Introduction
Knee osteoarthritis affects millions of people
worldwide (1). It is mainly
characterized by cartilage lesions, subchondral bone sclerosis and
aseptic inflammation of the synovium (2). Previous studies have identified that
the pathogenesis of osteoarthritis (OA) is initially caused by
structural modification in the subchondral bone in response to
changes in the mechanical environment (3-5).
It has also been reported that subchondral bone of OA shows
dysregulated bone modified by osteoblast and osteoclast activity
(6), finally resulting in the
formation of sclerosis (7).
Transforming growth factor β (TGFβ), canonically
binds to its cell surface receptor and then directly phosphorylates
Smad2/3 to translocate the signaling molecule into the nucleus and
interact with other transcriptional factors, playing an important
role in the development of OA (8-13).
However, the effect of TGFβ on OA varies depending on the sites it
acts on. Regarding cartilage, the inhibition of TGFβ1 in
chondrocytes could decrease the expression of collagen and
proteoglycans in developing knee joints (14-16), suggesting that TGFβ1 might be a
therapeutic agent for OA. Conversely, in adult knee joints,
chondrocyte TGFβ1 could induce extracellular matrix-degrading
enzymes (17). Yet, in the
subchondral bone of OA, a large amount of TGFβ was activated in the
extracellular matrix (8).
Moreover, it has been suggested that osteoblastic TGFβ signaling in
subchondral bone might play an important role in the pathogenesis
of OA by altering mesenchymal stem cell (MSC) osteogenic activity
(9).
Several studies have emphasized that osteocytes play
an important regulatory role in maintaining bone metabolism
(18,19). It has been found that osteocytes,
the most abundant mechanosensory cells, are involved in
loading-increased anabolism of cortical bone via inhibition of the
TGFβ-Smad2/3 pathway (20).
Moreover, osteocyte morphology in OA has been found to be altered,
exhibiting rough and rounded cell bodies with fewer and
disorganized dendrites (21). A
dysregulated expression of the osteocyte markers (22), apoptosis (23), and degradative enzymes (24) was also observed in OA.
Although osteocytes have been identified to play
vital roles in OA development, it is unclear how osteocytes respond
to abnormally activated TGFβ in the extracellular matrix of
osteochondral bone in the late OA. Therefore, the aim of the
present study was to explore the association between osteocyte TGFβ
signaling and the remodeling of the subchondral bone in relation to
different cartilage damage, which will lay the foundation for
further research on the role of osteocyte TGFβ signaling in OA.
Materials and methods
Patients
Chinese patients who had undergone total knee
arthroplasty due to OA rather than rheumatoid arthritis, included 7
males and 13 females (21 knees), with an average age of 68 years
(age range, 60-78 years). The mean body mass index of males and
females was 25.18±1.81 and 26.34±2.05, respectively. A total of 21
tibial plateau specimens were collected from The First Affiliated
Hospital of Chongqing Medical University (Chongqing, China) between
May 2018 and May 2019 (Table I).
Standard surgical procedures were performed during knee
arthroplasty and specimen collection did not involve any clinical
intervention. The collection of human specimens and animal
experiments in the present study were approved by the Ethics
Committee of the First Affiliated Hospital of Chongqing Medical
University (Permit number: 2015-316), under which the effect of
Smad7 on chondrogenesis and endochondral ossification (25), osteocyte TGFβ-Smad4 on
osteoblastic and osteoclastic differentiation (26) had been previously have identified.
Written informed consent was obtained from participants.
 | Table IBasic characteristics of
participants. |
Table I
Basic characteristics of
participants.
| Gender | Population | Right knee | Left knee | BMI | Joint instability
historya |
|---|
| Male | 7 | 5 | 2 | 25.18±1.81 | 4 |
| Female | 13 | 8 | 6 | 26.34±2.05 | 7 |
Specimen collection and processing
The tibial plateaus of patients were removed during
surgery and rapidly transferred to the laboratory at on-ice. After
collecting gross images, the tibial plateaus were aseptically cut
into pieces of ~0.5x0.5x0.2 cm using bone scissors. The areas of
cartilage wear were divided into full cartilage, partial cartilage
and full defect groups. Specimens were radiographed using a bone
density instrument (kubtecNC), 50% of which then underwent RNA and
protein isolation and the other half of which was soaked in 4%
paraformaldehyde at room temperature for 24 h, decalcified in 10%
EDTA for 3 weeks, dehydrated in graded alcohol, embedded and cut
into 5-mm thick sections.
Bone mineral density (BMD) analysis
Small pieces of specimens were radiographed using a
kubtecNC instrument with automatic exposure at 45 KV, 500 mA. The
BMD of the subchondral bone area was measured and analyzed using
kubtec Digicom BMD Processor.
Hematoxylin and eosin (H&E) and
safranin O staining H&E staining
Paraffin sections were baked at 59°C for 30 min,
dewaxed in xylene and hydrated in a series of gradient alcohol,
followed by immersion in hematoxylin dye solution at room
temperature for 5 min to stain the nuclei, in hydrochloric acid for
5 sec for differentiation, and in lithium carbonate to blue the
nuclei. They were then immersed in eosin at room temperature for 5
min to stain the cytoplasm. Finally, once they were dehydrated and
transparent, they were sealed with resin.
Safranin O staining
Slices were baked, dewaxed and hydrated as
previously described. Next, they were immersed in freshly prepared
Weigert stain for 5 min, differentiated in acid for 15 sec and
immersed in the green staining solution for 5 min and in the
Safranin O dye solution for 5 min at room temperature, according to
the manufacturer's protocol (G1371; Beijing Solarbio Science &
Technology Co., Ltd.). They were then washed with a weak acid
solution for 30 sec to remove the remaining solid green. Finally,
once they were dehydrated and transparent, they were sealed with
resin.
Immunohistochemistry
Sections were baked, dewaxed and hydrated as
previously described. The antigen was then repaired by proteinase K
(0.3 mg/ml; Merck KGaA) treatment at 37°C for 30 min. Endogenous
enzyme activity was extinguished using 3% hydrogen peroxide for 10
min. Slices were blocked with goat serum (cat. no. 5425; Cell
Signaling Technology, Inc.) at 37°C for 1 h and incubated with
primary antibody overnight at 4°C [rabbit anti-TGFβ1, cat. no.
3709, 1:100; rabbit anti-phosphorylated (p)-Smad2/3, cat. no.
#8828S, 1:200; Cell Signaling Technology, Inc.; rabbit anti-a
disintegrin and metalloproteinase with thrombospondin motifs 4
(Adamts4), cat. no. #ab185722, 1:200; Abcam], incubated with
secondary antibody for 1 h at room temperature [horseradish
peroxidase (HRP)-conjugated goat anti-rabbit secondary antibody,
cat. no. #7074, 1:1,000; Cell signaling Technology, Inc.; goat
anti-rabbit lgG/Cy3, cat. no. bs-0295G-Cy3; 1:1,000; Bio-synthesis
Inc.]. 3′-Diaminobenzidine (DAB, Bio-synthesis Inc.) was added for
5 min and then 4′, 6-diamidino-2-phenylindole or hematoxylin was
used to counterstain the nuclei at room temperature for 5 min. The
slides were observed under a light or fluorescence microscope
(magnification, ×40, ×100 or ×200).
RT-qPCR
Subchondral bones from human knees were ground
within liquid nitrogen. Next, total RNA extraction was performed
using TRIzol (Thermo Fisher Scientific, Inc.) and reverse
transcribed into cDNA with PrimeScript RT Reagent kit (Takara Bio,
Inc.) with the following conditions: 37°C for 15 min and 85°C for 5
sec. qPCR analysis of alkaline phosphatase (ALP), osteopontin (OPN)
and osteocalcin (OCN) mRNA was performed using the CFX96 Real time
PCR Detection system (Bio-Rad Laboratories, Inc.) with SYBR Premix
Ex Taq II (Takara Bio, Inc.). The thermocycling conditions of qPCR
were as follows: 95°C for 30 sec; and 40 cycles of 95°C for 5 sec
and 60°C for 5 sec. GAPDH was used as a reference gene. All sample
values were normalized to GAPDH expression using the
2−ΔΔCq method as described previously (27). The qPCR primer sequences were as
follows: ALP forward, 5′-ACA CCA ATG TAG CCA AGA ATG TCA-3′ and
reverse, 5′-GAT TCG GGC AGC AGC GGT TAC T-3; OPN forward, 5′-ACA
CTT TCA CTC CAA TCG TCC-3′ and reverse, 5′-TGC CCT TTC CGT TGT TGT
CC-3′; OCN forward, 5′-CAG CGG CCC TGA GTC TGA-3′ and reverse,
5′-GCC GGA GTC TGT TCA CTA CCT TA-3′; and Gapdh forward, 5′-CTA CAC
TGA GGA CCA GGT TGT CT-3′ and reverse, 5′-TTG TCA TAC CAG GAA ATG
AGC TT-3′.
