1. Introduction
Peripheral artery disease (PAD) is characterized by
lower limb ischemia due to atherosclerotic plaque formation
(1). Critical limb ischemia
(CLI) is the most severe form of PAD and is often associated with
diabetes, age, hypercholesterolemia and smoking (2). The incidence of PAD is predicted to
increase due to the increasing rates of diabetes and obesity in the
population, together with aging (3). CLI, in fact, promotes the
development of non-healing ulcers with consequent tissue necrosis
with gangrene and rest pain. Patients with CLI are mainly treated
with surgical bypass or endovascular procedures in order to restore
perfusion, thus preventing limb amputation (4).
Notwithstanding the increase in the use of these
procedures, up to 30% of patients with CLI cannot be revascularized
and the mortality rate remains high (5). The wound healing process is
impaired in diabetic foot ulcers and plays a causative role in limb
amputations (6). In total, 75%
of amputations out of one million individuals per year are
performed on patients with type 2 diabetes mellitus (T2DM)
(7). The mechanisms of skin
wound healing impairment in T2DM remain poorly known, despite the
high incidence rate.
Recently, cell therapy has become an attractive
alternative for the treatment of patients with no-option CLI
(8-10), as well as for patients with
diabetic ulcers (8,10-12). The primary goal of cell therapy
is to induce therapeutic angiogenesis and neovascularization,
promoting collateral vessel formation, and tissue regeneration in
non-healing skin lesions (13).
The present study reviews the current state of the
cell therapy field, focusing on intra-operative autologous cell
concentrates in CLI in diabetic patients. Moreover, the clinical
indications that are moving from the no-option for
revascularization for patients with CLI to the new concept of cell
therapy as an adjuvant therapy to also increase healing in
revascularized patients are discussed.
2. Cell therapy: Unfractioned mixed cell
population concentrate or pure stem/progenitor cell
concentrate
Increasing interest in cell-based therapy for the
treatment of CLI has arisen, although there is confusion as per the
use of the term 'stem cell' therapy in clinical research, regarding
the cell population used. The term 'stem' or more appropriately
'progenitor' cell is used both for homogeneous cells produced by
culture expansion (in authorized cell factory facilities) and, in
some cases, for cell concentrates, which are heterogeneous, mixed
population, containing only a small fraction of multipotent cells
produced intra-operatory, resulting in misunderstanding and
confusion.
To correctly use the term 'stem cell therapy', the
cells should have been isolated from a pellet of cell concentrate,
followed by culture expansion or selective concentration of a pure
stem/progenitor cell population (14) and then characterized for their
self-renewal capacity, the expression of specific cell surface
markers and for their multilineage differentiation capacity
(15). In this case, the
obtained cell population can be referred to as 'mesenchymal stem
cells (MSCs) used for stem cell therapy'.
In contrast to pure MSC therapy, cell concentrates
produced intra-operatory are generally derived by point of care
devices (summarized in Table I)
and should be described as 'cell concentrate' or 'mixed cells
populations', specifying the source of tissue used, which in CLI
are commonly the following: Bone marrow (BM), adipose tissue (AT),
or peripheral blood (PB).
 | Table IPoint of care (POC) devices used to
produce autologous cell concentrate. |
Table I
Point of care (POC) devices used to
produce autologous cell concentrate.
| Tissue sources | Withdrawal volume
(ml) | Device name | Cell
populations | Procedure | Cell
characterization (Refs.) |
|---|
| Bone marrow | 60 | MarrowStim Zimmer
Biomet | MNC,
CD34+/MSC | Single use device
kit to be centrifuged | Yes (170) |
| 240 | BMAC-Terumo | MNC, CD34+/MSC | Single use device
kit to be centrifuged | Yes (171) |
| Blood and bone
marrow | 40-180 | Angel-Arthrex | cPRP | Automated system
based on centrifugation and sensors technology | No |
| 120 | Sepax | MNC, TNC | Fully automated GMP
compliant system for processing of umbilical cord blood, BM,
PB. | Yes (172) |
| Peripheral
blood | 120 | Pall
Celeris/MonoCells Athena/Hematrate Cook Regentec | MNC, TNC | Single use
selective filter-based technology on cell membrane potential. No
equipment needed. | Yes (65) |
| Adipose tissue | 100-130 | Lipogems | SVF
micro-fragmented fat | Mechanical
fragmentation through metal beads stainless steel marbles followed
by centrifugation | Yes (58) |
| 25 | Adiprep TERUMO | Nucleated Cells and
ASCs | Adipose cell
concentrates from AT centrifugation | No |
| 20 | HyTissue FIDIA | SVF
micro-fragmented fat | Adipose cell
fragmented concentrate from AT centrifugation after filtration | No |
The lack of a standardized description of cell
therapies creates confusion and difficulty of comparison between
the different basic research and published papers. Recently, the
DOSES tool was developed by International Expert Consensus to
improve standardization and transparency in describing cell
therapies (16). 'D' stands for
donor (i.e., autologous, allogenic, xenogeneic); 'O' for origin of
the tissue (i.e., BM, PB, AT, or other); 'S' for the separation
method (minimal manipulation such as centrifugation or filtration,
laboratory culture or purified through affinity separation); 'E'
for exhibited cell characteristics (including, but not limited to
the expression of cell surface markers, functional/performance
attributes); and 'S' for the site of delivery (i.e.,
intra-muscular, intravenous and intra-articular) (16).
A mixed cell concentrate, that includes a
combination of different cell types, instead of a pure population
concentrate, is easier to produce and may offer enhanced benefits,
since it provides different lineage precursors or a crosstalk
between different cell populations (17).
The aim of the present review was to summarize and
clarify the differences in tissue sources, type of cells used in
cell therapies, and to provide further clinical indications and
outcomes of current autologous cell-based therapies in CLI.
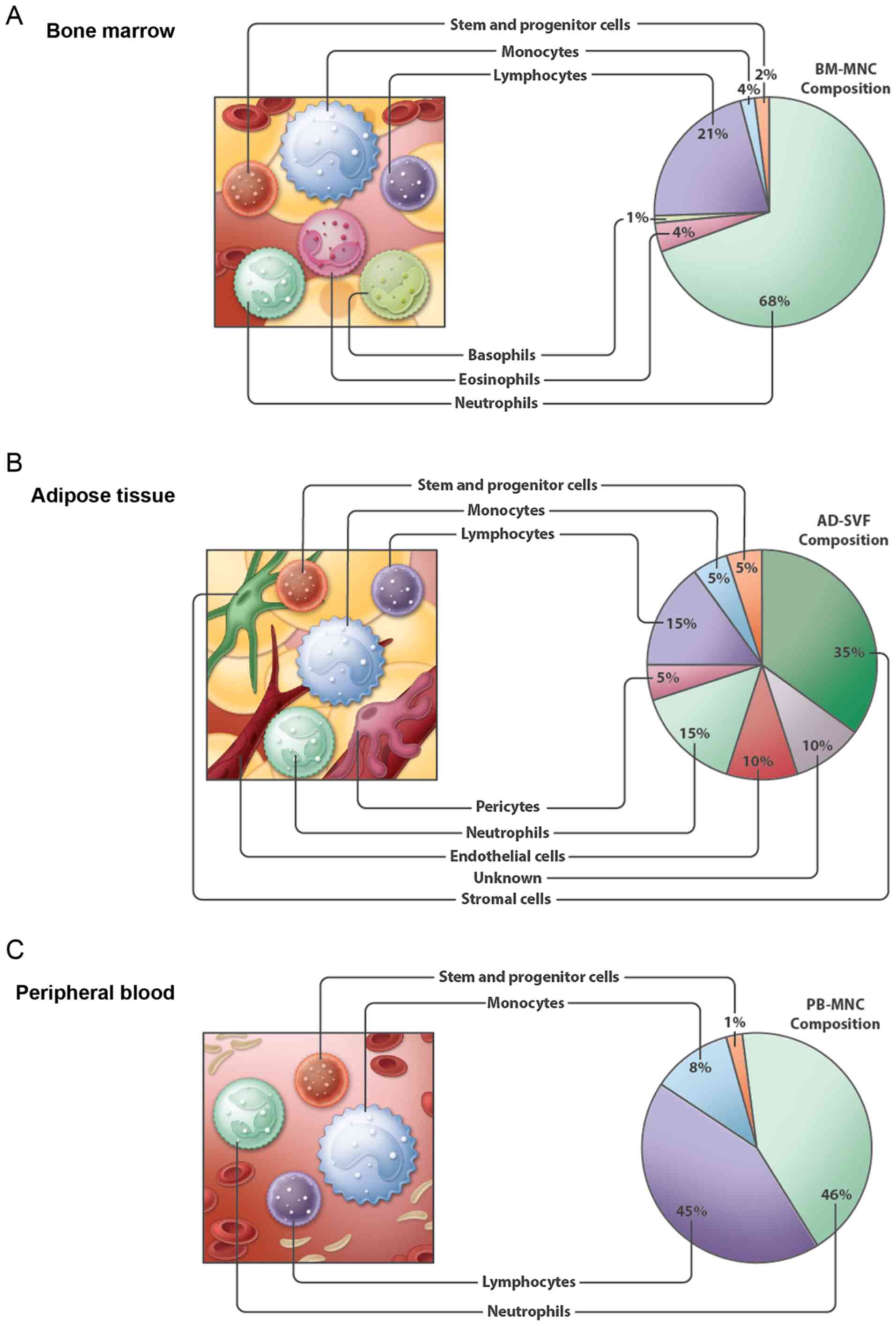
Cells derived from BM
BM contains blood cells at different differentiation
stages (18). The nucleated
cells [BM-derived mononuclear cells (BM-MNCs)] are heterogeneous
population containing endothelial progenitors cells (EPCs), MSCs
and hematopoietic stem cells (HSCs), that increase angiogenesis and
can be exploited to ameliorate poor tissue perfusion (19).
Although MSCs in BM are only a small percentage of
the total nucleated cells, they can be expanded 100- to 10,000-fold
over a period of several weeks in culture (20). As previously described, MSCs can
also be isolated from various tissue sources, including AT. BM-MSCs
were the first identified MSCs, and consequently are the most
well-characterized and have been studied extensively. MSCs for cell
therapy according to the International Society for Cellular Therapy
ISCT) criteria should be: i) Plastic-adherent fibroblastic-like
shape; ii) positive for CD90, CD73, CD105, CD34, CD11b and CD45,
and negative for HLA-DR; iii) capable of differentiating into three
mesodermal lineages: Chondroblasts, osteoblasts and adipocytes
(15).
BM-MSCs are a promising cell type for cell therapy;
however, they require in vitro culture expansion that
entails several limitations, such as high costs, two-step surgery
and safety in human treatments.
In vitro expanded cells, in fact, necessitate
genetic stability, sterility and culture expansion cytokine
removal. For this reason, they are currently under the regulatory
authorities strict guidelines for human use (21).
Conversely, BM-MNCs [also known as bone marrow
aspirate concentrate (BMAC)] can be prepared simply by BM harvest
and centrifugation in a one-step intra-operatory implant with
minimal cell manipulation (Table
I). Therefore, the BM-MNC concentrate seems to be an attractive
alternative to BM-MSCs, although it contains only a small
percentage of stem cells (Fig.
1A).
Mechanisms of action of cells derived
from BM
a) MSCs
MSCs have been the subject of scientific
investigation since their discovery in the late 1960s. The first
hypothesis was based on the migration of MSCs, following
administration, to the injury sites, their implant and
differentiation into cells capable of regenerating damaged or not
functional connective tissues. As shown by the results from
hundreds of animal studies and numerous human trials, it has become
clear that the cells do not engraft in the percentage or time to
adequately explain the results in terms of tissue replacement
(22-24). The new hypotheses indicates that
MSCs heal injured tissue by enhancing cell viability and/or
proliferation, reducing cell apoptosis and sometimes modulating the
immune responses (25). The
healing capacity of MSCs is based on paracrine activity through
secreted growth factors, cytokines, hormones, extracellular
vesicles (i.e., exosomes) containing peptides/proteins, mRNAs and
microRNAs (miRNAs or miRs), that may have immunomodulatory and
anti-inflammatory effects and pro-survival effects (25). Recently, it was demonstrated that
the success of MSC therapy is not due to cell engraftment and
replacement efficiency (26).
MSCs modulate the local immune responses and facilitate tissue
repair through a paracrine release, but do not reconstitute damaged
tissue.
Since MSCs are environmentally sensitive, improving
their biological activities will help to ameliorate their
therapeutic features (27).
Therefore, it is important to define the environment in which they
are implanted in order to avoid unexpected behaviors (28). Moreover, successful therapies
should take the paracrine effects of MSCs into account (29,30). Indeed, it has been shown that
inflammation modulates the multilineage potential,
immunomodulation, the immunophenotyped and hematopoietic features
of MSCs, and should be tightly controlled in cell therapy in order
to increase efficiency (26).
For example, in ischemic tissue, despite limited
cell survival, BM-MSCs secrete higher levels of vascular
endothelial growth factor (VEGF) compared to fibroblasts, thus
angiogenic properties of MSCs occur through paracrine and autocrine
effects, and depend on tissue source (31).
As previously demonstrated, the administration of
MSCs or conditioned media does not improve revascularization
immediately, but only when administered one day following the
induction of ischemia in a mouse model (32). Thus, inflammatory processes
impair the therapeutic efficacy of MSCs, and administration timing
has been proven to be crucial (26,33,34).
The 'immune centric revolution' or 'immune centric
approach' suggests that the regenerative capacity of stem cells is
controlled and orchestrated by the local immune system consequently
to tissue damage, with macrophages being the main actors and
coordinators of the injury response, able to promote endogenous
repair (35). It has recently
been demonstrated that the immune system plays a critical role in
tissue healing in addition to stem cells and growth factors
(36). Actual regenerative
strategies may be reinforced by the control of the immune-mediated
tissue repair and regeneration mechanisms as an alternative to stem
cells and growth factors therapies (37). Immune cells have recently emerged
as key components of the niche microcosm and prominent effectors of
stem cell behaviors (37).
During tissue damage, stem cells communicate with the frontline of
resident immune sentinels to organize the response: Immune
effectors, as monocyte/macrophages, quickly enter from circulation,
infiltrating the stressed tissue to remove pathogens, to start the
repair process and restore homeostasis. Briefly, stem cells sense,
communicate with, and co-opt resident immune cells to preserve the
tissue homeostasis (37).
