Introduction
Psoriasis is an immune-mediated inflammatory disease
with a global prevalence of 2-3% (1,2).
Chronic plaque or psoriasis vulgaris (PsV), the most common
subtype, is a multifactorial condition involving complex genetic,
immunologic and environmental interactions (1,2).
Genetic studies have identified numerous PsV risk loci, primarily
associated with immune pathways, inflammatory cascades and
epidermal homeostasis, underscoring its polygenic yet partially
elucidated genetic nature (3,4).
Vitamin D (VitD) has attracted attention in
psoriasis research due to its pleiotropic effects on key psoriatic
elements (5-9).
Recent data further support a broader cutaneous VitD-related
metabolome that may influence skin homeostasis and inflammation
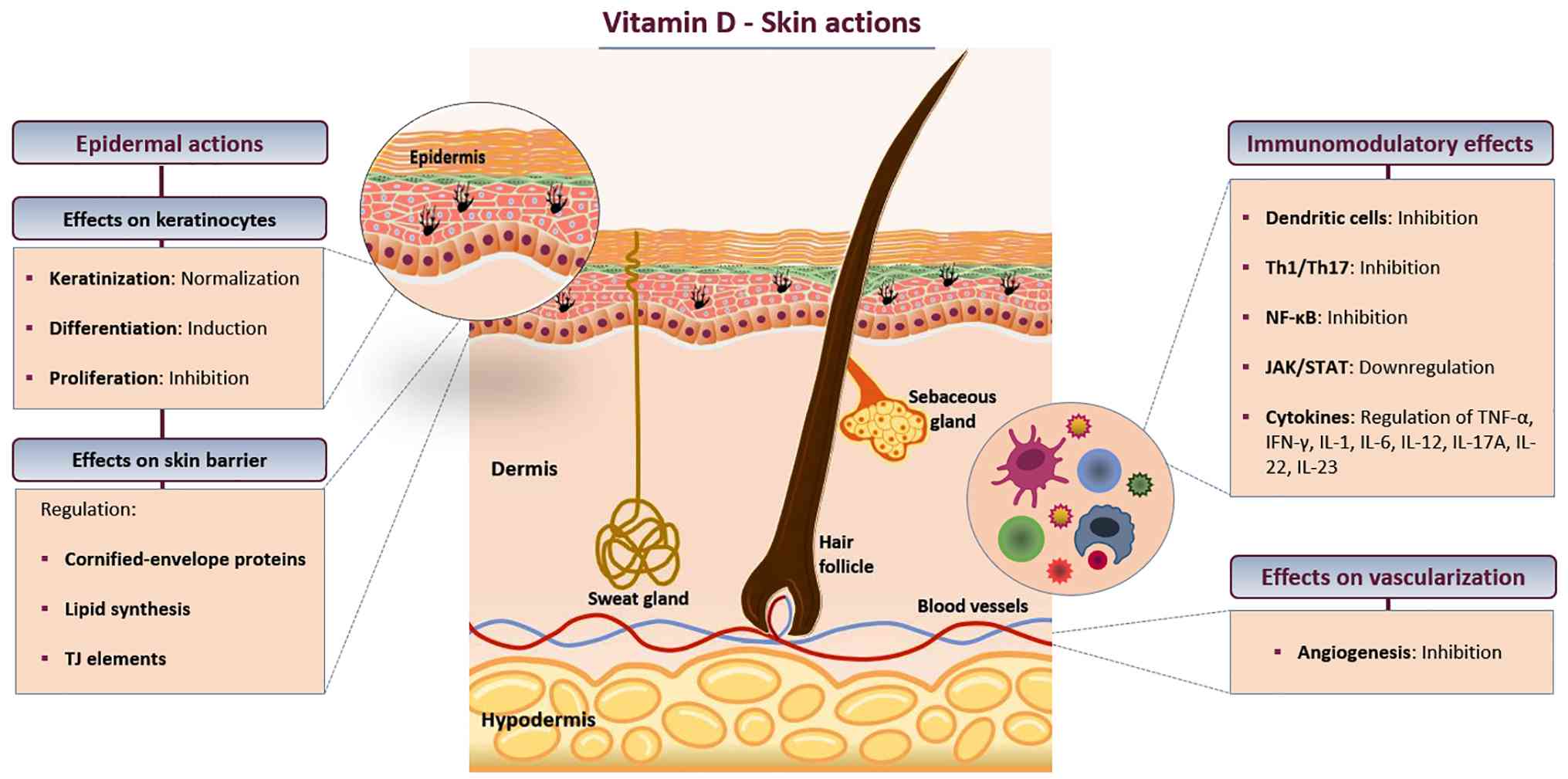
(10). VitD promotes keratinocyte
differentiation while inhibiting proliferation, thereby
counteracting the epidermal hyperplasia of psoriatic plaques
(5,6). It also enhances skin barrier
integrity by regulating cornified-envelope proteins, such as
involucrin and loricrin, lipid synthesis and tight junction
components, including claudins (5,7).
Beyond its epidermal actions, VitD exerts anti-inflammatory and
immunomodulatory effects, including the suppression of plasmacytoid
dendritic cells (central initiators of psoriatic inflammation) and
inhibition of the T helper (Th)-1/Th17 axis, downregulating
associated cytokines (e.g., TNF-α, IFN-γ, IL-1, IL-2, IL-6, IL-8,
IL-12, IL-17, IL-22 and IL-23) (5,6). In
addition, VitD interferes with major psoriasis-related pathways,
including NF-κB and JAK/STAT signaling, and also exerts
anti-angiogenic activity, thereby mitigating neovascularization in
psoriatic lesions (Fig. 1)
(5,8,9).
Previous studies have reported a potential link
between VitD deficiency and psoriasis, demonstrating inverse
associations between serum VitD levels and disease risk or severity
(5,11,12).
In addition, altered VitD receptor (VDR) expression has been
observed in psoriatic skin (5,7).
From a therapeutic perspective, phototherapy, widely used in
psoriasis management, may partly exert its effects by elevating
serum VitD levels and/or upregulating VDR expression in lesional
skin (5,13,14).
Furthermore, VitD-based interventions have been shown to be
beneficial in psoriasis. Although oral supplementation remains
controversial across studies, topical VitD analogs are established
treatment modalities (5).
Since the nuclear VDR is the main mediator of most
biological actions of active 1,25-dihydroxy VitD3
(5), the VDR gene has been
investigated in relation to psoriasis (15). Located on chromosome 12q13.11, the
VDR gene is highly polymorphic containing numerous
single-nucleotide polymorphisms (SNPs) that may alter VDR
expression or function (16-18).
Among the most widely studied VDR variants are FokI (rs2228570;
exon 2; +30920 C>T), near the start codon and BsmI (rs1544410;
intron 8; + 63980 G>A) and TaqI (rs731236; exon 9; +65058 T >
C) both in the 3'-untranslated region (3'-UTR) (16-18).
FokI involves a T-to-C substitution that alters the translation
initiation site (ATG to ACG), creating two VDR isoforms of
different length (427 vs. 424 amino acids) and transcriptional
capacity (17,18). The shorter isoform (associated with
the C allele) is more transcriptionally active (16-19),
potentially enhancing downstream VitD/VDR signaling. FokI is thus a
VDR SNP that exhibits a functional impact on protein activity. By
contrast, the 3'-UTR non-functional BsmI (G-to-A substitution) and
TaqI (T-to-C transition) variants do not alter the protein
structure but may influence VDR gene expression and protein levels
by affecting mRNA stability, splicing patterns or through linkage
disequilibrium (LD) with other functional polymorphisms within the
VDR locus (16-19).
Particularly for TaqI, its location within a CpG island, where
allele-dependent methylation patterns (TT absent, TC partial and CC
complete) have been described, could further modulate VDR
expression in ethnic-, disease- or tissue/cell-specific contexts
(17,19,20).
A number of studies have suggested potential
associations between these VDR variants and psoriasis. However, the
results have been inconsistent, even within certain populations,
possibly due to ethnic genetic or epigenetic variation and/or
differences in psoriasis clinical spectrum among cohorts,
emphasizing the need for ethnically and clinically stratified
research. In addition, associations between these VDR SNPs and
psoriasis-related clinical features remain understudied and may
benefit from phenotype stratification (15,16,21-23).
