Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune
inflammatory disease that primarily affects the joints but may also
present with a wide range of extra-articular manifestations. With a
global prevalence of 0.5-1.0%, it predominantly occurs in
middle-aged and elderly populations (1) Patients with RA are at increased risk
of opportunistic infections due to underlying immune dysregulation
and the frequent use of immunosuppressive therapies, particularly
among those with comorbidities and high disease activity (2). Biological agents, including tumor
necrosis factor inhibitors (for example adalimumab or etanercept)
and interleukin-6 receptor antagonists (such as tocilizumab), have
been well documented to elevate the risk of
Aspergillus-related pulmonary infections, such as invasive
pulmonary aspergillosis (IPA) and chronic pulmonary aspergillosis
(CPA) (3,4). Notably, the diagnosis of pulmonary
aspergilloma remains challenging due to its non-specific clinical
manifestations, often requiring a multimodal approach combining
clinical, radiological, microbiological and pathological evidence
(5).
The present study reports a rare case of pulmonary
aspergilloma in a patient with RA who developed the infection as a
result of disease-related immune dysregulation and long-term
immunosuppressive therapy. The patient was a 75-year-old woman with
RA and a pre-existing pulmonary cavity secondary to prior
tuberculosis. Following prolonged immunosuppressive treatment, the
patient was diagnosed with pulmonary aspergilloma. Through detailed
morphological analysis of bronchoalveolar lavage fluid and lung
tissue specimens, the current report aims to enhance diagnostic
awareness of pulmonary aspergilloma, emphasize the infection risk
associated with long-term immunosuppressive therapy in patients
with autoimmune diseases, and highlight the diagnostic and
management challenges posed by Aspergillus infections,
particularly CPA, for infectious disease specialists.
Case report
Case presentation
In January 2024, a 75-year-old woman presented to
Hangzhou First People's Hospital with recurrent polyarticular
swelling and pain for >2 years, accompanied by a 1-week history
of productive cough. The patient had been diagnosed with RA 2 years
previously. Physical examination revealed swelling, pain and
stiffness of the interphalangeal and wrist joints of the index and
middle fingers of both hands, without obvious joint deformity. The
patient subsequently received immunosuppressive therapy with
tocilizumab 400 mg monthly injections in January, February, March
and April 2022. Despite treatment, the condition of the patient
progressed, and a boutonniere deformity developed in the right
middle finger. The patient also had a history of pulmonary
tuberculosis and poorly controlled RA; 1 week before admission, the
patient developed a cough with yellow sputum and was admitted in
Hangzhou First People's Hospital for further evaluation. On
admission, the blood pressure of the patient was 174/81 mmHg
(reference: 90-139/60-89 mmHg). The patient was conscious and
alert, with no cyanosis of the lips. Lung auscultation revealed no
obvious dry or wet rales, and the remainder of the physical
examination was unremarkable. Peripheral blood analysis showed a
white blood cell count of 11.4x109/l (reference:
4.0-10.0x109/l), neutrophil count of 73.6% (reference:
50-70%), lymphocyte count of 16.9% (reference: 20-40%), red blood
cell count of 4.11x1012/l (reference: 3.68-5.13x10¹²/l),
hemoglobin level of 117 g/l, (reference: 110-150 g/l) platelet
count of 241x1012/l (reference:
100-300x109/l), hypersensitive C-reactive protein level
of 36.1 mg/l (reference: 0-3 mg/l) and erythrocyte sedimentation
rate of 53 mm/h (reference: 0-20 mm/h). Urinalysis revealed occult
blood (dry chemistry) ++, leukocyte esterase (dry chemistry) +, red
blood cell count of 36/µl (reference: 0-13 /µl and mixed red blood
cell morphology. Mycobacterium tuberculosis (MTB) antigen
ESAT-6 was 13.00 (reference: <5) and MTB antigen CFP10 was 8.00
(reference: <5) with a positive T-SPOT test (Xiamen Wantai
Biological Pharmacy Enterprise Co., Ltd.). Sputum smears for
acid-fast bacilli and cryptococcal antigen were negative (data not
shown). Molecular testing for MTB and rifampicin resistance showed
no detection of MTB DNA by Xpert assay (Cepheid Inc.).
Bronchoscopic brush smears for acid-fast bacilli were negative
(data not shown). Laboratory test results are summarized in
Table I.
 | Table ILaboratory test results. |
Table I
Laboratory test results.
