1. Introduction
Since the inception of its outbreak, Coronavirus
disease 2019 (COVID-19) has spread worldwide, claiming
>1,840,000 lives (1). In
addition to its global impact, COVID-19 has alarmed the healthcare
community on the danger and harm of nosocomial infection.
Nosocomial infection of COVID-19 has been discovered and reported
in numerous healthcare facilities on a global scale.
A total of 48 COVID-19 cases, including 28
healthcare professionals (HCPs), 13 patients and 7 accompanying
persons (ACPs) were associated with a nosocomial infection case in
the pediatric dialysis unit of the University Hospital of Münster
(Münster, Germany) (2). Among
these cases, 4 COVID-19 cases had a 15-min face-to-face contact
with healthcare workers without wearing personal protective
equipment (PPE) and 7 other healthcare workers were infected while
treating patients with COVID-19 at a distance of <2 meters
without PPE (2). Carter et
al (3) reported that 196
nosocomial COVID-19 cases (NC) out of 1,564 patients were from 11
hospitals in the UK and Italy. The mortality rate of NC patients
was 27% and the median survival time in NC patients was 14 days
(3). Wang et al (4) found that 57 cases were infected
through hospital-associated transmission among 138 hospitalized
patients with COVID-19, including 17 inpatients, 31 HCPs from
general wards, 7 HCPs from the emergency department and 2 HCPs from
the intensive care unit (ICU). Notably, an index case with
abdominal symptoms caused 14 infections, including 10 HCPs with
nosocomial COVID-19 infection and 4 hospitalized patients with an
atypical abdominal symptom and fever (4). This index case with great capacity
to cause infection was presumed to be a superspreader (4). Similar nosocomial infection cases
were also found in France (5,6),
Canada (7), China (8) and South Korea (9) (Table
I). Hence, it is urgent to determine the cause of these
nosocomial infection cases.
 | Table ISome nosocomial infection events of
COVID-19. |
Table I
Some nosocomial infection events of
COVID-19.
| First author,
year | Site | Number of
infections | Reported timeline
(2020) | Events | Patient
outcomes | Refs. |
|---|
| Schwierzeck et
al, 2020 | Münster,
Germany | 48 | N/A | 48 cases including
28 HCPs, 13 patients and 7 accompanying persons | N/A | (2) |
| Carter et
al, 2020 | 11 hospitals in UK
and Italy | 196 | Feb 27-Apr 28 | 27.0% of patients
with nosocomial infection died, and the median survival time was 14
days | 53 died | (3) |
| Wang et al,
2020 | Zhongnan Hospital,
Wuhan, China | 57 | Jan 1-28 | 57 people were
confirmed with COVID-19, including 17 inpatients and 40 HCPs | N/A | (4) |
| Luong-Nguyen et
al, 2020 | Ile-de-France,
France | 15 | Mar 1-Apr 5 | 15 patients
developed nosocomial COVID-19 infection (all of them had
co-morbidities) | 2 died, 7
hospitalized and 6 discharged | (5) |
| Vanhems, 2020 | Lyon area,
France | 8 | Mar 10-13 | 6 cases were
infected by 2 potential index cases, including one HCP | 2 died | (6) |
| Elkrief et
al, 2020 | Canada | 47 | Mar 3-May 23 | The nosocomial
infection rate was 19% among 252 patients with cancer and
COVID-19 | 22 died, 7
hospitalized, 3 critically-ill and 15 outpatients | (7) |
| Lai et al,
2020 | Tongji Hospital,
Wuhan, China | 77 | Jan 1-Feb 9 | The infection rate
of HCPs was 1.1%; 70 HCPs were infected in general clinics or
wards, 7 in fever clinics or wards | N/A | (8) |
| Ji et al,
2020 | South Korea | 119 | Feb 11-Mar 2 | The first patient
was diagnosed with COVID-19 two days after his death; 119 patients
were confirmed with COVID-19 | 7 died | (9) |
| Ji et al,
2020 | Wuhan Mental Health
Center, Wuhan, China | 80 | Jan 12-Feb 8 | ~50 patients and 30
HCPs were confirmed with COVID-19 | N/A | (9) |
2. Transmission model of COVID-19
Nosocomial infections of COVID-19 include exogenous
and endogenous infection, and pose a great threat to inpatients,
HCPs and ACPs. Exogenous infection, also known as cross infection,
is caused by pathogens that directly come from the environment
through the HCP's hands or contaminated objects (10). In endogenous infection, patients,
especially those who are immunocompromised, are infected by the
normal flora from patients or the pathogens from hospital (10). It is hence essential to revisit
the modes of transmission of COVID-19.
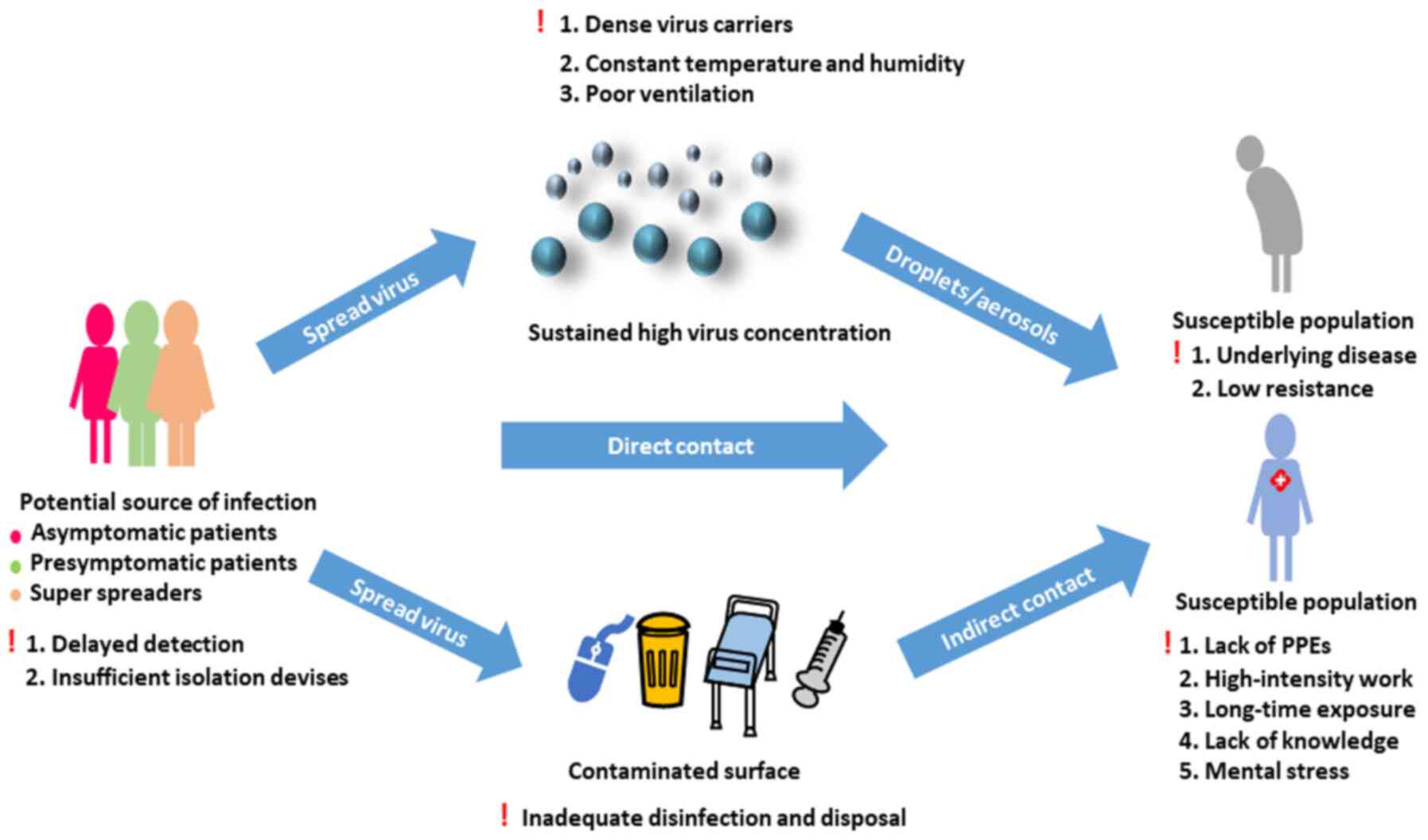
Source of infection
It is well understood that confirmed patients with
COVID-19 are the main sources of infection in human-to-human
transmission of COVID-19. Asymptomatic cases and superspreaders may
also be potential sources of infection. Additionally, other
patients with low immunity and infected patients with no or only
mild symptoms may gather in hospital to spread the virus in the
community through social interactions. Thus, nosocomial infection
acts as a contributing factor of an outbreak (11,12).
