Introduction
Chronic heart failure (CHF) is the advanced stage or
end-stage of various heart diseases. The pathogenesis of CHF
involves the renin-angiotensin-aldosterone system and excessive
neurohormonal activation. Immune system activation and a number of
inflammatory cytokines are involved in CHF (1–4).
High mobility group box-1 (HMGB1) is a conserved
nuclear DNA-binding protein involved in the maintenance of
nucleosome structure and in DNA recombination, replication, and
gene transcription (5–8). HMGB1 is released passively from
necrotic or damaged cells and is actively secreted by immune cells,
including monocytes, macrophages, and dendritic cells (8). HMGB1 is a potent extracellular
cytokine involved in cellular activation and triggers a rigorous
inflammatory response through interactions with its receptors
(8,9). Extracellular HMGB1 binds to a
variety of cell surface receptors, including receptors for advanced
glycation end products (RAGE) (10), toll-like receptor (TLR)2, and TLR4
(11), leading to the activation
of downstream physiologic and pathologic responses (12). The binding of HMGB1 to RAGE
receptors results in the activation of mitogen-activated protein
kinases (MAPKs) and of the nuclear factor-κB (NF-κB) transcription
factor, which induces the production of various pro-inflammatory
cytokines (13). In addition,
previous studies have demonstrated that HMGB1 is pivotal in
cardiovascular diseases, including atherosclerosis, myocardial
ischemia/reperfusion injury, CHF, and myocardial infarction
(14). In particular, CHF is
considered to be an inflammatory disease and HMGB-1 is important in
its progression (10,15,16). A high level of HMGB-1 is often
found in patients with CHF, where it is released by activated
macrophages and, in turn, induces the expression of other
inflammatory cytokines that are able to amplify macrophage
recruitment, starting a vicious circle (17).
Statins are inhibitors of
3-hydroxy-3-methylglutaryl-coenzyme A reductase and are used
extensively for treatment of coronary heart diseases due to their
cholesterol-lowering effects (18). Furthermore, statins exert
beneficial pleiotropic effects, including plaque stabilization,
anti-inflammatory effects, and the prevention of endothelial
dysfunction (19). In addition,
statins protect endothelial cells against ischemia reperfusion
injury through the HMGB1/TLR4 pathway (20,21). However, whether statins can
influence the HMGB1/RAGE/NF-κB pathway and the production of
inflammatory agents remains to be fully elucidated.
Therefore, in the present study, it was hypothesized
that rosuvastatin may attenuate myocardial injury by inhibiting the
expression of HMGB1 and RAGE. To test this hypothesis, adriamycin
(ADR)-treated rats were used. The aim of the present study was to
assess whether rosuvastatin attenuates myocardial injury in
ADR-treated rats and whether the activation of HMGB1/RAGE is
involved.
Materials and methods
Animals
Male Sprague-Dawley rats aged 6–8 weeks (220–260 g)
were obtained from the Animal Center of the Chinese Academy of
Sciences (Shanghai, China). The rats were housed under a 12-h
dark-light cycle at 20–25°C and 40–60% humidity, with five
rats/cage, and free access to food and water. The experiments were
performed following 1 week of adaptive feeding. The experiments
were performed in accordance with the NIH Guide for the Care and
Use of Laboratory Animals and were approved by the Animal Care and
Use Committee of Nanjing Medical University (Nanjing, China).
During the experiment, the following criteria were used to indicate
end of life of the experimental animals: i) significant weight loss
(>30% weight loss) or cachexia; ii) complete loss of appetite
for >24 h or poor appetite (<50% of normal diet) for >3
days; ii) unable to eat or drink water under no anesthesia or
sedation; iv) depression or hypothermia (<37°C) under no
anesthesia or sedation; v) clinical symptoms of severe functional
loss of organs and treatment failure; vi) expiratory dyspnea; vii)
severe diarrhea and peritonitis; viii) tremors and paralysis; or
ix) severe ulcerations of the skin.
Grouping
The rats were randomized into the following groups
(n=10/group): i) Control group, rats administered with 0.9% saline
solution without ADR at 1 mg/kg/day for 14 days via intraperitoneal
injection and with 0.9% saline without rosuvastatin at a dosage of
1 mg/kg/day for 6 weeks by gavage administration; ii) ADR group,
rats injected with equal volumes of ADR solution (ADR dissolved in
0.9% saline solution, 10 mg/ml) for 2 weeks plus administration of
equal volumes of 0.9% saline solution without rosuvastatin; iii)
ADR+rosuvastatin group, rats administered with equal volumes of ADR
for 2 weeks and rosuvastatin (1 mg/kg/day) (22) solution for 6 weeks (rosuvastatin
was dissolved in 0.9% saline solution, 10 mg/ml). All rats received
the drug at 10 a.m. and the intraperitoneal injection at 9 a.m. (1
h prior to gavage). ADR was purchased from Haizheng Chemical Co.,
Ltd. (Zhejiang, China). Rosuvastatin was provided by AstraZeneca
(London, UK). All examinations and sample collection
(echocardiography, blood collection, and myocardial tissue
collection) were performed at 12 weeks.
Enzyme-linked immunosorbent assay
(ELISA)
Blood samples were collected from the ophthalmic
artery and the serum was separated by centrifugation at 1,500 × g
for 15 min at 4°C. The levels of blood urea nitrogen (BUN; cat. no.
R0119), creatinine (Cr; cat. no. R0120), alanine aminotransferase
(ALT; cat. no. R0116), aspartate aminotransferase (AST; cat. no.
R0117), lactate dehydrogenase (LDH; cat. no. R0042), creatine
kinase isoenzyme-MB (CK-MB; cat. no. R0043), triglycerides (TG;
cat. no. R0794), total cholesterol (CHO; cat. no. R0794),
low-density lipoprotein cholesterol (LDL-C; cat. no. R0794), and
high density lipoprotein cholesterol (HDL-C; cat. no. R0794) in
serum samples were determined using ELISA kits (Nanjing Senbeijia
Biological Technology Co., Ltd., Nanjing, China), according to the
manufacturer’s protocol.
Echocardiography measurements
Echocardiography was performed to assess the heart
function of the rats 12 weeks following the first treatment,
according to a previously published method (23). The rats were anesthetized using
chloral hydrate (5%, 0.7 ml/100 g, equivalent to 350 mg/kg) via
intraperitoneal injection. Images were captured using a 12-MHz
linear transducer connected to a Vivid 7 echocardiography machine
(GE Healthcare Life Sciences, Chalfont, UK). A two-dimensional
short-axis view of the left ventricle was obtained at the level of
the papillary muscle and two-dimensional targeted M-mode tracings
were recorded. The detection indices were as follows: Systolic left
ventricular internal dimension (LVIDs), diastolic left ventricular
internal dimension (LVIDd), left ventricular ejection fraction
(LVEF), left ventricular end-diastolic pressure (LVEDP), and left
ventricular fractional shortening (LVFS). All these parameters were
measured over three consecutive cardiac cycles.
