Introduction
The musculoskeletal system functions as an
integrated unit in which skeletal muscle and bone exhibit
bidirectional communication beyond their traditional biomechanical
roles. The interdependence between the skeletal muscle and bone is
particularly evident in response to mechanical loading, where
physical activity simultaneously influences muscle contractility
and skeletal architecture (1).
The concept of the 'muscle-bone unit' has evolved substantially
over the past decade, shifting from a purely mechanical paradigm
toward the recognition of complex biochemical crosstalk mediated by
secreted factors (2). Skeletal
muscle, which is now understood to function as an endocrine organ,
produces and releases a diverse array of cytokines, peptides and
extracellular vesicles, which are collectively termed myokines
(3). These factors act in
autocrine, paracrine and endocrine manners to coordinate interorgan
communication, with bone representing one of the most
physiologically relevant targets (4).
The clinical significance of muscle-bone crosstalk
has been highlighted by the parallel aging-related epidemics of
sarcopenia and osteoporosis, conditions that frequently coexist and
share overlapping pathogenic mechanisms (5). Observational studies have shown
that reduced in muscle mass and strength, strongly correlate with
bone loss and fracture risk, suggesting the involvement of common
regulatory pathways (6).
However, the molecular underpinnings of this association have
remained incompletely understood until recent advances in myokine
biology provided mechanistic insights. Gries et al (7) comprehensively summarized the
spectrum of muscle-derived factors that influence bone metabolism,
highlighting the functional heterogeneity within this signaling
network. Complementing this, Kaji (2) provided an updated framework for
understanding how exercise-induced myokines orchestrate cellular
responses in bone, emphasizing the importance of context-dependent
signaling.
The identification of irisin as an
exercise-responsive myokine with osteogenic properties has
catalyzed considerable research interest. Subsequent studies have
demonstrated that irisin promotes osteoblast differentiation
through multiple mechanisms, including activation of bone
morphogenetic protein (BMP)/SMAD signaling and stabilization of
β-catenin (8,9). Conversely, myostatin, a member of
the transforming growth factor-beta (TGF-β) superfamily, exerts
catabolic effects on bone by inhibiting osteoblast differentiation
and promoting mesenchymal stem cell adipogenesis (10,11). This functional dichotomy
illustrates that the net effect of exercise on bone homeostasis
depends on the balance between anabolic and catabolic myokine
signals. Recent systematic reviews have consolidated evidence that
myokines such as IL-6, IL-15 and osteocrin contribute to this
regulatory network, with effects that are often exercise
modality-dependent and influenced by factors including intensity,
duration and training status (12).
Emerging evidence has further expanded the
conceptual framework by incorporating immune and metabolic
dimensions into the muscle-bone crosstalk paradigm. Skeletal
muscle-derived IL-33 has been shown to regulate bone metabolism via
CD8+ T cell-secreted chemokine ligand 5 (CCL5),
establishing a direct immunological axis linking muscle activity to
skeletal homeostasis (13).
Additionally, chronic low-grade inflammation characteristic of
aging, termed inflammaging, disrupts normal myokine profiles and
contributes to the pathogenesis of both sarcopenia and osteoporosis
(14). The recognition that
myokines function as immunomodulators within the bone niche has
prompted re-evaluation of exercise interventions as strategies to
counteract inflammation-driven bone loss.
The present review aims to synthesize current
knowledge regarding the molecular signaling mechanisms through
which exercise-induced myokines regulate bone homeostasis, with
particular focus on the key signaling pathways, the emerging
paradigm of muscle-bone-immune interactions, and the translational
implications for therapeutic development in bone disorders.
The present narrative review was conducted to
synthesize current evidence on myokine-mediated exercise regulation
of bone homeostasis. A comprehensive literature search was
performed in the PubMed database (https://pubmed.ncbi.nlm.nih.gov/) for articles
published from January 2000 to May 2026. The search terms included
combinations of the following keywords: 'myokines', 'exercise',
'bone homeostasis', 'osteoblast', 'osteoclast', 'osteocyte',
'irisin', 'myostatin', 'interleukin-6', 'signaling pathway',
'Wnt/β-catenin', 'MAPK', 'PI3K/AKT', 'NF-κB', 'TGF-β/BMP',
'muscle-bone crosstalk', 'muscle-bone-immune axis', 'osteoporosis',
'sarcopenia', 'therapeutic targets', 'biomarkers', 'Multiomics',
'single-cell', 'spatial transcriptomics', 'organ-on-chip', and
'machine learning'. Only English-language articles were included.
Both original research and review articles were considered. Studies
involving human subjects, animal models, in vitro
experiments, and methodological innovations were included if they
addressed the molecular mechanisms, signaling pathways, or
therapeutic implications of myokines in bone homeostasis. Reference
lists of retrieved articles were manually screened to identify
additional relevant studies.
Exercise-induced myokine secretion: Sources,
regulation and bone targeting
Skeletal muscle functions as an endocrine organ,
secreting a diverse array of cytokines, peptides and extracellular
vesicles that are collectively termed myokines and that mediate
interorgan communication (15).
Exercise serves as a powerful physiological stimulus that
profoundly alters the myokine secretome in a manner dependent on
contraction mode, intensity and duration (1). These exercise-induced factors act
locally within muscle and distally on bone, where they orchestrate