Asymptomatic individuals
AsymptomatiC patients are those without clinical
manifestations but with positive nucleic acid results of Severe
Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) or chest
imaging (13). Asymptomatic
individuals may not be ill enough to seek medical care, and this
allows them to participate in a larger range of activities. Wang
et al (14) stated that
the transmissibility of asymptomatiC patients was fairly limited
due to the lack of symptoms, including coughing and sneezing.
Hence, they are unlikely to be the major driving force of
transmission (14). However, Li
et al (15) demonstrated
that 86% of all patients with COVID-19 infection in China were
asymptomatic individuals in the early stage, and they caused 79% of
the documented COVID-19 cases with observed symptoms and the rapid
spread throughout the country before the travel restrictions. These
studies indicate that the discussion on COVID-19 transmissibility
of asymptomatic individuals remains to be clarified.
Progress in COVID-19 containment has revealed that
the proportion of asymptomatic individuals was higher than previous
projections in Wuhan, China (40-50% of all cases) (16). However, some studies have shown
that this proportion may be as low as 10% (16,17). It has been reported that
asymptomatic individuals can be divided into inapparent cases,
which do not appear symptomatic for the incubation period and can
even obtain positive results from laboratory tests, and
presymptomatic cases (17).
During the incubation period, presymptomatic individuals can
transmit COVID-19 even before onset of clinical symptoms (18). He et al (18) found that the highest
infectiousness occurred before symptom onset, and 44% of secondary
cases originated from presymptomatic cases. Kimball et al
(19) reported that a rapid
transmission of COVID-19 occurred in a skilled nursing facility in
King County (WA, USA). About half of infected individuals were
asymptomatic or presymptomatic on the day of nucleic acid testing,
and they may therefore contribute to the transmission of COVID-19
(19).
Superspreaders
Individuals who have a greater than average
capability of infecting more people are known as superspreaders
(20). Medical experts have
claimed that superspreaders may trigger a fresh outbreak (19). It is hence necessary to analyze
the epidemic chain of transmission of COVID-19 originating from a
superspreader considering the increased strain virulence, and the
differences in hosts and co-infection with another pathogen should
be taken into account (21).
Additionally, asymptomatic and mild symptomatic individuals may be
another type of infection source of superspreading events (SSEs)
due to lack of awareness and containment measures (22). In addition, the combined effects
of biology, behavior and environmental factors may lead to
superspreading events (20).
During SARS and Middle East Respiratory Syndrome
outbreaks, nosocomial transmission was associated with SSEs, and
numerous patients, including HCPs and ACPs, were infected with
those events (23).
Additionally, hospitals are relatively closed environments with
often dense populations and poor ventilation, and are therefore
more likely to be a transmission site compared with an open
environment (24). Moreover,
unrecognized or misdiagnosed infection cases in 11 directly
transmitted infections, including SARS, were shown to be the main
reason of SSEs, followed by the mode of transmission, contact
frequency and co-infection (25).
In addition to the aforementioned scenarios,
SARS-CoV-2 was detected in some discharged patients, who may still
be potential virus carriers (26). Furthermore, it was reported that
reverse transcription PCR test results may not fully correlate with
transmissibility (27). The
World Health Organization (WHO) suggests that patients should be
released from isolation >10 days after symptom onset and after
>3 additional days without symptoms (28).
Transmission routes
COVID-19 primarily spreads via air droplets and
direct contact, but SARS-CoV-2 RNA can also be found in fecal
specimens and the virus may be spread via an excretory route
(29). Although neonatal
infections of COVID-19 have been observed, there is no direct
evidence of vertical mother-to-child transmission (30). Fan et al (31) analyzed two confirmed expectant
mothers, and SARS-CoV-2 was not detected in any of the products of
conception and newborns. This analysis indicated that the risk of
vertical transmission route of COVID-19 was relatively low
(31).
Liu et al (32) reported that the trace of
SARS-CoV-2 RNA was extremely high in small and non-ventilated
mobile toilets in public areas of two hospitals in Wuhan (China),
and relatively low in the isolation and ventilated rooms. Notably,
some cases of HCP infection in China were associated with aerosol
transmission in relatively closed environments, long-term exposures
and high-concentration pathogen aerosol environments (33,34). The size of droplets is variable
due to the force and pressure at emission, evaporation and
environment influence; droplets (5-10 µm in diameter) remain
in the air for a short time and settle within 1 m of the source,
while aerosols (≤5 µm) disseminate in the air over long
distances (35,36). A large droplet can become an
aerosol in less than a second (35). van Doremalen et al
(37) reported that SARS-CoV-2
is viable and infectious in aerosols for 3 h. It has been shown
that the virus can still be detected at a distance of 4 m from
patients (38). If considering
only the droplets and direct contact transmission of COVID-19, the
recommended distance for HCPs from patients can be decreased to 1 m
(35).
Susceptible population
Patients of all ages are susceptible to COVID-19,
especially elderly males (>55 years old) with underlying
diseases, such as diabetes, hypertension and cardio-vascular
disease (39). Hospitalized
patients in nursing homes or skilled care facilities with moderate
to severe asthma, severe heart disease or low immunity (cancer,
immunodeficiency or severe obesity) are all high-risk COVID-19
populations of endogenous infection (40).
Another noteworthy aspect of endogenous infection is
healthcare-associated infections for critically ill patients caused
by other pathogenic microorganisms. For example,
ventilator-associated pneumonia (VAP) is the most common
complication of mechanical ventilation (41). The estimated mortality of VAP is
13% (41). Zhou et al
(42) reported that secondary
infections occurred in 27/57 non-survivors of COVID-19, and VAP
occurred in 10/32 patients who underwent invasive mechanical
ventilation. He et al (43) reported that the nosocomial
infection rate among patients with COVID-19 was 7.1%; the most
common infection was pneumonia, followed by bacteremia and urinary
tract infection. The pathogens involved were Coagulase negative
staphylococcus (27.9%), Acinetobacter (20.9%),
Pseudomonas aeruginosa (14%), Enterococcus faecium
(11.6%) and Klebsiella pneumoniae (9.3%) (43). Under these circumstances, the
death rate among patients with nosocomial infection was 15.4%
(43).
3. Influencing factors associated with
nosocomial infection
Lack of self-protection and containment measures may
cause a cluster of cases in a hospital. During the early stages of
the COVID-19 outbreak, the shortage of PPE and lack of awareness of
the importance of personal protections were the main factors of new
cases (34,44). In addition, healthcare workers in
non-communicable disease departments did not have sufficient
knowledge on how to deal with potentially infectious diseases
(9). This explains why
non-communicable healthcare workers may be more likely to be
infected (45). Additionally, in
flu season, the transmissibility of the virus was almost always
underestimated. Furthermore, numerous patients in long-term nursing
facilities with little or no isolation equipment increase the risk
of cross-infection (46).
