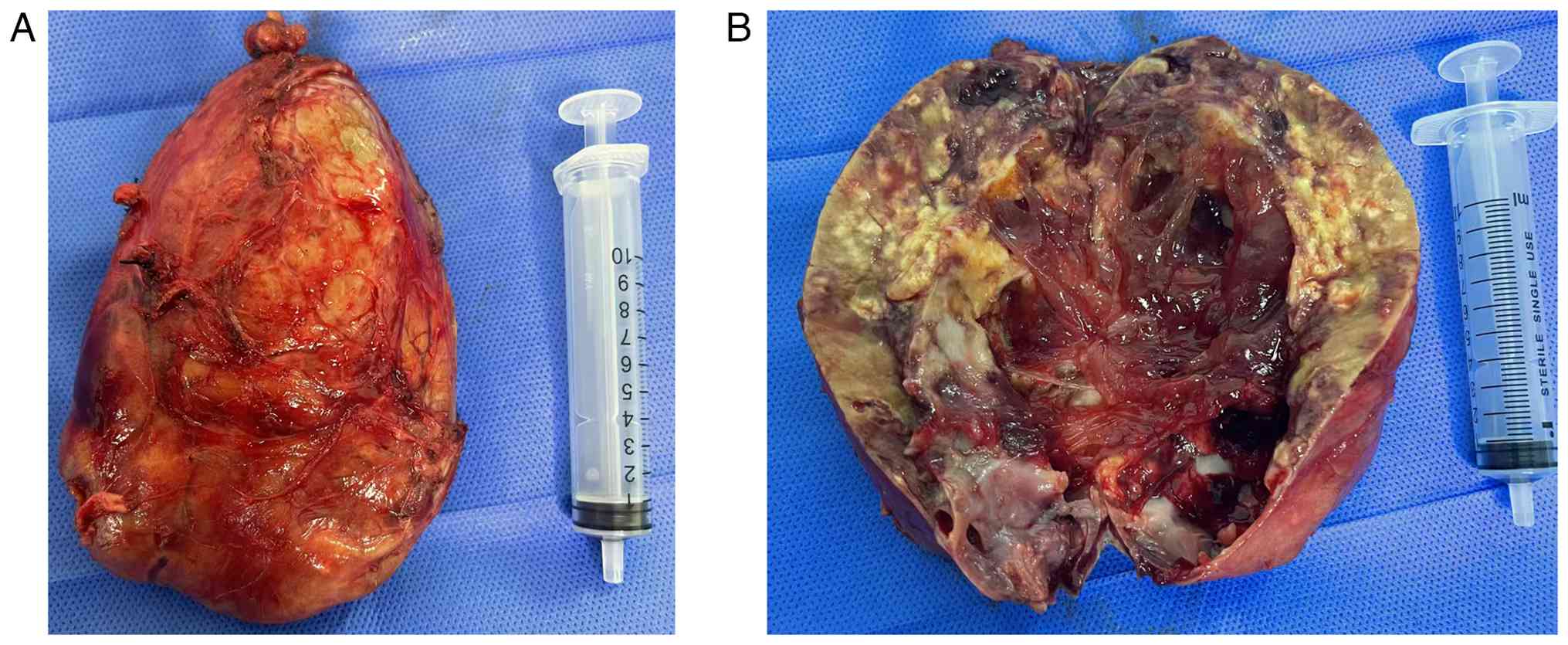
Routine postoperative pathological examination
revealed a grey-red irregular mass measuring 13x7x6 cm, as shown in
Fig. 3A. After cutting open the
tumor, it could be seen that the section was cystic and solid,
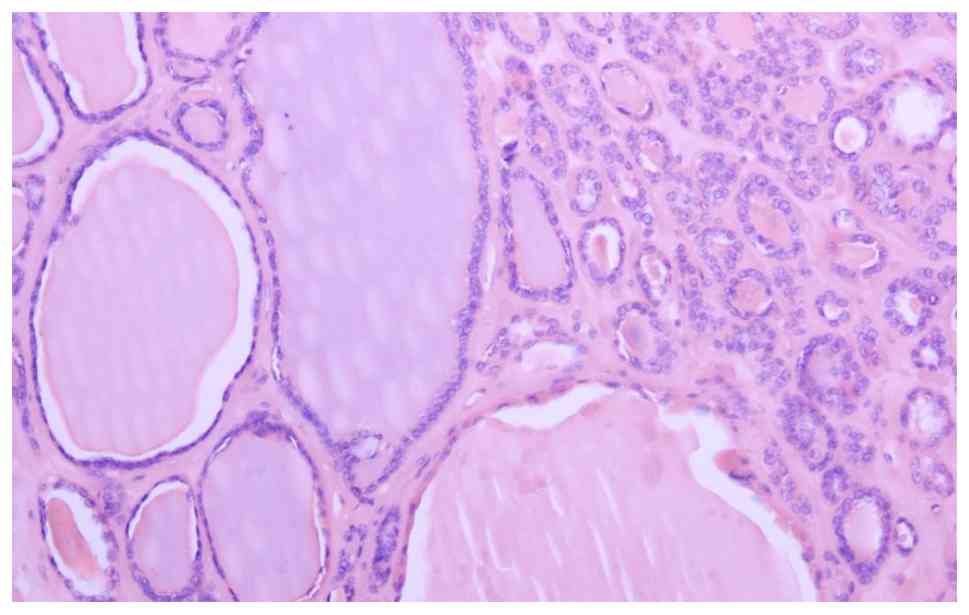
containing a gray red jelly-like substance, as shown in Fig. 3B. Tissue specimens were fixed with
4% formalin at room temperature for 12 h, embedded in paraffin at
60˚C for 15 min, cut into 4 µm sections, stained for 5 min at room
temperature with hematoxylin and eosin, and observed under a light
microscope (Nikon Corporation). The pathological findings indicated
nodular goiter, marked by cystic degeneration, fibrosis,
calcification and necrosis (Fig.
4).
A total of 5 days after the partial thyroidectomy, a
comprehensive evaluation of the patient revealed that the surgical
incision had healed well. The cervical drainage tube had been
removed and the symptoms of breathing difficulties had improved.
The patient was discharged from hospital. Furthermore, 2 months
after discharge, the patient returned to the institution for a
scheduled follow-up evaluation. The clinical assessment indicated a
complete resolution of the aforementioned dyspnoea. Laboratory
investigations revealed the following thyroid function parameters:
i) FT3 at 4.45 pmol/l; ii) FT4 at 14.40 pmol/l; and iii) TSH at
5.101 µmol/l, collectively indicating the onset of subclinical
hypothyroidism post-thyroid tumor resection (Table I). The patient commenced oral
levothyroxine therapy at a dosage of 25 mg daily. Follow-up for
re-examination was scheduled every 3 months for thyroid function
determination. Color Doppler ultrasound and CT were performed 6
months after the operation.
 | Table IThyroid function indices and serum
calcium levels before and after thyroid artery embolization. |
Table I
Thyroid function indices and serum
calcium levels before and after thyroid artery embolization.
| Test item | Normal range | Preoperative
value | Postoperative
value |
|---|
| FT3, pmol/l | 2.77-6.31 | 6.48 | 4.45 |
| FT4, pmol/l | 10.44-24.38 | 7.19 | 14.40 |