cellular responses critical for maintaining bone homeostasis
(16). Understanding the
regulatory mechanisms governing myokine secretion and their
specific targeting of bone cells is fundamental to leveraging these
molecules for therapeutic benefit in bone disorders (Fig. 1).
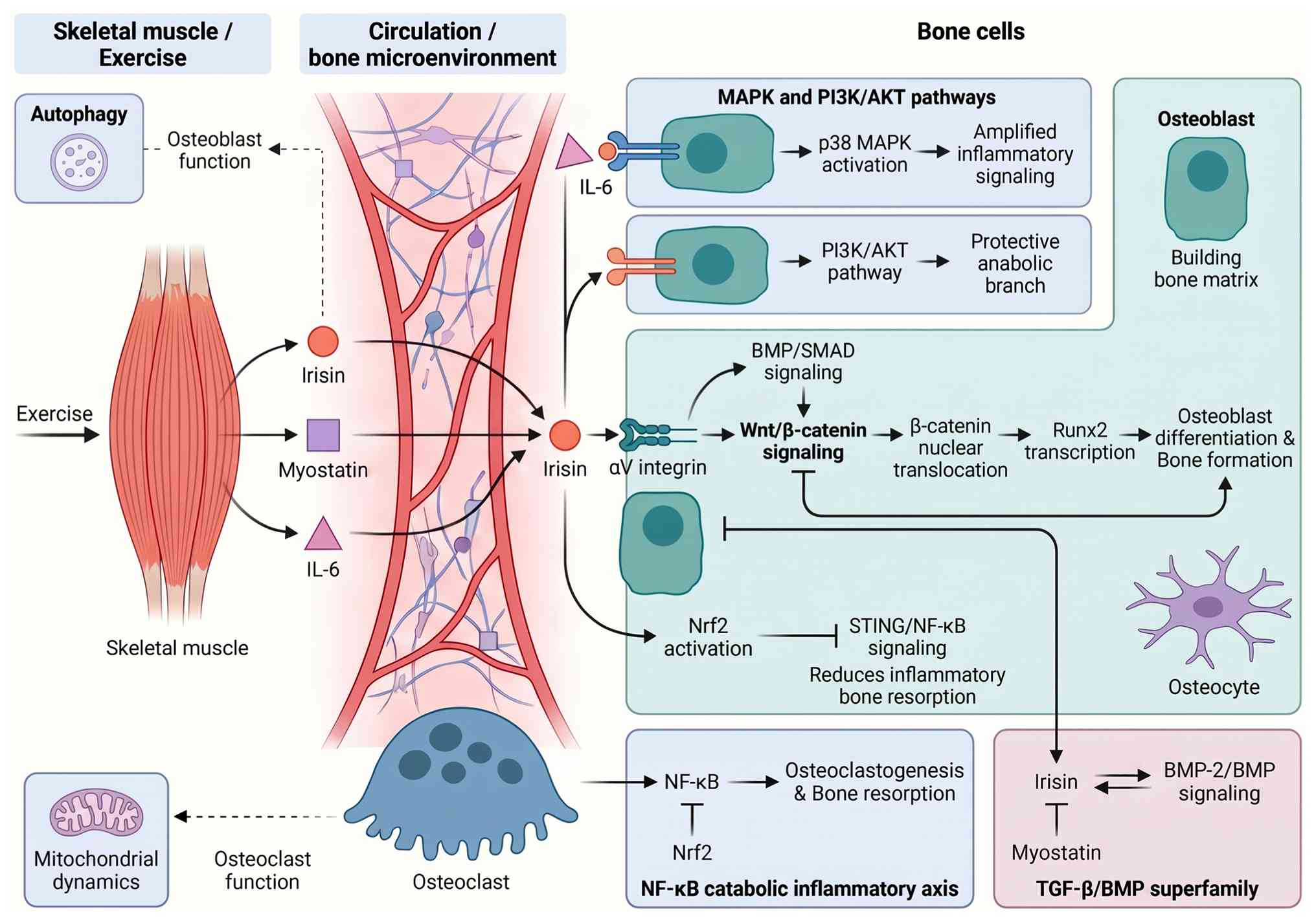
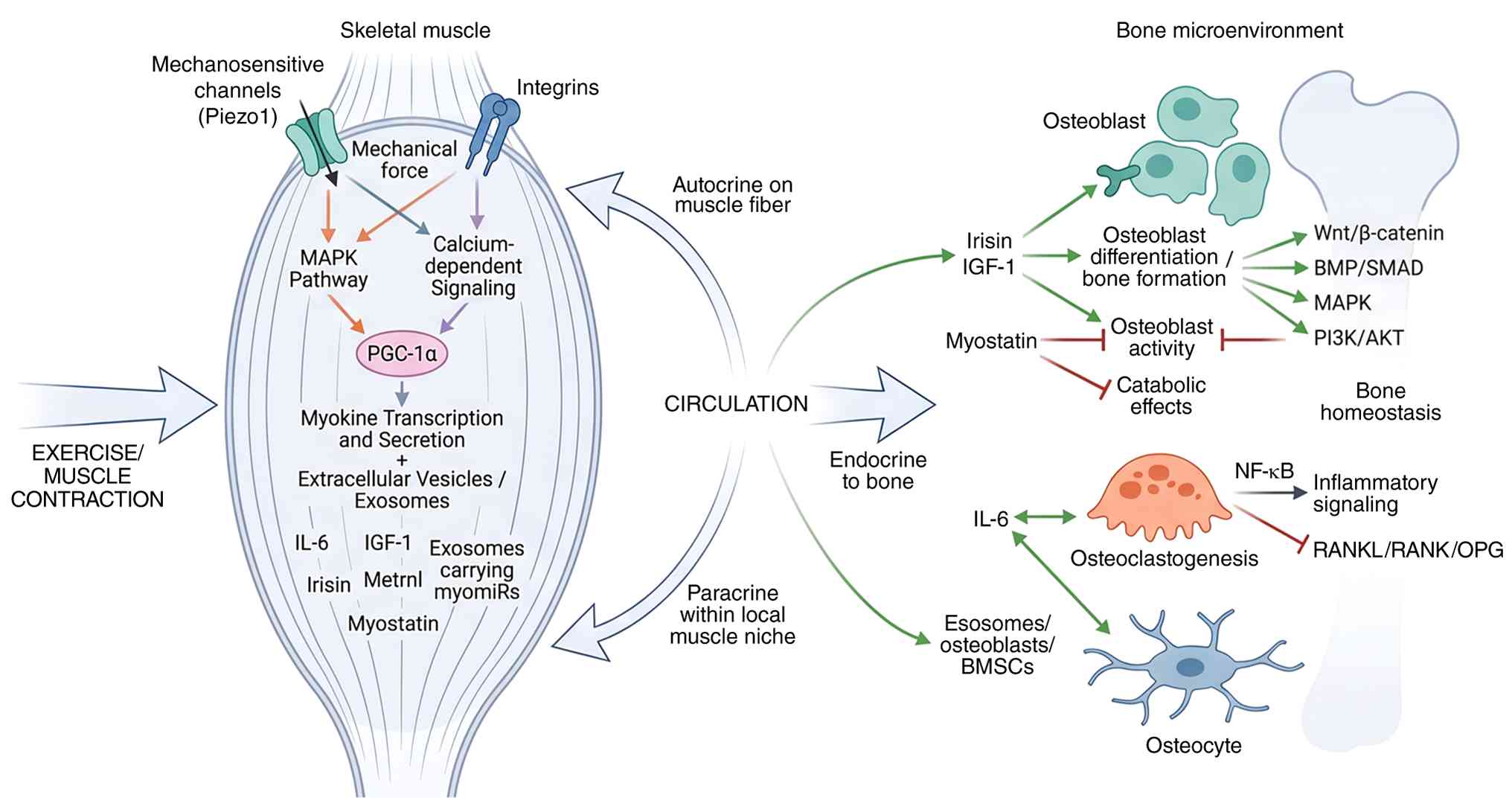 | Figure 1Schematic illustration of
exercise-induced myokine secretion and its multi-level actions on
bone homeostasis. Mechanical forces during exercise activate PGC-1α
and mechanotransduction pathways in skeletal muscle, promoting
secretion of myokines (for example, irisin, IL-6 and myostatin) and
release of extracellular vesicles. These factors act in endocrine,
paracrine, and autocrine manners to regulate osteoblasts,
osteoclasts, and osteocytes, thereby controlling bone homeostasis.
RANK, receptor activator of nuclear factor-κB; RANKL, RANK ligand;
OPG, osteoprotegerin; PGC-1α, peroxisome proliferator-activated
receptor gamma coactivator 1-alpha; BMP, bone morphogenetic
protein; IGF-1, insulin-like growth factor-1; IL-6,
interleukin-6. |
Defining myokines and exercise-dependent
regulation
Myokines are defined as cytokines or peptides
synthesized and released by skeletal muscle fibers, a concept that
has expanded the understanding of muscle as a secretory organ
(17). Their expression is
dynamically regulated by contractile activity, with both acute and
chronic exercise eliciting distinct secretory profiles (18). The myokine repertoire includes
classical cytokines such as interleukin-6 (IL-6), growth factors
such as insulin-like growth factor-1 (IGF-1), and novel peptides
such as irisin and meteorin-like protein (Metrnl) (1,19). A systematic review by Jaśkiewicz
et al (16) emphasized
that the characterization of myokines based on exercise context is
essential, as their effects on bone metabolism can be
context-dependent and even opposing. For instance, while irisin is
consistently anabolic for bone, myostatin exerts catabolic effects,
demonstrating the functional heterogeneity within this family
(12).
Mechano-transduction in skeletal muscle:
Contraction-coupled myokine release
The mechanical forces generated during muscle
contraction are transduced into biochemical signals that initiate
myokine synthesis and secretion (20). This mechano-transduction process,
mediated by mechanosensitive channels (for example, Piezo1) and
integrins, triggers the activation of multiple signaling cascades,
including the mitogen-activated protein kinase (MAPK) and
calcium-dependent pathways, which converge on transcriptional
regulators such as peroxisome proliferator-activated receptor gamma
coactivator 1-alpha (PGC-1α) (21). PGC-1α is a master regulator of
the exercise-responsive myokine program, driving the expression of
irisin and other secreted factors (22). Studies utilizing in vitro
biomechanical stimulation of muscle constructs have demonstrated
that cyclic stretch alone is sufficient to modulate myokine
secretion, confirming that mechanical strain is a direct and potent
regulator (20). Furthermore,
the release of myokines is not solely transcriptionally regulated;
post-translational processing and secretion via extracellular
vesicles also play critical roles (23,24). For example, exosomes derived from
exercised muscle carry myo-miRs and proteins that can directly
influence osteoblast function (23,24).
Endocrine, paracrine and autocrine
actions on bone cells
Upon secretion, myokines exert their effects through
three primary modes of action: Autocrine signaling on the secreting
myofiber, paracrine signaling on neighboring cells within the
muscle niche, and endocrine signaling on distant organs such as
bone (4,18). For bone homeostasis, the
endocrine actions of myokines have been the most extensively
studied. Gomarasca et al (17) provided a comprehensive overview
of how myokines such as irisin, IL-6 and myostatin enter the
circulation and interact with specific receptors on osteoblasts,
osteoclasts and osteocytes. However, paracrine signaling within the
local muscle-bone microenvironment is also critical, particularly
in regions of muscle-bone attachment (7,25). The concept of a functional
'muscle-bone unit' underscores the importance of both systemic and
local crosstalk (26).
Importantly, recent evidence suggests that autocrine myokine loops
within muscle may influence muscle health and, consequently, the
secretory capacity of the muscle, indirectly impacting bone
(2).
Influence of exercise type, intensity and
duration on myokine profiles
The myokine response is highly sensitive to the
exercise modality (direct human evidence). Resistance training,
characterized by high mechanical load, preferentially stimulates
the secretion of factors like IGF-1 and myostatin, whereas
endurance exercise, involving repetitive, lower-load contractions,
is a robust inducer of irisin, IL-6 and Metrnl (27,28). The dose-response relationship
between exercise intensity and myokine secretion is non-linear. For
instance, acute high-intensity interval training has been shown to
elicit a distinct myokine profile, with a pronounced increase in
IL-6 and a concomitant, albeit transient, suppression of bone
formation markers (29,30). Conversely, moderate-intensity
continuous exercise may produce a more sustained elevation of
osteogenic myokines such as irisin (31,32). Duration also plays a key role; a
single marathon race can induce a significant but temporary rise in
sclerostin (SOST) and other myokines, reflecting an acute stress
response (31). By contrast,
chronic exercise training leads to adaptations in the basal myokine
setpoint, often resulting in a favorable baseline profile for bone
health (33,34). Agostinete et al (28) demonstrated that in adolescents,
the bone benefits of resistance training were mediated through
distinct myokine pathways compared with impact sports, emphasizing
that the qualitative nature of the exercise stimulus dictates the
myokine signature.
