The muscarinic acetylcholine (ACh) receptor (M
receptor or mAChR), also known as the muscarinic ACh receptor, is
an important type of neurotransmitter receptor widely expressed in
various tissues and organs of the human body. As a G
protein-coupled membrane receptor, it regulates different
intracellular signaling transduction mechanisms in the body
(1), and has become a target for
various chemical drugs (2,3).
The cholinergic receptors can be divided into muscarinic ACh
receptors and nicotinic ACh receptors (N receptor), and the
majority of them in the heart are muscarinic ACh receptors.
Therefore, studying the function and disease regulation of
muscarinic ACh receptors in the heart is particularly important.
Currently, there are a total of five subtypes of muscarinic ACh
receptors, which are named M1-M5, and only three subtypes of
muscarinic ACh receptors with biological functions have been
discovered, which are M1, M2 and M3 (4). According to literature reports,
these three functional muscarinic ACh receptors play an important
role in the physiological and pathological regulation of the heart
(5). However, researchers still
have not fully clarified the myocardial function and
pathophysiological mechanisms mediated by muscarinic ACh receptors.
Known regulation of muscarinic ACh receptors in developing
cardiomyopathy involves pathological changes such as myocardial
infarction, myocardial fibrosis, cardiac hypertrophy, myocardial
contraction and arrhythmia, as well as regulation of myocardial
inflammation and non-nerve ACh systems (6). These cardiomyopathies are commonly
affected by myocardial apoptosis and necrosis, oxidative stress,
mitochondrial dysfunction and autophagy, fission and biogenesis,
etc. The exact mechanism by which muscarinic receptors affect these
cardiomyopathies is still worthy of further in-depth research. For
the present review, studies on recent research progress related to
the impact of muscarinic ACh receptors on myocardial function were
collected, aiming to discover the potential signaling transduction
mechanism of muscarinic ACh receptors in the cardiomyocytes and
providing a theoretical basis for further studying myocardial
protective drugs that act on muscarinic ACh receptors.
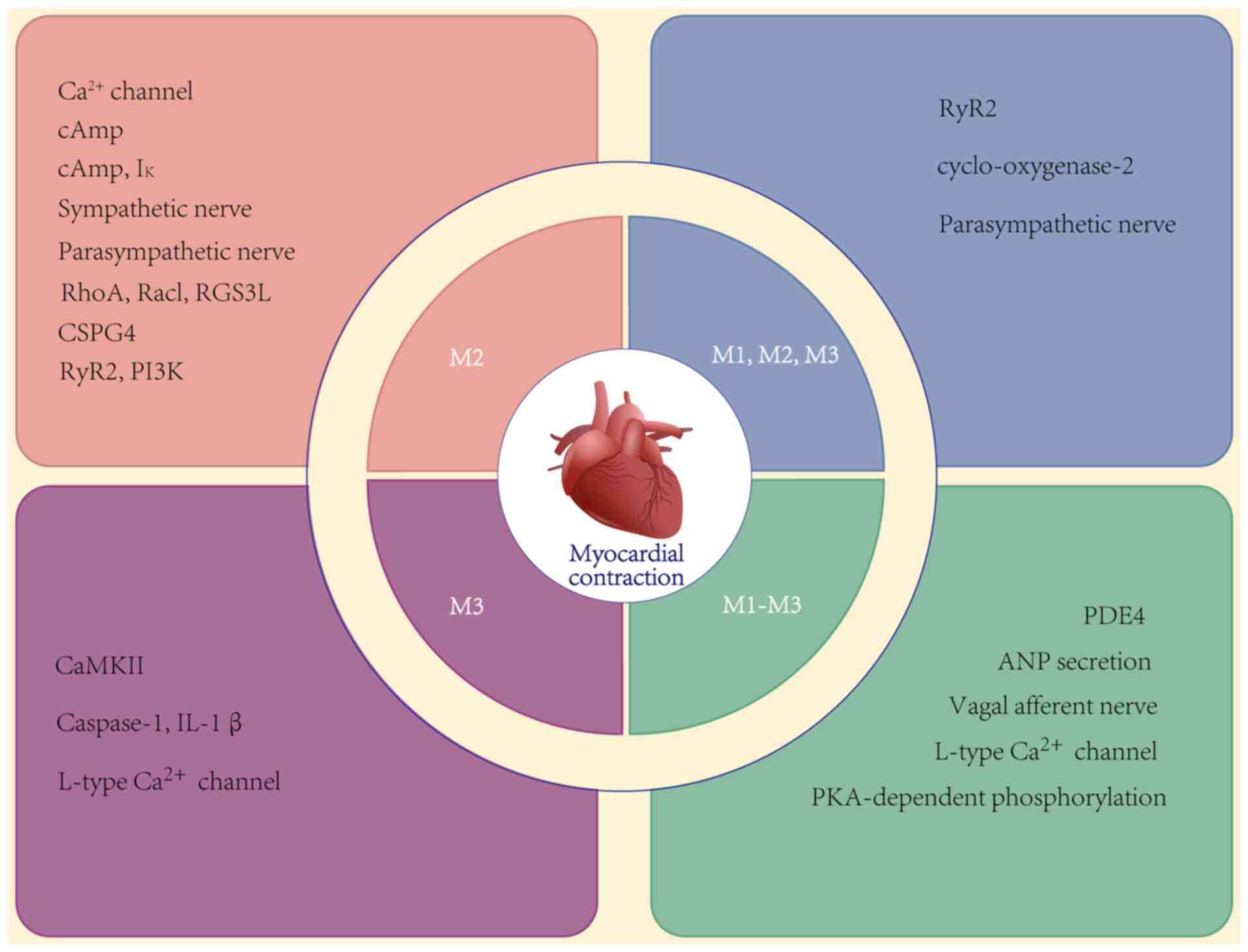
The muscarinic ACh receptor is an important signal
transduction mediator present on the membrane of cardiomyocytes,
which regulates myocardial contraction (7-9).
Over the years, the regulatory mechanism of the M2 muscarinic ACh
receptor in cardiomyocytes has been widely reported. It has been
pointed out that ACh, phthalimide-azo-iperoxo and
naphthalimide-azo-iperoxo can reduce the myocardial contraction
force and cardiac output by binding to the M2 muscarinic ACh
receptor of cardiomyocytes (10,11). A study also found that bile acids
have a new function of slowing down myocardial contraction through
the M2 muscarinic ACh receptor (12). Another study reported that an
agonist or inhibitor of the M2 muscarinic ACh receptor can regulate
the contraction function of the heart by regulating Ras homolog
family member A and Rac family small GTPase 1 through the long
isoform of the regulator of G protein signaling 3 (13). On the contrary, M2 muscarinic ACh
receptor inhibitors such as scopolamine, N-methylscopolamine and
[(3R,4R)-3-(3cyclopropyl-1,2,4,oxadiazol-5-yl)-1-azabicyclo[2.2.1]heptane]
(L-687,306), have been studied and shown to have the effect of
increasing the heart rate and myocardial contraction in rats
(14). The calcium channel in
cardiomyocytes has long been considered an important pathway for
regulating myocardial contraction. It has been reported that ACh
can regulate calcium ions in cardiomyocytes, affecting the
actomyosin interaction mechanism and the stretching of the
sarcomere, thereby changing the myocardial contraction function
(15). Furthermore, myocardial
diseases are highly associated with the functional obstacle of
ryanodine receptor (RyR2). It has been reported that the muscarinic
ACh receptor can reduce the stimulation of the parasympathetic
nervous system and calcium ion/calcium-dependent protein kinase II
(CaMKII)-dependent reactivity, decrease the phosphorylation of RyR2
Ser-2814, lead to increased systolic calcium ion release and reduce
the leakage of abnormal calcium ions, thereby improving calcium ion
cycling efficiency (16). In
addition, it has been proven that muscarinic ACh receptors can
regulate the L-type calcium signal channel, CaMKII and the
phosphoinositide 3-kinase (PI3K)-protein kinase B (AKT)-neuronal
nitric-oxide synthase signaling pathway involved in cardiomyocyte
contraction function (17,18). In all, the muscarinic ACh
receptor controls the homeostasis of calcium ion currents in
cardiomyocytes. The energy metabolism of the heart is also one of
the important functions affected by muscarinic ACh receptors. The
response to M2 receptor activation could be observed when the
agonist stimulates cyclic adenosine monophosphate (cAMP) production
(19). There are relevant
research reports that the non-selective muscarinic ACh receptor
inhibitor atropine can enhance myocardial contraction by blocking
cAMP-specific phosphodiesterase type 4 (20). The changes in cAMP affect protein
kinase A-dependent phosphorylation targets, such as L-type calcium
channels, which play an important role in regulating myocardial
contractility (19). Ursolic
acid could enhance muscarinic ACh receptor-mediated atrial
natriuretic peptide secretion and regulate myocardial contraction
(21). It has been reported that
ACh can regulate the contractility of atrial myocardium by
activating muscarinic receptors and regulating the kinetics of the
actin myosin interaction in cardiomyocytes (15). The release of ACh between
cardiomyocytes can be affected by neural and drug regulation
(22,23). Muscarinic ACh receptors are also
involved in the activation of atrial cyclo-oxygenase-2 and
autoantibody mediates the positive/negative inotropic response to
muscarinic agonists (24,25).
In the heart muscle, the function of the muscarinic ACh receptor is
closely related to the beating and stopping of the heart. It has
been suggested that stimulating the muscarinic ACh receptor can
lead to sudden cardiac arrest, while muscarinic ACh receptor
inhibitors can effectively protect against this symptom (26). Age can regulate the activity of
muscarinic ACh receptors on cardiomyocytes and ultimately affect
myocardial contractility. As age increases, the activity of the
muscarinic ACh receptor decreases, ultimately affecting myocardial
contraction (27-29). The aforementioned research
indicates that the muscarinic ACh receptor can regulate myocardial
contraction of the heart, laying a foundation for the study of
pathological effects of the muscarinic ACh receptor. The effects of
muscarinic ACh receptors on myocardial contraction are listed in
Table I and shown in Fig. 1.
The impact of the muscarinic ACh receptor on
myocardial infarction is significant. Acute myocardial infarction
is the risk disease with the highest mortality rate among patients
with heart disease. The underlying pathogenesis and influencing
factors have been the focus of medical research for numerous years
(30). In myocardial infarction,
the muscarinic ACh receptor can affect the onset and course of
myocardial infarction. Meanwhile, the muscarinic ACh receptor in
the cardiomyocytes can express increased expression in the
conduction block caused by myocardial infarction (31). Some studies have pointed out that
muscarinic ACh receptor inhibitors can worsen the condition of
myocardial infarction by inhibiting the muscarinic ACh receptor on
the cardiomyocyte (32). In
basic and clinical research on myocardial infarction, it has been
shown that the regulation of muscarinic ACh receptors can induce
the occurrence of myocardial infarction, which in turn leads to
heart failure (18,33). The mechanism of action of
muscarinic ACh receptors mediating myocardial infarction is
relatively complex, and it may involve multiple signaling pathways
(34). Among them, the
regulation of calcium channels is the main reason for triggering
myocardial contraction and affecting the disease process of
myocardial infarction. It has been shown that the
receptor-interacting protein 3-induced activation of CaMKII in
cardiomyocytes can trigger oxidative stress in cardiomyocytes,
which has always been an important cause of myocardial infarction
(35). This may be caused by
affecting the opening of the mitochondrial permeability transition
pore and myocardial necrosis. In response to the above mechanism of
myocardial infarction injury, the pharmacological community has
carried out corresponding research on the protective effects of
muscarinic ACh receptors. Certain studies have reported that the
agonist effect of drugs on muscarinic ACh receptors can alleviate
myocardial infarction (36,37). Agitating muscarinic ACh receptors
can protect against myocardial infarction through extracellular
signal-regulated kinase 1/2 (ERK1/2)- and PI3K/AKT-mediated
signaling pathways (38), and
play a protective role in hypoxia and injury of cardiomyocytes
(39). ACh can also alleviate
the injury of cardiomyopathy by affecting adenosine
5′-monophosphate-activated protein kinase (AMPK) signaling and
mitochondrial cristae reconstruction through interaction with
muscarinic ACh receptors (40).
Studies have shown that ACh can reduce the transient calcium
amplitude of muscarinic ACh receptors to regulate the levels of
calcium and iron, thereby alleviating oxidative stress injury
(41). Vagal nerve stimulation
experiments have shown that the increase in ACh levels can
upregulate the expression of vascular endothelial growth factor
A/B, and promote angiogenesis and protection, thereby playing a
protective role in myocardial infarction (42,43). This result was later confirmed by
the repair of the injured coronary artery and cardiomyocytes during
infarction through the M2 muscarinic ACh receptor (44). Studies have shown that
acetylcholinesterase (AChE) inhibitors can better protect against
myocardial ischemia, myocardial infarction and heart failure than
simply stimulating the release of ACh (45,46).
