Introduction
Cancer pain is a common and challenging complication
in patients with malignant tumors, which seriously affects their
quality of life. Bone metastasis is one of the most notable causes
of cancer pain (1).
Epidemiological studies have demonstrated that bone metastases
occur in 65-75% of patients with advanced breast cancer and
prostate cancer, and in 30-40% of patients with lung cancer
(2). Furthermore, ~70% of patients
with bone metastases experience moderate-to-severe pain, making it
a notable clinical burden (3). The
majority of patients with advanced tumors experience cancer pain,
and the pain caused by bone metastases is particularly severe,
which has a notable impact on the quality of life of the patients
and their survival (4). In China,
the incidence of cancer pain ranges from 40-90%, reaching >80%
in patients with advanced malignant tumors. Approximately one-third
of these patients suffer from moderate-to-severe pain, with some
patients experiencing persistent pain until mortality (5).
Opioids are currently the first-line drugs for the
treatment of moderate-to-severe cancer pain and common opioids
include oxycodone hydrochloride controlled-release tablets,
morphine, oxycodone and fentanyl. Morphine, as a representative of
opioids, is a potent analgesic that can effectively relieve all
types of severe pain, but long-term use is prone to tolerance and
dependence, with risk of additional adverse effects, including
constipation, nausea, vomiting and respiratory depression (6). Oxycodone is a semi-synthetic opioid
with dual receptor agonism, precise analgesic effect and good
relief for moderate-severe pain (7). Oxycodone hydrochloride
controlled-release tablets utilize unique controlled-release
technology that allows the drug to be released slowly in vivo,
maintaining a stable blood concentration and prolonging the
duration of analgesia (8,9). Fentanyl, on the other hand, is a
potent opioid analgesic with a rapid onset and short duration of
analgesic action and is commonly used for anesthesia-assisted
analgesia and the management of breakthrough pain (10). Studies have shown that long-term
use of opioids is prone to drug resistance and multiple adverse
effects, such as constipation, nausea, vomiting and respiratory
depression, thereby reducing the treatment compliance of the
patient and their overall quality of life (11,12).
Therefore, how to reduce the dosage and adverse effects of opioids
while effectively controlling pain is a key issue in the field of
cancer pain management for bone metastases that needs to be
urgently addressed.
Gabapentin is a γ-aminobutyric acid analogue with an
analgesic mechanism that inhibits neurotransmitter release,
primarily by binding to the α2δ subunit in neuronal voltage-gated
Ca2+ channels (13). Although
gabapentin has a unique analgesic mechanism and good drug
metabolism properties, it does not bind to plasma proteins, but
instead crosses the blood-brain barrier using the L-type amino acid
transporter protein 1(14).
Furthermore, gabapentin does not undergo hepatic metabolism, which
avoids any effect on the hepatic cytochrome P450 system and reduces
interactions with other drugs (15). However, gabapentin needs to enter
the neuronal cytoplasm through a neutral amino acid transporter in
order to be effective (16) and
the limited transport capacity of this transporter results in an
oral bioavailability of only 33-66% (17). Therefore, gabapentin is often used
in combination with analgesic drugs with different mechanisms of
action in order to optimize the analgesic effect. For example, in
clinical practice, gabapentin has been found to have a synergistic
analgesic effect when used in combination with opioids, potentially
reducing the required dose of opioids (18,19).
A number of clinical studies (20-23)
have been conducted on the efficacy of opioids combined with
gabapentin compared with opioids alone in the treatment of
cancer-related pain due to bone metastases from malignant tumors,
but the results of these studies are not yet fully consistent.
These differences may stem from numerous factors including study
design, sample size, interventions and characteristics of the study
population. Therefore, it is necessary to conduct a systematic
evaluation and meta-analysis of the existing studies to
comprehensively assess the differences in efficacy between the two
treatment regimens and to provide more reliable evidence for the
clinical treatment of cancer pain from bone metastases.
Materials and methods
Inclusion and exclusion criteria.
Inclusion criteria
Inclusion criteria ensured the type of study was: i)
A randomized controlled trial (RCT) or non-randomized controlled
trial (NRCT); ii) the study population consisted of patients with a
definitive diagnosis of cancer pain due to bone metastases from
malignant tumors, regardless of cancer type or stage; iii) the
intervention was gabapentin in combination with opioid regimen; iv)
the control group was treated with opioids alone; and v) the
outcome metrics needed to include the numerical rating scale (NRS)
for assessing pain intensity. No restrictions were placed on
publication language or year.
Exclusion criteria. Exclusion criteria
ensured studies that did not provide complete data or were unable
to extract the required information, case reports, conference
abstracts, review articles and duplicate publications were
excluded.
Search strategy. Scope of search
Searches were conducted using Chinese and English
literature databases including China National Knowledge
Infrastructure (https://www.cnki.net), VIP
(https://www.cqvip.com), Wanfang Data (https://www.wanfangdata.com.cn), PubMed
(https://pubmed.ncbi.nlm.nih.gov), Embase
(https://www.embase.com) and Web of Science
(https://www.webofscience.com). The
search was conducted from the time of database construction to the
21st of November 2024.
Search terms. Chinese words for cancer pain,
cancer-related pain, gabapentin, morphine, oxycodone, oxycodone
hydrochloride controlled-release tablets, fentanyl, tramadol,
codeine and opioids were used as search terms. In English, ‘cancer
pain’, ‘malignant pain’, ‘tumor pain’, ‘oncologic pain’,
‘neoplastic pain’, ‘gabapentin’, ‘neurontin’, ‘morphine’,
‘oxycodone’, ‘fentanyl’, ‘tramadol’ and ‘opioid’ were used as
search terms. The specific search strategies are detailed in
Table SI.
Literature data extraction and quality
assessment. Data extraction
Data screening and extraction was carried out
independently by two researchers. Duplicate entries were eliminated
at the initial screening stage using EndNote X9.3.3 (Clarivate)
software and literature unrelated to the study topic was screened
by reading the title and abstract. In cases of disagreement at the
initial screening stage, a third researcher was sought to discuss
and reach an agreement. Extracted information included basic
information about the included studies, study population and
interventions, risk of bias assessment, outcome indicators and
outcome measure data.
Quality assessment. A systematic approach was
used in the present study to assess the risk of bias and
methodological quality of the included literature. For RCTs, the
Cochrane Risk of Bias Assessment Tool (24) was applied. Furthermore, for NRCTs,
the Newcastle-Ottawa Scale (25)
was used. The two types of studies were carefully evaluated
separately, starting with the key areas of randomization, blinding
and confounding control. Evaluations were completed independently
by two researchers and disagreements were resolved through a
discussion or third-party arbitration. Studies were finally
categorized according to the risk of bias level (‘high’, ‘medium’
or ‘low’).
Outcome indicator. Pain score was the main
indicator of outcome and was assessed by the NRS.
Statistical processing
Meta-analysis was performed using R software
(version 4.3.0; Posit Software, PBC) with the ‘meta’ package
(26). Pain scores were described
by mean difference (MD). Estimation intervals for overall
parameters are expressed as 95% CIs. Random-effects models were
used for all pooled analyses regardless of the I2
values. Statistical heterogeneity was assessed using the Q test and
the I2 statistic. Z-tests were used to analyze the
combined statistics. Subgroup analyses were performed based on
study type (RCT vs. NRCT), sample size (small, <40 patients per
group vs. large, ≥40 patients per group) and treatment regimen
(specific opioid types). Sensitivity analyses using the
leave-one-out method (27) were
conducted to assess the robustness of the findings. Funnel plots
were used to determine publication bias. A test level (α) value of
0.05 was considered to indicate a statistically significant
difference.
