Introduction
Kidney and ureter duplication is among the most
common congenital anomalies of the kidney and urinary tract,
representing a frequent structural variant in clinical urology
(1,2). Due to its diverse clinical
manifestations, misdiagnosis or a missed diagnosis could cause
difficulties in surgical treatment (3,4).
Epidemiological studies have reported an overall incidence ranging
from 0.3 to 2.0% in the general population, with autopsy series
indicating incidence rates of ~1:125 to 1:150 live births (5-7).
The condition displays a distinct female predominance, with a
female-to-male ratio of ~2:1. Unilateral involvement is
approximately six times more frequent than bilateral disease.
Complete duplication accounts for ~40% of all cases, while
incomplete duplication constitutes the remaining 60% (1,8).
Embryologically, ureteral duplication arises from
abnormal budding or premature bifurcation of the ureteric bud from
the mesonephric duct during early fetal development, disrupting the
healthy formation of a single collecting system for the kidney and
ureter (9). Under healthy
conditions, a single ureteric bud induces the differentiation of
the metanephric blastema to form one renal pelvis and ureter. When
developmental interference occurs, supernumerary or early-splitting
ureteric buds lead to separate or partially fused collecting
systems, resulting in duplex kidneys and duplicated ureters
(10-12).
Stones complicating ureteral duplication remain
relatively uncommon, with an incidence of 3-8% in patients with
duplex collecting systems, and can be particularly elusive when
located in communicating or blind-ending segments, mimicking
bladder calculi on imaging (13).
Early and accurate diagnosis along with timely intervention are
critical to preserve renal function, relieve symptoms and prevent
recurrence. To enhance clinical awareness and provide evidence for
clinical practice, the current study presents a rare case of
complete ureteral duplication with occult calculi successfully
managed with endoscopic laser lithotripsy and stent placement.
Case report
A 50-year-old woman sought medical attention at the
Second Hospital of Lanzhou University (Lanzhou, China) for
intermittent hematuria for 1 month (symptoms appeared in February
2022). The patient reported gross hematuria 1 month prior, which