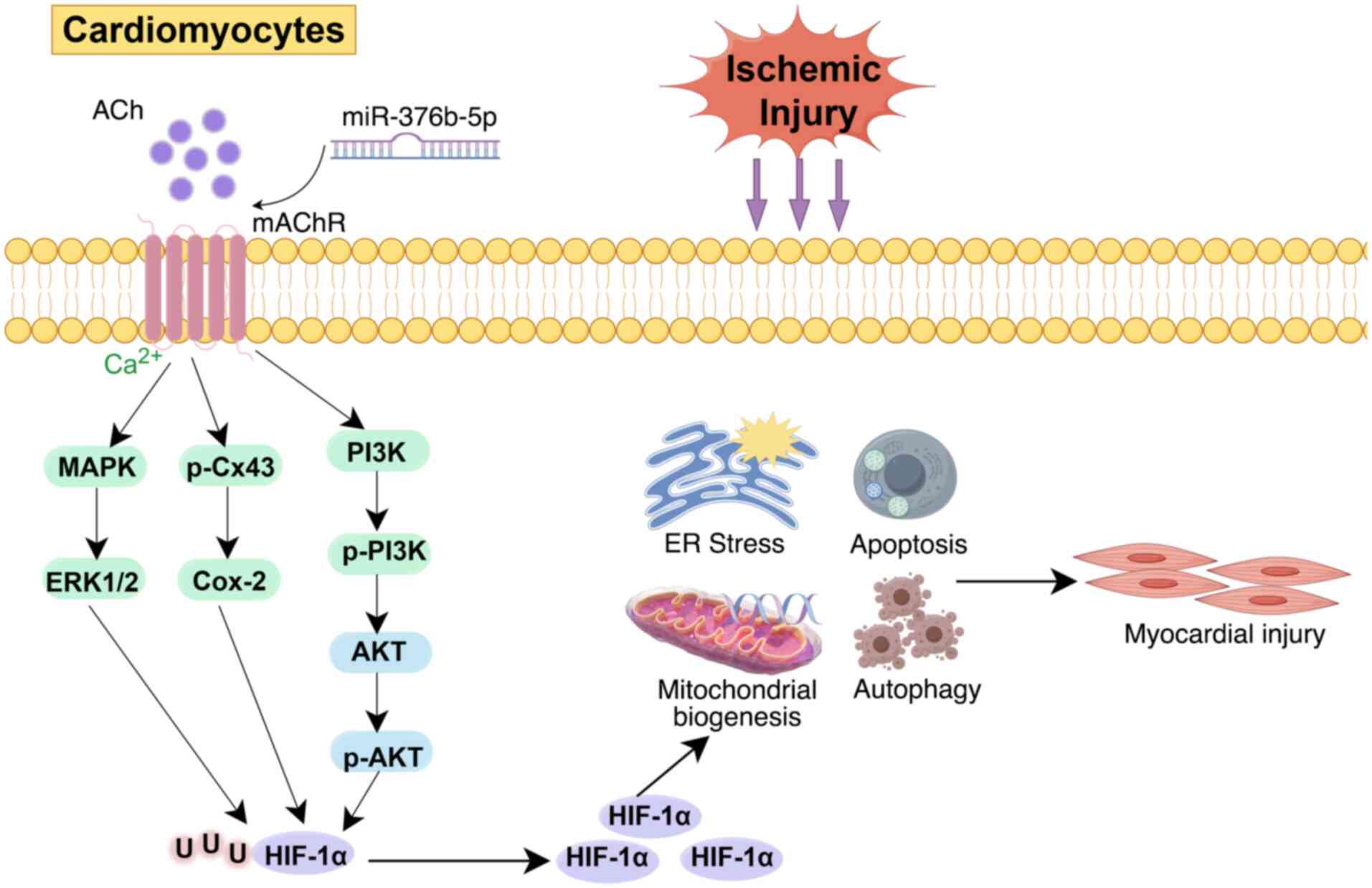
In recent years, the M3 muscarinic ACh receptor, as
an important regulatory receptor in cardiomyocytes, has received
widespread attention from the cardiovascular research community.
Another study showed that inhibiting microRNA (miR)-376b-5p can
affect the activation of the M3 muscarinic ACh receptor, thereby
regulating downstream calcium signaling and reactive oxygen
species-related cardioprotection pathways (47). Zhao et al (48) reported that agonist activation of
the M3 muscarinic ACh receptor can alleviate myocardial injury
caused by myocardial ischemia by regulating connexin 43 (Cx43)
phosphorylation and cyclooxygenase-2 expression. Another study
showed that chlorine-based choline can alleviate myocardial injury
under the transverse aortic constriction myocardial ischemic model
by agonist activation of the M3 muscarinic ACh receptor, while the
M3 muscarinic ACh receptor inhibitor
4-diphenylacetoxy-N-methylpiperidine methiodide had the opposite
effect (49,50). Inhibiting the M3 muscarinic ACh
receptor was also observed to promote the influx of calcium ions
into cells after myocardial ischemia, interfering with normal
cellular energy metabolism and accelerating the death of
cardiomyocytes (18). Wang et
al (51) reported the
signaling role of beta-catenin in the regulation of the downstream
anti-apoptotic protein Bcl-2 mediated by the M3 muscarinic ACh
receptor. Therefore, the regulatory role of the M3 muscarinic ACh
receptor on myocardial infarction is relatively certain (Fig. 2).
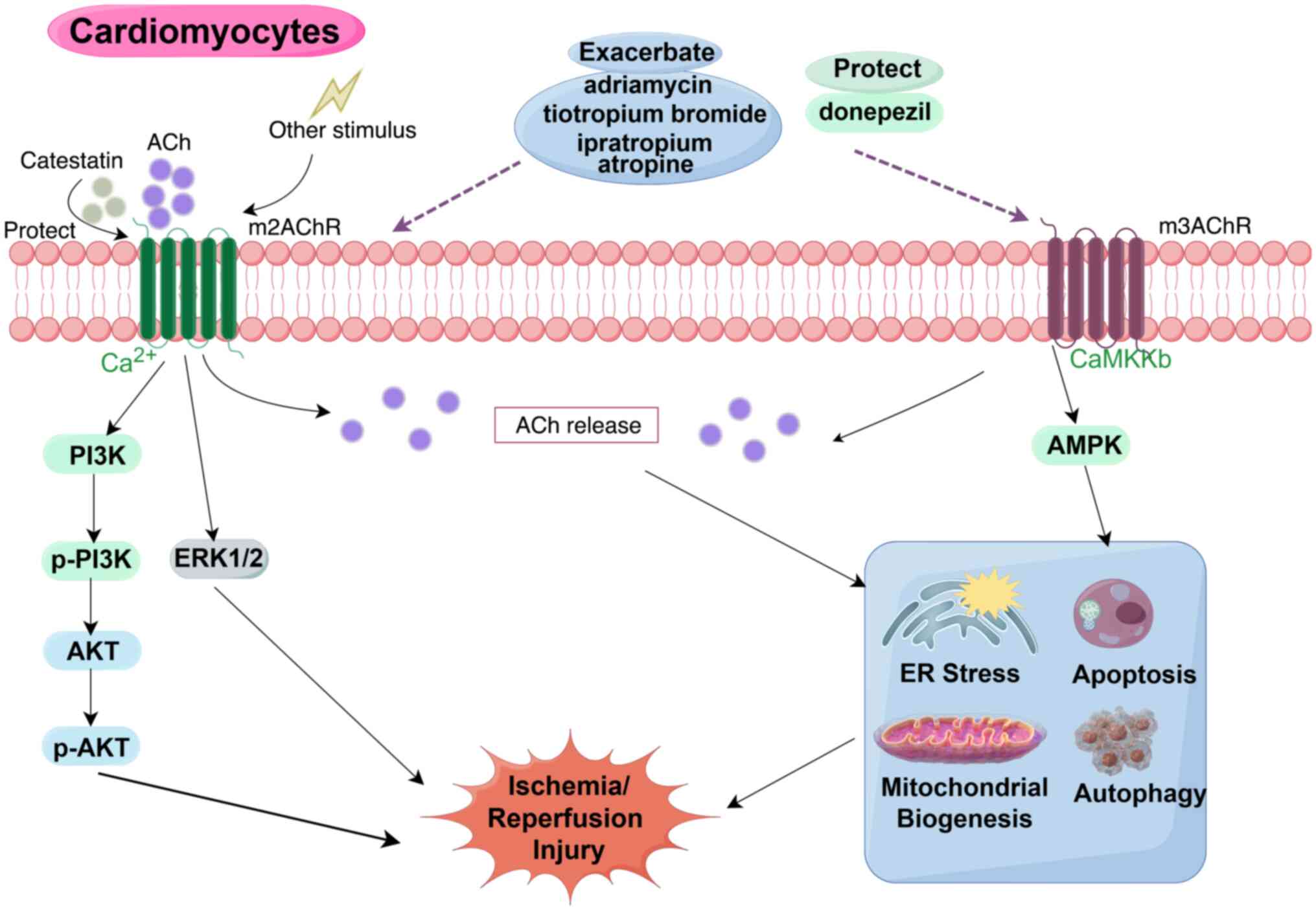
Existing studies have shown that
ischemia/reperfusion injury is closely related to the regulation of
muscarinic ACh receptors (Fig.
3). According to relevant research reports, various
anti-muscarinic ACh receptor drugs, including ipratropium,
tiotropium bromide, atropine and adriamycin, have been reported to
increase the incidence of ischemic/reperfusion myocardial injury by
regulating the muscarinic ACh receptor, resulting in cardiac
toxicity (18,52,53). ACh can play a protective role in
ischemic reperfusion injury by stimulating the muscarinic ACh
receptor. Therefore, exploring the protective mechanism of the
muscarinic ACh receptor against ischemic reperfusion injury is
becoming a new research hotspot in the field of myocardial
ischemia/reperfusion injury. There is evidence that by stimulating
the muscarinic ACh receptor on the heart, it can have a significant
protective effect on the mouse myocardial ischemia-reperfusion
injury model, reducing the area of myocardial injury caused by
ischemia-reperfusion (34). It
was also shown that stimulation of the myocardial muscarinic ACh
receptor can cause the release of ACh mediated by the muscarinic
ACh receptor, resulting in a response of ischemic preconditioning,
which can protect against myocardial ischemia-reperfusion injury
(54). Donepezil and other
cholinergic receptor agonists can protect against cell apoptosis
after myocardial ischemia-reperfusion injury by regulating the
level of phosphorylated (p)-Cx43 (ser368) and the balance of
mitochondrial activity and autophagy (55). ACh can also alleviate endoplasmic
reticulum stress in myocardial cells and increase cell viability
(56), blocking mitochondrial
unfolding protein, thereby reducing myocardial cell apoptosis
induced by hypoxia/reoxygenation (57). Existing studies have shown that
vagus nerve stimulation activating the muscarinic ACh receptor can
reduce mitochondrial function through the M3 muscarinic ACh
receptor/CaMK kinase b/AMPK signaling pathway to protect against
myocardial ischemic injury (58). The mechanism of this ischemic
myocardial injury may be myocardial cell apoptosis and related
metabolic dysfunction. Experiments with catestatin binding to the
M2 muscarinic ACh receptor indicate that the M2 muscarinic ACh
receptor can play a myocardial protective role by regulating the
ERK1/2 and PI3K/AKT signaling pathways in cells (38).