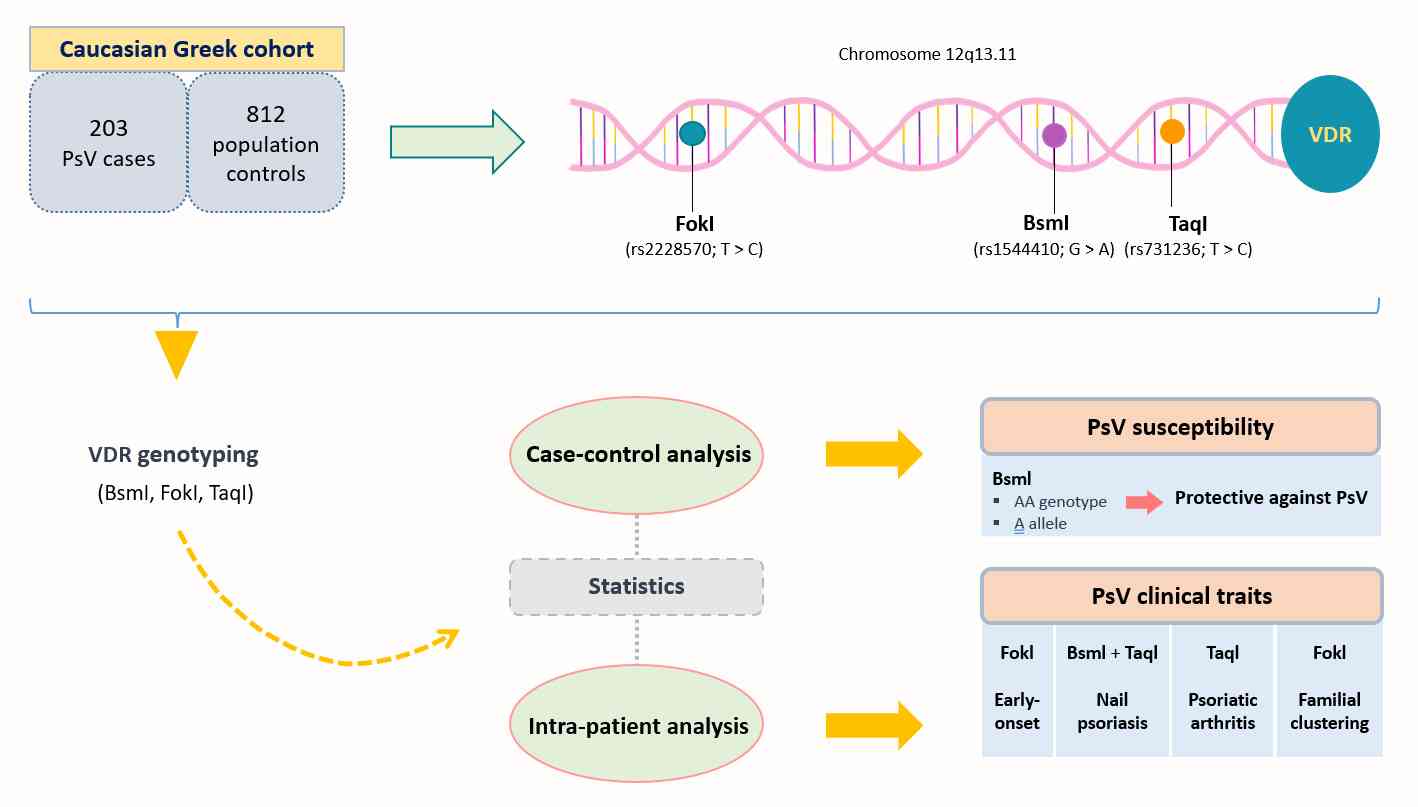
To the best of our knowledge, the impact of VDR
FokI, BsmI and TaqI on psoriasis has not yet been studied in the
Greek population. Given the ethnic variability in genetic
polymorphisms (18) and the
clinical diversity of psoriasis across studies, this study aimed to
investigate the role of three common VDR gene variants, namely FokI
(rs2228570), BsmI (rs1544410) and TaqI (rs731236), in PsV
susceptibility and clinical phenotype in a Caucasian Greek cohort
(Fig. 2).
Patients and methods
Study design, population and
settings
In this single-center, cross-sectional study,
unrelated adult subjects of Caucasian Greek origin (203 PsV cases
and 812 controls) were included. The cases were prospectively
enrolled from January 2019 to December 2022 at the psoriasis
outpatient unit of ‘A. Sygros’ Hospital (Athens, Greece) and met
the following inclusion criteria: i) Age ≥18 years; ii) confirmed
PsV diagnosis, with or without psoriatic arthritis (PsA); and iii)
Greek ancestry. Patients aged <18 years, those with non-plaque
psoriasis subtypes or non-Greek ancestry and affected first- to
third-degree blood relatives of enrolled participants were excluded
from the study. Controls comprised age (±5 years)-, sex- and
ethnicity-matched unrelated individuals from the general
population. The control group data were retrospectively obtained
from fully anonymized and de-identified datasets provided by New
Genomed LLC for research purposes, based on a collaboration
framework between New Genomed LLC and the National and Kapodistrian
University of Athens (Athens, Greece). The study protocol was
approved by the Institutional Review Board of ‘A. Sygros’ Hospital
(approval no. 2962/13-6-2018) and conducted in accordance with the
Helsinki Declaration. All participants provided written informed
consent for blood collection, genotyping and use of their genetic
and demographic data for research purposes, following the European
Medicines Agency guidelines (24).
Clinico-epidemiological
assessments
PsV was diagnosed clinically and/or histologically
by board-certified dermatologists. Predefined sociodemographic and
disease-related clinical data were collected through standardized
questionnaires. Disease severity was assessed based on previous
international consensus criteria (25): Patients with a body surface area
(BSA) <10 and/or no affected special location (scalp, face,
palms/soles, nails or genitalia) who were managed exclusively with
topical agents were classified as mild; cases with BSA ≥10 and/or
special site involvement and/or a history of systemic treatment or
phototherapy were categorized as severe. Early-onset PsV was
defined as disease initiation before age 40 and familial psoriasis
was recorded when one or more first- to third-degree relatives were
affected. Data collected from control subjects included age, sex
and ethnicity.
Sample collection, DNA extraction and
genotyping
Peripheral blood (5 ml) was collected from PsV cases
into EDTA tubes. Genomic DNA was isolated using the PureLink™
Genomic DNA Mini Kit (Thermo Fisher Scientific, Inc.) according to
the manufacturer's protocol and stored at -20˚C until analysis.
Genotyping of the selected VDR SNPs, namely FokI (rs2228570), BsmI
(rs1544410) and TaqI (rs731236), was carried out by real-time PCR
on a LightCycler® 480 System (Roche Diagnostics GmbH)
using allele-specific simple probes (LightSNiP assays; TIB MOLBIOL
Syntheselabor GmbH), with all primers and probes supplied as part
of the commercial assay and used according to the manufacturer's
instructions, followed by melting-curve analysis. Genotype
determination was based on the manufacturer-defined melting-peak
profiles. Primer/probe sequence information is not disclosed by the
manufacturer.
Statistical analysis
Descriptive statistics are presented as frequencies
with percentages for categorical data and as means ± SD or medians
with interquartile range (IQR) for continuous variables after
assessment of normality by the Shapiro-Wilk test. Associations of
VDR variants with PsV susceptibility (PsV cases vs. controls) and
clinical variables (intra-patient comparisons) were evaluated using
logistic regression or χ2/Fisher's exact test, as
appropriate, to calculate odds ratios (ORs) with 95% CIs. All
association analyses were conducted under dominant, recessive,
overdominant and allelic genetic models, with the major allele as
the reference. The Benjamini-Hochberg false discovery rate (FDR)
correction was applied to adjust P-values for multiple testing at a
significance level of 5%. The Hardy-Weinberg equilibrium (HWE) for
each SNP was assessed among controls using the χ2 test,
with P>0.05 indicating no significant deviation. All analyses
were two-sided and performed using STATA/IC (version 16.1;
StataCorp, LLC).