worsened after physical activity. Ultrasound examination revealed a
bladder stone and a stone in the left kidney in March 2022.
However, cystoscopy revealed no bladder stones, confirming that
there was a diagnostic error in the patient's case. At the Second
Hospital of Lanzhou University (Lanzhou, China), a left ureteral
double-J tube was inserted in March 2022. Later in that month, the
patient visited the Department of Urology at Zhangye People's
Hospital Affiliated to Hexi University (Zhangye, China). After
admission, a physical examination revealed the absence of bilateral
renal percussion pain, no obvious mass in the lower abdomen and no
tenderness in the ureteral tract. Ultrasonography revealed an
unclear upper urinary tract and strong echogenicity in the bladder.
Intravenous pyelography (IVP) revealed postoperative changes after
left ureteral double-J tube insertion, including multiple dense
nodular shadows in the left kidney and bladder and urinary tract
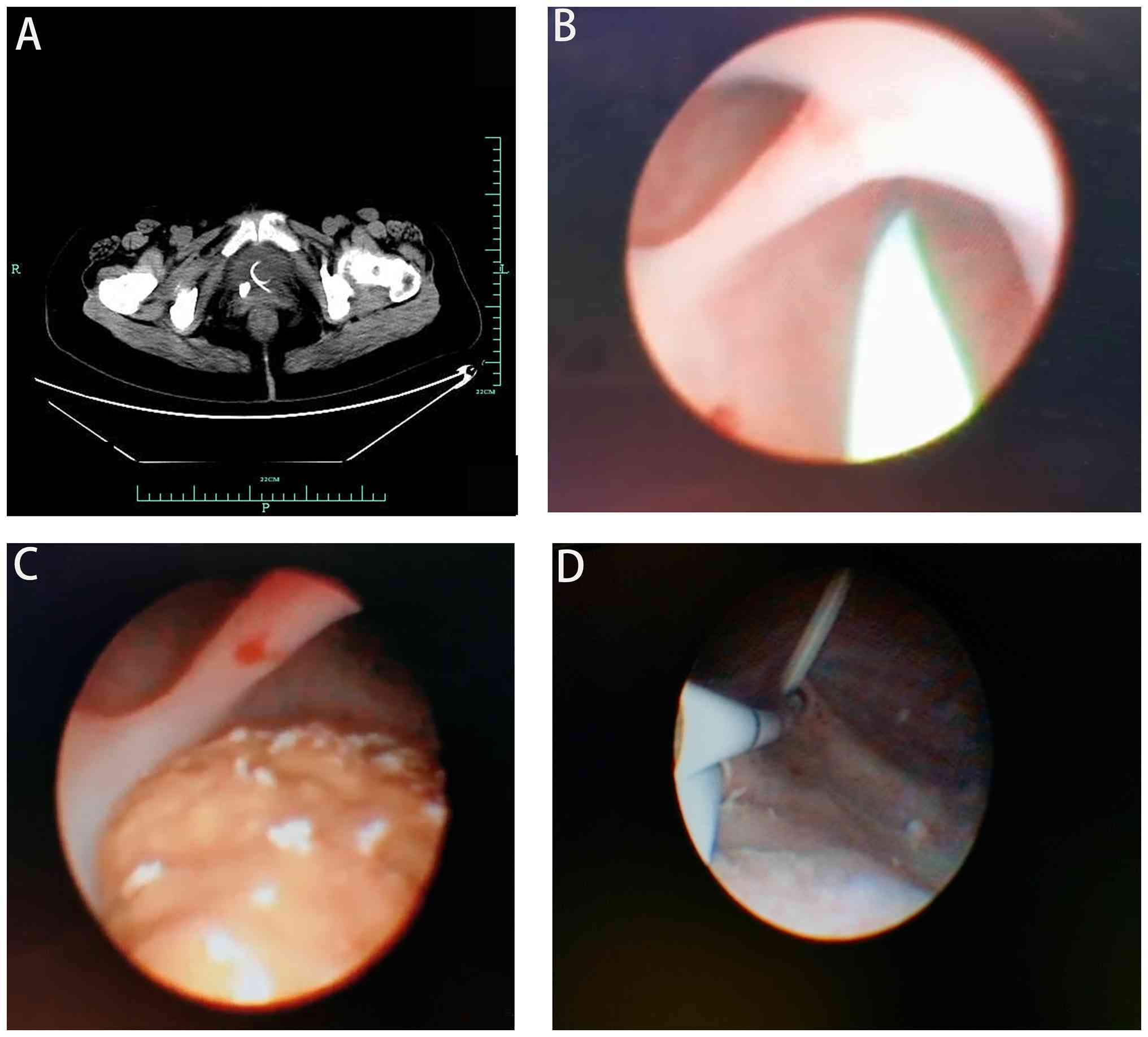
stones. Computed tomography (CT) revealed bladder stones and the
left ureteral double-J tube (Fig.
1A). Routine urine tests revealed the following: 1,269 white
blood cells/µl (normal range, 0-10 white blood cells/µl); 5,134 red
blood cells/µl (normal range, 0-5 red blood cells/µl); and
positivity (++) for protein [normal value, (-) for protein]. Serum
creatinine and BUN levels were within normal ranges.
Cystoscopy was performed 3 days after admission
under general anesthesia in March 2022. The cystoscopy revealed the
curled end of the double-J tube at the left ureteral opening in a
good position. A 6.4/8.0 F ureteroscope was used to enter the
bladder through the urethra, with a slit-shaped right ureteral
opening and clear urine spraying. Under the guidance of a zebra
guidewire, the ureteroscope was inserted into the lower segment of
the right ureter. No stones were found. The urinary tract was
divided into two parts (Fig. 1B),
and an endoscopy was performed along each cavity. The renal nipple
was flattened in the lower renal pelvis, and a blind end was
observed at the junction of the upper renal pelvis, making it
impossible for the endoscope to pass through. No stone shadows were
observed upon returning to the bladder for further exploration.