Sex, age and circadian modulation of
exercise-induced myokine secretion
Biological variability, including sex, age and
circadian rhythms, significantly modulates the myokine response to
exercise. Sex hormones directly influence myokine expression;
estrogen deficiency, as observed in postmenopausal women, alters
the secretion of IL-6, myostatin, and other factors that regulate
osteoclastogenesis (6,35,36). Norton et al (35) showed that estrogen regulates
myokines that enhance osteoclast differentiation, providing a
mechanistic link between menopause and increased bone resorption.
Aging is associated with a state of chronic low-grade inflammation
and anabolic resistance, which blunts the myokine response to
exercise (37). This age-related
dysregulation contributes to the pathogenesis of sarcopenia and
osteoporosis (37). Furthermore,
circadian rhythms regulate the expression and secretion of
myokines, with some, such as irisin, exhibiting diurnal variation
(21). The timing of exercise
can therefore influence the magnitude and efficacy of the myokine
response, a concept with implications for optimizing exercise
prescription (21). Koltun et
al (38) observed that prior
training status also modifies the myokine and bone turnover
response to acute exercise, suggesting an interaction between
fitness level and these biological factors. Collectively, these
modulators must be considered when interpreting myokine data and
designing personalized exercise interventions. Critically, the
relative contribution of endocrine vs. paracrine myokine signaling
to bone homeostasis remains unclear, and the lack of standardized
exercise protocols limits cross-study comparisons.
Throughout the present review, human studies are
prioritized for translational relevance; animal and in vitro
studies are indicated as such. Established mechanisms refer to
findings replicated across multiple laboratories, whereas emerging
hypotheses are based on limited data.
Molecular mechanisms of myokine action on
bone cells
The cellular response of bone to exercise-induced
myokines is mediated through a complex network of signaling
pathways that converge on the three principal bone cell types:
Osteoblasts, osteoclasts and osteocytes. Myokines exert pleiotropic
effects on these cells, either promoting bone formation or
suppressing resorption, with the net outcome depending on the
specific myokine, its concentration, and the cellular context
(Fig. 2).
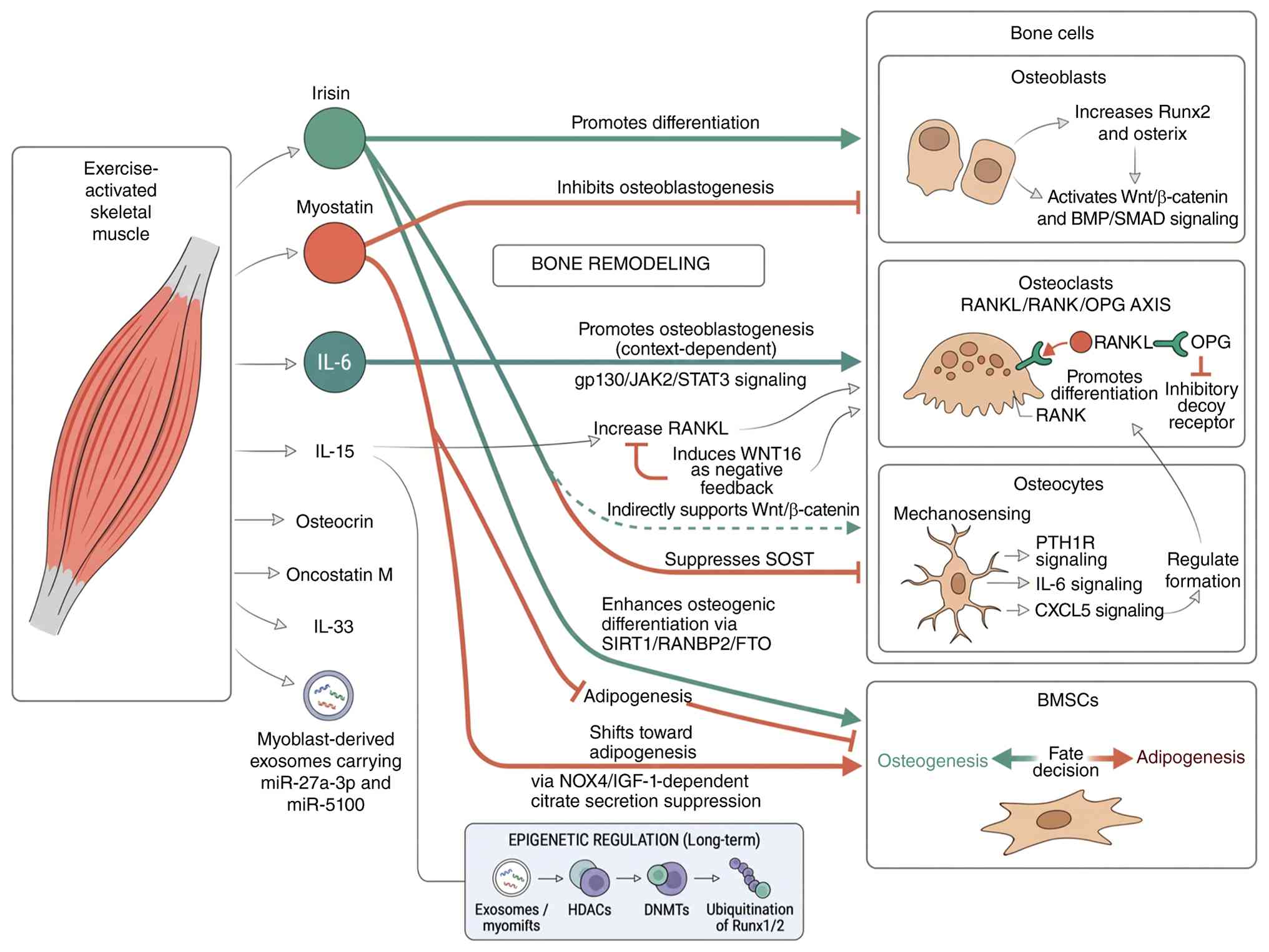 | Figure 2Myokine signaling networks regulating
bone cell fate. Green modules indicate anabolic myokines and
pro-osteogenic pathways promoting bone formation; red modules
represent catabolic myokines and pro-resorptive pathways driving
bone loss. These myokines regulate the activity of major bone cells
to balance bone remodeling. HDACs, histone deacetylases; BMSCs,
bone marrow mesenchymal stem cells; RANK, receptor activator of
nuclear factor-κB; RANKL, RANK ligand; OPG, osteoprotegerin; PTH1R,
parathyroid hormone 1 receptor; DNMTs, DNA methyltransferases; BMP,
bone morphogenetic protein; miR, microRNA; SOST, sclerostin; CXCL5,
C-X-C motif chemokine ligand 5; SIRT1, sirtuin1; NOX4, nicotinamide
adenine dinucleotide phosphate oxidase 4; IGF-1, insulin-like
growth factor-1; GP130, glycoprotein 130; IL, interleukin. |
Osteoblast differentiation and activity:
Irisin, myostatin and osteocrin
Myokines critically influence osteoblastogenesis by
modulating key transcriptional programs. Irisin, a cleaved product
of fibronectin type III domain-containing protein 5, is a
well-characterized osteogenic myokine. Studies have demonstrated
that irisin enhances the osteogenic differentiation of various
mesenchymal stem cells' (MSCs) populations, including dental
bud-derived MSCs and pre-osteoblastic MC3T3-E1 cells, by
upregulating the expression of master osteogenic transcription
factors such as runt-related transcription factor 2 (Runx2) and
osterix (39,40). The downstream signaling pathways
mediating these effects, including Wnt/β-catenin and BMP/SMAD, are
discussed in detail in Section 4. By contrast, myostatin acts as a
potent negative regulator of bone formation by suppressing
IGF-1-dependent citrate secretion via nicotinamide adenine
dinucleotide phosphate oxidase 4 (10,41). The balance between anabolic and
catabolic myokines dictates the net osteogenic outcome in response
to exercise (42). Irisin
enhances osteogenic differentiation (established, multiple in
vitro/animal studies). However, the effects of these myokines
are context-dependent and can vary with species, model system,
dose, disease state, exercise modality, sex, age, and assay
method.
Osteoclastogenesis and bone resorption:
IL-6, IL-15 and the receptor activator of nuclear factor-κB ligand
(RANKL)/receptor activator of nuclear factor-κB
(RANK)/osteoprotegerin (OPG) axis
Myokines exert profound control over osteoclast
differentiation and activity, primarily through modulation of the
RANKL/RANK/OPG axis. IL-6, a myokine robustly induced by exercise,
has a dual and context-dependent role in osteoclastogenesis. IL-6
can promote the proliferation of osteoclast precursors and
stimulate the production of inflammatory mediators, thereby
enhancing osteoclast formation (42). In line with this, IL-6 deficiency
has been shown to enhance intramembranous ossification following
stress fracture, suggesting that its suppression can be beneficial
for bone repair (43). However,
the effect of IL-6 is nuanced, as signaling through the
glycoprotein 130 receptor can also lead to the induction of
osteoclastogenesis via the Janus kinase 2 (JAK2)/signal transducer
and activator of transcription 3 (STAT3) pathway, a mechanism that
can be exacerbated by conditions such as hyperglycemia (44,45). The critical balance is further
regulated by myokines such as oncostatin M, which can stimulate
RANKL expression, but also induce the negative feedback regulator
WNT16 to limit excessive osteoclast formation (46,47). Collectively, these myokines
regulate bone resorption by finely tuning the RANKL/OPG ratio and
downstream signaling pathways.