Results
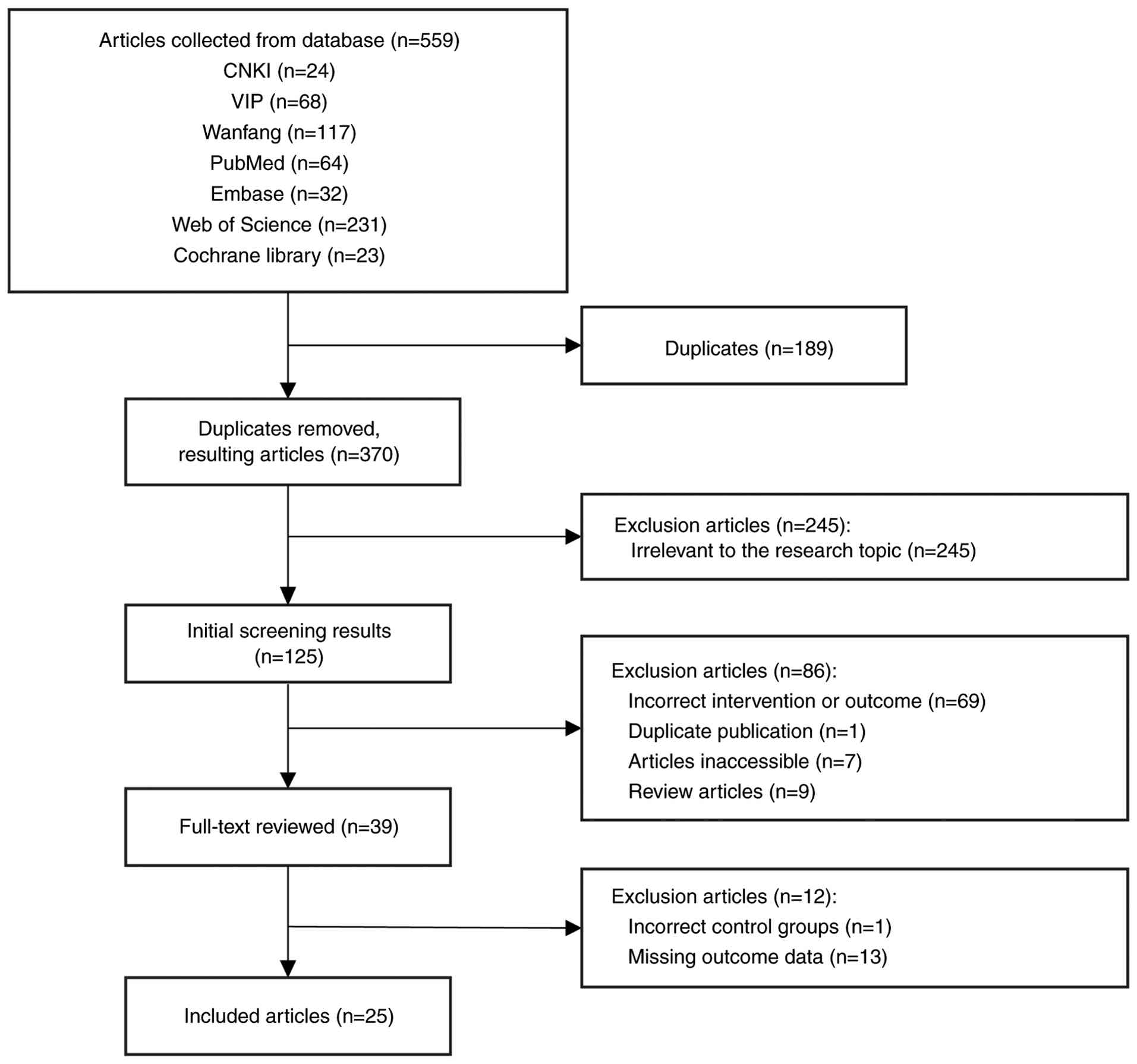
Literature search results
A total of 559 relevant papers were retrieved from
the present literature search and 39 papers were finally assessed
in full text. Among the 39 included literature, 13 studies with
missing data and 1 study with a wrong intervention were further
excluded, leaving 25 studies that met the present study inclusion
criteria retained for meta-analysis (Fig. 1). Among them, 6 studies were NRCTs
and 19 studies were RCTs.
Basic characteristics of the included
literature. A total of 1,805 patients were included in the
present study with 563 patients included across six NRCTs (20,28-32)
and 1,242 patients included in 19 RCTs (33-51).
The mean age of patients ranged from 45-68 years. The majority of
studies included patients with numerous cancer types, with lung,
breast and prostate cancer being the most common primary tumors
associated with bone metastases. Specific information on the
included literature is outlined in Table I.
 | Table IBaseline characteristics of the
included literature. |
Table I
Baseline characteristics of the
included literature.
| | | | Sample size | Ratio of men to
women | Age composition,
years | Intervention | |
|---|
| First author,
year | Study type | Total sample
size | Control | Experimental | Control | Experimental | Control | Experimental | Control | Experimental | (Refs.) |
|---|
| Li et al,
2010 | NRCT | 53 | 32 | 21 | 18:14 | 9:12 | 57.31±13.19 | 57.05±12.38 | Controlled release
oxycodone + gabapentin | Controlled release
oxycodone | (20) |
| Su et al,
2013 | RCT | 80 | 40 | 40 | 21:19 | 22:18 | 57.3±12.9 | 57.5±11.8 | Fentanyl patch +
gabapentin | Fentanyl patch | (33) |
| Liu et al,
2014 | RCT | 41 | 21 | 20 | 14:7 | 12:8 | 60.30±10.48 | 60.30±10.48 | Morphine sulfate
extended-release tablets + gabapentin | Morphine sulfate
extended-release tablets | (34) |
| Qin et al,
2015 | RCT | 40 | 20 | 20 | - | - | - | - | Oxycodone
hydrochloride + gabapentin | Oxycodone
hydrochloride | (35) |
| Chen et al,
2015 | RCT | 61 | 30 | 31 | 18:12 | 17:14 | 67.4±12.1 | 66.7±11.9 | Morphine sulfate
extended-release tablets + gabapentin | Morphine sulfate
extended-release tablets | (36) |
| Zhang, 2016 | RCT | 90 | 45 | 45 | 0:21 | 23:22 | 47.0±2.9 | 49.6±2.5 | Morphine sulfate
extended-release tablets + gabapentin | Morphine sulfate
extended-release tablets | (37) |