| Laboratory
tests | Results | Reference
range |
|---|
| White blood cell
count, /l |
11.4x109 |
4-10x109 |
| Neutrophils, % | 73.6 | 50-70 |
| Lymphocytes, % | 16.9 | 17-50 |
| Red blood cell
count, /l |
4.11x1012 |
3.5-5.0x1012 |
| Hemoglobin,
g/l | 117 | 110-150 |
| Platelet count,
/l |
241x109 |
100-300x109 |
| Serum amyloid A,
mg/l | 270.6 | ≤10 |
| Serum transferrin
saturation, % | 9.18 | 33-35 |
| Serum iron,
µmol/l | 3.9 | 7.8-32.2 |
| Total iron-binding
capacity | 42.5 µmol/l | 45-81 µmol/l |
| Urinary red blood
cells, /µl | 36 (mixed) | <3 |
| Urinary occult
blood | (++) | (-) |
| Rheumatoid factor,
IU/ml | 23.2 | 0-20 |
| Leukocyte
esterase | (+) | (-) |
| Anti-nuclear
antibody | Positive
(1:100) | (-) |
| Sub-karyotype of
anti-nuclear antibody | No karyotype | \ |
| Cyclic
citrullinated peptide antibody, U/ml | >500.00 | 0-20 |
| hypersensitive
C-reactive protein, mg/l | 36.1 | <10 |
| Erythrocyte
sedimentation rate, mm/h | 53 | 0-15 |
| BALF nucleated cell
count, /µl | 260 | <100 |
| BALF neutrophils,
% | 82 | <50 |
| GM assay | 0.98 | <0.5 |
Upper abdominal ultrasonography (including liver,
bile, pancreas and spleen): revealed gallbladder polyposis, right
kidney stones and a small amount of pleural effusion (Figs. S1 and S2). Routine electrocardiography and
vectorcardiography demonstrated sinus rhythm with frequent atrial
premature beats (with differential intraventricular conduction),
presenting as double rhythm, and notched P waves. ST-segment and
T-wave abnormalities were noted (ST segments in leads I, II, III,
aVL, aVF and V4-V6 showed horizontal depression of 0.03-0.09 mV; T
waves in leads I, aVL, V3 and V4 were low and flat; and leads II,
III, aVF, V5 and V6 showed biphasic changes). A prolonged Q-T
interval was also observed (460 ms; normal maximum: 380 ms).
Transthoracic echocardiography showed left heart enlargement, left
ventricular insufficiency, mild regurgitation of the mitral,
tricuspid and aortic valves, and arrhythmia, with a Simpson
ejection fraction of 0.42. Chest computed tomography (CT; plain
scan plus high-resolution target scan) revealed slightly increased
lung markings bilaterally, with multiple nodular, patchy, and
strip-like high-density shadows. Some lesions had indistinct
margins, and an air crescent sign was observed in certain areas
(Fig. 1B). Multiple infectious
lesions were present in both lungs, some showing a tendency toward
chronic fibrosis (Fig. S3).
Additional small nodules measuring 3-6 mm in diameter were noted
bilaterally. Multiple calcified lymph nodes were observed in the
left hilum and mediastinum. No significant pleural thickening was
identified, while an arcuate effusion was present in the left