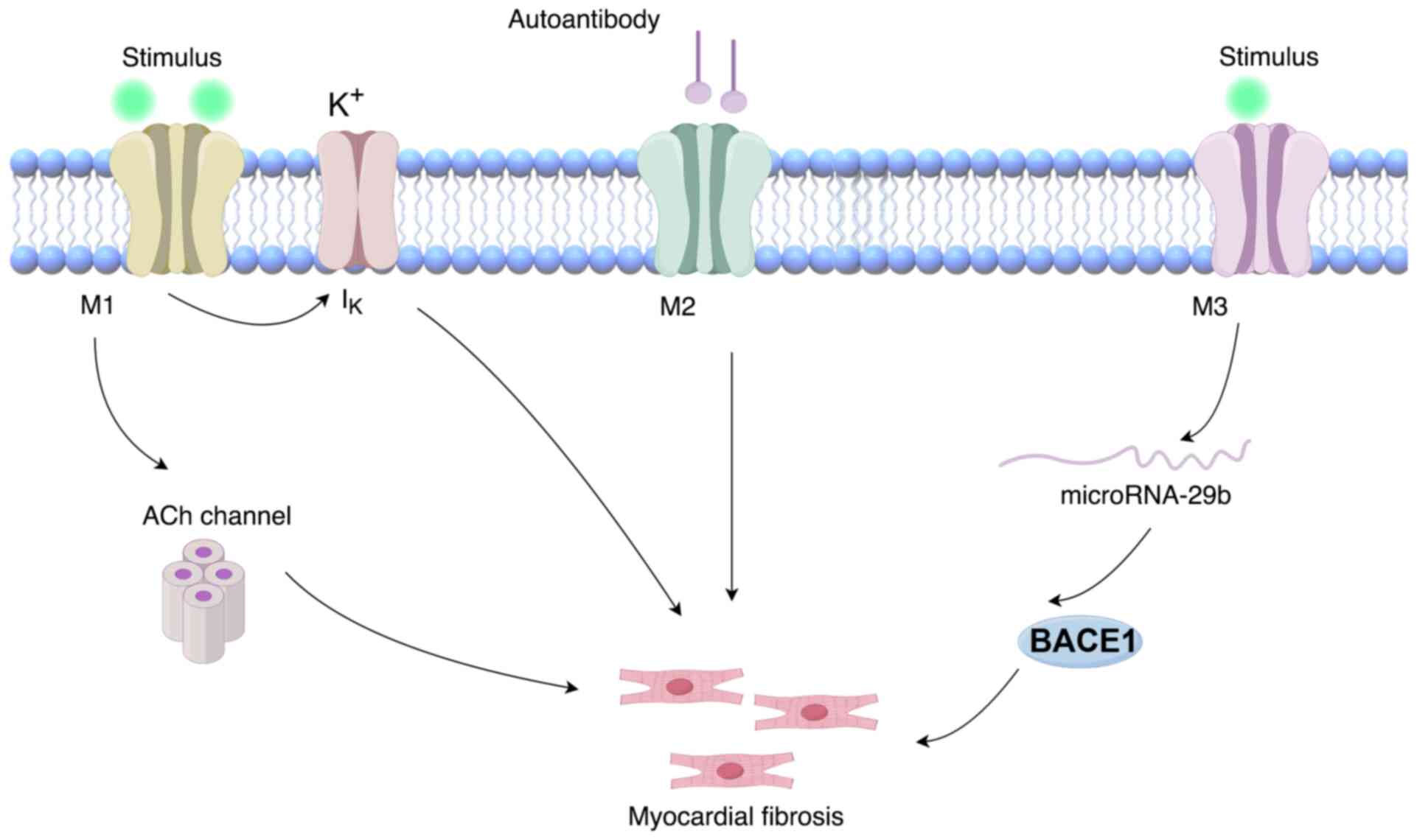
Myocardial fibrosis can occur in various
cardiovascular diseases and has been considered one of the most
common conditions in cardiomyopathy, the pathogenesis of which
remains to be fully elucidated. Although cardiac fibroblasts are
the main cells that constitute heart tissue, the mechanism of
muscarinic ACh receptor-induced myocardial fibrosis still requires
further research (Fig. 4). In
addition, relevant neural studies have shown that stimulation of
the vagus nerve, which is the same as the parasympathetic nerve,
and exogenous stimulation of the M3 muscarinic ACh receptor, can
alleviate the process of myocardial fibrosis via the
miR-29b/beta-site app cleaving enzyme 1 axis both in vivo
and in in vitro experimental models (49,59). An in vitro experimental
study showed that inhibiting ACh levels can induce the formation of
cardiac fibroblasts (60). A
previous clinical study has shown that the amount of M2 muscarinic
ACh receptor autoantibody can be used as a suitable detection
method for judging the severity of the pathological and
physiological conditions of patients with left atrial fibrosis
(61). In addition, recent
experimental results of a human mechanistic study also showed that
the level of M2 muscarinic ACh receptor autoantibody in the serum
of patients with atrial fibrosis was significantly higher than that
in the non-atrial fibrosis group, and immunohistochemical analysis
and western blot analysis of left atrial appendage tissue suggested
that M2 muscarinic ACh receptor is closely related to the process
of myocardial fibrosis (62).
All of the above evidence indicated that the muscarinic ACh
receptor has an important connection with the onset, diagnosis and
treatment of myocardial fibrosis. Another study showed that the M1
muscarinic ACh receptor is significantly upregulated in patients
with chronic atrial fibrillation and can affect atrial fibrillation
by regulating the IK,Ach channel in human atrial
myocytes (63).
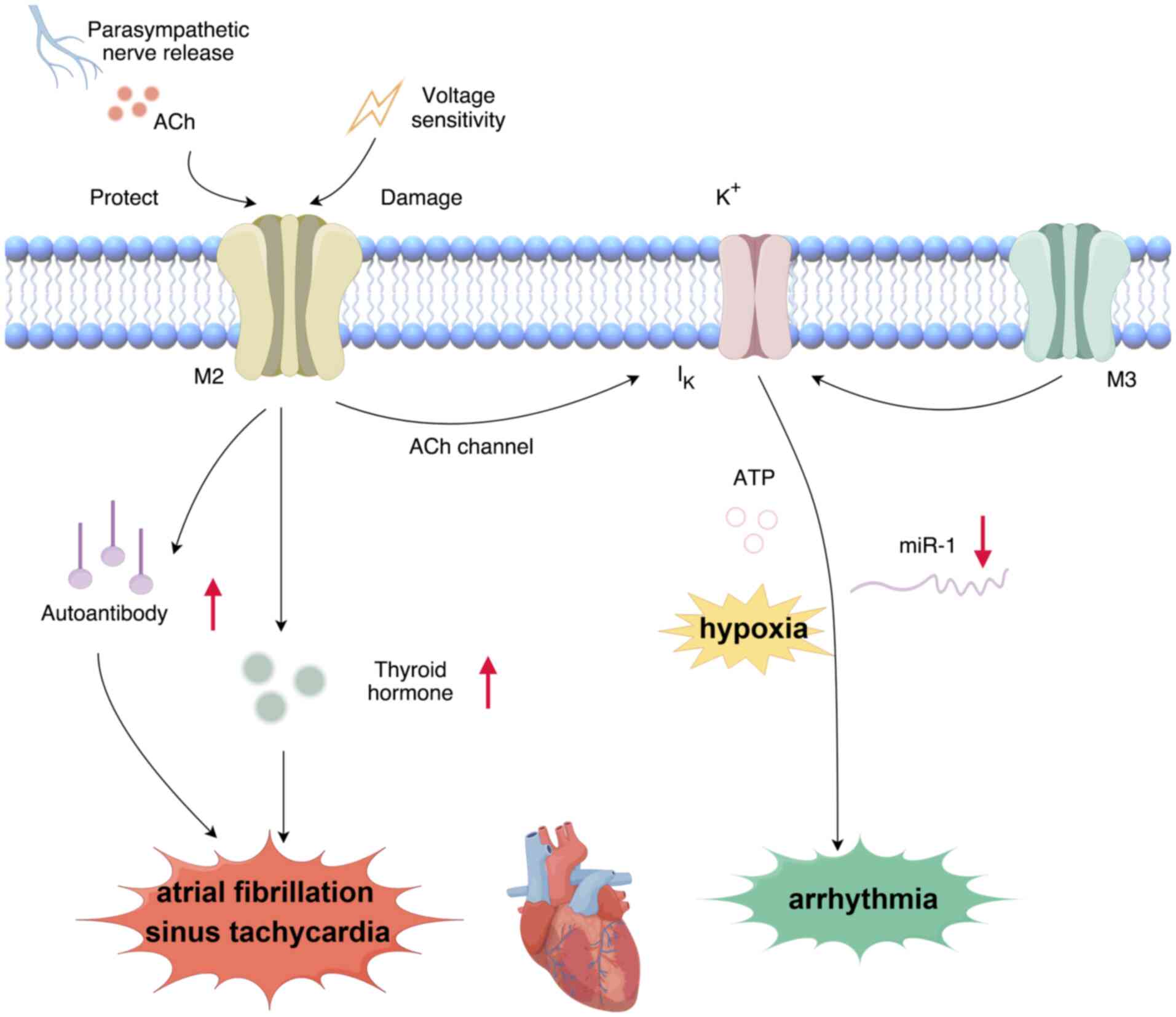
Recently, it has been shown that arrhythmia is
related to the regulation of muscarinic ACh receptors (Fig. 5). Activation of the muscarinic
ACh receptor can reduce heart rate and even cause bradycardia
(64). Studies have confirmed
that blocking the parasympathetic nerve in the heart is an
important factor in inducing ventricular arrhythmia and increasing
myocardial energy consumption (65). In the study of arrhythmia, the
regulatory mechanism of IK channels has recently
attracted attention. Studies have shown that agonists of muscarinic
ACh receptors, including ACh, can alleviate the symptoms of cardiac
arrhythmia without affecting the contractility of the heart
(66). The mechanism includes
hypoxia and regulation of IK-ATP (67-69). Atrial fibrillation is one of the
important symptoms in patients with arrhythmia, and it is closely
related to the regulatory effect of muscarinic ACh receptors on
heart function. Therefore, numerous scholars have conducted
in-depth research on the association between atrial fibrillation
and myocardial muscarinic ACh receptors. It has been shown that
inhibiting the release of ACh can effectively inhibit the effect of
atrial fibrillation in patients after cardiac surgery (70). The specific manifestation showed
that M2 muscarinic Ach receptors could induce the release of
autoantibodies and thyroid hormones, promoting the susceptibility
to atrial fibrillation and sinus tachycardia (27,71). Researchers have found that the
level of autoantibodies to M2 muscarinic ACh receptors in patients
with atrial fibrillation shows a significant increase (62). Another study reported that
changes in the voltage sensitivity of M2 muscarinic ACh receptors
can lead to heart diseases such as atrial fibrillation and sinus
tachycardia (72). Furthermore,
M3 muscarinic ACh receptor overexpression was observed to reduce
the incidence and mortality of arrhythmia after myocardial
ischemia-reperfusion injury. This effect may be mediated by
downregulating the expression of arrhythmogenic miR-1 and
increasing the inward rectifier potassium current, which may be a
new anti-arrhythmic strategy for diagnosis (73). Other studies have shown that the
release of ACh triggered by parasympathetic nerve cells can
increase the sensitivity of animals to arrhythmia and increase the
heart rate (74-76).
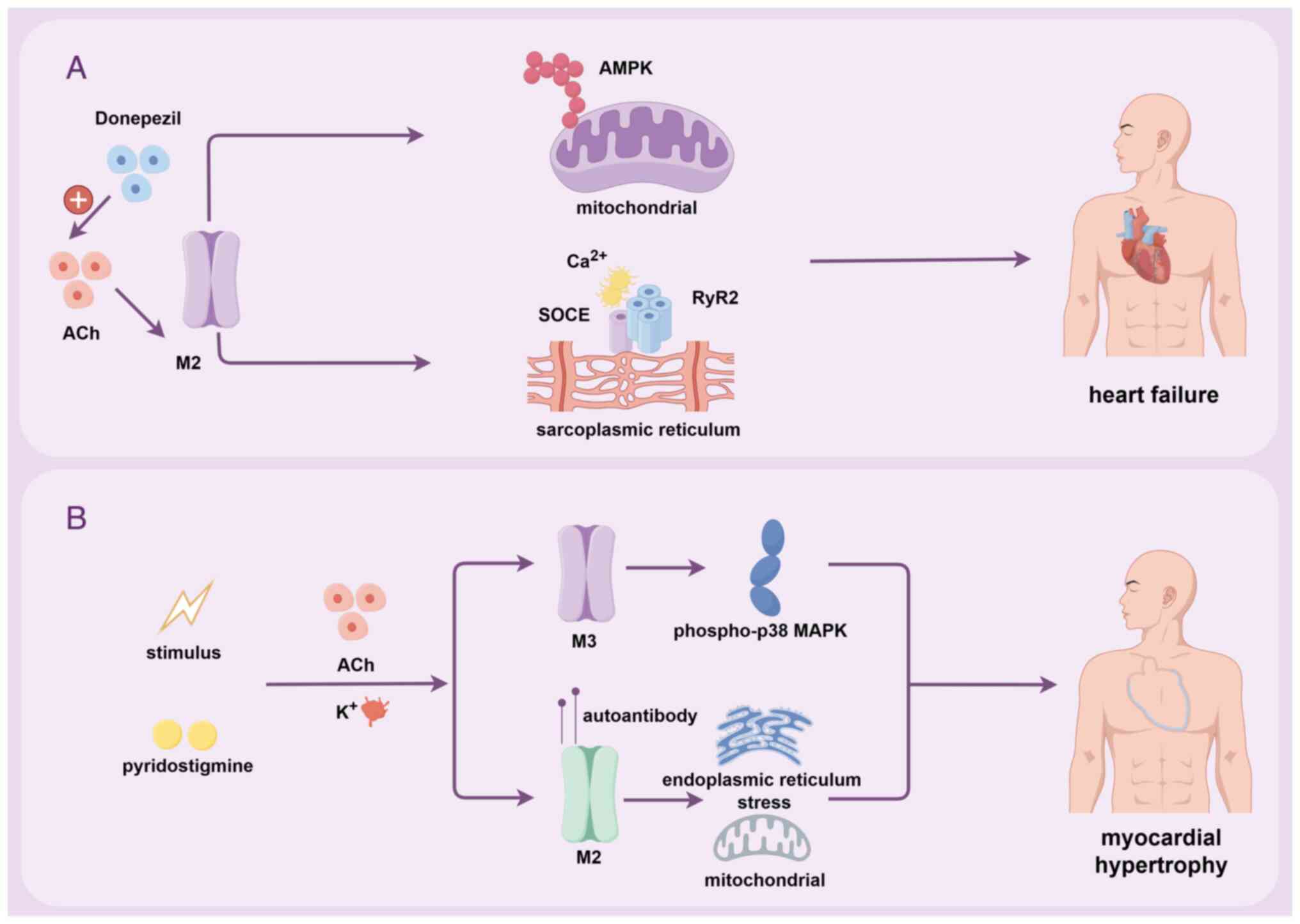
An increasing number of studies have shown that
stimulating the muscarinic ACh receptor through drugs or neural
transmission may become an important means of treating heart
failure (77) (Fig. 6). Certain studies have shown that
the continuous excitation of muscarinic ACh receptor by ACh can
release calcium ions through the RyR2-mediated calcium store of the
sarcoplasmic reticulum in cardiomyocytes, and the regulation of
calcium signals related to store-operated calcium entry can
alleviate heart failure (78,79). Another study has shown that ACh
can serve as a key compensatory mediator in the development of
heart failure in mice by stimulating the M2 muscarinic ACh receptor
of cardiomyocytes to alleviate the occurrence and development of
ventricular remodeling and heart failure (80,81). The drug donepezil, which has the
function of AChE inhibitor, can increase ACh in rat hearts and play
a long-term protective effect on heart failure (82). Research data show that increasing
ACh by using central or peripheral AChE inhibitors can effectively
improve heart failure and the heart's autonomic nervous imbalance
and hemodynamic changes in patients with hypertension (83). ACh can regulate the effect of
AMPK on mitochondrial cristae remodeling by stimulating the
muscarinic ACh receptor, thereby alleviating the hypertrophy of
cardiomyocytes induced by palmitic acid (40).