Isolation and co-culture mouse osteocytes
and bone marrow stromal cells (BMSCs)
Mice were sacrificed by cervical dislocation after
inhaling 2.5% concentration of isoflurane (RWD Life Science Co.,
Ltd.) and all efforts were made to minimize the suffering of the
animals included in present study. Death was confirmed when the
mice were ceased breathing and had no heartbeat and dilated pupils.
The tibial and femoral diaphyses were dissected from 5, 10-week-old
mice, cut into 1-2-mm pieces, and incubated in collagenase type I
and EDTA 9 times, as previously described (28). Next, primary mouse osteocytes were
cultured in α-minimal essential medium (Thermo Fisher Scientific,
Inc.) supplemented with 10% fetal bovine serum (TBD0130HYT;
Tianjing TBD Science Co., Ltd.), 1% penicillin and streptomycin (GE
Healthcare Life Sciences), and 50 µM β-Mercaptoethanol (Merck
KGaA). Next, osteocytes were digested with trypsin and seeded at a
density of ~40,000 cells per well (24 well plate; Wuxi Nest Biology
& Technology Co., Ltd.), and TGFβ1 protein (PeproTech, Inc.) or
LY2109761 (MedChemExpress, Inc.) was added for 1 h, prior to
co-culture with wild-type mouse BMSCs flushed from the femur and
tibia. The method of isolating mouse bone marrow cells was
previously described (29).
Alkaline phosphatase (ALP) and tartrate
resistant acid phosphatase (TRAP) staining
The co-cultured mouse cells were fixed with 4%
paraformaldehyde at room temperature for 10 min and the dye
solution was added following the manufacturer's protocol of ALP
(catalog no. C3206; Beyotime Institute of Biotechnology) and TRAP
(catalog no. 387; Sigma-Aldrich; Merck KGaA) staining kits.
ALP-stained cells were incubated at room temperature for 30 min and
TRAP-stained cells at 37°C for 1 h.
Western blotting
Protein extraction from mouse osteocytes and human
knee subchondral bone was performed using 2% SDS lysis buffer
containing 100 mM Tris-HCL and 100 mM β-Mercaptoethanol. Total
protein was determined using a BCA protein Assay kit (Beyotime
Institute of Biotechnology). Total protein (20 µg) was
electrophoresed on 5-10% Bis-Tris gels (Thermo Fisher Scientific,
Inc.) and transferred to polyvinylidene fluoride membranes (EMD
Millipore). Membranes were blocked with 5% skimmed milk for 1 h at
room temperature and incubated with primary antibodies against
p-Smad2/3, Smad2 and β-actin (rabbit anti-p-Smad2/3, cat. no.
#8828S; 1:1,000; rabbit anti-Smad2; cat. no. #5339; 1:1,000; rabbit
anti-β-actin; cat. no. #4970, 1:1,000; Cell signaling Technology,
Inc.) overnight at 4°C, followed by incubation with corresponding
HRP-conjugated secondary antibody (goat anti-rabbit secondary
antibody, cat. no. #7074, 1:1,000; Cell Signaling Technology, Inc.)
at room temperature for 1 h. The blots were visualized using
Immobilon Western Chemiluminescent HRP Substrate (EMD Millipore)
and analyzed by Image Lab 6.0.1. software (Bio-Rad Laboratories,
Inc.).
Image and statistical analysis
All images were obtained using a light or
fluorescence microscope (Olympus Corporation) and analyzed by Image
J Pro (National Institutes of Health; version 1.50 g). Data are
expressed as the mean ± standard deviation and analyzed with SPSS
software (version 21; IBM, Corp.). One-way analysis of variance
followed by Student-Newman Keuls post hoc test was performed to
analyze inter- and intra-group differences. A t-test was used to
compare two groups. The correlations between osteocyte p-Smad2/3
expression and other bone turnover parameters were calculated with
Pearson's correlation coefficients. P<0.05 was considered to
indicate a statistically significant difference.
Results
Increased sclerosis of subchondral bone
underneath the eroding cartilage
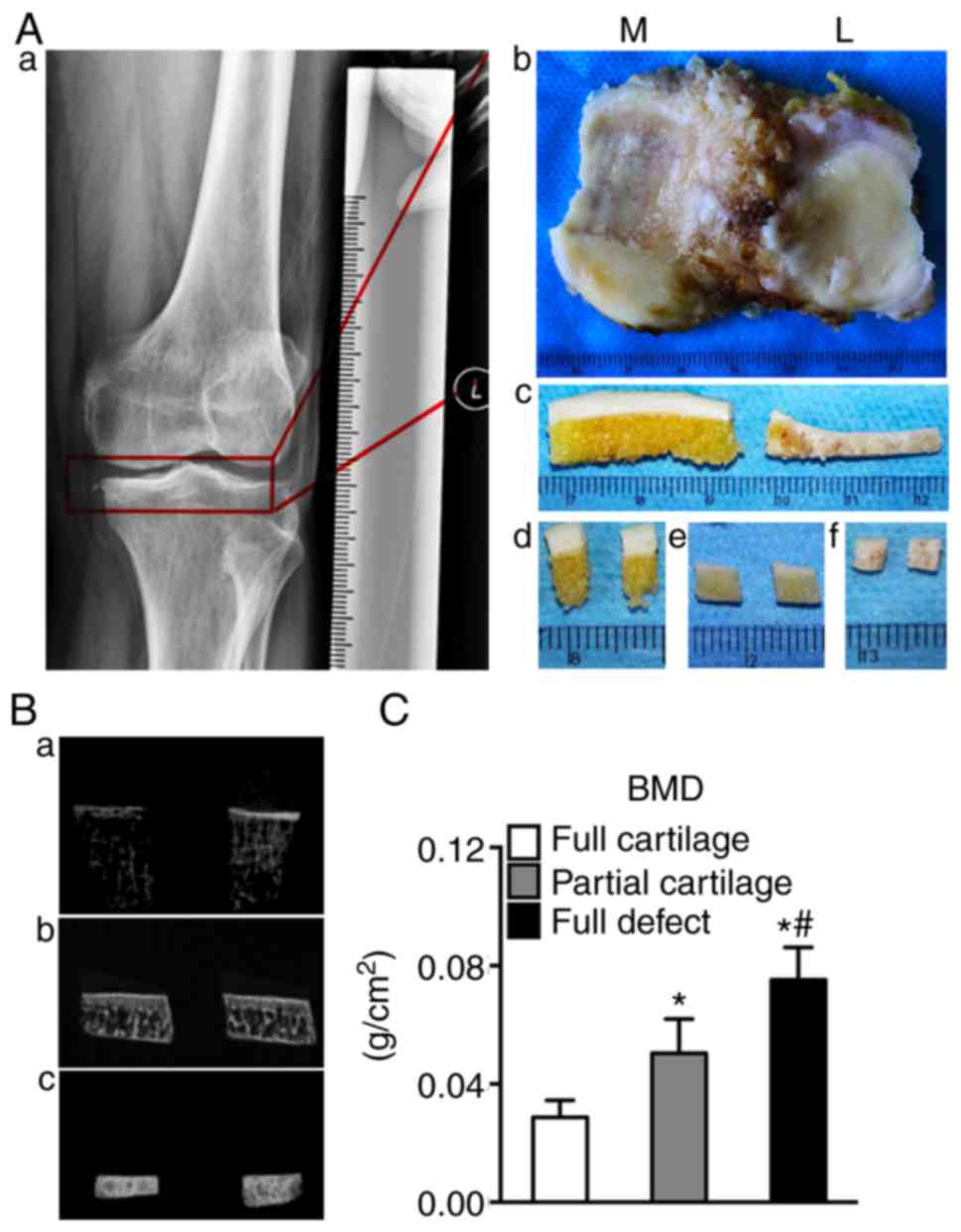
The degrees of cartilage degeneration were distinct
in the medial and lateral plateaus, especially when it came to 67%
(14:21) of patients with valgus and varus deformities. The tibial
plateaus of human with 'normal' cartilage had a milky color and
smooth surface, with mild cartilage degeneration showing as
yellowish and coarse surface, and severe degeneration as a full
thickness cartilage defect, sclerotic subchondral bone and
extensive fractures (Fig. 1A).