MSCs are positively regulated by macrophages.
Indeed, it has been demonstrated in vitro that MSC
proliferation, vitality and paracrine functions are improved by
macrophage-derived growth factors (38). Indeed, the crosstalk between
macrophages and MSCs is not unidirectional. Implanted MSCs provoke
a shift to an anti-inflammatory M2-like macrophage phenotype (see
paragraph below entitled 'a) Monocytes/macrophages' under
'Mechanisms of action of cells derived from PB') in different
tissues, such as the injured myocardium (33).
Hypoxia has been shown to decrease both M1 to M2
macrophage transition and anti-inflammatory interleukin (IL)-10
macrophage production, suggesting a possible reduced therapeutic
effects of bone marrow MSCs in a hypoxic environment (39).
b) BM-MNCs
The implantation of autologous BM-MNCs into ischemic
skeletal muscles has been proven successful in developing
angiogenesis and collateral vessel formation in human trials
(40-42). The mechanisms of angiogenesis by
BM-MNC implantation have been evaluated in several studies,
suggesting that the differentiation of BM-MNCs into endothelial
cells (ECs) is a rare condition in skeletal muscle tissues
(43). However, cytokines and
chemokines released from MNCs are able to activate pre-existing EC
sprouting through either a direct or an indirect mechanism. It has
been demonstrated that cytokines released from BM-MNCs implanted in
ischemic sites are the main players in angiogenesis induction
(44) (Fig. 2).
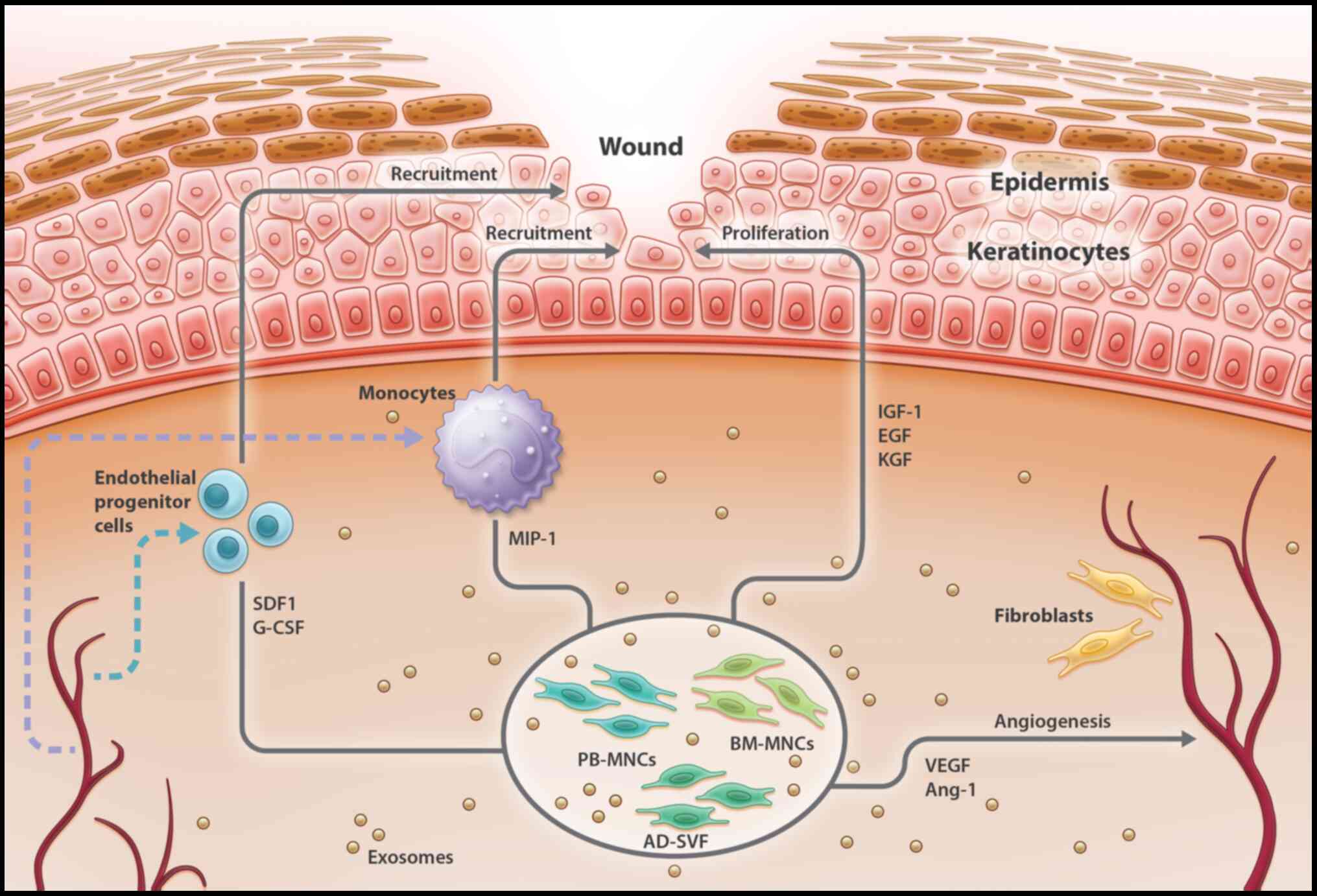 | Figure 2Paracrine effects of different
autologous cell therapies in diabetic foot ulcers healing. This
figure summarizes the paracrine effects of different sources used
for cell therapies: PB-MNCs, BM-MNCs and AD-SVF. These cells are
administered intramuscular or intra-arterial and act through
paracrine mechanisms that target different tissue cells
(endothelial cells, keratinocytes, fibroblasts and monocytes)
indicated in the figure, concurring to the amelioration of wound
healing. In a cutaneous wound the administered cells release
cytokines and chemokines that enhance EPCs and monocytes
recruitment into the wound, keratinocyte, fibroblast proliferation
and angiogenesis. Additionally, healing capacity is accelerated by
paracrine activity of exosomes secreted by all cellular types
allowing intercellular communication. BM-MNCs, bone marrow-derived
mesenchymal cells; AD-SVF, adipose-derived stromal vascular
fraction; PB-MNCs, peripheral blood mononuclear cells; Ang-1,
angiopoietin-1; EGF, epidermal growth factor; EPC, endothelial
progenitor cell; G-CSF, granulocyte colony-stimulating factor;
IGF-1, insulin-like growth factor 1; KGF, keratinocyte growth
factor; MCP-1, monocyte chemoattractant protein 1; MIP-1,
macrophage inflammatory protein-1; SDF1, stromal cell-derived
factor-1; VEGF, vascular endothelial growth factor. |
Moreover, the acute phase of ischemia is the optimum
stage for cell-based therapeutics with BM-MNCs, because of the
robust upregulation of IL-1β expression, and a consequent positive
effect on the angiogenic potential of BM-MNCs (45).
Cutaneous wound healing is a multi-step complicated
process in which the skin repairs itself after injury. BM-MNCs
participate in this process with various cell populations, such as
MSCs, inflammatory cells, fibrocytes, and not only release
cytokines, promoting wound repair, but also differentiate into
keratinocytes and dermal myofibroblasts (46). BM-MNCs in fact, release
endothelial growth factor (EGF), insulin growth factor (IGF-1) and
keratinocyte growth factor (KGF) to promote keratinocyte
proliferation. VEGF, angiopoietin 1 (Ang-1) and macrophage
inflammatory protein (MIP)-1, which are all proangiogenic
cytokines, recruit monocytes in the wound, while stromal-derived
factor 1 (SDF-1) and granulocyte-colony stimulating factor (G-CSF)
secretion recruit EPCs (46)
(Fig. 2).
In a macrophage depleted mouse model, it was
demonstrated that the major contribution of BM-MNCs to wound
healing was linked to the proangiogenic effects of macrophages
contained in the BM (47).
Finally, BMNCs act as a repair source, by supporting
angiogenesis and vasculogenesis, and producing several growth
factors through a paracrine effect (17,19,40,48) (Fig. 2). Similar to MCSs, BM-MNCs also
act via different mechanisms; however, it is not clear which BM-MNC
cellular population is optimal for CLI treatment (49,50).
Cells derived from adipose tissue
There are two classes of cells in the AT: Stromal
cells also known as the stromal vascular fraction (SVF) and mature
adipocytes (MAs), the major component of the AT volume.
According to the ISCT and the International
Federation of Adipose Therapeutics and Science (IFATS), the main
cell types in the AD-SVF are blood and stromal cells, such as red
cells, platelets, ECs and EPCs, a heterogeneous population of
nucleated cells, including leukocytes (CD45+),
lymphocytes (CD4+) and monocytes/macrophages
(CD14+) (51-53) (Fig. 1B). The SVF also contains
multi-potent mesenchymal stem/progenitor cells able to
differentiate into, chondrocytes, osteoblasts, myocytes,
adipocytes, pericytes and fibroblasts (14). Indeed, it has been reported that
AT contains adipose-derived regenerative cells (ADRCs) and
adipose-derived stem/progenitor cells (ADSCs), which are
multipotent mesenchymal stem cells, able to regenerate damaged
tissues (54).
ADSCs are becoming important in the field of
regenerative medicine and stem cell research. However, the
isolation of ADSCs requires extensive manipulation, consisting of
an in vitro selection following a collagenase digestion of
the adipose derived stromal vascular fraction (AD-SVF) and an
expansion process, that prevents an immediate use in the clinical
practice. ADSCs are more suitable than BM-MSCs in the clinical use
since the AT can be repeatedly obtained by liposuction, a
well-established and minimally invasive procedure (50). Moreover, the AT stem cell
concentration is approximately 500-fold greater than the
concentration obtained from an equivalent amount of BM aspirate
(55).
In contrast to ASCs, the AD-SVF represents a
minimally processed cell population which can be used immediately
(14). However, the term ADSC is
sometimes improperly used to refer to AD-SVF, increasing confusion
in clinical results of stem cell-based therapies (56).
Moreover, it has been proven that harvesting site,
lipo-aspiration, and reinjection techniques strongly influence the
quality of AD-SVF cells (57)
and should be considered when using an AT-based cell-therapy.
AD-SVF cell therapy has been proposed as a novel
therapy for damaged tissue regeneration and repair. Since fat
tissue is abundant, easy to isolate, and rich in stem/progenitor
cells able to secrete angiogenic growth factors, AT-based therapy
has been considered one of the favorite candidates for non-healing
wounds. For this reason recently, point of care devices have been
placed on the market for the production of micro-fragmented adipose
tissue (58), also known as the
nanograft and adipose cells concentration systems that contain
AD-SVF (Table I).
Mechanisms of action of cells derived
from adipose tissue
The therapeutic efficacy of the AD-SVF is based on
immunomodulatory, anti-inflammatory regenerative and angiogenic
effects, and on the interaction of different cell populations
present in the AD-SVF (Fig.
2).
A superior angiogenic effect of fresh AD-SVF
compared to cultured ADSCs has been observed, in mice with hindlimb
ischemia (59). In vitro,
ASCs secrete higher levels of VEGF, hepatocyte growth factor and,
transforming growth factor (TGF)β (60) compared to BM-MSCs, and exhibit a
greater vascularization potency in a mouse model of hindlimb
ischemia (61).
The nucleated cell therapeutic potential of AD-SVF
is largely unknown. Recently, the AT-resident monocyte role in
tissue vascularization has been shown (62). Regarding the angiogenic cell
population present in the adipose tissue, it has been shown that
SVF monocytes (CD14+) are more efficient in inducing
angiogenesis than ADSCs derived from AD-SVF, suggesting that
adipose monocytes may represent a new angiogenesis cell-based
therapy (62).
Of note, these data are in line with the observation
that macrophages in fat grafts are strongly responsible for tissue
regeneration (63). The
depletion of macrophages impairs strongly fat graft survival and
angiogenesis, reduces stem cell recruitment, as well as, the rate
of retention. Conversely, an upregulation/activation of macrophages
allows survival and angiogenesis increase, indicating that
macrophages are crucial for tissue revascularization and
regeneration (63).
Pericytes of AD-SVF regulate vessel stability and
vascular contractility (64), by
contributing to angiogenesis, promoting EC survival and endothelial
spreading (Fig. 2). Thus far,
the AD-SVF nucleated cells clinical outcome is not known when
implanted in subcutaneous tissue in humans. The paracrine effects
of cytokines released by AD-SVF cells can be innovative, and is
strictly associated to cell survival in the implanted tissue
(52).
Accordingly, it has been shown that SVF cells mainly
contain blood-derived cells, ADSCs, and ECs (Fig. 1B), and most of them do not
survive 4 days following transplantation, although CD34+
ADSCs remain viable after 14 days when implanted in ischemic tissue
(64).
Cells derived from PB
PB-MNCs used in autologous cell therapy are a
heterogeneous population composed of both CD34−
(lymphocytic and monocytic) and CD34+ HSCs and EPCs
(Fig. 1C) (65).
The therapeutic properties of the MNC population
were initially attributed to the CD34+ EPC component,
since EPCs are considered to be protective in both acute and
chronic vascular injury (66).
EPCs present in the adult human PB CD34+ stem-cell
population play a major role in postnatal neo-vascularization
following BM mobilization (48).
The immune system, as already described, is fundamental in tissue
homeostasis, development, and wound repair. Immune system cells and
secretomes are able to repair damaged tissues (67-70) as observed by Metchnikoff in the
late 1800s (71). Recent studies
have confirmed earlier observations and have demonstrated that the
immune system regulates and control tissue regeneration (35-37,72). Since then, our
understanding of immune cell role in tissue regeneration, in
particular macrophages and T-lymphocytes, has improved (67,72). Moreover, PB-MNCs can be produced
easily by point of care system based on selective filtration
(65) (Table I).
Mechanisms of action of cells derived
from PB
Initially, EPCs were considered the only BM-derived
cells capable to differentiate into vascular endothelium and to
induce angiogenesis. Therefore, PB that contains only a small
fraction of EPC compared to BM, were used following mobilization
with G-CSF in order to increase the stem cells concentration in PB
(73).
