Introduction
Endodontic therapy primarily aims to cure or prevent
periradicular periodontitis (1,2).
Failure to identify and treat all root canals can result in
unsuccessful root canal treatment, as bacteria persist and multiply
in overlooked canals, potentially causing unresolved existing
inflammation or novel inflammatory episodes in the periapical
tissues (3,4). Therefore, a thorough understanding of
the root canal anatomy and its variations is key in comprehensive
debridement and shaping.
The mandibular first molar, which most frequently
requires endodontic therapy (5),
typically has two roots, the mesial and distal (6). The mesial root usually houses two
canals and the distal root may contain one or two canals. However,
a recent investigation using micro-CT scanning indicated that the
root canal anatomy of the mandibular first molar appears more
intricate (7). Variations may
include a third canal in the developmental groove of the mesial
root, termed the middle mesial canal (MMC), with a prevalence of
0.26-45.80% (8). Additionally, the
rare occurrence of a third canal in the distal root, known as the
middle distal canal (MDC), varies with ethnicity and ranges from
0.2 to 3.0% (9). Given its rarity,
the presence of six root canals in the mandibular first molar has
been documented in a limited number of cases (9-20).
The present report illustrates a successful instance of root canal
retreatment in such a complex case.
Case report
A 40-year-old Chinese female patient with no notable
medical history presented to The Third People's Hospital of Chengdu
(Chengdu, China) in November 2023 with chief complaints of pain in
the lower right molar during mastication, persisting for 2 months.
Additionally, the patient reported that the restoration on the same
tooth had fractured 1 day earlier. The patient also recalled having
undergone ‘endodontic treatment’ (July 2008) at the People's
Hospital of Wenjiang District (Sichuan, China). This previous
therapy involved partial pulp removal and mummification therapy on
teeth nos. 45 and 46, followed by bridge restorations, which
progressively deteriorated. Clinical examination revealed a notable
fistula tract on the soft tissue surrounding tooth no. 46, which
elicited slight pain and discharged pus upon palpation. The probing
depth of the gingival sulcus was normal at all points except for
the buccal intermediate of tooth no. 46, where a localized
periodontal pocket measuring 7 mm was noted. Following the removal
of the crown, tooth no. 46 displayed grade 1 mobility according to
Miller's mobility index (21).
Vertical percussion on the affected teeth caused noticeable pain
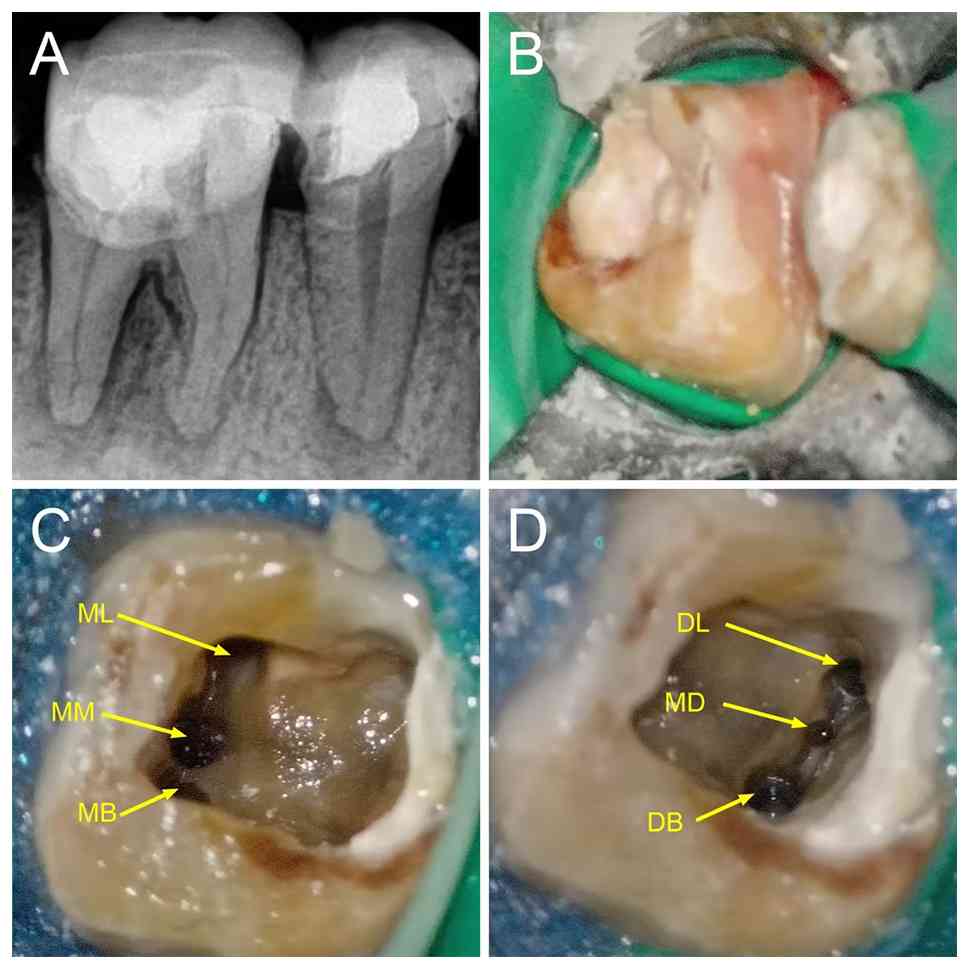
and pulpal electro-vitality tests yielded no response. Periapical