Another fissure-shaped opening was observed ~2 cm from the ureteral
opening of the right bladder wall. A ureteroscope was guided into
this opening using a guidewire, and a stone was found in the ureter
(Fig. 1C). The guidewire was
removed, and a 200-µm holmium laser fiber, with a light energy of
1.0 W and a frequency of 20 Hz, was inserted. The holmium laser
shattered the stones, and the ascension of the ureteroscope
continued. This opening (fissure-shaped opening was observed ~2 cm
from the ureteral opening of the right bladder wall) was fused and
converged with the original ureteral opening (the normal opening of
the right ureter). A ureteral stent tube was placed in each ureter
(Fig. 1D), and an F18 urinary
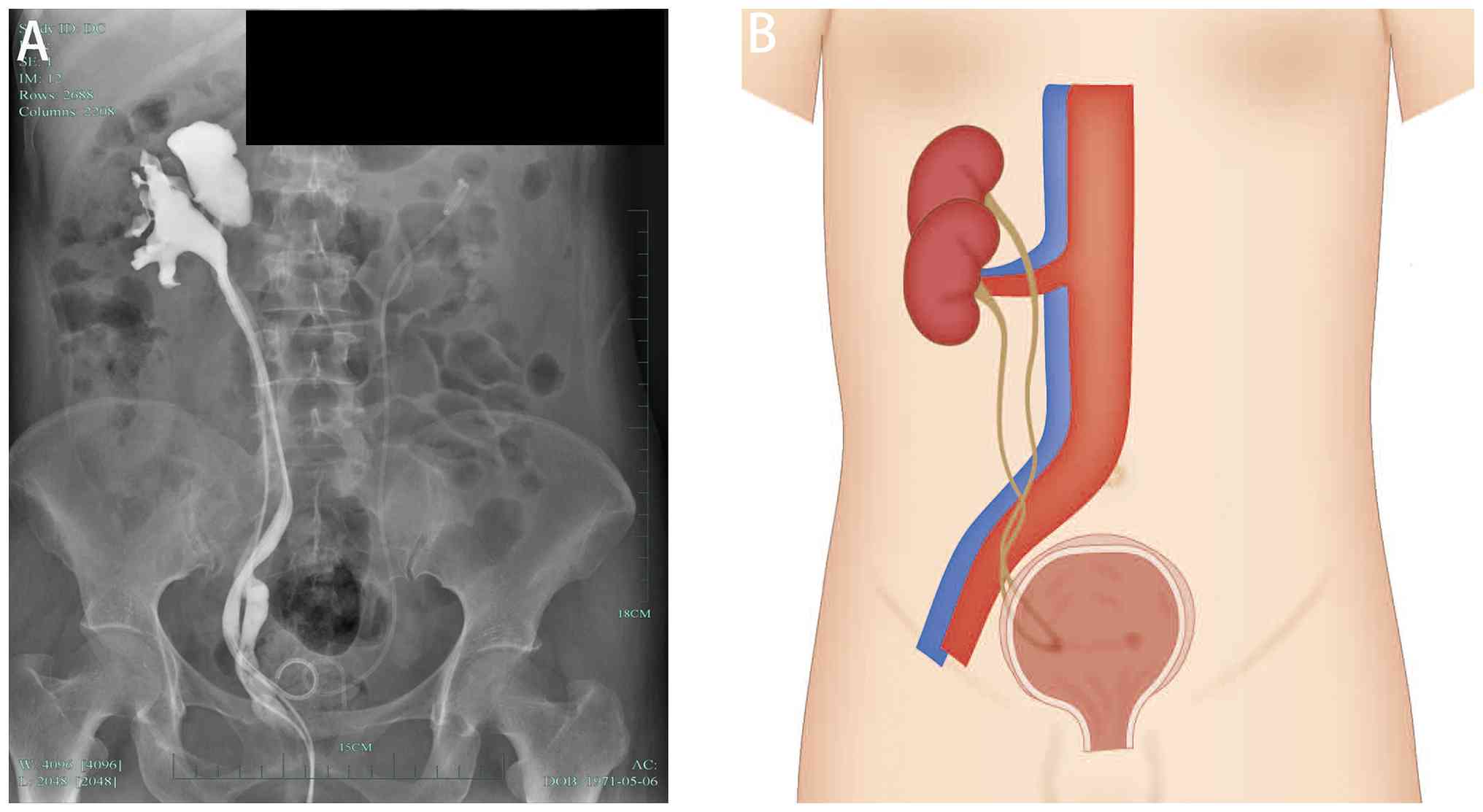
catheter was placed. Surgery was then completed. Blood creatinine
and urea nitrogen levels were within normal limits. Postoperative
retrograde pyelography revealed two kidneys and two ureters on the
right side. The lower segments of each ureter were fused together