thoracic cavity (Fig. 1C).
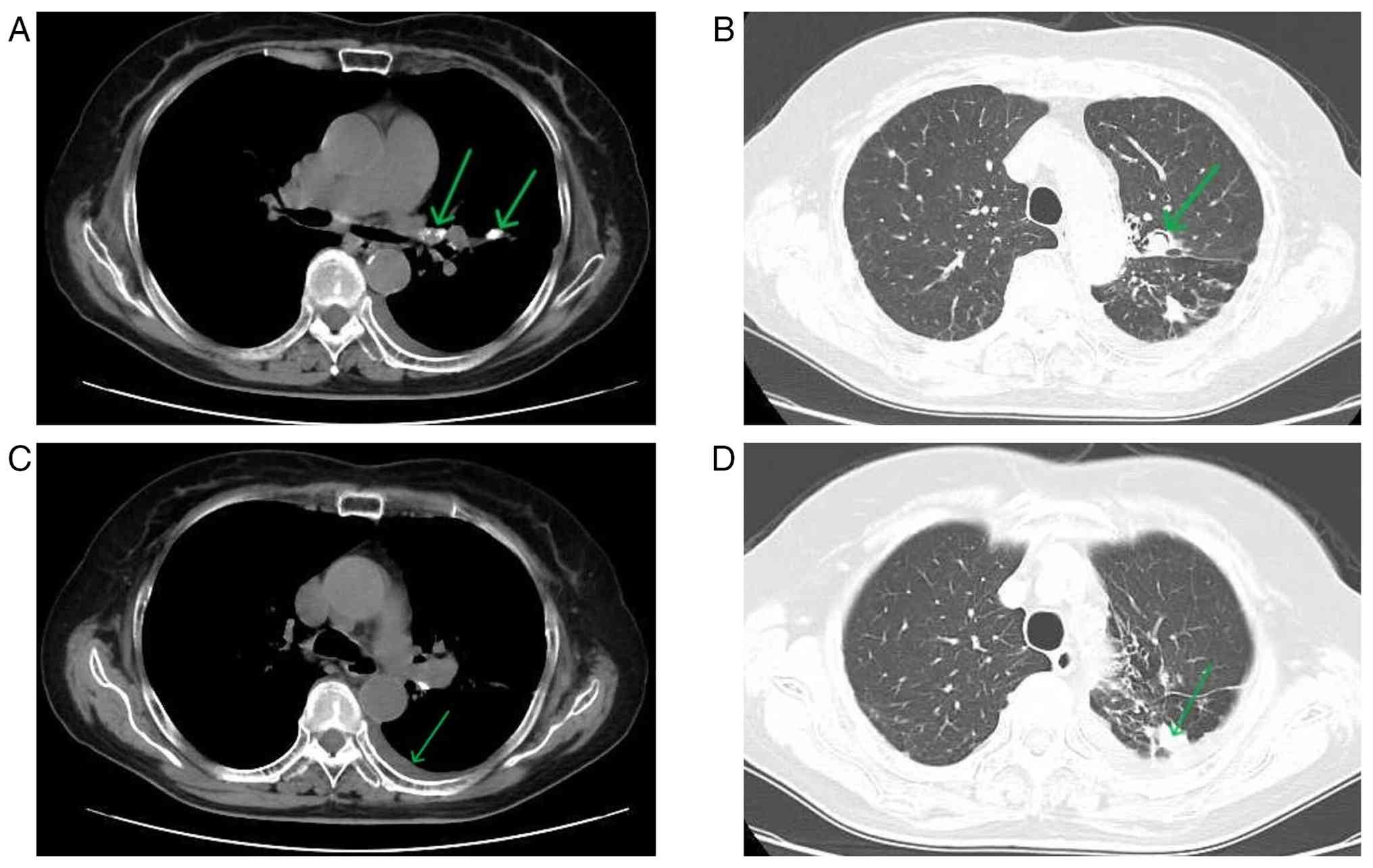 | Figure 1Imaging findings. (A) Calcified lymph
nodes (indicated by arrows); (B) air crescent sign (crescent-shaped
low-density area within a high-density nodule, indicated by arrow);
(C) left pleural effusion (arcuate fluid density shadow, indicated
by arrow); (D) left lung inflammatory lesion (patchy high-density
shadow with ill-defined border, indicated by arrow). CT parameters:
120 kV, 80 mAs, 1-mm slice thickness, lung window (WL: -600 HU, WW:
1,500 HU), mediastinal window (WL: 40 HU, WW: 400 HU). CT, computed
tomography; WL. |
Cell morphology analysis of
bronchoalveolar lavage fluid (BALF)
Cytological examination of the BALF revealed
blood-tinged fluid, with a total nucleated cell count of 260
cells/µl (reference: 100-200 cells/µl). Differential cell count
analysis identified a predominant neutrophilic inflammatory
pattern, with 82% neutrophils (reference: <3%), 6% lymphocytes
(reference: 5-15%), 9% alveolar macrophages (reference: 80-95%),
and 3% eosinophils (reference: <1%).
Microscopic evaluation revealed numerous dense
fungal clusters, with thick, intertwined hyphae aggregated into
irregular masses and clumps (Fig.
2A, C and F). Clear septation of the fungal hyphae
(a key morphological marker for Aspergillus) was visualized
under high-magnification staining (Fig. 2B and D), and abundant fungal mycelia were
further confirmed by fluorescence staining (Fig. 2E). No fungal spores were detected
in the BALF specimens; however, the hyphal morphological features
were highly suggestive of Aspergillus infection, which was
subsequently verified by fungal culture and phenotypic
identification (Fig. 2H and
I).
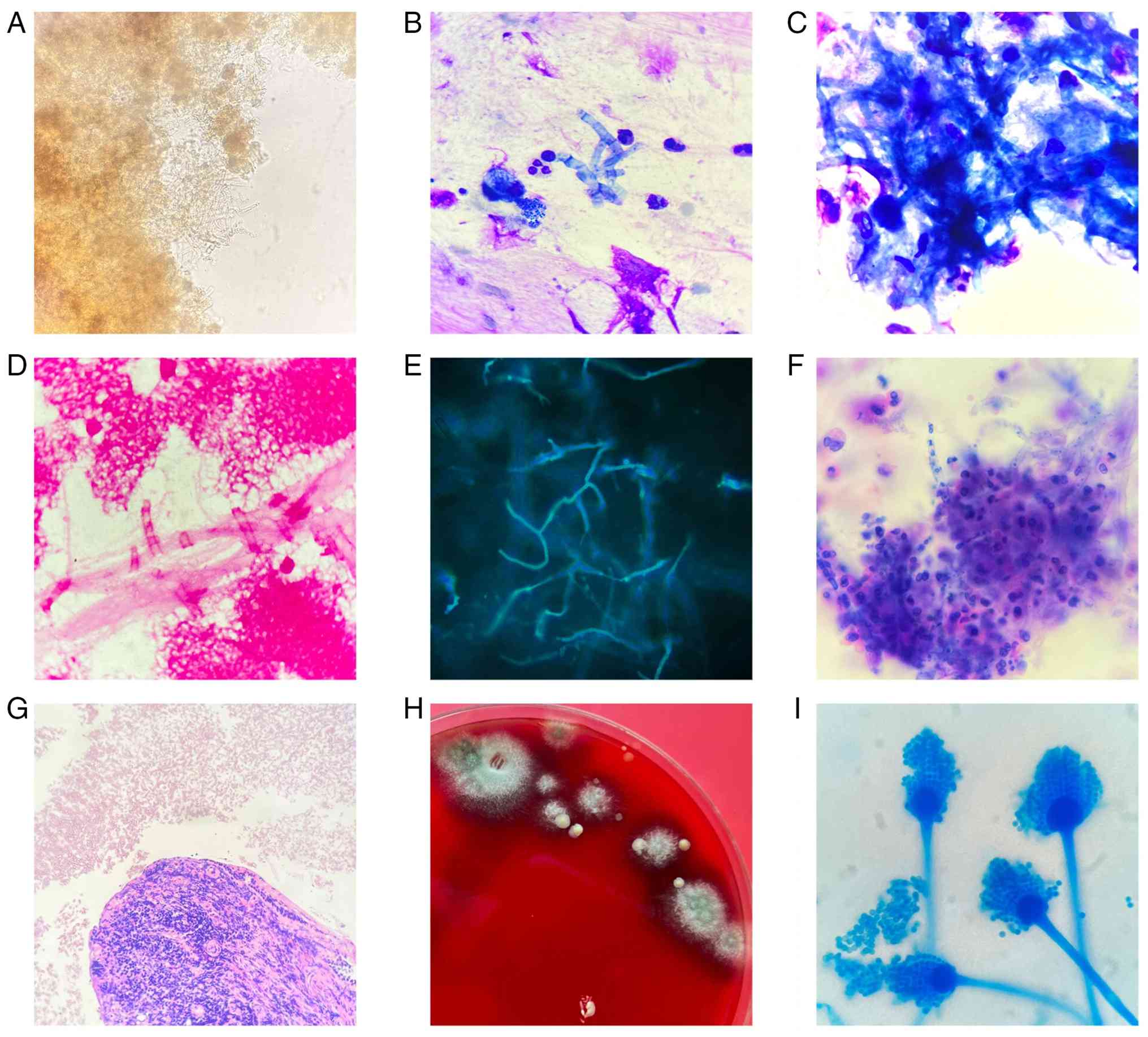 | Figure 2Morphology of pulmonary
Aspergillus fumigatus aspergilloma. (A) BALF, wet film
unstained (magnification, x400), a large number of fungi can be
seen in dense clusters, and the mycelium can be seen at the edge of
each other and disorderly arrangement. (B) BALF, Wright-Giemsa
stain (magnification x1,000), small segments of mycelia-like
bamboo, dyed light blue, and mycelia division is clear. (C) BALF,
Reichsen-Giemsa staining (magnification x1,000), numerous mycelial
interleaved fungal clusters. (D) BALF, Gram staining
(magnification, x1,000), mycelium staining is light, and obviously
visible. (E) BALF, fungal fluorescence staining (magnification,
x400), showing a large number of fungal mycelia. (F) BALF cell
block (magnification, x400), clumps of Aspergillus hyphae.
(G) A biopsy of the anterior segment of the upper lobe of the lung,
broken mucosal tissues (magnification, x100), extensive
infiltration of lymphocytes, plasma cells and neutrophils in the