| TSH, µIU/ml | 0.380-4.340 | 3.089 | 5.101 |
| PTH, pg/ml | 15-65 | 69.10 | 64.37 |
| Ca+,
mmol/l | 2.11-2.58 | 2.39 | 2.25 |
Discussion
In the present clinical case, sustained airway
compression by the mass led to the development of tracheomalacia
and grade 2 tracheal stenosis. A comparative analysis of pre- and
post-thyroid artery embolization CT imaging indicated that the
calculation and reporting of estimated goiter volume remained
stable 3 days after the procedure, showing no considerable
reduction compared with the preoperative state. The tracheal
stenosis showed improvement, as the minimum tracheal diameter
increased from 4.75 to 7.54 mm at the corresponding anatomical
level. Notably, the comparison of pre- and post-thyroid artery
embolization revealed no marked change in tumor volume. However, a
notable increase in tracheal diameter was observed. This finding
indicates that the initial relief of tracheal compression was not
due to changes in tumor volume. However, it resulted from reduced
blood flow perfusion in the thyroid gland. The patient exhibited a
notable improvement in symptoms of dyspnoea and no distress was
observed during rest. The oxygen saturation levels of the patient
increased from 92 to 98%, falling within the normal physiological
range. The clinical observations suggested that thyroid artery
embolization effectively reduces tracheal compression. At 1 week
post-embolization, the anesthesiology department at Weifang
People's Hospital performed a thorough preoperative evaluation and
approved the patient for left thyroidectomy under general
anesthesia. The surgical procedure was conducted through a standard
cervical incision, resulting in complete resection of the left
thyroid gland without the need for a combined cervicothoracic
approach, thus reducing surgical trauma and enhancing patient
outcomes. Additionally, following thyroid artery embolization, the
patient experienced transient neck pain and localized discomfort as
the only adverse reactions, with no other complications or systemic
effects noted during the clinical course.