Next, the alternation of sclerosis in subchondral bone was
confirmed by BMD assay and sclerosis was shown to increase with the
increasing cartilage erosion severity (0.029±0.006 vs. 0.050±0.012
vs. 0.075±0.011; respectively; P<0.05; Fig. 1B and C).
Altered structure of subchondral bone
underneath the worn cartilage
The structural changes in the subchondral bone from
human knees were further examined (Fig. 2Ba-c). It was found that, along
with elevated cartilage defects, the bone volume/total tissue
volume ratio (BV/TV) was also increased (0.24±0.08 vs. 0.49±0.24
vs. 0.73±0.17; P<0.05). The thickness of the subchondral bone
plate (SBP Th.) was significantly increased in the partial
cartilage group compared with that in the full cartilage (0.80±0.07
vs. 0.13±0.04; P<0.05) and full defect groups. There was a
significant decrease in the partial cartilage group compared with
the full defect group (2.11±0.37 vs. 0.13±0.04; P<0.05).
Similarly, the thickness of the calcified cartilage (CC Th.) in the
partial cartilage group was increased compared with that in the
full cartilage group (0.16±0.06 vs. 0.11±0.06; P<0.05). In
addition, the bone marrow cavity was mainly filled with adipocytes
in 'normal' subchondral bone (black arrow), which were gradually
replaced with bone marrow cells, in which some new trabecular bone
(blue arrow) was formed locally (Fig.
2Aa-f). These results indicated that the more obvious the
cartilage destruction, the more severe the subchondral bone
structure changes, eventually leading to the formation of
subchondral bone sclerosis.
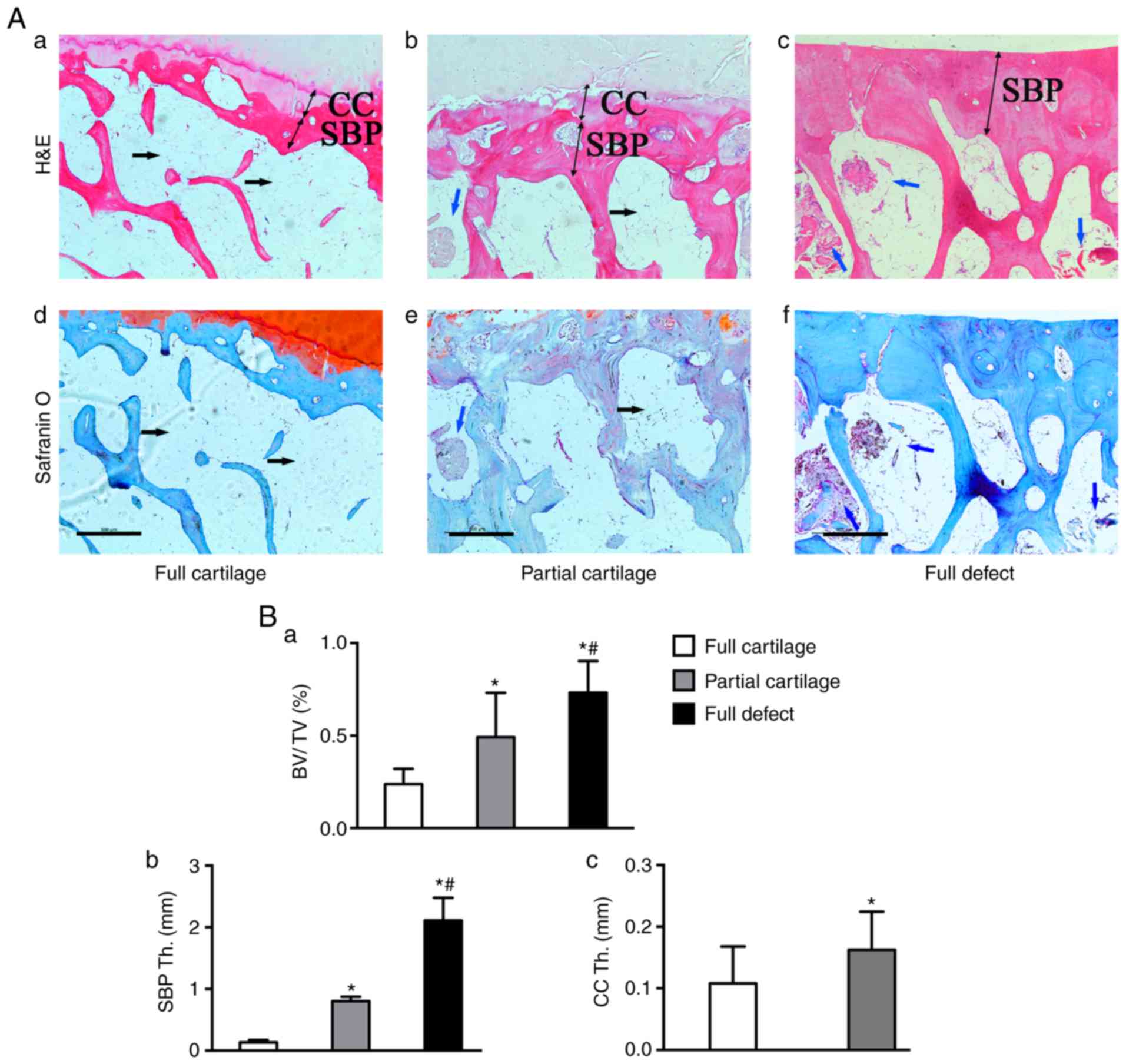 | Figure 2Alternation of the microstructure in
subchondral bone from human knee. (A) H&E staining of the (a)
full, (b) partial cartilage and (c) full defect. (Ad-f) Safranin
O/fast green staining in (d) full, (e) partial cartilage and (f)
full defect groups. In the full cartilage group, the bone marrow
cavity was mainly filled with adipose tissue (black arrow), but in
the partial cartilage and especially in full defect groups, it was
composed of bone marrow cells (blue arrow), in which new trabecular
bone formed locally (red color in H&E and blue in safranin O
staining). Quantitative results showing that subchondral bone
possesses a (Ba) higher BV/TV fraction, (Bb) SBP Th. and CC Th. in
cartilage wear groups, as compared with (Bc) the full cartilage
group. *P<0.05 vs. the full cartilage and
#P<0.05 vs. the partial cartilage groups, n=21. Scale
bar, 500 µm. H&E, hematoxylin and eosin; BV/TV, Bone
volume/total tissue volume; CC Th., Thickness of calcified
cartilage; SBP Th., Thickness of subchondral bone plate. |
Turnover of osteogenic and osteoclastic
activities of the subchondral bone significantly increases with the
increasing severity of OA
To explore the causes leading to structural changes
in subchondral bone, the metabolic parameters of the bone were
detected. It was found that, even in the full cartilage group, some
bone islands had begun to form locally in the calcified cartilage
zone and proteoglycans in the surrounding cartilage matrix were
gradually lost (Fig. 3Aa-c).
Moreover, chondrocytes degenerated more severely in the partial
cartilage group, multiple cell clusters developed and were sparsely
distributed, and more proteoglycans were lost (Fig. 3Ad-f).
