Introduction
Intravenous leiomyomatosis (IVL) is a leiomyoma that grows within the venous system; the tumor resides inside the veins but typically does not invade the venous wall. IVL usually originates from the pelvic veins and extends in a cephalad direction along the venous system, potentially involving the iliac veins, inferior vena cava and even the heart (1). IVL was first reported by Birck-Hirschfeld in 1896(2) and is a leiomyoma that typically grows without invasion of the venous wall. IVL is a rare smooth muscle tumor, classified as a borderline tumor due to its histologically benign appearance yet malignant biological behavior, including its propensity for vascular invasion. IVL predominantly affects women aged between 20 and 70 years, with a median age of 45 years. Since its first description in 1896, it remains a clinically rare entity, with only ~800 cases documented to date. The tumor typically originates from the uterus, and exhibits slow growth and well-defined margins, sharing similar histopathological features with benign uterine leiomyoma; however, its biological behavior is marked by the potential for venous invasion. This aggressive characteristic of infiltrating the venous system imparts a degree of biological malignancy to the disease (3). Notably, the etiology of IVL remains unclear (4); however, patients with IVL often have a history of uterine leiomyoma or a previous hysterectomy (1). In its early stages, IVL often presents with non-specific clinical symptoms, such as abdominal pain and vaginal bleeding. If the condition is not recognized and treated early, or if it is misdiagnosed as another entity, the potential for centripetal extension along the venous system may be overlooked. As the disease progresses, it can lead to palpitations, syncope and even cardiac arrest, potentially leading to sudden death (1).
The present study describes the case of a 48-year-old female patient diagnosed with IVL of the uterus. This disease presents insidiously and is challenging to diagnose in its early stages. Furthermore, there are currently no definitive guidelines to guide the diagnosis and management of this condition. The present study aimed to provide a reference for the clinical diagnosis and treatment of IVL of the uterus, with the goal of achieving better therapeutic outcomes. IVL of the uterus typically presents with patients complaints of heavy menstrual bleeding and anemia. These symptoms are non-specific and may occur in various gynecological conditions, such as adenomyosis, adenomyoma and submucosal uterine leiomyoma, making misdiagnosis and missed diagnosis likely. Early diagnosis is crucial for IVL, as the condition progresses in a retrograde manner over time, potentially affecting the superior and inferior vena cavae, and even cardiac vessels, with severe cases proving fatal. IVL frequently coexists with uterine fibroids (as in the current case), further complicating its diagnosis. Integrating relevant literature and expert consensus, IVL is currently managed through follow-up protocols akin to those for uterine malignancies such as endometrial cancer.