X-rays indicated high-density images in the crowns of teeth nos. 45
and 46, extending into the pulp cavity, with indistinct root canal
images suggesting the presence of calcified canals. Additionally,
diffuse radiolucent areas were observed in the apical regions of
both teeth and the periodontal ligament space surrounding the
cervical third and root bifurcation was widened (Fig. 1A). A dental cone-beam CT (CBCT)
scan was recommended to improve understanding of the severity of
the disease and the morphology of the root canal system. However,
the patient declined this examination. Based on the clinical
examination and radiographic findings, tooth no. 46 was diagnosed
with chronic apical periodontitis. After being fully informed about
their condition, the patient was given the option of non-surgical
endodontic treatment or implant placement following extractions,
with additional periodontal therapy potentially required. The
patient opted for endodontic retreatment. Before beginning the
treatment, the patient provided informed consent for all diagnostic
and therapeutic procedures. Additionally, the Ethics Review Board
of Chengdu Third People's Hospital (Sichuan, China) granted
approval for the present report (approval no. 2025-S-83).
The first root canal treatment was performed in
November 2023. Following removal of the defective restorations,
teeth nos. 45 and 46 were isolated with a rubber dam (Fig. 1B). The previous filling material
and secondary caries were removed and the pulp mummification
materials within the pulp chamber were accessed. Furthermore, an
endodontic ultrasound ET20 tip compatible with the Suprasson P5
Newtron device (both Acteon; Satelec), was employed to clear the
pulp cavity of calcified and necrotic tissue. Subsequently, marked
calcification was noted on the chamber floor, which appeared light
brown and complicated the identification of the root canal
orifices. With the aid of a dental operating microscope (DOM; Zumax
Medical Co., Ltd.), a DG-16 endodontic explorer (Hu-Friedy) was
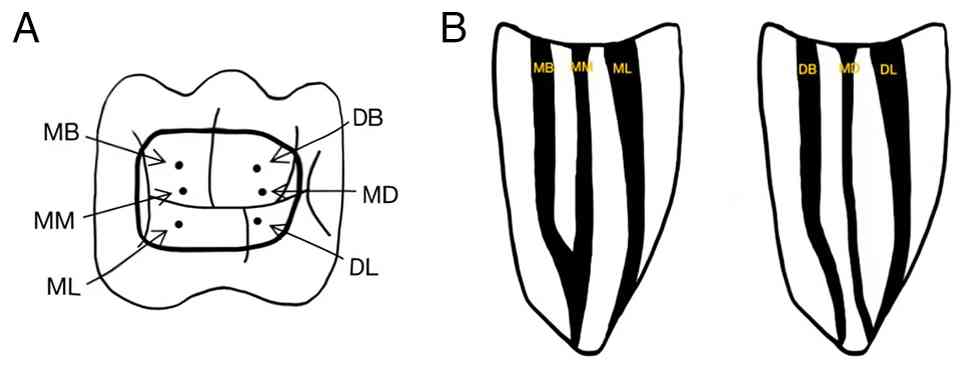
used to probe the root canal orifices and the orifices of the
mesiobuccal (MB), mesiolingual (ML), distobuccal (DB) and
distolingual (DL) canals were initially detected. The wide
separation of the MB and ML orifices raised suspicions of
additional root canals. An ET25 ultrasonic tip (Acteon) was used to
remove the calcified tissue in the isthmus between these orifices.
The ‘champagne bubble test’ (22)
was applied by flooding the pulp chamber with 3% sodium
hypochlorite (NaClO). The effervescence rising from the isthmus
areas guided the tip of a DG-16 explorer, leading to the
identification of an additional middle mesial (MM) canal. The same
method between the DL and DB orifices revealed the middle distal
(MD) root canal.