Lastly, ACPs may be exposed to the virus without personal
protection; therefore, family visits may also increase the
potential risk of COVID-19 exposure and infection (9).
The personal protection of HCPs is an important
topic. Two studies concluded that HCP-infected COVID-19 cases were
mostly due to lack of PPE at the very beginning of the pandemic
(33,34). A high-stress work environment may
have further weakened the immunity of healthcare workers, and
long-time exposure to patients may have rapidly increased their
risk of infection (34).
Additionally, these healthcare workers may not have received enough
professional training in infectious disease control and prevention
(33) (Fig. 1).
4. Preventative and containment strategies
for nosocomial infection
Monitoring and controlling nosocomial infections are
important routines in a hospital, as every hospital should
implement effective programs according to its actual condition.
This process typically involves four essential components: i)
Conducting scientific surveillance and control measures; ii)
Retaining professional epidemiologists; iii) Installing an
infection control staff every 250 beds; and iv) A system for
statistical analysis of nosocomial infection rates (47).
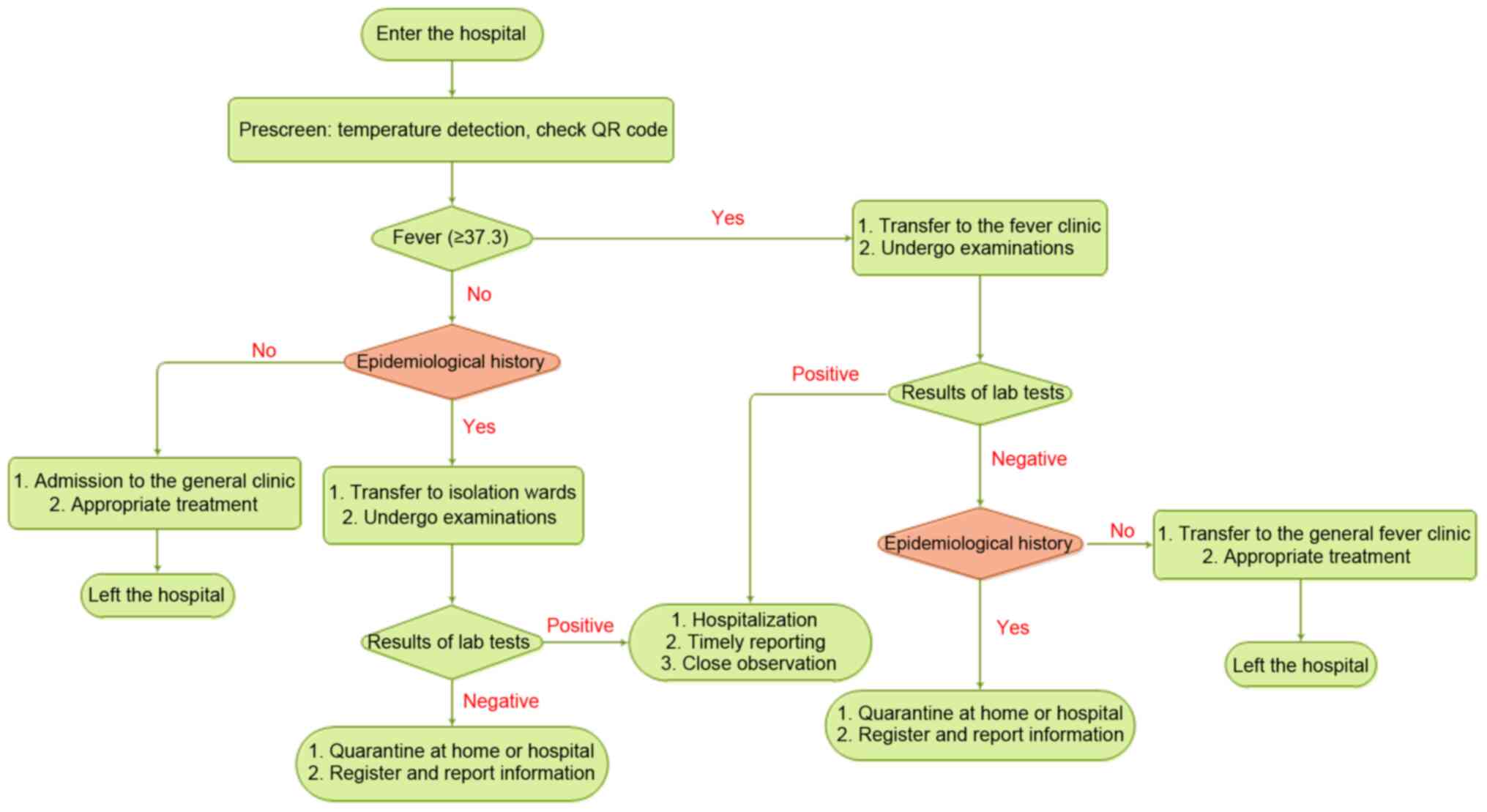
Triage of patients with COVID-19 for
disease management
In the early stages of the COVID-19 outbreak, a
large number of hospitals established 3- or 4-tiered patient triage
strategies to reduce contact between the susceptible population and
potential sources of infection (48,49). At these hospitals, nurses
prescreen patients at the entrance of the main lobby by checking
the body temperature and scanning health QR codes. The three colors
of QR codes (red, yellow and green) correspond to different risk
levels (49). Patients would
then be divided into different groups according to their body
temperatures (Fig. 2).
Patients with a high body temperature would be
transferred to a fever clinic through specific routes, accompanied
by HCPs with sufficient protection, and epidemiologists would
perform detailed COVID-19 checks (48). Other patients with no fever would
be allowed for entrance into the general clinic, and specialists of
all departments would prescreen for suspected cases according to
the patients' body temperatures, epidemiological histories and QR
codes (49). Patients with an
epidemiological history, including a history of visiting the
epidemic area within 14 days, contacting patients with symptoms
suggestive of COVID-19 or from an epidemic area within 14 days, and
epidemiological linkage with COVID-19, but with normal body
temperatures would also receive the same treatments in different
areas, while asked to stay in an isolation room for further
treatment (48). The suspected
patients' condition would be registered in detail and reported to
the relevant departments (48).
Reconciling the mismatch between hospital capacity
and a large number of patients in a short-term period is a
thought-provoking process. Currently, appropriate self-isolation is
emphasized for most self-healing and suspected patients to reduce
unnecessary visits to the hospital. There are a number of
additional tools for reducing the consumption of unnecessary
medical resources, such as mobile applications that can track
geographic routes so that patients can self-report their own
physical conditions and test results of COVID-19. Healthcare
institutions can then find out where the outbreak centers are and
take corresponding measures and allot materials by analyzing the
data collected through these apps (50). Canadian scientists suggested that
suspected patients with COVID-19 may be detected and monitored at
home while equipped with instruments for measuring body
temperature, blood pressure and heart rate (51). Additionally, HCPs can communicate
safely with patients through remote monitoring systems (51). The effectiveness of home care
depends on factors including professional guidance and management,
and adequate measurements for nursing at home in cases of suitable
conditions of the patients (52).
Furthermore, patients can be screened by telephone
before they enter the hospital in order for HCPs to prepare for
isolation before patients who need urgent care arrive to the
hospital (53). In addition,
internet hospitals in China provide medical consultation services
for the public in order to alleviate the public's alarm, impart
personal protection knowledge and correct inappropriate medical
behaviors, thereby reducing unnecessary visits to hospitals
(54).