Case report
A married female patient, aged 48 years, presented with menorrhagia lasting 12 days. In June 2025, the patient presented to a local hospital after they experienced increased menstrual flow without an apparent cause, approximately double the usual volume. Bleeding ceased spontaneously after 6 days with no other discomfort. In July 2025, a local hospital blood test indicated anemia. Ultrasound findings (Fig. S1) were as follows: A hypoechoic area within the uterine myometrium, suggesting suspected myoma (~60x49 mm); adenomyosis, a hypoechoic mass in the left adnexal region, suggesting suspected broad ligament myoma or uterine myoma (~72x38 mm); and heterogeneous endometrial echoes. Further investigation was thus recommended. Notably, cardiac ultrasound was not performed, nor was treatment initiated.
The patient subsequently sought further consultation at Hebei General Hospital (Shijiazhuang, China). Color Doppler ultrasound (Fig. S2) at this hospital in July 2025 demonstrated the following: Uterine fibroid (~57x54x46 mm) and a left-sided hypoechoic uterine mass (~76x54x49 mm). Given the chief complaints of menorrhagia and anemia, atypical clinical presentation, absence of marked endometrial abnormalities and concurrent pelvic mass, the patient was admitted with a provisional diagnosis of a pelvic mass. As of July 2025, the patient had a 3-month history of hypertension, which was well-controlled with regular medication. Their past obstetric history included two full-term deliveries, and no other medical conditions, surgical history or notable family history was reported. Menarche occurred at age 14 years with highly irregular cycles ranging from 23 to 120 days; menstrual flow lasted ~4 days per cycle, with moderate flow and no dysmenorrhea. Their last menstrual period before July 2025 was in June 2024. On admission to Hebei General Hospital, their vital signs were as follows: Temperature, 36.6˚C; pulse, 87 bpm; respiration, 20 breaths/min; blood pressure, 146/86 mmHg. Cardiopulmonary examination revealed no abnormalities. Gynecological examination detected the following: Vulva, postpartum; vagina, patent with minimal discharge; cervix, smooth but enlarged, with no tenderness on elevation; uterus, anteverted. A 7-cm firm, non-tender mass that was bilaterally palpable was also detected, as well as an additional 5-cm firm, non-tender solitary mass at the fundus, and the adnexa was bilaterally unremarkable. Complete blood count indicated anemia, whereas a tumor marker panel showed no notable abnormalities. The diagnosis at the initial admission was of a pelvic mass.
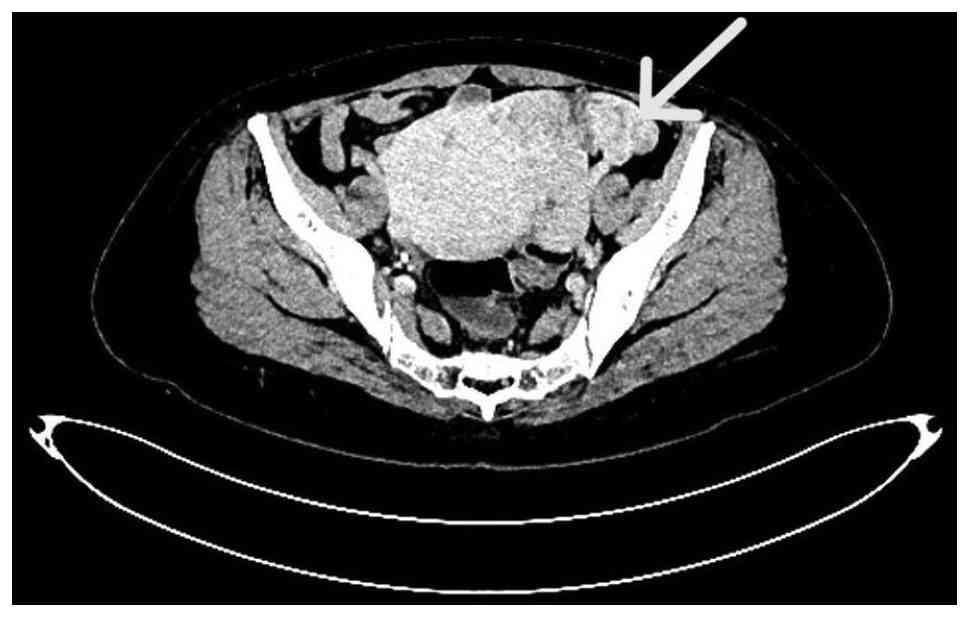
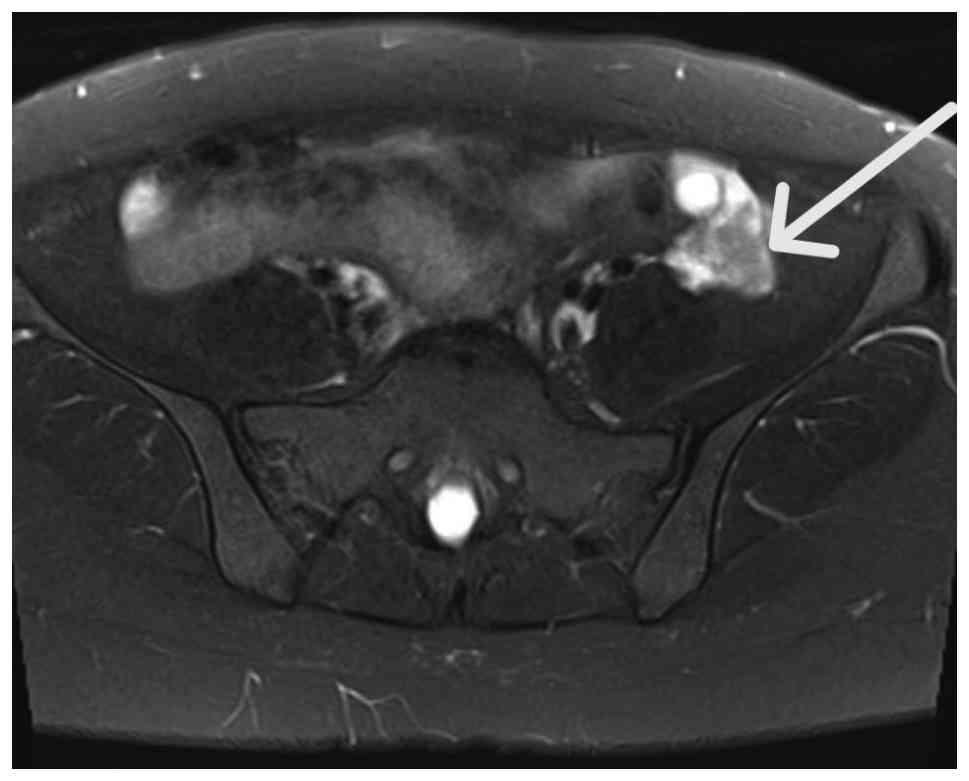
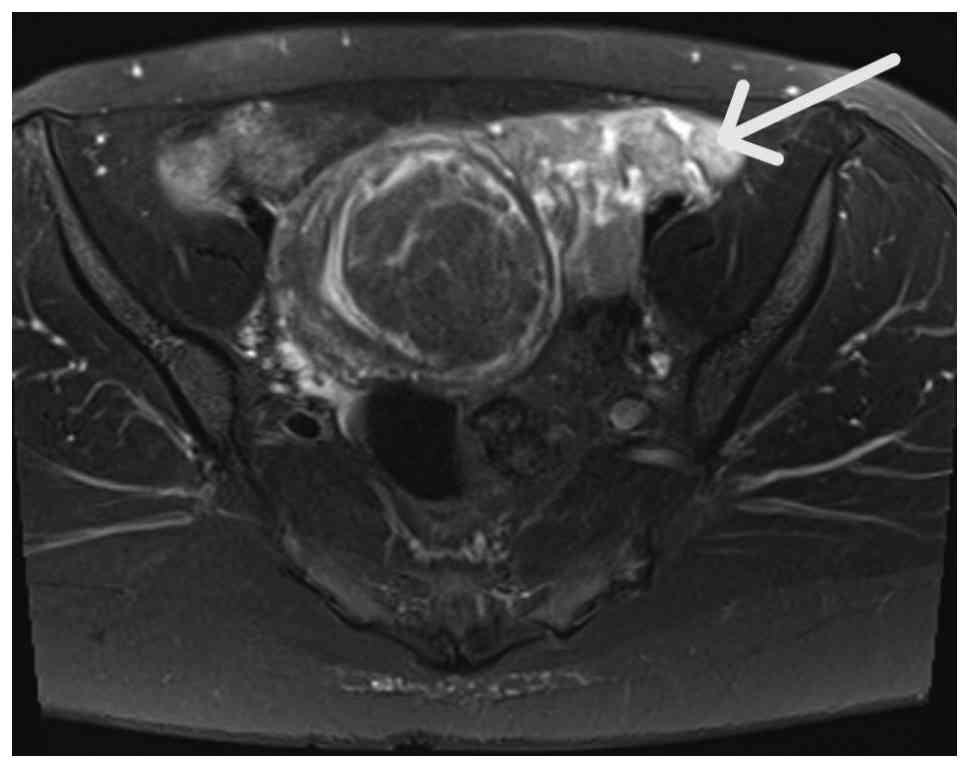
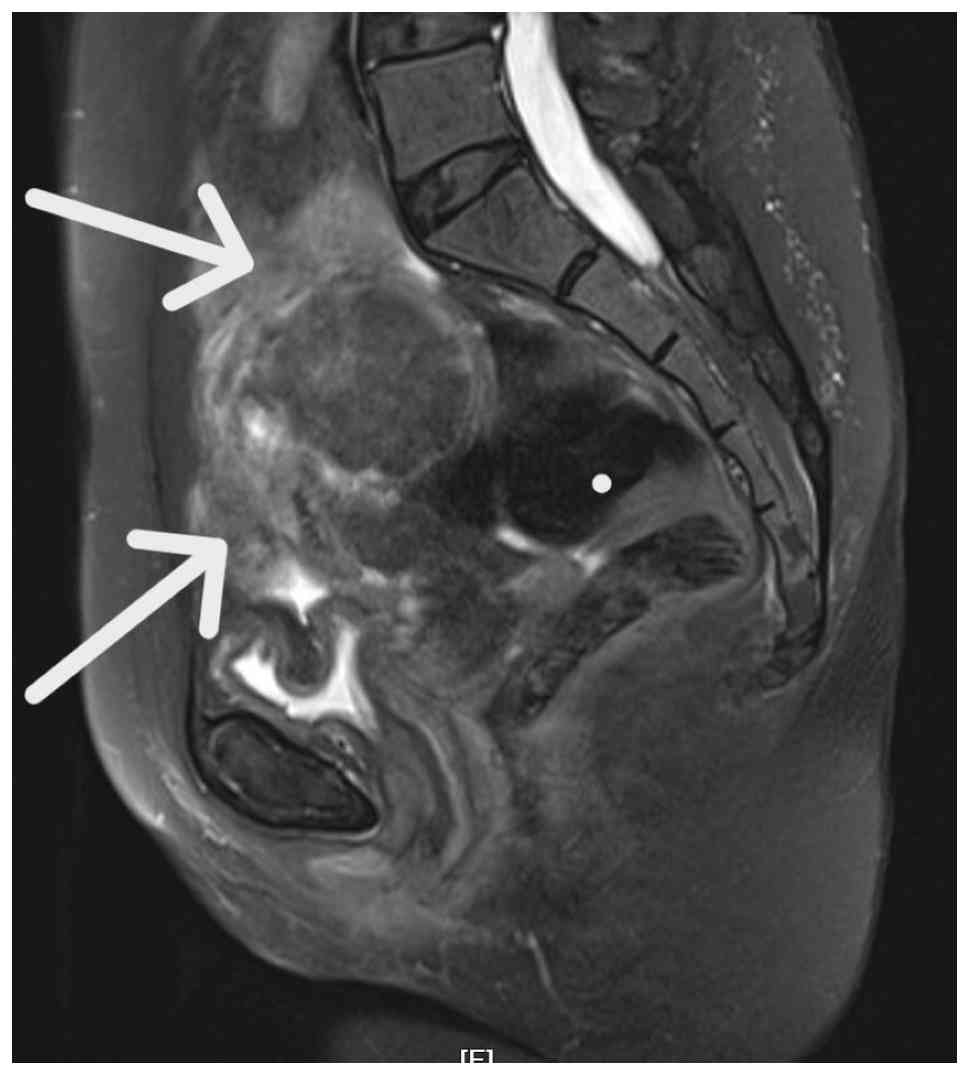
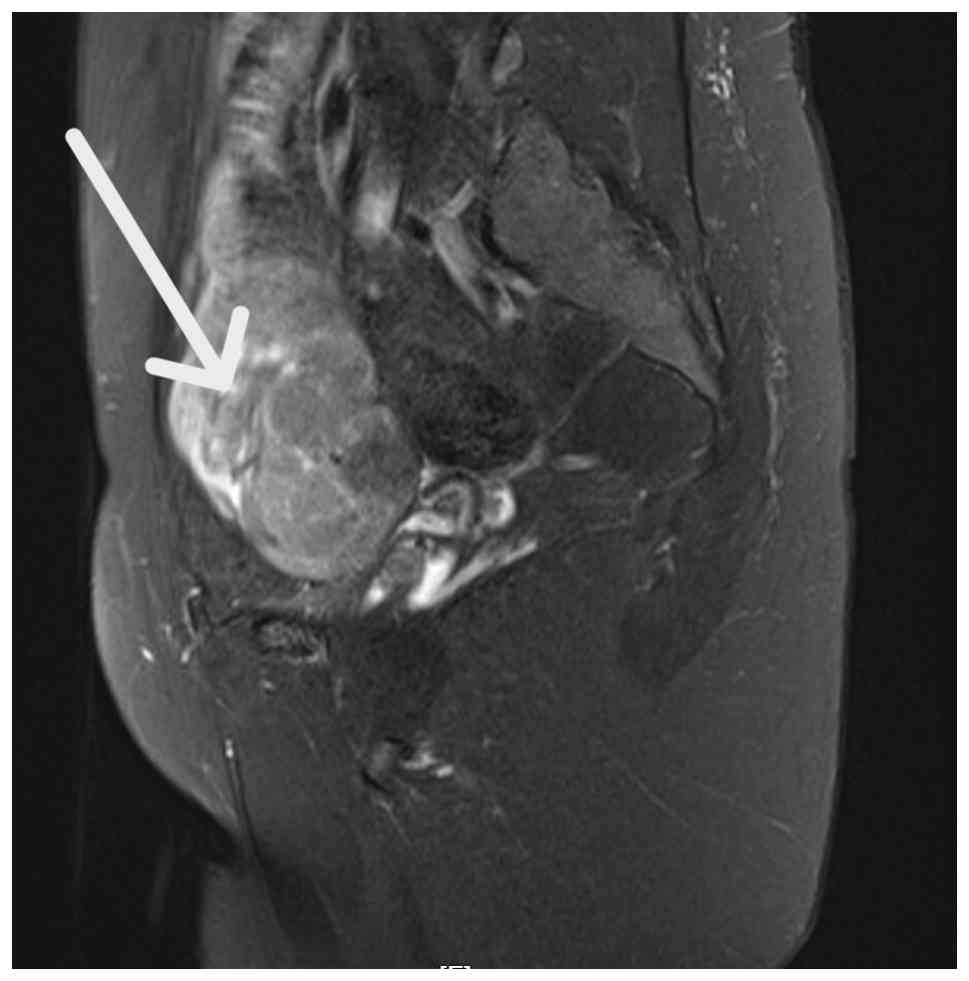