Preoperative radiographic images revealed a
narrowed, blurred root canal contour, suggestive of diffuse
calcification. During the initial attempt at canal negotiation with
stainless steel hand files, the operator encountered calcification
in the upper portion of the root canal. Under direct visualization
of the DOM, the ultrasonic ET20 tip was used cautiously to remove
calcified deposits and establish straight-line access to the
coronal portion of the canal. However, due to limited visibility,
negotiating the apical portion, particularly in curved, narrowed
segments, posed notable challenges, increasing the risk of root
perforation or file fracture. To decrease potential complications,
a staged approach utilizing C+ files was employed to address the
apical segment. This strategy leveraged the high flexural strength
of C+ files, in combination with EDTA irrigation, to lubricate the
canal and facilitate debris removal. The canal was instrumented to
the apical foramen, with the working length determined using the
electronic Root ZX II Apex Locator (J. Morita Corp.). A total of
six root canals were prepared in tooth no. 46, including three
mesial canals (ML, MM and MB) and three distal canals (DL, MD and
DB). During root preparation, it was observed that the MM canal was
confluent with the MB canal at the apical third, while the distal
root comprised three separate canals. The canals were shaped using
ProTaper Gold rotary instruments (Dentsply Sirona) with a
crown-down instrumentation technique (23). The ultimate dimension size was
achieved by expanding from the initial file by three sizes. For the
narrow additional root canals (MM and MD), a conservative shaping
strategy using the TruNatomy system (Dentsply Sirona) was adopted
to avert excessive dentin removal and lateral root perforation. MB,
ML, DB and DL canals were prepared to an F3 file size, the MM canal
expanded to an F2 size and the MD canal was shaped to an apical
diameter of 0.20 mm with a 4% taper (Fig. 1C and D). Throughout the mechanical preparation
phase, each root canal was irrigated with 20 ml 3% NaClO using
conventional syringe irrigation to ensure adequate and thorough