Results
Sociodemographic and clinical
disease-specific data
A total of 1,015 unrelated Greek subjects [203
patients with PsV (63.6% male) and 812 controls (60% male);
case-control ratio 1:4] were included in the study. The median age
was 54 years (IQR: 44-64; range: 22-86) in the PsV group and 55
years (IQR: 45-65; range: 22-91) in the control group, with no
significant difference in age (P=0.310) or sex distribution
(P=0.395). Among PsV cases, the median age at PsV onset was 32
years (IQR: 20-44; range: 5-66) and 136 (67%) patients had
early-onset disease (<40 years). Severe PsV was observed in 156
(76.8%) cases. Special site involvement included the scalp in 115
(56.7%), nails in 85 (41.9%) and genitals in 55 (27.1%) patients,
while the Koebner phenomenon was present in 68 (33.5%). A family
history of psoriasis was reported in 112 (55.2%) patients.
Metabolic comorbidities and PsA were the most commonly associated
conditions (47.3 and 30.5%, respectively). Sociodemographic and
clinical disease-related data of the study group are summarized in
Table I.
 | Table IEpidemiological and disease-specific
clinical data of the study population. |
Table I
Epidemiological and disease-specific
clinical data of the study population.
|
Clinico-epidemiological data | PsV cases
(n=203) | Controls
(n=812) |
P-valuea |
|---|
| Sex, n (%) | | | 0.395 |
|
Male | 129 (63.6) | 487 (60.0) | |
|
Female | 74 (36.4) | 325 (40.0) | |
| Median age, years
(IQR; range) | 54 (44.0-64.0;
22-86) | 55 (45.0-65.0;
22-91) | 0.310 |
| Median BMI,
kg/m2 (IQR; range) | 28.6 (24.6-32.5;
18.4-49.4) | - | - |
|
Overweight/obese
(BMI ≥25), n (%) | 142 (70.0) | - | - |
|
Normal
weight (BMI, <25), n (%) | 61 (30.0) | - | - |
| Smoking status, n
(%) | | | |
|
Current | 98 (48.3) | - | - |
|
Former | 50 (24.6) | - | - |
|
Never | 55 (27.1) | - | - |
| Median age at PsV
onset, years (IQR; range) | 32 (20.0-44.0;
5-66) | - | - |
| Early-onset PsV
(<40 years), n (%) | 136 (67.0) | - | - |
| Median disease
duration, years (IQR; range) | 19 (10.0-30.0;
1-60) | - | - |
| Disease severity, n
(%) | | | |
|
Mild | 47 (23.2) | - | - |
|
Severe | 156 (76.8) | - | - |
| Special site
involvement, n (%) | | | |
|
Nails | 85 (41.9) | - | - |
|
Scalp | 115 (56.7) | - | - |
|
Genitals | 55 (27.1) | - | - |
| Koebner response
(yes), n (%) | 68 (33.5) | - | - |
| Psoriasis family
history (yes), n (%) | 112 (55.2) | - | - |
| Comorbidities
(yes), n (%) | 168 (82.8) | - | - |
|
Metabolic
diseaseb | 96 (47.3) | - | - |
|
PsA | 62 (30.5) | - | - |
|
Thyroid
disorder | 56 (27.6) | - | - |
| Current treatment
(yes), n (%) | 185 (91.1) | - | - |
|
Topical | 29 (15.7) | - | - |
|
Phototherapy | 4 (2.2) | - | - |
|
Systemic | 152 (82.1) | - | - |
Genotype and allele distributions of
VDR variants in PsV cases vs. controls
Genotype and allele frequency distributions of the
studied VDR SNPs in PsV cases and controls and their associations
with PsV susceptibility are presented in Tables II and III. Genotype frequencies of all VDR
variants were in HWE among controls (FokI, P=0.743; BsmI, P=0.206;
TaqI, P=0.400).
| Table IIGenotype and allele frequency
distribution of the VDR SNPs in PsV cases and controls. |
Table II
Genotype and allele frequency
distribution of the VDR SNPs in PsV cases and controls.
| A, FokI
(rs2228570) |
|---|
|
Genotype/allele | PsV cases (n=203),
n (%) | Controls (n=812), n
(%) |
|---|
| CC | 96 (47.29) | 380 (46.80) |
| TC | 83 (40.89) | 348 (42.86) |
| TT | 24 (11.82) | 84 (10.34) |
| C | 275 (67.73) | 1,108 (68.23) |
| T | 131 (32.27) | 516 (31.77) |
| HWE P-value | - | 0.743 |
| B, BsmI
(rs1544410) |
|
Genotype/allele | PsV cases (n=203),
n (%) | Controls (n=812), n
(%) |
| GG | 62 (30.54) | 214 (26.36) |
| GA | 107 (52.71) | 388 (47.78) |
| AA | 34 (16.75) | 210 (25.86) |
| G | 231 (56.90) | 816 (50.25) |
| A | 175 (43.10) | 808 (49.75) |
| HWE P-value | - | 0.206 |
| C, TaqI
(rs731236) |
|
Genotype/allele | PsV cases (n=203),
n (%) | Controls (n=812), n
(%) |
| TT | 65 (32.02) | 252 (31.03) |
| CT | 88 (43.35) | 390 (48.03) |
| CC | 50 (24.63) | 170 (20.94) |
| T | 218 (53.69) | 894 (55.05) |
| C | 188 (46.31) | 730 (44.95) |
| HWE P-value | - | 0.400 |
| Table IIIGenetic model analysis of the VDR
SNPs in PsV cases and controls. |
Table III
Genetic model analysis of the VDR
SNPs in PsV cases and controls.
| A, FokI
(rs2228570) |
|---|
| Genetic model | OR (95% CI) | P-value | Adjusted
P-value |
|---|
| Dominant TT + TC
vs. CC | 0.980
(0.720-1.334) | 0.900 | 0.900 |
| Recessive TT vs. TC
+ CC | 1.162
(0.717-1.882) | 0.542 | 0.900 |
| Overdominant TC vs.
TT + CC | 0.922
(0.675-1.260) | 0.611 | 0.900 |
| Allelic T vs.
C | 1.023
(0.810-1.291) | 0.849 | 0.900 |
| B, BsmI
(rs1544410) |
| Genetic model | OR (95% CI) | P-value | Adjusted
P-value |
| Dominant AA + GA
vs. GG | 0.814
(0.581-1.140) | 0.231 | 0.231 |
| Recessive AA vs. GA
+ GG | 0.577
(0.386-0.861) | 0.007 | 0.028 |
| Overdominant GA vs.
GG + AA | 1.218
(0.895-1.657) | 0.210 | 0.231 |
| Allelic A vs.
G | 0.765
(0.614-0.953) | 0.016 | 0.032 |
| C, TaqI
(rs731236) |
| Genetic model | OR (95% CI) | P-value | Adjusted
P-value |
| Dominant CC + CT
vs. TT | 0.955
(0.687-1.329) | 0.786 | 0.786 |
| Recessive CC vs. CT
+ TT | 1.234
(0.860-1.771) | 0.254 | 0.508 |
| Overdominant CT vs.
TT + CC | 0.828
(0.607-1.129) | 0.233 | 0.508 |
| Allelic C vs.
T | 1.056
(0.849-1.314) | 0.624 | 0.786 |
After FDR correction, the BsmI variant remained
significantly associated with PsV susceptibility in both the
recessive (AA vs. GA + GG; OR: 0.577; 95% CI: 0.386-0.861; P=0.007;
adjusted P=0.028) and allelic (A vs. G; OR: 0.765; 95% CI:
0.614-0.953; P=0.016; adjusted P=0.032) models. The AA genotype and
A allele of BsmI were less common in PsV cases compared with
controls (16.8 vs. 25.9% and 43.1 vs. 49.8%, respectively),
suggesting a protective effect against PsV. No significant
differences were found between PsV cases and controls for the FokI
and TaqI variants in any of the models studied, indicating no
association with PsV susceptibility in this cohort.
Subgroup analysis based on
disease-specific clinical features
Among PsV cases, intra-patient subgroup analyses
revealed significant associations with disease-related clinical
traits. In comparisons between early- and late-onset PsV cases
(<40 vs. ≥40 years), the FokI variant was significantly
associated with age at disease onset in both the dominant (TT + TC
vs. CC; OR: 2.551; 95% CI: 1.396-4.660; P=0.002; adjusted P=0.036)
and allelic (T vs. C; OR: 2.172; 95% CI: 1.346-3.507; P=0.001;
adjusted P=0.022) models, suggesting that presence of the T allele
may predispose to earlier onset of PsV (Tables IV and V). Regarding special-site involvement,
both BsmI and TaqI exhibited significant associations with nail
psoriasis, as shown in Tables VI
and VII. BsmI was associated
with psoriatic onychia in the dominant (AA + GA vs. GG; OR: 2.755;
95% CI: 1.427-5.319; P=0.003; adjusted P=0.040) and allelic (A vs.