| Zhang et al,
2016 | RCT | 42 | 21 | 21 | - | - | 51 | 51 | Morphine
hydrochloride extended-release tablets + gabapentin | Morphine
hydrochloride extended-release tablets | (38) |
| Zhao, 2016 | NRCT | 118 | 118 | 118 | 18:52 | 18:52 | 52.7±9.8 | 52.7±9.8 | Morphine +
Gabapentin | Morphine | (28) |
| Chen et al,
2017 | RCT | 55 | 28 | 27 | 15:13 | 14:13 | 54.5±7.4 | 54.5±7.4 | Oxycodone
hydrochloride + gabapentin | Oxycodone
hydrochloride | (39) |
| Jiang, 2017 | RCT | 80 | 40 | 40 | 19:21 | 22:18 | 58.7 | 58.7 | Oxycodone
hydrochloride controlled-release tablets + gabapentin | Oxycodone
hydrochloride controlled-release tablets | (40) |
| She et al,
2017 | RCT | 100 | 52 | 48 | 31:21 | 30:18 | 58 | 58 | Morphine
hydrochloride extended-release tablets + gabapentin | Morphine
hydrochloride extended-release tablets | (41) |
| Yan et al,
2018 | RCT | 122 | 61 | 61 | - | - | 61 | 61 | Morphine sulfate
extended-release tablets + gabapentin | Morphine sulfate
extended-release tablets | (42) |
| Ru et al,
2018 | RCT | 70 | 36 | 34 | 19:17 | 18:16 | 63±15 | 62±15 | Oxycodone
hydrochloride + gabapentin | Oxycodone
hydrochloride | (43) |
| Fu, 2018 | RCT | 60 | 30 | 30 | 17:13 | 18:12 | 66.81±4.25 | 67.52±4.12 | Morphine sulfate
extended-release tablets + gabapentin | Morphine sulfate
extended-release tablets | (44) |
| Yan, 2018 | RCT | 60 | 30 | 30 | 13:17 | 14:16 | 55.6 | 55.6 | Oxycodone
hydrochloride extended-release tablets + gabapentin | Oxycodone
hydrochloride extended-release tablets | (45) |
| Zhou et al,
2019 | RCT | 65 | 32 | 33 | 17:15 | 18:15 | - | - | Oxycodone
extended-release tablets + gabapentin | Oxycodone
extended-release tablets | (46) |
| Meng, 2019 | RCT | 76 | 39 | 37 | 23:16 | 22:15 | 56.34±6.91 | 56.24±6.75 | Oxycodone
hydrochloride + gabapentin | Oxycodone
hydrochloride | (47) |
| Zhu, 2020 | RCT | 67 | 30 | 37 | 14:16 | 18:19 | 58.59±4.62 | 58.67±4.36 | Morphine sulfate
extended-release tablets + gabapentin | Morphine sulfate
extended-release tablets | (48) |
| Zhao and Xia,
2020 | NRCT | 56 | 28 | 28 | 17:11 | 16:12 | 56.11±9.70 | 52.61±9.51 | Fentanyl patch +
gabapentin | Fentanyl patch | (29) |
| Zhang, 2021 | RCT | 89 | 44 | 45 | 24:20 | 26:19 | 58.46±4.59 | 58.43±4.62 | Oxycodone
hydrochloride + gabapentin | Oxycodone
hydrochloride | (49) |
| Jiang et al,
2021 | NRCT | 84 | 42 | 42 | 27:15 | 26:16 | 58.42±5.18 | 58.39±5.16 | Oxycodone