debridement. This was followed by ultrasonic (27-32 kHz) agitation,
performed 3 times per canal, with each cycle lasting 20 sec. A
photodynamic disinfection system (EasyinSmile) was used to enhance
root canal disinfection. A low-viscosity thionine blue, acting as
the photosensitizer (PS), was injected into each root canal,
followed by agitation with an endo activator (EasyinSmile) to
ensure uniform distribution. The activator tip was positioned 2 mm
from the apex, activated for 30 sec and repeated twice. Residual PS
was removed by irrigation with 10 ml sterile saline, after which
the canals were dried with absorbent paper points, filled with
calcium hydroxide and the coronal portion was sealed with
glass-ionomer cement.
At the 10-day follow-up, the patient reported
improvement, experiencing no discomfort in the affected tooth.
Vertical percussion of tooth no. 46 elicited no pain and the sinus
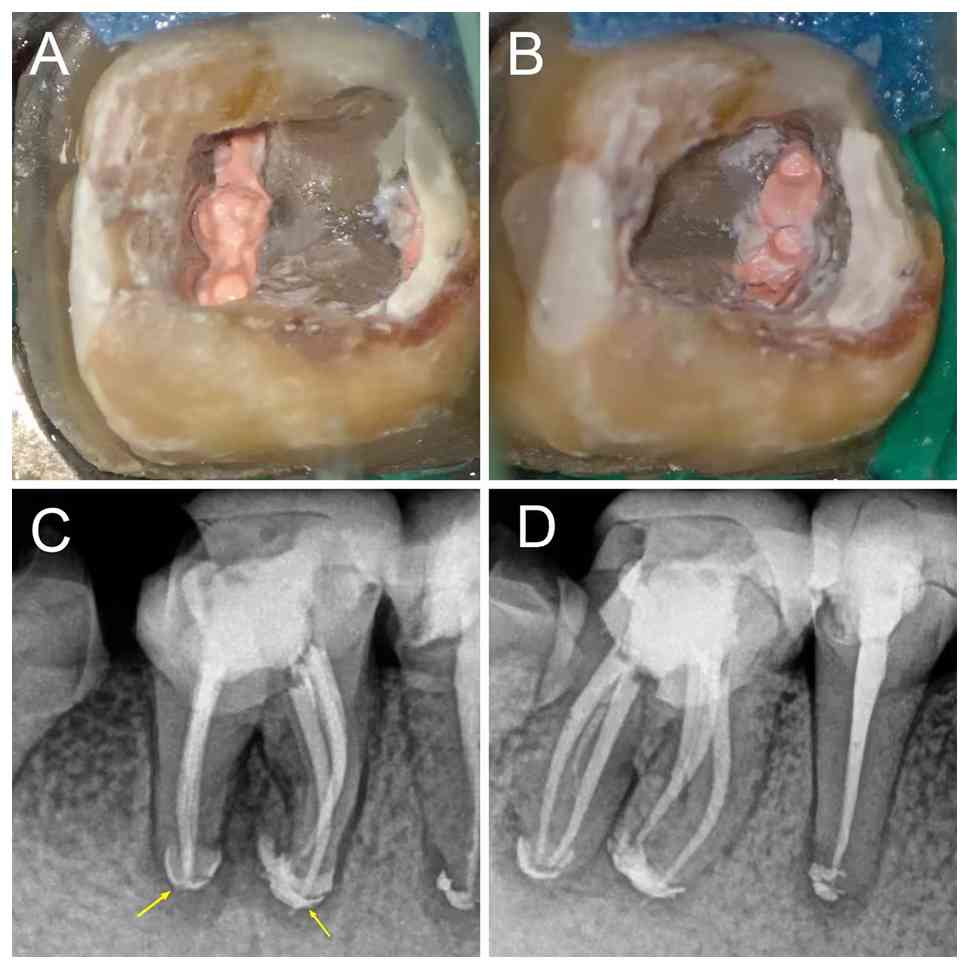
tract had resolved. The tooth was isolated with a rubber dam and
the root canal was rinsed using 20 ml 3% NaClO and ultrasonic
activation before being obturated with the ‘continuous wave of
condensation’ technique (24)
using gutta-percha and iRoot SP bioceramic sealer (Innovative
BioCeramix, Inc.; Fig. 2A and
B). The root canal orifices were
sealed with Filtek™ Z350 XT flowable composite resin (3M
ESPE; 3M Deutschland GmbH), and the crown was restored using
Filtek™ P60 composite resin (3M ESPE; 3M Deutschland
GmbH). Postoperative multi-angle radiographs confirmed the correct
placement of the gutta-percha cones. Notably, some iRoot SP paste
extruded from the apical foramen to ensure maximal sealing
(Fig. 2C and D). After completing the root canal
treatment, the patient was referred to the Department of
Prosthodontics at Chengdu Third People's Hospital (Sichuan, China)
for the fabrication of a full ceramic crown to protect tooth no.
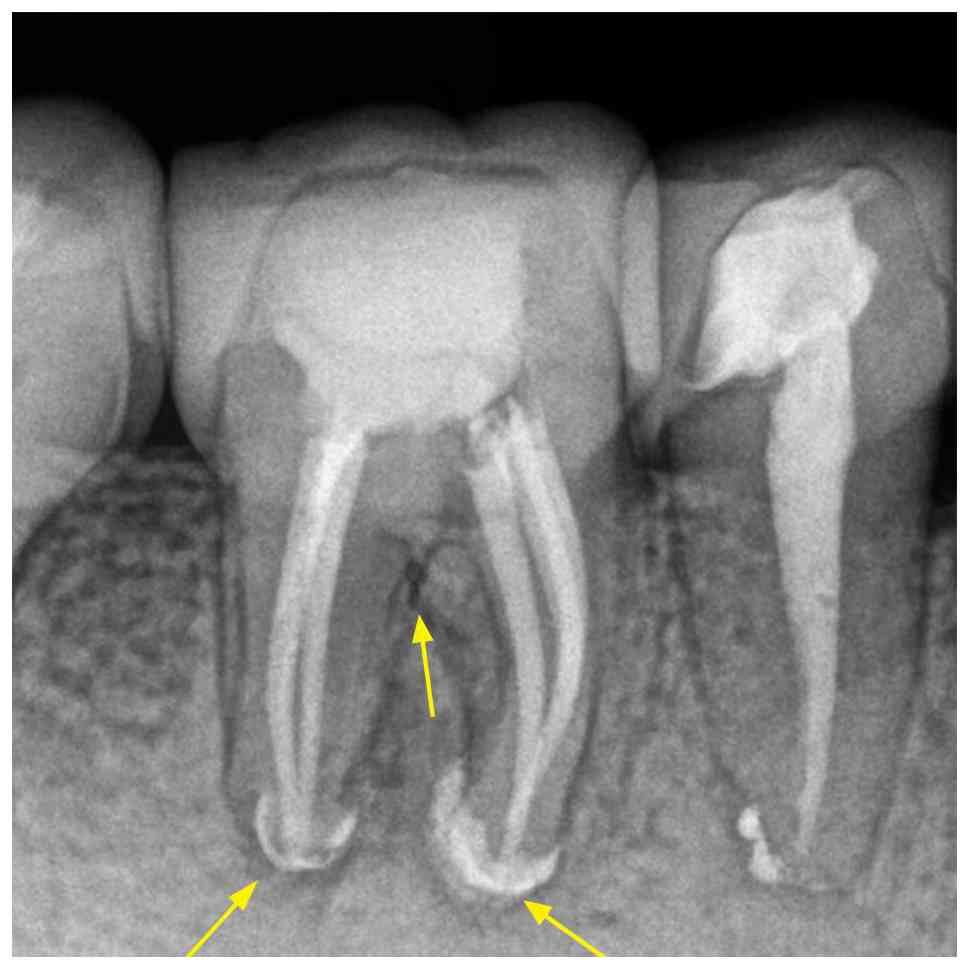
46. At the 6 month follow-up (June 2024), the patient reported no
discomfort with the treated tooth no. 46. Clinical examination
revealed healthy surrounding gingiva without redness or swelling, a
negative percussion response and normal periodontal probing depths.