Osteocyte mechano-sensing and
intercellular communication
Osteocytes, the most abundant bone cells, function
as the primary mechano-sensors in bone and are also key targets of
myokine signaling. Exercise-induced mechanical loading is
transduced by osteocytes, which then release signaling molecules
that coordinate bone remodeling. Previous evidence suggests that
myokines can modulate this process. For instance, mechanical strain
in osteocytes has been shown to influence the secretion of
parathyroid hormone 1 receptor, which in turn regulates osteoclast
formation through modulation of IL-6 and C-X-C motif chemokine
ligand 5 (48). Furthermore, the
myokine irisin has been shown to influence osteocyte function
indirectly by affecting the inflammatory milieu. A key mechanism
involves the regulation of SOST, an osteocyte-derived inhibitor of
bone formation. In pathological conditions such as particle-induced
osteolysis, suppression of the SOST gene activates osteocyte
Wnt/β-catenin signaling, preventing bone resorption (49). This underscores the critical role
of osteocytes as intermediaries that integrate mechanical and
humoral signals, including myokines, to orchestrate local bone
remodeling.
Crosstalk with bone marrow mesenchymal
stem cells (BMSCs)
BMSCs are the common precursors for osteoblasts and
adipocytes, and their lineage commitment is highly sensitive to
myokine signaling. The secretome of exercised muscle, including
myokines and myoblast-derived exosomes, directly influences BMSC
fate. Irisin has been demonstrated to enhance the osteogenic
differentiation of BMSCs while simultaneously inhibiting their
adipogenic differentiation, a dual action that favors bone
formation (50,51). This effect is mediated through
the sirtuin 1/RANBP2/FTO signaling axis, which governs the
stability of key osteogenic transcripts (51). By contrast, myostatin has been
shown to inhibit the osteogenic potential of BMSCs, promoting a
shift towards adipogenesis, which contributes to the age-related
decline in bone mass (10).
Moreover, exosomes derived from myoblasts carry myomiRs such as
miR-27a-3p and miR-5100, which can be taken up by pre-osteoblasts
and BMSCs to promote osteogenic differentiation, highlighting a
non-canonical mode of myokine delivery (52). Thus, myokines exert a critical
regulatory role in determining the differentiation trajectory of
BMSCs within the bone marrow niche.
Epigenetic and post-translational
regulation by exercise-responsive myokines
The sustained effects of exercise on bone health are
increasingly attributed to myokine-induced epigenetic
modifications. These changes alter chromatin structure and gene
expression patterns without altering the DNA sequence itself,
providing a mechanism for long-term adaptation. Exercise training
has been shown to induce changes in the expression of myomiRs and
osteomiRs, which are small non-coding RNAs that regulate gene
expression post-transcriptionally (53). For example, myoblast-derived
exosomes enriched with specific microRNAs can modulate osteogenic
gene expression in recipient bone cells (52). Furthermore, myokine signaling can
influence the activity of histone deacetylases and DNA
methyltransferases, thereby regulating the accessibility of
promoters for key transcription factors involved in osteoblast and
osteoclast differentiation (54). Post-translational modifications,
such as ubiquitination, also play a role; irisin facilitates the
ubiquitination and activation of Runx1/2, linking myokine signaling
directly to the activation of osteogenic transcription factors
(50). Mechanistically, irisin
induces non-proteolytic K63-linked ubiquitination of RUNX2, which
enhances its transcriptional activity by promoting nuclear
retention, facilitating coactivator recruitment, and stabilizing
the protein without targeting it for proteasomal degradation. This
is distinct from K48-linked ubiquitination, which typically marks
proteins for degradation. The K63-linked ubiquitination of RUNX2
thereby sustains osteogenic gene expression and promotes osteoblast
differentiation (50). These
epigenetic and post-translational layers of regulation explain how
the transient secretion of myokines during exercise can translate
into durable changes in bone cell function and overall bone
homeostasis.
Key myokine signaling pathways in bone
homeostasis
This section focuses specifically on signaling
pathways activated by exercise-induced myokines (irisin, myostatin
and IL-6) in bone cells. Studies of general pathway biology without
direct myokine involvement are cited as background only when
explicitly noted. The skeletal response to exercise-derived
myokines is governed by a complex intracellular signaling network
that translates secreted cues into specific cellular outcomes in
bone. These pathways do not operate in isolation; rather, they
constitute an integrated signaling circuitry that determines
whether the net effect favors bone formation or resorption. The
Wnt/β-catenin cascade serves as a central anabolic axis, while the
MAPK, phosphatidylinositol-3-kinase (PI3K)/protein kinase B (AKT)
and nuclear factor kappa B (NF-κB) pathways mediate both osteogenic
and catabolic responses depending on the specific myokine and
cellular context. Additionally, the TGF-β/BMP superfamily and
emerging regulators of autophagy and mitochondrial dynamics add
further layers of complexity (Fig.
3). A comprehensive understanding of these molecular mechanisms
is essential for identifying therapeutic targets and optimizing
exercise interventions for bone disorders.
Wnt/β-catenin cascade: A central anabolic
hub
The canonical Wnt/β-catenin signaling pathway is a
critical mediator of the osteogenic effects of several
exercise-responsive myokines. Irisin, the most extensively studied
myokine in this context, has been shown to activate this pathway to
promote osteoblast differentiation. Mechanistically, recombinant
irisin prevents the reduction in osteoblast differentiation induced
by simulated microgravity through increasing β-catenin expression,
thereby preserving osteogenic capacity (55). These findings are primarily
derived from in vitro and rodent studies; human data remain
limited. Further supporting this, irisin promotes osteogenesis by
activating the BMP/SMAD signaling pathway via αV integrin, a
cascade that converges with and enhances Wnt signaling to regulate
bone mass in mice (8). This dual
activation of BMP and Wnt pathways underscores the integrated
nature of myokine signaling. Conversely, myostatin, a negative
regulator of muscle mass, antagonizes these anabolic pathways.
Genetic and pharmacologic inhibition of myostatin in a murine model
of osteogenesis imperfecta led to improved bone properties, an
effect partly attributed to disinhibition of Wnt signaling
(56). Collectively, these
findings position the Wnt/β-catenin cascade as a key node where
anabolic and catabolic myokine signals converge to dictate
osteoblast function.
MAPK and PI3K/AKT pathways: Dual
regulators of bone cell fate
The MAPK and PI3K/AKT pathways are ubiquitously
involved in transducing myokine signals, yet their effects on bone
are highly context-dependent. The MAPK family, including p38,
extracellular signal-regulated kinase (ERK) and c-Jun N-terminal
kinase (JNK), mediates both pro-osteogenic and pro-resorptive
actions. For instance, IL-6, a myokine robustly induced by
exercise, stimulates its synthesis in osteoblast-like cells via p38
MAPK regulation, establishing a positive feedback loop that can
amplify inflammatory signals (57,58). Furthermore, recent evidence
indicates that exercise-derived irisin prevents bone loss by
activating nuclear factor erythroid 2-related factor 2 (Nrf2) and
inhibiting the stimulator of interferon genes (STING)/NF-κB
signaling axis, highlighting crosstalk between these pathways
(59). The dual nature of MAPK
signaling is further illustrated by studies on osteoclastogenesis.
Thus, while MAPK activation can promote inflammation-driven bone
loss, it is also a necessary component of the mechano-transduction
machinery that maintains bone health, necessitating a nuanced
interpretation of its role.
NF-κB and inflammatory signaling in bone
remodeling
The NF-κB pathway is a master regulator of
inflammatory responses and a central driver of osteoclastogenesis.
Numerous myokines and exercise-associated factors exert their
effects on bone by modulating this pathway. However, direct
evidence linking these compounds to exercise-induced myokine
signaling is lacking. The relevance of this pathway in the context
of exercise is highlighted by recent work showing that
exercise-derived irisin prevents bone loss through Nrf2 activation
and subsequent inhibition of STING/NF-κB signaling, providing a
direct mechanistic link between physical activity, a myokine, and
suppression of inflammatory bone resorption (59). Moreover, the chronic low-grade
inflammation associated with aging and sarcopenia is intimately
linked to NF-κB dysregulation. The inflammation-energy metabolism
axis has been identified as a central driver of
sarcopenia-osteoporosis, emphasizing that NF-κB acts as a key
mediator of this pathological crosstalk (60). These studies collectively affirm
that the therapeutic potential of myokines lies partly in their
capacity to fine-tune NF-κB activity, shifting the balance from
catabolic inflammation toward anabolic bone formation.
TGF-β/BMP superfamily: From myostatin to
BMPs
Members of the TGF-β superfamily, including BMPs and
myostatin, are pivotal in the muscle-bone crosstalk. While BMPs are
well-established inducers of osteogenesis, myostatin acts as a
potent inhibitor. A complex interplay exists whereby IL-6
potentiates BMP-2-induced osteogenesis and adipogenesis via two
different BMPR1A-mediated pathways, indicating that inflammatory
myokines can modulate the osteogenic efficacy of BMPs (61). In the context of aging, BMP-4
rescues the bone regenerative potential of old muscle-derived stem
cells via regulation of cell cycle inhibitors, suggesting that
enhancing BMP signaling could counteract age-related declines in
bone repair (62). Conversely,
the inhibitory effects of myostatin on bone are well-documented.