but then opened separately into the bladder (Fig. 2). The patient was satisfied with
the treatment outcome. The patient was discharged without
complications and advised to continue follow-up observation as
recommended by the physician. The patient underwent a follow-up CT
scan of the urinary system 1 month after surgery, and no residual
stones were found. After discharge, a follow-up examination 6
months later indicated no abnormalities. Subsequently, a urinary
system CT was performed once a year, revealing no recurrence of the
urinary stones. Family members also underwent physical examinations
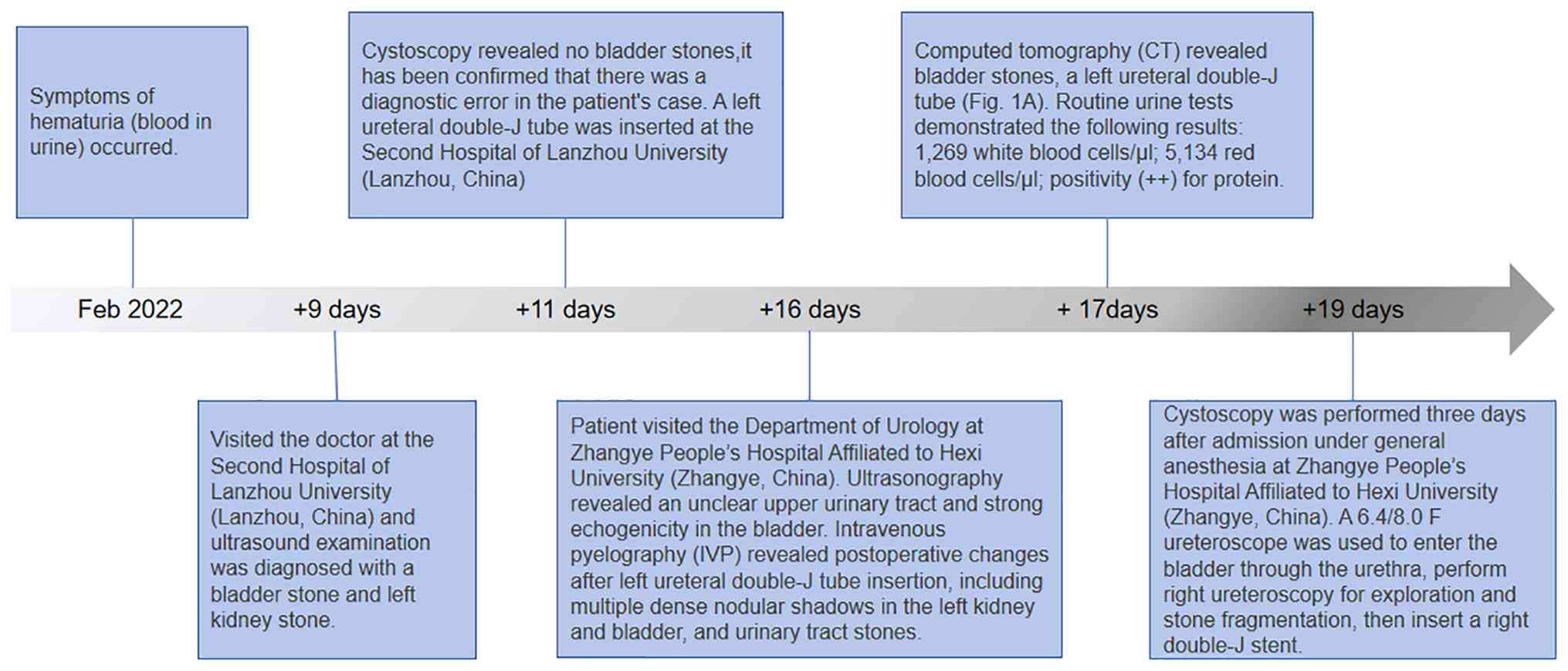
to rule out any urinary system abnormalities. The patient timeline
is presented in Fig. 3.
Discussion
Renal ureteral malformations mainly originate during
early embryonic development, where ureteral buds emerge from the
mesonephric duct and gradually grow and differentiate to form
structures such as the ureters and renal pelvis (14-16).