Furthermore, X-ray images exhibited a successful non-surgical root
canal treatment, with a visible decrease in the dark shadow
surrounding the furcation and root apex. A residual high-density
radiopaque area corresponding to the extruded sealer was observed
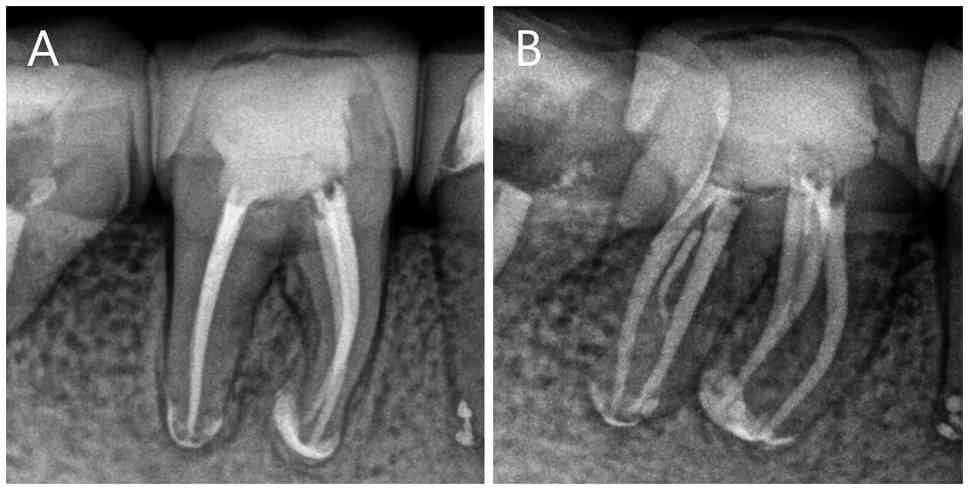
(Fig. 3). At 24 month follow-up in
November 2025, the patient remained asymptomatic. Multi-angle
radiographic evaluation revealed complete resolution of the
periapical and furcation radiolucencies, with a decrease in the
extent of the extraradicular high-density area (Fig. 4A and B). Thus, continuous follow-up every 6-12
months with the patient is important; if the patient experiences
unresolved periapical inflammation or recurrent discomfort, apical
surgery may be considered.
Discussion
The present case demonstrated notable challenges due
to complex and variable root canal morphology, specifically due to
the presence of six canals, including the MMC and MDC. Procedural
complexity was increased by calcification that obscured canal
orifices, limited visualization and the inherent difficulties
associated with non-surgical endodontic retreatment, including the
removal of resistant filling materials and regaining apical
patency. According to the classification system for root and root
canal morphology outlined by Ahmed et al (25), tooth no. 46 presented with two
roots, a mesial root classified as M3-2 (three canals,
with the MB and MM canals merging in the apical third and the ML
canal remaining separate) and a distal root classified as
D3-3 (three independent canals). Thus, the overall
configuration of this tooth was
246M3-2D3-3 (Fig. 5). The majority of reported cases
with additional root canals have described a confluent
configuration (9,10,12-16,18).
However, cases featuring three separate root canals (11,17,20)
are rare. Since Vertucci and Williams (26) identified the presence of MMC in the
mandibular first molar in 1974, considerable research (8,9,27)
has been conducted on the incidence of MMC. Results have varied
widely, influenced by factors such as sample size, methodology,
instrumentation and the technical proficiency of researchers. The
incidence of MMC ranges from 0.26 to 45.8% (8), with a prevalence of 1.9% identified
in the Chinese population in a study by Ni et al (27). The occurrence of MDC is rarer, with
reports varying from 0.2 to 3.0% (9).
CBCT is a diagnostic tool in contemporary endodontic
practice (28). By generating
ultra-thin cross-sectional images from multiple angles, CBCT
minimizes geometric distortion, image elongation and shortening
(29). However, the routine use of
CBCT remains controversial due to the high radiation exposure
(30) and cost. In the present
case, the absence of CBCT data compromised the accurate assessment
of root canal morphology. When CBCT imaging is unavailable,
conventional periapical radiographs alone are often insufficient to
visualize the complexity and number of root canals. In such
situations, the use of multi-angled radiographic projections may
enhance diagnostic accuracy. Additionally, the DOM and ultrasonic
instruments are key for identifying and negotiating concealed
canals while preserving the remaining tooth structure. The DOM
provides notable magnification and illumination, enhancing the
visibility of the pulp chamber and chamber floor (31). The enhanced view offered by DOM
allows dental ultrasonic devices to remove dentin debris or
calcification with greater precision and clarity than conventional
handpieces (32). When used in
conjunction with the microprobe DG-16, meticulous probing along the
sulcus increases the likelihood of discovering additional canals.