Frontline HCPs have a distinctly higher risk of
infection, especially those who re-use PPE or do not have adequate
PPE (55). Htun et al
(56) proposed a Staff Health
Surveillance System to monitor employee travel experience, sick
leave and detailed information, and record body temperature and N95
mask usage. These data provide important references for the
management and protection for HCPs.
Specially redesigned wards in hospitals
for patients with COVID-19
The Chinese Health Commission specifies that fever
clinics are to be divided into special consulting rooms,
specifically used for receiving patients with a high risk of
COVID-19, and general consulting rooms, to receive patients with a
low risk or a clear non-COVID cause of fever (48). These fever clinics, also known as
wards, are located in a separate area and the entrance for patients
is different from that of healthcare workers (49). The wards provide a convenient way
of isolation from the outside and they are divided into two parts:
One for isolating confirmed cases, which can host multiple
patients, and the other for suspicious patients, where only one
person is allowed per room (57). A buffer zone is located between
the clean, semi-clean and contaminated areas to reduce staff
exposure to infected cases, and HCPs take strict self-protection
measures and go through disinfection before entering and leaving
the contaminated area (58).
Ventilation of the isolation ward is required to reach 60 l/s, and
the distances between beds are set to at least 1 m (59). The number of isolation rooms is
determined based on the epidemic condition and the number of
patients received.
It is important to design and install appropriate
isolation procedures, such as physical barriers or partitions to
guide patients to different areas, curtains in the shared area to
isolate patients, and installing and maintaining air treatment
systems with directional, filtering equal capacity to maintain air
circulation (60). Tang et
al (61) suggested that the
doors and windows of the isolation room should be kept closed to
avoid reverse airflow.
High-risk treatment procedures that
should be avoided
According to the transmission modes of COVID-19,
treatment procedures that produce droplets and aerosols are high
risk. Loeb et al (62)
demonstrated that auxiliary intubation, suctioning before
intubation and operating an oxygen mask were high-risk activities.
Patients' secretions, saliva or blood may aerosolize to the
environment while receiving treatment, especially in the
stomatology department, with possible apparatus contamination
(63). Hence, the risk of
crossinfection increases through direct contact (63). Moreover, the virus can be
detected in conjunctival swabs of patients with eye symptoms
(64), indicating that patients
who received slit lamp examination and direct ophthalmoscopy, as
well as ophthalmologists, have a high risk of infection (65).
Incidentally, each medical department should suspend
all unnecessary inspections to decrease the chance of transmission
(65); only urgent surgeries
should be arranged at the end of the day to reduce the risk of
hospital infection (63,66). Additionally, the number of health
care assistants should be minimized, and patients who are at
different risk levels of infection should be placed separately to
reduce cross-infection (67).
The risk of nosocomial infection can be analyzed
from two aspects: i) Daily risk of exposure, and ii) Total number
of days of exposure. It has been shown that patients in the high
daily risk department for a short time may have the same chance to
be infected as patients in the low daily risk department for a long
time (68). For each department,
it is necessary to decrease the daily risk through various
protective and disinfection measures, and shorten the treatment
time of patients by reducing unnecessary treatment procedures
(69).
Environmental surveillance and
disinfection in wards and HCP offices should be enhanced
van Doremalen et al (37) has reported that the half-life of
SARS-CoV-2 in aerosol is 1.1-1.2 h and has a longer viability
period on stainless steel and plastic surfaces, with half-lives of
5.6 and 6.8 h, respectively. Constant humidity and temperature for
an extended period of time in the hospital may further prolong the
survival period of the virus (32). Coronavirus is sensitive to
ultraviolet light and heat, and most disinfectants (except for
chlorhexidine) can effectively inactivate the virus (70,71). Kampf et al (70) reported that using 62-71% ethanol,
0.5% hydrogen peroxide or 0.1% sodium hypochlorite can effectively
inactivate human coronavirus within 1 min; however, 0.05-0.2%
benzalkonium chloride or 0.02% chlorhexidine and gluconate are less
effective.
The virus can be widely distributed on the floor,
computer mouse, trash cans and even bed handrails, and can be
detected in 4 m of air surrounding a patient (38). Compared with contaminated areas,
clean and semi-clean areas exhibited more sites where the virus was
detected. Moreover, the contamination in isolation wards was even
worse than that in ICUs (58,72). These results indicate that HCPs
may be exposed to a higher risk in isolation wards and semi-clean
areas instead of contaminated areas. Therefore, it is important to
enhance daily disinfection, particularly on key surfaces such as
handle rails, switches and computer keyboards.
The wards of discharged patients should be fully
disinfected. Sheets, curtains, ventilation, lighting and all
surfaces should be carefully cleaned (73). For medical procedures that may
generate aerosols, effective air isolation measures, including
single rooms, negative pressure, frequent ventilation and powered
air-purifying respirators, are required (74). Each department should formulate
their own disinfection strategies, ensuring that all surfaces are
cleaned and disinfected after daily operations (63,65,75).
Self-protection is important for
HCPs
PPE
Masks, goggles, protective clothing and good hand
hygiene directly decreases the risk of nosocomial infection
(76). Casanova et al
(77) found that the coronavirus
can survive >24 h on an N95 respirator, and at least for 4 h on
other PPE. Therefore, it is important to train HCPs on how to wear
and remove PPE correctly, and promptly dispose of used PPE. The
correct order of wearing PPE is as follows: Hairnet, gown (with a
back closure, may require two people), filter mask, goggles and
finally two layers of gloves, with the inner layer covering up the
wrist (75).
In order to improve the efficiency of protective
devices, the usage of PPE is determined by the risk level of each
patient, and the prevention measures are formulated according to
the risk assessment of the epidemic (66). The WHO recommends using PPE for
HCPs depending on the aerosol-generating procedures in different
settings and the infection risk of patients. HCPs should wear
medical masks and eye protection when screening patients without
direct contact within 1 m (78).
HCPs should use respirator N95 of FFP2 or FFP3 standard, gown,
gloves, eye protection (goggles or face shield) and apron when
collecting diagnostic respiratory samples in enclosed spaces or
directly taking care of patients with COVID-19 (where
aerosol-generating procedures are frequently performed) (78). When aerosol-generating procedures
are not performed, the respirator can be replaced by a medical
mask, and the apron is not required. When HCPs treat patients with
symptoms suggestive of COVID-19, HCPs should use a medical mask,
gown, gloves and eye protection (78). In addition, lab technicians who
may handle the specimens from suspected or confirmed patients
should use a medical mask, eye protection, gown and gloves, and
should maintain a physical distance of at least 1 m (78).
Hand hygiene
Transmission through HCP hands in contact with
contaminated surfaces also increases the risk of exogenous
nosocomial infections (79).
Hand cleaning and disinfection are the main steps that can stop
pathogens from being transmitted from the patient to the HCP
(80). HCPs in all departments
need to thoroughly wash their hands before examination, after
touching patients, after collecting patients' oral mucosa, blood
and body fluids, and after touching equipment without sterilization
(81). Pessoa-Silva et al
(82) investigated the hand
hygiene conditions of 149 newborn nursing staff, and the results
revealed that the use of gloves did not completely protect HCP
hands from bacterial contamination. Since numerous HCPs still
believe that the purpose of using gloves is only for
self-protection rather than protecting patients, hand washing
compliance needs to be further rein-forced. Hands should also be
strictly sterilized before wearing gloves to avoid infection caused
by broken gloves (83).