Fibroblast growth factor-2 targets SOST in bone and myostatin in
skeletal muscle to mitigate the deleterious effects of
glucocorticoids on musculoskeletal degradation, highlighting a dual
therapeutic strategy (63). More
recently, the effect of recombinant irisin on BMP-2-induced
osteogenesis has been investigated, revealing that irisin can
modulate this process, further illustrating the interconnectedness
of these signaling hierarchies (64). Mechanistically, irisin enhances
BMP-2-induced osteogenesis by promoting the nuclear translocation
of phosphorylated SMAD1/5/8 and increasing the transcriptional
activity of Runx2, thereby synergizing with BMP-2 to drive
osteoblast differentiation. This modulatory effect is dependent on
the activation of the MAPK pathway, as pharmacological inhibition
of MAPK abrogates the irisin-mediated enhancement of BMP-2
signaling. The therapeutic implications are significant, as
modulating the balance between osteogenic BMP signaling and
catabolic myostatin signaling offers a promising avenue for
treating bone disorders. The balance between osteogenic BMP
signaling and catabolic myostatin signaling is critical for bone
homeostasis. As aforementioned, myostatin inhibits osteoblast
differentiation (10,41), whereas irisin promotes
osteogenesis through BMP/SMAD and Wnt/β-catenin pathways (55). Exercise and mechanical loading
favor the anabolic balance by upregulating osteogenic myokines such
as irisin while modulating the expression of catabolic factors
(22). Therapeutic strategies
aimed at shifting this balance toward BMP signaling hold promise
for treating bone disorders. Irisin modulates BMP-2-induced
osteogenesis (emerging, requires in vivo validation).
Autophagy and mitochondrial dynamics in
myokine-targeted bone cells
Emerging evidence underscores the importance of
cellular quality control mechanisms, particularly autophagy and
mitochondrial dynamics, in mediating the effects of myokines on
bone homeostasis. These processes are critical for the survival,
differentiation and function of osteoblasts and osteoclasts.
Conversely, the preservation of mitochondrial health appears
crucial for anabolic responses. Mitochondrial oxidative stress or
decreased autophagy in osteoblast lineage cells is not sufficient
to mimic the deleterious effects of aging on bone
mechano-responsiveness, suggesting that these processes interact
with other age-related factors (65). The role of myokines in regulating
these pathways is an emerging frontier. For instance, the
protective effects of irisin against bone loss have been linked to
Nrf2 activation, a master regulator of antioxidant responses that
also influences autophagy (59).
Furthermore, Piezo1 activation suppresses bone marrow adipogenesis
to prevent osteoporosis by inhibiting a mechano-inflammatory
autocrine loop, a process intimately linked to cellular metabolism
and mechano-transduction (66).
These studies collectively point toward a paradigm where myokines
not only activate classic signaling cascades but also orchestrate
broader cellular homeostatic programs to sustain bone health.
Collectively, the synthesis of these signaling
pathways presented in the present review highlights that the net
effect of exercise on bone homeostasis depends on the balance
between anabolic (for example, Wnt/β-catenin and PI3K/AKT) and
catabolic (for example, NF-κB and myostatin/TGF-β) signals. This
integrated view extends beyond previous pathway-specific reviews by
emphasizing crosstalk and context-dependency. A major limitation is
that most studies use supraphysiological recombinant myokine
concentrations that may not reflect the complex, pulsatile nature
of exercise-induced secretion in vivo.
Muscle-bone-immune interactions: Emerging
roles in bone disorders
The traditional view of the muscle-bone unit as a
purely biomechanical entity has been substantially revised by the
recognition that these tissues communicate through a sophisticated
network of biochemical signals, with the immune system serving as a
critical intermediary. The muscle-bone-immune axis is defined as a
reciprocal signaling network wherein exercise-induced myokines
directly modulate immune cells within the bone microenvironment,
and these immune cells in turn regulate osteoblasts and
osteoclasts; conversely, bone-derived osteokines (for example,
osteocalcin) and immune cell-derived factors can also influence
skeletal muscle function, establishing true bidirectionality
(22). The present review
focuses primarily on the myokine-mediated direction from muscle to
bone via immune intermediaries, which represents the
best-characterized arm of this axis. The core components include:
i) Skeletal muscle-derived myokines (for example, IL-33, irisin,
IL-6 and myostatin) as initiating signals; ii) immune cell
populations (CD8+ T cells and macrophages) and their
secreted factors (for example, CCL5); and iii) bone cells as final
effectors. In the primary direction addressed in the present
review, signal flow proceeds from muscle (myokine secretion during
exercise) to immune cells (activation or suppression) to bone
(altered formation or resorption). Feedback signals from bone and
immune cells to muscle, while less extensively characterized, are
acknowledged to complete the bidirectional loop. This tripartite
interaction is particularly relevant in the pathogenesis of common
bone disorders, where chronic inflammation, aging and hormonal
shifts converge to disrupt homeostasis (Table I). A conceptual framework for
these complex interactions is provided in Fig. 4, illustrating how myokines
derived from exercising muscle can modulate macrophage
polarization, T-cell subsets, and inflammatory signaling pathways
to ultimately influence bone remodeling, fracture healing, and the
progression of conditions such as osteoporosis and
osteoarthritis.
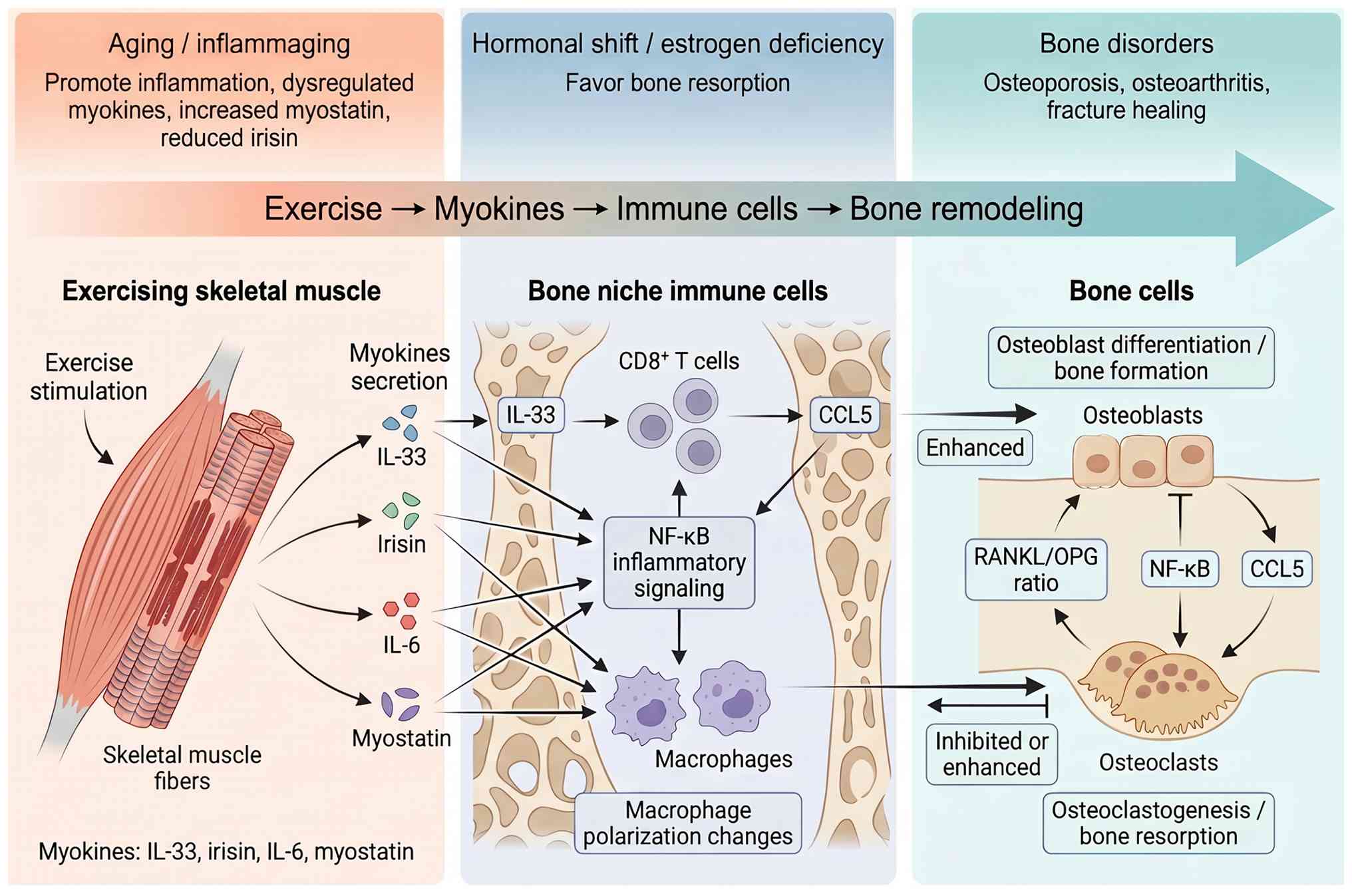 | Figure 4Muscle-bone-immune axis in bone
homeostasis. Exercise-induced myokines modulate immune cells
(macrophages, CD8+ T cells) in the bone niche,
regulating osteoblast and osteoclast activity via key pathways
(NF-κB, CCL5 and RANKL/OPG). Aging, inflammation, and sex hormones
influence this crosstalk, affecting bone remodeling. RANKL,
receptor activator of nuclear factor-κB ligand; CCL5, chemokine
ligand 5; OPG, osteoprotegerin; NF-κB, nuclear factor kappa B; IL,
interleukin. |
 | Table IKey studies on muscle-bone-immune
interactions in bone homeostasis. |
Table I
Key studies on muscle-bone-immune
interactions in bone homeostasis.