Despite the limitations posed by the absence of CBCT in the present
case, the MMC and MDC were identified using multi-angle X-ray
apical radiographs and magnification equipment. Other methods for
identifying variant root canals include staining the floor of the
pulp chamber with 1% methylene blue dye, performing the champagne
bubble test with NaClO, guided troughing techniques or the ‘red
line test’ (33).
Another challenge in the present case was the
retreatment of calcified root canals. The patient had undergone
pulp mummification 15 years ago, with recurrent signs developing.
Pulp mummification therapy aims to coagulate and necrose tissue and
microorganisms near the mummifying agents, rather than achieving
thorough cleaning and disinfection of the root canal (34). Such treatment typically results in
conditions such as residual pulpitis and chronic or acute
periapical inflammation due to incomplete treatment (4). Although calcification may partially
seal the root canal system, it complicates subsequent cleaning,
disinfection and filling if the initial treatment fails. Effective
retreatment of calcified canals requires the correct selection of
rotary files and preparation techniques (35). The C+ file is suitable due to its
high resistance to bending, which allows it to navigate calcified
canals without distortion (36).
Manual files, used alongside EDTA or NaClO, not only serve as
lubricants but also facilitate the removal of debris and smear
layers from the canal (37). In
mechanical preparation, it is typically advisable to increase the
working width of the root canal to remove more infected dentin
(38). However, additional root
canal variations typically present as narrow, tortuous, curved or
communicating with one of the primary root canals. The final
working width should be controlled to avoid excessive dentin
removal, which may weaken the root structural integrity or result
in lateral root perforation (39).
Mechanical preparation alone is typically insufficient to
completely remove tissue debris and bacterial biofilms, especially
in small or irregularly shaped root canals. As a result, effective
cleaning and disinfection require the integration of complementary
irrigation techniques (40,41).
Traditional syringe irrigation, sonic, ultrasonic and negative
pressure irrigation systems have been adopted (42). These methods enhance debris removal
and more effectively eradicate bacterial biofilms in the apical
regions (43).
Root canal obturation represents the final stage of
endodontic therapy and aims to hermetically seal the canal system
and eliminate residual microorganisms. Optimal obturation is
achieved when the filling material terminates precisely at the
apical foramen (44). However,
apical inflammation or operator-induced over-preparation may result
in sealer extrusion (45). Owing
to its superior biocompatibility, iRoot SP is used in contemporary
obturation protocols (46).
Previous studies have shown that extruded iRoot SP may undergo
gradual dissolution in periapical tissue fluids, followed by
phagocytosis or encapsulation by fibrous tissue (47-49).
Another investigation reported that iRoot SP extrusion does not
adversely affect periapical healing (50). Ultimately, the clinical outcome is
influenced by both the composition and the amount of extruded
sealer. Thus, long-term follow-up is key in patients with sealer
extrusion. This represents another limitation of the present
report. The presence of a high-density image beyond the apical area
in X-ray films suggested extrusion of the sealer material following
root canal obturation. Across the follow-up period, the suspicious
area of high density appeared to decrease. However, this may still
lead to variations in treatment outcomes.
In conclusion, the present report demonstrated that
successful retreatment of a mandibular first molar with six canals
is achievable through systematic canal exploration and disciplined
operative strategies, even without CBCT. Clinicians should suspect
additional canals when encountering atypical chamber anatomy or
calcification and rely on multi-angled radiographs, DOM-assisted
inspection and ultrasonic troughing to localize hidden orifices.
Careful long-term follow-up is recommended, particularly when
sealer extrusion or extensive root calcification is present.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
ML managed the treatment of the patient, conceived
the study and collected the clinical data. CW was responsible for
analyzing and interpreting the data and wrote the manuscript. ML
and CW confirm the authenticity of all the raw data. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
Informed consent was obtained from the patient for
all diagnostic and therapeutic procedures described in the present
case report. In addition, approval was granted by the Ethics Review
Board of Chengdu Third People's Hospital (approval no.
2025-S-83).
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of the present case report and any
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ørstavik D and Pitt Ford TR: Essential
Endodontology: Prevention and Treatment of Apical Periodontitis.
Blackwell Science, Oxford, 1998.
|
|
2
|
Trope M: The vital tooth-its importance in
the study and practice of endodontics. Endod Topics. 5(1)2003.
|
|
3
|
Wu MK, R'oris A, Barkis D and Wesselink
PR: Prevalence and extent of long oval canals in the apical third.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 89:739–743.