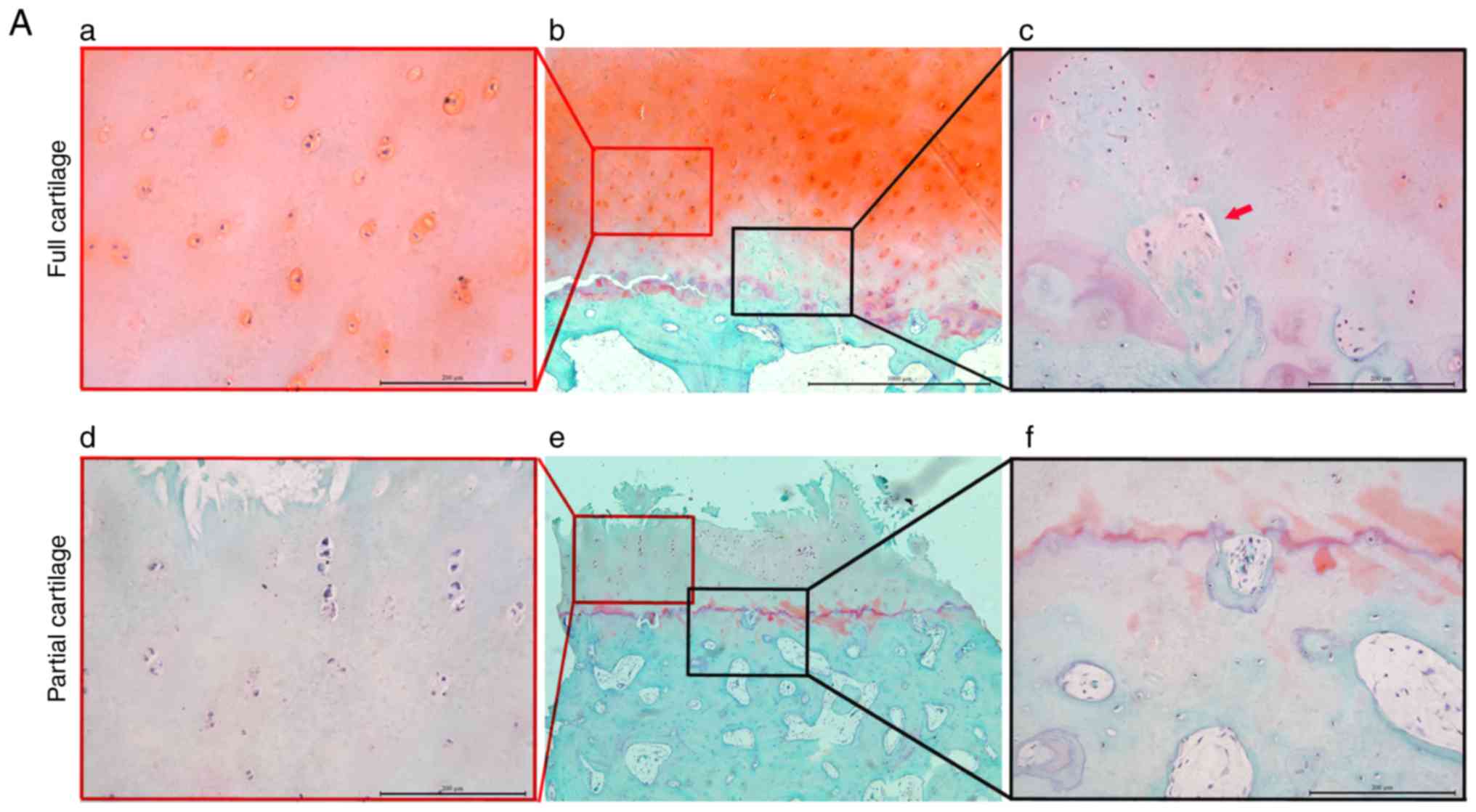 | Figure 3Turnover of osteogenic and
osteoclastic activities in subchondral bone from human knee.
Safranin O/fast green staining for architecture alternation in the
(Ab) full and (Ae) partial cartilage groups. Alternation in the
architecture of (Aa and d) cartilage and bone island (red arrow)
formation (Ac and f) locally at the calcified cartilage zone. (B)
The expression of osteogenic markers (a) ALP, (b) OPN and (c) OCN
in subchondral bone was analyzed by reverse
transcription-quantitative PCR. Bone resorption in subchondral bone
was assayed by (C) TRAP stain and positive cells were stained red
(blue arrow). (D) Quantitative analysis was performed by counting
TRAP+ cells per horizon. *P<0.05 vs. the
full cartilage and #P<0.05 vs. the partial cartilage
groups, respectively, n=21. Scale bar in Ab and e, 1,000 µm and in
others, 200 µm. TRAP, tartrate resistant acid phosphatase; ALP,
alkaline phosphatase; OPN, osteopontin; OCN, osteocalcin. |
The mechanism that leads to subchondral bone
sclerosis was further explored. The mRNA expression of the
osteogenic marker ALP and OPN (Fig.
3Ba and b) in the subchondral bone increased significantly with
the severity of cartilage defects (1.41±1.77 vs. 3.68±3.63 vs.
6.69±4.30; P<0.05; 0.19±0.09 vs. 0.34±0.31 vs. 0.57±0.26;
P<0.05). However, the expression of OCN mRNA (Fig. 3Bc) was only increased in the
partial cartilage and full defect groups, as compared with the full
cartilage group (0.35±0.18, 0.37±0.26 vs. 0.22±0.16; P<0.05),
but there was no significant difference between the full defect
group and the partial cartilage group (0.37±0.26 vs. 0.35±0.18;
P=0.74). Similarly, it was found that the number of
TRAP+ cells per horizon in both the partial cartilage
and full defect groups was significantly increased compared with
that in the full cartilage group (1.06±0.76, 7.48±1.80 vs.
4.37±1.34; P<0.05), but in the full defect group it was
decreased compared with that in the partial cartilage group
(4.37±1.34 vs. 7.48±1.80, P<0.05) (Fig. 3C and D). These results indicated
that abnormal knee joint stress can significantly enhance the
turnover of the osteogenic and osteoclastic activity in the
subchondral bone, and that subchondral bone sclerosis occurs to
cope with the abnormal mechanical loading.
Activation of osteocyte TGFβ signaling in
subchondral bone underneath the partial and full defect
cartilage
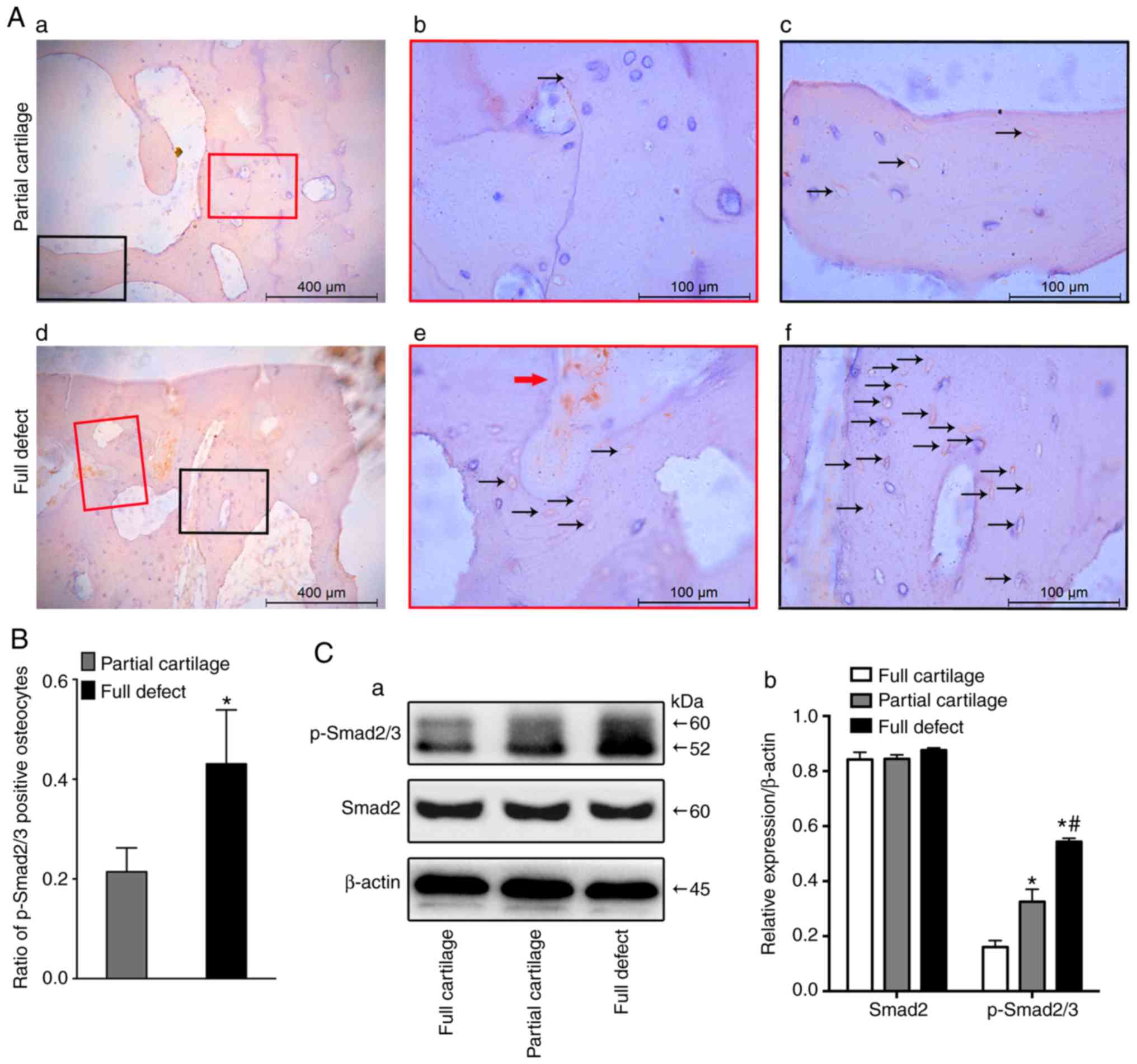
In order to investigate whether osteocyte TGFβ
signaling is activated in subchondral bone throughout the
development of human OA, the expression of activated TGFβ1 in three
different groups was first examined. The results showed that the
higher the degree of cartilage defect, the higher the expression of
activated TGFβ1 in the subchondral bone marrow matrix (Fig. S1). Furthermore, the activation of
the TGFβ signaling pathway was detected with immunohistochemistry
(Fig. 4A). Results showed that a
much higher number of p-Smad2/3+ osteocytes existed in
the full defect group, compared with the partial cartilage group
(0.43±0.11 vs. 0.21±0.05; P<0.001; Fig. 4B). It was also found that the
osteocyte TGFβ signaling pathway was activated in an osteoarthritic
mouse model by excising the anterior cruciate ligament (data not
shown). Consistent with a previous result (9), the TGFβ signaling pathway of bone
marrow stromal cells (red arrow) was also activated in the
subchondral bone of human osteoarthritic specimens (Fig. 4Ad and e). Furthermore, the western
blotting results for p-Smad2/3 showed that, as the degree of
cartilage erosion increased, the activation of the TGFβ signal
pathway in subchondral bone became more obvious (Fig. 4Ca and b).