| Authors, year | Myokine | Immune
cell/pathway | Study type | Key finding | (Refs.) |
|---|
| Liu et al,
2025 | IL-33 | CD8+ T
cells/CCL5 | Rodent study | IL-33 mediates
muscle-bone crosstalk via CD8+ T cells | (13) |
| Colaianni et
al, 2021 | Irisin | Senescent marker
p21 | Human
correlation | Irisin correlates
with BMD in older adults | (67) |
| Chang et al,
2022 | IL-6 | Osteoclast
precursors | In
vitro | IL-6 promotes
osteoclast precursor proliferation | (42) |
| Arrieta et
al, 2019 | Myostatin | Systemic
inflammation | Human study | Higher myostatin in
active, non-frail older adults | (68) |
| Ghayomzadeh et
al, 2022 | Exercise
training | Systemic
inflammation | Human
intervention | Combined training
improves bone mass, reduces inflammation | (73) |
| Chen et al,
2025 | Irisin | Systemic
inflammation | Human
intervention | Alternating
aerobic/resistance exercise increases irisin and BMD | (71) |
| Testa et al,
2022 | Exercise
training | STAT3 pathway | Rodent study | Resistance training
reduces STAT3 activation and muscle atrophy | (74) |
| Hu et al,
2026 | Irisin | STING/NF-κB
pathway | Rodent study | Exercise-derived
irisin prevents bone loss via Nrf2/STING/NF-κB | (59) |
| Oranger et
al, 2023 | Irisin |
Inflammatory/angiogenic factors | Rodent study | Irisin modulates
fracture healing factors | (76) |
Myokines as immunomodulators in the bone
niche
Myokines function as pivotal immunomodulators,
directing the activity of immune cells that reside within or
infiltrate the bone niche. A landmark study by Liu et al
(13) demonstrated that skeletal
muscle-derived IL-33 mediates muscle-to-bone crosstalk by
regulating CD8+ T cells, which in turn secrete CCL5 to
influence bone metabolism (13).
This finding establishes a direct immunological axis connecting
muscle activity to bone homeostasis. Complementing this, Colaianni
et al (67) showed that
irisin positively correlates with bone mineral density in older
adults, an effect partially mediated by its capacity to reduce the
senescent marker p21 in osteoblasts, thereby counteracting
age-related cellular dysfunction. The immunomodulatory capacity of
the muscle secretome is further exemplified by studies showing that
biomechanical stimulation of muscle constructs directly influences
the paracrine signaling to bone cells, with the release of exosomes
and soluble factors that can alter the inflammatory milieu
(20). IL-33 mediates
muscle-to-bone crosstalk via CD8+ T cells (single study,
independent replication pending).
Chronic low-grade inflammation and
myokine dysregulation in aging
Aging is characterized by a state of chronic
low-grade inflammation, termed 'inflammaging', which is intimately
linked to the pathogenesis of sarcopenia and osteoporosis. This
systemic inflammatory environment profoundly disrupts the myokine
profile. Evans et al (37) highlighted that sarcopenia, a core
component of age-related musculoskeletal decline, is underpinned by
anabolic resistance and exacerbated by chronic inflammation. This
is supported by studies showing that serum myostatin levels, a
catabolic myokine, are higher in more physically active and
non-frail older adults, suggesting a complex compensatory mechanism
that can be further modulated by exercise (68). The inflammatory-energy metabolism
axis has been identified as a central driver of the
sarcopenia-osteoporosis syndrome, with NF-κB acting as a key
mediator of this pathological crosstalk (69). In line with this, Buchmann et
al (70) demonstrated that
the metabolic syndrome exacerbates the association between low
muscle mass and elevated inflammatory markers in older adults,
indicating a synergistic relationship between metabolic
dysfunction, inflammation and myokine dysregulation. Consequently,
the age-related decline in anabolic myokines such as irisin and the
elevation of catabolic factors including myostatin create a
permissive environment for bone loss. To overcome age-related bone
loss caused by declining irisin and rising myostatin, several
strategies have been proposed. Exercise training, particularly
resistance and combined aerobic-resistance modalities, remains the
most effective approach to restore irisin levels and suppress
myostatin expression in older adults (71). Pharmacologically, recombinant
irisin administration has shown bone-protective effects in
preclinical models (72), while
myostatin inhibition via genetic or pharmacologic approaches
improves bone properties (56).
A combination of exercise and targeted myokine-based therapies may
offer synergistic benefits for counteracting age-related
musculoskeletal decline.
Exercise-mediated myokine control in
osteoporosis and sarcopenia
Exercise is a potent non-pharmacological strategy to
counteract the myokine dysregulation observed in osteoporosis and
sarcopenia, leveraging the immunomodulatory properties of myokines.
A study by Ghayomzadeh et al (73) demonstrated that combined
resistance and aerobic training for six months improved bone mass
and physical function in HIV-infected individuals, an effect linked
to a reduction in systemic inflammation. Similarly, in
postmenopausal women, alternating aerobic with resistance exercise
was shown to improve bone mineral density and increase circulating
irisin levels (71). The
mechanisms underlying these benefits are multifaceted. For
instance, resistance training has been shown to reduce the
activation of STAT3 and attenuate muscle atrophy in tumor-bearing
mice, highlighting its capacity to counteract inflammation-driven
muscle wasting (74). In the
context of osteoporosis, exercise-derived irisin has been found to
prevent bone loss by activating the Nrf2 antioxidant pathway and
inhibiting the STING/NF-κB inflammatory axis (59). Furthermore, the gut-bone axis has
been identified as a mediator of exercise modality-dependent
suppression of inflammatory osteoclastogenesis in
ovariectomy-induced bone loss, suggesting that the systemic
anti-inflammatory effects of exercise are transduced through
multiple pathways, including the modulation of the gut microbiota
(75). These findings
collectively underscore that exercise, through its influence on
myokines, serves as a powerful regulator of the chronic
inflammation that underpins age-related musculoskeletal
disorders.
Myokine involvement in post-traumatic
osteoarthritis and fracture healing
The muscle-bone-immune axis plays a critical role in
the response to acute injury, such as fracture and the pathogenesis
of post-traumatic osteoarthritis (PTOA). Following a fracture, the
local inflammatory response is essential for healing, but its
dysregulation can lead to complications. Oranger et al
(76) demonstrated that irisin
modulates inflammatory, angiogenic and osteogenic factors during
fracture healing, suggesting a beneficial role for this myokine in
the repair process. This is supported by studies in rat models
showing that irisin promotes fracture healing by enhancing both
osteogenesis and angiogenesis (77). In the context of PTOA,
exercise-induced modulation of irisin has been shown to have
protective effects on the muscle-bone unit, potentially by
mitigating the inflammatory response that drives cartilage
degradation and subchondral bone changes (78). Açan et al (79) further corroborated the role of
irisin in fracture healing, finding it comparable to hyaluronic
acid and platelet-rich plasma in a rat model. Conversely, elevated
levels of pro-inflammatory cytokines can be detrimental. Blockade
of IL-6 signaling at the fracture site has been revealed to
accelerate bone healing, suggesting that fine-tuning this
inflammatory pathway, potentially through myokine-mediated
regulation, is critical for optimal repair (80). These studies highlight that
myokines are not merely passive markers but active participants in
the immune-regulated processes of tissue repair and regeneration
following musculoskeletal injury.
Sex hormone interactions with myokine
signaling in bone homeostasis
Sex hormones, particularly estrogen, exert profound
effects on both the immune system and the musculoskeletal system,
with their decline in aging contributing to the pathogenesis of
osteoporosis and sarcopenia. Estrogen deficiency alters the
secretion of myokines that enhance osteoclast differentiation and
activity, establishing a direct mechanistic link between menopause
and increased bone resorption (81). The interaction between sex
hormones and myokine signaling is complex and bidirectional. For
instance, Norton et al (35) showed that estrogen regulates
myokines that specifically enhance osteoclast differentiation,
providing a mechanistic basis for the accelerated bone loss
observed in postmenopausal women (81). In a study of oligo-amenorrheic
athletes, the route of estrogen administration was found to impact
bone turnover markers, suggesting that hormonal milieu directly
modulates the skeletal response to factors influenced by exercise
(82). Furthermore, sex
differences in myokine expression are evident in pathological
states. In older adults, serum myostatin and IGF-1 have been
identified as sex-specific biomarkers of frailty and low muscle
mass, indicating that the relationship between myokines and
musculoskeletal health is modulated by sex (83). Recent work by Weaver et al
(84) demonstrated that global
deletion of Girk3 increases bone mass in female but not male mice,
further emphasizing the sexually dimorphic nature of factors
regulating bone metabolism. These findings underscore the necessity
of considering sex as a biological variable when investigating
myokine-based therapies and designing exercise interventions for
bone disorders.