2000.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Nair PNR: Pathogenesis of apical
periodontitis and the causes of endodontic failures. Crit Rev Oral
Biol Med. 15:348–381. 2004.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Wayman BE, Patten JA and Dazey SE:
Relative frequency of teeth needing endodontic treatment in 3350
consecutive endodontic patients. J Endod. 20:399–401.
1994.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Skidmore AE and Bjorndal AM: Root canal
morphology of the human mandibular first molar. Oral Surg Oral Med
Oral Pathol. 32:778–784. 1971.PubMed/NCBI View Article : Google Scholar
|
|
7
|
AL-Rammahi HM, Chai WL, Nabhan MS and
Ahmed HMA: Root and canal anatomy of mandibular first molars using
micro-computed tomography: A systematic review. BMC Oral Health.
23(339)2023.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Penukonda R, Pattar H, Nambiar P and
Al-Haddad A: Middle mesial canal in mandibular first molar: A
narrative review. Saudi Dent J. 35:468–475. 2023.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Hasan M, Rahman M and Saad N: Case Report:
Mandibular first molar with six root canals: A rare entity. BMJ
Case Rep. 2014(bcr2014205253)2014.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Ramachandran VS, Vidhya Shankari S,
Rathakrishnan M, Chandrasegaran V and Kumaraguru K: Management of
three rooted mandibular first molar with six canals: A case report.
Cureus. 11(e6280)2019.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Jabali AH: Middle mesial and middle distal
canals in mandibular first molar. J Contemp Dent Pract. 19:233–236.
2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Martins JN and Anderson C: Endodontic
treatment of the mandibular first molar with six roots canals-two
case reports and literature review. J Clin Diagn Res. 9:ZD06–ZD08.
2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Baziar H, Daneshvar F, Mohammadi A and
Jafarzadeh H: Endodontic management of a mandibular first molar
with four canals in a distal root by using cone-beam computed
tomography: A case report. J Oral Maxillofac Res.
5(e5)2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Sinha N, Singh B, Langaliya A, Mirdha N,
Huda I and Jain A: Cone beam computed topographic evaluation and
endodontic management of a rare mandibular first molar with four
distal canals. Case Rep Dent. 2014(306943)2014.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Acharya N, Singh A, Samant PS and Gautam
V: Endodontic management of radix paramolaris with six canals: A
clinical case report. Kathmandu Univ Med J (KUMJ). 11:338–341.
2013.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Gupta S, Jaiswal S and Arora R: Endodontic
management of permanent mandibular left first molar with six root
canals. Contemp Clin Dent. 3 (Suppl 1):S130–S133. 2012.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Ryan JL, Bowles WR, Baisden MK and
McClanahan SB: Mandibular first molar with six separate canals. J
Endod. 37:878–880. 2011.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Aminsobhani M, Shokouhinejad N, Ghabraei
S, Bolhari B and Ghorbanzadeh A: Retreatment of a 6-canalled
mandibular first molar with four mesial canals: A case report. Iran
Endod J. 5:138–140. 2010.PubMed/NCBI
|
|
19
|
Yesilsoy C, Porras O and Gordon W:
Importance of third mesial canals in mandibular molars: Report of 2
cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.
108:e55–e58. 2009.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Lee SJ, Jang KH, Spangberg LSW, Kim E,
Jung IY, Lee CY and Kum KY: Three-dimensional visualization of a
mandibular first molar with three distal roots using computer-aided
rapid prototyping. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod. 101:668–674. 2006.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Aminoshariae A, Mackey SA, Palomo L and
Kulild JC: Declassifying mobility classification. J Endod.
46:1539–1544. 2020.
|
|
22
|
Faruqi FA, Mirza AJ and Moosa R: Champagne
bubble test: An authentic method to find hard-to-find canals during
root canal therapy. Acta Sci Dent Sci. 5:68–71. 2021.
|
|
23
|
Morgan LF and Montgomery S: An evaluation
of the crown-down pressureless technique. J Endod. 10:491–498.
1984.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Buchanan LS: The continuous wave of
condensation technique: A convergence of conceptual and procedural
advances in obturation. Dent Today. 13:80–82, 84-85.
1984.PubMed/NCBI
|
|
25
|
Ahmed HMA, Versiani MA, De-Deus G and
Dummer PMH: A new system for classifying root and root canal
morphology. Int Endod J. 50:761–770. 2017.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Vertucci FJ and Williams RG: Furcation
canals in the human mandibular first molar. Oral Surg Oral Med Oral
Pathol. 38:308–314. 1974.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Ni N, Cao S, Han L, Zhang L, Ye J and
Zhang C: Cone-beam computed tomography analysis of root canal
morphology in mandibular first molars in a Chinese population: A
clinical study. Evid Based Endod. 3(1)2018.
|
|
28
|
Ahmed HMA: A critical analysis of
laboratory and clinical research methods to study root and canal
anatomy. Int Endod J. 55 (Suppl 2):S229–S280. 2022.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Patel S, Dawood A, Ford TP and Whaites E:
The potential applications of cone beam computed tomography in the
management of endodontic problems. Int Endod J. 40:818–830.