It is now clear that both monocytes and the
lymphocyte itself, forming the PB-MNC mixed cell concentrate, are
also involved in angiogenesis (74,75), arteriogenesis (76) and in tissue regeneration
(77,78).
The angiogenic potency of human PB-MNCs isolated by
a selective filtration-based point-of-care device has been proven
both in vitro and in vivo (65). Human PB-MNCs isolated secrete a
panel of angiogenic molecules and are capable of migrating in
response to SDF-1 and VEGF gradient. It has been shown that PB-MNC
injection induces neovascularization (i.e., capillary, arteriole
and regenerative fiber numbers increase) upon hindlimb ischemia in
mice (65). Notably, human
PBMNCs can be detected in the murine ischemic tissue after 7 days.
A similar effect has been shown in a in vivo potency assay,
using BMNCs in comparison with expanded bone marrow cells enriched
in CD90+ stem cells (79).
In agreement, PB-MNCs exhibit a comparable or
superior angiogenic capacity to that of BM-MNCs in a hindlimb
ischemia mouse model, suggesting that EPCs do not play a pivotal
role in the PB-MNC mediated limb ischemia treatment (80). Due to these considerations, an
increasing number of clinical studies are using non mobilized
PB-MNCs for the treatment of CLI (75,81-84).
a) Monocytes/macrophages
The marked angiogenic and arteriogenic ability of
monocytes is well described and known for years (85-87).
Studies on the role of monocytes in arteriogenesis
have been accomplished since 1970. Schaper et al described
that monocytes adhere to ECs using electron microscopy (88). Subsequently, different studies
demonstrated that monocytes are recruited to the collateral artery
during arteriogenesis in rabbit and murine models of hindlimb
ischemia (85,89). Moreover, mice with monocyte
deficiency exhibit decreased blood flow and arteriogenesis upon
femoral artery ligation compared to the controls (90). Monocyte recruitment requires the
presence of chemokines, such as monocyte chemoattractant protein-1
(MCP-1), that is overexpressed in hypoxic tissue. Monocyte
recruitment to ischemic sites induces angiogenesis in a
MCP-1-dependent manner, suggesting a physiological and
homo-functional role of monocytes in neovascularization (17,87). It has been shown that MCP-1
injection provokes collateral artery growth, as well as, monocyte
accumulation around the arterial walls in ischemic porcine and
rabbit and hindlimb ischemia, suggesting that monocyte recruitment
is a required condition for high collateralization, thus explaining
monocyte accumulation in targeted vessels (91).
Monocytes and macrophages play a key role in
promoting a collateral circulation following arterial occlusion
through the production of proangiogenic factors and the formation
of a vascular plexus by bridging to sprouting ECs (92). Recently, it has been shown in
live imaging that macrophages are immediately recruited to the
wound area after injury and are strongly involved in the entire
repair phase (74) (Fig. 2). Moreover, macrophage ablation
results in impaired neoangiogenesis. It has been recently observed
that inflammatory macrophages are sufficient to drive vessel
sprouting via VEGF signaling during wound repair (74).
Macrophages form primitive, non-endothelial
'vessels' terned vascular mimicry (VM) channels, structurally and
functionally connected to the systemic vasculature and that hypoxia
is an important mediator of VM formation (93).
In 2016, an unexpected role of macrophages in the
repair of brain vascular ruptures was described, where macrophages
mediated the repair by adhesion and mechanical forces creation
(94). In that study, the
authors suggested that this mechanism was potentially conserved to
PB vessel repair. Another study demonstrated that macrophages from
recruited monocytes promoted arteriogenesis and tissue repair
following ischemia (76).
Macrophages promote angiogenesis by secreting
pro-angiogenic factors and modulating angiogenesis via cell-to-cell
contacts with ECs, that promote the differentiation of
pro-angiogenic macrophages (95). Macrophages and ECs communicate
through secreted microvesicles, such as exosomes, in the
angiogenesis process (95)
(Fig. 2).
Apart from the angiogenic and arteriogenic ability,
monocytes are involved in tissue regeneration via soluble factors
(96-99), also in diabetic lesions (100-102). Tissue macrophages increase
following injury, due to active monocyte recruitment from PB and to
their differentiation into macrophages (103). Physiological wound healing
consists of three phases: i.e., Acute inflammation,
angiogenesis/proliferation and remodeling. Monocytes/macrophages
are the cells majorly required during the wound healing process and
can polarize either into the M1 (inflammatory) or in M2
(anti-inflammatory) phenotype, depending on specific signals during
tissue recruitment (98,104,105).
During the process of wound healing, macrophages
evolve with the stages. In the normal healing process, the
macrophage population switches from a pro-inflammatory (M1) to an
anti-inflammatory phenotype (M2), promoting the migration and
proliferation of fibroblasts and keratinocytes to repair cutaneous
tissue. Moreover, in this phase, the proliferation of ECs to repair
vasculature is also observed. By contrast, in chronic wounds and
diabetic wounds, macrophages retain a pro-inflammatory
characteristic, and the ulcers remain indefinitely in the first
inflammatory stage of wound healing (98).
b) Lymphocytes
Apart from monocytes, lymphocytes are also relevant
to adult vascular repair. T-lymphocytes play a key role in
collateral vessel formation as suggested by the
CD4+-T-helper lymphocyte knockout murine model (106). Indeed, in
CD4+-deficient mice, reduced numbers of
monocytes/macrophages have been observed in the ischemic muscles;
thus, a crosstalk between monocytes and T-lymphocytes is required
(106).
Pre-stimulated T-cell monocytes induce
neovascularization in hindlimb ischemia in mice, suggesting that
monocytes may be used as novel potential candidates for
regenerative cell therapy in patients with PAD (107). It has been shown that
CD4-knockout mice have an impaired arteriogenic response to acute
hindlimb ischemia (108) and
that CD8+ T-lymphocytes are necessary for arteriogenesis
and for CD4+ cell recruitment via the release of IL-16
expression (109). Zouggari
et al confirmed that regulatory T-cells (Tregs) are
important for neovascularization following ischemia (110), and that natural killer cells
also play a role in angiogenesis by the secretion of interferon-γ
(111).
There are significantly more CD4+ Th1
cells, but fewer Tregs in ischemic tissues from patients with T2D
than from normoglycemic patients with PAD (112). It has been shown that Th1 cells
impair vascular regeneration in individuals with T2D in a paracrine
manner, while Tregs potentiate regeneration (112). Recently, it has been observed
that Treg lymphocytes are able to polarize macrophages and activate
satellite cells in ischemic tissue (113).
Further studies are required to ameliorate and
strengthen Treg function in tissue regeneration for clinical use
(70).
c) CD34+ cells and
EPCs
The therapeutic benefits of administering
CD34+ cells to patients with CLI have been largely
attributed to the angiogenic capacity of EPCs. The discrepancy in
treatment outcome of using CD34+ cells in previous
studies may refer to the fact that EPCs comprise only a minor
percentage of CD34+ cells that also include several
subpopulations of HSCs. In fact, EPCs account for merely 1% of all
circulating MNCs (114)
(Fig. 1C).
The percentage of circulating EPCs that are able to
differentiate in ECs and form collateral vessel formation is very
small (115). Moreover, the
pro-angiogenic role of circulating EPCs is based on paracrine
effects and not on differentiation into ECs (116).
The true EPCs are CD14+CD34 low cells and
are effectively able to differentiate in ECs in vitro but
their role in vivo is not confirmed (117). Conversely, the co-culture of
CD34+ cells with CD34− cells induces a strong
neovascularization improvement in vitro compared to that
with only CD34+ cells, indicating that a mixed MNC
population behaves more efficiently than purified CD34+
cells (118).
This result was also observed in clinical trials
where mixed PB-MNCs induced a better therapeutic effect compared to
pure CD34+ cells (119).
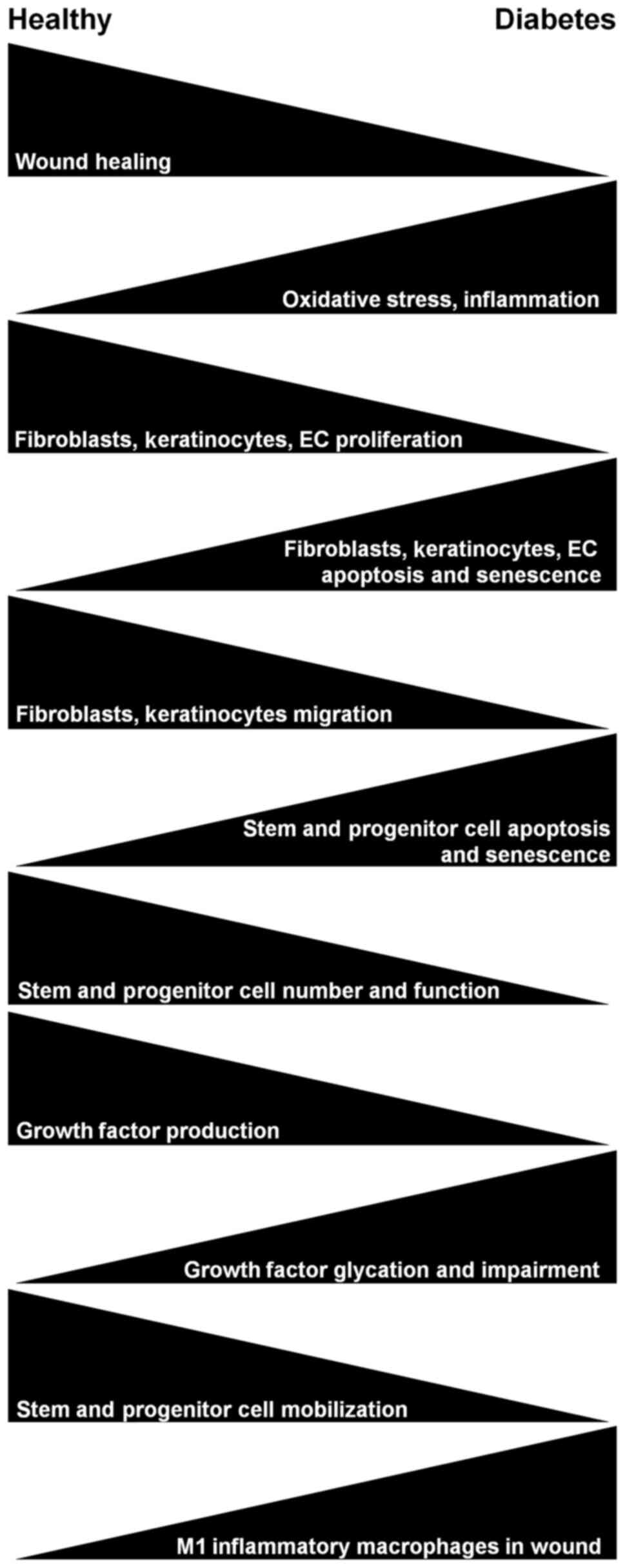
3. Diabetes impairs the angiogenic and
regenerative capacity of autologous cell therapy
T2DM induces a shortage of vascular regenerative
cells and angiogenic capacity, increasing the risk of
cardiovascular diseases. T2DM causes several impairments that delay
wound healing (Fig. 3) and also
affects the autologous cell therapy of the different cell
population deriving from BM, AT and PB (summarized in Table II).
| Table IIEffects of T2DM on different sources
of autologous cell concentrate. |
Table II
Effects of T2DM on different sources
of autologous cell concentrate.
| Autologous cell
concentrate source | Effects of
T2DM | (Refs.) |
|---|
| Bone marrow | Reduced stem cell
mobilization | (120-122) |
| Decreased EPC
number | (123,124,126) |
| Reduced
CD34+ and EPC sensitivity to hypoxia | (127) |
| Hostile
microenvironment for resident SCs, induced by microvessels, sensory
neuron rarefaction, fat accumulation | (122) |
| Reduction of
angiogenic factors (VEGF, SDF-1, HIF1α), functional impairment of
growth factors | (122,125) |
| Decreased wound
macrophages number and increased M1 polarization | (7) |
| Adipose tissue | Reduced ADSC
production of growth factors | (134) |
| Reduced ADSC
angiogenic potential due to depletion of subpopulations | (66) |
| ADSC dysfunction
due to apoptosis and impaired autophagy | (141) |
| Vascular smooth
muscle cell and pericyte dysfunction | (122) |
| Peripheral
blood | Reduced
CD34+ proliferation, migration, production of growth
factors and sensitivity to hypoxia | (127) |
| Reduced monocyte
migration towards VEGF-A | (128) |
In fact, T2DM causes functional BM impairment
(120). Indeed, in response to
G-CSF, the mobilization and angiogenic ability of CD34+
cells is increased in healthy subjects, but not in patients with
T2DM (121,122). Therefore, in T2DM, tissue
repair is impaired, increasing the possibility of cardiovascular
complications (122).
Moreover, T2DM is also associated with a decrease in
BM-derived EPCs, compromising their mobilization, recruitment and
function due to increased apoptosis (123,124). It has been shown that in T2DM,
there is also a reduction of angiogenic factors, i.e., VEGF, SDF-1,
HIF1α, necessary for the recruitment of PB-MNCs to ischemic sites
in T2DM (122);
post-translational modifications such as glycation can modify
growth factor angiogenic capacity; indeed, fibroblast growth
factor-2 (FGF-2) glycation inhibits the angiogenic capacity
compared to unmodified FGF-2 (125).
Notably, BM-derived EPCs from diabetic mice have
been shown to exhibit a decreased ability to induce capillary
density formation in vivo. Furthermore, EPCs derived from
p66Shc knockout mice display less oxidative stress in diabetes and
behave like wild-type EPCs (126). These data demonstrate that the
diabetic EPC impairment of angiogenic properties and survival is
partially associated with increased oxidative stress and decreased
nitric oxide (NO) bioavailability (126).
Furthermore, EPCs derived from diabetic patients do
not respond to hypoxia and display an impairment in paracrine
function and in angiogenic potential (127). Indeed, CD34+ cells
of patients with T2DM release lower concentrations of hepatocyte
growth factor, stem cell factor, thrombopoietin and HIF1α, whereas
they release higher levels of inflammatory cytokines (i.e.,
TNF-alfa and IL-1β) compared to CD34+ cells from healthy
subjects. As a consequence, these cells demonstrate an impairment
in migration under hypoxic conditions, as well as a vasoreparative
dysfunction (127).