Under normal circumstances, ureteral buds develop according to a
specific pattern, ultimately creating a single functional
collection system for the ureters and kidneys (9). However, when certain factors
interfere with this normal developmental process, premature or
excessive branching of the ureteral bud may occur, thereby causing
repetitive ureteral malformations (17). Such abnormalities may be related to
genetic, environmental or unknown factors during embryonic
development (18). Although the
specific genetic pattern is not yet fully understood, mutations in
or abnormal expression of ACTA2, ACTG2, BNC2, CHRM3 and HNF1B,
among others, may be associated with repetitive ureteral
malformations (19).
Genetic factors are substantial in this condition.
Ureteral duplication is recognized as part of the spectrum of
congenital anomalies of the kidney and urinary tract, with evidence
supporting autosomal dominant inheritance with incomplete
penetrance (20). Familial studies
have revealed that individuals with an affected first-degree
relative retain a markedly increased risk (21,22).
Molecular investigations have linked duplication phenotypes to
mutations or expression abnormalities in genes governing ureteric
budding and outgrowth, such as roundabout guidance receptor 2,
GEN1, RET and glial cell derived neurotrophic factor, and
downstream mediators of the MAPK/ERK pathway.
These genes regulate critical steps in branching
morphogenesis and tissue interaction, with dysfunction that could
induce duplicated or ectopic ureteric buds (18,19).
Environmental and maternal factors further contribute to
developmental disruption. Adverse intrauterine conditions
(including maternal infection, febrile illness, and exposure to
tobacco, alcohol, toxic chemicals or certain medications) might
interfere with mesonephric-duct and ureteric-bud development,
increasing the likelihood of congenital urinary anomalies. Although
the precise interactions between genes and the environment remain
elusive, current evidence supports a multifactorial model combining
genetic predisposition and environmental triggers (22). Future research with larger cohorts,
familial analyses and molecular profiling is warranted to clarify
causal pathways and identify actionable risk factors.
The patient described in the present case report was
a middle-aged woman with recurrent gross hematuria as the primary
clinical manifestation. The characteristics of the bladder stones
were clearly displayed on imaging examination, but no stones were
found during cystoscopy. Ureteroscopy revealed that the hidden
location of the stones was in the communication section between the
right repeated ureteral orifices, which was very shallow and
difficult to distinguish from the bladder stones on imaging. The
patient had stones in the lower segment of the ureter, but no
symptoms of obstruction were observed. This was related to
compensation caused by the mutual communication of the right
repeated ureteral orifice; therefore, the patient did not present
with clinical manifestations such as upper urinary tract
obstruction and hydronephrosis. Ureteroscopy revealed a duplicated
right kidney, with the upper renal pelvic ureteral junction at the
blind end. Duplicate ureteral malformations cannot be visualized
during the excretion period of CT urography, leading to
difficulties in the clinical diagnosis (23).
In the present case, the diagnosis was difficult,
with multiple examinations indicating bladder stones. However,
cystoscopy did not detect the presence of stones, confusing the
clinical diagnosis. The clinical manifestations of recurrent
ureteral malformation are diverse. Some patients may be
asymptomatic and the malformations may only be incidentally
discovered during physical examination, there have been no reports
of repeated kidneys, repeated ureters, repeated ureteral openings,
mutual communication between repeated ureteral openings or hidden
stones in the communication segment, both domestically and
internationally. In terms of diagnosis, the combined application of
imaging examination methods such as IVP and CT provided strong
support for the accurate diagnosis of the present case, which is
consistent with the comprehensive diagnostic methods emphasized in
previous literature (24,25). However, the specific morphology and
degree of deformities may vary among cases, and treatment plans
must be selected based on individual circumstances. Ultrasound, a
non-invasive and convenient examination method, can first detect
abnormalities in the renal structure and dilation of the ureter in
most cases, providing clues for further diagnosis (26). However, ultrasound has certain
limitations in displaying the entire ureter and observing subtle
structures; therefore, it is necessary to combine IVP and CT
(5). CT scans provide more
detailed anatomical information, not only accurately displaying the
structure of the kidneys and ureters but also detecting lesions in
surrounding tissues, which is of great importance for the
differential diagnosis and surgical planning. IVP can clearly
display the morphology and course of the renal pelvis and ureter,
which is of great value for clarifying the anatomical structure of
the duplicated ureter and assessing renal function (23,27).