Education and training for HCPs and the
public can decrease the risk of transmission
Patients in community or hospital isolation should
strictly comply with medical guidance and wash their hands with
water or soap for at least 20 sec or with an alcohol-based hand
sanitizer, avoid touching their eyes, cover their nose and mouth
with tissues when coughing or sneezing, and disinfect objects and
surfaces that are always touched (84). Patient education will increase
awareness for hand hygiene (85). Based on a survey performed on a
Chinese population, 98% of the participants would wear masks when
they went outdoors; additionally, participants with a high
socioeconomic status, especially females, were more educated about
COVID-19 and complied better to PPE usage and hand hygiene guidance
(86).
Sufficient knowledge and on-premises work experience
may improve the ability of HCPs to better handle COVID-19, since
incorrect attitudes and practices directly increase the risk of
infection (87). In the early
stages of the outbreak, the health administrative department of
hospitals in China conducted professional training for medical
workers through demonstrations, videos and other methods, including
personal protection measures, medical waste disposal and emergency
treatment agreements, and experts supervised the entire process of
professional training. Before participating in the treatment of
COVID-19, HCPs were subjected to medical examination and daily
self-monitoring of respiratory symptoms (88). High-risk HCPs who were pregnant,
>55 years of age or had a history of chronic diseases or acute
fever were exempted from SARS-CoV-2-associated work (89).
Disposing medical wastes correctly to
reduce avoidable transmission
During the COVID-19 outbreak, the demand of PPE and
medical supplies increased dramatically. Wang et al
(90) estimated that the daily
demand for masks reached 900 million in China. There were too many
medical wastes to be disposed of properly to reduce the potential
risk of transmission among HCPs, patients and the public. Different
types of waste should be collected in specific containers with
labels to avoid accidental injury of cleaning staff and decrease
the financial costs on waste disposal (91). Installing temporary disposal
facilities and incinerators may relieve the pressure of a sharp
increase in waste, and the risk of transportation may be influenced
by the haul distance and location of facilities, which should be
taken seriously according to economic costs and distance (92). Medical waste disposal procedures
include collection and separation of medical wastes, transportation
facility, proper waste disposal and staff protection and training
(93). The WHO has given
detailed advice on waste collection and destruction, as well as
personnel training and protection (94). According to this advice, Chinese
scientists gave guidance on the disinfection of wastes during the
COVID-19 outbreak (95).
Logistic support measures are sustaining
epidemic prevention efforts
With the surge in the number of infected cases, the
demand of transportation vehicles and HCPs for transportation of
patients and equipment for critically ill patients also increased
sharply. Deployment and supply of personnel, equipment and drugs
are of significance in treatment efficiency and containment of any
epidemic. A fast and economical logistics model should be
established according to the outbreak situation in various places.
He and Liu (96) proposed that
the sensitive-exposure-infection-recovery model may be considered
as a basis of predicting the medical needs of various regions and
formulating a material distribution plan. The 'Eagle-Eyed Observer'
is a logistics support system that can monitor the physiological
index of HCPs before and after entering the isolation ward, guide
the HCPs to use PPE correctly and deal with used PPE, monitor the
patient's situation and ward environment, and even organize medical
supplies properly (97).
5. Conclusion and future perspectives
COVID-19 can be transmitted by direct contact with
blood, body fluids, tissues of patients, droplets and surfaces
contaminated by the virus. To date, nosocomial infections have
occurred to varying degrees in different countries around the
world. In hospitals, high population density, large numbers of
susceptible people and the gathering of potential sources of
infection are all contributing factors for nosocomial infections. A
great amount of effort goes into nosocomial infection control of
COVID-19. It is necessary to call for doctors' First Visit
Responsibility in saving patients with COVID-19 and determine the
handling of HCPs with direct or continuous exposure to infected
patients.
Technology has played a crucial role in the
prevention and control of COVID-19 in four ways. Firstly,
artificial intelligence (AI)-driven robots or AI-assisted equipment
have been very effective in fighting against the virus. It takes 1
min for a robot equipped with an AI-enabled fever-screening system
to check the temperature of 200 people in an efficient and accurate
manner; robot deliveries supported by cutting-edge technologies
show promising potential for reducing direct exposure to the highly
contagious virus (98).
Secondly, digital technologies, such as big data and cloud
computing, have been heavily utilized in containing and preventing
outbreaks. There is an application prospect for the use of digital
technologies in the evaluation of disease outbreaks. Thirdly,
remote healthcare services backed by 5G communication technology
are among the potential applications to ensure communication
services for hospitals in different regions. Finally, remote visual
medical treatment systems may aid in assisting front-line practices
for healthcare workers to work remotely without direct exposure or
continuous exposure to infected patients. This comprehensive
network may serve an important role in minimizing the incidence of
nosocomial infection.
Nosocomial infection constitutes an important part
of an epidemic, especially in high-risk populations with
insufficient prevention and control measures, including psychiatric
hospitals and long-term care facilities. Improving the ability of
detecting the mild or asymptomatic and presymptomatic individuals
as early as possible is the key point in the current stage of the
epidemic. Maintaining a safe distance, isolation measures, adequate
material supplies and advanced tele-medicine are important measures
to control the epidemic. Limitations in the present review of the
small-scale cases with COVID-19 infection are due to the finite
number of nosocomial infection cases that have been reported.
Further research on the association between nosocomial infection
with subtypes of COVID-19 infection, such as the ordinary, severe
or critical type, the days in hospital, ICU or relapse, and mutual
infections during hospitalization, are deemed valuable for guiding
clinical nursing and treatment. The present review indicates that
once an epidemic occurs, a comprehensive analysis network may
provide a powerful guideline for the next unknown virus or even the
resurgence of COVID-19, and may pave the way to handle similar
public health emergencies in the future.
Funding
This study was supported by grants from the
Department of Science and Technology of Sichuan Province (grant no.
20YFS0435), the Health Care of Sichuan Provincial cadres (grant no.
2020-227) and the Science & Technology Bureau of Chengdu (grant
nos. YF05-00198-SN and YF05-00060-SN).
Availability of data and materials
Not applicable.
Authors' contributions
QD and DZ contributed to the writing, reviewing and
editing of the manuscript. QD and WH confirmed the authenticity of
the data. QD, XL, QX, TW and HJ provided resources and created the
figures. DZ and WH were involved in the conception of the study and
provided supervision. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Acknowledgments
Not applicable.
References
|
1
|
World Health Organization (WHO): WHO
coronavirus disease (COVID-19) dashboard. https://covid19.who.int/. Accessed January 19,
2021.
|
|
2
|
Schwierzeck V, König JC, Kühn J, Mellmann
A, Correa-Martínez CL, Omran H, Konrad M, Kaiser T and Kampmeier S:
First reported nosocomial outbreak of severe acute respiratory
syndrome corona-virus 2 (SARS-CoV-2) in a pediatric dialysis unit.
Clin Infect Dis. ciaa491Apr 27–2020.Epub ahead of print.
|
|
3
|
Carter B, Collins JT, Barlow-Pay F,
Rickard F, Bruce E, Verduri A, Quinn TJ, Mitchell E, Price A,
Vilches-Moraga A, et al: Nosocomial COVID-19 infection: Examining
the risk of mortality. The COPE-nosocomial study (COVID in Older
PEople). J Hosp Infect. 106:376–384. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J,
Wang B, Xiang H, Cheng Z, Xiong Y, et al: Clinical characteristics
of 138 hospitalized patients with 2019 novel coronavirus-infected
pneumonia in Wuhan, China. JAMA. 323:1061–1069. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Luong-Nguyen M, Hermand H, Abdalla S,
Cabrit N, Hobeika C, Brouquet A, Goéré D and Sauvanet A: Nosocomial
infection with SARS-Cov-2 within departments of digestive surgery.