2007.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Cohnen M, Kemper J, Möbes O, Pawelzik J
and Mödder U: Radiation dose in dental radiology. Eur Radiol.
12:634–637. 2002.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Keleş A and Keskin C: Detectability of
middle mesial root canal orifices by troughing technique in
mandibular molars: A micro-computed tomographic study. J Endod.
43:1329–1331. 2017.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Mendes EB, Soares AJ, Martins JNR, Silva
EJNL and Frozoni MR: Influence of access cavity design and use of
operating microscope and ultrasonic troughing to detect middle
mesial canals in extracted mandibular first molars. Int Endod J.
53:1430–1437. 2020.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Mohammadi Z, Asgary S, Shalavi S and
Abbott PV: A clinical update on the different methods to decrease
the occurrence of missed root canals. Iran Endod J. 11:208–213.
2016.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Reshmi B: Pulp mummification agents used
in dentistry. J Pharm Sci Res. 12:1544–1545. 2020.
|
|
35
|
Peters OA: Current challenges and concepts
in the preparation of root canal systems: A review. J Endod.
30:559–567. 2004.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Lopes HP, Elias CN, Mangelli M, Lopes WSP,
Amaral G, Souza LC and Siqueira JF Jr: Buckling resistance of
pathfinding endodontic instruments. J Endod. 38:402–404.
2012.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Chen G and Chang YC: Effects of liquid-
and paste-type EDTA on smear-layer removal during rotary root-canal
instrumentation. J Dent Sci. 6:41–47. 2011.
|
|
38
|
Aminoshariae A and Kulild JC: Master
apical file size-smaller or larger: A systematic review of healing
outcomes. Int Endod J. 48:639–647. 2015.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Kılıç Y, Karataşlıoğlu E and Kaval ME: The
effect of root canal preparation size and taper of middle mesial
canals on fracture resistance of the mandibular molar teeth: An in
vitro study. J Endod. 47:1467–1471. 2021.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Metzger Z, Solomonov M and Kfir A: The
role of mechanical instrumentation in the cleaning of root canals.
Endod Topics. 29:87–109. 2013.
|
|
41
|
Siqueira Junior JF, Rôças IDN,
Marceliano-Alves MF, Pérez AR and Ricucci D: Unprepared root canal
surface areas: Causes, clinical implications, and therapeutic
strategies. Braz Oral Res. 32 (Suppl 1)(e65)2018.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Gu LS, Kim JR, Ling J, Choi KK, Pashley DH
and Tay FR: Review of contemporary irrigant agitation techniques
and devices. J Endod. 35:791–804. 2009.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Kumar K, Teoh YY and Walsh LJ: Root canal
cleaning in roots with complex canals using agitated irrigation
fluids. Aust Endod J. 49:56–65. 2023.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Kim S, Jung H, Kim S, Shin SJ and Kim E:
The influence of an isthmus on the outcomes of surgically treated
molars: A retrospective study. J Endod. 42:1029–1034.
2016.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Ricucci D and Langeland K: Apical limit of
root canal instrumentation and obturation, part 2. A histological
study. Int Endod J. 31:394–409. 1998.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Zhang W, Li Z and Peng B: Ex vivo
cytotoxicity of a new calcium silicate-based canal filling
material. Int Endod J. 43:769–774. 2010.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Li J, Chen L, Zeng C, Liu Y, Gong Q and
Jiang H: Clinical outcome of bioceramic sealer iRoot SP extrusion
in root canal treatment: A retrospective analysis. Head Face Med.
18(28)2022.PubMed/NCBI View Article : Google Scholar
|
|
48
|
de Miranda Candeiro GT, Correia FC, Duarte
MAH, Ribeiro-Siqueira DC and Gavini G: Evaluation of radiopacity,
pH, release of calcium ions, and flow of a bioceramic root canal
sealer. J Endod. 38:842–845. 2012.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Yoshino P, Nishiyama CK, Modena KC, Santos
CF and Sipert CR: Histological evaluation of the biocompatibility
of three root canal sealers. J Endod. 39:1401–1406. 2013.
|
|
50
|
Chybowski EA, Glickman GN, Patel Y, Fleury
A, Solomon E and He J: Clinical outcome of non-surgical root canal
treatment using a single-cone technique with endosequence
bioceramic sealer: A retrospective analysis. J Endod. 44:941–945.
2018.PubMed/NCBI View Article : Google Scholar
|