G; OR: 1.999; 95% CI: 1.337-2.986; P=0.001; adjusted P=0.022)
models, indicating that presence of the A allele may increase the
risk of nail involvement. Similarly, TaqI C allele presence was
associated with nail disease under both the dominant (CC + CT vs.
TT; OR: 3.063; 95% CI: 1.590-5.899; P=0.001; adjusted P=0.022) and
allelic (C vs. T; OR: 1.948; 95% CI: 1.305-2.907; P=0.001; adjusted
P=0.022) models.
| Table IVGenotype and allele frequency
distribution of the VDR SNPs in early- and late-onset PsV
cases. |
Table IV
Genotype and allele frequency
distribution of the VDR SNPs in early- and late-onset PsV
cases.
| A, FokI
(rs2228570) |
|---|
|
Genotype/allele | Early PsV <40
years (n=136), n (%) | Late PsV ≥40 years
(n=67), n (%) |
|---|
| CC | 54 (39.71) | 42 (62.69) |
| TC | 62 (45.59) | 21 (31.34) |
| TT | 20 (14.70) | 4 (5.97) |
| C | 170 (62.50) | 105 (78.36) |
| T | 102 (37.50) | 29 (21.64) |
| B, BsmI
(rs1544410) |
|
Genotype/allele | Early PsV <40
years (n=136), n (%) | Late PsV ≥40 years
(n=67), n (%) |
| GG | 43 (31.62) | 19 (28.36) |
| GA | 74 (54.41) | 33 (49.25) |
| AA | 19 (13.97) | 15 (22.39) |
| G | 160 (58.82) | 71 (52.99) |
| A | 112 (41.18) | 63 (47.01) |
| C, TaqI
(rs731236) |
|
Genotype/allele | Early PsV <40
years (n=136), n (%) | Late PsV ≥40 years
(n=67), n (%) |
| TT | 46 (33.82) | 19 (28.36) |
| CT | 60 (44.12) | 28 (41.79) |
| CC | 30 (22.06) | 20 (29.85) |
| T | 152 (55.88) | 66 (49.25) |
| C | 120 (44.12) | 68 (50.75) |
| Table VGenetic model analysis of the VDR
SNPs in early- and late-onset PsV cases. |
Table V
Genetic model analysis of the VDR
SNPs in early- and late-onset PsV cases.
| A, FokI
(rs2228570) |
|---|
| Genetic model | OR (95% CI) | P-value | Adjusted
P-value |
|---|
| Dominant TT + TC
vs. CC | 2.551
(1.396-4.660) | 0.002 | 0.036 |
| Recessive TT vs. TC
+ CC | 2.716
(0.889-8.293) | 0.079 | 0.404 |
| Overdominant TC vs.
TT + CC | 1.835
(0.991-3.400) | 0.054 | 0.364 |
| Allelic T vs.
C | 2.172
(1.346-3.507) | 0.001 | 0.022 |
| B, BsmI
(rs1544410) |
| Genetic model | OR (95% CI) | P-value | Adjusted
P-value |
| Dominant AA + GA
vs. GG | 0.856
(0.450-1.628) | 0.636 | 0.830 |
| Recessive AA vs. GA
+ GG | 0.563
(0.265-1.194) | 0.134 | 0.499 |
| Overdominant GA vs.
GG + AA | 1.230
(0.684-2.209) | 0.489 | 0.734 |
| Allelic A vs.
G | 0.789
(0.509-1.223) | 0.264 | 0.641 |
| C, TaqI
(rs731236) |
| Genetic model | OR (95% CI) | P-value | Adjusted
P-value |
| Dominant CC + CT
vs. TT | 0.774
(0.409-1.467) | 0.433 | 0.718 |
| Recessive CC vs. CT
+ TT | 0.665
(0.343-1.289) | 0.227 | 0.641 |
| Overdominant CT vs.
TT + CC | 1.100
(0.608-1.987) | 0.753 | 0.894 |
| Allelic C vs.
T | 0.766
(0.495-1.185) | 0.208 | 0.641 |
| Table VIGenotype and allele frequency
distribution of the VDR SNPs in PsV cases with and without nail
involvement. |
Table VI
Genotype and allele frequency
distribution of the VDR SNPs in PsV cases with and without nail
involvement.
| A, FokI
(rs2228570) |
|---|
|
Genotype/allele | With nail PsV
(n=85), n (%) | Without nail PsV
(n=118), n (%) |
|---|
| CC | 36 (42.35) | 60 (50.85) |
| TC | 38 (44.71) | 45 (38.14) |
| TT | 11 (12.94) | 13 (11.01) |
| C | 110 (64.71) | 165 (69.92) |
| T | 60 (35.29) | 71 (30.08) |
| B, BsmI
(rs1544410) |
|
Genotype/allele | With nail PsV
(n=85), n (%) | Without nail PsV
(n=118), n (%) |
| GG | 16 (18.82) | 46 (38.98) |
| GA | 48 (56.47) | 59 (50.00) |
| AA | 21 (24.71) | 13 (11.02) |
| G | 80 (47.06) | 151 (63.98) |
| A | 90 (52.94) | 85 (36.02) |
| C, TaqI
(rs731236) |
|
Genotype/allele | With nail PsV
(n=85), n (%) | Without nail PsV
(n=118), n (%) |
| TT | 16 (18.82) | 49 (41.52) |
| CT | 43 (50.59) | 45 (38.14) |
| CC | 26 (30.59) | 24 (20.34) |
| T | 75 (44.12) | 143 (60.59) |
| C | 95 (55.88) | 93 (39.41) |
| Table VIIGenetic model analysis of the VDR
SNPs in PsV cases with and without nail involvement. |
Table VII
Genetic model analysis of the VDR
SNPs in PsV cases with and without nail involvement.
| A, FokI
(rs2228570) |
|---|
| Genetic model | OR (95% CI) | P-value | Adjusted
P-value |
|---|
| Dominant TT + TC
vs. CC | 1.408
(0.803-2.469) | 0.232 | 0.641 |
| Recessive TT vs. TC
+ CC | 1.200
(0.510-2.824) | 0.676 | 0.859 |
| Overdominant TC vs.
TT + CC | 1.312
(0.744-2.311) | 0.348 | 0.659 |
| Allelic T vs.
C | 1.268
(0.833-1.929) | 0.268 | 0.641 |
| B, BsmI
(rs1544410) |
| Genetic model | OR (95% CI) | P-value | Adjusted
P-value |
| Dominant AA + GA
vs. GG | 2.755
(1.427-5.319) | 0.003 | 0.040 |
| Recessive AA vs. GA
+ GG | 2.650
(1.242-5.657) | 0.012 | 0.108 |
| Overdominant GA vs.
GG + AA | 1.297
(0.741-2.272) | 0.363 | 0.676 |
| Allelic A vs.
G | 1.999
(1.337-2.986) | 0.001 | 0.022 |
| C, TaqI
(rs731236) |
| Genetic model | OR (95% CI) | P-value | Adjusted
P-value |
| Dominant CC + CT
vs. TT | 3.063
(1.590-5.899) | 0.001 | 0.022 |
| Recessive CC vs. CT
+ TT | 1.725
(0.907-3.280) | 0.096 | 0.432 |
| Overdominant CT vs.
TT + CC | 1.661
(0.944-2.921) | 0.078 | 0.404 |
| Allelic C vs.