hydrochloride + gabapentin | Oxycodone
hydrochloride | (30) |
| Sun, 2021 | NRCT | 60 | 30 | 30 | 15:15 | 13:17 | 52.81±13.76 | 52.85±13.73 | Morphine sulfate
extended-release tablets + gabapentin | Morphine sulfate
extended-release tablets | (31) |
| Jiang et al,
2021 | RCT | 50 | 25 | 25 | 16:9 | 18:7 | 51.9±10.7 | 52.4±12.3 | Oxycodone
hydrochloride controlled-release tablets + gabapentin | Oxycodone
hydrochloride controlled-release tablets | (50) |
| Teng et al,
2021 | NRCT | 74 | 34 | 40 | 19:15 | 23:17 | 59.00±6.20 | 57.13±6.09 | Morphine +
gabapentin | Morphine | (32) |
| Qi, 2024 | RCT | 112 | 56 | 56 | 10:22 | 11:21 | 56.06±14.47 | 56.23±14.18 | Oxycodone
hydrochloride + gabapentin | Oxycodone
hydrochloride | (51) |
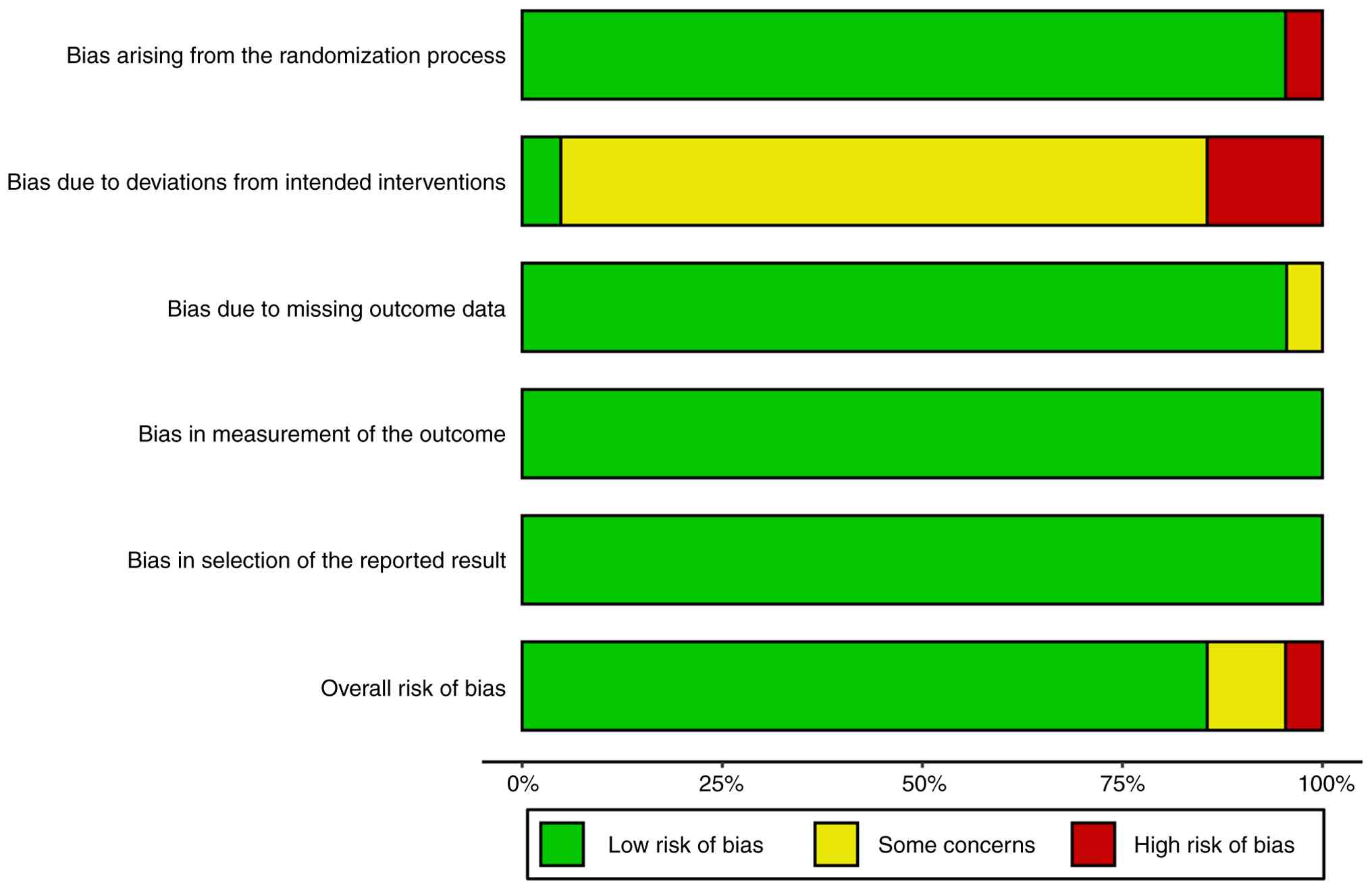
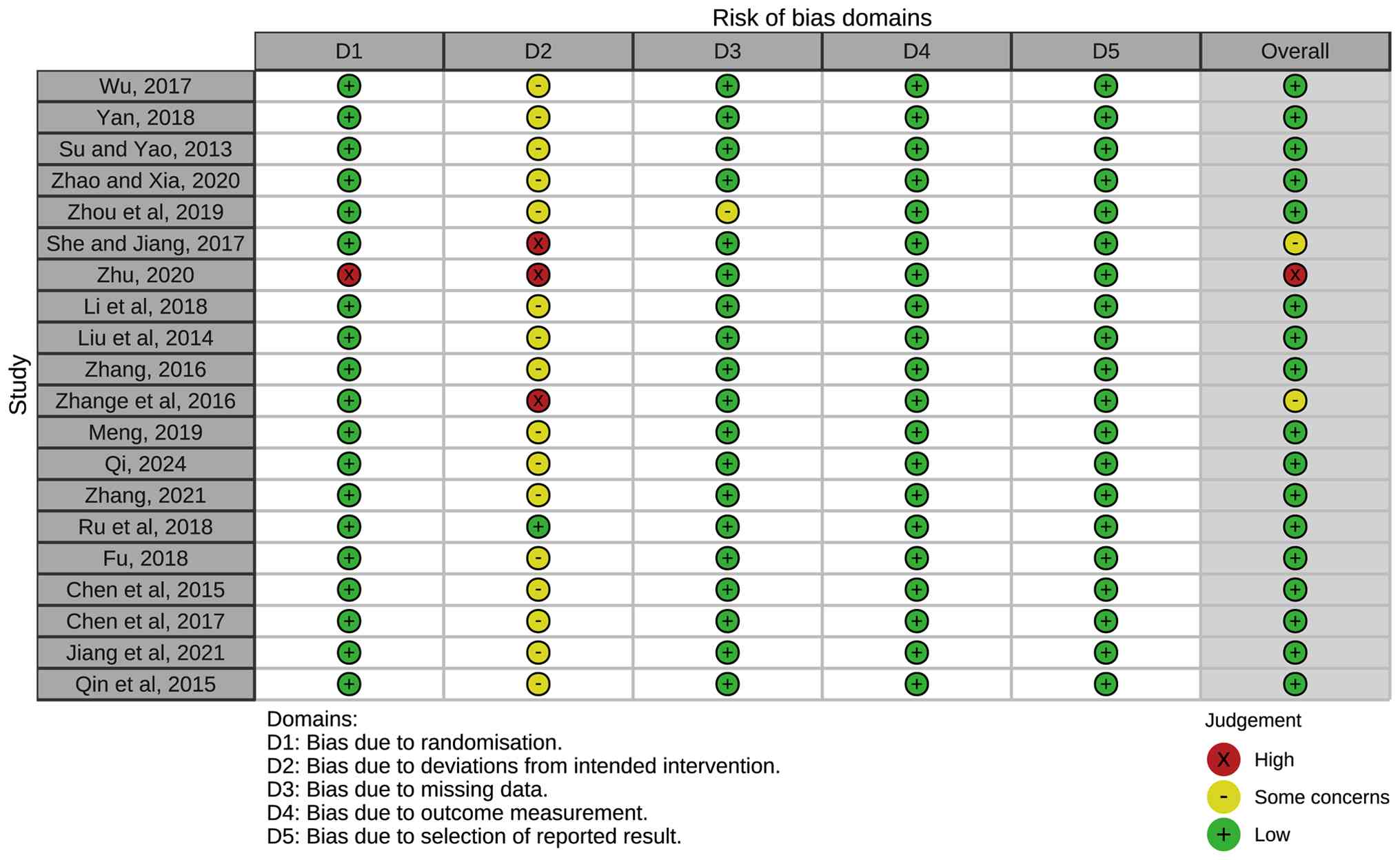
Results of the quality assessment of
the included literature
Overall quality of the included literature was found
to be moderate-high. The RCT quality rating scale is detailed in
Figs. 2 and 3. The majority of RCTs demonstrated
adequate random sequence generation and allocation concealment,
though blinding procedures were not always clearly described. The
overall quality scores of the NRCTs ranged from 5-7 stars, as
detailed in Table II, indicating
acceptable methodological quality with adequate selection of
participants and comparability between groups.
| Table IINewcastle-Ottawa Scale for
non-randomized controlled trials. |
Table II
Newcastle-Ottawa Scale for
non-randomized controlled trials.
| First author,
year | Representativeness
of the exposed group | Selection of
non-exposed groups | Determination of
exposure | No observed outcome
indicators occurred at study entry | Comparability of
exposed and non-exposed groups | Adequacy of outcome
evaluations | Sufficiently long
follow-up | Adequate
follow-up | Total | (Refs.) |
|---|
| Li et al,
2010 | a | - | a | - | - | a | a | a | 5 | (20) |
| Zhao, 2016 | a | a | a | - | b | a | - | - | 6 | (28) |
| Teng et al,
2021 | a | a | a | a | b | a | a | a | 9 | (32) |
| Sun, 2021 | a | a | a | - | b | a | a | - | 7 | (31) |
| Jiang et al,
2021 | a | a | a | - | b | a | - | - | 6 | (30) |
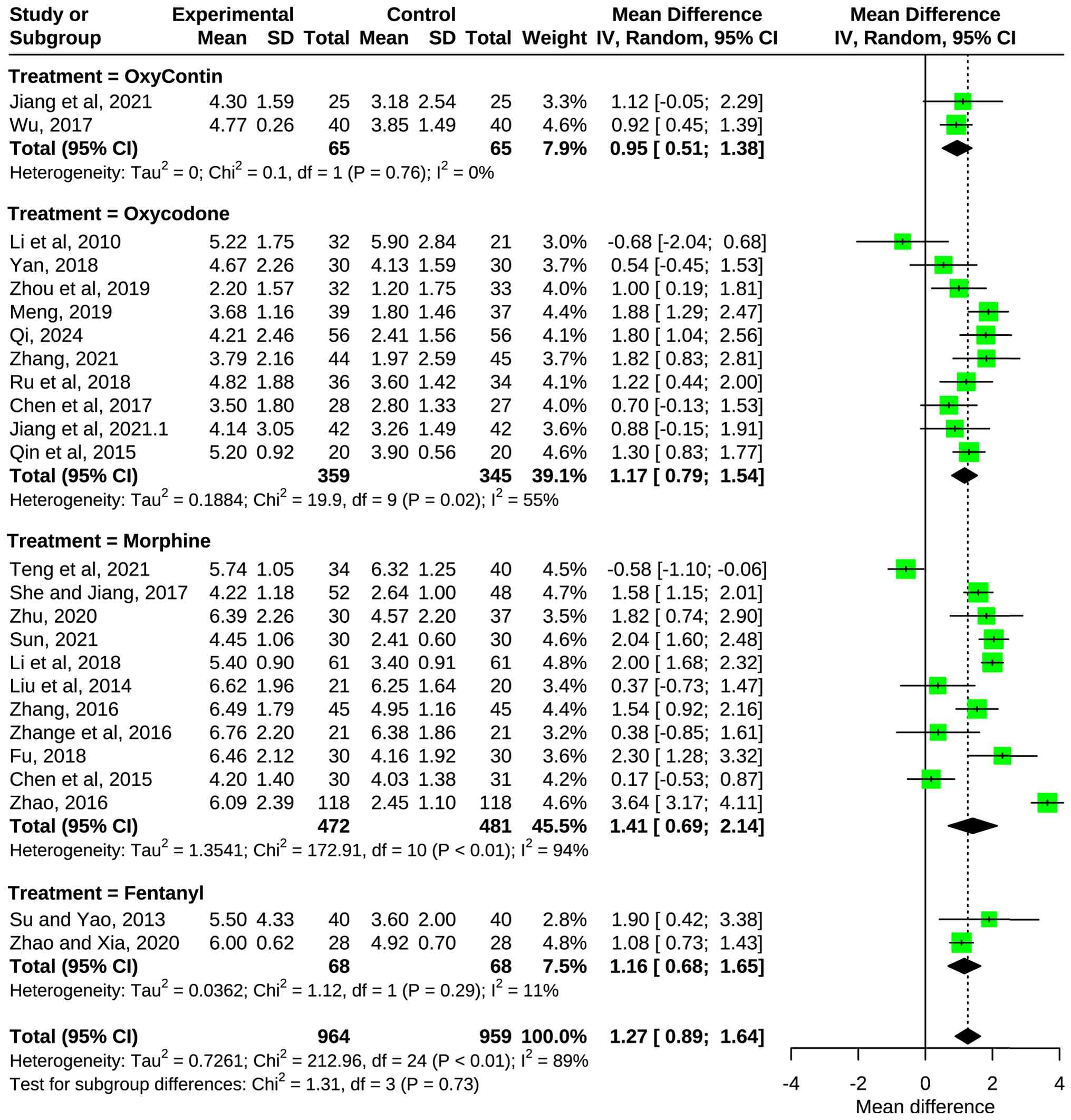
Clinical efficacy. Overall
analysis
In the present study, all 25 included studies used
pain scores as an indicator of clinical efficacy, assessed using
the NRS. The results, shown in Fig.