By contrast, T2DM monocytes are less affected than
CD34+ stem cells (102). A comparative study of the
angiogenic potential of CD34+ stem cells or
monocytic-like (CD14+) endothelial progenitors of
PB-MNCs in diabetes demonstrated that monocytic progenitors
stimulate vascular growth and healing in diabetes, although not as
rapidly or effectively as CD34+ cell treatment (102). Thus, in diabetic conditions
with compromised CD34+ cells, CD14++ cells
can provide a good therapeutic option. Most probably,
CD14+ cells mediate healing, since they exhibit an
increased sensitivity to MCP-1 and VEGF, by their capacity to
induce angiopoietins in diabetic patients (102).
Conversely, another demonstrated that monocytes
have a reduced migratory ability towards VEGF-A in patients with
T2DM (128). The increase in
oxidative stress and advanced glycation end products in diabetic
monocytes induces VEGFR-1 signaling pathway activation, leading to
a desensitization of the VEGFR-1 response. Furthermore, monocytes
in a T2DM contest are dysfunctional and exhibit a VEGF resistance,
causing cellular dysfunction (128).
T2DM-affected wounds are characterized by an
increase in inflammation due to the excessive presence of M1
macrophages (129,130), probably due to hyperglycemia
and the dysregulation of hematopoietic stem cell differentiation
towards macrophages.
During the inflammatory initial phase of wound
healing, macrophages display both M1 and M2 phenotypes, although in
healed wounds, the predominant switch is towards the M2 phenotype
in the proliferative phase. In diabetic and chronic ulcers, this
switch is highly reduced (7,131).
It has been demonstrated that the higher
recruitment of monocytes/macrophages in a muscle lesion polarizes
the inflammatory M1 into the anti-inflammatory M2 phenotype,
inducing myogenic differentiation and repair (132). Furthermore, as previously
demonstrated, in a diabetic wound not healed after 2 months from
revascularization, the PB-MNC implant leads to efficient
angiogenesis, the inhibition of the inflammatory marker, NF-κB, and
polarizes macrophages from the M1 to the M2 phenotype, inducing a
complete healing (133).
Recently, it was observed that a novel epigenetic
mechanism in diabetic HSCs causes macrophage number decrease and
their polarization towards M1 (7). Diabetes has been demonstrated to
impair adipose tissue-derived stem cell wound healing capacity in
mice (134). ADSCs from
diabetic patients exhibit a reduction in VEGF secretion and
proliferation, as well as an impaired angiogenic capacity (66,135,136).
4. Clinical trials in no-option
patients
In 15-20% of patients with CLI, revascularization
is not possible or not effective, with a consequent increased risk
of major amputation. This condition is defined as no-option CLI, it
is most frequent in diabetic patients and also in patients with
end-stage renal disease, who could have heavily calcified arteries
below the knee and below the ankle.
Over the past decade, various meta-analyses on cell
therapy in no-option patients have been published mainly on BM-MNCs
and PB-MNCs, including both patients with arteriopathy and diabetic
patients with CLI.
Benoit et al evaluated 45 clinical trials,
of which 7 were randomized for a total of 1,272 treated patients
with a significant reduction in amputations in patients treated
with autologous cell therapy (PB-MNC and BM-MNC) compared to
patients treated with medical therapy (137). Liew et al, in a
meta-analysis of 16 randomized and controlled trials (RCTs)
considering 774 patients, reported a significant reduction in major
amputations, a complete healing of the lesions, and an increased
ankle arm index (ABI) (138).
Both PB-MNCs and BM-MNCs significantly reduced the risk of major
amputation. PB-MNCs also significantly improve wound healing.
Jiang et al defined wound healing as the
primary end-point in a meta-analysis on RCTs (139). Autologous cellular therapies
with BM-MNCs or PB-MNCs were significantly associated with improved
wound healing in 12 clinical studies of 290 patients. No
differences in wound healing were found between BM-MNCs and
mobilized PB-MNCs, and autologous cell therapies were not
associated with any increased risk for side-effects (139).
Ai et al analyzed 25 trials that included
both PB-MNCs and BM-MNCs, and reported that cell therapy
significantly reduced the amputation rate and increased
amputation-free survival (AFS) (140). Cell-based therapy significantly
ameliorated the ABI, increased the rate of ulcer healing and
transcutaneous oximetry (TcPO2), reducing limb pain and
improving the movement. No significant association between the
injected cell number and the therapeutic effect has been described
(140).
Rigato et al performed a meta-analysis on 19
RCTs (837 patients), 8 non-randomized trials (338 patients) and 41
uncontrolled studies (1,177 patients), including studies with
BM-MNCs and PB-MNCs, mobilized and non-mobilized in patients
without indications for revascularization (8). However, Rigato et al
(8) observed that considering a
limited number of studies with a better quality of controls, there
was a very poor effect of cell therapy. The primary analysis of
RCTs revealed that cell therapy significantly reduced the risk of
amputations by 37%, improved amputation-free survival by 18% and
increased the rate of ulcer healing by 59%. Furthermore, cell
therapy significantly improved the ABI, TcPO2, pain free
walking distance and reduced pain at rest. The analysis on non-RCTs
revealed that cell therapy can prevent amputation even in 50% of
treated patients (8).
When different cell types were compared, the
meta-analysis also revealed that PB-MNCs, but not other cell types,
significantly decreased the amputation rate and the AFS (8). BM-MNCs only significantly improved
wound healing, whereas both BM and PB-MNCs significantly
improvedthe ABI, TcPO2 and the rest pain score (8). Accordingly, Peeters Weem et
al, in a meta-analysis of placebo controlled trials,
demonstrated that BM-derived cell therapy did not give any
advantage on the primary outcome survival, measures of amputation
and AFS in CLI-affected patients (141).
In the MOBILE randomized double-blind study, 152
patients (155 limbs) with Rutherford 4 or Rutherford 5 critical
limb ischemia were randomized to receive an injection of BM-MNCs or
the placebo (142). At one
year, there was no significant difference in the rate of AFS
between the two groups. However, a post hoc analysis at two years
revealed that there was a significant difference between the BM-MNC
group and the placebo, with a hazard ratio of 0.49 in favor of cell
therapy at 52 weeks. The analysis also revealed that while BM-MNCs
did provide a significant benefit for patients without diabetes at
Rutherford stage 4, they did not provide any benefit for diabetic
patients and/or those with Rutherford stage 5. Therefore, these
results would suggest a negative impact of diabetes on BM-MNC
therapy for peripheral ischemia.
Accordingly, a retrospective study on 367 patients
revealed that Rutherford's stage 5 was the best indication for
autologous cell therapy in PAD; 50% of Rutherford's stage 6
patients who initially had major tissue loss, overstepping
metatarsus phalangeal level (Rutherford's stage 6), all went
through a major amputation, suggesting that treatment was performed
in a too advanced stage in some patients (143).
In a recent meta-analysis on a limited number of
cases (7 studies on 224 patients) of diabetic foot with lesions
classified by the Wagner scale, Shu et al demonstrated a
benefit of autologous cell therapies on both complete and partial
healing of injuries (144).
Guo et al, in a meta-analysis including 6
eligible RCTs on diabetic foot treatments, revealed that autologous
stem cell administration (one study with BM-MSCs, two studies with
BMMNCs, one with PBMNCs, one with BNMNC enriched in
CD90+ cells, and one with SVF) was significantly
effective in ulcer healing. Subgroup analyses indicated that stem
cells exerted beneficial effects on ulcer sizes of ≥5
cm2 and <5 cm2, as well as cell on
patients aged ≥70 years and <70 years, suggesting a positive
role for stem cells in the treatment of diabetic foot ulcers
(145).
Recently, a systematic review and meta-analysis on
27 RCTs, involving 1,186 patients and 1,280 limbs, revealed that
autologous stem cell therapy (including BM-MSCs, BM-MNCs, PB-MNC,
CD34+ cells and CD133+ cells), ameliorated
clinical outcomes in terms of the ulcer healing rate, ABI, pain
free walking distance improvement, amputation rate and rest pain
score reduction, but not in major limb salvage improvement,
compared to conventional therapies (146). On the other hand, cell therapy
reduced amputations and increased the ulcer healing rate in
diabetic patients. Larger double-blinded, randomized,
placebo-controlled, multi-center trials with the long-term
follow-up of high quality are warranted to confirm efficacy and
safety of autologous cell therapy for PAD (146).
As regards the use of cellular therapies from AT in
the treatment of CLI, there are only limited studies on animal
models (147) and a limited
number of clinical trials.
The first clinical study by Lee et al
included 12 thromboangiitis obliterans (TAO), 3 diabetic patients
with PAD with ischemic resting pain in one limb with/without
non-healing ulcers and necrotic foot treated by multiple
intramuscular ASC injections (148). Of note, the stromal vascular
fraction of diabetic patients and TAO produced lesser colonies
compared to SVF obtained from abdominal liposuction of 3 healthy
donors in a colony forming unit assay (148). Moreover, SVF from diabetic
patients exhibited a lower proliferative ability than the SVF from
TAO and healthy patients. Conversely, the SVF from diabetic
patients exhibited a similar angiogenic factor expression to the
healthy control patients. After 6 months of ADSC implantation,
66.7% of patients exhibited improved pain rating scales and in
claudication or walking distance. Moreover, the vascular collateral
network increased during the 6-months follow-up period. Thus,
multiple intramuscular SVF injections may represent a safe
alternative to therapeutic angiogenesis obtainment in patients with
CLI refractory to other treatments (148).
The Cell-DREAM phase I trial evaluated the safety
and feasibility of intramuscular injections of autologous ASCs,
cultured for 2 weeks and then injected into the ischemic leg. The
results revealed an increase in TcPO2 in the majority of
patients and wound healing improvement in both non-diabetic and
diabetic patients (149).
However, that study presents a major size limitation, since only 7
patients were treated.
The study by Darinskas et al included 15
patients with rest pain and some with ulcerations; SVF was injected
once or twice in the ischemic limb along the arteries (150). Clinical improvement in terms of
pain, meters of claudication and ABI occurred in 86.7% of patients,
but only 6 patients out of 15 had ulcers and two patients underwent
major amputation, although the amputation sites healed completely.
Moreover, the vascular collateral network formation of arteries was
observed by digital subtraction angiography upon SVF cell therapy
(150).
Recently, Moon et al published a pilot study
on SVF cell treatment around the wounds of 1o diabetic feet
(151). TcPO2 values
increased at 12 weeks after the SVF injection, and cutaneous
microvascular blood flow also increased without any adverse event;
none of the patients had CLI, as indicated from an initial TcPO2
>30 mmHg (151).
To date, to the best of our knowledge, only one
randomized trial on 114 patients comparing standard care to
micro-fragmented adipose tissue implants has been published
(152). At 6 months of
follow-up, 80% of micro-fragmented adipose tissue-treated feet
healed compared to the control group, where only 46% healed. Wound
healing was improved in the treatment group; however, no effect was
observed on the pain scale between the two groups. These
observations suggest that autologous micro-fragmented adipose
tissue local injection can improve the healing rate after minor
amputations in diabetic foot. In that study, all patients had
adequate perfusion, as assessed by TcPO2 ≥30 mmHg, as in
the study by Moon et al (151), and micro-fragmented adipose
tissue injection was used as an adjuvant of stump healing and not
for its angiogenic property.
In conclusion, the above-described clinical studies
on AT-derived cells are all controlled pilot studies performed on a
limited number of patients. Well-designed RCTs are necessary to
verify reliability, safety, and efficacy on diabetic patients with
CLI.
Critical issues in clinical trials
Trials and meta-analyses are not exempt to some
limitations; the latter will be discussed in the following few
paragraphs.
a) Definition of no-option
patients
This definition may sometimes change across
countries and within different centers depending on the surgeons'
expertise, and this can create confusion and inconsistency in the
results obtained in multicentric studies and meta-analyses.
b) Type of administration
The majority of cell therapy trials for CLI have
utilized intramuscular cell delivery although intra-arterial
injection has also been used (153,154). The meta-analysis by Rigato
et al indicated that the intra-muscular injection was
associated with better results compared to intra-arterial delivery
(8).
c) Cell number and frequency of
implants
The clinical trials reported thus far use variable
number of cells implanted and different frequencies of implants for
cell therapy. In a pilot randomized controlled trial, patients who
received 4 repeated BM-MNC injections vs. 1 single treatment
exhibited an increase in pain-free walking distance, whereas the
ABI and pain were not altered at 24 weeks after the injections
(155). Accordingly, Kang et
al confirmed that several treatments were more effective than a
higher number of cells administered in one single treatment
(156). Moreover, Beugels et
al, in a rat model, demonstrated that the centrifuged human BM
suspension containing low and medium concentrations of mesenchymal
and hematopoietic stem cells significantly improved vascularization
in limb ischemia, but that the effect was almost lost with higher
stem cell doses (157).
d) G-CSF mobilization
The cellular mobilization in regenerative therapy
is a long-debated topic. Mobilization has been widely used;
however, it has been suggested that the mobilization of
CD34+ stem cells from the BM through the administration
of G-CSF is not efficient in diabetic patients (121). Particularly, the mobilization
potentially useful for the activity of stem cells does not appear
useful in PB-MNC treatments; in fact, no-option patients with CLI
treated with no-mobilized PB-MNCs have been shown to respond
positively to the treatment (75,81-84). Moreover, in a previous study,
there were no differences in AFS in no-option patients treated with
pure CD34+ or PB-MNCs (119). Furthermore, the SCELTA TRIAL
suggests the 'non-inferiority' of non-mobilized PB-MNCs compared to
BM-MNCs (84).
From no-option patients to adjuvant
therapy
The clinical trials described thus far involve
no-option patients; however, cellular therapy can also be
considered as adjuvant therapy in patients undergoing
revascularization (158). These
therapies can be useful in diabetic patients, where the evolution
of ulcerative lesions is not always closely related to proper
revascularization (159-161).
Arterial revascularization has been recognized a condition
necessary for the obtainment of a positive clinical outcome.
However, in a retrospective trial, Lehalle et al
demonstrated that revascularization was not sufficient for wound
healing in diabetic patients (143). Moreover, the same study also
observed that 20% of wounds healed of diabetic patients were going
to develop new ulcers after 3 years. Okazaki et al, in 304
revascularized patients, observed that only 56.3, 63.4 and 64.0% of
wounds healed at 1, 2 and 3 years, respectively (161).