T | 1.948
(1.305-2.907) | 0.001 | 0.022 |
In comparisons based on comorbid PsA, the TaqI
variant exhibited a significant association under the allelic model
(C vs. T; OR: 0.477; 95% CI: 0.308-0.741; P=0.001; adjusted
P=0.022), suggesting that carriers of the C allele (CC/CT) may be
less likely to develop PsA (Table
VIII and IX).
| Table VIIIGenotype and allele frequency
distribution of the VDR SNPs in PsV cases with and without
psoriatic arthritis. |
Table VIII
Genotype and allele frequency
distribution of the VDR SNPs in PsV cases with and without
psoriatic arthritis.
| A, FokI
(rs2228570) |
|---|
|
Genotype/allele | With PsA (n=62), n
(%) | Without PsA
(n=141), n (%) |
|---|
| CC | 30 (48.39) | 66 (46.81) |
| TC | 27 (43.55) | 56 (39.72) |
| TT | 5 (8.06) | 19 (13.47) |
| C | 87 (70.16) | 188 (66.67) |
| T | 37 (29.84) | 94 (33.33) |
| B, BsmI
(rs1544410) |
|
Genotype/allele | With PsA (n=62), n
(%) | Without PsA
(n=141), n (%) |
| GG | 25 (40.32) | 37 (26.24) |
| GA | 27 (43.55) | 80 (56.74) |
| AA | 10 (16.13) | 24 (17.02) |
| G | 77 (62.10) | 154 (54.61) |
| A | 47 (37.90) | 128 (45.39) |
| C, TaqI
(rs731236) |
|
Genotype/allele | With PsA (n=62), n
(%) | Without PsA
(n=141), n (%) |
| TT | 28 (45.16) | 37 (26.24) |
| CT | 26 (41.94) | 62 (43.97) |
| CC | 8 (12.90) | 42 (29.79) |
| T | 82 (66.13) | 136 (48.23) |
| C | 42 (33.87) | 146 (51.77) |
| Table IXGenetic model analysis of the VDR
SNPs in PsV cases with and without psoriatic arthritis. |
Table IX
Genetic model analysis of the VDR
SNPs in PsV cases with and without psoriatic arthritis.
| A, FokI
(rs2228570) |
|---|
| Genetic model | OR (95% CI) | P-value | Adjusted
P-value |
|---|
| Dominant TT + TC
vs. CC | 0.939
(0.516-1.707) | 0.836 | 0.921 |
| Recessive TT vs. TC
+ CC | 0.563
(0.200-1.586) | 0.277 | 0.641 |
| Overdominant TC vs.
TT + CC | 1.171
(0.640-2.146) | 0.609 | 0.822 |
| Allelic T vs.
C | 0.851
(0.538-1.344) | 0.488 | 0.734 |
| B, BsmI
(rs1544410) |
| Genetic model | OR (95% CI) | P-value | Adjusted
P-value |
| Dominant AA + GA
vs. GG | 0.527
(0.280-0.990) | 0.046 | 0.355 |
| Recessive AA vs. GA
+ GG | 0.938
(0.418-2.101) | 0.875 | 0.921 |
| Overdominant GA vs.
GG + AA | 0.588
(0.322-1.074) | 0.084 | 0.404 |
| Allelic A vs.
G | 0.734
(0.465-1.155) | 0.161 | 0.561 |
| C, TaqI
(rs731236) |
| Genetic model | OR (95% CI) | P-value | Adjusted
P-value |
| Dominant CC + CT
vs. TT | 0.432
(0.231-0.807) | 0.009 | 0.108 |
| Recessive CC vs. CT
+ TT | 0.349
(0.153-0.797) | 0.012 | 0.108 |
| Overdominant CT vs.
TT + CC | 0.920
(0.503-1.683) | 0.787 | 0.914 |
| Allelic C vs.
T | 0.477
(0.308-0.741) | 0.001 | 0.022 |
In analyses stratified by family history of
psoriasis, the recessive model of FokI (TT vs. TC + CC; OR: 6.769;
95% CI: 1.950-23.503; P=0.003; adjusted P=0.040) was significantly
associated with familial disease, indicating that the TT genotype
may contribute to familial clustering of psoriasis (Tables X and XI).
| Table XGenotype and allele frequency
distribution of the VDR SNPs in PsV cases with and without
psoriasis family history. |
Table X
Genotype and allele frequency
distribution of the VDR SNPs in PsV cases with and without
psoriasis family history.
| A, FokI
(rs2228570) |
|---|
|
Genotype/allele | With psoriasis FH
(n=112), n (%) | Without psoriasis
FH (n=91), n (%) |
|---|
| CC | 49 (43.75) | 47 (51.65) |
| TC | 42 (37.50) | 41 (45.05) |
| TT | 21 (18.75) | 3 (3.30) |
| C | 140 (62.50) | 135 (74.18) |
| T | 84 (37.50) | 47 (25.82) |
| B, BsmI
(rs1544410) |
|
Genotype/allele | With psoriasis FH
(n=112), n (%) | Without psoriasis
FH (n=91), n (%) |
| GG | 38 (33.92) | 24 (26.37) |
| GA | 58 (51.79) | 49 (53.85) |
| AA | 16 (14.29) | 18 (19.78) |
| G | 134 (59.82) | 97 (53.30) |
| A | 90 (40.18) | 85 (46.70) |
| C, TaqI
(rs731236) |
|
Genotype/allele | With psoriasis FH
(n=112), n (%) | Without psoriasis
FH (n=91), n (%) |
| TT | 40 (35.71) | 25 (27.48) |
| CT | 45 (40.18) | 43 (47.25) |
| CC | 27 (24.11) | 23 (25.27) |
| T | 125 (55.80) | 93 (51.10) |
| C | 99 (44.20) | 89 (48.90) |
| Table XIGenetic model analysis of the VDR
SNPs in PsV cases with and without psoriasis family history. |
Table XI
Genetic model analysis of the VDR
SNPs in PsV cases with and without psoriasis family history.
| A, FokI
(rs2228570) |
|---|
| Genetic model | OR (95% CI) | P-value | Adjusted
P-value |
|---|
| Dominant TT + TC
vs. CC | 1.373
(0.788-2.393) | 0.263 | 0.641 |
| Recessive TT vs. TC
+ CC | 6.769
(1.950-23.503) | 0.003 | 0.040 |
| Overdominant TC vs.
TT + CC | 0.731
(0.417-1.285) | 0.277 | 0.641 |
| Allelic T vs.
C | 1.723
(1.123-2.645) | 0.012 | 0.108 |
| B, BsmI
(rs1544410) |
| Genetic model | OR (95% CI) | P-value | Adjusted
P-value |
| Dominant AA + GA
vs. GG | 0.698
(0.380-1.282) | 0.246 | 0.641 |
| Recessive AA vs. GA
+ GG | 0.676
(0.323-1.415) | 0.299 | 0.659 |
| Overdominant GA vs.
GG + AA | 0.921
(0.529-1.603) | 0.770 | 0.904 |
| Allelic A vs.
G | 0.766
(0.506-1.160) | 0.187 | 0.631 |
| C, TaqI
(rs731236) |
| Genetic model | OR (95% CI) | P-value | Adjusted
P-value |
| Dominant CC + CT
vs. TT | 0.682
(0.374-1.244) | 0.212 | 0.641 |
| Recessive CC vs. CT
+ TT | 0.939
(0.495-1.783) | 0.848 | 0.921 |
| Overdominant CT vs.
TT + CC | 0.750
(0.429-1.311) | 0.312 | 0.659 |
| Allelic C vs.
T | 0.828
(0.548-1.249) | 0.344 | 0.659 |
The studied VDR SNPs showed no evidence of
association with other clinico-epidemiological parameters,
including BMI, disease severity, scalp or genital involvement and
the Koebner phenomenon, in this cohort (all P>0.05; Tables SI, SII, SIII, SIV, SV, SVI, SVII and SVIII). A graphical abstract summarizing
the study design and main findings is provided in Fig. 2.
Discussion
In this study, the role of three common VDR variants
(FokI, BsmI and TaqI) in PsV susceptibility and clinical phenotype
was evaluated in a Caucasian Greek cohort. The case-control
analysis supported an association between BsmI and PsV
susceptibility in the recessive and allelic models, whereas no
associations were observed for FokI or TaqI. Subgroup comparisons
further indicated associations with major disease-related clinical
traits, including age at onset, nail or joint involvement and
familial clustering.
For BsmI, carriers of the AA genotype exhibited a
42.3% reduced risk of PsV compared with G-allele carriers (GA/GG).
The allelic model further supported this pattern, demonstrating a
protective effect of the A allele against PsV. The BsmI variant has
already been associated with psoriasis, but findings vary by
ethnicity (21,23,26,27).
The present results align with case-control studies and
meta-analyses indicating a protective role of the A allele and/or
AA genotype in Caucasian and Asian populations (21,23,27).
In this context, a Japanese study reported increased PsV risk for
the GG genotype, while the A allele and AA genotype appeared
protective (27). Two
meta-analyses supported this trend, demonstrating an inverse
association between the A allele and PsV risk in overall
populations, although significance was lost after correction and in
Asian populations, despite undefined psoriasis subtypes and
precluded intra-European evaluation (21,23).