mucosal interstitium (black arrow): Also see Aspergillus
cluster (red arrow). It can be seen that Aspergillus cluster
and lung tissue separation, in line with the formation of
aspergilloma structure characteristics. (H) Lavage culture, colony
after 3 days of Columbia blood plate culture, arrow point. (I)
A. fumigatus after 3 days of lavage culture, phenol cotton
blue staining (magnification, x1,000). BALF, bronchoalveolar lavage
fluid. |
Microbiological examination. Culture and
identification of bacteria and fungi from BALF yielded growth of
Aspergillus fumigatus. Routine bacterial and fungal cultures
were otherwise negative, with no additional fungal or bacterial
growth detected. The Aspergillus galactomannan (GM) assay
was positive, with a value of 0.98, supporting the diagnosis of
Aspergillus infection. Sputum cultures were repeatedly
negative for bacterial and fungal pathogens.
Pathological examination. The pathological
report of the ‘left anterior lobe brush smear’ showed scattered
hyperplasia of bronchial mucosal epithelial cells without
significant atypia. Another pathological report of the ‘BALF cell
block (left upper lobe proper branch)’ revealed no malignant cells;
however, clusters of Aspergillus hyphae were noted.
Pathological examination of the ‘biopsy of the anterior left upper
lobe’ demonstrated fragmented mucosal tissue with extensive
infiltration of lymphocytes, plasma cells and neutrophils within
the mucosal interstitium, along with visible Aspergillus
clusters. Metagenomic next-generation sequencing (mNGS) of two BALF
samples further supported Aspergillus infection, and these two
samples correspond to the two datasets under accession no.
PRJNA1397972 in the National Center for Biotechnology Information
Sequence Read Archive database.
Treatment and follow-up. The patient received
antifungal therapy with oral voriconazole at a dose of 200 mg every
12 h (q12 h). The patient's inflammatory indices decreased
significantly and normalized after treatment. The specific paired
pre- and post-treatment levels (reference range in parentheses)
were: white blood cell count (WBC) 11.4x109/l
(4-10x109/l) → 5.4x109/l
(3.6-9.6x109/l); neutrophil percentage (NEUT%) 73.6%
(50-70%) → 60.2% (40-75%); absolute neutrophil count
8.4x109/l (1.8-6.3x109/l) →
3.3x109/l (1.8-6.3x109/l); hypersensitive
C-reactive protein (hs-CRP) 36.1 mg/l (<10 mg/l) → 9.5 mg/l
(0-17.0 mg/l). All elevated markers returned to the normal range
after treatment, and the patient was discharged after her condition
improved. After discharge, oral voriconazole 200 mg q12h was
continued for 6 months. At follow-up in November 2024, the
patient's cough and sputum symptoms resolved completely.