To further characterize the location and nature of the left-sided hypoechoic uterine mass, contrast-enhanced pelvic CT with three-dimensional reconstruction was performed in July 2025 (5 days after admission). The findings indicated that the mass originated from the left uterine lateral wall, most likely representing a leiomyoma; a separate independent mass was located to the left of the uterus, continuous with the left ovarian vein; and a filling defect was observed within the left ovarian vein, suggesting possible IVL. Concurrently, minimal pelvic effusion was noted (Fig. 1). Subsequently, pelvic magnetic resonance imaging (MRI) with non-contrast, contrast-enhanced and diffusion-weighted imaging sequences was performed. The findings revealed that the intrauterine mass was consistent with uterine leiomyoma and the left paracervical mass could not be excluded as a hemorrhagic uterine fibroid. Additionally, a Nabothian cyst of the cervix was noted (Figs. 2, 3, 4 and 5). Based on careful consideration of the imaging findings, a provisional diagnosis of IVL of the uterus was made. Notably, no authoritative, standardized diagnostic or treatment guidelines currently exist for this condition; however, according to existing expert consensus, these tumors typically originate within pelvic veins and exhibit continuous, centripetal growth along the venous system. To date, to the best of our knowledge, no reports of metastatic spread via direct invasion have been documented. The two recognized primary routes of infiltration are: i) Left/right uterine vein > internal iliac vein > common iliac vein > inferior vena cava; ii) left ovarian vein > left renal vein > inferior vena cava, or right ovarian vein > inferior vena cava (1). Consequently, further investigation was considered necessary to determine the presence of extravascular uterine venous invasion.
In July 2025 (5 days after admission), bilateral iliac vein and inferior vena cava color Doppler ultrasound revealed no notable abnormalities. In accordance with current expert consensus recommendations, non-contrast and contrast-enhanced CT with three-dimensional reconstruction of the kidneys was performed (data not shown). Imaging evaluation suggested a high probability of bilateral renal cystic lesions, classified as Bosniak I (5). CT imaging revealed a mildly hypodense lesion in the spleen, considered likely to be a hemangioma. Color Doppler ultrasound of the bilateral lower limbs and intermuscular veins showed no marked abnormalities. Consequently, the disease was considered to be confined to the pelvic veins, without involvement of the iliac veins, inferior vena cava or right heart. Extrapelvic vascular infiltration was not suspected and echocardiography was deemed unnecessary. The preoperative diagnosis was pelvic mass, with differential diagnoses primarily including tumors of uterine or ovarian origin, and IVL of the uterus. A multidisciplinary consultation involving vascular surgery was completed and a combined treatment plan was formulated. Should vascular intervention be required intraoperatively, it was decided that vascular surgery specialists would provide intraoperative assistance.