However, additional studies have found no association or even
opposite effects (15,22,28).
In this context, the present data suggest that among
the studied VDR variants, BsmI may represent a PsV
susceptibility-related marker in the Greek population. From a
biological perspective, this 3' non-coding variant may be
associated with regulation of VDR expression (i.e., via altered
mRNA stability and/or LD with functional polymorphisms), rather
than receptor structural changes (16-19).
Altered VDR expression may, in turn, affect VitD/VDR-mediated
signaling relevant to PsV pathogenesis, given the roles of VitD in
key processes involved in psoriatic inflammation, including
keratinocyte proliferation/differentiation, epidermal barrier
function and immune responses (5-9).
However, further research is needed to determine whether rs1544410
itself has regulatory effects or reflects other functional
variants, particularly given population and/or ethnic differences
in LD architecture (18).
Both FokI and TaqI showed no impact on PsV
susceptibility in the present cohort. Although findings vary among
populations (15,21-23,28),
a number of studies in Caucasian, Asian and North African
(Egyptian) groups have similarly reported no association between
these variants and PsV risk (21,29-34).
Divergent results across studies may reflect differences in ethnic
or population genetic backgrounds, including LD structure, as well
as in epigenetic variation, environmental exposures or
methodological factors such as study design, sample size or
psoriasis subtype composition (18).
Intra-patient analyses indicated additional
phenotype-specific associations. Among PsV cases, FokI appeared to
be associated with age at disease onset under the dominant and
allelic models. In the dominant model (TT + TC vs. CC), T-allele
carriers (TT/TC) exhibited a nearly 2.6-fold increased risk of
early-onset PsV (<40 years). This was further supported by the
allelic model (T vs. C), indicating that the FokI T allele may
predispose to earlier disease onset. Although age-at-onset effects
of VDR SNPs have been explored (33-42),
only one study has shown an association between the BsmI GG
genotype and early-onset disease (<40 years) in a Caucasian
(Turkish) cohort of mixed psoriasis subtypes (n=102) (37).
FokI was also associated with familial psoriasis
under the recessive model (TT vs. TC + CC). Patients with PsV
carrying the TT genotype were nearly 6.8 times more likely to
report an affected first- to third-degree relative compared with
C-allele carriers (TC/CC), suggesting that FokI may play a role in
heritable patterns of psoriasis. Although not directly comparable,
a study in a Caucasian (British) PsV cohort (n=205) found that the
FokI C allele combined with a promoter variant reduced the risk of
non-familial (sporadic) psoriasis (34). Since that effect was
haplotype-dependent, the present finding may represent one of the
first single-variant indications that FokI itself could contribute
to familial clustering of psoriasis.
Notably, the FokI TT genotype in this cohort seemed
to be associated with both early-onset PsV and familial disease,
features that frequently co-occur clinically, as early-onset
psoriasis tends to cluster in families (43). Mechanistically, FokI (T-to-C
substitution) alters the translation initiation site (ATG to ACG),
resulting in a longer, less active VDR isoform in T allele carriers
(16-19),
which may impair downstream VitD/VDR-mediated effects on skin
homeostasis and immune responses. Thus, compromised VitD/VDR
signaling in TT homozygotes may reflect a genetic overlap,
potentially involving FokI, which could contribute to both familial
aggregation and early disease onset. This aligns with the known
clinical tendency of early-onset PsV to cluster in families
(43), but requires further
validation.
Significant associations were also observed for nail
psoriasis with both BsmI and TaqI under the dominant and allelic
models. In the dominant model, carriers of the BsmI A allele
(AA/GA) and the TaqI C allele (CC/CT) exhibited a ~2.8- and
~3.1-fold increased risk of nail involvement, respectively. The
allelic models also indicated higher risk of nail disease for both
the BsmI A and TaqI C alleles. This contrasts with an Asian
(Korean) PsV cohort (n=104) in which neither variant was associated
with nail psoriasis (40).
TaqI was further associated with PsA comorbidity
under the allelic model (C vs. T), indicating that the C allele may
protect against joint disease in this cohort. Although relevant
data are limited (40,44,45),
a Caucasian (Turkish) study (n=51) has similarly shown an
association between the TaqI T allele and increased PsA risk
(44). These findings suggest that
TaqI may influence extra-cutaneous manifestations of PsV,
modulating the overall disease burden beyond the skin.
Of note, while the BsmI A allele seemed to be
protective in the present case-control setting, it was associated
with nail involvement among PsV cases. This pattern may indicate
phenotype-modifying effects after disease onset. Although the
functional impact of VDR variants on VitD signaling remains
unclear, both BsmI and TaqI may exert tissue- and/or cell-specific
regulatory effects on VDR expression (18,19),
potentially influencing phenotype-specific inflammatory cascades
involved in nail psoriasis. In addition, as the TaqI C allele
creates a CpG site prone to DNA methylation (17,19,20),
the present findings suggest that, in addition to genetic
variation, epigenetic modifications at this locus may underlie
tissue-specific inflammation, with possible implications for both
nail and joint disease.
Furthermore, the TaqI C allele in this cohort was
associated with both psoriatic onychia and arthritis, two
clinically related features, but with inverse effect patterns.
While nail involvement often predicts increased arthritis risk
(1,46), the C allele appeared to be
protective against PsA while predisposing to nail disease. These
divergent effects within the nail-joint axis may arise from
distinct genetic and/or epigenetic drivers, including differences
in the genetic architecture of cutaneous vs. joint disease
(1,47) and in allele-dependent TaqI
methylation (17,19,20),
potentially resulting in tissue-specific VitD/VDR signaling. As
methylation status varies by ethnicity, disease state or tissue
type (17,19,48),
TaqI may exert phenotype-specific effects driven by
context-dependent epigenetic regulation. This warrants further
investigation within the nail-joint spectrum of psoriatic
disease.
Key strengths of the present study include the focus
on a single ethnic group (Greek subjects) and a specific psoriasis
subtype (PsV), reducing genetic and phenotypic heterogeneity. The
relatively large control group (n=812; 1:4 case-control ratio) is
also an advantage compared with commonly used 1:1 or 1:2 designs in
genetic association studies (15,22,23,28).
In addition, the inclusion of several clinical traits, beyond
case-control comparisons, provides insights into whether VDR
variation may contribute to PsV phenotype. The FDR correction for
multiple testing further improves the reliability of the
results.
However, certain limitations require consideration.
First, the PsV sample (n=203) is relatively modest for detecting
subtle effects. Second, although the single-center, ethnically and
clinically uniform design enhances internal validity, it may limit
the generalizability of the present findings to other psoriasis
subtypes or populations with different genetic, epigenetic or
environmental backgrounds. In addition, while cases and controls
were matched on age, sex and ethnicity, the population controls
lacked detailed clinical and exposure data, preventing detection of
psoriasis status or potential confounders. However, given the
national psoriasis prevalence in Greece (~2.2%) (2,49),
the expected number of psoriasis cases among 812 controls is low,
reducing, but not eliminating, the risk of misclassification.
Furthermore, only three VDR SNPs were analyzed, without
investigating rare variants or haplotypes. Finally, VitD-related
confounders (VitD serum levels, dietary or supplemental intake, sun
exposure), which could influence VDR activity, were not
assessed.
While VDR has not emerged as a psoriasis
susceptibility locus in genome-wide association studies (GWAS)
(3), several lines of evidence
still support its biological relevance, including the role of the
VitD/VDR axis in key psoriatic components, altered VDR expression
in psoriatic skin, the widespread use of topical VitD analogs in
psoriasis treatment, variable but suggestive associations for FokI,
BsmI and TaqI in prior studies and the potential epigenetic
regulation at the TaqI CpG site (5-9,15-17,19-23).
Emerging data also indicate additional cutaneous VitD-related
bioactive metabolites, some with alternative receptor targets,
underscoring the broader secosteroid network in the skin (10). By design, GWAS, which apply
stringent significance thresholds and often treat psoriasis as a
single trait across diverse clinical and ethnic backgrounds, could
miss variants with small-to-moderate or indirect effects influenced
by LD patterns and/or ethnic-, disease subtype- or
epigenetic-related factors (19,50,51).
Thus, the associations observed in the present genetically and
clinically uniform cohort could reflect ethnic- and/or
phenotype-specific VDR effects that may be too weak to be captured
in GWAS (19).