The vascular supply of the thyroid gland originates
mainly from three principal arterial sources and the bilateral
superior thyroid arteries contributed to ~70% of the overall blood
perfusion (15,16). The vascular anatomy indicates that
selective embolization of the superior thyroid arteries alone can
greatly compromise the vascular integrity of the gland (15,16).
In the present case, owing to the notable size of the
intrathyroidal mass, a thorough embolization approach was
implemented, directed at the superior and inferior thyroid arteries
bilaterally to maximize therapeutic efficacy (15,16).
Furthermore, 500-700 µm microspheres were employed alongside
560-710 or 710-1,000 µm gelatin sponge particles for embolization,
considering the absorbable characteristics of gelatin sponge that
promote the subsequent recanalization of the embolized vessels.
This therapeutic approach aligned with the decision to perform
unilateral thyroidectomy. Short-term vascular embolization notably
diminishes thyroid blood supply, thereby lowering surgical
complexity (17). After the
reabsorption of gelatin sponge particles, the thyroid arteries
undergo recanalization, thereby restoring blood supply to the
unaffected thyroid lobe, and preserves thyroid functionality
(17).
Current literature regarding thyroid artery
embolization primarily focuses on its role in managing Graves'
disease. However, studies that specifically examine the use of
thyroid artery embolization in the treatment of thyroid masses
remain limited (11,15-17).
Yilmaz et al (17)
conducted a clinical investigation on the non-surgical management
of nodular goiter through thyroid artery embolization. This study
indicated that 25 of 56 patients developed a range of
complications, which included hoarseness, visual disturbances,
hyperthyroidism, groin hematoma and cervical pain (17). The patient only exhibited cervical
pain after treatment, without the occurrence of any of the
aforementioned complications. The postoperative increase in TSH
levels aligned with anticipated results after unilateral
thyroidectomy, thereby demonstrating the safety profile of the
selected thyroid artery embolization method. Tartaglia et al
(2) reported a clinical case of a
patient with retrosternal goiter complicated by hyperthyroidism,
who received preoperative arterial embolization. The surgical
intervention was performed 30 days after embolization and imaging
studies indicated a reduction in thyroid mass volume (2). However, the mass remained in the
retrosternal position. Consequently, a prolonged interval between
embolization and surgery may lead to vessel recanalization, which
can result in marked intraoperative hemorrhage (2).
Ramos et al (3) reported the clinical case of a patient
with a giant retrosternal goiter complicated by papillary thyroid
carcinoma, who received preoperative thyroid artery embolization.
The surgical team noted a considerable decrease in intraoperative
hemorrhage relative to similar procedures (3). The treatment strategy included total
thyroidectomy, necessitating lifelong exogenous levothyroxine
replacement therapy for the patient. By contrast, the decision to
perform unilateral thyroidectomy not only effectively alleviated
compressive symptoms but also optimally preserved thyroid tissue
and physiological function. Postoperatively, the patient required
only temporary exogenous thyroid hormone supplementation until the
remaining thyroid tissue restored sufficient secretory function,
eliminating the need for extended hormone replacement therapy, and
this approach enhanced their quality of life (18).
In summary, thyroid artery embolization is a safe
and efficacious therapeutic intervention and within the present
case report, this treatment approach allowed the patient to avoid
thoracotomy, reduced the surgical risks and complications and
improved the long-term quality of life.
Acknowledgements
Not applicable.