In the present case, the IVP failed to detect the duplicated
structures early. Postoperative retrograde pyelography was
necessary to clearly display the dilation and tortuosity of the
duplicated kidneys and ureters, which helped determine the location
and degree of the lesion.
In conclusion, due to the diversity and lack of
specificity in the clinical manifestations of recurrent ureteral
malformations, they pose certain challenges to clinical diagnosis.
Some patients may not have obvious symptoms in the early stages and
the malformations may only be incidentally discovered during
physical or imaging examinations for other reasons. In patients
with symptoms, the symptoms may vary and include lower back pain,
abdominal pain, hematuria, frequent urination and urgency (4,6).
These symptoms are similar to those of other urinary system
diseases and can easily lead to misdiagnosis or a missed diagnosis.
Therefore, improving doctors' understanding of ureteral
malformations and strengthening research on its clinical
characteristics, diagnostic methods and treatment strategies have
important clinical significance. The present case suggests that by
comprehensively using multiple imaging examination methods and by
proficiently using cystoscopy and ureteroscopy, diagnostic accuracy
can be improved. In clinical practice, personalized diagnosis and
treatment plans should be developed based on the patient's specific
situation, and attention should be paid to postoperative follow-up
observations.
Acknowledgements
Not applicable.
Funding
Funding: The present study was funded by grants from the Gansu
Province Youth Science and Technology Research and Development
‘Unveiling and Leading’ Project (Five Small Innovation Achievements
Project; grant no. GQK2024068), the Gansu Province Youth Talent
Project (grant no. 2025QNGR61) and the Hexi University 14th Science
and Technology Innovation Project (grant no. 164).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
HZ, LW and JY drafted the manuscript and designed
the study. RY, SN and FY contributed substantially to the
conceptualization and design of the study. FY completed the
surgery. FY and JY approved the final version of the manuscript for
publication. FY and JY confirm the authenticity of all the raw
data. All authors have read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of the data and images included in the
present study.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Didier RA, Chow JS, Kwatra NS, Retik AB
and Lebowitz RL: The duplicated collecting system of the urinary
tract: Embryology, imaging appearances and clinical considerations.
Pediatr Radiol. 47:1526–1538. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Jaiman S and Ulhøj BP: Bilateral
intravesical ureterocele associated with unilateral partial
duplication of the ureter and other anomalies: proposal of a new
variant to the classification of ureterocles based on a perinatal
autopsy, review of the literature and embryology. APMIS.
118:809–814. 2010.PubMed/NCBI View Article : Google Scholar
|
|
3
|
La Fianza A, Mussati G, Prevedoni Gorone
MS and Vercelli A: Diagnostic imaging of inverted Y duplication of
the ureter with anomalous point angle. A case report. Minerva Urol
Nefrol. 58:157–159. 2006.PubMed/NCBI
|
|
4
|
Somoza Argibay I, Méndez Gallart R, Gómez
Tellado M, Pais Piñeiro E, Liras Muñoz J, Vázquez Martull E and
Vela Nieto D: Treatment of pyeloureteral duplication associated
with ureterocele or ectopic ureter. Actas Urol Esp. 25:731–736.
2001.PubMed/NCBI View Article : Google Scholar : (In Spanish).
|
|
5
|
Houat AP, Guimarães CTS, Takahashi MS,
Rodi GP, Gasparetto TPD, Blasbalg R and Velloni FG: Congenital
anomalies of the upper urinary tract: A comprehensive review.
Radiographics. 41:462–486. 2021.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Pohl HG and Belman AB: Congenital
anomalies of the urinary tract. Curr Pediatr Rev. 10:123–132.
2014.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Boato RT, Aguiar MB, Mak RH, Colosimo EA,
Simões E Silva AC and Oliveira EA: Maternal risk factors for
congenital anomalies of the kidney and urinary tract: A
case-control study. J Pediatr Urol. 19:199.e1–199.e11.