Myocardial hypertrophy is a common clinical
cardiomyopathy, which is also closely related to the induction of
muscarinic ACh receptor (84).
One of the reasons for myocardial hypertrophy may be related to the
decrease in K+ repolarization associated with the M3
muscarinic ACh receptor, which leads to the harmful myocardial
remodeling. Overexpression of M3 muscarinic ACh receptor in
cardiomyocytes can alleviate the adverse myocardial remodeling
(85). Wang et al
(86) found that cardiac
hypertrophy can play a protective role by inhibiting the P38/p-p38
mitogen-activated protein kinase signaling pathway and blocking the
M3 muscarinic ACh receptor. The role of M2 muscarinic ACh receptor
in regulating myocardial hypertrophy is also relatively obvious.
Studies show that aerobic exercise can improve myocardial
hypertrophy by regulating M2 muscarinic ACh receptors, affecting
mitochondrial quality control and endoplasmic reticulum stress in
cardiomyocytes (87). It has
been shown that autoantibodies to M2 muscarinic ACh receptor can
also cause myocardial hypertrophy in rabbits (88). The AChE inhibitor pyridostigmine
can improve myocardial hypertrophy by prolonging the duration of
ACh on the M2 muscarinic ACh receptor. These results were confirmed
by echocardiography, immunofluorescence and precipitation methods
(89). Intermittent excessive
activation of M2 muscarinic ACh receptors can also exacerbate
myocardial hypertrophy through oxidative stress (90).
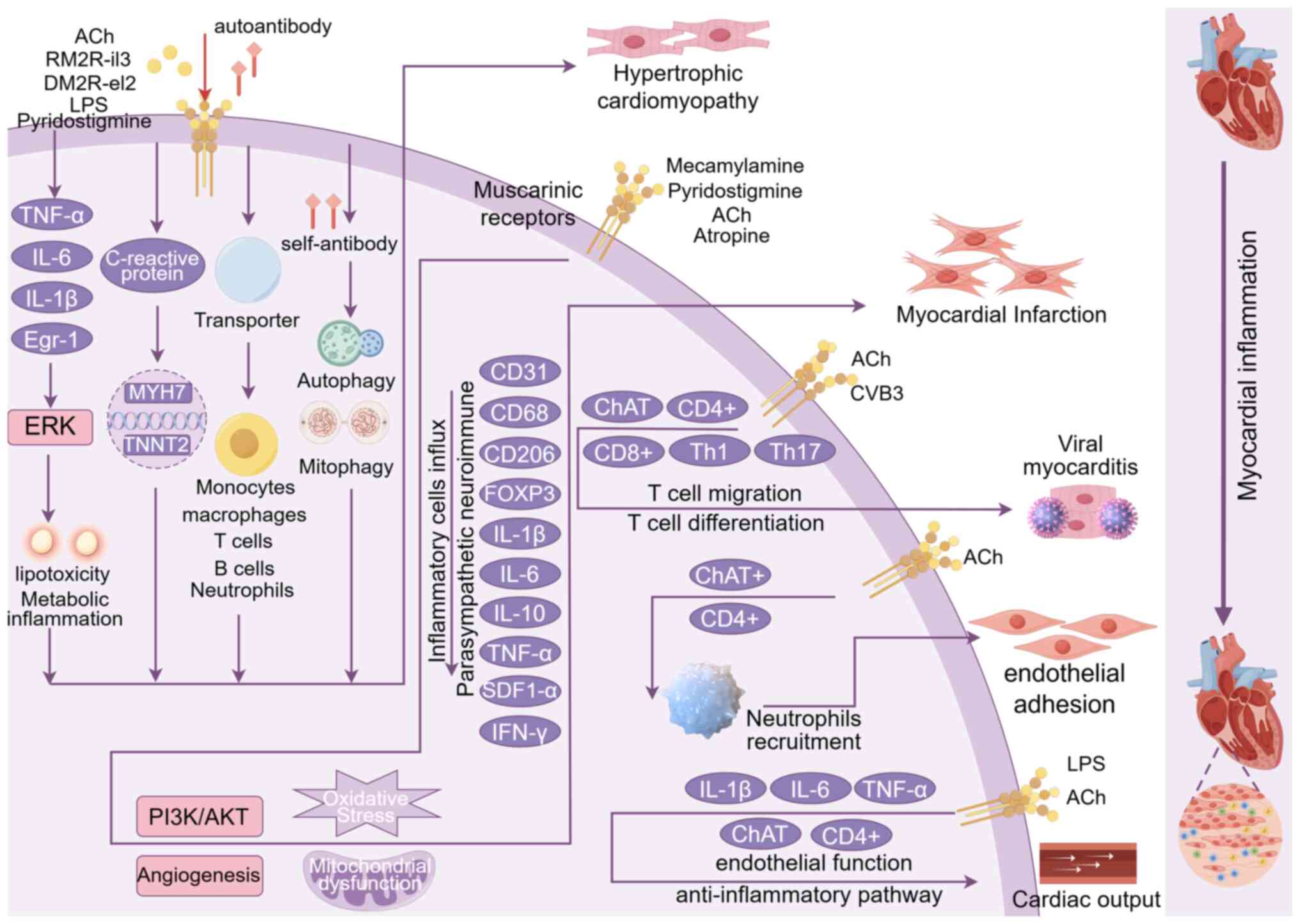
The regulation of the inflammatory response by the
muscarinic ACh receptor has also been widely studied (Fig. 7). The role of the muscarinic ACh
receptor in regulating myocardial inflammation is mainly achieved
by affecting neural transmission and changes in lymphocytes.
Studies have shown that, compared to the normal group, myocardial
inflammation confirmed by enzyme-linked immunosorbent assay is
closely related to the increase in the level of self-antibodies
mediated by the M2 muscarinic ACh receptor (91), and the autoimmune antibodies show
a role in heart function damage and myocardial inflammation
(92). Through stimulating
cholinergic neurons, a study showed good anti-inflammatory effects
in a heart model of Wistar rats through immunohistochemistry and
cytokine measurement (93). In
addition, a study suggested that the inhibition of AChE by
bromocriptine enhances the function of ACh, thereby preventing
inflammatory autonomic dysfunction (94). The muscarinic ACh receptor can
also regulate the inflammatory immune mediators of myocardial
cells, such as the anti-inflammatory effect of T lymphocytes
(95). Cox et al
(96) reported that infection
can promote the increase in the expression of ACh transferase
(ChAT) in CD4+T and CD8+T cells, thereby enhancing the immune
response. Furthermore, the release of ACh and ChAT+ B lymphocytes
has been shown to inhibit the activation of macrophages (97). In the viral myocarditis mouse
model, the anti-inflammatory pathway of ACh may be achieved through
the differentiation of CD4+ T cells and the regulation of the
expression of Th1 and Th17 cytokines (98). This may reveal the current
regulatory mechanism of myocardial inflammation, such as myocardial
cell lesions and cell infiltration symptoms. Exogenous ACh
stimulation may activate the PI3K/AKT pathway (99), and the ERK/early growth
response-1 pathway (100,101), thereby alleviating inflammation
and oxidation. Similarly, it has been found that a small population
of ChAT+ natural killer cells, which are, however,
transcriptionally distinct, have immune protective effects in a
mouse model (102). The
stimulation of the muscarinic ACh receptor can also alleviate
cardiac inflammation through the muscarinic ACh and nicotine
receptors. Recently, the regulatory effect of the non-neuronal
cholinergic system on myocardial inflammation has also been
reported (97). A study
suggested that the non-neuronal cholinergic system can regulate the
activation and inhibition of inflammatory cells, such as the number
of macrophages and Forkhead box protein P3+ T cells in myocardium
through the muscarinic ACh receptor (103). However, studies have indicated
that, although the non-neuronal cholinergic system can regulate the
release of ACh and produce the effect of stimulating the muscarinic
ACh receptor, it was not found to improve or exacerbate the
myocardial inflammatory response (104,105). Therefore, whether the
non-neuronal cholinergic system can play a role in the myocardial
inflammatory response still requires further research. All of the
roles of myocardial inflammation through the regulation of
muscarinic ACh receptors are listed in Table II.