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR) analysis
The mRNA expression levels of HMGB1 and RAGE were
determined by RT-qPCR analysis. Total RNA was extracted with TRIzol
(Promega Corporation, Madison, WI, USA), according to the
manufacturer’s protocol. Total cDNA was synthesized using the
HiScript II 1st Strand cDNA Synthesis kit (+gDNA wiper), purchased
from Vazyme Biotech Co., Ltd. (Nanjing, China). The cDNA was then
amplified by PCR. The forward and reverse primers were as follows:
HMGB1 forward, 5′-CCT GAG AAT GTA TCC CCA AAA GC-3′ and reverse,
5′-CAG TCA AGT TTC CTG AGC AA TCC-3′ (product size: 149 bp); RAGE
forward, 5′-TAGCCA TGG ACC TCA GGA AAG-3′ and reverse, 5′-CCA ATG
AGC AGA GCG GCT AT-3′ (product size: 159 bp); and GAPDH forward,
5′-GGT GGA CCT CAT GGC CTA CA-3′ and reverse, 5′-TTG TGA GGG AGA
TGC TCA GTG T-3′ (product size: 246 bp). PCR was performed with
12.5 μl Maxima SYBR Green/ROX qPCR Master Mix (2X; Thermo
Scientific, Inc., K0221, Waltham, MA, USA), 0.75 μl forward
primers (10 μM), 0.75 μl reverse primer (10
μM), 2 μl cDNA and 9 μl distilled water, at
95°C for 15 sec, 60°C for 30 sec, and 30 sec at 72°C for 40 cycles,
according to the manufacturer’s protocol. The comparative Ct method
was used to calculate the relative abundance of the mRNA and the
results for target gene expression were compared with those for
GAPDH. The results were obtained from three independent
experiments. The 2−ΔΔCq method
(24) was calculated to represent
the relative mRNA expression of target genes.
Western blot analysis
Myocardial tissues from the left ventricle were
completely homogenized and centrifuged at 13,000 × g for 15 min at
4°C. The supernatant was collected. An equal volume of 5X SDS
sample buffer was added, and the samples were boiled for 10 min.
Protein concentration was measured using the BCA method. The
samples (50 μg of protein per lane) were subjected to
electrophoresis on 10% SDS-polyacrylamide gels for 30 min at 80 V
followed by 80 min at 120 V. The proteins were transferred onto
polyvinylidene fluoride membranes (Immobilon-PSQ; EMD Millipore,
Billerica, MA, USA) for 1 h at 100 V and 300 mA. The membranes were
blocked with 5% skimmed milk for 2 h at room temperature and
incubated overnight at 4°C with rabbit anti-HMGB1 monoclonal
antibody (1:1,000; cat. no. ab79823; Abcam, Cambridge, MA, USA),
rabbit anti-RAGE polyclonal antibody (1:1,000; cat. no. ab3611;
Abcam), and rabbit GAPDH monoclonal antibody (1:1,000; cat. no.
M20006; Abmart, Berkeley Heights, NJ, USA). The membranes were
washed three times for 10 min each time in PBS with 0.1% Tween-20
(PBST) and were incubated with horseradish peroxidase-conjugated
anti-rabbit immunoglobulin G secondary antibody (1:1,000; cat. no.
7074; Cell Signaling Technology, Inc., Danvers, MA, USA) at room
temperature for 2 h. The blotted protein bands were visualized by
enhanced chemiluminescence (Amersham; GE Healthcare Life Sciences),
and exposed to X-ray films. The developed films were digitized
using an Epson Perfection 2480 scanner (Seiko Co., Ltd., Nagano,
Japan). The optical densities were obtained using Glyko Bandscan
software version 4.5 (Glyko Inc., Novato, CA, USA).
Histology and immunohistochemistry
The rats were sacrificed following 12 weeks of
treatment and cardiac tissues were harvested. The tissue samples
were formalin-fixed, embedded in paraffin, and sectioned at 3–5
μm. The sections were stained with hematoxylin and eosin
(H&E). The histological examination of all sections was
performed with an optical microscope in a blinded-manner.
Immunohistochemistry was performed to detect HMGB1
and RAGE. Briefly, the paraffin sections were dewaxed in xylene and
rehydrated through graded ethanol to water. Antigens were retrieved
by boiling in 10 mM citrate buffer (pH 6.0) and endogenous
peroxidase activity was quenched in methanol containing 3% hydrogen
peroxide. The sections were incubated in phosphate-buffered saline
(PBS) containing 3% bovine serum albumin (Sigma-Aldrich; Merck
KGaA, Darmstadt, Germany) to block nonspecific binding, and with
anti-HMGB1 monoclonal antibody (1:1,000; Abcam) and anti-RAGE
polyclonal antibody (1:800; Abcam) overnight at 4°C, followed by a
15-min period of washing in PBS. The sections were then incubated
with HRP-conjugated IgG (1:500; Santa Cruz Biotechnology, Inc.,
Dallas, TX, USA) for 60 min at room temperature. Those cells in
which HMGB1 and RAGE were expressed in the extranuclear space were
considered to be HMGB1-positive and RAGE-positive cells. The
positive cells were identified, counted and analyzed with an
optical microscope by two pathologists.
Flow cytometry
Tumor necrosis factor (TNF)-α, interferon (IFN)-γ,
interleukin (IL)-4, and IL-10 were measured using the CBA Rat
Soluble Protein Detection kit (Bio-Rad Laboratories, Inc.). The
samples and standards (50 μl each) were incubated in Falcon
tubes with capture beads for 1 h at room temperature in the dark.
The phycoerythrin detection reagent was added to each tube for an
additional 2 h of incubation at room temperature in the dark. The
samples were washed, and the bead pellets were re-suspended in
washing buffer. The re-suspended samples were run on a flow
cytometer (FACS Canto II; BD Biosciences, Franklin Lake, NJ, USA)
equipped with the BD FACSDiva software version 6.1.3. A total of
2,000 events in the gated bead population were collected, and the
5-parameter data were saved for subsequent analysis using BD FCAP
Array software version 3.0. Serum concentrations were derived using
the standard curve and are expressed in pg/ml.
Statistical analysis
SPSS 18.0 (SPSS, Inc., Chicago, IL, USA) was used
for statistical analysis. Data are expressed as the mean ± standard
error of the mean and were analyzed using one-way analysis of
variance followed by the Tukey’s post hoc test. P<0.05
(two-sided) was considered to indicate a statistically significant
difference.
Results
Characteristics of the rats
Three weeks prior to drug administration, the rats
in each group had normal water intake, their hair was soft, and
they were active. At the beginning of week 4, the rats in the ADR
group became lethargic, had decreased food and water intake, slow
movement, loss of hair luster, decreased activity, and symptoms of
eyeball hyperemia and diarrhea. One rat died on each of days 35,
47, and 70 of the experiment in the ADR group, and the survival
rate was 70%. The rats in the ADR+rosuvastatin group showed similar
symptoms to rats in the ADR group, although they occurred later and
were milder. One rat died on day 72 in this group; the survival
rate was 90%. The rats in the control group were generally in good
conditions and none of the rats died. All deceased rats were found
during routine rounds, and none of the rats met the criteria for
end of life as all symptoms were observed to be mild to moderate.
The maximum weight loss observed in rats was ~25%, and the
mortality rate was 30%, which was similar to a previous study
(25).
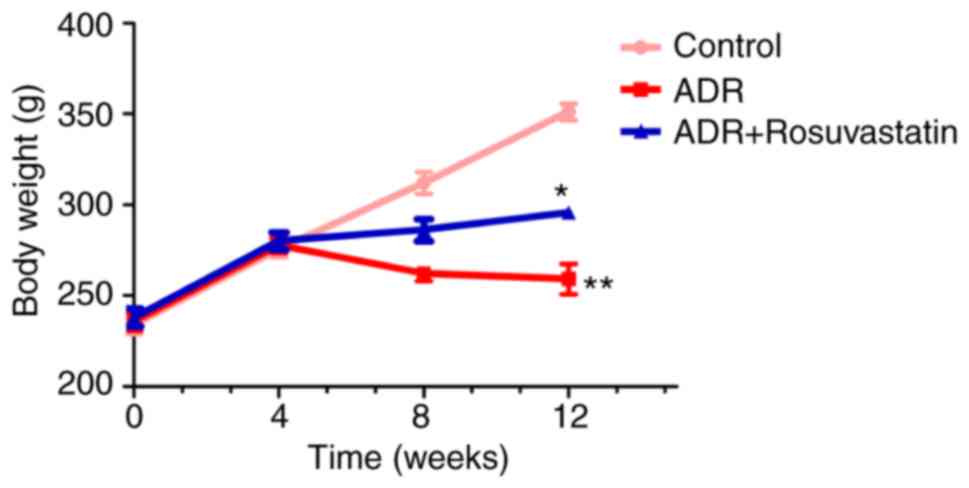
The weights of the rats were measured prior to model
establishment (0 weeks) and at 4, 8, and 12 weeks following model
establishment. The weight of the rats in the control group
increased during each subsequent time period. At 4 weeks prior to
model establishment, the weights of the rats in the ADR and
ADR+rosuvastatin groups maintained the same trend of growth as
those in the control group. At 4 weeks post-modeling, the body
weight of the rats in the ADR group did not increase or decrease.