Discussion
Pathogenesis
The present patient had poorly controlled RA for 2
years and had received four standard monthly doses of tocilizumab
as immunosuppressive therapy. The patient also had multiple
comorbidities, including gallbladder polyposis, right kidney
stones, pleural effusion, arrhythmias (frequent atrial and
ventricular premature beats) and chronic heart failure. Advanced
age, RA-associated immune dysregulation, long-term
immunosuppressive therapy and pre-existing comorbidities constitute
major high-risk factors for Aspergillus infection (6). Notably, the patient's history of
pulmonary tuberculosis resulted in the formation of tuberculous
cavities. These avascular structures provide an ideal niche for
Aspergillus colonization, as supported by a study from New
Delhi reporting that 57% of post-tuberculosis patients develop
pulmonary aspergillosis (7), with
tuberculous cavities facilitating microbial persistence and
survival (8). Such colonization
may ultimately lead to aspergilloma formation, the hallmark
radiological feature of CPA, along with the characteristic air
crescent sign on chest CT (9).
Aspergillus species are saprophytic molds
that thrive on decaying organic matter and produce airborne conidia
that are readily inhaled by humans (10). Clinical manifestations depend on
host immune status and underlying pulmonary structure and are
broadly classified as allergic bronchopulmonary aspergillosis, CPA
and IPA (11), with aspergilloma
considered a pathognomonic manifestation of CPA (12). Aspergillus is the most
common cause of pulmonary fungal balls, which are termed
aspergillomas. Immunocompromised individuals, including those with
chronic diseases such as asthma, chronic obstructive pulmonary
disease, diabetes and rheumatic diseases (13), as well as those undergoing
chemotherapy, organ transplantation or invasive medical procedures,
are particularly susceptible to tuberculosis-fungal co-infections,
which may result in severe pulmonary dysfunction and increased
mortality (14). Over the past 5
decades, the global incidence of invasive fungal infections has
markedly increased, driven by the expanding population of
susceptible hosts .
The present case underscores the importance of
heightened vigilance for Aspergillus infections,
particularly CPA, in patients receiving long-term immunosuppressive
therapy (15). In addition to
corticosteroids, biological agents, including tumor necrosis factor
inhibitors (infliximab, etanercept and adalimumab), anti-CD20
monoclonal antibodies (rituximab), anti-CD28 fusion proteins
(abatacept) and interleukin-6 receptor antagonists (tocilizumab),
have been associated with an increased risk of fungal infections in
patients with autoimmune diseases (4,16,17).
Consistent with these findings, Baliga et al (18) reported five cases of pulmonary
aspergillosis in immunosuppressed patients with antineutrophil
cytoplasmic antibody-associated vasculitis. Deana et al
(19) described pulmonary
aspergillosis following tocilizumab therapy in a patient with
coronavirus disease 2019. These reports parallel the current case,
in which CPA developed after four standard monthly doses of
tocilizumab, suggesting that cumulative immunosuppression, rather
than dosing frequency alone, plays a critical role in infection
risk (20). For high-risk patients
requiring biological therapy, the 2023 Spanish Society of
Rheumatology guidelines recommend abatacept as a safer alternative
due to its lower associated infection risk (21). In addition, mesenchymal stem cell
therapy has emerged as a potential treatment strategy for RA,
demonstrating effective inhibition of T-cell proliferation with
minimal reported adverse effects (22,23).
Diagnostic challenges
The initial potential misclassification of the
current case as IPA highlights the diagnostic complexity of
Aspergillus-related pulmonary diseases. According to the
2016 European Society of Clinical Microbiology and Infectious
Diseases guidelines for CPA, the clinical features observed in the
present patient, including the presence of an aspergilloma within a
pre-existing tuberculous cavity, an air crescent sign on chest CT,
and the absence of neutropenia or high-dose corticosteroid use,
support a diagnosis of CPA (aspergilloma subtype) rather than IPA.
This distinction is critical for accurate clinical management and
appropriate research reporting. The diagnosis of CPA relies on a
combination of clinical, radiological, microbiological and
pathological evidence, as no single diagnostic gold standard exists
(5).
i) BALF-based diagnostics. Direct
morphological identification of septate, branching hyphae
consistent with Aspergillus species enables early diagnosis
and is considerably faster than culture-based methods, which may
require days to weeks (17). Knox
et al (16) emphasized the
pivotal role of BALF cytomorphology in the diagnosis of pulmonary
fungal infections, including aspergillosis. Furthermore, the BALF
GM assay, using a cutoff value of >0.5, demonstrates a
sensitivity of 89% and specificity of 79% for Aspergillus
infections (24). In the present
patient, a GM value of 0.98 provided strong microbiological support
for diagnosis.
ii) Imaging findings. The presence of an air
crescent sign and an aspergilloma within a pre-existing tuberculous
cavity represents classic CT hallmarks of CPA, both of which were
clearly demonstrated in the current case.
iii) Metagenomic NGS (mNGS). This technique
offers high sensitivity, rapid pathogen identification, and a broad
detection spectrum, including mixed infections (25). It has been shown to outperform
conventional etiological methods and serum (1,3)-β-D-glucan testing in patients with
pulmonary aspergillosis (26).
iv) Laboratory and histopathological
findings. Elevated total white blood cell counts and neutrophil
levels (27), consistent with our
patient's laboratory results, support an inflammatory response.
Furthermore, pathological biopsy revealing isolated
Aspergillus clusters, separated from the surrounding lung
tissue, confirms the structural characteristics of an aspergilloma.