Shiraki et al, in a retrospective study on
871 patients, of which 734 with trophic lesions and 553 diabetic
patients, revealed that 33% patients did not heal at 1 year
following successful PTA revascularization (160). These data were confirmed by
Robinson et al, who that demonstrated a mean of 209 days
healing time following revascularization (162).
Another retrospective study on 179 patients with
CLI and tissue loss demonstrated that a higher rate of major
amputation was recorded in non-healing patients within 4 months
from revascularization, while patients with wounds which healed in
3 months exhibited the lowest amputation rate (163). All these studies clearly
suggest that successful revascularization not always ensures wound
healing and that can determine an amputation, especially in
diabetic patients.
BM-MNC cell therapy as an adjuvant of
revascularization has already been described with encouraging
results (158). More recently,
Persiani et al observed that diabetic patients at Fontaine
stage IV treated with PB-MNCs as adjuvant therapy in
revascularization, exhibited an improvement trend in the amputation
rate, ulcerative lesions, TcPO2 and pain reduction
(82).
5. Conclusions and future perspectives
The studies reported in the present review describe
cell therapy in vascular limb rescue surgery in diabetic patients
and its usefulness in those patients who are either not eligible
for revascularization or in revascularization failures.
Currently, the optimal cellular source for
angiogenic therapies remains undefined, since most of the trials of
BM-MNCs and PB-MNCs have confirmed comparable clinical results in
line with the major meta-analyses, where a single implant for each
cell concentrate was compared.
Clinical studies on cell therapy from AT for the
treatment of CLI and diabetic patients are still limited. The
selection between BM-MNCs and PB-MNCs can be affected by the
cellular concentrate, reliability of the treatment and the
characteristics of the patients.
The higher concentration of stem cells in BM-MNCs
has led to an extensive use of this technique compared to PB-MNCs,
where the number of CD34+ cells is much lower. Moreover,
cell therapy with PB-MNCs leads to a good angiogenic and wound
healing effect, with the great advantage of minor withdrawal
invasiveness, which allows one to repeat cell implants several
times.
It is now clear that T2DM affects cell
functionality both in BM and in AT. Moreover, while
CD34+ stem cells are considered compromised, PB-MNCs
seem to be less affected in functionality, albeit not all the
studies agree on this point (128). Thus, in T2DM with CLI, PB-MNC
cell therapy could guarantee a better therapeutic outcome.
Furthermore, a meta-analysis demonstrated a decrease in amputation
rates and an increase in AFS periods and clinical parameters such
as ABI, TcPO2, and the VAS score, indicating that this
approach could be effective in no-option diabetic patients
(8).
Ultimately, different studies described in the
present review suggest the use of autologous cell therapies as
promising tools of revascularization adjuvant for wound healing in
diabetic patients with no-option CLI; however, further analyses are
necessary to confirm preliminary positive outcomes.
Although over the past years autologous cell
therapies were mainly based on the stem cell populations for
treating patients with no-option CLI, recently several studies have
observed that the capacity of stem cells is influenced and
orchestrated by local immune responses to tissue damage, with
monocytes/macrophages as key players of tissue repair (35-37). Moreover, diabetes strongly
impairs stem cell populations in BM, PB and AT. The paradigm shift,
from stem cells to immune cell-based therapy, is known as the
immune-centric revolution, that was recently confirmed by a study
that found that stem cell therapy did not improve heart function by
producing new cardiomyocytes, but by inducing an immune response
due to the activation of macrophages (164). Those authors observed that the
benefit was likely to be related to the local and acute immune
response rather than to the regenerative capacity of the stem cells
themselves, clearly demonstrating that the immune-modulation
triggered by the immune system is at the basis of the repair
mechanism. In line with this immune centric vision, a randomized,
controlled, multi-center study using autologous peripheral blood
total nuclear cells (TNCs) that will enroll up to 350 diabetic
patients with no-option CLI, is ongoing (HT-CLI pivotal trial
NCT03809494). The results of this trial will give a clear vision of
the importance of immune cells population in angiogenesis and wound
healing. A number of research groups are focusing on immune cell
regenerative effects on different tissues, such as skeletal muscle
(165,166).
Furthermore, given the increasing number of
diabetic patients and the significant percentages of patients with
non-healing lesions even following effective revascularization,
adjuvant cell therapy may soon take hold. However, more controlled
clinical trials will be needed to prove this hypothesis.
Finally, a promising approach for therapeutic
angiogenesis and wound healing resides in the study of exosomes
derived by MNCs. Recently, it was demonstrated that MSC-derived
exosomes played a pivotal role in enhancing the proliferation and
migration of fibroblasts of both normal donors and patients with
chronic wound (167). Moreover,
these exosomes induce angiogenesis in vitro, since ECs can
uptake them. Exosomes are fundamental for angiogenic improvement
and similar to miRNAs, are useful in activating signaling pathways
involved in angiogenesis. The exosomes can also contain active
transcription factors, such as STAT3, able to induce the
transcriptional upregulation of different growth factors; i.e.,
SDF1, IL-6, HGF and nerve growth factor (NGF) that are all
compromised in chronic wounds, particularly in diabetic patients.
Further, it was shown that exosome-depleted conditioned medium had
impaired angiogenesis response (167).
Recently, exosomes of human induced pluripotent
stem cell-derived mesenchymal stem cells (hiPSC-MSCs) have
demonstrated to be efficacious and to be an interesting alternative
for cell transplantation therapy. MSCs exosomes have been shown to
be efficacious in repairing injured tissues in a rat skin wound
model (168).
The therapeutic approach based on exosomes has been
demonstrated to be effective also in different diseases, and an
interesting approach has been developed in cancer therapy, in which
ADSCs overexpressing a miR-125b bearing a specific ExoMotif
sequence tag enhance the loading into extracellular vesicles. These
vesicles have then been used to deliver this anti-metastatic miRNA
in hepatocellular carcinoma cells, reducing their proliferation
(169).
A similar method can be used with exosomes as a
therapeutic approach in chronic wounds, using autologous MNCs
engineered to overexpress a specific miRNA or a transcription
factor useful for angiogenesis and wound healing improvement. The
latter could be injected subcutaneously around wound sites to
ameliorate healing.
Availability of data and materials
Not applicable.
Authors' contributions
AM, MCF, MR and SF were involved in the conception
and design of the manuscript. AM, MCF and SF drafted the
manuscript. AM, MCF, MR and SF revised the manuscript. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Acknowledgments
The authors apologize to the many researchers whose
work was not cited in the present review. The authors would like to
thank Dr Robert Monticone of the Laboratory of Cardiovascular
Science, National Institute on Aging (NIA), National Institutes of
Health (NIH), Baltimore, MD, USA, for the English proofreading.
Abbreviations:
|
Ang-1
|
angiopoietin
|
|
ADRCs
|
adipose-derived regenerative
cells
|
|
ADSCs
|
adipose-derived stem/progenitor
cells
|
|
AD-SVF
|
adipose-derived stromal vascular
fraction
|
|
AFS
|
amputation-free survival
|
|
AT
|
Adipose tissue
|
|
BM
|
bone marrow
|
|
BMAC
|
bone marrow aspirate concentrate
|
|
BM-MNCs
|
bone marrow-derived mononuclear
cells
|
|
CLI
|
critical limb ischemia
|
|
EPCs
|
endothelial progenitor cells
|
|
EGF
|
endothelial growth factor
|
|
G-CSF
|
granulocyte-colony stimulating
factor
|
|
IFATS
|
International Federation of Adipose
Therapeutics and Science
|
|
IGF-1
|
insulin growth factor
|
|
IL-1β
|
interleukin 1β
|
|
ISCT
|
International Society for Cellular
Therapy
|
|
KGF
|
keratinocyte growth factor
|
|
HSCs
|
hematopoietic stem cells
|
|
PAD
|
peripheral artery disease
|
|
PB
|
peripheral blood
|
|
PB-MNCs
|
peripheral blood mononuclear
cells
|
|
MCP-1
|
monocyte chemoattractant
protein-1
|
|
MIP-1
|
macrophage inflammatory protein 1
|
|
MSCs
|
mesenchymal stem cells
|
|
SDF-1
|
stromal-derived factor 1
|
|
SVF
|
stromal vascular fraction
|
|
TAO
|
thromboangiitis obliterans
|
|
T2DM
|
type 2 diabetes mellitus
|
|
TGFβ
|
transforming growth factor β
|
|
TNC
|
total nuclear cell
|
|
VM
|
vascular mimicry
|
|
VEGF
|
vascular endothelial growth
factor
|
References
|
1
|
Fowkes FGR, Rudan D, Rudan I, Aboyans V,
Denenberg JO, McDermott MM, Norman PE, Sampson UK, Williams LJ,
Mensah GA and Criqui MH: Comparison of global estimates of
prevalence and risk factors for peripheral artery disease in 2000
and 2010: A systematic review and analysis. Lancet. 382:1329–1340.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cooke JP and Losordo DW: Modulating the
vascular response to limb ischemia: Angiogenic and cell therapies.
Circ Res. 116:1561–1578. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Criqui MH and Aboyans V: Epidemiology of
peripheral artery disease. Circ Res. 116:1509–1526. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Teraa M, Conte MS, Moll FL and Verhaar MC:
Critical limb ischemia: Current trends and future directions. J Am
Heart Assoc. 5:e0029382016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Reinecke H, Unrath M, Freisinger E,
Bunzemeier H, Meyborg M, Lüders F, Gebauer K, Roeder N, Berger K
and Malyar NM: Peripheral arterial disease and critical limb
ischaemia: Still poor outcomes and lack of guideline adherence. Eur
Heart J. 36:932–938. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Freisinger E, Malyar NM, Reinecke H and
Lawall H: Impact of diabetes on outcome in critical limb ischemia
with tissue loss: A large-scaled routine data analysis. Cardiovasc
Diabetol. 16:412017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yan J, Tie G, Wang S, Tutto A, DeMarco N,
Khair L, Fazzio TG and Messina LM: Diabetes impairs wound healing
by Dnmt1-dependent dysregulation of hematopoietic stem cells
differentiation towards macrophages. Nat Commun. 9:332018.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rigato M, Monami M and Fadini GP:
Autologous cell therapy for peripheral arterial disease: Systematic
review and meta-analysis of randomized, nonrandomized, and
noncontrolled studies. Circ Res. 120:1326–1340. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Qadura M, Terenzi DC, Verma S, Al-Omran M
and Hess DA: Concise review: Cell therapy for critical limb
ischemia: An integrated review of preclinical and clinical studies.
Stem Cells. 36:161–171. 2018. View Article : Google Scholar
|
|
10
|
Dubský M, Jirkovská A, Bem R, Nemcová A,
Fejfarová V and Jude EB: Cell therapy of critical limb ischemia in
diabetic patients-State of art. Diabetes Res Clin Pract.
126:263–271. 2017. View Article : Google Scholar
|
|
11
|
Dubský M, Jirkovská A, Bem R, Fejfarova V,
Pagacova L, Sixta B, Varga M, Langkramer S, Sykova E and Jude EB:
Both autologous bone marrow mononuclear cell and peripheral blood
progenitor cell therapies similarly improve ischaemia in patients
with diabetic foot in comparison with control treatment. Diabetes
Res Clin Pract. 29:369–376. 2013.
|
|
12
|
Weck M, Slesaczeck T, Rietzsch H, Münch D,
Nanning T, Paetzold H, Florek HJ, Barthel A, Weiss N and Bornstein
S: Noninvasive management of the diabetic foot with critical limb
ischemia: Current options and future perspectives. Ther Adv
Endocrinol Metab. 2:247–255. 2011. View Article : Google Scholar
|
|
13
|
Parikh PP, Liu ZJ and Velazquez OC: A
molecular and clinical review of stem cell therapy in critical limb
ischemia. Stem Cell Int. 2017:37508292017.
|
|
14
|
Zuk PA, Zhu M, Mizuno H, Huang J, Futrell
JW, Katz AJ, Benhaim P, Lorenz HP and Hedrick MH: Multilineage
cells from human adipose tissue: Implications for cell-based
therapies. Tissue Eng. 7:211–228. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Dominici M, Le Blanc K, Mueller I,
Slaper-Cortenbach I, Marini F, Krause D, Deans R, Keating A,
Prockop Dj and Horwitz E: Minimal criteria for defining multipotent
mesenchymal stromal cells. The international society for cellular
therapy position statement. Cytotherapy. 8:315–317. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Murray IR, Chahla J, Safran MR, Krych AJ,
Saris DBF, Caplan AI, LaPrade RF, Cell Therapies Communication and
Expert Group: International expert consensus on a cell therapy
communication tool: DOSES. J Bone Joint Surg Am. 101:904–911. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Silvestre JS, Smadja DM and Levy BI:
Postischemic revascularization: From cellular and molecular
mechanisms to clinical applications. Physiol Rev. 93:1743–1802.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Verfaillie C, Blakolmer K and McGlave P:
Purified primitive human hematopoietic progenitor cells with
long-term in vitro repopulating capacity adhere selectively to
irradiated bone marrow stroma. J Exp Med. 172:509–602. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Finney MR, Greco NJ, Haynesworth SE,
Martin JM, Hedrick DP, Swan JZ, Winter DG, Kadereit S, Joseph ME,
Fu P, et al: Direct comparison of umbilical cord blood versus bone
marrow-derived endothelial precursor cells in mediating
neovascularization in response to vascular ischemia. Biol Blood
Marrow Transplant. 12:585–593. 2005. View Article : Google Scholar
|
|
20
|
Xiang Y, Zheng Q, Jia BB, Huang GP, Xu YL,
Wang JF and Pan ZJ: Ex vivo expansion and pluripotential
differentiation of cryopreserved human bone marrow mesenchymal stem
cells. J Zhejiang Univ Sci B. 8:136–146. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Veronesi F, Giavaresi G, Tschon M, Borsari
V, Nicoli Aldini N and Fini M: Clinical use of bone marrow, bone
marrow concentrate, and expanded bone marrow mesenchymal stem cells
in cartilage disease. Stem Cells Dev. 22:181–192. 2013. View Article : Google Scholar
|
|
22
|
D'souza N, Rossignoli F, Golinelli G,
Grisendi G, Spano C, Candini O, Osturu S, Catani F, Paolucci P,
Horwitz EM and Dominici M: Mesenchymal stem/stromal cells as a
delivery platform in cell and gene therapies. BMC Med. 13:1862015.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Liang X, Ding Y, Zhang Y, Tse HF and Lian
Q: Paracrine mechanisms of mesenchymal stem cell-based therapy:
Current status and perspectives. Cell Transplant. 23:1045–1059.