2023.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Katsoufis CP, DeFreitas MJ, Infante JC,
Castellan M, Cano T, Safina Vaccaro D, Seeherunvong W, Chandar JJ
and Abitbol CL: Risk assessment of severe congenital anomalies of
the kidney and urinary tract (CAKUT): A birth cohort. Front
Pediatr. 7(182)2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Kispert A: Ureter development and
associated congenital anomalies. Nat Rev Nephrol. 21:366–382.
2025.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Jain S, Encinas M, Johnson EM Jr and
Milbrandt J: Critical and distinct roles for key RET tyrosine
docking sites in renal development. Genes Dev. 20:321–333.
2006.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Nagalakshmi VK and Yu J: The ureteric bud
epithelium: Morphogenesis and roles in metanephric kidney
patterning. Mol Reprod Dev. 82:151–166. 2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Brockwell M, Hergenrother S, Satariano M,
Shah R and Raina R: Pathophysiology of congenital anomalies of the
kidney and urinary tract: A comprehensive review. Cells.
13(1866)2024.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Aggarwal D, Parmar K, Mathew J and Kumar
S: Sheathless synchronous flexible ureterorenoscopy with holmium
laser lithotripsy in complete duplex renal collecting system with
stones. Urol Case Rep. 37(101707)2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Chen RY and Chang H: Renal dysplasia. Arch
Pathol Lab Med. 139:547–551. 2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Renkema KY, Winyard PJ, Skovorodkin IN,
Levtchenko E, Hindryckx A, Jeanpierre C, Weber S, Salomon R,
Antignac C, Vainio S, et al: Novel perspectives for investigating
congenital anomalies of the kidney and urinary tract (CAKUT).
Nephrol Dial Transplant. 26:3843–3851. 2011.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Schedl A: Renal abnormalities and their
developmental origin. Nat Rev Genet. 8:791–802. 2007.PubMed/NCBI View
Article : Google Scholar
|
|
17
|
Mederacke M, Conrad L, Doumpas N, Vetter R
and Iber D: Geometric effects position renal vesicles during kidney
development. Cell Rep. 42(113526)2023.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Du X, Yu M, Ju H, Xue S, Li Y, Wu X, Xu H
and Shen Q: Inhibition of MAPK/ERK pathway activation rescues
congenital anomalies of the kidney and urinary tract (CAKUT) in
Robo2PB/+ Gen1PB/+ mice. Biochem Biophys Res
Commun. 653:153–160. 2023.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Woolf AS, Lopes FM, Ranjzad P and Roberts
NA: Congenital disorders of the human urinary tract: Recent
insights from genetic and molecular studies. Front Pediatr.
7(136)2019.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Atwell JD and Allen NH: . The
interrelationship between paraureteric diverticula, vesicoureteric
reflux and duplication of the pelvicaliceal collecting system: A
family study. Br J Urol. 52:269–273. 1980.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Santavá A, Utíkalová A and Santavý J: .
Heredity and origin of duplication of the pelvicalyceal collecting
system. Acta Univ Palacki Olomuc Fac Med. 126:209–218.
1990.PubMed/NCBI
|
|
22
|
Yu W, Hu X and Cao B: Viral infections
during pregnancy: The big challenge threatening maternal and fetal
health. Matern Fetal Med. 4:72–86. 2021.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Xie N, Huang X, Zhou J, Zhang H and Ma W:
CTU findings of duplex kidney in kidney: A rare duplicated renal
malformation. Open Med (Wars). 16:651–654. 2021.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Papatsoris A, Alba AB, Galán Llopis JA,
Musafer MA, Alameedee M, Ather H, Caballero-Romeu JP, Costa-Bauzá
A, Dellis A, El Howairis M, et al: Management of urinary stones:
State of the art and future perspectives by experts in stone
disease. Arch Ital Urol Androl. 96(12703)2024.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Dell'Aversana F, Pezzullo M and Scaglione
M: Imaging in urolithiasis. Urol Clin North Am. 52:51–59.
2025.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Dias T, Sairam S and Kumarasiri S:
Ultrasound diagnosis of fetal renal abnormalities. Best Pract Res
Clin Obstet Gynaecol. 28:403–415. 2014.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Deng J, Lu X and Liu Y: Ectopic insertion
of a duplicated ureter into prostatic urethra: Demonstration by 3D
multi-detector computed tomography urography. J Xray Sci Technol.
24:661–664. 2016.PubMed/NCBI View Article : Google Scholar
|