Translational implications: Myokines as
therapeutic targets and biomarkers
The convergence of preclinical and clinical evidence
positions myokines at the forefront of translational strategies for
bone disorders. These endogenous exercise-responsive factors offer
dual therapeutic potential: as targets for biopharmaceutical
development and as circulating biomarkers for disease
stratification and monitoring (Table II). However, translating
myokine-based concepts into clinical practice requires overcoming
substantial hurdles related to protein stability, bioavailability,
immunogenicity and the inherent heterogeneity of both myokine
signatures and patient populations.
| Table IITranslational studies on
myokine-based therapeutic strategies, biomarker applications and
personalized exercise interventions in bone disorders. |
Table II
Translational studies on
myokine-based therapeutic strategies, biomarker applications and
personalized exercise interventions in bone disorders.
| Authors, year | Intervention | Study type | Evidence level | Key finding | (Refs.) |
|---|
| Chen et al,
2020 | Recombinant
irisin | Preclinical
(rodent) | Preclinical | Irisin prevents
osteoblast differentiation deficits under microgravity | (55) |
| Colucci et
al, 2021 | Recombinant
irisin | Preclinical
(rodent) | Preclinical | Systemic irisin
accelerates fracture healing | (72) |
| Cheng et al,
2024 | Concurrent aerobic
+ resistance training | Meta-analysis | Moderate | Distinct effects on
circulating irisin levels | (90) |
| Adilakshmi et
al, 2024 | Exercise
training | Clinical (healthy
adults) | Preliminary | Exercise
modality-dependent alterations in myokines | (92) |
| Bettariga et
al, 2024 | Exercise
training | Meta-analysis | Moderate | Exercise mode
effects on myokine expression | (93) |
| Shen et al,
2024 | Circulating
irisin | Meta-analysis | Moderate | Lower irisin
associated with osteoporosis in women | (95) |
| Song et al,
2021 | Circulating
irisin | Meta-analysis | Moderate | Lower irisin in
type 2 diabetes | (96) |
| Alexopoulos et
al, 2021 | Myostatin +
CPK/albumin | Clinical
(cirrhosis) | Preliminary | Myostatin
combinations improve sarcopenia discrimination | (98) |
| Kim et al,
2025 | Extracellular
vesicle markers | Clinical (older
adults) | Preliminary | EV markers linked
to low muscle mass | (104) |
| Zhang et al,
2025 | Circulating
irisin | Meta-analysis | Moderate | Lower irisin in
sarcopenia | (106) |
Myokine-based therapeutic strategies
Recombinant myokines and their mimetics represent a
direct approach to recapitulating the osteogenic benefits of
exercise in patients unable to engage in physical activity.
Preclinical studies have demonstrated the efficacy of recombinant
irisin in preventing osteoblast differentiation deficits under
simulated microgravity through β-catenin stabilization (55), and systemic administration of
irisin accelerated fracture healing in murine models (72). Preclinical studies suggest that
recombinant irisin may prevent osteoblast differentiation deficits.
However, these findings are largely preclinical; clinical evidence
in humans is lacking, and significant hurdles including short
half-life, potential immunogenicity, and high manufacturing costs
remain to be addressed. These findings are complemented by evidence
that irisin promotes osteogenesis via BMP/SMAD signaling through αV
integrin (8), establishing a
mechanistic rationale for its therapeutic application. Conversely,
strategies targeting catabolic myokines have also emerged. Genetic
and pharmacologic inhibition of myostatin improved bone properties
in osteogenesis imperfecta models (56,85), suggesting that neutralizing this
negative regulator could yield anabolic benefits. Nevertheless,
several challenges impede clinical translation. Compared with
existing bone drugs such as parathyroid hormone (PTH) analogs
(anabolic) and denosumab (anti-resorptive), myokine-based therapies
have not yet demonstrated superior efficacy in head-to-head
comparisons. PTH analogs have well-established pharmacokinetic
profiles and long-term safety data, while denosumab offers
convenient biannual subcutaneous dosing. By contrast, recombinant
myokines face critical limitations including short half-life
(typically minutes to hours), potential immunogenicity due to
non-human post-translational modifications, and high manufacturing
costs associated with eukaryotic expression systems required for
proper bioactivity. Furthermore, the optimal dosing regimen,
long-term safety and potential off-target effects of myokine-based
therapies remain unknown. Advanced delivery platforms, including
PEGylation (86), fusion protein
technologies (87) and
extracellular vesicle-based systems (88), are being explored to enhance
pharmacokinetic profiles and tissue targeting. However, the optimal
formulation strategy must balance improved stability against
potential alterations in bioactivity and immunogenicity profiles.
Recombinant myokines are typically produced in prokaryotic or
eukaryotic expression systems. To overcome poor permeability, low
stability and lack of suitable delivery systems, several strategies
have been explored, including PEGylation (86), fusion protein technologies
(87), extracellular
vesicle-based systems (88) and
nanoparticle formulations (89).
Critically, the long-term safety of recombinant myokines is
unknown, and the biomarker literature is plagued by inconsistent
assay methodologies, making clinical translation speculative
without rigorous head-to-head comparisons with existing bone
drugs.
Personalized exercise prescription
The recognition that myokine responses are highly
dependent on exercise modality, intensity and individual biological
characteristics has profound implications for precision-based
exercise prescription. Meta-analytical evidence indicates that
concurrent aerobic and resistance training yields distinct effects
on circulating irisin levels compared with single-modality
approaches (90). Moreover,
resistance training has been shown to reduce STAT3 activation and
attenuate muscle atrophy in tumor-bearing mice (74,89), highlighting modality-specific
molecular pathways. In clinical populations, combined resistance
and aerobic training improved bone mass and reduced systemic
inflammation in HIV-infected individuals (91), while alternating aerobic with
resistance exercise enhanced bone mineral density and irisin levels
in postmenopausal women (86).
The differential myokine signatures elicited by various exercise
regimens support the concept of tailoring prescriptions based on
baseline myokine profiles, disease status and treatment goals
(92,93). Recent evidence also suggests that
exercise-induced metabolic reprogramming and immune modulation may
underpin some of the bone-protective effects, further emphasizing
the need for personalized approaches (94). Nevertheless, translating these
findings into standardized clinical protocols requires rigorous
validation of dose-response relationships and identification of
predictive biomarkers that identify patients most likely to benefit
from specific exercise modalities.
Myokine profiles as diagnostic and
prognostic biomarkers
Circulating myokine levels have garnered substantial
interest as non-invasive biomarkers for bone disorders, sarcopenia
and associated musculoskeletal conditions. Systematic reviews and
meta-analyses have demonstrated that lower irisin levels correlate
with osteoporosis in women (95), type 2 diabetes mellitus (96) and diabetic nephropathy (97), suggesting its potential as a
diagnostic marker. While observational studies report correlations
between circulating myokine levels and bone disorders, these
findings are associative rather than causal. Major limitations
include substantial heterogeneity in assay methodologies, lack of
standardized reference ranges, limited longitudinal evidence and
the absence of robust clinical validation. Furthermore, circulating
myokine levels reflect composite tissue sources rather than
muscle-specific secretion. Conversely, elevated myostatin levels
have been associated with muscle wasting in various pathologies,
including cirrhosis (98),
chronic kidney disease (99) and
cancer (100), although the
relationship is complex and may be influenced by disease stage and
patient characteristics. Emerging evidence indicates that myostatin
in combination with creatine phosphokinase or albumin may improve
discrimination of sarcopenia in cirrhosis (98,101), and the
myostatin-to-appendicular skeletal muscle mass ratio has been
proposed as a more sensitive marker than myostatin alone in older
women (102). Longitudinal
studies have identified plasma biomarkers associated with muscle
function decline (103) and
sarcopenia (101), while
extracellular vesicle-derived markers show promise for detecting
low muscle mass and physical performance deficits (104). The prognostic utility of
myokines is further supported by findings that irisin levels
predict cardiac contractile dysfunction in heart failure and
correlate with outcomes in hepatocellular carcinoma (105). However, a major limitation of
myokines as tissue-specific biomarkers is their lack of exclusivity
to skeletal muscle. For example, irisin is also produced by adipose
tissue, brain, liver and other organs, and its expression can be
influenced by non-exercise factors such as metabolic state,
inflammation and circadian rhythms. Similarly, myostatin is
expressed in adipose tissue and heart, and IL-6 is produced by
multiple cell types including immune cells and adipocytes.
Consequently, circulating myokine levels reflect a composite of
tissue sources rather than muscle-specific secretion, confounding
their interpretation as pure muscle-bone signaling markers. A major
limitation is the lack of tissue specificity (well-established).
Despite these promising associations, several limitations persist,
including substantial heterogeneity in assay methodologies, lack of
standardized reference ranges, and the influence of sex, age and
circadian rhythms on circulating levels (106). Future efforts must prioritize
assay harmonization and validation in large, well-characterized
cohorts to establish clinical utility.