At 12 weeks post-model establishment, the weight of the rats in the
ADR group was significantly decreased compared with that in the
control group (P<0.01). The weight of the rats in the
ADR+rosuvastatin group was significantly higher than that in the
ADR group (P<0.05) (Fig.
1).
At the end of study, no significant differences in
BUN, Cr, ALT, LDH, TG, or HDL-C were observed among the three
groups. The serum levels of CHO and LDL-C were significantly lower
in the ADR+rosuvastatin group compared with those in the other
groups (P<0.05). The serum levels of AST and CK-MB were elevated
in the ADR group compared with those in the control group and were
significantly lower in the ADR+rosuvastatin group than in the ADR
group (P<0.05; Table I).
 | Table IBiochemical indices in each group at
the end of the study. |
Table I
Biochemical indices in each group at
the end of the study.
| Index | Control | ADR |
ADR+rosuvastatin |
|---|
| Bun | 5.46±0.10 | 6.29±0.43 | 6.42±0.68 |
| Cr | 24.92±3.00 | 26.24±3.13 | 24.56±1.92 |
| ALT | 42.00±6.18 | 47.20±8.28 | 35.80±3.68 |
| AST | 78.7±4.44 | 246.6±63.10b | 117.0±30.5c |
| CK-MB | 420±72 | 2,848±1,443b | 491±72d |
| LDH | 1,218±214 | 1,049±521 | 347±73.9 |
| CHO | 3.13±0.38 | 3.10±0.30 | 1.44±0.12a,c |
| TG | 1.26±0.45 | 1.07±0.30 | 0.55±0.06 |
| HDL | 1.36±0.20 | 0.90±0.03 | 1.17±0.22 |
| LDL | 0.61±0.07 | 0.60±0.08 | 0.25±0.05a,c |
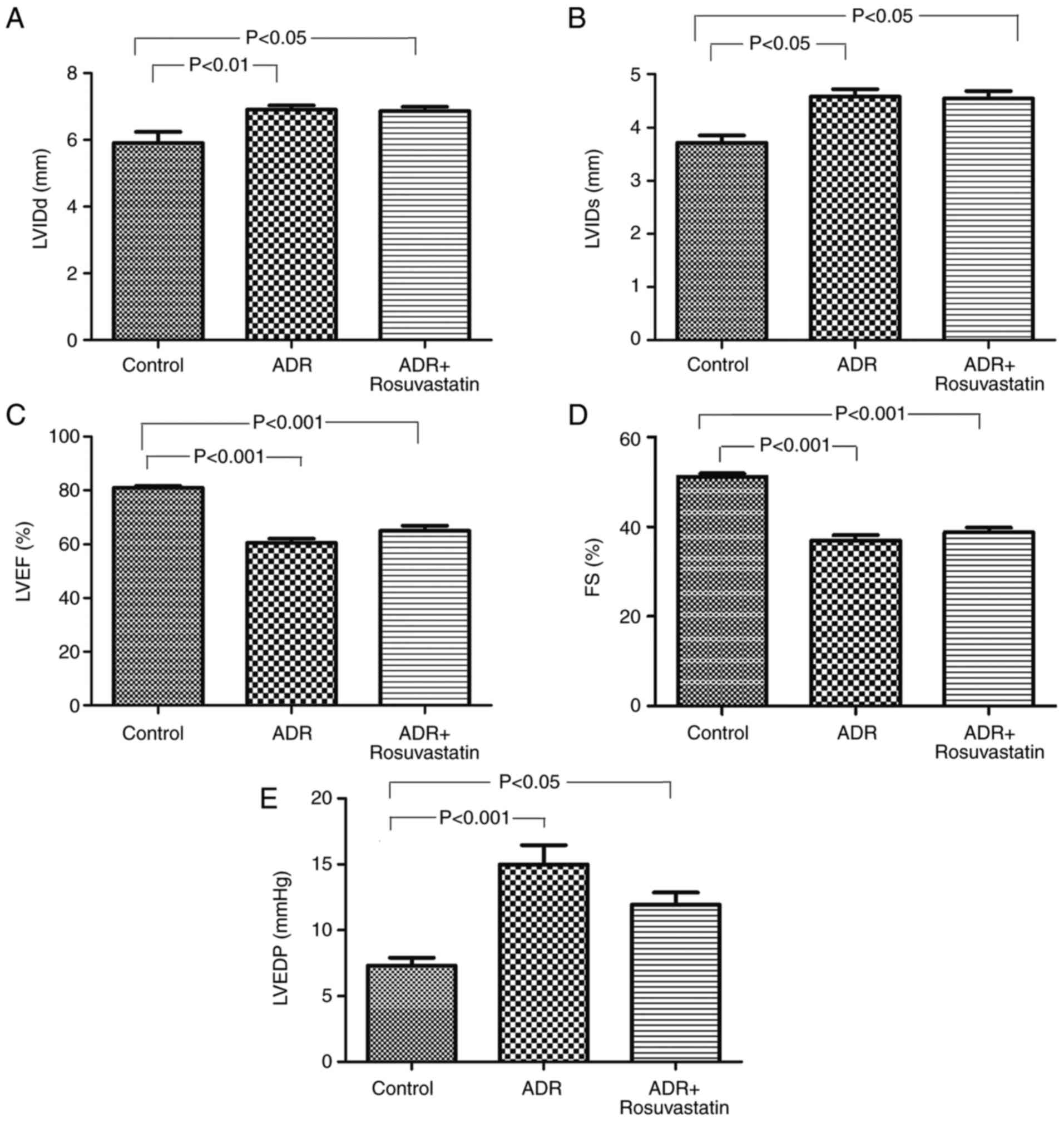
In order to determine whether ADR affected the
cardiac function of the rats, echocardiography was performed at 12
weeks following the first treatment. The echocardiography revealed
that, compared with the control group, the rats in the ADR and
ADR+rosuvastatin groups exhibited significant left ventricular
dilation and systolic dysfunction. The LVIDd, and LVIDs in these
two groups were significantly higher than those in the control
group (P<0.05). The LVEF and LVFS in these two groups were
significantly lower than those in the control group (P<0.05),
whereas the LVEDP was higher (P<0.05; Fig. 2A-E). Rosuvastatin itself did not
improve the heart function (LVIDd, LVIDs, LVEF and LVFS) of the
ADR-treated rats.