Occasionally, it was observed that the activated
p-Smad2/3 of chondrocytes in the full cartilage group was mainly
located at the hypertrophic zone (Fig. S2Aa-c). However, the activated
p-Smad2/3 was activated throughout the layers in the partial
cartilage group (Fig. S2Ad-f).
Mechanistically, the expression of chondrocyte matrix-degrading
enzymes is the main manifestation of articular cartilage
degeneration (30,31). Therefore, the expression of
Adamts4, an important cartilage matrix-degrading enzyme, was then
examined in the cartilage, in the partial and full cartilage
groups. Of note, the expression of chondrocyte Adamts4 in the
partial cartilage group showed the same trend as that of p-Smad2/3
(Fig. S2B). These results
indicated that abnormal TGFβ may be correlated with the occurrence
of OA.
Association between osteocyte p-Smad2/3
and BMD, osteogenic markers, and TRAP+ cells in
subchondral bone
Pearson's correlation analysis revealed that the
ratios of p-Smad2/3+ osteocytes were positively
correlated with subchondral BMD, ALP and OPN mRNA expression,
suggesting that osteocyte p-Smad2/3 activation in subchondral bone
was positively associated with the severity of OA (Fig. 5Aa-c, Table II). However, it was negatively
correlated with TRAP+ cells (Fig. 5Ad, Table II). To further verify the role of
osteocyte TGFβ signaling, mouse osteocytes were isolated and
purified in vitro and co-cultured with mouse bone marrow
MSCs. TGFβ1 protein or the selective inhibitor of TGFβ receptor
type 1/2 (LY2109761) was added prior to co-culture with MSCs to
activate or inhibit the TGFβ signaling pathway in osteocytes,
respectively (Fig. 5Ba and b). It
was found that the exogenously over-activated TGFβ-Smad2/3
signaling in osteocytes could enhance the expression of ALP in bone
marrow stromal cells (Fig. 5Cb)
and promote the formation of TRAP+ cells (Fig. 5Ce). In addition, the inhibition of
its TGFβ signaling pathway can suppress the basal osteogenic and
osteoclastic promoting effects (Fig.
5Cc and f).
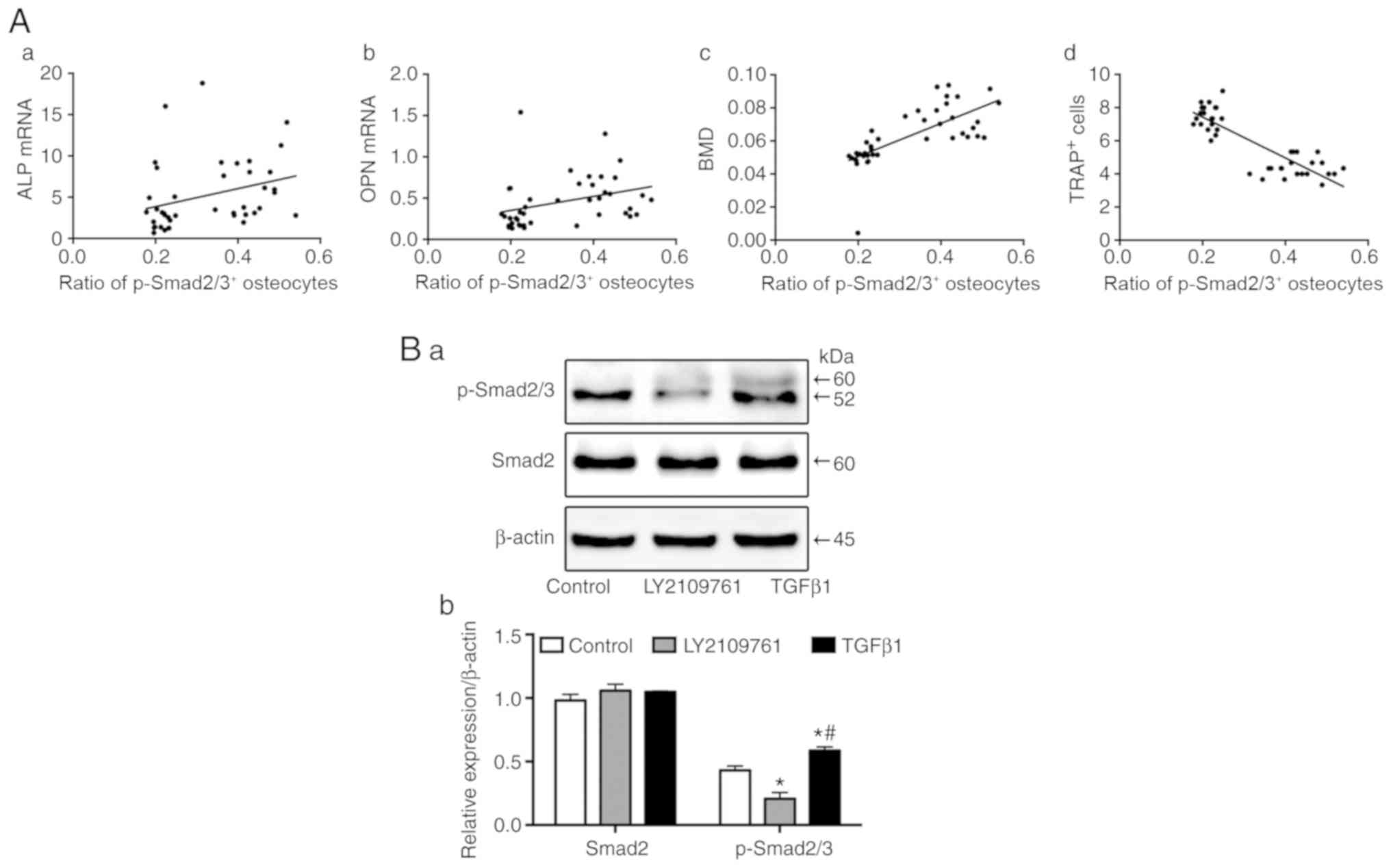 | Figure 5Association between
p-Smad2/3+ osteocytes and bone turnover states. Scatter
plot diagrams of the association between the ratio of
p-Smad2/3+ osteocytes and (Aa) ALP mRNA, (Ab) OPN mRNA,
(Ac) BMD of human subchondral bone, and (Ad) TRAP+ cells
in the partial cartilage and full defect groups. Exogenous TGFβ1
protein and the selective inhibitor of TGFβ receptor type 1/2
(LY2109761) respectively activated and inhibited the expression of
p-Smad2/3 in mouse osteocytes in vitro, as compared with the
control group using (Ba) western blotting and (Bb) its quantitative
analysis. ALP staining and TRAP staining assays were performed in
the (Ca and d) control, (Cb and e) osteocyte TGFβ1 overexpression
and (Cc and f) osteocyte TGFβ inhibited co-cultured groups. The
results showed that (Cb and e) p-Smad2/3+ osteocytes
promoted mouse MSCs osteogenic and osteoclastic differentiation,
(Cc and f) while p-Smad2/3- mouse osteocytes suppressed
them when co-cultured for 11 days. *P<0.05 vs. the
control and #P<0.05 vs. the LY2109761 groups, n=3.