Non-specific respiratory symptoms, such as cough and productive
sputum, are common in immunocompromised patients (28). This lack of specificity frequently
leads to diagnostic delays, which may adversely affect treatment
outcomes. Therefore, we recommend early implementation of BALF
cytological examination, GM testing and mNGS in immunosuppressed
patients presenting with respiratory symptoms, complemented by
multidisciplinary evaluation to exclude diseases with overlapping
clinical and radiological features (29), thereby facilitating timely and
accurate diagnosis of CPA.
Treatment dilemmas
The management of pulmonary aspergilloma, a subtype
of CPA, remains controversial, with the choice between surgical and
conservative approaches guided by patient-specific factors
(30). Surgical resection is
presently considered the gold standard for symptomatic patients
with recurrent or severe hemoptysis, as it is associated with a
5-year survival rate of 84%, which is significantly higher than
that achieved with medical therapy alone (41%) (31). However, postoperative
complications, including bleeding, empyema, bronchopleural fistula
and Aspergillus seeding, occur in ~28% of patients with
cavitary disease, a rate that is 5-10 times higher than that
observed in the general population (32). By contrast, among asymptomatic
patients, survival outcomes are comparable between surgical and
medical management (75 vs. 65%, respectively) (31), supporting a conservative treatment
strategy in this group.
Conservative management of aspergilloma is often
challenging because the avascular nature of pulmonary cavities and
aspergillomas limits antifungal drug penetration (29). Nonetheless, antifungal therapy can
effectively alleviate clinical symptoms. Voriconazole is preferred
over itraconazole for patients with aspergilloma or cavitary
disease, as it is associated with fewer adverse effects and more
reliable achievement of therapeutic drug concentrations (33-34).
Other non-surgical interventions, including endovascular antifungal
infusion and bronchoscopic resection under general anesthesia, have
been described in a small retrospective study (35).
Learning points
Clinicians should maintain a high index of suspicion
for Aspergillus infection, particularly CPA, in older adults
with autoimmune diseases such as RA who are receiving biological
therapy, especially tocilizumab. This is particularly important in
patients with pre-existing pulmonary cavities, such as those
resulting from prior tuberculosis. Standardized terminology and
accurate disease classification, specifically distinguishing CPA
from IPA, are essential for effective clinical communication and
management. Multimodal diagnostic approaches, including BALF
morphology, GM assay, mNGS, imaging and histopathological
examination, facilitate early and accurate diagnosis. For
asymptomatic patients with CPA who have comorbidities that preclude
surgical intervention, voriconazole-based conservative therapy may
achieve favorable outcomes. Moreover, selection of biological
agents for high-risk patients with RA should adhere to relevant
clinical guidelines to minimize the risk of opportunistic fungal
infections.
Conclusion
Older adults, immunocompromised populations and
patients with autoimmune diseases, particularly those receiving
immunosuppressive therapy, should be carefully monitored for the
development of Aspergillus infections, especially CPA. The
disease often presents with an insidious onset and non-specific
clinical manifestations. Morphological examination of BALF provides
valuable diagnostic specificity and may enable early presumptive
diagnosis. GM testing and mNGS of BALF should be performed promptly
when Aspergillus infection is suspected. When combined with
comprehensive assessment of imaging, histopathology,
microbiological and molecular findings, early and accurate
diagnosis can be achieved, thereby guiding appropriate antifungal
therapy. A history of pulmonary tuberculosis and the presence of
pulmonary aspergilloma further increase the complexity of
antifungal management. Overall, heightened clinical vigilance for
rare infections in patients with rheumatic diseases receiving
immunosuppressive agents, together with early diagnosis of fungal
infections, is essential for effective treatment outcomes.
Supplementary Material
Additional grayscale abdominal
ultrasound images of the gallbladder. The upper panel shows a
longitudinal view of the gallbladder, again demonstrating the
non-shadowing, non-mobile hyperechoic lesions of gallbladder
polyposis for confirmation. The lower panel presents a transverse
view of the gallbladder and adjacent hepatic parenchyma, showing no
evidence of biliary tract dilatation or additional focal
lesions.
Grayscale abdominal ultrasound images
of the gallbladder and right kidney. The upper panel shows a
longitudinal view of the gallbladder, demonstrating non-shadowing,
non-mobile hyperechoic lesions attached to the gallbladder mucosa,
consistent with gallbladder polyposis. The lower panel presents a
transverse view of the right kidney, with hyperechoic foci within
the renal collecting system suggestive of nephrolithiasis, and a
small anechoic fluid collection in the right costophrenic angle
consistent with mild pleural effusion.
Chest CT showing bilateral lung
lesions. This axial view at the level of the trachea demonstrates
multiple infectious lesions distributed in both lungs, with some
lesions showing a tendency toward chronic fibrosis. A focal area of
increased attenuation is visualized in the left lower lobe,
consistent with the described pathological changes. The central
airways and mediastinal structures appear unremarkable at this
slice level. CT, computed tomography.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by Zhejiang Provincial
Science and Technology Program for Disease Prevention and Control
(grant no. 2025JK256).
Availability of data and materials
The raw mNGS data generated in the present study may
be found in the National Center for Biotechnology Information
Sequence Read Archive database under accession number PRJNA1397972
or at the following URL: https://www.ncbi.nlm.nih.gov/sra/PRJNA1397972. All
other relevant data in the present study may be requested from the
corresponding author.