J Visc Surg. 157:S13–S18. 2020. View Article : Google Scholar
|
|
6
|
Vanhems P: Fast nosocomial spread of
SARS-CoV2 in a French geriatric unit lyon study group on covid-19
infection. Infect Control Hosp Epidemiol. 41:866–867. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Elkrief A, Desilets A, Papneja N,
Cvetkovic L, Groleau C, Lakehal YA, Shbat L, Richard C, Malo J,
Belkaid W, et al: High mortality among hospital-acquired COVID-19
infection in patients with cancer: A multicentre observational
cohort study. Eur J Cancer. 139:181–187. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lai X, Wang M, Qin C, Tan L, Ran L, Chen
D, Zhang H, Shang K, Xia C, Wang S, et al: Coronavirus disease 2019
(COVID-2019) infection among health care workers and implications
for prevention measures in a tertiary hospital in Wuhan, China.
JAMA Netw Open. 3:e2096662020. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ji H, Liu L, Huang T and Zhu Y: Nosocomial
infections in psychiatric hospitals during the COVID-19 outbreak.
Eur J Psychiatry. 34:177–179. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kerwat K, Graf J and Wulf H: Nosocomial
infections. Anasthesiol Intensivmed Notfallmed Schmerzther.
45:30–31. 2010.In German. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fu C and Wang S: Nosocomial infection
control in healthcare settings: Protection against emerging
infectious diseases. Infect Dis Poverty. 5:302016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Cao GW, Zhang BX and Chen XP:
Consideration on improving public health emergency management
ability of current medical health system. Zhonghua Liu Xing Bing
Xue Za Zhi. 41:1588–1594. 2020.In Chinese. PubMed/NCBI
|
|
13
|
Gao Z, Xu Y, Sun C, Wang X, Guo Y, Qiu S
and Ma K: A systematic review of asymptomatic infections with
COVID-19. J Microbiol Immunol Infect. May 15–2020.Epub ahead of
print. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wang Y, Kang H, Liu X and Tong Z:
Asymptomatic cases with SARS-CoV-2 infection. J Med Virol.
92:1401–1403. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Li R, Pei S, Chen B, Song Y, Zhang T, Yang
W and Shaman J: Substantial undocumented infection facilitates the
rapid dissemination of novel coronavirus (SARS-CoV-2). Science.
368:489–493. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Qiu J: Covert coronavirus infections could
be seeding new outbreaks. Nature. Mar 20–2020.Epub ahead of print.
View Article : Google Scholar
|
|
17
|
Wu ZY: Contribution of asymptomatic and
pre-symptomatic cases of COVID-19 in spreading virus and targeted
control strategies. Zhonghua Liu Xing Bing Xue Za Zhi. 41:801–805.
2020.In Chinese. PubMed/NCBI
|
|
18
|
He X, Lau EHY, Wu P, Deng X, Wang J, Hao
X, Lau YC, Wong JY, Guan Y, Tan X, et al: Temporal dynamics in
viral shedding and transmissibility of COVID-19. Nat Med.
26:672–675. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kimball A, Hatfield KM, Arons M, James A,
Taylor J, Spicer K, Bardossy AC, Oakley LP, Tanwar S, Chisty Z, et
al: Asymptomatic and presymptomatic SARS-CoV-2 infections in
residents of a long-term care skilled nursing facility-king county,
Washington, march 2020. MMWR Morb Mortal Wkly Rep. 69:377–381.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Cave E: COVID-19 super-spreaders:
Definitional quandaries and implications. Asian Bioeth Rev. 1–8.
May 16–2020.Epub ahead of print. PubMed/NCBI
|
|
21
|
Stein RA: Super-Spreaders in infectious
diseases. Int J Infect Dis. 15:e510–e513. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Al-Tawfiq JA and Rodriguez-Morales AJ:
Super-spreading events and contribution to transmission of MERS,
SARS, and SARS-CoV-2 (COVID-19). J Hosp Infect. 105:111–112. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chowell G, Abdirizak F, Lee S, Lee J, Jung
E, Nishiura H and Viboud C: Transmission characteristics of MERS
and SARS in the healthcare setting: A comparative study. BMC Med.
13:2102015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Frieden TR and Lee CT: Identifying and
interrupting super-spreading events-implications for control of
severe acute respiratory syndrome coronavirus 2. Emerg Infect Dis.
26:1059–1066. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lloyd-Smith JO, Schreiber SJ, Kopp PE and
Getz WM: Superspreading and the effect of individual variation on
disease emergence. Nature. 438:355–359. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lan L, Xu D, Ye G, Xia C, Wang S, Li Y and
Xu H: Positive RT-PCR test results in patients recovered from
COVID-19. JAMA. 323:1502–1503. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Xiao AT, Tong YX and Zhang S: False
negative of RT-PCR and prolonged nucleic acid conversion in
COVID-19: Rather than recurrence. J Med Virol. 92:1755–1756. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
World Health Organization (WHO): Home care
for patients with suspected or confirmed COVID-19 and management of
their contacts. https://www.who.int/publications/i/item/home-care-for-patients-with-suspected-novel-coronavirus-(ncov)-infection-presenting-with-mild-symptoms-and-management-of-contacts.
License: CC BY-NC-SA 30IGO Accessed August 12, 2020.
|
|
29
|
Holshue ML, DeBolt C, Lindquist S, Lofy
KH, Wiesman J, Bruce H, Spitters C, Ericson K, Wilkerson S, Tural
A, et al: First case of 2019 novel coronavirus in the united
states. N Engl J Med. 382:929–936. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chen H, Guo J, Wang C, Luo F, Yu X, Zhang
W, Li J, Zhao D, Xu D, Gong Q, et al: Clinical characteristics and
intrauterine vertical transmission potential of COVID-19 infection
in nine pregnant women: A retrospective review of medical records.
Lancet. 395:809–815. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Fan C, Lei D, Fang C, Li C, Wang M, Liu Y,
Bao Y, Sun Y, Huang J, Guo Y, et al: Perinatal transmission of
COVID-19 associated SARS-CoV-2: Should we worry? Clin Infect Dis.
ciaa226Mar 17–2020.Epub ahead of print. View Article : Google Scholar
|
|
32
|
Liu Y, Ning Z, Chen Y, Guo M, Liu Y, Gali
NK, Sun L, Duan Y, Cai J, Westerdahl D, et al: Aerodynamic analysis
of SARS-CoV-2 in two Wuhan hospitals. Nature. 582:557–560. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wang J, Zhou M and Liu F: Reasons for
healthcare workers becoming infected with novel coronavirus disease
2019 (COVID-19) in China. J Hosp Infect. 105:100–101. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Sun H, Lu M, Chen S, Cheng Z, Xiong Y and
Wang X: Nosocomial SARS-CoV-2 infection among nurses in wuhan at a
single centre. J Infect. 80:e41–e42. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Bahl P, Doolan C, de Silva C, Chughtai AA,
Bourouiba L and MacIntyre CR: Airborne or droplet precautions for
health workers treating COVID-19? J Infect Dis. jiaa189Apr
26–2020.Epub ahead of print. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
World Health Organization (WHO):
Transmission of SARS-CoV-2: Implications for infection prevention
precautions. https://www.who.int/publications/i/item/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations.
License: CC BY-NC-SA 30 IGO Accessed July 9, 2020.
|
|
37
|
van Doremalen N, Bushmaker T, Morris DH,
Holbrook MG, Gamble A, Williamson BN, Tamin A, Harcourt JL,
Thornburg NJ, Gerber SI, et al: Aerosol and surface stability of
SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med.