4, showed that the MD of all studies combined was 1.26 with a
95% CI of 0.88-1.65, indicating that the combination therapy
(oxycodone hydrochloride controlled-release tablets combined with
gabapentin, morphine combined with gabapentin, oxycodone combined
with gabapentin and fentanyl combined with gabapentin) demonstrated
a significant difference and the combination may be more helpful in
reducing pain scores and relieving cancer pain (Z=6.45;
P<0.0001). However, overall, I2=88.7% for all studies
combined, suggesting a high degree of heterogeneity among the 25
included studies.
Subgroup analysis by study type. To explore
potential sources of heterogeneity, subgroup analysis was conducted
based on study type (Fig. S1).
For NRCTs, the pooled MD was 1.11 (95% CI, -0.15-2.37; P=0.08;
I2=96.9%), indicating no significant difference and high
heterogeneity. For RCTs, the pooled MD was 1.31 (95% CI, 1.03-1.59;
P<0.0001; I2=65.0%), demonstrating a significant
analgesic advantage with moderate heterogeneity. The test for
subgroup differences showed no significant difference between RCTs
and NRCTs (P=0.77 for random effects model), suggesting that study
design may not be the primary source of heterogeneity.
Subgroup analysis by sample size. Subgroup
analysis stratified by sample size revealed important differences
(Fig. S2). For studies with small
sample sizes (<40 patients per group), the pooled MD was 0.95
(95% CI, 0.54-1.37; P<0.0001; I2=73.9%), showing
significant efficacy with notable heterogeneity. For studies with
large sample sizes (≥40 patients per group), the pooled MD was 1.57
(95% CI, 0.97-2.17; P<0.0001; I2=92.3%), indicating
even greater efficacy but with higher heterogeneity. The test for
subgroup differences suggested a notable difference between small
and large sample size groups (P=0.10 for random effects model),
indicating that sample size may contribute to heterogeneity and
affect treatment effect estimates.
Subgroup analysis by treatment regimen.
Further subgroup analysis was performed based on the specific
opioid used in combination with gabapentin (Fig. S3). The MD of the oxycodone
hydrochloride controlled-release tablets subgroup was 0.95 (95% CI,
0.51-1.38; I2=0.0%; P=0.76 for heterogeneity), showing
significant efficacy with no heterogeneity. The MD of the oxycodone
subgroup was 1.17 (95% CI, 0.79-1.55, I2=54.8%; P=0.02),
demonstrating significant efficacy with moderate heterogeneity. The
MD of the morphine subgroup was 1.41 (95% CI, 0.68-2.14;
I2=94.2%; P<0.01), showing significant efficacy but
with very high heterogeneity. The fentanyl subgroup MD was 1.16
(95% CI, 0.68-1.65, I2=10.8%; P=0.29 for heterogeneity),
indicating significant efficacy with low heterogeneity. The test
for subgroup differences revealed a significant association
(P=0.0004 for random-effects model), suggesting that the type of
opioid is a significant contributor to the overall
heterogeneity.
Subgroup analysis excluding morphine. Due to
the high heterogeneity observed in the morphine subgroup, a
sensitivity analysis was conducted excluding morphine studies
(Fig. S4). The pooled MD was 1.17
(95% CI, 0.92-1.42; P=0.0449; I2=42.8%), showing that
after removing morphine studies, the overall heterogeneity notably
decreased from 88.7 to 42.8%, while maintaining statistical
significance. This suggests that differences in morphine studies
contribute markedly to the overall heterogeneity.
Subgroup analysis of RCTs only. To provide
the highest level of evidence, only RCTs were analyzed (Fig. S5). The pooled MD for RCTs was 1.31
(95% CI, 1.03-1.59; P<0.0001; I2=65.0%), confirming
the significant benefit of combination therapy even when
restricting analysis to the most rigorous study designs. The
reduced heterogeneity compared with the overall analysis (65.0 vs.
88.7%) suggested that study design does contribute to
heterogeneity, though notable heterogeneity remains even among
RCTs.
Sensitivity analysis. Leave-one-out
sensitivity analysis was performed to assess the influence of
individual studies on the overall results (Fig. S6). Analysis showed that the pooled
MD ranged from 1.22 (95% CI, 0.82-1.63) to 1.36 (95% CI, 1.02-1.71)
when omitting each study sequentially, with all CIs remaining >0
and statistically significant. This indicated that no single study
had an excessive influence on the overall results, confirming the
robustness and reliability of the present findings.
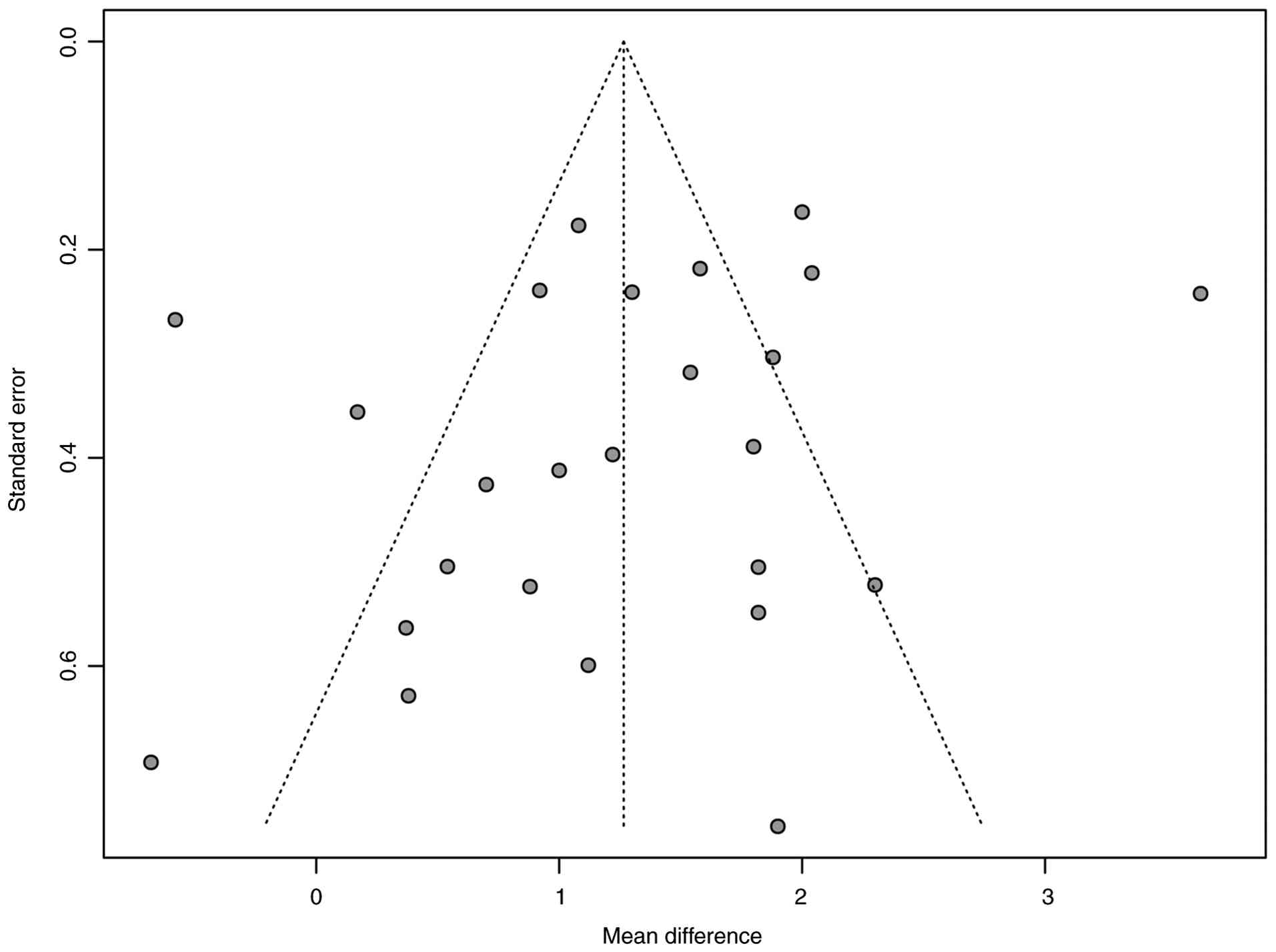
Publication bias
An analysis of publication bias was performed for
all included studies. The results are shown in Fig. 5 and the funnel plot is largely
symmetrical, indicating a low likelihood of publication bias.