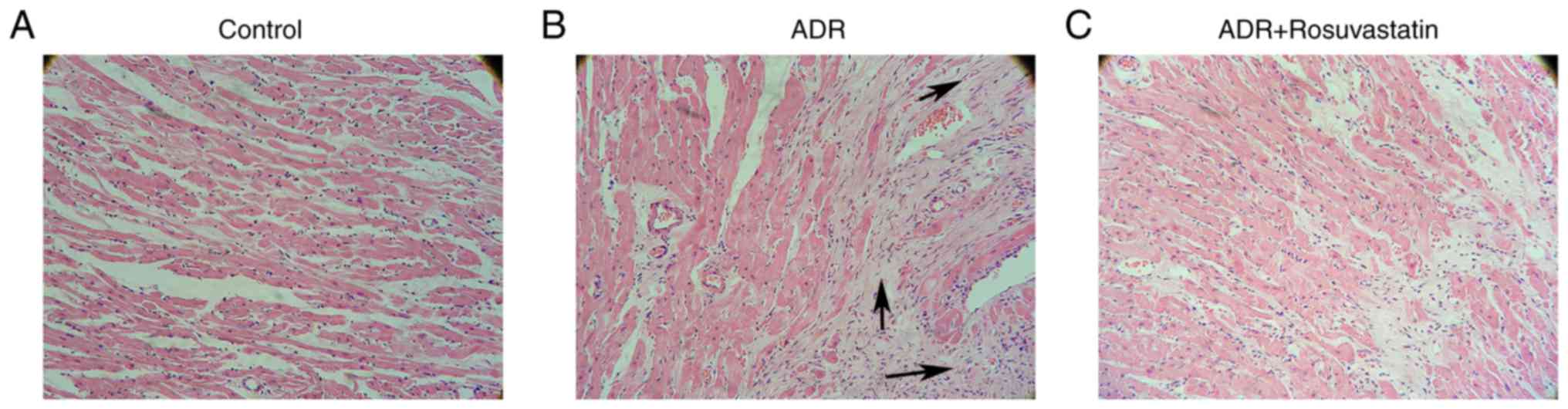
The H&E-stained sections of left ventricular
myocardial tissue are shown in Fig.
3A-C. The tissues from the ADR group showed enhancement and
loose arrangement of the myocardial fibers, loss of myocytes, and
vacuolar degeneration. The administration of rosuvastatin improved
cardiac morphology and alleviated pathological lesions.
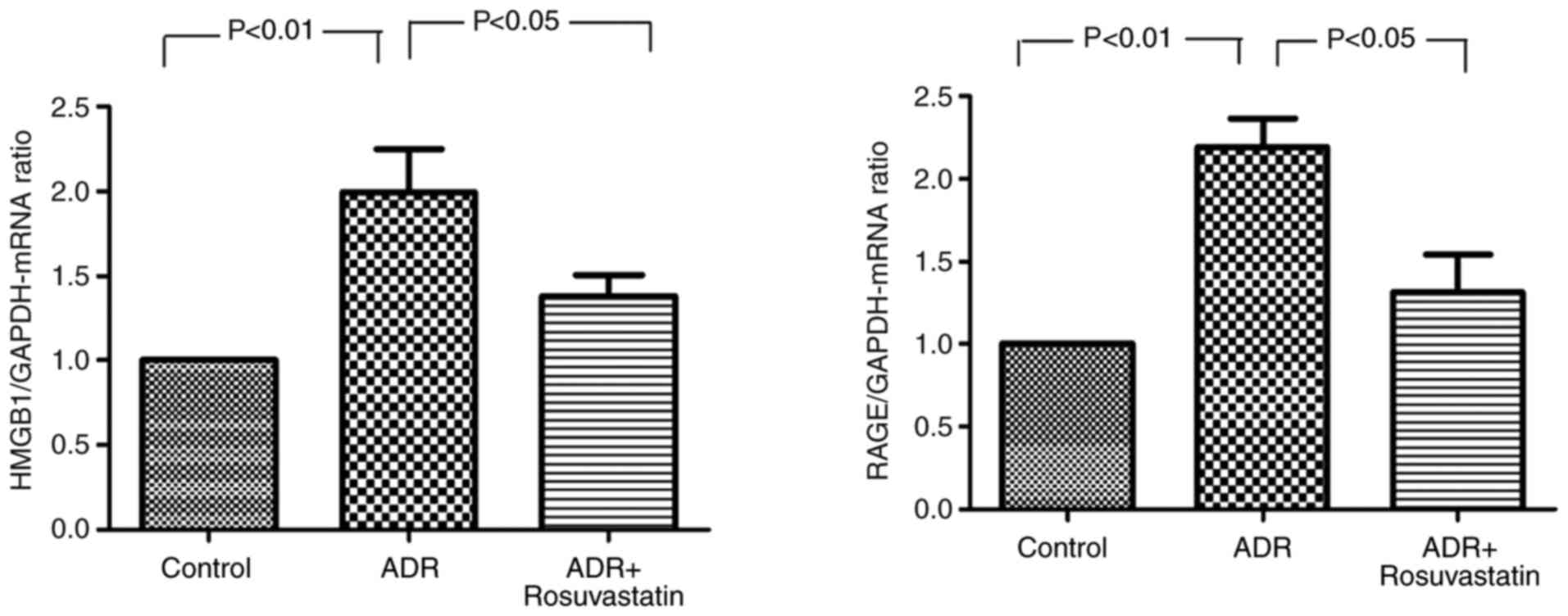
Effect of rosuvastatin on the expression
of HMGB1 and RAGE
The mRNA expression levels of HMGB1 and RAGE in the
myocardium were significantly higher in the ADR group compared with
those in the control group (P<0.01 and P<0.01, respectively).
In the ADR+rosuvastatin group, the mRNA levels of HMGB1 and RAGE in
the myocardium were signifi-cantly lower compared with those in the
ADR group (P<0.05 and P<0.05, respectively; Fig. 4).
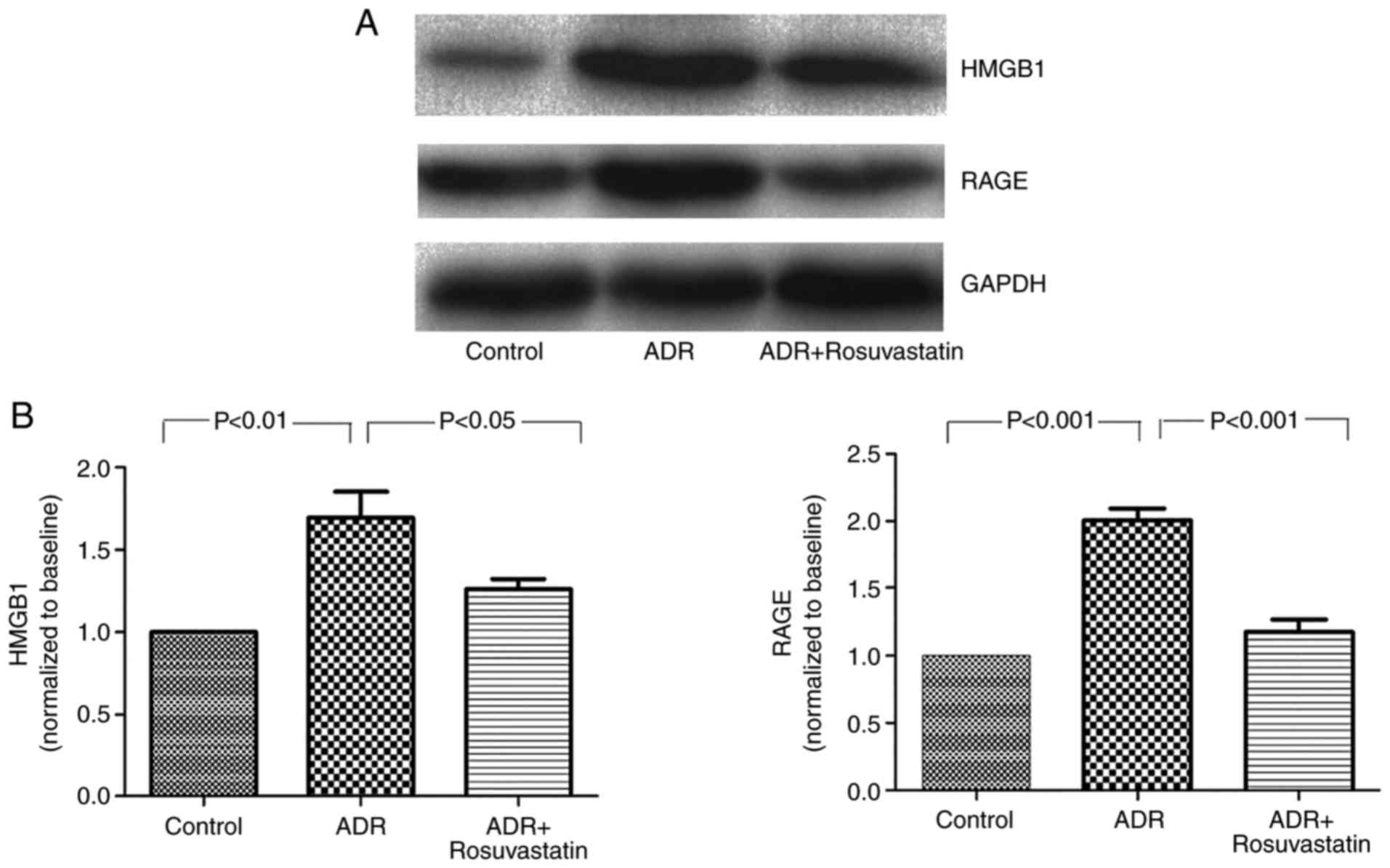
To determine the effect of rosuvastatin on the
expression of HMGB1 and RAGE in the ADR-treated rats, western blot
analysis was performed to detect changes in the protein levels of
HMGB1 and RAGE. The results showed low protein levels of HMGB1 and
RAGE in the control group. The protein levels of HMGB1 and RAGE
were significantly higher in the myocardium of the ADR group
compared with those of the control group (P<0.01 and P<0.001,
respectively). The increased levels of HMGB1 and RAGE were markedly
suppressed in the ADR+rosuvastatin group (P<0.05 and P<0.001,
respectively; Fig. 5A and B).