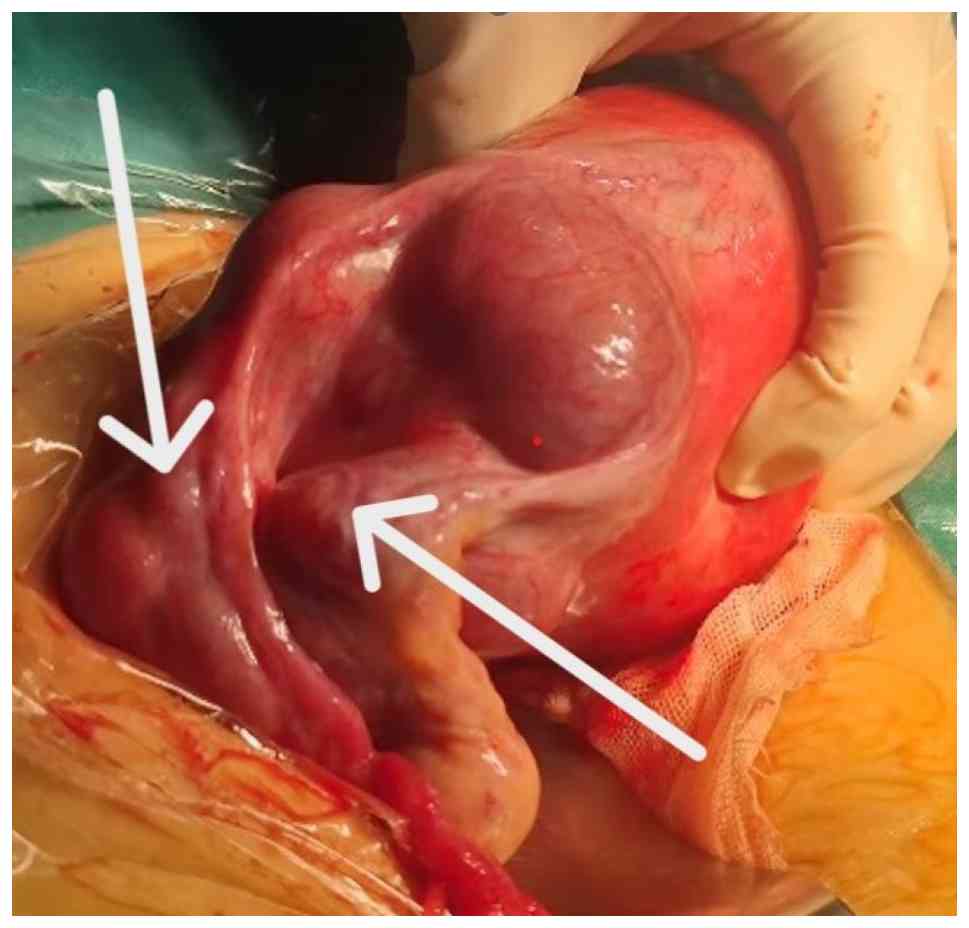
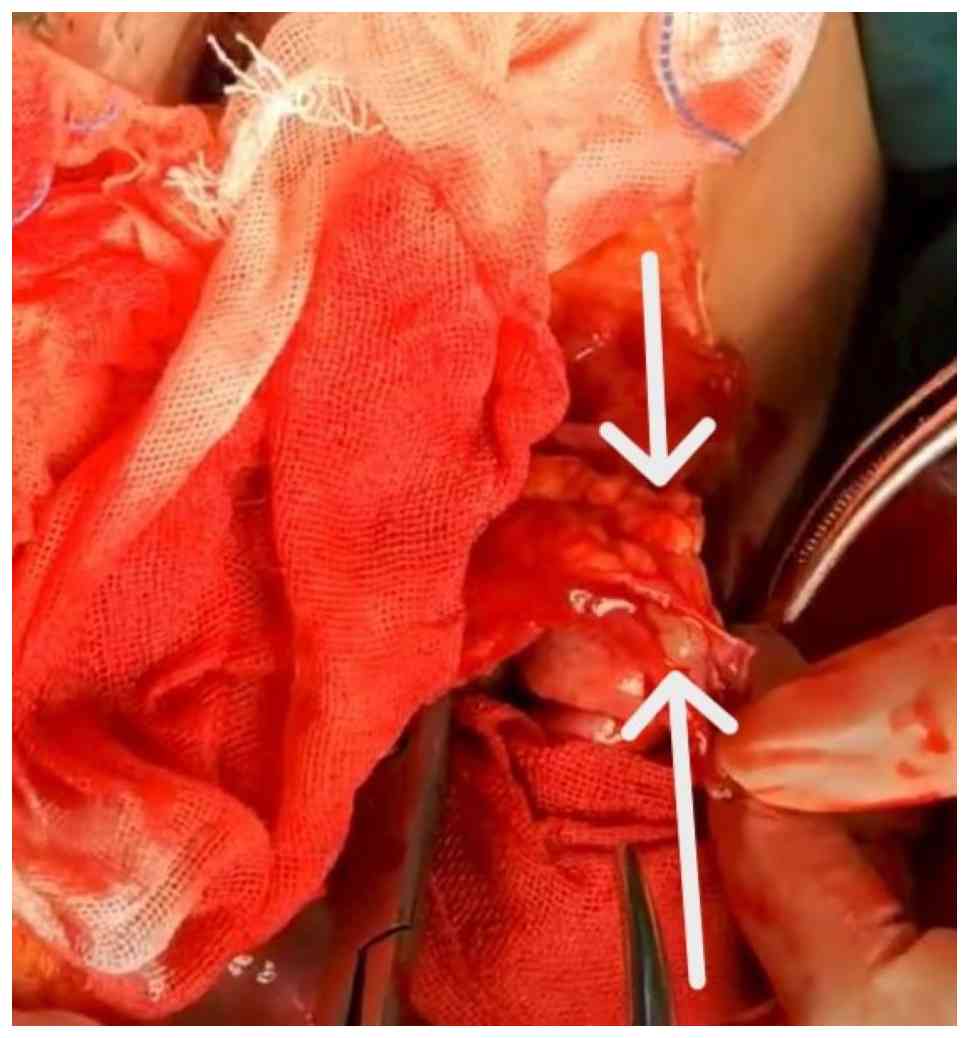
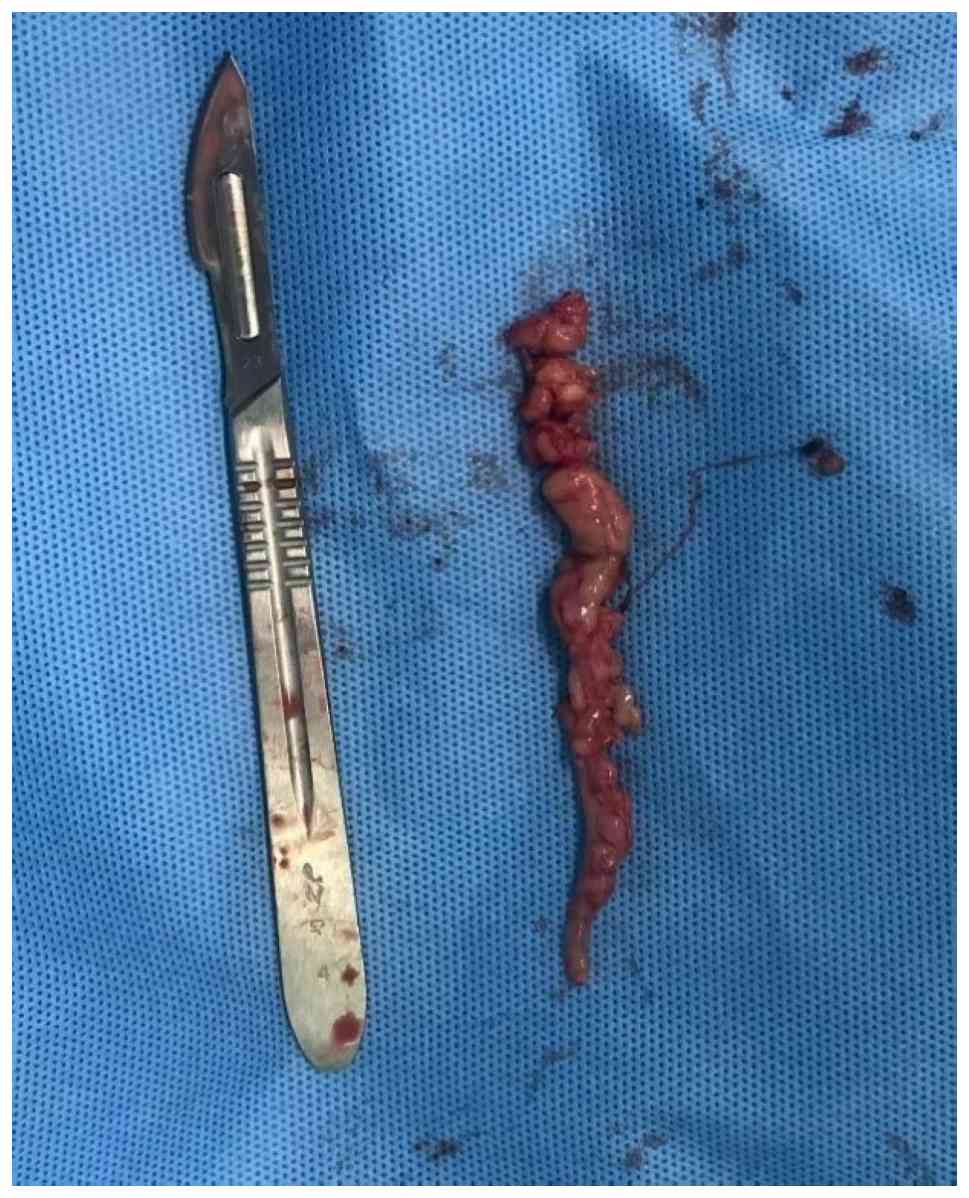
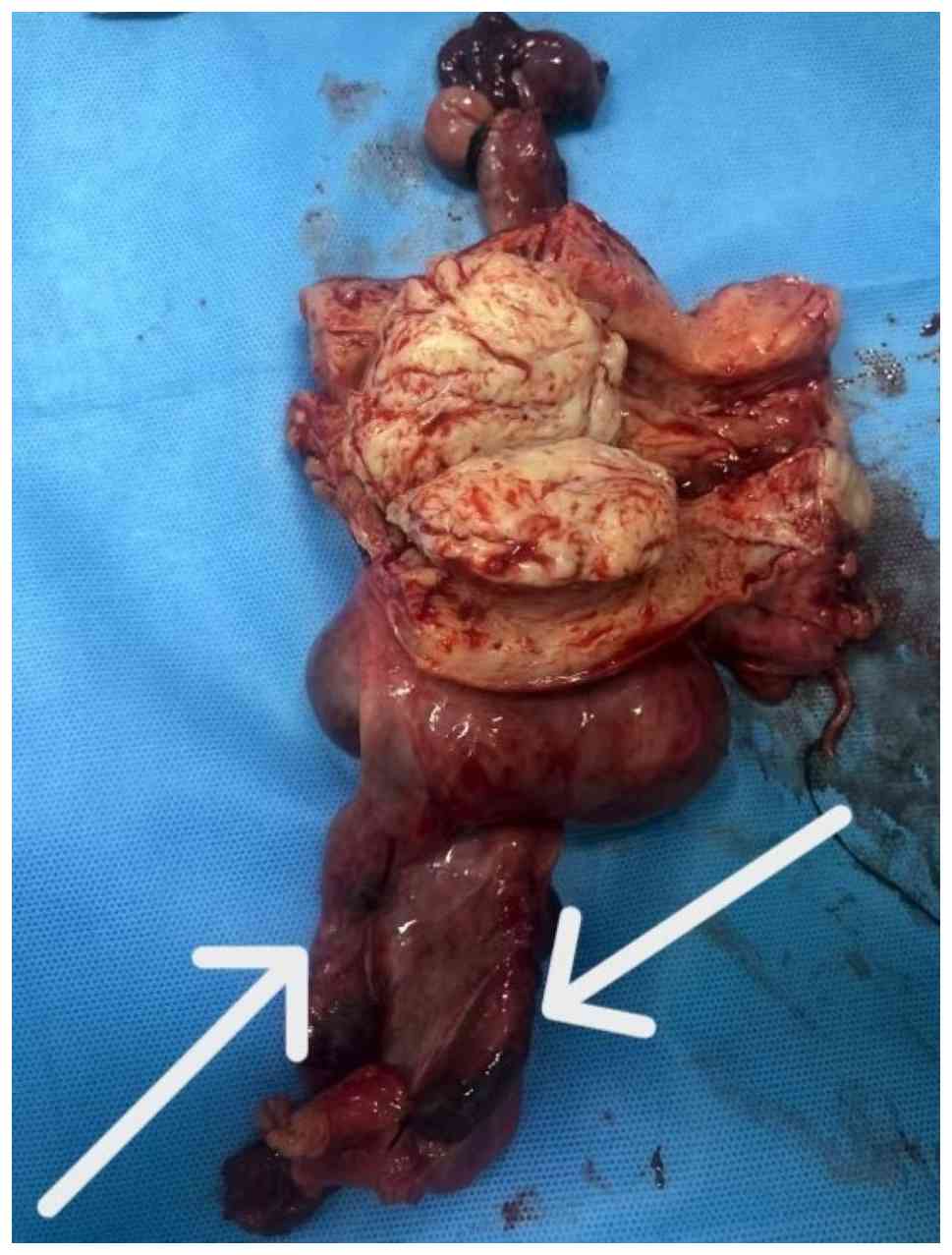
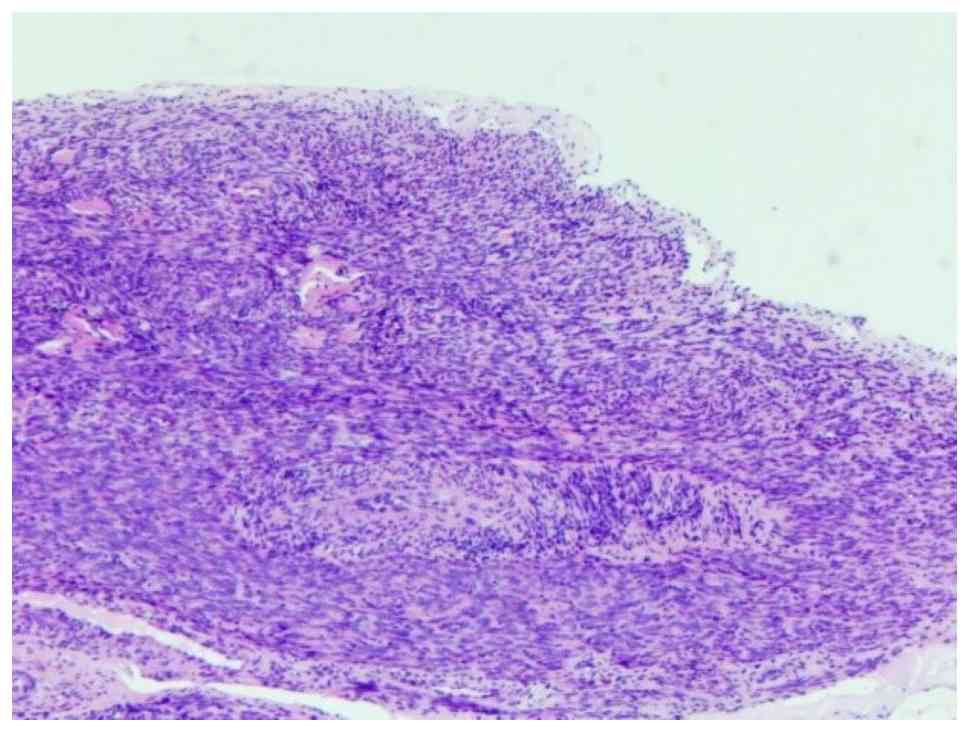
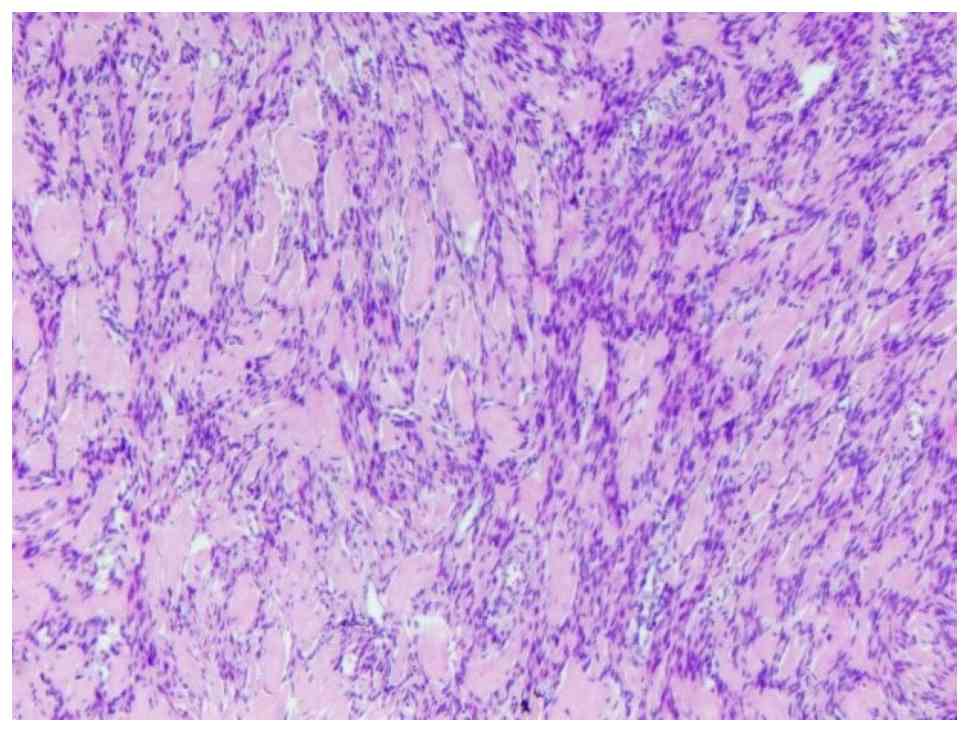
All preoperative evaluations were completed, revealing no notable surgical contraindications. In July 2025 (5 days after admission), an exploratory laparotomy was performed under general anesthesia. Intraoperative findings were as follows: Adhesions were noted between segments of the intestine and the left pelvic wall; the uterus was enlarged, comparable in size to a second-trimester pregnancy; a leiomyoma nodule ~7 cm in diameter was observed at the uterine fundus; the left lateral wall and cornu of the uterus exhibited outward bulging and tortuosity, forming a mass ~5 cm in diameter with convoluted and engorged vessels. Within these vessels, firm leiomyoma lesions growing along the venous lumen were palpable. Both adnexa appeared grossly normal. No evidence of tumor rupture or hemorrhage was identified (Fig. 6). An intraoperative consultation with vascular surgery was requested. Exploration revealed worm-like