Visual inspection of the funnel plot and statistical tests suggest
that the meta-analysis results are unlikely to be notably affected
by unpublished negative studies.
Discussion
The present meta-analysis comprehensively evaluated
the efficacy of opioids combined with gabapentin compared with
opioids alone in treating cancer-related pain due to bone
metastases from malignant tumors. The findings demonstrated that
combination therapy provides improved pain relief compared with
opioid monotherapy, with the pooled MD=1.26 points on the NRS
scale, which represents a clinically meaningful improvement in pain
control.
Opioids have been the primary analgesic drugs for
cancer pain management, but they are more effective for nociceptive
pain and have relatively limited efficacy for neuropathic pain
components. In addition, long-term use of opioids is prone to drug
tolerance, requiring increased dosage or shorter dosing intervals
to maintain pain relief (50). Due
to the more pronounced side effects of opioids, experienced
clinicians tend to favor opioid-based combinations with a view to
controlling cancer pain while reducing the opioid dose (39). For example, a retrospective study
by Shinde et al (51) found
that 80% of patients with cancer pain were treated with a
combination of adjuvant medications.
Gabapentin is a drug with an analgesic mechanism
different from that of opioids with mild and rare side effects. It
is more effective in relieving chronic pain, especially neuropathic
pain, and does not develop tolerance with repeated application
(48). Eckhardt et al
(52) found that gabapentin
increased opioid blood concentrations after adding gabapentin to
opioids used in patients with cancer pain. In patients with cancer
pain and either poor pain control or on a high dose of analgesic
drugs, a combination of drugs could be considered to further
enhance the analgesic effect or reduce the dose of analgesic drugs,
as different types of analgesic drugs exhibit different mechanisms
and can enhance the analgesic effect through numerous pathways.
The present meta-analysis results are consistent
with previous reports. For example, Xinlin et al (53) found that the application of
oxycodone hydrochloride controlled-release tablets combined with
gabapentin in the treatment of neuropathic cancer pain was more
effective compared with that of oxycodone hydrochloride
controlled-release tablets alone (91.67 vs. 70.83%). However, it is
important to note that some individual studies (20,32)
have reported less pronounced benefits or no significant
differences, which may be attributable to variations in study
populations, treatment protocols or methodological limitations.
The high heterogeneity observed in the present
analysis (I2=88.7%) warranted comprehensive subgroup and
sensitivity analyses. The present subgroup analyses revealed that
sources of heterogeneity were significantly associated with
multiple factors. Study type analysis showed that while both RCTs
and NRCTs suggested benefit, RCTs demonstrated more consistent
results with lower heterogeneity (I2=65.0 vs. 96.9%).
Sample size analysis indicated that larger studies tended to show
greater treatment effects, though with higher heterogeneity,
possibly reflecting more diverse patient populations or longer
treatment durations in larger trials.
Most notably, treatment regimen analysis revealed
marked differences among opioid types. The oxycodone hydrochloride
controlled-release tablets subgroup showed the lowest heterogeneity
(I2=0%), suggesting consistent efficacy across studies.
By contrast, the morphine subgroup exhibited high heterogeneity
(I2=94.2%), which may be due to several factors. First,
different formulations of morphine (immediate-release vs.
sustained-release) have different pharmacokinetic profiles and may
interact differently with gabapentin. Second, morphine is
extensively metabolized to active metabolites
(morphine-3-glucuronide and morphine-6-glucuronide) and patient
variability in metabolism could lead to inconsistent responses.
Third, morphine studies included more heterogeneous patient
populations with varying baseline pain severity and cancer types.
When morphine studies were excluded in the present sensitivity
analysis, overall heterogeneity notably decreased to 42.8%, while
maintaining statistical significance, demonstrating that morphine
studies were a notable source of heterogeneity.
The pharmacokinetic and pharmacodynamic properties
of different opioids may explain these differences. Oxycodone
hydrochloride controlled-release tablets provide stable drug
release and consistent blood levels, potentially leading to more
predictable interactions with gabapentin. Oxycodone has dual µ- and
κ-opioid receptor activity, which may synergize differently with
the mechanism of gabapentin. Fentanyl, being highly lipophilic and
potent, may exhibit distinct interaction patterns with gabapentin
(54,55). These mechanistic differences,
combined with variations in study protocols, dosing regimens and
patient characteristics, likely contribute to the observed
heterogeneity.
The present sensitivity analyses, particularly the
leave-one-out analysis, demonstrated that no single study
disproportionately influenced the overall results, demonstrating
the robustness of the present findings. Analysis restricted to RCTs
only provided the highest level of evidence supporting combination
therapy, with maintained significance and reduced heterogeneity
compared with the overall analysis.
Regarding safety considerations, while the primary
focus of the present study was efficacy, the limited reporting of
adverse events in the included studies precluded a comprehensive
meta-analysis of safety outcomes. This represents a notable
limitation, as the clinical decision to use combination therapy
must balance efficacy gains against potential increases in adverse
effects. Gabapentin is generally well-tolerated, with common side
effects including dizziness, somnolence and peripheral edema, which
are typically mild and dose-dependent (56). When combined with opioids, there is
a theoretical concern for additive central nervous system
depression. Future studies should aim to systematically collect and
report adverse event data to enable thorough safety assessments.
Clinicians using combination therapy should carefully monitor
patients for side effects and adjust doses accordingly.
The clinical implications of the present findings
are notable. A reduction of ~1.26 points on the NRS represents a
meaningful improvement for patients with severe cancer pain. This
magnitude of effect may translate to improved function, quality of
life and potentially reduce opioid requirements. However, the
presence of heterogeneity suggests that response to combination
therapy may vary among patients. Factors such as the specific
opioid used, baseline pain characteristics (nociceptive vs.
neuropathic components), patient age, renal function (affecting
gabapentin clearance) and concurrent medications should be
considered when implementing combination therapy.
Despite the clinical importance of the present
study, a number of limitations should be acknowledged. First, while
both RCTs and NRCTs were included to maximize available evidence,
the inclusion of NRCTs may introduce selection bias and
confounding. However, the present subgroup analysis by study type
did not exhibit significant differences and the RCT-only analysis
confirmed the main findings. Second, the languages of the included
studies were limited to Chinese and English, which may introduce
language bias and miss relevant studies published in other
languages. Third, safety could not be adequately assessed due to
inconsistent and incomplete reporting of adverse events across
studies. Fourth, variations in gabapentin dosing regimens (ranging
from 300-1,800 mg daily) and treatment durations across studies may
have contributed to heterogeneity, however this could not be fully
explored due to insufficient data. Fifth, the mechanisms underlying
the apparent differences in efficacy among different opioid types
remain incompletely understood and warrant further investigation.