Rosuvastatin decreases the proportion of
HMGB1- and RAGE-positive cells in the myocardium of ADR-treated
rats
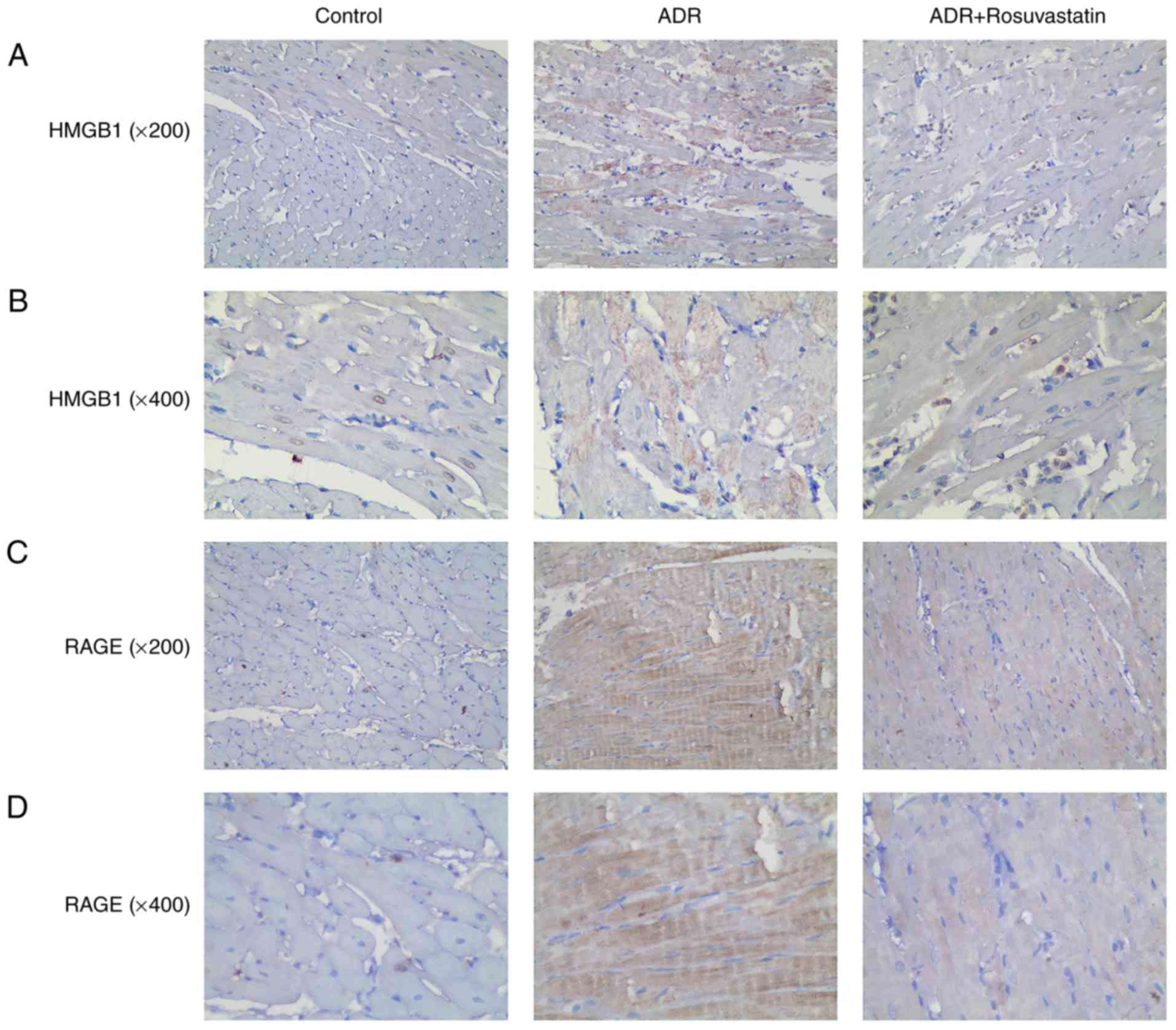
Immunohistochemistry was performed to investigate
the localization and expression of HMGB1 and RAGE in the rat
myocardial tissue. Those myocardial cells in which HMGB1 was found
in the cytoplasm were considered to be HMGB1-positive cells. Few
HMGB1 and RAGE-positive cells were observed in the control group.
Higher numbers of HMGB1 and RAGE-positive cells were observed in
the ADR group. Rosuvastatin significantly decreased HMGB1- and
RAGE-positivity. These results showed that rosuvastatin
significantly reduced HMGB1 and RAGE immunoreactivity in the
myocardium of the ADR-treated rats (Fig. 6A-D).