Authors' contributions
YZ contributed to study conception and design,
collated clinical cases, acquired and interpreted data, drafted the
manuscript, and provided experimental and writing guidance. YL
performed morphological examination of bronchoalveolar lavage
fluid. FZ prepared laboratory experiments and assisted with sample
processing. XW conducted culture, identification and morphological
analysis of pathogenic microorganisms. XH collected imaging data
and performed diagnostic analysis. JJ contributed to study
conception and design and provided critical revision and writing
guidance. RZ contributed to data analysis and interpretation,
drafted the manuscript and critically revised the intellectual
content. YZ and RZ confirm the authenticity of all raw data. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Affiliated Hangzhou First People's Hospital (Westlake
University School of Medicine; approval no. 2025ZN488-1) with a
waiver of written informed consent, as the patient's data and
images were fully de-identified and the publication posed no
potential risks to the patient's privacy or rights. The study was
conducted in accordance with the Declaration of Helsinki.
Patient consent for publication
Patient consent for publication was waived by the
Ethics Committee of Affiliated Hangzhou First People's Hospital
(Westlake University School of Medicine; approval no. 2025ZN488-1).
All patient data and images have been fully de-identified, and the
publication poses no potential risks to the patient's privacy or
rights.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Venetsanopoulou AI, Alamanos Y, Voulgari
PV and Drosos AA: Epidemiology of rheumatoid arthritis: Genetic and
environmental influences. Expert Rev Clin Immunol. 18:923–931.
2022.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Fragoulis GE, Nikiphorou E, Dey M, Zhao
SS, Courvoisier DS, Arnaud L, Atzeni F, Behrens GM, Bijlsma JW,
Böhm P, et al: 2022 EULAR recommendations for screening and
prophylaxis of chronic and opportunistic infections in adults with
autoimmune inflammatory rheumatic diseases. Ann Rheum Dis.
82:742–753. 2023.PubMed/NCBI View Article : Google Scholar
|
|
3
|
AL-Janabi Ali: Therapeutic effects of
Rheumatoid Arthritis on Aspergillosis development. Rev Clin Med.
6:155–164. 2019.
|
|
4
|
Lease ED and Alexander BD: Fungal
diagnostics in pneumonia. Semin Respir Crit Care Med. 32:663–672.
2011.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Barac A, Vujovic A, Drazic A, Stevanovic
G, Paglietti B, Lukic K, Stojanovic M and Stjepanovic M: Diagnosis
of chronic pulmonary aspergillosis: Clinical, radiological or
laboratory? J Fungi (Basel). 9(1084)2023.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Denning DW, Cadranel J, Beigelman-Aubry C,
Ader F, Chakrabarti A, Blot S, Ullmann AJ, Dimopoulos G and Lange
C: European Society for Clinical Microbiology and Infectious
Diseases and European Respiratory Society. Chronic pulmonary
aspergillosis: Rationale and clinical guidelines for diagnosis and
management. Eur Respir J. 47:45–68. 2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Singla R, Singhal R and Rathore R: Risk
factors for chronic pulmonary aspergillosis in post-TB patients.
Int J Tuberc Lung Dis. 25:324–426. 2021.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Park Y, Kim TS, Yi CA, Cho EY, Kim H and
Choi YS: Pulmonary cavitary mass containing a mural nodule:
Differential diagnosis between intracavitary aspergilloma and
cavitating lung cancer on contrast-enhanced computed tomography.
Clin Radiol. 62:227–232. 2007.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Carter C, Kahai R, Cunningham J, Kilduff
J, Hough N, Baxter C, Connell D and Shah A: Chronic pulmonary
aspergillosis-a guide for the general physician. Clin Med (Lond).
24(100019)2024.PubMed/NCBI View Article : Google Scholar
|
|
10
|
McCormick A, Loeffler J and Ebel F:
Aspergillus fumigatus: Contours of an opportunistic human
pathogen. Cell Microbiol. 12:1535–1543. 2010.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Russo A, Tiseo G, Falcone M and Menichetti
F: Pulmonary aspergillosis: An evolving challenge for diagnosis and
treatment. Infect Dis Ther. 9:511–524. 2020.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Portaels J, Crombrugge EV, Broeck WVD,
Lagrou K, Laval K and Nauwynck H: Aspergillus fumigatus
spore proteases alter the respiratory mucosa architecture and
facilitate equine herpesvirus 1 infection. Viruses.
16(1208)2024.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Dabuo B, Xorlali N, Timothy Amoliga N,
Kono Atibodu Z, Mavis Newman P, Mohammed A, Mohammed A, Adongsakiya
Ali R and Abudu A: Aspergillus and Aspergillosis in People
with Chronic Diseases. In: Razzaghi-Abyaneh M, Rai M,
Shams-Ghahfarokhi M, (eds.). Infectious Diseases. IntechOpen, 2023.
https://doi.org/10.5772/intechopen.111863.
|
|
14
|
Amiri MRJ, Siami R and Khaledi A:
Tuberculosis status and coinfection of pulmonary fungal infections
in patients referred to reference laboratory of health centers
ghaemshahr city during 2007-2017. Ethiop J Health Sci. 28:683–690.