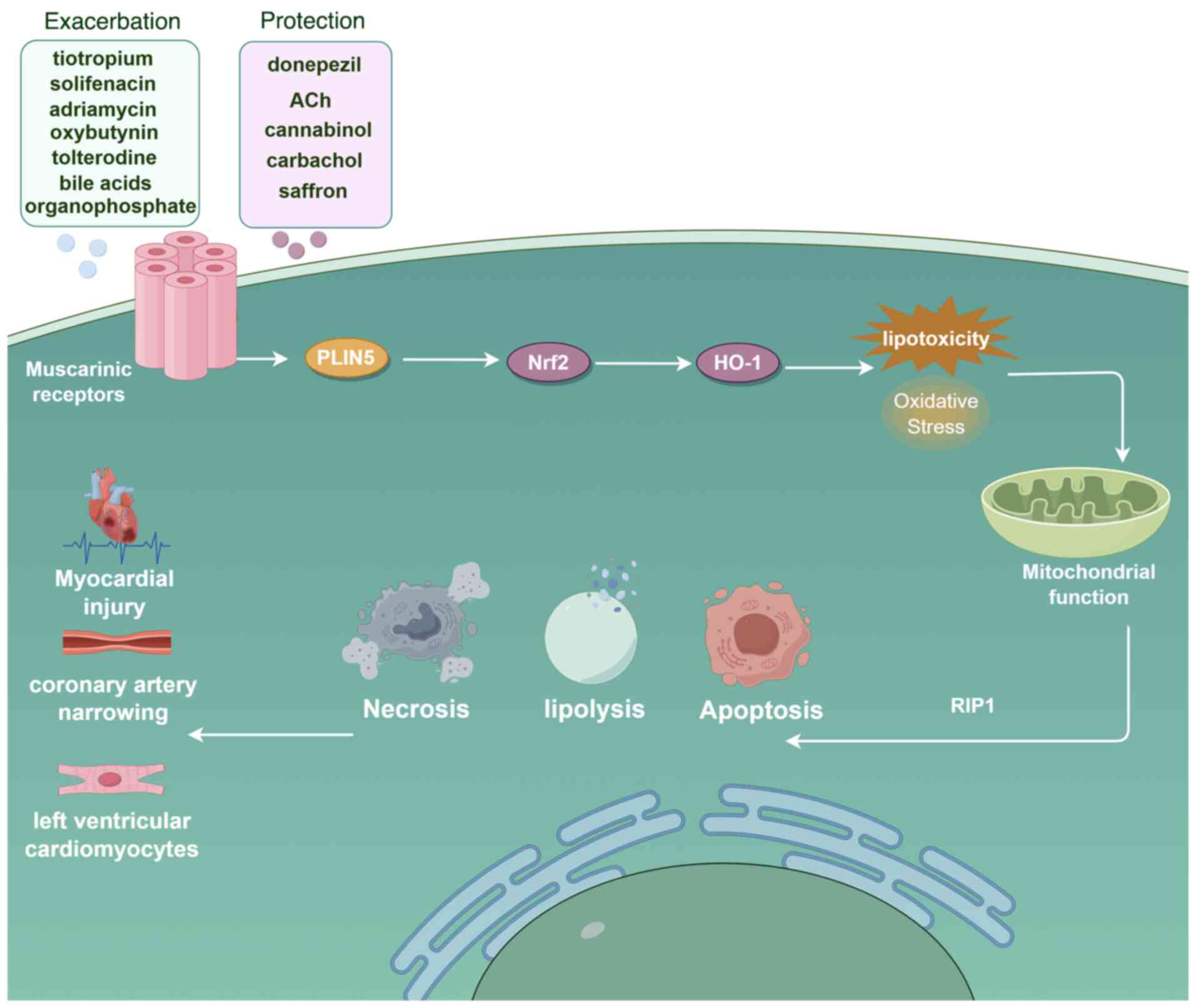
Long-term clinical studies have found that numerous
anti-muscarinic ACh receptor drugs have cardiotoxic effects on the
heart (32,106). Long-acting muscarinic ACh
inhibitors such as tiotropium and other tracheal dilating drugs
have been reported to exacerbate myocardial injury (107,108) and increase the incidence rate
of acute coronary syndrome (109). The use of muscarinic ACh
receptor inhibitors such as oxybutynin, solifenacin and
tolterodine, which are used to treat hair loss, has been found to
be associated with the incidence rate of myocardial disease
(110). Adriamycin has long
been considered to have cardiotoxic effects, but its mechanism of
toxicity in the body has remained elusive. In recent years, studies
on its regulation of the muscarinic ACh receptor in cardiomyocytes
have been ongoing. Research suggests that the activation of the
muscarinic ACh receptor can protect against myocardial injury and
cardiomyocyte apoptosis caused by adriamycin, mediated by the
nuclear factor erythroid 2-related factor 2/heme-oxygenase-1
pathway (111). It has been
shown that donepezil can protect against oxidative stress and
mitochondrial function deficiency, reduce the apoptotic ratio of
Bax/Bcl-2 and cleaved-caspase 3/caspase 3, and protect against
receptor-interacting protein kinase 1-mediated necrosis of
cardiomyocytes caused by adriamycin by activating the muscarinic
ACh receptor (112). Another
study indicated that saffron can exert antioxidant properties and
inhibit the apoptosis pathway of myocardial cells through the M2
muscarinic ACh receptors, thereby preventing myocardial toxicity
caused by organophosphate poisoning (113). Furthermore, increased ACh under
parasympathetic stimulation can inhibit the programmed death of
cardiomyocytes, protecting against adriamycin-induced myocardial
toxicity (114). In addition,
high concentrations of bile acids were shown to produce cardiotoxic
effects by acting on the M2 muscarinic ACh receptor (12). ACh can promote lipolysis and
activate mitochondrial interactions through perilipin 5,
effectively inhibiting cardiomyocyte apoptosis and lipotoxicity
(115). The release of large
amounts of carbachol stimulates ACh to activate the muscarinic ACh
receptor, leading to coronary artery narrowing and changes in the
structure of left ventricular cardiomyocytes in rats, causing
myocardial toxicity, while long-term treatment with cannabinol can
significantly inhibit this toxic effect (116). A schematic illustrating the
mechanisms of drugs acting on muscarinic ACh receptors with
cardiotoxic effects is provided in Fig. 8.
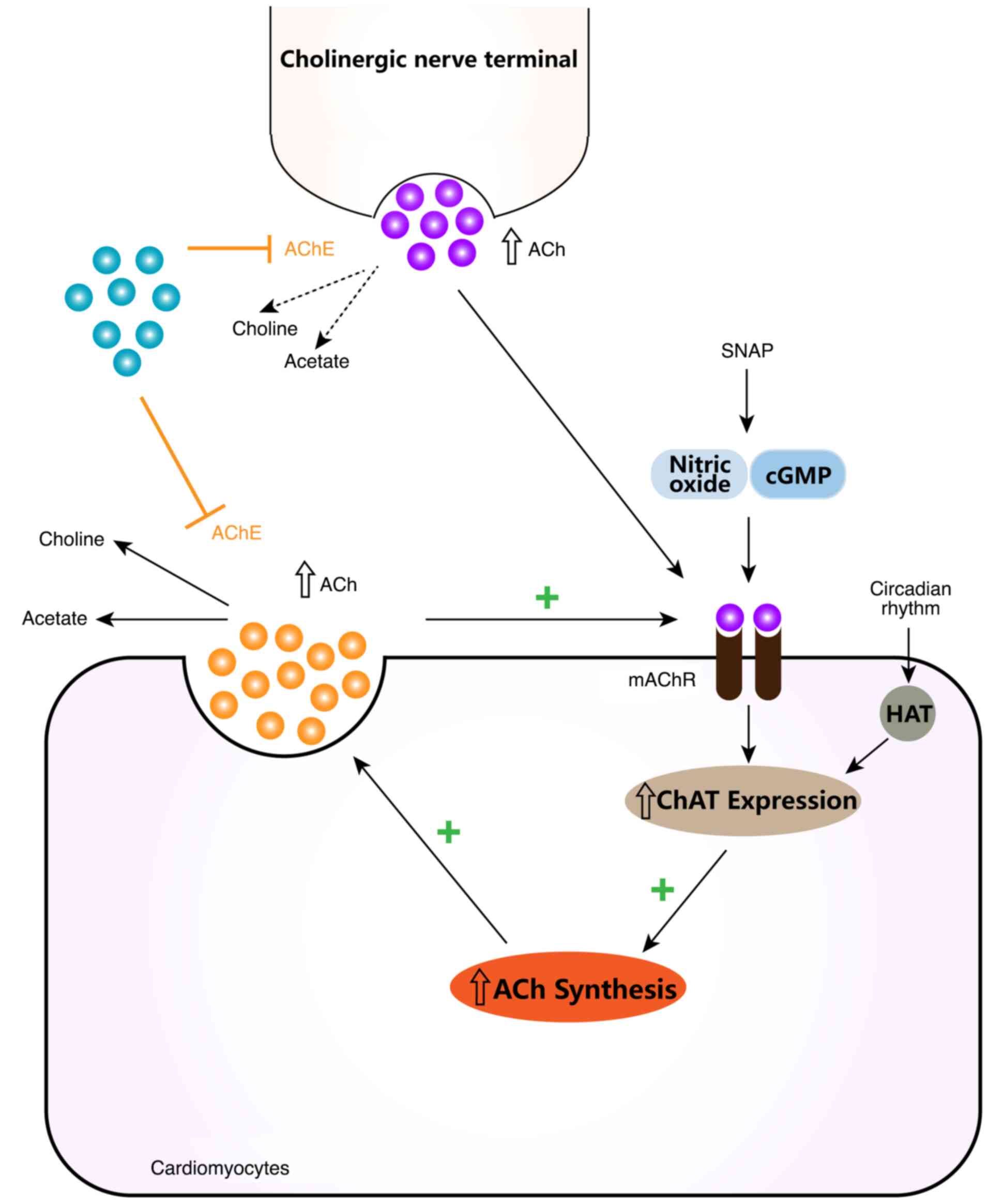
With the continuous deepening of the research on
muscarinic ACh receptors, a unique cholinergic regulatory factor
production and circulatory system was discovered in recent years,
which has attracted widespread attention from pharmacologists. The
degradation of ACh in the body by AChE also maintains it at an
appropriate level, which may be due to the regulatory function of
the non-neural cholinergic system (NNCS) (117). In the heart, this is a
self-regulating cholinergic synthesis and secretion system of
cardiomyocytes, and except for nerve cells, almost all components
of the neural ACh system are retained. The NNCS may contain
components such as ChAT, ACh, nicotinic/muscarinic ACh receptor,
high-affinity choline uptake and cholinesterase. They can
participate in cell proliferation, migration, differentiation, cell
barrier formation, programmed cell death, hypoxia/reoxygenation
injury and other cellular functions and metabolic processes
(118-120). The acute promyelocytic leukemia
cell line NB-4 can regulate the expression of M3 muscarinic ACh
receptors under the stimulation of choline, thus exerting its
anti-inflammatory effects in vivo (121). ChAT-transgenic cells have been
confirmed to have the potential of systemic anti-inflammatory
response, which can alleviate inflammatory lesions (122,123). Cardiomyocytes increase the
expression of AChE through the activation of muscarinic ACh
receptors and ChAT gene transcription, and then synthesize ACh.
Both RNA interference experiments of ChAT gene and M-receptor
inhibitor competition experiments have proved this (124). Further research showed that,
through the regulation of the NNCS in cardiomyocytes, the
expression of ChAT is higher in female hearts than in males. The
circadian rhythm has an important impact on histone
acetyltransferase activity, thereby regulating the expression of
ChAT (125). The newly
discovered S-nitroso-N-acetyl-DL-penicillamine can produce nitric
oxide and cyclic guanosine monophosphate, activate the expression
of the AChE gene and the function of muscarinic ACh receptors, and
have a protective effect against myocardial injury (126). The muscarinic ACh receptors on
the NNCS are presented in Fig.
9. Although numerous relevant research achievements have been
made in this direction in recent years, there are still many gaps
and deficiencies in the study of NNCS in cardiomyocytes that need
to be filled. In the future, this may provide a new diagnostic and
therapeutic method for myocardial infarction and inflammatory
protection.
The muscarinic ACh receptor and cardiac myocytes are
both involved in the regulation of heart function. Current research
on the myocardial function and diseases related to the muscarinic
ACh receptor shows that its range of action is closely related to
numerous heart diseases and physiological functions, but its
potential mechanism of action is still being continuously explored.
So far, the function and structure of the muscarinic ACh receptor
have been successively excavated by the research community, but the
regulatory role it plays in the function of cardiomyocytes, as well
as its physiological and pathological mechanisms of action, still
remain to be fully elucidated. This article summarized the research
progress on myocardial contraction and related diseases mediated by
muscarinic ACh receptors. It was found that muscarinic ACh
receptors can play important roles in regulating calcium
homeostasis, mitochondrial dysfunction, cardiomyocyte apoptosis and
autophagy, inflammatory cells and mediators, providing potential
new research directions for the development of cardiomyopathy drugs
in the future. With the introduction of the new concept of the
myocardial NNCS, the research on the muscarinic ACh receptor in the
field of myocardial function and related diseases shows further
extensive prospects and value. These findings will provide new
theoretical evidence for muscarinic ACh receptors as potential
targets for myocardial protective drugs.
Not applicable.
CS was involved in writing the original draft, data
curation and conceptualization of the study. QZ contributed to
writing the original draft and was responsible for methodology and
visualization. ZS and YL were involved in reviewing and editing the
manuscript. SC contributed to the review and editing of the
manuscript and was responsible for the supervision and
conceptualization of the study. Data authentication is not
applicable. All authors have read and approved the final
manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
Not applicable.
This work was supported by the National Natural Science
Foundation of China (grant no. 81904147), the Youth Research
Project of Health Commission of Anhui Province (grant no.
AHWJ2023A30241), the Scientific Research Foundation of Education
Department of Anhui Province of China (grant no. 2024AH051007) and
the Scientific Research Foundation of Education Department of Anhui
Province of China (grant no. 2023AH050842).
|
1
|
Lymperopoulos A, Cora N, Maning J, Brill
AR and Sizova A: Signaling and function of cardiac autonomic
nervous system receptors: Insights from the GPCR signalling
universe. FEBS J. 288:2645–2659. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Santos R, Ursu O, Gaulton A, Bento AP,
Donadi RS, Bologa CG, Karlsson A, Al-Lazikani B, Hersey A, Oprea TI
and Overington JP: A comprehensive map of molecular drug targets.