Scale bar, 200 µm. ALP, alkaline phosphatase; OPN, Osteopontin;
BMD, bone marrow density; TRAP, tartrate resistant acid
phosphatase; TGFβ, transcriptional growth factor β. |
| Table IICorrelation coefficients. |
Table II
Correlation coefficients.
| Bone turnover
parameter | Ratio of
p-smad2/3-positive osteocytes
|
|---|
| R | P-value |
|---|
| ALP mRNA | 0.3056 | 0.0491 |
| OCN mRNA | 0.1176 | 0.4582 |
| OPN mRNA | 0.3257 | 0.0353 |
| BMD | 0.7041 | <0.0001 |
| TRAP+
cells | −0.8517 | <0.0001 |
Discussion
Subchondral bone sclerosis is an important
pathological feature in advanced OA (32). Mechanically, altered bone
remodeling finally leads to subchondral sclerosis, which causes
uneven stress on the overlying cartilage and ultimately accelerates
its degeneration (10).
Therefore, preventing altered remodeling can help delay the
progression of cartilage degeneration, thereby elevating the
average age of OA patients that need surgical treatment. Moreover,
it has been found that osteoblast TGFβ signaling in subchondral
bone plays an important role in the pathogenesis of OA by altering
MSC osteogenic activity (9). It
has also found that osteocyte morphology changes in the specimens
from OA patients, with the secreted cytokine of sclerositin (SOST)
decreasing and dentin matrix acidic phosphoprotein 1 increasing
(21). Although a large number of
studies have emphasized the key regulatory role of osteocytes in
the maintenance of metabolism (33-36), the expression of osteocyte TGFβ
signaling in the subchondral of advanced OA remains unclear. In the
present study, it was found osteocyte TGFβ was abnormally activated
under the cartilage wear region and was closely associated with the
subchondral bone structural alternation and cartilage wearing. To
the best of our knowledge, this is the first study to explore the
association of osteocyte TGFβ with OA. This provides a preliminary
basis and theoretical guidance for further exploration of the role
and mechanism of osteocyte TGFβ signaling in OA.
Although cartilage degeneration is a characteristic
pathological change in OA, subchondral bone structural changes
caused by bone remodeling disorders are considered to be an
important pathological change that precedes cartilage degeneration.
This was further confirmed by MRI examination of bone marrow damage
in subchondral bone, where it was found that bone marrow lesions in
the subchondral bone had occurred before cartilage changes
(37). Moreover, in early OA, the
subchondral bone is mainly characterized by bone resorption
(38), which is characterized by
a decrease in the mass fraction of trabecular bone, with its
increase appearing during late OA along with sclerosis (39). The present study also found an
increase in the bone mass parameters and sclerosis in subchondral
bone from human knee of middle-advanced OA. Studies have shown that
cartilage degeneration in OA is strongly associated with
subchondral bone sclerosis, regardless of whether the increase
(40) or decrease (38) in sclerosis will result in
cartilage degeneration. Therefore, simply reducing subchondral bone
remodeling by inhibiting bone resorption does not necessarily
attenuate the progression of OA. The double-balanced regulation of
bone resorption and bone formation may be an effective method to
cope with the increase in the turnover of subchondral bone during
OA. Namely, inhibiting bone remodeling if high sclerosis is the
underlying cause of OA may be beneficial, since that may prevent an
increase in bone stiffness. However, if decreased mineralization is
the underlying cause, inhibiting remodeling may have a negative
effect, since it may prevent 'normalization' of the apparent bone
sclerosis.
It should also be noted that other factors may play
a role as well, as TGFβ has been detected to be abundantly
expressed in OA bone (11) and
synovial tissue (41). In the
present experiments, it was found that activated TGFβ1 was also
expressed in subchondral bone in the middle and late stage of OA,
and it showed an increased expression trend with the increase in
cartilage defect. Furthermore, neutralizing the TGFβ protein in
subchondral bone can effectively delay the OA process (12). Micro-fractures occur in the
subchondral bone of early OA due to loadbearing, which increases
the activity of osteoclasts (42)
and activates latent TGFβ in the extracellular matrix (43). It has been suggested that
activated TGFβ in the bone marrow can regulate the migration of
MSCs via osteoblasts and induce osteogenic differentiation
(44), which cause early
non-coupled osteogenesis and osteoclastogenesis, accelerating the
formation of local bone islands. Moreover, the conditional
inhibition of osteoblast TGFβ signaling can alleviate the
progression of OA (9).
How do the osteocytes, the most abundant
mechanosensory cells, respond to abnormally activated TGFβ in the
extracellular matrix when there is an abnormal stress distribution
on the subchondral bone in advanced OA? It has been found that
loading can cause an increase in the anabolism of cortical bone and
that its mechanism is associated with the inhibition of the
TGFβ-smad2/3 pathway in osteocytes (20). However, in the present study, it
was first discovered that the osteocyte TGFβ pathway in the
subchondral bone of OA patients was activated. Moreover, as
previously reported (3,5,37),
the structure of the subchondral bone significantly changed in the
middle and late stages of OA, bone formation increased, and bone
sclerosis was enhanced in the region of the subchondral bone under
cartilage wear, further indicating that subchondral bone sclerosis
is associated with cartilage.
Bone resorption in the subchondral bone of OA is
also enhanced, especially in the early stage of OA, which was
manifested by a decrease in bone density (38). Zhen et al (9) found that the osteoblast TGFβ
signaling only increased the activity of osteoclasts at an early
stage in the animal model of OA. It was also found that the
osteoclast activity was stronger in the subchondral bone in the
area underneath severely worn cartilage, especially full defect
cartilage, which indicated bone resorption by osteoclasts is still
elevated in the middle and late stages of OA. At the same time, it
was verified in vitro that the activation of osteoblast TGFβ
signaling can induce osteogen-esis and osteoclast differentiation
of MSCs co-cultured with it. It is suggested that osteocyte TGFβ
signaling may regulate the coupled bone resorption and bone
formation metabolism. These results indicated that abnormal bone
remodeling occurs in the subchondral bone underneath the
loadbearing cartilage and eventually leads to the formation of
sclerosis locally in the subchondral bone, since bone formation is
stronger than bone resorption. During this process, osteocytes play
an central role in regulating this dynamic bone metabolism.
It has been found that the reduction of BMD in the
subchondral bone in early OA and sclerosis in late OA was
associated with an increased expression of SOST (32,45). Moreover, knocking out SOST
increased the development of sclerosis in subchondral bone
(46). Furthermore, as the degree
of OA progresses, the expression of SOST in the subchondral bone
decreases (46). In the late
stage of osteo-blasts, TGFβ regulates the expression of its SOST
via its ECR5 enhancer (47).
However, it was found that PTH can inhibit the expression of SOST
(48). This suggests that in
late-stage OA, TGFβ may inhibit the expression of SOST through the
PTH pathway, Ansari et al (49) demonstrated that osteocyte
PTHrP/PTH regulates their gene expression, which is involved in
matrix mineralization. Although direct evidence that links the
aberrant activation of osteocyte TGFβ to subchondral bone sclerosis
is still lacking, the present observations suggested a possible
relationship.
In addition to the effect that TGFβ signaling has on
bone, it may influence cartilage. Although TGFβ1-Smad2/3 signaling
is required to control chondrocyte hypertrophic differentiation in
immature articular cartilage (14), the activation of TGFβ signaling in
mature articular cartilage will result in an extremely high
expression of metalloproteinase 13, resulting in the loss of
proteoglycans and increased expression of type X collagen (13). Occasionally, it was found that, in
the process of degenerative changes in mature cartilage, the
TGFβ-activated chondrocytes exhibited significant temporal and
spatial characteristics, by which chondrocyte TGFβ signaling
activation varies in different degrees of OA cartilage (temporal)
and in different layers of cartilage (spatial). Initially this was
only in the hypertrophic zone in the early stage, followed by a
gradual spread to the superficial layer, and finally the activation
of the TGFβ-Smad2/3 signaling pathway in throughout the chondrocyte
layer. Mechanistically, the expression of cartilage-matrix
degrading enzymes is the main manifestation of articular cartilage
degeneration (30,31). Therefore, the expression of
Adamts4, an important cartilage matrix-degrading enzyme, in
cartilage was then examined in the partial and full cartilage
groups. Of note, the expression of chondrocytic Adamts4 in the
partial cartilage group showed the same trend as that of p-Smad2/3.