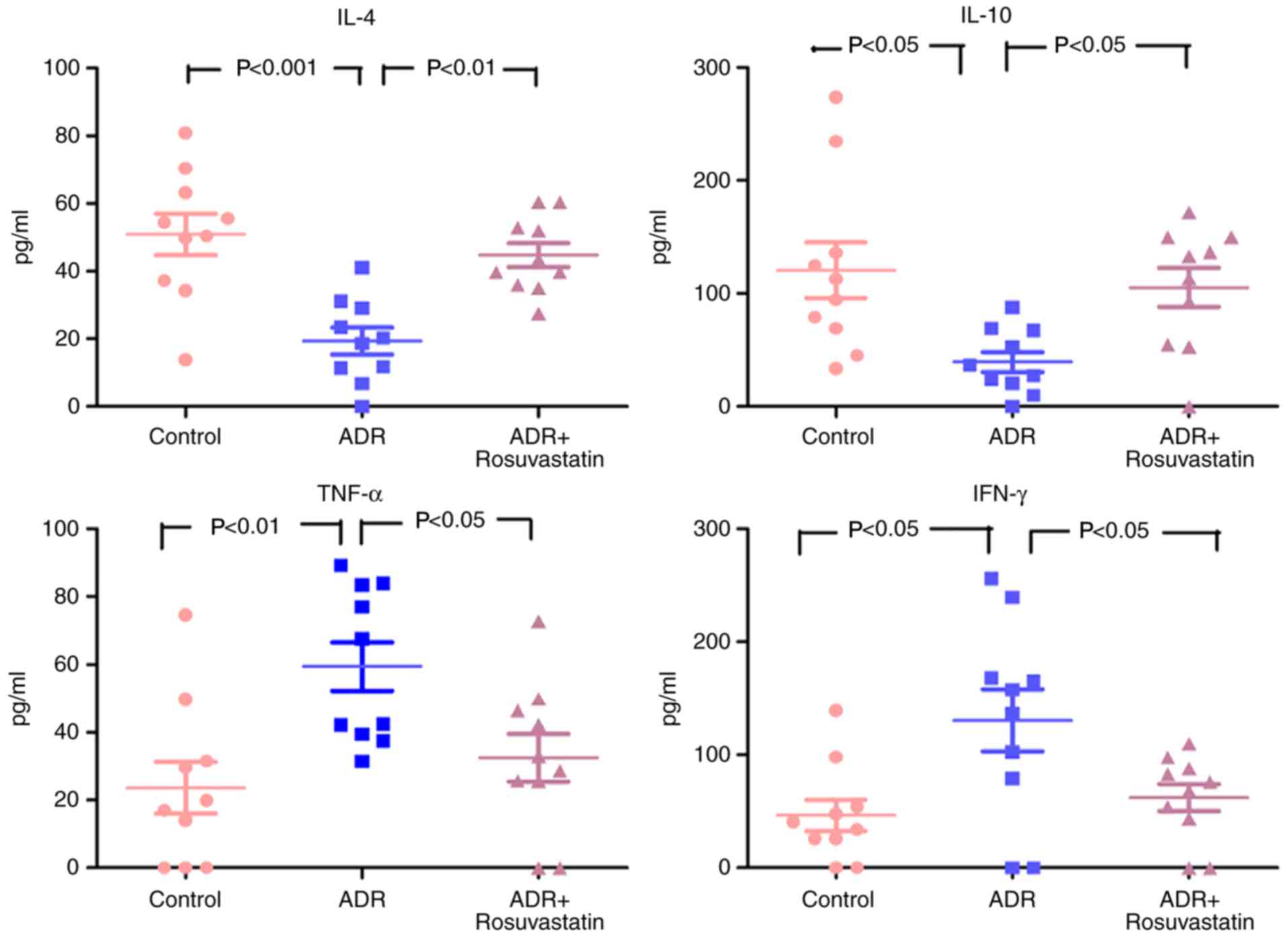
Levels of pro-inflammatory and
anti-inflammatory cytokines in the serum
As shown in Fig.
7, the serum levels of TNF-α and IFN-γ were low, and the levels
of IL-4 and IL-10 were high in the control group. In the ADR group,
the serum levels of TNF-α and IFN-γ were increased, whereas the
levels of IL-4 and IL-10 were decreased. Rosuvastatin significantly
decreased the serum levels of TNF-α and IFN-γ and elevated the
serum levels of IL-4 and IL-10 in the ADR+rosuvastatin group
(Fig. 7).
Discussion
Statins have been shown to mediate HMGB1 and its
different receptors, including RAGE or TLR2/TLR4, to exert
cytoprotective actions and anti-inflammatory effects by inhibiting
the expression of various proinflammatory cytokines (26–28). HMGB1 can activate inflammatory
pathways when released from dying cells (14). In the heart, pre- and
post-conditioning with rosuvastatin has been shown to reduce
ischemia/reperfusion myocardial injury through the inhibition of
HMGB1 (29,30). Therefore, the present study aimed
to investigate the effects of rosuvastatin in ADR-treated rats. The
results suggested that the protective effects of rosuvastatin may
be associated with a reduction of the HMGB1/RAGE-mediated
inflammatory response in rats treated with ADR.
Rosuvastatin is one of the most potent statins and
has well-established lipid-lowering effects in addition to
pleiotropic effects, including anti-inflammatory and endothelial
protective effects (31–33). Accordingly, the present study
showed improved biochemical indices and histopathology following
rosuvastatin treatment. These results are supported by previous
studies; Fei et al (34)
showed that rosuvastatin had protective effects on the risk of
acute myocardial injury through lowering of vascular endothelial
growth factor A. In addition, Kim et al (35) showed that rosuvastatin prevented
the long-term detrimental effects of ADR on left ventricular
function. Ke et al (30)
and Du et al (29) showed
that pre- and post-conditioning with rosuvastatin reduces
ischemia/reperfusion myocardial injury through the inhibition of
HMGB1. However, the direct effects of rosuvastatin on cardiac
function were not observed in the present study. This may be due to
the model itself or to the short treatment time. In addition, the
main effect of statins is to lower the blood cholesterol levels,
whereas their pleiotropic effects are secondary effects.
The present study revealed that rosuvastatin
significantly inhibited the expression of HMGB1 and RAGE. Xu et
al (36) showed that
atorvastatin inhibited the expression of RAGE in rat aortas, Yang
et al (20) showed that
statins decreased the activation of HMGB1, and Jin et al
(37) showed that atorvastatin
decreased the serum levels of HMGB1. HMGB1 binding to RAGE results
in the upregulation of proinflammatory cytokines, including TNF-α
and IFN-γ, following ADR injury (38). These results are supported by Gao
et al (39), who showed
that HMGB1 and RAGE mediated the overexpression of TNF-α, and by a
number of previous studies (40–42). Similar results have been obtained
for IFN-γ (43–45).
A previous study demonstrated that HMGB1-haptoglobin
β complexes binding to CD163 result in the release of
anti-inflammatory cytokines, including IL-10 in sterile and
infectious inflammation (38). In
addition, HMGB1 binding to RAGE results in anti-inflammatory
cytokines, including IL-4 and IL-10, being upregulated following
inflammatory injury (40,46,47). Du et al (29) showed that post-conditioning with
rosuvastatin decreased markers of oxidative stress in rats
following ischemia/reperfusion injury. In addition, Ke et al
(30) showed that preconditioning
with rosuvastatin decreased ischemia/reperfusion injury by reducing
the accumulation of inflammatory cells and regulatory T cells in
the heart, which is associated with increased production of
inflammatory cytokines, including TNF-α and IFN-γ, and dysregulated
anti-inflammatory cytokines, including IL-4 and IL-10 (48). In the present study, it was found
that the administration of rosuvastatin in the ADR-treated rats
inhibited the expression of HMGB1 and RAGE, in addition to the
decrease of TNF-α and IFN-γ and increase of IL-4 and IL-10.
Together, these results suggest that the activation of HMGB1/RAGE
by rosuvastatin may result in improved functional recovery.
However, additional investigations are necessary to examine the
effects of rosuvastatin on inflammatory cells, regulatory T cells,
and a comprehensive cytokine panel in ADR heart injury. In
addition, previous studies have shown that HMGB1 can activate the
phosphoinositide 3-kinase/Akt and TLR4/NF-κB pathways during heart
ischemia/reperfusion injury, high-lighting the role of HMGB1 in
heart injury (20,49–51). The effects of rosuvastatin on
pathways including PI3K/Akt and TLR4/NF-κB in the context of heart
injury also require investigation in the future.
The present study did not show that rosuvastatin
significantly improved left ventricular structure and function or
LVEF. This may be due to a number of reasons, including
administration time and dose of statin. It had been reported that
the improvement of LVEF by statins is time-dependent, and that
long-term treatment may be more beneficial in improving LVEF
(52). It was hypothesized that
changes in serological parameters and the expression of
inflammatory cytokines by rosuvastatin may occur ahead of changes
in myocardial tissue. Additional investigations are necessary to
address this issue.