2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Lu M and Zhang L, Li Y, Wang H, Guo X,
Zhou J, Duan L, Si X, Xu Y and Zhang L: Recommendation for the
diagnosis and management of immune checkpoint inhibitor related
infections. Thorac Cancer. 11:805–809. 2020.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Knox KS and Meinke L: Role of
bronchoalveolar lavage diagnostics in fungal infections. Clin Chest
Med. 30:355–365. 2009.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Lion T, (ed.): Human Fungal Pathogen
Identification: Methods and Protocols. New York, NY, Springer New
York, 2017. https://doi.org/10.1007/978-1-4939-6515-1.
|
|
18
|
Baliga S, Yadav S, Sagdeo P and
Balakrishnan C: Invasive fungal infection in ANCA-associated
vasculitis: Between the Devil and Deep blue sea. Case series and
review of the literature. Clin Rheumatol. 43:785–797.
2024.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Deana C, Vetrugno L, Bassi F and De Monte
A: Tocilizumab administration in COVID-19 patients: Water on the
fire or gasoline? Med Mycol Case Rep. 31:32–34. 2021.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Patterson TF, Thompson GR III, Denning DW,
Fishman JA, Hadley S, Herbrecht R, Kontoyiannis DP, Marr KA,
Morrison VA, Nguyen MH, et al: Practice guidelines for the
diagnosis and management of aspergillosis: 2016 update by the
infectious diseases society of America. Clin Infect Dis. 63:e1–e60.
2016.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Balsa A, Díaz Del Campo Fontecha P, Silva
Fernández L, Valencia Martín J, Nistal Martínez V, León Vázquez F,
Hernández Hernández MV, Corominas H, Cáliz Cáliz R, Aguado García
JM, et al: Recommendations by the Spanish Society of Rheumatology
on risk management of biological treatment and JAK inhibitors in
patients with rheumatoid arthritis. Reumatol Clin (Engl Ed).
19:533–548. 2023.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Tsiapalis D, Floudas A, Tertel T, Boerger
V, Giebel B, Veale DJ, Fearon U and O'Driscoll L: Therapeutic
effects of Mesenchymal/Stromal stem cells and their derived
extracellular vesicles in rheumatoid arthritis. Stem Cells Transl
Med. 12:849–862. 2023.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Di Nicola M, Carlo-Stella C, Magni M,
Milanesi M, Longoni PD, Matteucci P, Grisanti S and Gianni AM:
Human bone marrow stromal cells suppress T-lymphocyte proliferation
induced by cellular or nonspecific mitogenic stimuli. Blood.
99:3838–3843. 2002.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Li C, Sun L, Liu Y, Zhou H, Chen J, She M
and Wang Y: Diagnostic value of bronchoalveolar lavage fluid
galactomannan assay for invasive pulmonary aspergillosis in adults:
A meta-analysis. J Clin Pharm Ther. 47:1913–1922. 2022.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Czurda S and Lion T: Broad-Spectrum
molecular detection of fungal nucleic acids by PCR-based
amplification techniques. Methods Mol Biol. 1508:257–266.
2017.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Bao S, Song H, Chen Y, Zhong C and Tang H:
Metagenomic next-generation sequencing for the diagnosis of
pulmonary aspergillosis in non-neutropenic patients: A
retrospective study. Front Cell Infect Microbiol.
12(925982)2022.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Hou X, Zhang H, Kou L, Lv W, Lu J and Li
J: Clinical features and diagnosis of chronic pulmonary
aspergillosis in Chinese patients. Medicine (Baltimore).
96(e8315)2017.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Jensen HE and Becker CB: Pathological
diagnosis of pulmonary aspergillosis. Semin Respir Crit Care Med.
45:41–49. 2024.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Ngo Nonga B, Bang GA, Jemea B, Savom E,
Yone P, Mbatchou N and Ze JJ: Complex pulmonary aspergilloma:
Surgical challenges in a third world setting. Surg Res Pract.
2018(6570741)2018.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Evans TJ, Lawal A, Kosmidis C and Denning
DW: Chronic pulmonary aspergillosis: Clinical presentation and
management. Semin Respir Crit Care Med. 45:88–101. 2024.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Shen C, Qiao G, Wang C, Jin F and Zhang Y:
Outcomes of surgery for different types of chronic pulmonary
aspergillosis: Results from a single-center, retrospective cohort
study. BMC Pulm Med. 22(40)2022.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Kim YT, Kang MC, Sung SW and Kim JH: Good
Long-term outcomes after surgical treatment of simple and complex
pulmonary aspergilloma. Ann Thorac Surg. 79:294–298.
2005.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Bongomin F, Harris C, Hayes G, Kosmidis C
and Denning DW: Twelve-month clinical outcomes of 206 patients with
chronic pulmonary aspergillosis. PLoS One.
13(e0193732)2018.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Tashiro M, Takazono T, Saijo T, Yamamoto
K, Imamura Y, Miyazaki T, Kakeya H, Ando T, Ogawa K, Kishi K, et
al: Selection of oral antifungals for initial maintenance therapy
in chronic pulmonary Aspergillosis: A longitudinal analysis. Clin
Infect Dis. 70:835–842. 2020.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Elaine Dumoulin and Christina Thornton:
Endoscopic aspergilloma management for non-surgical patients. Eur
Respir J. 62 (suppl 67)(PA460)2023.
|