2014. View Article : Google Scholar
|
|
24
|
Spees JL, Lee RH and Gregory CA:
Mechanisms of mesenchymal stem/stromal cell function. Stem Cell Res
Ther. 7:1252016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Liew A and O'Brien T: Therapeutic
potential for mesenchymal stem cell transplantation in critical
limb ischemia. Stem Cell Res Ther. 3:282012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Najar M, Krayem M, Merimi M, Burny A,
Meuleman N, Bron D, Raicevic G and Lagneaux L: Insights into
inflammatory priming of mesenchymal stromal cells: Functional
biological impacts. Inflamm Res. 67:467–477. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Naji A, Suganuma N, Espagnolle N, Yagyu
KI, Baba N, Sensebé L and Deschaseaux F: Rationale for determining
the functional potency of mesenchymal stem cells in preventing
regulated cell death for therapeutic use. Stem Cells Transl Med.
6:713–719. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ma S, Xie N, Li W, Yuan B, Shi Y and Wang
Y: Immunobiology of mesenchymal stem cells. Cell Death Differ.
21:216–225. 2014. View Article : Google Scholar :
|
|
29
|
Kusuma GD, Carthew J, Lim R and Frith JE:
Effect of the micro-environment on mesenchymal stem cell paracrine
signaling: Opportunities to engineer the therapeutic effect. Stem
Cells Dev. 26:617–631. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kim N and Cho SG: Overcoming
immunoregulatory plasticity of mesenchymal stem cells for
accelerated clinical applications. Int J Hematol. 103:129–137.
2016. View Article : Google Scholar
|
|
31
|
Hoffmann J, Glassford AJ, Doyle TC,
Robbins RC, Schrepfer S and Pelletier MP: Angiogenic effects
despite limited cell survival of bone marrow-derived mesenchymal
stem cells under ischemia. Thorac Cardiovasc Surg. 58:136–142.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kinnaird T, Stabile E, Burnett MS, Shou M,
Lee CW, Barr S, Fuchs S and Epstein SE: Local delivery of
marrow-derived stromal cells augments collateral perfusion through
paracrine mechanisms. Circulation. 109:1543–1549. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ben-Mordechai T, Holbova R, Landa-Rouben
N, Harel-Adar T, Feinberg MS, Abd Elrahman I, Blum G, Epstein FH,
Silman Z, Cohen S and Leor J: Macrophage subpopulations are
essential for infarct repair with and without stem cell therapy. J
Am Coll Cardiol. 62:1890–1901. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Pinto AR, Godwin JW and Rosenthal NA:
Macrophages in cardiac homeostasis, injury responses and progenitor
cell mobilisation. Stem Cell Res. 13:705–714. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Forbes SJ and Rosenthal N: Preparing the
ground for tissue regeneration: From mechanism to therapy. Nat Med.
20:857–869. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Julier Z, Park AJ, Briquez PS and Martino
MM: Promoting tissue regeneration by modulating the immune system.
Acta Biomater. 53:13–28. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Naik S, Larsen SB, Cowley CJ and Fuchs E:
Two to tango: Dialog between immunity and stem cells in health and
disease. Cell. 175:908–920. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Anton K, Banerjee D and Glod J:
Macrophage-associated mesenchymal stem cells assume an activated,
migratory, pro-inflammatory phenotype with increased IL-6 and
CXCL10 secretion. PLoS One. 7:e350362012. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Faulknor RA, Olekson MA, Ekwueme EC,
Krzyszczyk P, Freeman JW and Berthiaume F: Hypoxia impairs
mesenchymal stromal cell-induced macrophage M1 to M2 transition.
Technology (Singap World Sci). 5:81–86. 2017.
|
|
40
|
Kajiguchi M, Kondo T, Izawa H, Kobayashi
M, Yamamoto K, Shintani S, Numaguchi Y, Naoe T, Takamatsu J, Komori
K and Murohara T: Safety and efficacy of autologous progenitor cell
transplantation for therapeutic angiogenesis in patients with
critical limb ischemia. Circ J. 71:196–201. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Matoba S, Tatsumi T, Murohara T, Imaizumi
T, Katsuda Y, Ito M, Saito Y, Uemura S, Suzuki H, Fukumoto S, et
al: Long-term clinical outcome after intramuscular implantation of
bone marrow mononuclear cells [therapeutic angiogenesis by cell
transplantation (TACT) trial] in patients with chronic limb
ischemia. Am Heart J. 156:1010–1018. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Tateishi-Yuyama E, Matsubara H, Murohara
T, Ikeda U, Shintani S, Masaki H, Amano K, Kishimoto Y, Yoshimoto
K, Akashi H, et al: Therapeutic angiogenesis for patients with limb
ischaemia by autologous transplantation of bone-marrow cells: A
pilot study and a randomised controlled trial. Lancet. 360:427–435.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Di Trapani M, Bassi G, Midolo M, Gatti A,
Kamga PT, Cassaro A, Carusone R, Adamo A and Krampera M:
Differential and transferable modulatory effects of mesenchymal
stromal cell-derived extracellular vesicles on T, B and NK cell
functions. Sci Rep. 6:241202016. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Kamihata H, Matsubara H, Nishiue T,
Fujiyama S, Tsutsumi Y, Ozono R, Masaki H, Mori Y, Iba O, Tateishi
E, et al: Implantation of bone marrow mononuclear cells into
ischemic myocardium enhances collateral perfusion and regional
function via side supply of angioblasts, angiogenic ligands, and
cytokines. Circulation. 104:1046–1052. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Qin SL, Li TS, Takahashi M and Hamano K:
In vitro assessment of the effect of interleukin-1beta on
angiogenic potential of bone marrow cells. Circ J. 70:1195–1199.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Wu Y, Zhao RC and Tredget EE: Concise
review: Bone marrow-derived stem/progenitor cells in cutaneous
repair and regeneration. Stem Cell. 28:905–915. 2010.
|
|
47
|
Okuno Y, Nakamura-Ishizu A, Kishi K, Suda
T and Kubota Y: Bone marrow-derived cells serve as proangiogenic
macrophages but not endothelial cells in wound healing. Blood.
117:5264–5272. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Asahara T, Masuda H, Takahashi T, Kalka C,
Pastore C, Silver M, Kearne M, Magner M and Isner JM: Bone marrow
origin of endothelial progenitor cells responsible for postnatal
vasculogenesis in physiological and pathological
neovascularization. Circ Res. 85:221–228. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Wang ZX, Li D, Cao JX, Liu YS, Wang M,
Zhang XY, Li JL, Wang HB, Liu JL and Xu BL: Efficacy of autologous
bone marrow mononuclear cell therapy in patients with peripheral
arterial disease. J Atheroscler Thromb. 21:1183–1196. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Powell RJ, Comerota AJ, Berceli SA, Guzman
R, Henry TD, Tzeng E, Velazquez O, Marston WA, Bartel RL, Longcore
A, et al: Interim analysis results from the RESTORE-CLI, a
randomized, double-blind multicenter phase II trial comparing
expanded autologous bone marrow-derived tissue repair cells and
placebo in patients with critical limb ischemia. J Vasc Surg.
54:1032–1041. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Bourin P, Bunnell BA, Casteilla L,
Dominici M, Katz AJ, March KL, Redl H, Rubin JP, Yoshimura K and
Gimble JM: Stromal cells from the adipose tissue-derived stromal
vascular fraction and culture expanded adipose tissue-derived
stromal/stem cells: A joint statement of the International
Federation for Adipose Therapeutics and Science (IFATS) and the
international society for cellular therapy (ISCT). Cytotherapy.
15:641–648. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Guillaume-Jugnot P, Daumas A, Magalon J,
Sautereau N, Veran J, Magalon G, Sabatier F and Granel B: State of
the art. Autologous fat graft and adipose tissue-derived stromal
vascular fraction injection for hand therapy in systemic sclerosis
patients. Curr Res Transl Med. 64:35–42. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Ong WK and Sugii S: Adipose-derived stem
cells: Fatty potentials for therapy. Int J Biochem Cell Biol.
45:1083–1086. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Guo J, Nguyen A, Banyard DA, Fadavi D,
Toranto JD, Wirth GA, Paydar KZ, Evans GR and Widgerow AD: Stromal
vascular fraction: A regenerative reality? Part 2: Mechanisms of
regenerative action. J Plast Reconstr Aesthetic Surg. 69:180–188.
2016. View Article : Google Scholar
|
|
55
|
Parker AM and Katz AJ: Adipose-derived
stem cells for the regeneration of damaged tissues. Expert Opin
Biol Ther. 6:567–578. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Park YB, Ha CW, Rhim JH and Lee HJ: Stem
cell therapy for articular cartilage repair: Review of the entity
of cell populations used and the result of the clinical application
of each entity. Am J Sports Med. 46:2540–2552. 2018. View Article : Google Scholar
|
|
57
|
Strong AL, Cederna PS, Rubin JP, Coleman
SR and Levi B: The current state of fat grafting: A review of
harvesting, processing, and injection techniques. Plast Reconstr
Surg. 136:897–912. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Bianchi F, Maioli M, Leonardi E, Olivi E,
Pasquinelli G, Valente S, Mendez AJ, Ricordi C, Raffaini M,
Tremolada C and Ventura C: A new nonenzymatic method and device to
obtain a fat tissue derivative highly enriched in pericyte-like
elements by mild mechanical forces from human lipoaspirates. Cell
Transplant. 22:2063–2077. 2013. View Article : Google Scholar
|
|
59
|
Harada Y, Yamamoto Y, Tsujimoto S,
Matsugami H, Yoshida A and Hisatome I: Transplantation of freshly
isolated adipose tissue-derived regenerative cells enhances
angiogenesis in a murine model of hind limb ischemia. Biomed Res.
34:23–29. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Rehman J, Traktuev D, Li J, Merfeld-Clauss
S, Temm-Grove CJ, Bovenkerk JE, Pell CL, Johnstone BH, Considine RV
and March KL: Secretion of angiogenic and antiapoptotic factors by
human adipose stromal cells. Circulation. 109:1292–1298. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Kim Y, Kim H, Cho H, Bae Y, Suh K and Jung
J: Direct comparison of human mesenchymal stem cells derived from
adipose tissues and bone marrow in mediating neovascularization in
response to vascular ischemia. Cell Physiol Biochem. 20:867–876.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Navarro A, Marín S, Riol N,
Carbonell-Uberos F and Miñana MD: Human adipose tissue-resident
monocytes exhibit an endothelial-like phenotype and display
angiogenic properties. Stem Cell Res Ther. 5:502014. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Cai J, Feng J, Liu K, Zhou S and Lu F:
Early macrophage infiltration improves fat graft survival by
inducing angiogenesis and hematopoietic stem cell recruitment.
Plast Reconstr Surg. 141:376–386. 2018. View Article : Google Scholar
|
|
64
|
Dong Z, Peng Z, Chang Q and Lu F: The
survival condition and immunoregulatory function of adipose stromal
vascular fraction (SVF) in the early stage of nonvascularized
adipose transplantation. PLoS One. 8:e803642013. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Spaltro G, Straino S, Gambini E, Bassetti
B, Persico L, Zoli S, Zanobini M, Capogrossi MC, Spirito R, Quarti
C and Pompilio G: Characterization of the pall celeris system as a
point-of-care device for therapeutic angiogenesis. Cytotherapy.
17:1302–1313. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Rennert RC, Sorkin M, Januszyk M, Duscher
D, Kosaraju R, Chung MT, Lennon J, Radiya-Dixit A, Raghvendra S,
Maan ZN, et al: Diabetes impairs the angiogenic potential of
adipose-derived stem cells by selectively depleting cellular
subpopulations. Stem Cell Res Ther. 5:792014. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Li J, Tan J, Martino MM and Lui KO:
Regulatory T-cells: Potential regulator of tissue repair and
regeneration. Front Immunol. 9:5852018. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Aurora AB and Olson EN: Immune modulation
of stem cells and regeneration. Cell Stem Cell. 15:14–25. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Spiller KL and Koh TJ: Macrophage-based
therapeutic strategies in regenerative medicine. Adv Drug Deliv
Rev. 122:74–83. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Zhang J, Yang Y, Yang Z, Li T and Chen F:
Snapshot: Targeting macrophages as a candidate for tissue
regeneration. Curr Issues Mol Biol. 29:37–48. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Tauber AI: Metchnikoff and the
phagocytosis theory. Nat Rev Mol Cell Biol. 4:897–901. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Wynn TA and Vannella KM: Macrophages in
tissue repair, regeneration, and fibrosis. Immunity. 44:450–462.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Huang PP, Yang XF, Li SZ, Wen JC, Zhang Y
and Han ZC: Randomised comparison of G-CSF-mobilized peripheral
blood mononuclear cells versus bone marrow-mononuclear cells for
the treatment of patients with lower limb arteriosclerosis
obliterans. Thromb Haemost. 98:1335–1342. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Gurevich DB, Severn CE, Twomey C,
Greenhough A, Cash J, Toye AM, Mellor H and Martin P: Live imaging
of wound angiogenesis reveals macrophage orchestrated vessel
sprouting and regression. EMBO J. 37:e977862018. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Moriya J, Minamino T, Tateno K, Shimizu N,
Kuwabara Y, Sato Y, Saito Y and Komuro I: Long-term outcome of
therapeutic neovascularization using peripheral blood mononuclear
cells for limb ischemia. Circ Cardiovasc Interv. 2:245–254. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Krishnasamy K, Limbourg A, Kapanadze T,
Gamrekelashvili J, Beger C, Häger C, Lozanovski VJ, Falk CS, Napp
LC, Bauersachs J, et al: Blood vessel control of macrophage
maturation promotes arteriogenesis in ischemia. Nat Commun.