The present study had certain limitations. There was
no statin-only group. However, previous studies have suggested that
treatment with statin alone did not differ significantly from the
control group in terms of the baseline blood biochemical indicators
(AST, ALT, and ALP), heart structure indicators (LVEF, LVFS, LVIDd,
and LVIDs), injury to other organs and tissues, and oxidative
stress indicators, including superoxide dismutase, malondialdehyde,
and catalase (53,54). Therefore, considering animal
protection, a statin-only group was not included in the present
study. In addition, only one dose of rosuvastatin was used,
however, preliminary experiments showed that 1.0 mg/kg/day led to
more significant improvement for myocardial dysfunction in the
ADR-treated rats compared to the other doses (0.1 and 5.0
mg/kg/day).
In conclusion, the present study suggested that ADR
can induce the expression of HMGB1 and RAGE in the myocardium of
ADR-treated rats, which can be inhibited by rosuvastatin. The
protective effects of rosuvastatin in ADR-treated rats may be
associated with the inhibition of HMGB1/RAGE pathway activation.
Despite this protective effect of rosuvastatin in the present
study, it did not improve cardiac function (LVIDd, LVIDs, LVEF, and
LVFS). Further investigation on the effects of rosuvastatin may
provide novel modalities for myocardial injury induced by ADR.
Funding
This study was supported by grants from the National
Natural Science Foundation of China (grant nos. 81270428, 81300999,
and 81470501).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors’ contributions
XL and HZ conceived the study and designed the
experiments. HZ, ZL and KD performed the experiments. HZ and ZL
collected and analyzed the experimental results. HZ wrote the
manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The experiments were performed in accordance with
the NIH Guide for the Care and Use of Laboratory Animals and were
approved by the Animal Care and Use Committee of Nanjing Medical
University.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Acknowledgments
The authors gratefully acknowledge Mrs. Ping Zhou
from the Department of Geriatrics (The Second Affiliated Hospital
of Nanjing Medical University, Nanjing, China) for her technical
assistance.
References
|
1
|
Christensen HM, Schou M, Goetze JP, Faber
J, Frystyk J, Flyvbjerg A and Kistorp C: Body mass index in chronic
heart failure: Association with biomarkers of neurohormonal
activation, inflammation and endothelial dysfunction. BMC
Cardiovasc Disord. 13:802013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kazymyrko VK, Kutovyi VV, Ivanyts’ka LM,
Dubkova AG and Silant’ieva TS: Biomarkers of iron metabolism and
inflammation in patients with chronic heart failure and various
types of left ventricular dysfunction (In Ukrainian). Lik Sprava.
19–22. 2013.
|
|
3
|
Ismahil MA, Hamid T, Bansal SS, Patel B,
Kingery JR and Prabhu SD: Remodeling of the mononuclear phagocyte
network underlies chronic inflammation and disease progression in
heart failure: Critical importance of the cardiosplenic axis. Circ
Res. 114:266–282. 2014. View Article : Google Scholar
|
|
4
|
Zykov KA, Tatenkulova SN, Masenko VP,
Kuznetsova TV, Rvacheva AV and Belenkov IuN: Characteristics of
autoimmune reactions in chronic cardiac failure of different
etiology (In Russian). Ter Arkh. 81:22–28. 2009.
|
|
5
|
Yamada S and Maruyama I: HMGB1, a novel
inflammatory cytokine. Clin Chim Acta. 375:36–42. 2007. View Article : Google Scholar
|
|
6
|
Bustin M and Reeves R: High-mobility-group
chromosomal proteins: Architectural components that facilitate
chromatin function. Prog Nucleic Acid Res Mol Biol. 54:35–100.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Park JS, Arcaroli J, Yum HK, Yang H, Wang
H, Yang KY, Choe KH, Strassheim D, Pitts TM, Tracey KJ, et al:
Activation of gene expression in human neutrophils by high mobility
group box 1 protein. Am J Physiol Cell Physiol. 284:C870–C879.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Scaffidi P, Misteli T and Bianchi ME:
Release of chromatin protein HMGB1 by necrotic cells triggers
inflammation. Nature. 418:191–195. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kostova N, Zlateva S, Ugrinova I and
Pasheva E: The expression of HMGB1 protein and its receptor RAGE in
human malignant tumors. Mol Cell Biochem. 337:251–258. 2010.
View Article : Google Scholar
|
|
10
|
Volz HC, Kaya Z, Katus HA and Andrassy M:
The role of HMGB1/RAGE in inflammatory cardiomyopathy. Semin Thromb
Hemost. 36:185–194. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Park JS, Svetkauskaite D, He Q, Kim JY,
Strassheim D, Strassheim D, Ishizaka A and Abraham E: Involvement
of toll-like receptors 2 and 4 in cellular activation by high
mobility group box 1 protein. J Biol Chem. 279:7370–7377. 2004.
View Article : Google Scholar
|
|
12
|
Zhang Q, O’Hearn S, Kavalukas SL and
Barbul A: Role of high mobility group box 1 (HMGB1) in wound
healing. J Surg Res. 176:343–347. 2012. View Article : Google Scholar
|
|
13
|
Li W, Sama AE and Wang H: Role of HMGB1 in
cardiovascular diseases. Curr Opin Pharmacol. 6:130–135. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ding HS and Yang J: High mobility group
box-1 and cardiovascular diseases. Saudi Med J. 31:486–489.
2010.PubMed/NCBI
|
|
15
|
Liu T, Zhang DY, Zhou YH, Han QF, Wang LH,
Wu L and Yao HC: Increased serum HMGB1 level may predict the fatal
outcomes in patients with chronic heart failure. Int J Cardiol.
184:318–320. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Volz HC, Laohachewin D, Schellberg D,
Wienbrandt AR, Nelles M, Zugck C, Kaya Z, Katus HA and Andrassy M:
HMGB1 is an independent predictor of death and heart
transplantation in heart failure. Clin Res Cardiol. 101:427–435.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Volz HC, Seidel C, Laohachewin D, Kaya Z,
Muller OJ, Pleger ST, Lasitschka F, Bianchi ME, Remppis A, Bierhaus
A, et al: HMGB1: The missing link between diabetes mellitus and
heart failure. Basic Res Cardiol. 105:805–820. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Blumenthal RS: Statins: Effective
antiatherosclerotic therapy. Am Heart J. 139:577–583. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Stalker TJ, Lefer AM and Scalia R: A new
HMG-CoA reductase inhibitor, rosuvastatin, exerts anti-inflammatory
effects on the microvascular endothelium: The role of mevalonic
acid. Br J Pharmacol. 133:406–412. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yang J, Huang C, Yang J, Jiang H and Ding
J: Statins attenuate high mobility group box-1 protein induced
vascular endothelial activation: A key role for TLR4/NF-kappaB
signaling pathway. Mol Cell Biochem. 345:189–195. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Han QF, Wu L, Zhou YH, Wang LH, Zhang DY,
Liu T and Yao HC: Simvastatin protects the heart against ischemia
reperfusion injury via inhibiting HMGB1 expression through PI3K/Akt
signal pathways. Int J Cardiol. 201:568–569. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Jones SP, Gibson MF, Rimmer DM III, Gibson
TM, Sharp BR and Lefer DJ: Direct vascular and cardioprotective
effects of rosuvastatin, a new HMG-CoA reductase inhibitor. J Am
Coll Cardiol. 40:1172–1178. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hauck L, Stanley-Hasnain S, Fung A, Grothe
D, Rao V, Mak TW and Billia F: Cardiac-specific ablation of the E3
ubiquitin ligase Mdm2 leads to oxidative stress, broad
mitochondrial deficiency and early death. PLoS One.
12:e01898612017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2−ΔΔCT method. Methods. 25:402–408. 2001. View Article : Google Scholar
|
|
25
|
Rabelo E, De Angelis K, Bock P, Gatelli
Fernandes T, Cervo F, Belló Klein A, Clausell N and Cláudia
Irigoyen M: Baroreflex sensitivity and oxidative stress in
adriamycin-induced heart failure. Hypertension. 38:576–580. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Zhu Z and Fang Z: Statin protects
endothelial cell against ischemia reperfusion injury through
HMGB1/TLR4 pathway. Int J Cardiol. 203:742016. View Article : Google Scholar
|
|
27
|
Haraba R, Suica VI, Uyy E, Ivan L and
Antohe F: Hyperlipidemia stimulates the extracellular release of
the nuclear high mobility group box 1 protein. Cell Tissue Res.