leiomyoma lesions growing within the venous lumen of the left ovarian vein, ~7 cm proximal to the left ovary. The venous vessels at the left lateral wall and cornu of the uterus were tortuous and clustered, entirely filled with leiomyoma lesions (Fig. 7). Based on the intraoperative findings, a diagnosis of IVL was considered. Given the lack of fertility aspirations of the patient, a total hysterectomy with bilateral salpingo-oophorectomy and lysis of pelvic adhesions was performed. A comprehensive exploration of the pelvic and abdominal veins was conducted: The left ovarian artery and vein were examined, with careful palpation confirming no worm-like tumor in the proximal segment. The left uterine veins were entirely filled by leiomyoma lesions, which extended downward along the deep uterine veins into the pelvic venous plexus. The postoperative pathology indicated the following: Uterine leiomyoma and IVL; proliferative endometrium; mild chronic inflammation of the cervix. In addition, bilateral fallopian tubes showed stromal small vessel dilation and congestion, with no notable ovarian pathology. The contents within the left deep uterine vein were consistent with IVL (Figs. 8 and 9). The diagnostic histological feature was the presence of worm-like tumor tissue within the vascular lumen. Under high-power magnification, the tumor cells appeared as benign spindle-shaped cells with elongated nuclei, showing no pathological mitotic figures or marked atypia. Additionally, the periphery of the tumor tissue was lined by endothelial cells [hematoxylin and eosin staining: 0.1-0.5% hematoxylin for 5-10 min and 0.5-1% eosin for 1-3 min; room temperature (20-25˚C); light microscope; magnifications, x100 and x400; Figs. 10 and 11].
In August, September and October 2025, every 28 days, the patient was subcutaneously injected with 3.75 mg leuprolide. The patient reported poor night-time rest, which was considered a potential side effect of the medication. Occasional palpitations were also reported; an electrocardiogram revealed no notable abnormalities. Concurrently, the patient was advised to undergo contrast-enhanced MRI, which they declined. The patient was informed of the relevant medical circumstances and advised to seek prompt medical attention should any discomfort arise. The last follow-up was in October 2025.