8:9522017. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Beer L, Zimmermann M, Mitterbauer A,
Ellinger A, Gruber F, Narzt MS, Zellner M, Gyöngyösi M, Madlener S,
Simader E, et al: Analysis of the secretome of apoptotic peripheral
blood mononuclear cells: Impact of released proteins and exosomes
for tissue regeneration. Sci Rep. 5:166622015. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Blomgran P, Blomgran R, Ernerudh J and
Aspenberg P: A possible link between loading, inflammation and
healing: Immune cell populations during tendon healing in the rat.
Sci Rep. 6:298242016. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Kirana S, Stratmann B, Prante C, Prohaska
W, Koerperich H, Lammers D, Gastens MH, Quast T, Negrean M, Stirban
OA, et al: Autologous stem cell therapy in the treatment of limb
ischaemia induced chronic tissue ulcers of diabetic foot patients.
Int J Clin Pract. 66:384–393. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Tateno K, Minamino T, Toko H, Akazawa H,
Shimizu N, Takeda S, Kunieda T, Miyauchi H, Oyama T, Matsuura K, et
al: Critical roles of muscle-secreted angiogenic factors in
therapeutic neovascularization. Circ Res. 98:1194–1202. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
81
|
De Angelis B, Gentile P, Orlandi F,
Bocchini I, Di Pasquali C, Agovino A, Gizzi C, Patrizi F, Scioli
MG, Orlandi A and Cervelli V: Limb rescue: A new
autologous-peripheral blood mononuclear cells technology in
critical limb ischemia and chronic ulcers. Tissue Eng Part C
Methods. 21:423–435. 2015. View Article : Google Scholar
|
|
82
|
Persiani F, Paolini A, Camilli D,
Mascellari L, Platone A, Magenta A and Furgiuele S: Peripheral
blood mononuclear cells therapy for treatment of lower limb
ischemia in diabetic patients: A single-center experience. Ann Vasc
Surg. 53:190–196. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Mutirangura P, Ruangsetakit C, Wongwanit
C, Chinsakchai K, Porat Y, Belleli A and Czeiger D: Enhancing limb
salvage by non-mobilized peripheral blood angiogenic cell
precursors therapy in patients with critical limb ischemia. J Med
Assoc Thail. 92:320–327. 2009.
|
|
84
|
Liotta F, Annunziato F, Castellani S,
Boddi M, Alterini B, Castellini G, Mazzanti B, Cosmi L, Acquafresca
M, Bartalesi F, et al: Therapeutic efficacy of autologous
non-mobilized enriched circulating endothelial progenitors in
patients with critical limb ischemia-the SCELTA trial. Circ J.
82:1688–1698. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Arras M, Ito WD, Scholz D, Winkler B,
Schaper J and Schaper W: Monocyte activation in angiogenesis and
collateral growth in the rabbit hindlimb. J Clin Invest. 101:40–50.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Anghelina M, Krishnan P, Moldovan L and
Moldovan NI: Monocytes/macrophages cooperate with progenitor cells
during neovascularization and tissue repair: Conversion of cell
columns into fibrovascular bundles. Am J Pathol. 168:529–541. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Capoccia BJ, Gregory AD and Link DC:
Recruitment of the inflammatory subset of monocytes to sites of
ischemia induces angiogenesis in a monocyte chemoattractant
protein-1-dependent fashion. J Leukoc Biol. 84:760–768. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Schaper J, König R, Franz D and Schaper W:
The endothelial surface of growing coronary collateral arteries.
Intimal margination and diapedesis of monocytes. A combined SEM and
TEM study. Virchows Arch A Pathol Anat Histol. 370:193–205. 1976.
View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Scholz D, Ito W, Fleming I, Deindl E,
Sauer A, Wiesnet M, Busse R, Schaper J and Schaper W:
Ultrastructure and molecular histology of rabbit hind-limb
collateral artery growth (arteriogenesis). Virchows Arch.
436:257–270. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Bergmann CE, Hoefer IE, Meder B, Roth H,
van Royen N, Breit SM, Jost MM, Aharinejad S, Hartmann S and
Buschmann IR: Arteriogenesis depends on circulating monocytes and
macrophage accumulation and is severely depressed in op/op mice. J
Leukoc Biol. 80:59–65. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Ito WD, Arras M, Winkler B, Scholz D,
Schaper J and Schaper W: Monocyte chemotactic protein-1 increases
collateral and peripheral conductance after femoral artery
occlusion. Circ Res. 80:829–837. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Fantin A, Vieira JM, Gestri G, Denti L,
Schwarz Q, Prykhozhij S, Peri F, Wilson SW and Ruhrberg C: Tissue
macrophages act as cellular chaperones for vascular anastomosis
downstream of VEGF-mediated endothelial tip cell induction. Blood.
116:829–840. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Barnett FH, Rosenfeld M, Wood M, Kiosses
WB, Usui Y, Marchetti V, Aguilar E and Friedlander M: Macrophages
form functional vascular mimicry channels in vivo. Sci Rep.
6:366592016. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Liu C, Wu C, Yang Q, Gao J, Li L, Yang D
and Luo L: Macrophages mediate the repair of brain vascular rupture
through direct physical adhesion and mechanical traction. Immunity.
44:1162–1176. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Baer C, Squadrito ML, Iruela-Arispe ML and
De Palma M: Reciprocal interactions between endothelial cells and
macrophages in angiogenic vascular niches. Exp Cell Res.
319:1626–1634. 2013. View Article : Google Scholar
|
|
96
|
Minutti CM, Knipper JA, Allen JE and Zaiss
DMW: Tissue-specific contribution of macrophages to wound healing.
Semin Cell Dev Biol. 61:3–11. 2017. View Article : Google Scholar
|
|
97
|
Ding J, Lei L, Liu S, Zhang Y, Yu Z, Su Y
and Ma X: Macrophages are necessary for skin regeneration during
tissue expansion. J Transl Med. 17:362019. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Krzyszczyk P, Schloss R, Palmer A and
Berthiaume F: The role of macrophages in acute and chronic wound
healing and interventions to promote pro-wound healing phenotypes.
Front Physiol. 9:4192018. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Wynn TA, Chawla A and Pollard JW:
Macrophage biology in development, homeostasis and disease. Nature.
496:445–455. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Kimball A, Schaller M, Joshi A, Davis FM,
den Dekker A, Boniakowski A, Bermick J, Obi A, Moore B, Henke PK,
et al: Ly6C Hi blood monocyte/macrophage drive chronic inflammation
and impair wound healing in diabetes mellitus. Arterioscler Thromb
Vasc Biol. 38:1102–1114. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Boniakowski AE, Kimball AS, Jacobs BN,
Kunkel SL and Gallagher KA: Macrophage-mediated inflammation in
normal and diabetic wound healing. J Immunol. 199:17–24. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Awad O, Dedkov EI, Jiao C, Bloomer S,
Tomanek RJ and Schatteman GC: Differential healing activities of
CD34+ and CD14+ endothelial cell progenitors. Arterioscler Thromb
Vasc Biol. 26:758–764. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Rodero MP, Licata F, Poupel L, Hamon P,
Khosrotehrani K, Combadiere C and Boissonnas A: In vivo imaging
reveals a pioneer wave of monocyte recruitment into mouse skin
wounds. PLoS One. 9:e1082122014. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Willenborg S and Eming SA:
Macrophages-sensors and effectors coordinating skin damage and
repair. J Dtsch Dermatol Ges. 12:214–221. 2014.
|
|
105
|
Gordon S and Martinez FO: Alternative
activation of macrophages: Mechanism and functions. Immunity.
32:593–604. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Van Weel V, Toes RE, Seghers L, Deckers
MM, de Vries MR, Eilers PH, Sipkens J, Schepers A, Eefting D, van
Hinsbergh VW, et al: Natural killer cells and CD4+ T-cells modulate
collateral artery development. Arterioscler Thromb Vasc Biol.
27:2310–2318. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Hellingman AA, Zwaginga JJ, Van Beem RT;
TeRM/Smart Mix Consortium; Hamming JF, Fibbe WE, Quax PH and
Geutskens SB: T-cell-pre-stimulated monocytes promote
neovascularisation in a murine hind limb ischaemia model. Eur J
Vasc Endovasc Surg. 41:418–428. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Stabile E, Burnett MS, Watkins C, Kinnaird
T, Bachis A, la Sala A, Miller JM, Shou M, Epstein SE and Fuchs S:
Impaired arteriogenic response to acute hindlimb ischemia in
CD4-knockout mice. Circulation. 108:205–210. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Stabile E, Kinnaird T, La Sala A, Hanson
SK, Watkins C, Campia U, Shou M, Zbinden S, Fuchs S, Kornfeld H, et
al: CD8+ T lymphocytes regulate the arteriogenic response to
ischemia by infiltrating the site of collateral vessel development
and recruiting CD4+ mononuclear cells through the expression of
interleukin-16. Circulation. 113:118–124. 2006. View Article : Google Scholar
|
|
110
|
Zouggari Y, Ait-Oufella H, Waeckel L,
Vilar J, Loinard C, Cochain C, Récalde A, Duriez M, Levy BI,
Lutgens E, et al: Regulatory T cells modulate postischemic
neovascularization. Circulation. 120:1415–1425. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Lee H, Schlereth SL, Park EY, Emami-Naeini
P, Chauhan SK and Dana R: A novel pro-angiogenic function for
interferon-Y-secreting natural killer cells. Invest Ophthalmol Vis
Sci. 55:2885–2892. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Leung OM, Li J, Li X, Chan VW, Yang KY, Ku
M, Ji L, Sun H, Waldmann H, Tian XY, et al: Regulatory T cells
promote apelin-mediated sprouting angiogenesis in type 2 diabetes.
Cell Rep. 24:1610–1626. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Burzyn D, Kuswanto W, Kolodin D, Shadrach
JL, Cerletti M, Jang Y, Sefik E, Tan TG, Wagers AJ, Benoist C and
Mathis D: A special population of regulatory T cells potentiates
muscle repair. Cell. 155:1282–1295. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
114
|
Ingram DA, Caplice NM and Yoder MC:
Unresolved questions, changing definitions, and novel paradigms for
defining endothelial progenitor cells. Blood. 106:1525–1531. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Basile DP and Yoder MC: Circulating and
tissue resident endothelial progenitor cells. J Cell Physiol.
229:10–16. 2014.
|
|
116
|
Rehman J, Li J, Orschell CM and March KL:
Peripheral blood 'endothelial progenitor cells' are derived from
monocyte/macrophages and secrete angiogenic growth factors.
Circulation. 107:1164–1169. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Romagnani P, Annunziato F, Liotta F,
Lazzeri E, Mazzinghi B, Frosali F, Cosmi L, Maggi L, Lasagni L,
Scheffold A, et al: CD14+CD34low cells with stem cell phenotypic
and functional features are the major source of circulating
endothelial progenitors. Circ Res. 97:314–322. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Rookmaaker MB, Verhaar MC, Loomans CJ,
Verloop R, Peters E, Westerweel PE, Murohara T, Staal FJ, van
Zonneveld AJ, Koolwijk P, et al: CD34+cells home, proliferate, and
participate in capillary formation, and in combination with
CD34-cells enhance tube formation in a 3-dimensional matrix.
Arterioscler Thromb Vasc Biol. 25:1843–1850. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Dong Z, Pan T, Fang Y, Wei Z, Gu S, Fang
G, Liu Y, Luo Y, Liu H, Zhang T, et al: Purified
CD34+cells versus peripheral blood mononuclear cells in
the treatment of angiitis-induced no-option critical limb
ischaemia: 12-Month results of a prospective randomised
single-blinded non-inferiority trial. EBioMedicine. 35:46–57. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Albiero M, Poncina N, Ciciliot S,
Cappellari R, Menegazzo L, Ferraro F, Bolego C, Cignarella A,
Avogaro A and Fadini GP: Bone marrow macrophages contribute to
diabetic stem cell mobilopathy by producing oncostatin M. Diabetes.
64:2957–2968. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
121
|
Fadini GP, Albiero M, Vigili de
Kreutzenberg S, Boscaro E, Cappellari R, Marescotti M, Poncina N,
Agostini C and Avogaro A: Diabetes impairs stem cell and
proangiogenic cell mobilization in humans. Diabetes Care.
36:943–949. 2013. View Article : Google Scholar :
|
|
122
|
Fadini GP, Spinetti G, Santopaolo M and
Madeddu P: Impaired regeneration contributes to poor outcomes in
diabetic peripheral artery disease. Arterioscler Thromb Vasc Biol.
40:34–44. 2020. View Article : Google Scholar
|
|
123
|
Loomans CJM, De Koning EJP, Staal FJ,
Rookmaaker MB, Verseyden C, de Boer HC, Verhaar MC, Braam B,
Rabelink TJ and van Zonneveld AJ: Endothelial progenitor cell
dysfunction: A novel concept in the pathogenesis of vascular
complications of type 1 diabetes. Diabetes. 53:195–199. 2004.
View Article : Google Scholar
|
|
124
|
Tepper OM, Galiano RD, Capla JM, Kalka C,
Gagne PJ, Jacobowitz GR, Levine JP and Gurtner GC: Human
endothelial progenitor cells from type II diabetics exhibit
impaired proliferation, adhesion, and incorporation into vascular
structures. Circulation. 106:2781–2786. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Facchiano F, Lentini A, Fogliano V,
Mancarella S, Rossi C, Facchiano A and Capogrossi MC: Sugar-induced
modification of fibroblast growth factor 2 reduces its angiogenic
activity in vivo. Am J Pathol. 161:531–541. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Di Stefano V, Cencioni C, Zaccagnini G,
Magenta A, Capogrossi MC and Martelli F: p66ShcA modulates
oxidative stress and survival of endothelial progenitor cells in
response to high glucose. Cardiovasc Res. 82:421–429. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Jarajapu YP, Hazra S, Segal M, Li Calzi S,
Jadhao C, Qian K, Mitter SK, Raizada MK, Boulton ME and Grant MB:
Vasoreparative dysfunction of CD34+ cells in diabetic individuals
involves hypoxic desensitization and impaired autocrine/paracrine
mechanisms. PLoS One. 9:e939652014. View Article : Google Scholar : PubMed/NCBI
|
|
128
|
Tchaikovski V, Olieslagers S, Böhmer FD
and Waltenberger J: Diabetes mellitus activates signal transduction
pathways resulting in vascular endothelial growth factor resistance
of human monocytes. Circulation. 120:150–159. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
129
|
Torres-Castro I, Arroyo-Camarena ÚD,
Martínez-Reyes CP, Gómez-Arauz AY, Dueñas-Andrade Y, Hernández-Ruiz
J, Béjar YL, Zaga-Clavellina V, Morales-Montor J, Terrazas LI, et
al: Human monocytes and macrophages undergo M1-type inflammatory
polarization in response to high levels of glucose. Immunol Lett.