346:361–368. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Prasad K: Do statins have a role in
reduction/prevention of post-PCI restenosis. Cardiovasc Ther.
31:12–26. 2013. View Article : Google Scholar
|
|
29
|
Du X, Hu X and Wei J: Postconditioning
with rosuvastatin reduces myocardial ischemia-reperfusion injury by
inhibiting high mobility group box 1 protein expression. Exp Ther
Med. 7:117–120. 2014. View Article : Google Scholar
|
|
30
|
Ke D, Fang J, Fan L, Chen Z and Chen L:
Regulatory T cells contribute to rosuvastatin-induced
cardioprotection against ischemia-reperfusion injury. Coron Artery
Dis. 24:334–341. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Shen Ma, Liu DW, Pan J, Yu J, Shi L, Deng
W, Zhu L, Yang L, Liu FJ, et al: Statin function as an
anti-inflammation therapy for depression in patients with coronary
artery disease by downregulating interleukin-1beta. J Cardiovasc
Pharmacol. 67:129–135. 2016. View Article : Google Scholar
|
|
32
|
Greque GV, Serrano CV Jr, Strunz CM,
Soeiro A, Santos M, Pivateli F, Jacob JL, Pesaro AE, Nicolau JC and
Kalil-Filho R: Preprocedural statin therapy, inflammation, and
myocardial injury in low-risk stable coronary artery disease
patients submitted to coronary stent implantation. Catheter
Cardiovasc Interv. 87:222–229. 2016. View Article : Google Scholar
|
|
33
|
Bonsu KO, Reidpath DD and Kadirvelu A:
Effects of statin treatment on inflammation and cardiac function in
heart failure: An adjusted indirect comparison meta-analysis of
randomized trials. Cardiovasc Ther. 33:338–346. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Fei L, Zhang J, Niu H, Yuan C and Ma X:
Effects of rosuvastatin and MiR-126 on myocardial injury induced by
acute myocardial infarction in rats: Role of vascular endothelial
growth factor A (VEGF-A). Med Sci Monit. 22:2324–2334. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Kim YH, Park SM, Kim M, Kim SH, Lim SY,
Lim SY, Ahn JC, Song WH and Shim WJ: Cardioprotective effects of
rosuvastatin and carvedilol on delayed cardiotoxicity of
doxorubicin in rats. Toxicol Mech Methods. 22:488–498. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Xu L, Zang P, Feng B and Qian Q:
Atorvastatin inhibits the expression of RAGE induced by advanced
glycation end products on aortas in healthy Sprague-Dawley rats.
Diabetol Metab Syndr. 6:1022014. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Jin D, Wu Y, Zhao L, Guo J, Zhang K and
Chen Z: Atorvastatin reduces serum HMGB1 levels in patients with
hyperlipidemia. Exp Ther Med. 4:1124–1126. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Yang H, Wang H, Wang Y, Addorisio M, Li J,
Postiglione MJ, Chavan SS, Al-Abed Y, Antoine DJ, Andersson U, et
al: The haptoglobin beta subunit sequesters HMGB1 toxicity in
sterile and infectious inflammation. J Intern Med. 282:76–93. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Gao XJ, Qu YY, Liu XW, Zhu M, Ma CY, Jiao
YL, Cui B, Chen ZJ and Zhao YR: Immune complexes induce TNF-alpha
and BAFF production from U937 cells by HMGB1 and RAGE. Eur Rev Med
Pharmacol Sci. 21:1810–1819. 2017.PubMed/NCBI
|
|
40
|
Kokkola R, Andersson A, Mullins G, Ostberg
T, Treutiger CJ, Arnold B, Nawroth P, Andersson U, Harris RA and
Harris HE: RAGE is the major receptor for the proinflammatory
activity of HMGB1 in rodent macrophages. Scand J Immunol. 61:1–9.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Andersson U and Tracey KJ: HMGB1 is a
therapeutic target for sterile inflammation and infection. Annu Rev
Immunol. 29:139–162. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Luan ZG, Zhang H, Yang PT, Ma XC, Zhang C
and Guo RX: HMGB1 activates nuclear factor-kappaB signaling by RAGE
and increases the production of TNF-alpha in human umbilical vein
endothelial cells. Immunobiology. 215:956–962. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Dumitriu IE, Baruah P, Bianchi ME,
Manfredi AA and Rovere-Querini P: Requirement of HMGB1 and RAGE for
the maturation of human plasmacytoid dendritic cells. Eur J
Immunol. 35:2184–2190. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Saidi H, Bras M, Formaglio P, Melki MT,
Charbit B, Herbeuval JP and Gougeon ML: HMGB1 is involved in
IFN-alpha production and TRAIL expression by HIV-1-exposed
plasmacytoid dendritic cells: Impact of the crosstalk with NK
cells. PLoS Pathog. 12:e10054072016. View Article : Google Scholar
|
|
45
|
Sirois CM, Jin T, Miller AL, Bertheloot D,
Nakamura H, Horvath GL, Mian A, Jiang J, Schrum J, Bossaller L, et
al: RAGE is a nucleic acid receptor that promotes inflammatory
responses to DNA. J Exp Med. 210:2447–2463. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Huang LF, Yao YM, Zhang LT, Dong N, Yu Y
and Sheng ZY: The effect of high-mobility group box 1 protein on
activity of regulatory T cells after thermal injury in rats. Shock.
31:322–329. 2009. View Article : Google Scholar
|
|
47
|
Dumitriu IE, Baruah P, Valentinis B, Voll
RE, Herrmann M, Nawroth PP, Arnold B, Bianchi ME, Manfredi AA and
Rovere-Querini P: Release of high mobility group box 1 by dendritic
cells controls T cell activation via the receptor for advanced
glycation end products. J Immunol. 174:7506–7515. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Liu J, Wang H and Li J: Inflammation and
inflammatory cells in myocardial infarction and reperfusion injury:
A double-edged sword. Clin Med Insights Cardiol. 10:79–84. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Wu B, Su Z, Lin R, Dai R, Chen C and Wu H:
Short-time pretreatment of rosuvastatin attenuates myocardial
ischemia and reperfusion injury by inhibiting high mobility group
box 1 protein expression. Int J Cardiol. 168:4946–4948. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Hu X, Xu C, Zhou X, Cui B, Lu Z and Jiang
H: PI3K/Akt signaling pathway involved in cardioprotection of
preconditioning with high mobility group box 1 protein during
myocardial ischemia and reperfusion. Int J Cardiol. 150:222–223.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Ding HS, Yang J, Gong FL, Yang J, Ding JW,
Li S and Jiang YR: High mobility group [corrected] box 1 mediates
neutrophil recruitment in myocardial ischemia-reperfusion injury
through toll like receptor 4-related pathway. Gene. 509:149–153.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Wang JQ, Wu GR, Wang Z, Dai XP and Li XR:
Long-term clinical outcomes of statin use for chronic heart
failure: A meta-analysis of 15 prospective studies. Heart Lung
Circ. 23:105–113. 2014. View Article : Google Scholar
|
|
53
|
Henninger C, Huelsenbeck S, Wenzel P,
Brand M, Huelsenbeck J, Schad A and Fritz G: Chronic heart damage
following doxorubicin treatment is alleviated by lovastatin.
Pharmacol Res. 91:47–56. 2015. View Article : Google Scholar
|
|
54
|
Mansouri E, Jangaran A and Ashtari A:
Protective effect of pravastatin on doxorubicin-induced
hepatotoxicity. Bratisl Lek Listy. 118:273–277. 2017.PubMed/NCBI
|