Discussion
As part of a routine gynecological examination, an ultrasound is essential for diagnosing IVL of the uterus. The present case clarifies the importance of progressive IVL imaging features. The ultrasound showed a hypoechoic mass, ~76x54x59 mm, on the left side of the uterus, which was closely associated with the uterine wall, irregular in shape and had heterogeneous echo enhancement. Color Doppler flow imaging showed branching blood flow signals. According to the literature, this matches typical ultrasound findings for IVL pelvic masses: Irregular shape and heterogeneous internal echoes. Crucially, if ultrasound detects ‘uterine fibroids’ that are ‘extrauterine’, ‘intravascular’ or ‘extraperitoneal’, it is recommended that clinicians immediately investigate for IVL. The low incidence and limited recognition of this disease by sonographers mean that ultrasound alone often misses diagnoses before surgery. Notably, some cases are discovered incidentally during myomectomy. Therefore, clinicians should not only identify ‘fibroids’ but also investigate their vascular relationships. When ultrasound strongly suggests IVL, comprehensive vascular imaging, such as CT or MRI, is essential. Comparing imaging findings clarifies the true range of the lesion (vascular involvement) and helps determine disease progression. This guides the surgical approach, timing and whether multidisciplinary intervention is needed, and it avoids inadequate preoperative assessment (5). Research has shown that combining ultrasound and CT imaging notably improves IVL diagnostic accuracy (6). IVL can extend along veins such as the iliac veins or inferior vena cava as the disease progresses. Conventional ultrasound has limitations in visualizing pelvic-external lesions; thus, it may miss distal thrombi or tumor emboli in the veins. On detection, a full imaging evaluation, including CT venography and transthoracic echocardiography, is needed. However, a gap in the knowledge remains, as clear ultrasound criteria for when to trigger immediate contrast-enhanced ultrasound or CT/MRI still remain to be elucidated. Such criteria could shift diagnosis from incidental discovery to intentional screening; this deserves further study.
Clinical manifestations of IVL are likely merely the initial sign of this disease, with symptoms not equating to the extent of disease involvement. The present case demonstrated that atypical clinical symptoms of IVL of the uterus (for example, abdominal pain and abnormal uterine bleeding) reflect only the minimal extent of tumor involvement. Relevant literature has established that IVL of the uterus can extend retrogradely along the venous system to the inferior vena cava, right heart or even pulmonary arteries. However, clinicians often underestimate the true progression of the disease due to the absence of symptoms such as chest tightness or lower limb edema. The cautionary importance of the current case lies in the fact that lesion localization should not be based solely on symptoms; instead, imaging should be actively employed to track its vascular course. When patients exhibit any signs of venous outflow obstruction (even mild), or have a history of uterine surgery or uterine fibroids (1), IVL of the uterus should be included in the differential diagnosis. Comprehensive vascular imaging should be performed proactively, rather than passively awaiting disease progression to cardiac involvement symptoms; this approach prevents severe IVL complications such as disseminated intravascular coagulation (7).
In differential diagnosis, one must distinguish between common imaging features and characteristics of biological behavior. While histopathologically similar to common uterine fibroids and often coexisting with them (1), the growth patterns of IVL are fundamentally different. The present case highlighted that gynecological ultrasound assessment must extend beyond detecting ‘hypoechoic masses’ to deliberately pursue the presence of ‘intravascular lesions’. This necessitates gynecological sonographers extending their observation beyond the tumor itself to its relationship with vascular structures, treating vascular involvement as the ‘central point’ for differential diagnosis. Regarding the differentiation of IVL from uterine leiomyosarcoma, both may invade blood vessels and the heart, but sarcoma typically exhibits non-continuous metastatic foci, frequently involving the lungs (1). The present case highlighted that upon detecting ‘intravascular thrombi’, their benign or malignant nature must be confirmed pathologically (through mitotic figures, cellular atypia and coagulative necrosis). Vascular invasion alone should not lead to a direct diagnosis of sarcoma. Imaging findings of ‘continuous extension’ (such as cord-like retrograde growth from pelvic veins to the heart) suggest IVL of the uterus, whereas ‘discontinuous’ or multiple pulmonary nodules are more indicative of malignancy.
The following core lessons regarding treatment strategies and long-term management can be drawn from the present report. The findings validate established principles for IVL of the uterus management, while deepening the existing understanding of disease progression and recurrence risk. Firstly, the concept of ‘individualized’ treatment should not be vague but grounded in explicit risk-benefit assessments. IVL of the uterus presents with two distinct yet clear clinical pathways: For younger patients with fertility aspirations, fertility-sparing surgery may be attempted provided the lesion is confined; whereas for the present 48-year-old patient who had completed childbearing, radical surgery (total hysterectomy with bilateral salpingo-oophorectomy) was selected to maximize the reduction of recurrence risk. The present case emphasized that individualized treatment for IVL should not be vaguely decided, but determined based on age, fertility aspirations and disease extent. While existing literature emphasizes individualization (1), it often lacks specific stratification criteria. The treatment of the present case, grounded in explicit recurrence rate data (for example, 75% recurrence after myomectomy vs. 7.6% after radical surgery), provides quantitative justification for selecting bilateral adnexectomy. This elevates treatment decisions from empirical judgement to evidence-based stratification. Secondly, the timing of multidisciplinary team (MDT) involvement should shift from ‘intraoperative consultation’ to ‘preoperative planning’. In the present case, anticipating possible IVL led to preoperative coordination with vascular surgery to formulate the surgical plan, thereby avoiding a second-stage operation. The lesson here is that MDT should not serve as an emergency stopgap measure for inadequate preparation, but rather be a routine preoperative process for suspected IVL cases. Existing research affirms the necessity of MDT but lacks clarity on its initiation timing (1). The current case demonstrated that early MDT involvement (even before imaging fully delineated the extent of the lesion) can optimize surgical planning, enabling complete primary resection, and avoiding the physical and economic burdens of multiple operations. This provides direction for standardizing and qualifying when an MDT consultation is required in clinical practice.
Recurrence rate data serve not only as prognostic indicators but also as decision-making criteria for postoperative management intensity. Based on recurrence rates ranging from 7.6 to 75% across different surgical approaches (1), the present study recommends bilateral adnexectomy to mitigate risk. The present case suggested that follow-up protocols should be stratified according to the extent of surgical radicality. For example, patients undergoing myomectomy alone (75% recurrence rate) should receive more frequent and prolonged imaging surveillance than those who undergo radical surgery (7.6% recurrence rate) (8). While current follow-up recommendations (for example, every 3-6 months for the first 2 years post-surgery) are standardized, future guidelines should establish ‘risk-stratified follow-up protocols based on initial surgical approach’. Patients at a high risk of recurrence may require shorter follow-up intervals or more sensitive monitoring methods (such as MRI instead of ultrasound).
Endocrine therapy is most commonly used for patients who are not suitable for surgery, have undergone incomplete tumor resection or as neoadjuvant treatment prior to surgery (1). Based on gonadotropin-releasing hormone (GnRH) analogues, endocrine therapy is not a curative approach for IVL of the uterus, it primarily serves as a ‘regulatory’ measure between multiple surgical interventions (1). GnRH agonists (GnRH-a) effectively suppress residual tumor growth, with recurrence upon discontinuation indicating a reversible mechanism that may prolong disease remission. Integrating current evidence-based guidelines and expert consensus, the indications, timing and limitations of endocrine therapy are summarized here to provide practical guidance. Primarily, GnRH-a is indicated for: Premenopausal patients undergoing ovarian preservation to reduce recurrence risk; patients unable to tolerate surgery due to poor general condition or extensive tumor involvement; or patients requiring delayed surgery, including as neoadjuvant therapy or bridging treatment between two-stage procedures. Regarding treatment timing, GnRH-a is used to extend surgical intervals: For patients requiring staged surgery (for example, addressing pelvic lesions before cardiac involvement), the interval between stages is typically 6 weeks to 3 months (9). Should prolongation be required, GnRH-a may be administered during this interval to suppress tumor growth and prevent recurrent cardiac invasion. Regarding preoperative neoadjuvant therapy, for patients unable to tolerate surgery in the short term, neoadjuvant GnRH-a can control tumor progression, creating more favorable conditions for surgery, whereas regarding adjuvant therapy of residual disease post-surgery, prompt initiation of endocrine therapy aids in delaying recurrence (9). Notably, residual lesions may exhibit rapid regrowth upon discontinuation, which can be re-suppressed by restarting therapy. This underscores the need for dynamic adjustment of treatment regimens based on recurrence risk. Regarding treatment duration and follow-up, definitive evidence establishing the optimal duration of postoperative anti-estrogen therapy remains lacking. Based on current data, a 6-month prophylactic course may be considered. Post-IVL recurrence rates range from 16.6 to 30.0%, rendering long-term follow-up critical: Imaging reviews (MRI or CT) every 3-6 months for the first 2 years post-surgery, followed by 6-12-monthly intervals thereafter. Patients with complete resection may undergo MRI assessment within the first 3-6 months, with subsequent reviews every 2-5 years based on disease staging (1). Endocrine therapy remains notably limited, primarily due to its inhibitory rather than curative effect, and long-term use induces hypoestrogenism, potentially leading to associated adverse effects. Current indications and treatment durations lack standardization. Future research on IVL of the uterus should focus on key issues such as ‘which patients genuinely benefit from prolonged endocrine therapy’ and ‘the optimal treatment duration’ to address existing knowledge gaps.