In conclusion, to the best of our knowledge, this
was the first study to explore VDR FokI (rs2228570), BsmI
(rs1544410) and TaqI (rs731236) variants in association with PsV in
a Greek population. The present results showed that BsmI may
contribute to disease susceptibility, while all three polymorphisms
may influence major clinical traits, including age at onset, nail
or joint involvement and familial clustering of PsV.
Although the functional consequences of these
variants are not fully elucidated, VDR genetic variation and
epigenetic modification may alter receptor activity or expression
levels, potentially modulating key processes disrupted in
psoriasis. In this regard, the present findings suggest that common
VDR variants may exert small, context-dependent effects that could
play a role in PsV initiation and phenotypic expression. Thus, the
VDR locus may represent a potential biomarker for personalized risk
stratification and clinical profiling in PsV. Further prospective
studies in larger Caucasian cohorts, integrating both genotypic and
phenotypic data, are needed to validate these findings and further
elucidate the complex genetic basis of PsV, particularly its links
to VitD/VDR signaling and its potential clinical implications.
Supplementary Material
Genotype and allele frequency
distribution of the VDR SNPs in PsV cases stratified by BMI
status.
Genetic model analysis of the VDR SNPs
in PsV cases stratified by BMI status.
Genotype and allele frequency
distribution of the VDR SNPs in mild and severe PsV cases.
Genetic model analysis of the VDR SNPs
in mild and severe PsV cases.
Genotype and allele frequency
distribution of the VDR SNPs in PsV cases with and without scalp
involvement.
Genetic model analysis of the VDR SNPs
in PsV cases with and without scalp involvement.
Genotype and allele frequency
distribution of the VDR SNPs in PsV cases with and without genital
involvement.
Genetic model analysis of the VDR SNPs
in PsV cases with and without genital involvement.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
ND and EN conceived and designed the study. PS and
NR contributed to clinical and laboratory data collection. MK
designed the experiments and AT, MP and PS performed the laboratory
analyses. AF supervised the statistical analyses and contributed to
statistical interpretation. PS conducted the literature review,
prepared the figures and tables and wrote the initial draft of the
manuscript. PS, MK, MP, NR, IS, AJS and DAS contributed to data
interpretation and critically revised the manuscript. PS finalized
the manuscript under the supervision of ND and EN. PS, MK and ND
confirm the authenticity of all the raw data. All authors reviewed
and approved the final manuscript.
Ethics approval and consent to
participate
The present study was conducted in accordance with
the ethical standards of the Institutional Review Board of ‘A.
Sygros’ Hospital (approval no. 2962/13-6-2018) and the Helsinki
Declaration. Written informed consent was obtained from all
participants prior to enrollment.
Patient consent for publication
Written informed consent for publication of
anonymized, de-identified clinical and genetic data was obtained
from all participants.
Competing interests
DAS is the Editor-in-Chief of the journal but had no
personal involvement in the reviewing process or any influence in
terms of adjudicating on the final decision, for the present
article. The other authors declare that they have no competing
interests.
References
|
1
|
Griffiths CEM, Armstrong AW, Gudjonsson JE
and Barker JNWN: Psoriasis. Lancet. 397:1301–1315. 2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Damiani G, Bragazzi NL, Karimkhani Aksut
C, Wu D, Alicandro G, McGonagle D, Guo C, Dellavalle R, Grada A,
Wong P, et al: The global, regional, and national burden of
psoriasis: Results and insights from the global burden of disease
2019 study. Front Med (Lausanne). 8(743180)2021.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Zhang M, Su W, Deng J, Zhai B, Zhu G, Gao
R, Zeng Q, Qiu J, Bian Z, Xiao H, et al: Multi-ancestry genome-wide
meta-analysis with 472,819 individuals identifies 32 novel risk
loci for psoriasis. J Transl Med. 23(133)2025.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Singh S, Pradhan D, Puri P, Ramesh V,
Aggarwal S, Nayek A and Jain AK: Genomic alterations driving
psoriasis pathogenesis. Gene. 683:61–71. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Brożyna AA, Slominski RM, Nedoszytko B,
Zmijewski MA and Slominski AT: Vitamin D signaling in psoriasis:
Pathogenesis and therapy. Int J Mol Sci. 23(8575)2022.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Gisondi P, Gracia-Cazaña T, Kurzen H and
Galván J: Calcipotriol/Betamethasone dipropionate for the treatment
of psoriasis: Mechanism of action and evidence of efficacy and
safety versus topical corticosteroids. J Clin Med.
13(4484)2024.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Visconti B, Paolino G, Carotti S,
Pendolino AL, Morini S, Richetta AG and Calvieri S:
Immunohistochemical expression of VDR is associated with reduced
integrity of tight junction complex in psoriatic skin. J Eur Acad
Dermatol Venereol. 29:2038–2042. 2015.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Liang W, Lin Z, Zhang L, Qin X, Zhang Y
and Sun L: Calcipotriol inhibits proliferation of human
keratinocytes by downregulating STAT1 and STAT3 signaling. J
Investig Med. 65:376–381. 2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Cao M, Mei L, Xiao M, Li J and Fang F:
Calcipotriol inhibits psoriasis-like angiogenic features in
K14-VEGF transgenic mice. Eur J Dermatol. 32:24–33. 2022.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Slominski AT, Kim TK, Janjetovic Z,
Slominski RM, Li W, Jetten AM, Indra AK, Mason RS and Tuckey RC:
Biological Effects of CYP11A1-Derived Vitamin D and Lumisterol
Metabolites in the Skin. J Invest Dermatol. 144:2145–2161.
2024.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Zhang Y, Jing D, Zhou G, Xiao Y, Shen M,
Chen X and Liu H: Evidence of a causal relationship between vitamin
D status and risk of psoriasis from the UK Biobank study. Front
Nutr. 9(807344)2022.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Lee YH and Song GG: Association between
circulating 25-hydroxyvitamin D levels and psoriasis, and
correlation with disease severity: A meta-analysis. Clin Exp
Dermatol. 43:529–535. 2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Elmelid A, Siekkeri Vandikas M, Gillstedt
M, Osmancevic A and Alsterholm M: The effect of narrow-band
ultraviolet B phototherapy on free and total vitamin D serum levels
in mild to severe plaque psoriasis. Biomolecules.
13(1018)2023.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Elgarhy LH, Eltatawy RA, Rizk O and Ismail
M: Vitamin D receptor expression in chronic plaque psoriasis before
and after narrowband ultraviolet B phototherapy. J Cutan Aesthet
Surg. 16:128–133. 2023.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Lee YH: Vitamin D receptor ApaI, TaqI,
BsmI, and FokI polymorphisms and psoriasis susceptibility: An
updated meta-analysis. Clin Exp Dermatol. 44:498–505.
2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Agliardi C, Guerini FR, Bolognesi E,
Zanzottera M and Clerici M: VDR gene single nucleotide
polymorphisms and autoimmunity: A narrative review. Biology
(Basel). 12(916)2023.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Poon AH, Gong L, Brasch-Andersen C,
Litonjua AA, Raby BA, Hamid Q, Laprise C, Weiss ST, Altman RB and
Klein TE: Very important pharmacogene summary for VDR.
Pharmacogenet Genomics. 22:758–763. 2012.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Uitterlinden AG, Fang Y, Van Meurs JB,
Pols HA and Van Leeuwen JP: Genetics and biology of vitamin D
receptor polymorphisms. Gene. 338:143–156. 2004.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Saccone D, Asani F and Bornman L:
Regulation of the vitamin D receptor gene by environment, genetics
and epigenetics. Gene. 561:171–180. 2015.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Andraos C, Koorsen G, Knight JC and
Bornman L: Vitamin D receptor gene methylation is associated with
ethnicity, tuberculosis, and TaqI polymorphism. Hum Immunol.
72:262–268. 2011.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Stefanic M, Rucevic I and Barisic-Drusko
V: Meta-analysis of vitamin D receptor polymorphisms and psoriasis
risk. Int J Dermatol. 52:705–710. 2013.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Liu JL, Zhang SQ and Zeng HM: ApaI, BsmI,
FokI and TaqI polymorphisms in the vitamin D receptor (VDR) gene
and the risk of psoriasis: A meta-analysis. J Eur Acad Dermatol
Venereol. 27:739–746. 2013.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Lee YH, Choi SJ, Ji JD and Song GG:
Vitamin D receptor ApaI, TaqI, BsmI, and FokI polymorphisms and
psoriasis susceptibility: A meta-analysis. Mol Biol Rep.