Nat Rev Drug Discov. 16:19–34. 2017. View Article : Google Scholar
|
|
3
|
Maeda S, Qu Q, Robertson MJ, Skiniotis G
and Kobilka BK: Structures of the M1 and M2 muscarinic
acetylcholine receptor/G-protein complexes. Science. 364:552–557.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Foster DJ: Muscarinic receptors: From
clinic to bench to clinic. Trends Pharmacol Sci. 43:461–463. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Saternos HC, Almarghalani DA, Gibson HM,
Meqdad MA, Antypas RB, Lingireddy A and AbouAlaiwi WA: Distribution
and function of the muscarinic receptor subtypes in the
cardiovascular system. Physiol Genomics. 50:1–9. 2018. View Article : Google Scholar
|
|
6
|
Palma JA: Muscarinic control of
cardiovascular function in humans: A review of current clinical
evidence. Clin Auton Res. 34:31–44. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Alom F, Miyakawa M, Matsuyama H, Nagano H,
Tanahashi Y and Unno T: Possible antagonistic effects of the TRPC4
channel blocker ML204 on M2 and M3 muscarinic receptors in mouse
ileal and detrusor smooth muscles and atrial myocardium. J Vet Med
Sci. 80:1407–1415. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Schoeller C, Hoffmann S, Adolph S,
Regenthal R and Abraham G: Expression of muscarinic acetylcholine
receptors in turkey cardiac chambers. Res Vet Sci. 136:602–608.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pontes CNR, Scalzo S, Jesus ICG, Jesus EF,
Nunes ADC, Mendonça MM, Mendes EP, Colugnati DB, Xavier CH, Pedrino
GR, et al: Angiotensin-(1-7) attenuates the negative inotropic
response to acetylcholine in the heart. Peptides. 158:1708622022.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Riefolo F, Matera C, Garrido-Charles A,
Gomila AMJ, Sortino R, Agnetta L, Claro E, Masgrau R, Holzgrabe U,
Batlle M, et al: Optical control of cardiac function with a
photoswitchable muscarinic agonist. J Am Chem Soc. 141:7628–7636.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Woudstra J, Feenstra RGT, Vink CEM,
Marques KMJ, Boerhout CKM, de Jong EAM, de Waard GA, van de Hoef
TP, Chamuleau SAJ, Eringa EC, et al: Comparison of the diagnostic
yield of intracoronary acetylcholine infusion and acetylcholine
bolus injection protocols during invasive coronary function
testing. Am J Cardiol. 217:49–58. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ibrahim E, Diakonov I, Arunthavarajah D,
Swift T, Goodwin M, McIlvride S, Nikolova V, Williamson C and
Gorelik J: Bile acids and their respective conjugates elicit
different responses in neonatal cardiomyocytes: Role of Gi protein,
muscarinic receptors and TGR5. Sci Rep. 8:71102018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Levay MK, Krobert KA, Vogt A, Ahmad A,
Jungmann A, Neuber C, Pasch S, Hansen A, Müller OJ, Lutz S and
Wieland T: RGS3L allows for an M2 muscarinic
receptor-mediated RhoA-dependent inotropy in cardiomyocytes. Basic
Res Cardiol. 117:82022. View Article : Google Scholar
|
|
14
|
Winger G, Jutkiewicz EM and Woods JH:
Comparison of the muscarinic antagonist effects of scopolamine and
L-687,306. Behav Pharmacol. 31:359–367. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Butova X, Myachina T, Simonova R,
Kochurova A, Bozhko Y, Arkhipov M, Solovyova O, Kopylova G,
Shchepkin D and Khokhlova: Peculiarities of the acetylcholine
action on the contractile function of cardiomyocytes from the left
and right atria in rats. Cells. 11:38092022. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Baine S, Thomas J, Bonilla I, Ivanova M,
Belevych A, Li J, Veeraraghavan R, Radwanski PB, Carnes C and
Gyorke S: Muscarinic-dependent phosphorylation of the cardiac
ryanodine receptor by protein kinase G is mediated by PI3K-AKT-nNOS
signaling. J Biol Chem. 295:11720–11728. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ho HT, Belevych AE, Liu B, Bonilla IM,
Radwański PB, Kubasov IV, Valdivia HH, Schober K, Carnes CA and
Györke S: Muscarinic stimulation facilitates sarcoplasmic reticulum
Ca release by modulating ryanodine receptor 2 phosphorylation
through protein kinase G and Ca/calmodulin-dependent protein kinase
II. Hypertension. 68:1171–1178. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cassambai S, Mee CJ, Renshaw D and Hussain
A: Tiotropium bromide, a long acting muscarinic receptor antagonist
triggers intracellular calcium signalling in the heart. Toxicol
Appl Pharmacol. 384:1147782019. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Dolejší E, Janoušková A and Jakubík J:
Muscarinic receptors in cardioprotection and vascular tone
regulation. Physiological research. 2024. View Article : Google Scholar
|
|
20
|
Perera RK, Fischer TH, Wagner M, Dewenter
M, Vettel C, Bork NI, Maier LS, Conti M, Wess J, El-Armouche A, et
al: Atropine augments cardiac contractility by inhibiting
cAMP-specific phosphodiesterase type 4. Sci Rep. 7:152222017.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kim HY, Choi HR, Lee YJ, Cui HZ, Jin SN,
Cho KW, Kang DG and Lee HS: Accentuation of ursolic acid on
muscarinic receptor-induced ANP secretion in beating rabbit atria.
Life Sci. 94:145–150. 2014. View Article : Google Scholar
|
|
22
|
Kawada T, Sonobe T, Nishikawa T, Hayama Y,
Li M, Zheng C, Uemura K, Akiyama T, Pearson JT and Sugimachi M:
Contribution of afferent pathway to vagal nerve stimulation-induced
myocardial interstitial acetylcholine release in rats. Am J Physiol
Regul Integr Comp Physiol. 319:R517–R525. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bencze M, Boros A, Behuliak M, Vavrinova
A, Vaneckova I and Zicha J: Changes in cardiovascular autonomic
control induced by chronic inhibition of acetylcholinesterase
during pyridostigmine or donepezil treatment of spontaneously
hypertensive rats. Eur J Pharmacol. 971:1765262024. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Harada N, Ochi K, Yaosaka N, Teraoka H,
Hiraga T, Iwanaga T, Unno T, Komori S, Yamada M and Kitazawa T:
Immunohistochemical and functional studies for M3 muscarinic
receptors and cyclo-oxygenase-2 expressed in the mouse atrium.
Auton Autacoid Pharmacol. 32:41–52. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Stavrakis S, Kem DC, Patterson E, Lozano
P, Huang S, Szabo B, Cunningham MW, Lazzara R and Yu X: Opposing
cardiac effects of autoantibody activation of β-adrenergic and M2
muscarinic receptors in cardiac-related diseases. Int J Cardiol.
148:331–336. 2011. View Article : Google Scholar
|
|
26
|
Camara H, da Silva Junior ED, Garcia AG,
Jurkiewicz A and Rodrigues JQD: Cardiac arrest induced by
muscarinic or adenosine receptors agonists is reversed by DPCPX
through double mechanism. Eur J Pharmacol. 819:9–15. 2018.
View Article : Google Scholar
|
|
27
|
Sassu E, Tumlinson G, Stefanovska D,
Fernández MC, Iaconianni P, Madl J, Brennan TA, Koch M, Cameron BA,
Preissl S, et al: Age-related structural and functional changes of
the intracardiac nervous system. J Mol Cell Cardiol. 187:1–14.
2024. View Article : Google Scholar
|
|
28
|
Poller U, Nedelka G, Radke J, Pönicke K
and Brodde OE: Age-dependent changes in cardiac muscarinic receptor
function in healthy volunteers. J Am Coll Cardiol. 29:187–193.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wang S, Jiang Y, Chen J, Dai C, Liu D, Pan
W, Wang L, Fasae MB, Sun L, Wang L and Liu Y: Activation of M3
muscarinic acetylcholine receptors delayed cardiac aging by
inhibiting the caspase-1/IL-1beta signaling pathway. Cell Physiol
Biochem. 49:1208–1216. 2018. View Article : Google Scholar
|
|
30
|
Arnett DK, Blumenthal RS, Albert MA,
Buroker AB, Goldberger ZD, Hahn EJ, Himmelfarb CD, Khera A,
Lloyd-Jones D, McEvoy JW, et al: 2019 ACC/AHA guideline on the
primary prevention of cardiovascular disease: A report of the
american college of Cardiology/American heart association task
force on clinical practice guidelines. Circulation. 140:e596–e646.
2019.PubMed/NCBI
|
|
31
|
Tompkins JD, Buckley U, Salavatian S,
Shivkumar K and Ardell JL: Vagally-mediated heart block after
myocardial infarction associated with plasticity of epicardial
neurons controlling the atrioventricular node. Front Synaptic
Neurosci. 14:9604582022. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Singh S, Loke YK and Furberg CD: Inhaled
anticholinergics and risk of major adverse cardiovascular events in
patients with chronic obstructive pulmonary disease: A systematic
review and meta-analysis. JAMA. 300:1439–1450. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Mazzadi AN, Pineau J, Costes N, Le Bars D,
Bonnefoi F, Croisille P, Porcher R and Chevalier P: Muscarinic
receptor upregulation in patients with myocardial infarction: A new
paradigm. Circ Cardiovasc Imaging. 2:365–372. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Buchholz B, Kelly J, Munoz M, Bernatené
EA, Méndez Diodati N, González Maglio DH, Dominici FP and Gelpi RJ:
Vagal stimulation mimics preconditioning and postconditioning of
ischemic myocardium in mice by activating different protection
mechanisms. Am J Physiol Heart Circ Physiol. 314:H1289–H1297. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Zhang T, Zhang Y, Cui M, Jin L, Wang Y, Lv
F, Liu Y, Zheng W, Shang H, Zhang J, et al: CaMKII is a RIP3
substrate mediating ischemia- and oxidative stress-induced
myocardial necroptosis. Nat Med. 22:175–182. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Lauro FV, Maria LR, Tomas LG, Francisco
DC, Rolando GM, Marcela RN, Virginia MA, Alejandra GE and Yazmin
OA: Design and synthesis of two new steroid derivatives with
biological activity on heart failure via the M2-muscarinic receptor
activation. Steroids. 158:1086202020. View Article : Google Scholar
|
|
37
|
Rinaldi R, Colucci M, Torre I, Ausiello D,
Bonanni A, Basile M, Salzillo C, Sanna T, Liuzzo G, Leone AM, et
al: Predicting the response to acetylcholine in ischemia or
infarction with non-obstructive coronary arteries: The ABCD score.
Atherosclerosis. 391:1175032024. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Liao F, Zheng Y, Cai J, Fan J, Wang J,
Yang J, Cui Q, Xu G, Tang C, Geng B, et al: Catestatin attenuates
endoplasmic reticulum induced cell apoptosis by activation type 2
muscarinic acetylcholine receptor in cardiac ischemia/reperfusion.
Sci Rep. 5:165902015. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Kakinuma Y, Tsuda M, Okazaki K, Akiyama T,
Arikawa M, Noguchi T and Sato T: Heart-specific overexpression of
choline acetyltransferase gene protects murine heart against
ischemia through hypoxia-inducible factor-1α-related defense
mechanisms. J Am Heart Assoc. 2:e0048872013. View Article : Google Scholar
|
|
40
|
Xue RQ, Zhao M, Wu Q, Yang S, Cui YL, Yu
XJ, Liu J and Zang WJ: Regulation of mitochondrial cristae
remodelling by acetylcholine alleviates palmitate-induced
cardiomyocyte hypertrophy. Free Radic Biol Med. 145:103–117. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Palee S, Apaijai N, Shinlapawittayatorn K,
Chattipakorn SC and Chattipakorn N: Acetylcholine attenuates
hydrogen peroxide-induced intracellular calcium dyshomeostasis
through both muscarinic and nicotinic receptors in cardiomyocytes.
Cell Physiol Biochem. 39:341–349. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Lv YX, Zhong S, Tang H, Luo B, Chen SJ,
Chen L, Zheng F, Zhang L, Wang L, Li XY, et al: VEGF-A and VEGF-B
coordinate the arteriogenesis to repair the infarcted heart with
vagus nerve stimulation. Cell Physiol Biochem. 48:433–449. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Travieso A, Jeronimo-Baza A, Faria D,
Shabbir A, Mejia-Renteria H and Escaned J: Invasive evaluation of
coronary microvascular dysfunction. J Nucl Cardiol. 29:2474–2486.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Alves-Lopes R, Neves KB and Touyz RM:
Muscarinic receptor type-3 in hypertension and
cholinergic-adrenergic crosstalk: Genetic insights and potential
for new antihypertensive targets. Can J Cardiol. 35:555–557. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Khuanjing T, Palee S, Chattipakorn SC and
Chattipakorn N: The effects of acetylcholinesterase inhibitors on
the heart in acute myocardial infarction and heart failure: From
cells to patient reports. Acta Physiol (Oxf). 228:e133962020.