382:1564–1567. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Guo ZD, Wang ZY, Zhang SF, Li X, Li L, Li
C, Cui Y, Fu RB, Dong YZ, Chi XY, et al: Aerosol and surface
distribution of severe acute respiratory syndrome coronavirus 2 in
hospital wards, Wuhan, China, 2020. Emerg Infect Dis. 26:1583–1591.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Chen N, Zhou M, Dong X, Qu J, Gong F, Han
Y, Qiu Y, Wang J, Liu Y, Wei Y, et al: Epidemiological and clinical
characteristics of 99 cases of 2019 novel coronavirus pneumonia in
Wuhan, China: A descriptive study. Lancet. 395:507–513. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Centers for Disease Control and Prevention
(CDC): People at Increased Risk And Other People Who Need to Take
Extra Precautions. https://www.cdc.gov/coronavirus/2019-ncov/hcp/underlying-conditions.html.
Updated January 4. 2021.
|
|
41
|
Boev C and Kiss E: Hospital-acquired
infections: Current trends and prevention. Crit Care Nurs Clin
North Am. 29:51–65. 2017. View Article : Google Scholar
|
|
42
|
Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z,
Xiang J, Wang Y, Song B, Gu X, et al: Clinical course and risk
factors for mortality of adult inpatients with COVID-19 in Wuhan,
China: A retrospective cohort study. Lancet. 395:1054–1062. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
He Y, Li W, Wang Z, Chen H, Tian L and Liu
D: Nosocomial infection among patients with COVID-19: A
retrospective data analysis of 918 cases from a single center in
Wuhan, China. Infect Control Hosp Epidemiol. 41:982–983. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
The L: COVID-19: Protecting health-care
workers. Lancet. 395:9222020. View Article : Google Scholar
|
|
45
|
Al Maskari Z, Al Blushi A, Khamis F, Al
Tai A, Al Salmi I, Al Harthi H, Al Saadi M, Al Mughairy A,
Gutierrez R and Al Blushi Z: Characteristics of healthcare workers
infected with COVID-19: A cross-sectional observational study. Int
J Infect Dis. 102:32–36. 2021. View Article : Google Scholar
|
|
46
|
McMichael TM, Currie DW, Clark S,
Pogosjans S, Kay M, Schwartz NG, Lewis J, Baer A, Kawakami V,
Lukoff MD, et al: Epidemiology of covid-19 in a long-term care
facility in king county, Washington. N Engl J Med. 382:2005–2011.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Haley RW, Culver DH, White JW, Morgan WM,
Emori TG, Munn VP and Hooton TM: The efficacy of infection
surveillance and control programs in preventing nosocomial
infections in US hospitals. Am J Epidemiol. 121:182–205. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Wang Q, Wang X and Lin H: The role of
triage in the prevention and control of COVID-19. Infect Control
Hosp Epidemiol. 41:772–776. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Huang T, Guo Y, Li S, Zheng Y, Lei L, Zeng
X, Zhong Q, Liu Y and Liu L: Application and effects of fever
screening system in the prevention of nosocomial infection in the
only designated hospital of coronavirus disease 2019 (COVID-19) in
Shenzhen, China. Infect Control Hosp Epidemiol. 41:978–981. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
McCullough PA, Eidt J, Rangaswami J, Lerma
E, Tumlin J, Wheelan K, Katz N, Lepor NE, Vijay K, Soman S, et al:
Urgent need for individual mobile phone and institutional reporting
of at home, hospitalized, and intensive care unit cases of
SARS-CoV-2 (COVID-19) infection. Rev Cardiovasc Med. 21:1–7. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Glauser W: Proposed protocol to keep
COVID-19 out of hospitals. CMAJ. 192:E264–E265. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Ramallo VJ, Rubio MM, Cuxart OE and Leoni
ME: Usefulness of Hospital at home in nosocomial infections:
Advantages and limitations. Rev Esp Quimioter. 30(Suppl 1):
S61–S65. 2017.
|
|
53
|
Borrelli E, Sacconi R, Querques L,
Zucchiatti I, Prascina F, Bandello F and Querques G: Taking the
right measures to control COVID-19 in ophthalmology: The experience
of a tertiary eye care referral center in Italy. Eye (Lond).
34:1175–1176. 2020. View Article : Google Scholar
|
|
54
|
Gong K, Xu Z, Cai Z, Chen Y and Wang Z:
Internet hospitals help prevent and control the epidemic of
COVID-19 in china: Multicenter user profiling study. J Med Internet
Res. 22:e189082020. View
Article : Google Scholar : PubMed/NCBI
|
|
55
|
Iannone P, Castellini G, Coclite D,
Napoletano A, Fauci AJ, Iacorossi L, D'Angelo D, Renzi C, La Torre
G, Mastroianni CM and Gianola S: The need of health policy
perspective to protect healthcare workers during COVID-19 pandemic.
A GRADE rapid review on the N95 respirators effectiveness. PLoS
One. 15:e02340252020. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Htun HL, Lim DW, Kyaw WM, Loh WJ, Lee LT,
Ang B and Chow A: Responding to the COVID-19 outbreak in Singapore:
Staff protection and staff temperature and sickness surveillance
systems. Clin Infect Dis. 71:1947–1952. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Agarwal A, Nagi N, Chatterjee P, Sarkar S,
Mourya D, Sahay RR and Bhatia R: Guidance for building a dedicated
health facility to contain the spread of the 2019 novel coronavirus
outbreak. Indian J Med Res. 151:177–183. 2020.PubMed/NCBI
|
|
58
|
Wang H, Mo P, Li G, Chen P, Liu J, Wang H,
Wang F, Zhang Y and Zhao Q: Environmental virus surveillance in the
isolation ward of COVID-19. J Hosp Infect. 105:373–374. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
59
|
World Health Organization (WHO): Infection
prevention and control during health care when novel coronavirus
(nCoV) infection is suspected. https://www.who.int/publications/i/item/10665-331495
License: CC BY-NC-SA 30 IGO Accessed March 19, 2020.
|
|
60
|
Centers for Disease Control and Prevention
(CDC): Interim Infection Prevention and Control Recommendations for
Healthcare Personnel During the Coronavirus Disease 2019 (COVID-19)
Pandemic. https://www.cdc.gov/coronavirus/2019-ncov/infection-control/control-recommendations.html.
Updated December 14, 2020.
|
|
61
|
Tang JW, Li Y, Eames I, Chan PK and
Ridgway GL: Factors involved in the aerosol transmission of
infection and control of ventilation in healthcare premises. J Hosp
Infect. 64:100–114. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Loeb M, McGeer A, Henry B, Ofner M, Rose
D, Hlywka T, Levie J, McQueen J, Smith S, Moss L, et al: SARS among
critical care nurses, toronto. Emerg Infect Dis. 10:251–255. 2004.
View Article : Google Scholar
|
|
63
|
Meng L, Hua F and Bian Z: Coronavirus
disease 2019 (COVID-19): Emerging and future challenges for dental
and oral medicine. J Dent Res. 99:481–487. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Wu P, Duan F, Luo C, Liu Q, Qu X, Liang L
and Wu K: Characteristics of ocular findings of patients with
coronavirus disease 2019 (COVID-19) in Hubei province, China. JAMA
Ophthalmol. 138:575–578. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Lai THT, Tang EWH, Chau SKY, Fung KSC and
Li KKW: Stepping up infection control measures in ophthalmology
during the novel coronavirus outbreak: An experience from Hong
Kong. Graefes Arch Clin Exp Ophthalmol. 258:1049–1055. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Liu Z, Zhang Y, Wang X, Zhang D, Diao D,
Chandramohan K and Booth CM: Recommendations for surgery during the
novel coronavirus (COVID-19) epidemic. Indian J Surg. 11:1–5.