Funding
Funding: The Research Project of Weifang Municipal Health
Commission (grant no. WFWSJK-2022-014) supported the present
study.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
JL and FW contributed to drafting the manuscript and
the design of the present study. JL, FW, YD and YW contributed to
the conceptualization and design of the present study, as well as
performing the surgery. JL and FW collected clinical information
and assisted with drafting the manuscript. YW and YD critically
revised the intellectual content of the manuscript. YW and YD
confirm the authenticity of all the raw data. All authors have read
and approved the final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of the present study and any accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Carlé A, Krejbjerg A and Laurberg P:
Epidemiology of nodular goitre. Influence of iodine intake. Best
Pract Res Clin Endocrinol Metab. 28:465–479. 2014.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Tartaglia F, Salvatori FM, Pichelli D,
Sgueglia M, Blasi S and Custureri F: Preoperative embolization of
thyroid arteries in a patient with a large cervicomediastinal
hyperfunctioning goiter. Thyroid. 17:787–792. 2007.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ramos HE, Braga-Basaria M, Haquin C, Mesa
CO, Noronha L, Sandrini R, Carvalho Gde A and Graf H: Preoperative
embolization of thyroid arteries in a patient with large
multinodular goiter and papillary carcinoma. Thyroid. 14:967–970.
2004.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Tartaglia F, Salvatori FM, Russo G, Blasi
S, Sgueglia M, Tromba L and Berni A: Selective embolization of
thyroid arteries for preresection or palliative treatment of large
cervicomediastinal goiters. Surg Innov. 18:70–78. 2011.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Tartaglia F, Sorrenti S, Maturo A and
Ulisse S: Selective embolization of the thyroid arteries (SETA):
Ten years' experience. Asian J Surg. 42:847–848. 2019.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Kaushik H, Deshmukh M, Gupte S, Kanchankar
N and Dongre A: A case report on primary pulmonary choriocarcinoma.
Cureus. 16(e63466)2024.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Sahoo B, Pitchaimuthu A, Swain PK and
Nayak M: Bleeding lymph node mass in a postoperative case of
thyroid carcinoma: Transarterial embolization to the rescue.
Cureus. 17(e86214)2025.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Dedecjus M, Tazbir J, Kaurzel Z, Strózyk
G, Zygmunt A, Lewiński A and Brzeziński J: Evaluation of selective
embolization of thyroid arteries (SETA) as a preresective treatment
in selected cases of toxic goitre. Thyroid Res. 2(7)2009.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Mahzari MM, Alanazi MM, Alabdulkareem YM,
Alharbi WA, Alzahrani AS, Alqahtani NA, Ajwah IM and Ardah HI:
Efficacy of anti-thyroid medications in patients with Graves'
disease. BMC Endocr Disord. 24(180)2024.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Zhao W, Gao BL, Yang HY, Li H, Song DP,
Xiang ST and Shen J: Thyroid arterial embolization to treat Graves'
disease. Acta Radiol. 48:186–192. 2007.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Xiao H, Zhuang W, Wang S, Yu B, Chen G,
Zhou M and Wong NC: Arterial embolization: A novel approach to
thyroid ablative therapy for Graves' disease. J Clin Endocrinol
Metab. 87:3583–3589. 2002.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Bonnici M, Nevin C and Boo S: Thyroid ima
artery embolization for the treatment of Graves' disease and
thyroid storm. Radiol Case Rep. 18:2641–2644. 2023.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Wright CD: Tracheomalacia. Chest Surg Clin
N Am. 13:349–357, viii. 2003.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Tikka T, Nixon IJ, Harrison-Phipps K and
Simo R: Predictors of the need for an extracervical approach to
intrathoracic goitre. BJS Open. 3:174–179. 2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Ducloux R, Sapoval M and Russ G:
Embolization of thyroid arteries in a patient with compressive
intrathoracic goiter ineligible to surgery or radioiodine therapy.
Ann Endocrinol (Paris). 77:670–674. 2016.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Yilmaz S and Habibi HA: Safety of
thyroidal artery embolization. J Vasc Interv Radiol.
33(200)2022.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Yilmaz S, Habibi HA, Yildiz A and Altunbas
H: Thyroid embolization for nonsurgical treatment of nodular
goiter: A single-center experience in 56 consecutive patients. J
Vasc Interv Radiol. 32:1449–1456. 2021.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Meyer C, Anderson D, Dong Z, Riddick JB,
Elrod M and Ayala M: Prediction of thyroid hormone replacement
following thyroid lobectomy: A long-term retrospective study. OTO
Open. 5(2473974x21992001)2021.PubMed/NCBI View Article : Google Scholar
|