Sixth, functional outcomes, quality of life measures and opioid
dose reduction were not assessed, which are notable
patient-centered outcomes. Finally, most included studies were from
China, which may limit generalizability to other populations.
Future research should address these limitations
through well-designed, adequately powered RCTs with standardized
outcome reporting, including comprehensive adverse event
monitoring, functional assessments and quality of life measures.
Research should explore optimal dosing strategies for both
gabapentin and opioids in combination therapy, identify patient
characteristics predictive of treatment response, compare different
opioid-gabapentin combinations directly, evaluate long-term
efficacy and safety beyond short-term pain control and investigate
mechanisms of synergy between gabapentin and specific opioids.
Additionally, pharmacoeconomic analyses would help inform clinical
decision-making by evaluating the cost-effectiveness of combination
therapy.
In conclusion, the results of the present
meta-analysis suggest that gabapentin in combination with opioids
is more effective compared with opioids alone for the treatment of
cancer-related pain from bone metastases, with a clinically
meaningful reduction in pain scores. However, notable heterogeneity
exists among studies, particularly related to the type of opioid
used. In clinical application, physicians need to fully consider
the specific conditions of patients, including the type and
severity of pain, prior opioid exposure, renal function and
potential drug interactions, to develop individualized treatment
plans. Careful monitoring for adverse effects is key. The
combination of oxycodone hydrochloride controlled-release tablets
with gabapentin appears particularly promising due to the low
heterogeneity observed in the included studies. Further research is
required to optimize treatment protocols and further understand
patient-specific factors that predict response to combination
therapy.
Supplementary Material
Subgroup analysis by study type (RCT
vs. ANRCT). RCT, randomized controlled trials; NRCT, non-randomized
controlled trials; Exp, experimental; Ctrl, control; MD, mean
difference.
Subgroup analysis by sample size
(small vs. large). MD, mean difference.
Subgroup analysis by treatment regimen
(opioid type). IV, inverse-variance.
Sensitivity analysis excluding
morphine studies. MD, mean difference.
Subgroup analysis including RCTs only.
RCTs, randomized controlled trials.
Leave-one-out sensitivity
analysis.
Search strategy.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
HZ, JF and ZT conceived and designed the study,
performed the literature review and analyzed and interpreted data.
HZ and JF drafted the manuscript. HL, JF and ZT confirm the
authenticity of all the raw data. All authors have read and
approved the final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Zhang Q, Hou L, Liu L, Li H, Chang J and
Feng L: Medication rule of modern traditional chinese medicine
compound prescriptions for the treatment of cancer-induced bone
pain based on data mining. World Chinese Medicine. 18:2815–2819.
2023.
|
|
2
|
Coleman RE: Clinical features of
metastatic bone disease and risk of skeletal morbidity. Clin Cancer
Res. 12:6243S–6249S. 2006.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Mercadante S and Fulfaro F: World Health
Organization guidelines for cancer pain: A reappraisal. Ann Oncol.
16 (Suppl 4):iv132–iv135. 2005.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Chang JY: A preclinical study of bone pain
patch for the treatment of bone metastases in prostate cancer.
Peking Union Medical College, 2024.
|
|
5
|
Min QM, Liu C and Liu L: Traditional
Chinese emotional nursing alleviates cancer pain in cancer
patients: A Meta analysis. Chinese Evidence-based Nursing.
10:2118–2122. 2024.
|
|
6
|
Wan Y, Deng H, Xia Y, Wen X and Yang G:
Qualitative study on perioperative experience of intrathecal
morphine pump implantation in patients with cancer pain. Journal of
Modern Medicine and Health. 41:113–116. 2025.
|
|
7
|
Chen X, Zheng L, Zhan L, Ye K, Wang J and
Gou B: Comparative study on the analgesic effect of
ultrasound-guided quadratus lumborum block combined with oxycodone
in different approaches after laparoscopic colorectal-carcinoma
surgery. Progress in Modern Biomedicine. 24:3061–3065. 2024.
|
|
8
|
Xu Y: Efficacy and safety of oxycodone
hydrochloride extended-release tablets in analgesia in patients
with intermediate and advanced malignant tumors. Chinese Journal of
Clinical Rational Drug Use. 18:109–112. 2025.
|
|
9
|
Yunbo B, Zhigang F and Jin J: Clinical
observation of oxycodone hydrochloride sustained-release tablets on
neuropathic pain in patients with primary lung cancer during
radiotherapy and chemotherapy. China Medicine. 20:47–52. 2025.
|
|
10
|
Wang XM, Li W, Li M, Shang TZ, Yu ZQ and
Zhang CL: Investigation on the Chinese medical staff for the
clinical application and cognitive status of transdermal fentanyl
patch in the treatment of cancer pain. Herald of Medicine.
42:1248–1254. 2023.
|
|
11
|
Swarm RA, Paice JA, Anghelescu DL, Are M,
Bruce JY, Buga S, Chwistek M, Cleeland C, Craig D, Gafford E, et
al: Adult cancer pain, version 3.2019, NCCN clinical practice
guidelines in oncology. J Natl Compr Canc Netw. 17:977–1007.
2019.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Yang J, Wahner-Roedler DL, Zhou X, Johnson
LA, Do A, Pachman DR, Chon TY, Salinas M, Millstine D and Bauer BA:
Acupuncture for palliative cancer pain management: Systematic
review. BMJ Support Palliat Care. 11:264–270. 2021.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Russo M, Graham B and Santarelli DM:
Gabapentin-friend or foe? Pain Pract. 23:63–69. 2023.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Chang CY, Challa CK, Shah J and Eloy JD:
Gabapentin in acute postoperative pain management. Biomed Res Int.
2014(631756)2014.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Xu JY: Evaluation of analgesic effects of
the combination of gabapentin or duloxetine with resveratrol.
Jiangsu Ocean University, 2022.
|
|
16
|
Biggs JE, Stemkowski PL, Knaus EE,
Chowdhury MA, Ballanyi K and Smith PA: Suppression of network
activity in dorsal horn by gabapentin permeation of TRPV1 channels:
Implications for drug access to cytoplasmic targets. Neurosci Lett.
584:397–402. 2015.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Hägg S, Jönsson AK and Ahlner J: Current
evidence on abuse and misuse of gabapentinoids. Drug Saf.
43:1235–1254. 2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
He YY, Chen ZH, Zhao L and Fan XG:
Clinical efficacy of gabapentin combined with amitriptyline in
patients with opioid tolerance and severe cancer pain: A
retrospective study. Journal of Third Military Medical University.
39:1939–1943. 2017.
|
|
19
|
Wu YC: Clinical study of gabapentin in
combination with opioids in cancer pain. Guangxi Medical
University, 2009.
|
|
20
|
Li XM, Liu DQ, Wu HY, Yang C and Yang L:
Controlled-release oxycodone alone or combined with gabapentin for
management of malignant neuropathic pain. Chin J Cancer Res.
22:80–86. 2010.
|
|
21
|
Caraceni A, Zecca E, Bonezzi C, Arcuri E,
Tur RY, Maltoni M, Visentin M, Gorni G, Martini C, Tirelli W, et
al: Gabapentin for neuropathic cancer pain: A randomized controlled
trial from the gabapentin cancer pain study group. J Clin Oncol.