View Article : Google Scholar
|
|
46
|
Shahim B, Xu H, Haugaa K, Zetterberg H,
Jurga J, Religa D and Eriksdotter M: Cholinesterase inhibitors are
associated with reduced mortality in patients with Alzheimer's
disease and previous myocardial infarction. Eur Heart J Cardiovasc
Pharmacother. 10:128–136. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Pan Z, Guo Y, Qi H, Fan K, Wang S, Zhao H,
Fan Y, Xie J, Guo F, Hou Y, et al: M3 subtype of muscarinic
acetylcholine receptor promotes cardioprotection via the
suppression of miR-376b-5p. PLoS One. 7:e325712012. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Zhao J, Su Y, Zhang Y, Pan Z, Yang L, Chen
X, Liu Y, Lu Y, Du Z and Yang B: Activation of cardiac muscarinic
M3 receptors induces delayed cardioprotection by preserving
phosphorylated connexin43 and up-regulating cyclooxygenase-2
expression. Br J Pharmacol. 159:1217–1225. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Zhao L, Chen T, Hang P, Li W, Guo J, Pan
Y, Du J, Zheng Y and Du Z: Choline attenuates cardiac fibrosis by
inhibiting p38MAPK signaling possibly by acting on M3 muscarinic
acetylcholine receptor. Front Pharmacol. 10:13862019. View Article : Google Scholar :
|
|
50
|
Liu H, Hofmann J, Fish I, Schaake B, Eitel
K, Bartuschat A, Kaindl J, Rampp H, Banerjee A, Hübner H, et al:
Structure-guided development of selective M3 muscarinic
acetylcholine receptor antagonists. Proc Natl Acad Sci USA.
115:12046–12050. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Wang YP, Hang PZ, Sun LH, Zhang Y, Zhao
JL, Pan ZW, Ji HR, Wang LA, Bi H and Du ZM: M3 muscarinic
acetylcholine receptor is associated with beta-catenin in
ventricular myocytes during myocardial infarction in the rat. Clin
Exp Pharmacol Physiol. 36:995–1001. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Harvey KL, Hussain A and Maddock HL:
Ipratropium bromide-mediated myocardial injury in in vitro models
of myocardial Ischaemia/reperfusion. Toxicol Sci. 138:457–467.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Nuntaphum W, Pongkan W, Wongjaikam S,
Thummasorn S, Tanajak P, Khamseekaew J, Intachai K, Chattipakorn
SC, Chattipakorn N and Shinlapawittayatorn K: Vagus nerve
stimulation exerts cardioprotection against myocardial
ischemia/reperfusion injury predominantly through its efferent
vagal fibers. Basic Res Cardiol. 113:222018. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Pickard JMJ, Burke N, Davidson SM and
Yellon DM: Intrinsic cardiac ganglia and acetylcholine are
important in the mechanism of ischaemic preconditioning. Basic Res
Cardiol. 112:112017. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Khuanjing T, Palee S, Kerdphoo S,
Jaiwongkam T, Anomasiri A, Chattipakorn SC and Chattipakorn N:
Donepezil attenuated cardiac ischemia/reperfusion injury through
balancing mitochondrial dynamics, mitophagy, and autophagy. Transl
Res. 230:82–97. 2021. View Article : Google Scholar
|
|
56
|
Intachai K, Chattipakorn SC, Chattipakorn
N and Shinlapawittayatorn K: Acetylcholine exerts cytoprotection
against hypoxia/reoxygenation-induced apoptosis, autophagy and
mitochondrial impairment through both muscarinic and nicotinic
receptors. Apoptosis. 27:233–245. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Xu M, Bi X, He X, Yu X, Zhao M and Zang W:
Inhibition of the mitochondrial unfolded protein response by
acetylcholine alleviated hypoxia/reoxygenation-induced apoptosis of
endothelial cells. Cell Cycle. 15:1331–1343. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Xue RQ, Sun L, Yu XJ, Li DL and Zang WJ:
Vagal nerve stimulation improves mitochondrial dynamics via an M3
receptor/CaMKKbeta/AMPK pathway in isoproterenol-induced myocardial
ischaemia. J Cell Mol Med. 21:58–71. 2017. View Article : Google Scholar
|
|
59
|
Li W, Yu J, Yang Y, Wang J, Liu Y, Wang J,
Hu J, Yuan Y and Du Z: M3 subtype of muscarinic
acetylcholine receptor inhibits cardiac fibrosis via targeting
microRNA-29b/beta-site app cleaving enzyme 1 axis. Cardiovasc Diagn
Ther. 14:143–157. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Liu JJ, Huang N, Lu Y, Zhao M, Yu XJ, Yang
Y, Yang YH and Zang WJ: Improving vagal activity ameliorates
cardiac fibrosis induced by angiotensin II: in vivo and in vitro.
Sci Rep. 5:2015.
|
|
61
|
Gurses KM, Yalcin MU, Kocyigit D, Kesikli
SA, Canpolat U, Yorgun H, Sahiner ML, Kaya EB, Hazirolan T, Ozer N,
et al: M2-muscarinic acetylcholine receptor autoantibody levels
predict left atrial fibrosis severity in paroxysmal lone atrial
fibrillation patients undergoing cryoablation. Europace.
17:239–246. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Ma G, Wu X, Zeng L, Jin J, Liu X, Zhang J
and Zhang L: Association of autoantibodies against M2-muscarinic
acetylcholine receptor with atrial fibrosis in atrial fibrillation
patients. Cardiol Res Pract. 2019:82718712019. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Heijman J, Kirchner D, Kunze F, Chrétien
EM, Michel-Reher MB, Voigt N, Knaut M, Michel MC, Ravens U and
Dobrev D: Muscarinic type-1 receptors contribute to IK,ACh in human
atrial cardiomyocytes and are upregulated in patients with chronic
atrial fibrillation. Int J Cardiol. 255:61–68. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Garcia-Domingo M, Garcia-Pedraza JA,
Fernandez-Gonzalez JF, Lopez C, Martin ML and Moran A: Fluoxetine
treatment decreases cardiac vagal input and alters the serotonergic
modulation of the parasympathetic outflow in diabetic rats. Int J
Mol Sci. 23:57362022. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Jungen C, Scherschel K, Eickholt C, Kuklik
P, Klatt N, Bork N, Salzbrunn T, Alken F, Angendohr S, Klene C, et
al: Disruption of cardiac cholinergic neurons enhances
susceptibility to ventricular arrhythmias. Nat Commun. 8:141552017.
View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Gergs U, Wackerhagen S, Fuhrmann T,
Schafer I and Neumann J: Further investigations on the influence of
protein phosphatases on the signaling of muscarinic receptors in
the atria of mouse hearts. Naunyn Schmiedebergs Arch Pharmacol.
39:5731–5743. 2024. View Article : Google Scholar
|
|
67
|
Magyar T, Árpádffy-Lovas T, Pászti B, Tóth
N, Szlovák J, Gazdag P, Kohajda Z, Gyökeres A, Györe B, Gurabi Z,
et al: Muscarinic agonists inhibit the ATP-dependent potassium
current and suppress the ventricle-Purkinje action potential
dispersion. Can J Physiol Pharmacol. 99:247–253. 2021. View Article : Google Scholar
|
|
68
|
Voigt N, Friedrich A, Bock M, Wettwer E,
Christ T, Knaut M, Strasser RH, Ravens U and Dobrev D: Differential
phosphorylation-dependent regulation of constitutively active and
muscarinic receptor-activated IK,ACh channels in patients with
chronic atrial fibrillation. Cardiovasc Res. 74:426–437. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Petersen J, Castro L, Bengaard AKP, Pecha
S, Ismaili D, Schulz C, Sahni J, Steenpass A, Meier C,
Reichenspurner H, et al: Muscarinic receptor activation reduces
force and arrhythmias in human atria independent of IK,ACh. J
Cardiovasc Pharmacol. 79:678–686. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Couselo-Seijas M, Lopez-Canoa JN,
Agra-Bermejo RM, Díaz-Rodriguez E, Fernandez AL, Martinez-Cereijo
JM, Durán-Muñoz D, Bravo SB, Velo A, González-Melchor L, et al:
Cholinergic activity regulates the secretome of epicardial adipose
tissue: Association with atrial fibrillation. J Cell Physiol.
234:10512–10522. 2019. View Article : Google Scholar
|
|
71
|
Deng J, Guo Y, Zhang G, Zhang L, Kem D, Yu
X, Jiang H and Li H: M2 muscarinic autoantibodies and
thyroid hormone promote susceptibility to atrial fibrillation and
sinus tachycardia in an autoimmune rabbit model. Exp Physiol.
106:882–890. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Moss R, Sachse FB, Moreno-Galindo EG,
Navarro-Polanco RA, Tristani-Firouzi M and Seemann G: Modeling
effects of voltage dependent properties of the cardiac muscarinic
receptor on human sinus node function. PLoS Comput Biol.
14:e10064382018. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Liu Y, Sun L, Pan Z, Bai Y, Wang N, Zhao
J, Xu C, Li Z, Li B, Du Z, et al: Overexpression of M3
muscarinic receptor is a novel strategy for preventing sudden
cardiac death in transgenic mice. Mol Med. 17:1179–1187. 2011.
View Article : Google Scholar
|
|
74
|
Olivas A, Gardner RT, Wang L, Ripplinger
CM, Woodward WR and Habecker BA: Myocardial infarction causes
transient cholinergic transdifferentiation of cardiac sympathetic
nerves via gp130. J Neurosci. 36:479–488. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Prado MB Jr and Adiao KJ:
Acetylcholinesterase inhibitors in myasthenic crisis: A systematic
review of observational studies. Neurocrit Care. 35:528–544. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Bober SL, Ciriello J and Jones DL: Atrial
arrhythmias and autonomic dysfunction in rats exposed to chronic
intermittent hypoxia. Am J Physiol Heart Circ Physiol.
314:H1160–H1168. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Cavalcante GL, Brognara F, Oliveira LVC,
Lataro RM, Durand MT, de Oliveira AP, da Nóbrega ACL, Salgado HC
and Sabino JPJ: Benefits of pharmacological and electrical
cholinergic stimulation in hypertension and heart failure. Acta
Physiol (Oxf). 232:e136632021. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Baine S, Bonilla I, Belevych A, Stepanov
A, Dorn LE, Terentyeva R, Terentyev D, Accornero F, Carnes CA and
Gyorke S: Pyridostigmine improves cardiac function and rhythmicity
through RyR2 stabilization and inhibition of STIM1-mediated calcium
entry in heart failure. J Cell Mol Med. 25:4637–4648. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Fernandez SF and Canty JM Jr: Adrenergic
and cholinergic plasticity in heart failure. Circ Res.
116:1639–1642. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Teixeira VP, Miranda K, Scalzo S,
Rocha-Resende C, Silva MM, Tezini GCSV, Melo MB, Souza-Neto FP,
Silva KSC, Jesus ICG, et al: Increased cholinergic activity under
conditions of low estrogen leads to adverse cardiac remodeling. Am
J Physiol Cell Physiol. 320:C602–C612. 2021. View Article : Google Scholar
|
|
81
|
Ma G, Chen L, Yue Y, Liu X, Wang Y, Shi C,
Song F, Shi W, Lo Y and Zhang L: Impact of autoantibodies against
the M2-muscarinic acetylcholine receptor on clinical outcomes in
peripartum cardiomyopathy patients with standard treatment. BMC
Cardiovasc Disord. 21:6192021. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Li M, Zheng C, Kawada T, Inagaki M, Uemura
K and Sugimachi M: Intracerebroventricular infusion of donepezil
prevents cardiac remodeling and improves the prognosis of chronic
heart failure rats. J Physiol Sci. 70:112020. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Williams AM, Shave RE, Coulson JM, White
H, Rosser-Stanford B and Eves ND: Influence of vagal control on
sex-related differences in left ventricular mechanics and
hemodynamics. Am J Physiol Heart Circ Physiol. 315:H687–H698. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Schultheiss HP, Fairweather D, Caforio
ALP, Escher F, Hershberger RE, Lipshultz SE, Liu PP, Matsumori A,
Mazzanti A, McMurray J and Priori SG: Dilated cardiomyopathy. Nat
Rev Dis Primers. 5:322019. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Chen X, Bai Y, Sun H, Su Z, Guo J, Sun C
and Du Z: Overexpression of m3 muscarinic receptor suppressed
adverse electrical remodeling in hypertrophic myocardium via
increasing repolarizing K+ currents. Cell Physiol Biochem.