However, the specific role and mechanism of the spatial
distribution of TGFβ in articular cartilage, was not studied in
depth in the present study, and the current research group will
further explore this phenomenon in the future.
Finally, the present study must admit several
limitations. First, only 21 participants were enrolled. Yet, the
aim of this preliminary study was to provide evidence of the
association between osteocyte TGFβ and bone turnover state in
subchondral bone of OA, and the authors believe that the sample
qualities were sufficient. Secondly, TGFβ signaling through the
smad2/3 pathway is its canonical pathway. Therefore, in present
study, the expression of TGFβ1 and pSmad2/3 was detected by
immunohistochemistry with reference to previous research findings
(8,9,12).
Although statistical correlation and in vitro analysis were
performed to determine the effect of activating osteocyte TGFβ
signaling pathway on osteogenesis and osteoclast differentiation, a
direct relationship between osteocyte TGFβ signal and the
development of OA remains to be elucidated. In future studies, the
authors will further investigate the effect of osteocyte TGFβ
signaling on the progression of OA by constructing transgenic mouse
models that conditionally regulate TGFβ signaling in osteocytes,
which would ultimately unveil the function of osteocyte TGFβ in OA
progression. Also, in order to clarify that TGFβ influences which
process of Smad2/3 pathway, the authors will next perform the
transfection experiments using miRNA and siRNA. Lastly, although in
the present study it was found that activated TGFβ signaling is
mainly found in osteocytes, bone marrow stromal cells and
osteoblasts, the role and localization of osteoclasts is unclear
because it is difficult to distinguish this from the cell shape
without special staining. Whether TGFβ signaling of osteoclasts is
activated may require osteoclast-specific markers and p-smad2/3
double-labeled immunohistochemical staining to confirm. The authors
consider these experiments outside the scope of the present study,
but they are valuable and the authors wish to finish these assays
in their future study.
Supplementary Data
Funding
This study was supported by National Natural Science
Foundation Program of China (grant no. 81572142).
Availability of data and materials
The data used and analyzed in this study are
available from the corresponding author upon reasonable
request.
Authors' contributions
GD and WH conceived and designed the study. GD, HX
and WH analyzed and interpreted the data. GD drafted the
manuscript. JL critically revised the manuscript for important
intellectual content. GD, HX, WeiX and XL obtained the study
materials and collected patient samples. GD and HX performed the
statistical analysis. NZ, CZ and WeiX provided administrative,
technical or logistic support. GD and HX collected data and
assembled the figures GD, HX, JL, NZ, WenX, XL and CZ performed the
experiments. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The ethics committee of the First Affiliated
Hospital of Chongqing Medical University approved the collection of
human specimens and the animal experiments in present study (Permit
number: 2015-316). Written informed consent was obtained from the
patients before surgery.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Acknowledgments
The authors would like to thank Dr Zhang Chen (The
General Hospital of Chongqing Iron and Steel, Chongqing, China) for
critical reading the manuscript.
References
|
1
|
Cross M, Smith E, Hoy D, Nolte S, Ackerman
I, Fransen M, Bridgett L, Williams S, Guillemin F, Hill CL, et al:
The global burden of hip and knee osteoarthritis: Estimates from
the global burden of disease 2010 study. Ann Rheum Dis.
73:1323–1330. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hugle T and Geurts J: What drives
osteoarthritis?-synovial versus subchondral bone pathology.
Rheumatology (Oxford). 56:1461–1471. 2017.
|
|
3
|
Adebayo OO, Ko FC, Wan PT, Goldring SR,
Goldring MB, Wright TM and van der Meulen MCH: Role of subchondral
bone properties and changes in development of load-induced
osteoarthritis in mice. Osteoarthritis Cartilage. 25:2108–2118.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kwan Tat S, Lajeunesse D, Pelletier JP and
Martel-Pelletier J: Targeting subchondral bone for treating
osteoarthritis: What is the evidence? Best Pract Res Clin
Rheumatol. 24:51–70. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hayami T, Pickarski M, Wesolowski GA,
McLane J, Bone A, Destefano J, Rodan GA and Duong LT: The role of
subchondral bone remodeling in osteoarthritis: Reduction of
cartilage degeneration and prevention of osteophyte formation by
alendronate in the rat anterior cruciate ligament transection
model. Arthritis Rheum. 50:1193–1206. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bertuglia A, Lacourt M, Girard C,
Beauchamp G, Richard H and Laverty S: Osteoclasts are recruited to
the subchondral bone in naturally occurring post-traumatic equine
carpal osteoarthritis and may contribute to cartilage degradation.
Osteoarthritis Cartilage. 24:555–566. 2016. View Article : Google Scholar
|
|
7
|
Bianco D, Todorov A, Čengić T, Pagenstert
G, Schären S, Netzer C, Hügle T and Geurts J: Alterations of
subchondral bone progenitor cells in human knee and hip
osteoarthritis lead to a bone sclerosis phenotype. Int J Mol Sci.
19:E4752018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zhao W, Wang T, Luo Q, Chen Y, Leung VY,
Wen C, Shah MF, Pan H, Chiu K, Cao X and Lu WW: Cartilage
degeneration and excessive subchondral bone formation in
spontaneous osteoarthritis involves altered TGF-β signaling. J
Orthop Res. 34:763–770. 2016. View Article : Google Scholar
|
|
9
|
Zhen G, Wen C, Jia X, Li Y, Crane JL,
Mears SC, Askin FB, Frassica FJ, Chang W, Yao J, et al: Inhibition
of TGF-β signaling in mesenchymal stem cells of subchondral bone
attenuates osteoarthritis. Nat Med. 19:704–712. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zhen G and Cao X: Targeting TGFβ signaling
in subchondral bone and articular cartilage homeostasis. Trends
Pharmacol Sci. 35:227–236. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cui Z, Crane J, Xie H, Jin X, Zhen G, Li
C, Xie L, Wang L, Bian Q, Qiu T, et al: Halofuginone attenuates
osteoarthritis by inhibition of TGF-beta activity and H-type vessel
formation in subchondral bone. Ann Rheum Dis. 75:1714–1721. 2016.
View Article : Google Scholar
|
|
12
|
Xie L, Tintani F, Wang X, Li F, Zhen G,
Qiu T, Wan M, Crane J, Chen Q and Cao X: Systemic neutralization of
TGF-β attenuates osteoarthritis. Ann N Y Acad Sci. 1376:53–64.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Aref-Eshghi E, Liu M, Harper PE, Doré J,
Martin G, Furey A, Green R, Rahman P and Zhai G: Overexpression of
MMP13 in human osteoarthritic cartilage is associated with the
SMAD-independent TGF-β signalling pathway. Arthritis Res Ther.
17:2642015. View Article : Google Scholar
|
|
14
|
van de Laar IM, Oldenburg RA, Pals G,
Roos-Hesselink JW, de Graaf BM, Verhagen JM, Hoedemaekers YM,
Willemsen R, Severijnen LA, Venselaar H, et al: Mutations in SMAD3
cause a syndromic form of aortic aneurysms and dissections with
early-onset osteoarthritis. Nat Genet. 43:121–126. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Serra R, Johnson M, Filvaroff EH, LaBorde
J, Sheehan DM, Derynck R and Moses HL: Expression of a truncated,
kinase-defective TGF-beta type II receptor in mouse skeletal tissue
promotes terminal chondrocyte differentiation and osteoarthritis. J
Cell Biol. 139:541–552. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Shen J, Li J, Wang B, Jin H, Wang M, Zhang
Y, Yang Y, Im HJ, O'Keefe R and Chen D: Deletion of the
transforming growth factor beta receptor type II gene in articular
chondrocytes leads to a progressive osteoarthritis-like phenotype
in mice. Arthritis Rheum. 65:3107–3119. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bakker AC, van de Loo FA, van Beuningen
HM, Sime P, van Lent PL, van der Kraan PM, Richards CD and van den
Berg WB: Overexpression of active TGF-beta-1 in the murine knee
joint: Evidence for synovial-layer-dependent chondro-osteophyte
formation. Osteoarthritis Cartilage. 9:128–136. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Klein-Nulend J, Bakker AD, Bacabac RG,
Vatsa A and Weinbaum S: Mechanosensation and transduction in
osteocytes. Bone. 54:182–190. 2013. View Article : Google Scholar
|
|
19
|
Chen H, Senda T and Kubo KY: The osteocyte
plays multiple roles in bone remodeling and mineral homeostasis.