39:6471–6478. 2012.PubMed/NCBI View Article : Google Scholar
|
|
24
|
European Medicines Agency: Position paper
on terminology in pharmacogenetics. EMEA/CPMP/3070/01. EMEA,
London, 2002. Available at: https://www.ema.europa.eu/en/documents/scientific-guideline/position-paper-terminology-pharmacogenetics_en.pdf.
|
|
25
|
Strober B, Ryan C, van de Kerkhof P, van
der Walt J, Kimball AB, Barker J and Blauvelt A: International
Psoriasis Council Board Members and Councilors. Recategorization of
psoriasis severity: Delphi consensus from the International
Psoriasis Council. J Am Acad Dermatol. 82:117–122. 2020.PubMed/NCBI View Article : Google Scholar
|
|
26
|
AbdElneam AI, Al-Dhubaibi MS, Bahaj SS and
Mohammed GF: The vitamin D receptor gene polymorphism rs1544410 T/T
genotype as a predictor of factor vitamin D thresholds deficiency
in patients with psoriasis vulgaris-A preliminary study. J Cosmet
Dermatol. 22:1642–1646. 2023.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Saeki H, Asano N, Tsunemi Y, Takekoshi T,
Kishimoto M, Mitsui H, Tada Y, Torii H, Komine M, Asahina A and
Tamaki K: Polymorphisms of vitamin D receptor gene in Japanese
patients with psoriasis vulgaris. J Dermatol Sci. 30:167–171.
2002.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Li J, Sun L, Sun J and Yan M: Pooling
analysis regarding the impact of human vitamin D receptor variants
on the odds of psoriasis. BMC Med Genet. 20(161)2019.PubMed/NCBI View Article : Google Scholar
|
|
29
|
A Anani HA, Khalifa WA, Althoqapy AA,
Maklad SS, Kamal H, Sabry D and Samir M: Frequency of genotypes and
allelic polymorphisms of vitamin D receptor in egyptian psoriatic
patients and their association with disease severity, immune
modulation of IL-22 levels and the response to topical calcipotriol
treatment: A case control study. Indian J Dermatol. 67:37–44.
2022.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Liu J, Wang W, Liu K, Wan D, Wu Z, Cao Z,
Luo Y, Xiao C and Yin M: Vitamin D receptor gene polymorphisms are
associated with psoriasis susceptibility and the clinical response
to calcipotriol in psoriatic patients. Exp Dermatol. 29:1186–1190.
2020.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Rucevic I, Stefanic M, Tokic S, Vuksic M,
Glavas-Obrovac L and Barisic-Drusko V: Lack of association of
vitamin D receptor gene 3'-haplotypes with psoriasis in Croatian
patients. J Dermatol. 39:58–62. 2012.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Polić MV, Rucević I, Barisić-Drusko V,
Miskulin M, Glavas-Obrovac L, Stefanić M, Karner I, Lipozencić J,
Bacun T and Mihaljević I: Polymorphisms of vitamin D receptor gene
in the population of eastern Croatia with psoriasis vulgaris and
diabetes mellitus. Coll Antropol. 36:451–457. 2012.PubMed/NCBI
|
|
33
|
Zuel-Fakkar NM, Kamel MM, Asaad MK, Mahran
MZ and Shehab AA: A study of ApaI and TaqI genotypes of the vitamin
D receptor in Egyptian patients with psoriasis. Clin Exp Dermatol.
36:355–359. 2011.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Halsall JA, Osborne JE, Pringle JH and
Hutchinson PE: Vitamin D receptor gene polymorphisms, particularly
the novel A-1012G promoter polymorphism, are associated with
vitamin D3 responsiveness and non-familial susceptibility in
psoriasis. Pharmacogenet Genomics. 15:349–355. 2005.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Richetta AG, Silvestri V, Giancristoforo
S, Rizzolo P, D'Epiro S, Graziano V, Mattozzi C, Navazio AS,
Campoli M, D'Amico C, et al: A-1012G promoter polymorphism of
vitamin D receptor gene is associated with psoriasis risk and lower
allele-specific expression. DNA Cell Biol. 33:102–109.
2014.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Zhou X, Xu LD and Li YZ: The association
of polymorphisms of the vitamin D receptor gene with psoriasis in
the Han population of northeastern China. J Dermatol Sci. 73:63–66.
2014.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Acikbas I, Sanlı B, Tepeli E, Ergin S,
Aktan S and Bagci H: Vitamin D receptor gene polymorphisms and
haplotypes (Apa I, Bsm I, Fok I, Taq I) in Turkish psoriasis
patients. Med Sci Monit. 18:CR661–6. 2012.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Ruggiero M, Gulisano M, Peruzzi B, Giomi
B, Caproni M, Fabbri P and Pacini S: Vitamin D receptor gene
polymorphism is not associated with psoriasis in the Italian
Caucasian population. J Dermatol Sci. 35:68–70. 2004.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Okita H, Ohtsuka T, Yamakage A and
Yamazaki S: Polymorphism of the vitamin D(3) receptor in patients
with psoriasis. Arch Dermatol Res. 294:159–162. 2002.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Park BS, Park JS, Lee DY, Youn JI and Kim
IG: Vitamin D receptor polymorphism is associated with psoriasis. J
Invest Dermatol. 112:113–116. 1999.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Mee JB and Cork MJ: Vitamin D receptor
polymorphism and calcipotriol response in patients with psoriasis.
J Invest Dermatol. 110:301–302. 1998.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Kontula K, Välimäki S, Kainulainen K,
Viitanen AM and Keski-Oja J: Vitamin D receptor polymorphism and
treatment of psoriasis with calcipotriol. Br J Dermatol.
136:977–978. 1997.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Ohata C, Anezaki H, Kaneko S, Okazaki F,
Ito K, Matsuzaka Y, Kikuchi S, Koike Y, Murota H, Miyagi T, et al:
Clinical characteristics of patients with psoriasis with family
history: A multicenter observational study. J Dermatol. 50:746–752.
2023.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Dayangac-Erden D, Karaduman A and
Erdem-Yurter H: Polymorphisms of vitamin D receptor gene in Turkish
familial psoriasis patients. Arch Dermatol Res. 299:487–491.
2007.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Neves JSF, Visentainer JEL, Reis DMDS,
Rocha Loures MA, Alves HV, Lara-Armi FF, de Alencar JB, Valentin
Zacarias JM and Sell AM: The Influence of Vitamin D Receptor Gene
Polymorphisms in Spondyloarthritis. Int J Inflam.
2020(8880879)2020.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Langenbruch A, Radtke MA, Krensel M,
Jacobi A, Reich K and Augustin M: Nail involvement as a predictor
of concomitant psoriatic arthritis in patients with psoriasis. Br J
Dermatol. 171:1123–1128. 2014.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Stuart PE, Nair RP, Tsoi LC, Tejasvi T,
Das S, Kang HM, Ellinghaus E, Chandran V, Callis-Duffin K, Ike R,
et al: Genome-wide association analysis of psoriatic arthritis and
cutaneous psoriasis reveals differences in their genetic
architecture. Am J Hum Genet. 97:816–836. 2015.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Meyer V, Saccone DS, Tugizimana F, Asani
FF, Jeffery TJ and Bornman L: Methylation of the vitamin D receptor
(VDR) Gene, together with genetic variation, race, and environment
influence the signaling efficacy of the toll-like receptor 2/1-VDR
pathway. Front Immunol. 8(1048)2017.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Stratigos AJ, Richard MA, Dessinioti C,
Paul C, Nijsten T, Gisondi P, Salavastru C, Taieb C, Trakatelli M,
Puig L, et al: The prevalence of skin diseases in Greece, impact on
quality of life and stigmatization: A population-based survey
study. JEADV Clin Pract. 3:591–599. 2024.
|
|
50
|
Visscher PM, Wray NR, Zhang Q, Sklar P,
McCarthy MI, Brown MA and Yang J: 10 Years of GWAS discovery:
Biology, function, and translation. Am J Hum Genet. 101:5–22.
2017.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Manolio TA, Collins FS, Cox NJ, Goldstein
DB, Hindorff LA, Hunter DJ, McCarthy MI, Ramos EM, Cardon LR,
Chakravarti A, et al: Finding the missing heritability of complex
diseases. Nature. 461:747–753. 2009.PubMed/NCBI View Article : Google Scholar
|