The core value of long-term follow-up lies in ‘dynamic risk assessment’ rather than mechanical repetition. When formulating specific follow-up plans, imaging modalities should be combined with individual risk stratification to enhance the sensitivity of early recurrence detection and clinical efficiency. Imaging-wise, MRI is recommended as the primary tool for long-term follow-up due to its superior soft tissue resolution for vascular and intraluminal lesions (10). For patients undergoing complete resection, an initial baseline MRI scan is advised between 3 and 6 months post-surgery to rule out early occult recurrence or residual disease (10). Risk-stratified (individualized) follow-up protocols should be dynamically adjusted based on initial surgical findings and patient characteristics, with the following strategies: Low-risk group (complete resection, no high-risk factors): Pelvic and abdominal MRI or CT every 6 months for the first 2 years post-surgery; thereafter, if stable, extend to every 12 months for ≥5 years; beyond 5 years, this may be further extended to every 2 years as appropriate. High-risk group (including patients with residual/fragmented tumor, ovarian preservation, age at diagnosis <45 years, concomitant parametrial vascular involvement): Imaging review every 3-6 months for the first 2 years post-surgery; every 6 months during years 3-5; if no recurrence signs persist after 5 years, this may be adjusted to every 12 months, with consideration for lifelong follow-up. Very high-risk group (for example, those with prior recurrence requiring reoperation or a history of inferior vena cava/cardiac involvement): Maintain imaging surveillance at least every 6-12 months even in the long-term postoperative period, with frequency determined by previous imaging findings and clinical symptom changes. Long-term follow-up is recommended. However, for low-risk patients with persistently negative long-term examinations, follow-up intervals may be extended or discontinued at the discretion of the clinician if imaging remains negative for >10 years, subject to individual circumstances. Continuous follow-up is essential for patients who have undergone ovarian preservation or endocrine therapy. This follow-up strategy, grounded in initial treatment protocols and risk assessment, aims to refine generalized approaches towards individualization, representing an area where guidelines may be optimized.
In conclusion, the management experience from the present case shifts IVL of the uterus treatment from ‘guideline adherence’ to ‘optimized protocols’, selecting surgical approaches based on quantified recurrence risk, achieving complete primary resection through preoperative MDT consultation, implementing precise monitoring via stratified follow-up and proactively managing the perioperative period through endocrine therapy. These insights offer practical wisdom for clinicians, particularly emphasizing that in rare disease management, ‘individualization’ must be grounded in data-driven stratification and multidisciplinary collaboration, rather than relying solely on vague, experiential judgements.
Supplementary Material
B-mode ultrasound. Evaluation of the morphology and echogenicity of the lesion, supplemented by color Doppler ultrasound to assess vascularity. For example, in the left adnexal region, a hypoechoic lesion measuring ~72x38 mm was detected, closely related to the uterus, with visible blood flow signals on color Doppler.
Color Doppler ultrasound. The area indicated by the arrow is the intravenous leiomyomatosis of the uterus.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be requested from the corresponding author.
Authors' contributions
YZ and FT confirm the authenticity of all the raw data. YZ and FT contributed to the conception of the study. YZ was responsible for writing the original draft and editing the manuscript. FT was responsible for reviewing and editing the manuscript. YZ was responsible for the acquisition of clinical data. FT was responsible for critical revision of the manuscript, and the analysis and interpretation of the data. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Ethics approval was provided by the Ethics Committee of Hebei General Hospital (Hebei, China). No information that could potentially compromise patient privacy or personal identity was included in this article.
Patient consent for publication
All the test results, images and permission for their publication were obtained with written informed consent from the patient.
Competing interests
The authors declare that they have no competing interests.
References
|
1
|
The Gynecological Oncology Group of the Chinese Medical Doctor Association's Obstetrics and Gynecology Physicians Branch. Clinical Diagnosis and Treatment Consensus for Pelvic Vein Intra-Smooth Muscle Tumors. Chin J Obst Gynecol. 58:252–258. 2023.(In Chinese).
|
|
2
|
Birch-Hirschfeld FV: Textbook of pathological anatomy. 5th edition. FCW Vogel, Leipzig, pp226-258, 1896.
|
|
3
|
Hu X and Du X: Research progress on uterine venous leiomyomatosis. J Tianjin Med Univ. 29:101–105. 2023.
|
|
4
|
He S and Jiang J: Clinical characteristics and treatment outcomes of angioleiomyoma of the female genital tract: A retrospective cohort study. BMC Womens Health. 24(479)2024.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Bosniak MA: The Bosniak renal cyst classification: 25 years later. Radiology. 262:781–785. 2012.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Xia M, Dai Q, Xu Z, Qi Z, Ouyang Y, Li J, Zhu Q, Jiang Y, Lyu K, Zhang Y, et al: Ultrasonic and CT characteristics of intravascular leiomyomatosis. Chin J Med Imaging Technol. 37:338–341. 2021.(In Chinese).
|
|
7
|
Sato H, Murakami K, Fujishima R, Otani T, Sakai K, Nishio K and Matsumura N: Uterine angioleiomyoma with disseminated intravascular coagulation: a case report. BMC Womens Health. 23(157)2023.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Fang Z, Lei L and Bao Z: Clinical analysis of 25 cases of intravascular smooth muscle tumor disease. J Cardiovasc Pulm Dis. 44:288–292. 2025.
|
|
9
|
Liu Y, Pan H, Wang H, Liao X and Yang L: Case report and clinical analysis of uterine intravascular leiomyoma. Mod Oncol Med. 32:3763–3768. 2024.
|
|
10
|
Boavida Ferreira J, Cabrera R, Santos F, Relva A, Vasques H, Gomes A, Guimarães A and Moreira A: Benign metastasizing leiomyomatosis to the skin and lungs, intravenous leiomyomatosis, and leiomyomatosis peritonealis disseminata: A series of five cases. Oncologist. 27:e89–e98. 2022.PubMed/NCBI View Article : Google Scholar
|