43:915–925. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Wang S, Han HM, Pan ZW, Hang PZ, Sun LH,
Jiang YN, Song HX, Du ZM and Liu Y: Choline inhibits angiotensin
II-induced cardiac hypertrophy by intracellular calcium signal and
p38 MAPK pathway. Naunyn Schmiedebergs Arch Pharmacol. 385:823–831.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Ma M, Chen W, Hua Y, Jia H, Song Y and
Wang Y: Aerobic exercise ameliorates cardiac hypertrophy by
regulating mitochondrial quality control and endoplasmic reticulum
stress through M2 AChR. J Cell Physiol. 236:6581–6596.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Matsui S, Fu ML, Hayase M, Katsuda S,
Yamaguchi N, Teraoka K, Kurihara T and Takekoshi N: Active
immunization of combined beta1-adrenoceptor and M2-muscarinic
receptor peptides induces cardiac hypertrophy in rabbits. J Card
Fail. 5:246–254. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
da Silva Gonçalves Bós D, Van Der Bruggen
CEE, Kurakula K, Sun XQ, Casali KR, Casali AG, Rol N, Szulcek R,
Dos Remedios C, Guignabert C, et al: Contribution of impaired
parasympathetic activity to right ventricular dysfunction and
pulmonary vascular remodeling in pulmonary arterial hypertension.
Circulation. 137:910–924. 2018. View Article : Google Scholar
|
|
90
|
Minassa VS, Aitken AV, Hott SC, de Sousa
GJ, Batista TJ, Gonçalves RCR, Coitinho JB, Paton JFR, Beijamini V,
Bissoli NS and Sampaio KN: Intermittent exposure to chlorpyrifos
results in cardiac hypertrophy and oxidative stress in rats.
Toxicology. 482:1533572022. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Duan X, Liu R, Luo XL, Gao XJ, Hu FH, Guo
C, Wang J, Hu XY, Chun YS, Yuan JS, et al: The relationship between
β1-adrenergic and M2-muscarinic receptor autoantibodies and
hypertrophic cardiomyopathy. Exp Physiol. 105:522–530. 2020.
View Article : Google Scholar
|
|
92
|
Ribeiro KC, Campelo RP, Rodrigues DDRF,
Mattos EC, Brandão IT, da Silva CL, Bouskela E, Martinez CG and
Kurtenbach E: Immunization with plasmids encoding M2 acetylcholine
muscarinic receptor epitopes impairs cardiac function in mice and
induces autophagy in the myocardium. Autoimmunity. 51:245–257.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Bezerra OC, Franca CM, Rocha JA, Neves GA,
Souza PRM, Teixeira Gomes M, Malfitano C, Loleiro TCA, Dourado PM,
Llesuy S, et al: Cholinergic stimulation improves oxidative stress
and inflammation in experimental myocardial infarction. Sci Rep.
7:136872017. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Barboza CA, Fukushima AR, Carrozzi N,
Machi JF, Dourado PMM, Mostarda CT, Irigoyen MC, Nathanson L,
Morris M, Caperuto EC and Rodrigues B: Cholinergic stimulation by
pyridostigmine bromide before myocardial infarction prevent cardiac
and autonomic dysfunction. Sci Rep. 9:24812019. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Halder N and Lal G: Cholinergic system and
its therapeutic importance in inflammation and autoimmunity. Front
Immunol. 12:6603422021. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Cox MA, Duncan GS, Lin GHY, Steinberg BE,
Yu LX, Brenner D, Buckler LN, Elia AJ, Wakeham AC, Nieman B, et al:
Choline acetyltransferase-expressing T cells are required to
control chronic viral infection. Science. 363:639–644. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Reardon C, Duncan GS, Brüstle A, Brenner
D, Tusche MW, Olofsson PS, Rosas-Ballina M, Tracey KJ and Mak TW:
Lymphocyte-derived ACh regulates local innate but not adaptive
immunity. Proc Natl Acad Sci USA. 110:1410–1415. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
De-Pu Z, Li-Sha G, Guang-Yi C, Xiaohong G,
Chao X, Cheng Z, Wen-Wu Z, Jia L, Jia-Feng L, Maoping C and
Yue-Chun L: The cholinergic anti-inflammatory pathway ameliorates
acute viral myocarditis in mice by regulating CD4+ T cell
differentiation. Virulence. 9:1364–1376. 2018. View Article : Google Scholar :
|
|
99
|
Wang Y, Liu Y, Li XY, Yao LY, Mbadhi M,
Chen SJ, Lv YX, Bao X, Chen L, Chen SY, et al: Vagus nerve
stimulation-induced stromal cell-derived factor-l alpha
participates in angiogenesis and repair of infarcted hearts. ESC
Heart Fail. 10:3311–3329. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Albano GD, Bonanno A, Moscato M, Anzalone
G, Di Sano C, Riccobono L, Wenzel SE and Profita M: Crosstalk
between mAChRM3 and beta2AR, via acetylcholine PI3/PKC/PBEP1/Raf-1
MEK1/2/ERK1/2 pathway activation, in human bronchial epithelial
cells after Long-term cigarette smoke exposure. Life Sci.
192:99–109. 2018. View Article : Google Scholar
|
|
101
|
Wu Q, Zhao M, Li D, He X and Zang W:
Cholinergic drugs reduce metabolic inflammation and diabetic
myocardial injury by regulating the gut bacterial component
lipopolysaccharide-induced ERK/Egr-1 pathway. FASEB J.
37:e229172023. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Jiang W, Li D, Han R, Zhang C, Jin WN,
Wood K, Liu Q, Shi FD and Hao J: Acetylcholine-producing NK cells
attenuate CNS inflammation via modulation of infiltrating
monocytes/macrophages. Proc Natl Acad Sci USA. 114:E6202–E6211.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Rocha-Resende C, da Silva AM, Prado MAM
and Guatimosim S: Protective and anti-inflammatory effects of
acetylcholine in the heart. Am J Physiol Cell Physiol.
320:C155–C161. 2021. View Article : Google Scholar
|
|
104
|
Plaschke K, Do TQM, Uhle F, Brenner T,
Weigand MA and Kopitz J: Ablation of the right cardiac vagus nerve
reduces acetylcholine content without changing the inflammatory
response during endotoxemia. Int J Mol Sci. 19:4422018. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Tarnawski L, Shavva VS, Kort EJ, Zhuge Z,
Nilsson I, Gallina AL, Martínez-Enguita D, Heller Sahlgren B,
Weiland M, Caravaca AS, et al: Cholinergic regulation of vascular
endothelial function by human ChAT+ T cells. Proc Natl
Acad Sci USA. 120:e22124761202023. View Article : Google Scholar
|
|
106
|
Suissa S, Dell'Aniello S and Ernst P:
Long-acting bronchodilator initiation in COPD and the risk of
adverse cardiopulmonary events: A population-based comparative
safety study. Chest. 151:60–67. 2017. View Article : Google Scholar
|
|
107
|
Rogliani P, Calzetta L, Matera MG, di
Daniele N, Girolami A, Cazzola M and Ora J: Inhaled therapies and
cardiovascular risk in patients with chronic obstructive pulmonary
disease. Expert Opin Pharmacother. 20:737–750. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Shin J and Lee JH: Effects of tiotropium
on the risk of coronary heart disease in patients with COPD: A
nationwide cohort study. Sci Rep. 12:166742022. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Parkin L, Williams S, Sharples K, Barson
D, Horsburgh S, Jackson R, Wu B and Dummer J: Dual versus single
long-acting bronchodilator use could raise acute coronary syndrome
risk by over 50%: A Population-based nested Case-control study. J
Intern Med. 290:1028–1038. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Arana A, Margulis AV, McQuay LJ, Ziemiecki
R, Bartsch JL, Rothman KJ, Franks B, D'Silva M, Appenteng K,
Varas-Lorenzo C and Perez-Gutthann S: Variation in cardiovascular
risk related to individual antimuscarinic drugs used to treat
overactive bladder: A UK cohort study. Pharmacotherapy. 38:628–637.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Guo F, Wang Y, Wang J, Liu Z, Lai Y, Zhou
Z, Liu Z, Zhou Y, Xu X, Li Z, et al: Choline potects the heart from
doxorubicin-induced cardiotoxicity through vagal activation and
Nrf2/HO-1 pathway. Oxid Med Cell Longev. 2022:47409312022.
View Article : Google Scholar
|
|
112
|
Khuanjing T, Ongnok B, Maneechote C,
Siri-Angkul N, Prathumsap N, Arinno A, Chunchai T, Arunsak B,
Chattipakorn SC and Chattipakorn N: Acetylcholinesterase inhibitor
ameliorates doxorubicin-induced cardiotoxicity through reducing
RIP1-mediated necroptosis. Pharmacol Res. 173:1058822021.
View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Khalaf HA and El-Mansy AAE: The possible
alleviating effect of saffron on chlorpyrifos experimentally
induced cardiotoxicity: Histological, immunohistochemical and
biochemical study. Acta Histochem. 121:472–483. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
114
|
Prathumsap N, Ongnok B, Khuanjing T,
Arinno A, Maneechote C, Apaijai N, Chunchai T, Arunsak B, Kerdphoo
S, Janjek S, et al: Vagus nerve stimulation exerts cardioprotection
against doxorubicin-induced cardiotoxicity through inhibition of
programmed cell death pathways. Cell Mol Life Sci. 80:212022.
View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Wu Q, Zhao M, He X, Xue R, Li D, Yu X,
Wang S and Zang W: Acetylcholine reduces palmitate-induced
cardiomyocyte apoptosis by promoting lipid droplet lipolysis and
perilipin 5-mediated lipid droplet-mitochondria interaction. Cell
Cycle. 20:1890–1906. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
116
|
Pedzinska-Betiuk A, Weresa J, Schlicker E,
Harasim-Symbor E, Toczek M, Kasacka I, Gajo B and Malinowska B:
Chronic cannabidiol treatment reduces the carbachol-induced
coronary constriction and left ventricular cardiomyocyte width of
the isolated hypertensive rat heart. Toxicol Appl Pharmacol.
411:1153682021. View Article : Google Scholar
|
|
117
|
Pickett MA, Dush MK and Nascone-Yoder NM:
Acetylcholinesterase plays a non-neuronal, non-esterase role in
organogenesis. Development. 144:2764–2770. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Wessler I and Kirkpatrick CJ:
Acetylcholine beyond neurons: The non-neuronal cholinergic system
in humans. Br J Pharmacol. 154:1558–1571. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Huang D, Zhang L, Liu Y, Wang J, Zhang J,
Baines KJ, Liu G, Hsu AC, Wang F, Chen Z, et al: Activated
non-neuronal cholinergic system correlates with non-type 2
inflammation and exacerbations in severe asthma. Ann Allergy Asthma
Immunol. 133:e64–e72.e4. 2024. View Article : Google Scholar
|
|
120
|
Braczko F, Fischl SR, Reinders J, Lieder
HR and Kleinbongard P: Activation of the nonneuronal cholinergic
cardiac system by hypoxic preconditioning protects isolated adult
cardiomyocytes from hypoxia/reoxygenation injury. Am J Physiol
HeartCirc Physiol. 327:H70–H79. 2024. View Article : Google Scholar
|
|
121
|
Chotirat S, Suriyo T, Hokland M, Hokland
P, Satayavivad J and Auewarakul CU: Cholinergic activation enhances
retinoic acid-induced differentiation in the human NB-4 acute
promyelocytic leukemia cell line. Blood Cells Mol Dis. 59:77–84.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Oikawa S, Kai Y, Mano A, Sugama S,
Mizoguchi N, Tsuda M, Muramoto K and Kakinuma Y: Potentiating a
non-neuronal cardiac cholinergic system reinforces the functional
integrity of the blood brain barrier associated with systemic
anti-inflammatory responses. Brain Behav Immun. 81:122–137. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
123
|
Rocha-Resende C, Weinheimer C, Bajpai G,
Adamo L, Matkovich SJ, Schilling J, Barger PM, Lavine KJ and Mann
DL: Immunomodulatory role of non-neuronal cholinergic signaling in
myocardial injury. JCI Insight. 5:e1289612019. View Article : Google Scholar : PubMed/NCBI
|
|
124
|
Kakinuma Y, Akiyama T and Sato T:
Cholinoceptive and cholinergic properties of cardiomyocytes
involving an amplification mechanism for vagal efferent effects in
sparsely innervated ventricular myocardium. FEBS J. 276:5111–5125.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Oikawa S, Kai Y, Mano A, Ohata H, Nemoto T
and Kakinuma Y: Various regulatory modes for circadian rhythmicity
and sexual dimorphism in the non-neuronal cardiac cholinergic
system. J Cardiovasc Transl Res. 10:411–422. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Oikawa S, Kai Y, Mano A, Nakamura S and
Kakinuma Y: A novel nitric oxide donor,
S-Nitroso-NPivaloyl-D-Penicillamine, activates a non-neuronal
cardiac cholinergic system to synthesize acetylcholine and augments
cardiac function. Cell Physiol Biochem. 52:922–934. 2019.
View Article : Google Scholar : PubMed/NCBI
|