Med Mol Morphol. 48:61–68. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Nguyen J, Tang SY, Nguyen D and Alliston
T: Load regulates bone formation and Sclerostin expression through
a TGFβ-dependent mechanism. PLoS One. 8:e538132013. View Article : Google Scholar
|
|
21
|
Jaiprakash A, Prasadam I, Feng JQ, Liu Y,
Crawford R and Xiao Y: Phenotypic characterization of
osteoarthritic osteocytes from the sclerotic zones: A possible
pathological role in subchondral bone sclerosis. Int J Biol Sci.
8:406–417. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Prasadam I, Farnaghi S, Feng JQ, Gu W,
Perry S, Crawford R and Xiao Y: Impact of extracellular matrix
derived from osteoarthritis subchondral bone osteoblasts on
osteocytes role of integrinβ1 and focal adhesion kinase signaling
cues. Arthritis Res Ther. 15:R1502013. View
Article : Google Scholar
|
|
23
|
Dolan EB, Haugh MG, Voisin MC, Tallon D
and McNamara LM: Thermally induced osteocyte damage initiates a
remodelling signaling cascade. PLoS One. 10:e01196522015.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Meo Burt P, Xiao L, Dealy C, Fisher MC and
Hurley MM: FGF2 high molecular weight isoforms contribute to
osteoarthropathy in male mice. Endocrinology. 157:4602–4614. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zhao C, Jiang W, Zhou N, Liao J, Yang M,
Hu N, Liang X, Xu W, Chen H, Liu W, et al: Sox9 augments
BMP2-induced chondro-genic differentiation by downregulating Smad7
in mesenchymal stem cells (MSCs). Genes Dis. 4:229–239. 2017.
View Article : Google Scholar
|
|
26
|
Dai Guangming RL, Chen H, Liu W, Chen Y,
He X, Liu W, Tu X and Huang W: Down-regulation of osteoeytic
TGFβ/Smad4 inhibits the osteoblastic and osteoelastic
differentiation in mouse BMSCs. Basic Clin Med. 37:786–791.
2017.
|
|
27
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar
|
|
28
|
Stern AR, Stern M, Van Dyke ME, Jähn K,
Prideaux M and Bonewald LF: Isolation and culture of primary
osteocytes from the long bones of skeletally mature and aged mice.
BioTechniques. 52:361–373. 2012.PubMed/NCBI
|
|
29
|
Boregowda SV, Krishnappa V and Phinney DG:
Isolation of mouse bone marrow mesenchymal stem cells. Methods Mol
Biol. 1416:205–223. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Yatabe T, Mochizuki S, Takizawa M,
Chijiiwa M, Okada A, Kimura T, Fujita Y, Matsumoto H, Toyama Y and
Okada Y: Hyaluronan inhibits expression of ADAMTS4 (aggrecanase-1)
in human osteoarthritic chondrocytes. Ann Rheum Dis. 68:1051–1058.
2009. View Article : Google Scholar :
|
|
31
|
Song RH, Tortorella MD, Malfait AM, Alston
JT, Yang Z, Arner EC and Griggs DW: Aggrecan degradation in human
articular cartilage explants is mediated by both ADAMTS-4 and
ADAMTS-5. Arthritis Rheum. 56:575–585. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Wu L, Guo H, Sun K, Zhao X, Ma T and Jin
Q: Sclerostin expression in the subchondral bone of patients with
knee osteoarthritis. Int J Mol Med. 38:1395–1402. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wood CL, Pajevic PD and Gooi JH: Osteocyte
secreted factors inhibit skeletal muscle differentiation. Bone Rep.
6:74–80. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Feng JQ, Ward LM, Liu S, Lu Y, Xie Y, Yuan
B, Yu X, Rauch F, Davis SI, Zhang S, et al: Loss of DMP1 causes
rickets and osteomalacia and identifies a role for osteocytes in
mineral metabolism. Nat Genet. 38:1310–1315. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Li X, Ominsky MS, Niu QT, Sun N, Daugherty
B, D'Agostin D, Kurahara C, Gao Y, Cao J, Gong J, et al: Targeted
deletion of the sclerostin gene in mice results in increased bone
formation and bone strength. J Bone Miner Res. 23:860–869. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Rosser J and Bonewald LF: Studying
osteocyte function using the cell lines MLO-Y4 and MLO-A5. Methods
Mol Biol. 816:67–81. 2012. View Article : Google Scholar
|
|
37
|
Kazakia GJ, Kuo D, Schooler J, Siddiqui S,
Shanbhag S, Bernstein G, Horvai A, Majumdar S, Ries M and Li X:
Bone and cartilage demonstrate changes localized to bone marrow
edema-like lesions within osteoarthritic knees. Osteoarthritis
Cartilage. 21:94–101. 2013. View Article : Google Scholar :
|
|
38
|
Siebelt M, Waarsing JH, Groen HC, Müller
C, Koelewijn SJ, de Blois E, Verhaar JA, de Jong M and Weinans H:
Inhibited osteoclastic bone resorption through alendronate
treatment in rats reduces severe osteoarthritis progression. Bone.
66:163–170. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Nakasa T, Ishikawa M, Takada T, Miyaki S
and Ochi M: Attenuation of cartilage degeneration by calcitonin
gene-related paptide receptor antagonist via inhibition of
subchondral bone sclerosis in osteoarthritis mice. J Orthop Res.
34:1177–1184. 2016. View Article : Google Scholar
|
|
40
|
Xie L, Ding F, Jiao J, Kan W and Wang J:
Total Hip and Knee arthroplasty in a patient with osteopetrosis: A
case report and review of the literature. BMC Musculoskelet Disord.
16:2592015. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Remst DF, Blom AB, Vitters EL, Bank RA,
van den Berg WB, Blaney Davidson EN and van der Kraan PM: Gene
expression analysis of murine and human osteoarthritis synovium
reveals elevation of transforming growth factor beta-responsive
genes in osteoarthritis-related fibrosis. Arthritis Rheumatol.
66:647–656. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Li ZC, Dai LY, Jiang LS and Qiu S:
Difference in subchondral cancellous bone between postmenopausal
women with hip osteoarthritis and osteoporotic fracture:
Implication for fatigue microdamage, bone microarchitecture, and
biomechanical properties. Arthritis Rheum. 64:3955–3962. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Hinz B: The extracellular matrix and
transforming growth factor-β1: Tale of a strained relationship.
Matrix Biol. 47:54–65. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Tang Y, Wu X, Lei W, Pang L, Wan C, Shi Z,
Zhao L, Nagy TR, Peng X, Hu J, et al: TGF-beta1-induced migration
of bone mesenchymal stem cells couples bone resorption with
formation. Nat Med. 15:757–765. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Zarei A, Hulley PA, Sabokbar A and Javaid
MK: Co-expression of DKK-1 and sclerostin in subchondral bone of
the proximal femoral heads from osteoarthritic hips. Calcif Tissue
Int. 100:609–618. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Bouaziz W, Funck-Brentano T, Lin H, Marty
C, Ea HK, Hay E and Cohen-Solal M: Loss of sclerostin promotes
osteoarthritis in mice via β-catenin-dependent and -independent Wnt
pathways. Arthritis Res Ther. 17:242015. View Article : Google Scholar
|
|
47
|
Loots GG, Keller H, Leupin O, Murugesh D,
Collette NM and Genetos DC: TGF-β regulates sclerostin expression
via the ECR5 enhancer. Bone. 50:663–669. 2012. View Article : Google Scholar
|
|
48
|
Li C, Wang W, Xie L, Luo X, Cao X and Wan
M: Lipoprotein receptor-related protein 6 is required for
parathyroid hormone-induced Sost suppression. Ann N Y Acad Sci.
1364:62–73. 2016. View Article : Google Scholar
|
|
49
|
Ansari N, Ho PW, Crimeen-Irwin B, Poulton
IJ, Brunt AR, Forwood MR, Divieti Pajevic P, Gooi JH, Martin TJ and
Sims NA: Autocrine and paracrine regulation of the murine skeleton
by osteocyte-derived parathyroid hormone-related protein. J Bone
Miner Res. 33:137–153. 2018. View Article : Google Scholar
|