2020.
|
|
67
|
Romano MR, Montericcio A, Montalbano C,
Raimondi R, Allegrini D, Ricciardelli G, Angi M, Pagano L and
Romano V: Facing COVID-19 in ophthalmology department. Curr Eye
Res. 45:653–658. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Freeman J and McGowan JE Jr: Risk factors
for nosocomial infection. J Infect Dis. 138:811–819. 1978.
View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Welt FGP, Shah PB, Aronow HD, Bortnick AE,
Henry TD, Sherwood MW, Young MN, Davidson LJ, Kadavath S, Mahmud E,
et al: Catheterization laboratory considerations during the
coronavirus (COVID-19) pandemic: From ACC's interventional council
and SCAI. J Am Coll Cardiol. 75:2372–2375. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Kampf G, Todt D, Pfaender S and Steinmann
E: Persistence of coronaviruses on inanimate surfaces and their
inactivation with biocidal agents. J Hosp Infect. 104:246–251.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
National Health Commission of the People's
Republic of China: Protocol on Prevention and Control of COVID- 19
(Edition 6). http://en.nhc.gov.cn/2020-03/29/c_78467.htm. Updated
March 29, 2020.
|
|
72
|
Lei H, Ye F, Liu X, Huang Z, Ling S, Jiang
Z, Cheng J, Huang X, Wu Q, Wu S, et al: SARS-CoV-2 environmental
contamination associated with persistently infected COVID-19
patients. Influenza Other Respir Viruses. 14:688–699. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Dancer SJ: Controlling hospital-acquired
infection: Focus on the role of the environment and new
technologies for decontamination. Clin Microbiol Rev. 27:665–690.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Wax RS and Christian MD: Practical
recommendations for critical care and anesthesiology teams caring
for novel corona-virus (2019-nCoV) patients. Can J Anaesth.
67:568–576. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Repici A, Maselli R, Colombo M, Gabbiadini
R, Spadaccini M, Anderloni A, Carrara S, Fugazza A, Di Leo M,
Galtieri PA, et al: Coronavirus (COVID-19) outbreak: What the
department of endoscopy should know. Gastrointest Endosc.
92:192–197. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Cheng VC, Chan JF, To KK and Yuen KY:
Clinical management and infection control of SARS: Lessons learned.
Antiviral Res. 100:407–419. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Casanova L, Rutala WA, Weber DJ and Sobsey
MD: Coronavirus survival on healthcare personal protective
equipment. Infect Control Hosp Epidemiol. 31:560–561. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
78
|
World Health Organization (WHO): Rational
use of personal protective equipment for coronavirus disease
(COVID- 19) and considerations during severe shortages. https://www.who.int/publications/i/item/rational-use-of-personal-protective-equipment-for-coronavirus-disease-(covid-19)-and-considerations-during-severe-shortages.
License: CC BY-NC-SA 30 IGO Accessed December 23, 2020.
|
|
79
|
Vermeil T, Peters A, Kilpatrick C, Pires
D, Allegranzi B and Pittet D: Hand hygiene in hospitals: Anatomy of
a revolution. J Hosp Infect. 101:383–392. 2019. View Article : Google Scholar
|
|
80
|
Pittet D, Allegranzi B, Sax H, Dharan S,
Pessoa-Silva CL, Donaldson L and Boyce JM: Evidence-Based model for
hand transmission during patient care and the role of improved
practices: Evidence-based model for hand transmission during
patient care and the role of improved practices. Lancet Infect Dis.
6:641–652. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Peng X, Xu X, Li Y, Cheng L, Zhou X and
Ren B: Transmission routes of 2019-nCoV and controls in dental
practice. Int J Oral Sci. 12:92020. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Pessoa-Silva CL, Dharan S, Hugonnet S,
Touveneau S, Posfay-Barbe K, Pfister R and Pittet D: Dynamics of
bacterial hand contamination during routine neonatal care. Infect
Control Hosp Epidemiol. 25:192–197. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Petroudi D: Nosocomial infections and
staff hygiene. J Infect Dev Ctries. 3:152–156. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Carlos WG, Dela Cruz CS, Cao B, Pasnick S
and Jamil S: Novel Wuhan (2019-nCoV) coronavirus. Am J Respir Crit
Care Med. 201:P7–P8. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Evans CT, Hill JN, Guihan M, Chin A,
Goldstein B, Richardson MS, Anderson V, Risa K, Kellie S and
Cameron KA: Implementing a patient education intervention about
methi-cillin-resistant Staphylococcus aureus prevention and effect
on knowledge and behavior in veterans with spinal cord injuries and
disorders: A pilot randomized controlled trial. J Spinal Cord Med.
37:152–161. 2014. View Article : Google Scholar :
|
|
86
|
Zhong BL, Luo W, Li HM, Zhang QQ, Liu XG,
Li WT and Li Y: Knowledge, attitudes, and practices towards
COVID-19 among Chinese residents during the rapid rise period of
the COVID-19 outbreak: A quick online cross-sectional survey. Int J
Biol Sci. 16:1745–1752. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Zhang M, Zhou M, Tang F, Wang Y, Nie H,
Zhang L and You G: Knowledge, attitude, and practice regarding
COVID-19 among healthcare workers in Henan, China. J Hosp Infect.
105:183–187. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Wang H, Wang S and Yu K: COVID-19
infection epidemic: The medical management strategies in
Heilongjiang province, China. Crit Care. 24:1072020. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Li T: Diagnosis and clinical management of
severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)
infection: An operational recommendation of peking union medical
college hospital (V2.0). Emerg Microbes Infect. 9:582–585. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Wang MW, Zhou MY, Ji GH, Ye L, Cheng YR,
Feng ZH and Chen J: Mask crisis during the COVID-19 outbreak. Eur
Rev Med Pharmacol Sci. 24:3397–3399. 2020.
|
|
91
|
Ali M, Wang W, Chaudhry N and Geng Y:
Hospital waste management in developing countries: A mini review.
Waste Manag Res. 35:581–592. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Yu H, Sun X, Solvang WD and Zhao X:
Reverse logistics network design for effective management of
medical waste in epidemic outbreaks: Insights from the coronavirus
disease 2019 (COVID-19) outbreak in Wuhan (China). Int J Environ
Res Public Health. 17:17702020. View Article : Google Scholar :
|
|
93
|
Awodele O, Adewoye AA and Oparah AC:
Assessment of medical waste management in seven hospitals in Lagos,
Nigeria. BMC Public Health. 16:2692016. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
World Health Organization (WHO): Infection
Prevention and Control of Epidemic- and Pandemic-Prone Acute
Respiratory Infections in Health Care. https://www.who.int/publications/i/item/infection-prevention-and-control-of-epidemic-and-pandemic-prone-acute-respiratory-infections-in-health-care
Accessed April 7, 2014.
|
|
95
|
COVID- 19 Emergency Response Key Places
Protection and Disinfection Technology Team, Chinese Center for
Disease Control and Prevention: Technical guideline for
disinfection of wastewater and wastes of medical organizations
during COVID- 19 outbreak. Zhonghua Yu Fang Yi Xue Za Zhi.
54:353–356. 2020.In Chinese.
|
|
96
|
He Y and Liu N: Methodology of emergency
medical logistics for public health emergencies. Transp Res E
Logist Transp Rev. 79:178–200. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Peng J, Ren N, Wang M and Zhang G:
Practical experiences and suggestions for the 'eagle-eyed
observer': A novel promising role for controlling nosocomial
infection in the COVID-19 outbreak. J Hosp Infect. 105:106–107.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Ye Q, Zhou J and Wu H: Using information
technology to manage the COVID-19 Pandemic: Development of a
technical framework based on practical experience in China. JMIR
Med Inform. 8:e195152020. View
Article : Google Scholar : PubMed/NCBI
|