22:2909–2917. 2004.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Keskinbora K, Pekel AF and Aydinli I:
Gabapentin and an opioid combination versus opioid alone for the
management of neuropathic cancer pain: A randomized open trial. J
Pain Symptom Manage. 34:183–189. 2007.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Ross JR, Goller K, Hardy J, Riley J,
Broadley K, A'Hern R and Williams J: Gabapentin is effective in the
treatment of cancer-related neuropathic pain: A prospective,
open-label study. J Palliat Med. 8:1118–1126. 2005.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Sterne JAC, Savović J, Page MJ, Elbers RG,
Blencowe NS, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge
SM, et al: RoB 2: A revised tool for assessing risk of bias in
randomised trials. BMJ. 366(l4898)2019.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Wells GA, Shea B, O'Connell D, Peterson J,
Welch V, Losos M, et al: The Newcastle-Ottawa Scale (NOS) for
assessing the quality of nonrandomised studies in meta-analyses.
Ottawa Hospital Research Institute, 2010.
|
|
26
|
Balduzzi S, Rücker G and Schwarzer G: How
to perform a meta-analysis with R: A practical tutorial. Evid Based
Ment Health. 22:153–160. 2019.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Viechtbauer W and Cheung MW: Outlier and
influence diagnostics for meta-analysis. Res Synth Methods.
1:112–125. 2010.PubMed/NCBI View
Article : Google Scholar
|
|
28
|
Zhao J: Clinical observation of morphine
combined with gabapentin in the treatment of moderate and severe
neuropathic cancer pain. China Practical Medicine. 11:105–107.
2016.
|
|
29
|
Zhao XH and Xia J: Efficacy of fentanyl
patch combined with gabapentin in the treatment of cancer pain in
pancreatic cancer. Strait Pharm J. 32:150–152. 2020.
|
|
30
|
Jiang W, Song H and Wang E: Analysis of
the clinical effect of oxycodone hydrochloride extended-release
tablets combined with gabapentin in the treatment of moderate to
severe cancer pain. J Med Theory Pract. 34:438–440. 2021.
|
|
31
|
Sun L: Clinical Analysis of Gabapentin
Combined with Morphine Sulfate Sustained-release Tablets in the
Treatment of Cancerous Neuropathic Pain. China Foreign Medical
Treatment. 40:101–103. 2021.
|
|
32
|
Teng L, Dai J, Shao H, Zhao L, Lin S,
Zhang W and Zou H: Gabapentin enhances the antinociceptive effect
of intrathecal morphine in refractory cancer pain patients. Support
Care Cancer. 29:7611–7616. 2021.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Su L: Clinical observation and care of
fentanyl patch combined with gabapentin in the treatment of bone
metastasis cancer pain. China Medical Engineering. 21:90–92.
2013.
|
|
34
|
Liu XC, Ding ZP and Zhou XF: Effects of
gabapentin combined with morphine sulfate sustained release tablets
on pain of middle-late stage cancer patients after chemotherapy and
radiotherapy. The Practical Journal of Cancer. (11):1504–1506.
2014.
|
|
35
|
Qin XB, Song CJ, Yu T, Li JY, Liu TF and
Chen XM: Efficacy observation of oxycodone hydrochloride
controlled-release tablets combined with gabapentin for the
treatment of malignant neuropathic pain. ACTA Academiae Medicinae
Xuzhou. (9):594–597. 2015.
|
|
36
|
Chen L, Shen W, Han X, Yuan Y, Liang D,
Yin Q, et al: Clinical observation of sustained-release morphine
sulphate combined with gabapentin in the treatment of cancer pain.
Chinese Journal of Pain Medicine. 21:679–683. 2015.
|
|
37
|
Zhang N: Effect and adverse reactions of
gabapentin combined with morphine sulfate controlled-release
tablets in the treatment of carcinoneuralgia. Chinese Journal of
Practical Nervous Diseases. 19:40–42. 2016.
|
|
38
|
Zhang LJ, et al: Analysis of the efficacy
of gabapentin combined with morphine hydrochloride extended-release
tablets in the treatment of patients with severe cancer pain. China
Health Care and Nutrition. 26:174–175. 2016.
|
|
39
|
Chen ZH, et al: Clinical observation of
oxycodone hydrochloride extended-release tablets combined with
gabapentin capsules in the treatment of cancer pain. Guangdong
Medical Journal. 38:136–138. 2017.
|
|
40
|
Jiang B: Clinical study of opioids in
combination with gabapentin in cancer pain. Qinghai University,
2017.
|
|
41
|
She XH and Jiang LY: A study on the effect
of gabapentin and morphine hydrochloride sustained-release tablets
in relieving pain in patients with cancer pain. Chinese Remedies
and Clinics. 17:1824–1826. 2017.
|
|
42
|
Yan HM, et al: Clinical observation of
gabapentin combined with morphine sulfate extended-release tablets
in the treatment of cancerous neuropathic pain. Zhejiang Clinical
Medical Journal. 20:1073–1075. 2018.
|
|
43
|
Ru AZ, et al: Analysis of the effect of
gabapentin combined with oxycodone hydrochloride in the treatment
of cancerous neuropathic pain. Health Vocational Education.
36:84–86. 2018.
|
|
44
|
Fu XZ: Effect of the combination of
morphine sulfate extended-release tablets and gabapentin capsules
in the treatment of cancer pain and its effect on quality of life.
Journal of North Pharmacy. 15:104–105. 2018.
|
|
45
|
Yan QY: Clinical study of opioids combined
with gabapentin in the treatment of cancer pain and analysis of
real-world cancer pain diagnosis and treatment. Hebei Medical
University, 2018.
|
|
46
|
Zhou H, Zhang H, Qian X and Ge W: Efficacy
and safety of gabapentin adjuvant therapy for neuropathic cancer
pain. China Pharmacist. 22:1278–1286. 2019.
|
|
47
|
Meng J: Effect of gabapentin combined with
oxycodone hydrochloride on patients with advanced cancer-induced
pain and its effect on pain media. Medical Information. 32:146–147.
2019.
|
|
48
|
Zhu RH: Clinical analysis of gabapentin
combined with morphine sulfate extended-release tablets in the
treatment of cancerous neuropathic pain. Health Guide.
(48)(100)2020.
|
|
49
|
Zhang X: Analysis of the effect of
gabapentin combined with oxycodone hydrochloride extended-release
tablets in the treatment of cancerous neuropathic pain.
Contemporary Medicine Forum. 19(23)2021.
|
|
50
|
Jiang W, Wang L, Wu T, Xiu X, Yang X and
Zhang S: Clinical efficacy of oxycontin combined with gabapentin on
neuropathic cancer pain and its effect on immune function. Int J
Clin Exp Med. 14:246–254. 2021.
|
|
51
|
Qi N: Observation of the efficacy of
gabapentin combined with oxycodone hydrochloride extended-release
tablets in the treatment of cancerous neuropathic pain. Health
Guide. (20):7–9. 2024.
|
|
52
|
Wu X, Li N, Zhu J, Wu Y, Du Y, et al:
Observation of opioid combined with corticosteroids or
anticonvulsants for advanced cancer patients with pain. Chinese
Clinical Oncology. 16:58–60. 2011.
|
|
53
|
Shinde S, Gordon P, Sharma P, Gross J and
Davis MP: Use of non-opioid analgesics as adjuvants to opioid
analgesia for cancer pain management in an inpatient palliative
unit: Does this improve pain control and reduce opioid
requirements? Support Care Cancer. 23:695–703. 2015.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Eckhardt K, Ammon S, Hofmann U, Riebe A,
Gugeler N and Mikus G: Gabapentin enhances the analgesic effect of
morphine in healthy volunteers. Anesth Analg. 91:185–191.
2000.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Wang X, Peng J and Wang X: Oxycodone
hydrochloride controlled-release tablet combined with gabapentin
for treatment of advanced cancer with neuropathic pain. Journal of
Modern Oncology. 20:1930–1932. 2012.
|
|
56
|
Gilron I: Gabapentin and pregabalin for
chronic neuropathic and early postsurgical pain: Current evidence
and future directions. Curr Opin Anaesthesiol. 20:456–472.
2007.PubMed/NCBI View Article : Google Scholar
|