176:81–89. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
130
|
Khanna S, Biswas S, Shang Y, Collard E,
Azad A, Kauh C, Bhasker V, Gordillo GM, Sen CK and Roy S:
Macrophage dysfunction impairs resolution of inflammation in the
wounds of diabetic mice. PLoS One. 5:e95392010. View Article : Google Scholar : PubMed/NCBI
|
|
131
|
Bannon P, Wood S, Restivo T, Campbell L,
Hardman MJ and Mace KA: Diabetes induces stable intrinsic changes
to myeloid cells that contribute to chronic inflammation during
wound healing in mice. Dis Model Mech. 6:1434–1447. 2013.PubMed/NCBI
|
|
132
|
Arnold L, Henry A, Poron F, Baba-Amer Y,
van Rooijen N, Plonquet A, Gherardi RK and Chazaud B: Inflammatory
monocytes recruited after skeletal muscle injury switch into
antiinflammatory macrophages to support myogenesis. J Exp Med.
204:1057–1069. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
133
|
Di Pardo A, Cappello E, Pepe G, Marracino
F, Carrieri V, Maglione V and Pompeo F: P-0717-Infusion of
autologous-peripheral blood mononuclear cells: A new approach for
limb salvage in patients with diabetes. In: Proceedings of the
International Diabetes Federation 2017 Congress; Abu Dhabi.
2017
|
|
134
|
Cianfarani F, Toietta G, Di Rocco G,
Cesareo E, Zambruno G and Odorisio T: Diabetes impairs adipose
tissue-derived stem cell function and efficiency in promoting wound
healing. Wound Repair Regen. 21:545–553. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
135
|
Kornicka K, Houston J and Marycz K:
Dysfunction of mesenchymal stem cells isolated from metabolic
syndrome and type 2 diabetic patients as result of oxidative stress
and autophagy may limit their potential therapeutic use. Stem Cell
Rev. 14:337–345. 2018. View Article : Google Scholar :
|
|
136
|
Inoue O, Usui S, Takashima SI, Nomura A,
Yamaguchi K, Takeda Y, Goten C, Hamaoka T, Ootsuji H, Murai H, et
al: Diabetes impairs the angiogenic capacity of human
adipose-derived stem cells by reducing the CD271+
subpopulation in adipose tissue. Biochem Biophys Res Commun.
517:369–375. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
137
|
Benoit E, O'donnell TF and Patel AN:
Safety and efficacy of autologous cell therapy in critical limb
ischemia: A systematic review. Cell Transplant. 22:545–562. 2013.
View Article : Google Scholar
|
|
138
|
Liew A, Bhattacharya V, Shaw J and Stansby
G: Cell therapy for critical limb ischemia: A meta-analysis of
randomized controlled trials. Angiology. 67:444–455. 2016.
View Article : Google Scholar
|
|
139
|
Jiang X, Zhang H and Teng M: Effectiveness
of autologous stem cell therapy for the treatment of lower
extremity ulcers: A systematic review and meta-analysis. Medicine
(Baltimore). 95:e27162016. View Article : Google Scholar
|
|
140
|
Ai M, Yan CF, Xia FC, Zhou SL, He J and Li
CP: Safety and efficacy of cell-based therapy on critical limb
ischemia: A meta-analysis. Cytotherapy. 18:712–724. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
141
|
Peeters Weem SM, Teraa M, De Borst GJ,
Verhaar MC and Moll FL: Bone marrow derived cell therapy in
critical limb ischemia: A meta-analysis of randomized placebo
controlled trials. Eur J Vasc Endovasc Surg. 50:775–783. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
142
|
Wang SK, Green LA, Motaganahalli RL,
Wilson MG, Fajardo A and Murphy MP: Rationale and design of the
MarrowStim PAD Kit for the treatment of critical limb ischemia in
subjects with severe peripheral arterial disease (MOBILE) trial
investigating autologous bone marrow cell therapy for critical limb
ischemia. J Vasc Surg. 65:1850–1857.e2. 2017. View Article : Google Scholar
|
|
143
|
Lehalle B, Jan P and Stoltz JF: Diabetic
patients on Rutherford's stage 5 is the best indication of stem
cell therapy in peripheral artery disease: A retrospective study on
367 patients. J Cell Immunother. 4:18–21. 2018. View Article : Google Scholar
|
|
144
|
Shu X, Shu S, Tang S, Yang L, Liu D, Li K,
Dong Z, Ma Z, Zhu Z and Din J: Efficiency of stem cell based
therapy in the treatment of diabetic foot ulcer: A meta-analysis.
Endocr J. 65:403–413. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
145
|
Guo J, Dardik A, Fang K, Huang R and Gu Y:
Meta-analysis on the treatment of diabetic foot ulcers with
autologous stem cells. Stem Cell Res Ther. 8:2282017. View Article : Google Scholar : PubMed/NCBI
|
|
146
|
Gao W, Chen D, Liu G and Ran X: Autologous
stem cell therapy for peripheral arterial disease: A systematic
review and meta-analysis of randomized controlled trials. Stem Cell
Res Ther. 10:1402019. View Article : Google Scholar : PubMed/NCBI
|
|
147
|
Hao C, Shintani S, Shimizu Y, Kondo K,
Ishii M, Wu H and Murohara T: Therapeutic angiogenesis by
autologous adipose-derived regenerative cells: Comparison with bone
marrow mononuclear cells. Am J Physiol Heart Circ Physiol.
307:H869–H879. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
148
|
Lee HC, An SG, Lee HW, Park JS, Cha KS,
Hong TJ, Park JH, Lee SY, Kim SP, Kim YD, et al: Safety and effect
of adipose tissue-derived stem cell implantation in patients with
critical limb ischemia: A pilot study. Circ J. 76:1750–1760. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
149
|
Bura A, Planat-Benard V, Bourin P,
Silvestre JS, Gross F, Grolleau JL, Saint-Lebese B, Peyrafitte JA,
Fleury S, Gadelorge M, et al: Phase I trial: The use of autologous
cultured adipose-derived stroma/stem cells to treat patients with
non-revascularizable critical limb ischemia. Cytotherapy.
16:245–257. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
150
|
Darinskas A, Paskevicius M, Apanavicius G,
Vilkevicius G, Labanauskas L, Ichim TE and Rimdeika R: Stromal
vascular fraction cells for the treatment of critical limb
ischemia: A pilot study. J Transl Med. 15:1432017. View Article : Google Scholar : PubMed/NCBI
|
|
151
|
Moon KC, Chung HY, Han SK, Jeong SH and
Dhong ES: Possibility of injecting adipose-derived stromal vascular
fraction cells to accelerate microcirculation in ischemic diabetic
feet: A pilot study. Int J Stem Cells. 12:107–113. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
152
|
Lonardi R, Leone N, Gennai S, Trevisi
Borsari G, Covic T and Silingardi R: Autologous micro-fragmented
adipose tissue for the treatment of diabetic foot minor
amputations: A randomized controlled single-center clinical trial
(MiFrAADiF). Stem Cell Res Ther. 10:2232019. View Article : Google Scholar : PubMed/NCBI
|
|
153
|
Teraa M, Sprengers RW, Schutgens RE,
Slaper-Cortenbach IC, van der Graaf Y, Algra A, van der Tweel I,
Doevendans PA, Mali WP, Moll FL and Verhaar MC: Effect of
repetitive intra-arterial infusion of bone marrow mononuclear cells
in patients with no-option limb ischemia: The randomized,
double-blind, placebo-controlled rejuvenating endothelial
progenitor cells via transcutaneous intra-arterial supplementation
(JUVENTAS) trial. Circulation. 131:851–860. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
154
|
Walter DH, Krankenberg H, Balzer JO, Kalka
C, Baumgartner I, Schlüter M, Tonn T, Seeger F, Dimmeler S,
Lindhoff-Last E and Zeiher AM; PROVASA Investigators: Intraarterial
administration of bone marrow mononuclear cells in patients with
critical limb ischemia a randomized-start, placebo-controlled pilot
trial (PROVASA). Circ Cardiovasc Interv. 4:26–37. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
155
|
Molavi B, Zafarghandi MR, Aminizadeh E,
Hosseini SE, Mirzayi H, Arab L, Baharvand H and Aghdami N: Safety
and efficacy of repeated bone marrow mononuclear cell therapy in
patients with critical limb ischemia in a pilot randomized
controlled trial. Arch Iran Med. 19:388–396. 2016.PubMed/NCBI
|
|
156
|
Kang WC, Oh PC, Lee K, Ahn T and Byun K:
Increasing injection frequency enhances the survival of injected
bone marrow derived mesenchymal stem cells in a critical limb
ischemia animal model. Korean J Physiol Pharmacol. 20:657–667.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
157
|
Beugels J, De Munter JPJM, Van Der Hulst
R, Kramer BW and Wolters ECH: Efficacy of different doses of human
autologous adult bone marrow stem cell transplantation on
angiogenesis in an immune deficient rat model with hind limb
ischemia. J Stem Cells Res Dev Ther. 5:1–6. 2019. View Article : Google Scholar
|
|
158
|
Kolvenbach R, Kreissig C, Cagiannos C,
Afifi R and Schmaltz E: Intraoperative adjunctive stem cell
treatment in patients with critical limb ischemia using a novel
point-of-care device. Ann Vasc Surg. 24:367–372. 2010. View Article : Google Scholar
|
|
159
|
Furgiuele S: Trattamento combinato della
arteriopatia periferica al IV stadio mediante rivascolarizzazione
endovascolare e terapia cellulare rigenerativa. Ital J Vasc
Endovasc Surg. 23:672016.
|
|
160
|
Shiraki T, Iida O, Takahara M, Soga Y,
Yamauchi Y, Hirano K, Kawasaki D, Fujihara M, Utsunomiya M, Tazaki
J, et al: Predictors of delayed wound healing after endovascular
therapy of isolated infrapopliteal lesions underlying critical limb
ischemia in patients with high prevalence of diabetes mellitus and
hemodialysis. Eur J Vasc Endovasc Surg. 49:565–573. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
161
|
Okazaki J, Matsuda D, Tanaka K, Ishida M,
Kuma S, Morisaki K, Furuyama T and Maehara Y: Analysis of wound
healing time and wound-free period as outcomes after surgical and
endovascular revascularization for critical lower limb ischemia. J
Vasc Surg. 67:817–825. 2018. View Article : Google Scholar
|
|
162
|
Robinson WP, Loretz L, Hanesian C, Flahive
J, Bostrom J, Lunig N, Schanzer A and Messina L: Society for
vascular surgery wound, ischemia, foot infection (WIfI) score
correlates with the intensity of multimodal limb treatment and
patient-centered outcomes in patients with threatened limbs managed
in a limb preservation center. J Vasc Surg. 66:488–498.e2. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
163
|
Reed GW, Salehi N, Giglou PR, Kafa R,
Malik U, Maier M and Shishehbor MH: Time to wound healing and major
adverse limb events in patients with critical limb ischemia treated
with endovascular revascularization. Ann Vasc Surg. 36:190–198.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
164
|
Vagnozzi RJ, Maillet M, Sargent MA, Khalil
H, Johansen AKZ, Schwanekamp JA, York AJ, Huang V, Nahrendorf M,
Sadayappan S and Molkentin JD: An acute immune response underlies
the benefit of cardiac stem cell therapy. Nature. 577:405–409.
2020. View Article : Google Scholar :
|
|
165
|
Dort J, Fabre P, Molina T and Dumont NA:
Macrophages are key regulators of stem cells during skeletal muscle
regeneration and diseases. Stem Cells Int. 2019:47614272019.
View Article : Google Scholar : PubMed/NCBI
|
|
166
|
Chisari E, Rehak L, Khan WS and Maffulli
N: The role of the immune system in tendon healing: A systematic
review. Br Med Bull. 133:49–64. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
167
|
Shabbir A, Cox A, Rodriguez-Menocal L,
Salgado M and Van Badiavas E: Mesenchymal stem cell exosomes induce
proliferation and migration of normal and chronic wound
fibroblasts, and enhance angiogenesis in vitro. Stem Cells Dev.
24:1635–1647. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
168
|
Zhang J, Guan J, Niu X, Hu G, Guo S, Li Q,
Xie Z, Zhang C and Wang Y: Exosomes released from human induced
pluripotent stem cells-derived MSCs facilitate cutaneous wound
healing by promoting collagen synthesis and angiogenesis. J Transl
Med. 13:492015. View Article : Google Scholar : PubMed/NCBI
|
|
169
|
Baldari S, Di Rocco G, Magenta A, Picozza
M and Toietta G: Extracellular vesicles-encapsulated MicroRNA-125b
produced in genetically modified mesenchymal stromal cells inhibits
hepatocellular carcinoma cell proliferation. Cells. 8:15602019.
View Article : Google Scholar
|
|
170
|
Woodell-May JE, Tan ML, King WJ, Swift MJ,
Welch ZR, Murphy MP and McKale JM: Characterization of the cellular
output of a point-of-care device and the implications for
addressing critical limb ischemia. Biores Open Access. 4:417–424.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
171
|
Sugaya H, Yoshioka T, Kato T, Taniguchi Y,
Kumagai H, Hyodo K, Ohneda O, Yamazaki M and Mishima H: Comparative
analysis of cellular and growth factor composition in bone marrow
aspirate concentrate and platelet-rich plasma. Bone Marrow Res.
2018:15498262018. View Article : Google Scholar : PubMed/NCBI
|
|
172
|
O'Connor SL, Sepulveda CA, Kaur I, Sumari
RD and McMannis JD: Characterization of BioSafe SEPAX manufactured
stem cell intended for cardiac cell therapy. Blood. 110:40642007.
View Article : Google Scholar
|