Synergistic effects with pharmacological
agents
The combination of myokine-targeted interventions
with existing pharmacological therapies offers opportunities for
additive or synergistic effects on bone health. Preclinical studies
have shown that PTH (1-34) treatment and mechanical loading
exert complementary osteogenic effects on trabecular and cortical
bone in ovariectomized mice (107), suggesting that myokine-inducing
exercise may enhance the efficacy of anabolic agents. Similarly,
the gut-bone axis has been identified as a mediator of exercise
modality-dependent suppression of inflammatory osteoclastogenesis
in ovariectomy-induced bone loss (75), indicating that exercise-induced
myokines may modulate the skeletal response to hormonal therapies.
The potential for drug-myokine interactions requires careful
consideration, as therapeutic proteins can influence cytochrome
P450 activity and alter the pharmacokinetics of co-administered
drugs (108). Conversely,
pharmacological agents may impact myokine expression and function.
For instance, recombinant human BMP-2-induced osteogenesis is
modulated by irisin (64),
suggesting potential synergy when combining growth factor therapies
with myokine-based strategies. The integration of exercise
interventions with bisphosphonates, denosumab, or PTH analogs
warrants systematic investigation in clinical trials designed to
evaluate both additive effects and potential interactions.
Barriers to clinical translation
Despite substantial progress, several barriers
impede the clinical translation of myokine-based diagnostics and
therapeutics. Bioavailability remains a critical challenge,
particularly for oral administration, where gastrointestinal
degradation and poor permeability limit absorption (109). Advanced delivery systems,
including nanoparticle formulations, microneedle technologies and
polymersomes, are under development to address these limitations
(89,110,111). The stability of therapeutic
proteins in biological fluids and during storage continues to pose
formulation challenges, with factors such as pH, temperature and
excipient composition influencing degradation pathways (112). Immunogenicity risk assessment
is essential for engineered myokine analogs, as anti-drug antibody
formation can neutralize efficacy and, in rare cases, trigger
adverse reactions (113). The
heterogeneity of myokine responses across populations, which is
influenced by age, sex, genetic variation and disease status,
complicates the development of standardized diagnostic cutoffs and
dosing regimens (106).
Furthermore, the complex interplay between myokines and other
circulating factors, including adipokines (114), necessitates a multi-analyte
approach for accurate disease characterization. Addressing these
barriers will require coordinated efforts in analytical method
development, physiologically based pharmacokinetic modeling, and
innovative formulation strategies tailored to the unique properties
of myokine-based therapeutics.
In summary, while myokines hold promise as
therapeutic targets and biomarkers, the current evidence is largely
preclinical or correlative. Cautious interpretation is warranted,
and rigorous clinical validation is required before translation
into practice.
Methodological advances and emerging
frontiers
This section highlights methodological advances with
demonstrated or potential application to myokine-mediated
muscle-bone crosstalk; examples from other bone-related fields are
included as background to illustrate broader technological
capabilities. Recent technological innovations have profoundly
expanded the capacity to investigate myokine-mediated muscle-bone
crosstalk at unprecedented resolution. The convergence of
multi-omics platforms, single-cell technologies, organ-on-chip
systems and artificial intelligence approaches is transforming the
understanding of exercise-regulated signaling networks and
accelerating the translation of myokine-based concepts toward
clinical applications (Table
III).
| Table IIIKey methodological advances in
myokine-mediated muscle-bone crosstalk research. |
Table III
Key methodological advances in
myokine-mediated muscle-bone crosstalk research.
| Authors, year | Technology
platform | Relevance to
myokines | Key finding | (Refs.) |
|---|
| Du et al,
2025 | Multi-omics
integration | Indirect | Identified androgen
receptor signaling in osteoporosis | (115) |
| Cui et al,
2025 | Integrative
multi-omics | Indirect | Deciphered
molecular mechanisms of Gu Shu Kang Granules | (116) |
| Liu et al,
2025 | Multi-omics +
multimodal data | Indirect | Repurposed
acebutolol for osteoporosis treatment | (117) |
| Wang et al,
2022 | Single-cell
RNA-seq | Indirect | Dissected immune
heterogeneity in osteoporosis | (119) |
| Xiao et al,
2023 | Spatial
transcriptomics | Indirect | Mapped spatial
organization of bone marrow signaling | (120) |
| Deng et al,
2025 | Spatial
transcriptomics | Direct | Decoded
communication networks in bone-muscle interface | (121) |
| Giza et al,
2022 | Microphysiological
system | Indirect | Modeled contractile
differences in young vs. old muscle cells | (122) |
| Suresh Kumar et
al, 2023 | Muscle-bone
co-culture chip | Direct | Biomechanical
stimulation of muscle modulates bone phenotype via myokines | (20) |
| Yin et al,
2026 | Muscle
regeneration-on-chip | Direct | Identified optimal
mechanical stimulation for muscle regeneration | (124) |
| Parafati et
al, 2025 | Muscle
lab-on-chip | Indirect | Revealed
microgravity-induced muscle degeneration | (125) |
| Zhou et al,
2024 | Machine learning +
single-cell analysis | Indirect | Identified shared
biomarkers in inflammatory arthritis | (126) |
| Zhang et al,
2022 | Network
pharmacology + molecular docking | Indirect | Revealed mechanisms
of Tripterygii Wilfordii against osteosarcoma | (128) |
Multi-omics approaches have emerged as powerful
strategies for comprehensive myokine discovery and validation. For
example, the multi-omics integration strategy used by Du et
al (115) to identify
androgen receptor signaling in osteoporosis could be directly
applied to profile the exercise-induced myokine secretome and
identify novel myokines that regulate bone homeostasis. Similarly,
the integrative multi-omics framework that deciphered molecular
mechanisms of herbal formulations in sarcopenia-osteoporosis could
be adapted to map the signaling networks through which
exercise-induced myokines (for example, irisin, IL-6 and myostatin)
exert their effects on bone cells (116). Furthermore, the multi-omics and
multi-modal data analysis approach used to repurpose drugs for
osteoporosis could be employed to identify existing compounds that
mimic or enhance the osteogenic effects of exercise-responsive
myokines (117). These
approaches are particularly powerful when integrated with causal
inference methods, as demonstrated in studies of inflammatory bone
disorders (118); such causal
inference frameworks could be applied to distinguish direct
myokine-mediated effects from indirect exercise-associated changes
in bone metabolism. Despite these advances, challenges persist
regarding data integration standardization and functional
validation throughput, limiting the direct translation of
multi-omics findings into clinically actionable myokine
targets.
Single-cell and spatial transcriptomics technologies
have revolutionized the understanding of cellular heterogeneity
within the muscle-bone-immune axis. These approaches enable the
dissection of cell-type-specific responses to exercise-derived
myokines and the mapping of intercellular communication networks.
The single-cell RNA sequencing approach used by Wang et al
(119) to dissect the
osteoimmunology microenvironment in osteoporosis could be directly
applied to identify which immune cell subsets (for example,
CD8+ T cells and macrophages) are specifically modulated
by exercise-induced myokines such as IL-33 and irisin.
Complementary spatial transcriptomic interrogation of the murine
bone marrow signaling landscape provides a template for mapping the
spatial distribution of myokine receptor expression within bone
niches, revealing which bone cell types are positioned to respond
to circulating myokines (120).
Notably, Deng et al (121) have specifically applied spatial
transcriptomics to decode cellular communication networks and
signaling pathways in bone-muscle crosstalk, providing a
methodological framework directly relevant to myokine research. The
integration of single-cell resolution with spatial context
represents a significant advance over bulk analyses, although the
high cost and technical complexity currently limit widespread
application.
Microphysiological systems and organ-on-chip
platforms have emerged as transformative tools for modeling
exercise effects on muscle-bone interactions under controlled
conditions. Giza et al (122) developed a microphysiological
system for studying contractile differences in young, active vs.
old, sedentary adult-derived skeletal muscle cells, enabling the
investigation of age-related alterations in myokine secretion.
Suresh Kumar et al (20)
demonstrated that biomechanical stimulation of muscle constructs
directly influences the phenotype of bone constructs by modulating
myokine secretion, providing direct evidence for the utility of
such systems in studying muscle-bone crosstalk. The miniaturized 3D
myotube contraction monitoring chip developed for modeling muscular
dystrophies could be adapted to measure real-time myokine release
from exercised muscle constructs and to test the effects of
specific mechanical loading patterns on myokine secretion profiles
(123). More recently, Yin
et al (124) developed a
muscle regeneration on a chip platform to study exercise-induced
microtrauma and identify optimal mechanical stimulation regimens;
such platforms could be coupled with bone cell co-cultures to
directly assess how exercise-mimetic mechanical stimuli regulate
myokine-mediated osteoblast differentiation. Parafati et al
(125) utilized a muscle
lab-on-chip model aboard the International Space Station to
demonstrate that microgravity accelerates skeletal muscle
degeneration; similar microphysiological systems could be used to
study how unloading-induced changes in myokine secretion contribute
to disuse osteoporosis. These platforms offer distinct advantages
over traditional cell culture by recapitulating the mechanical and
architectural features of native tissue, yet challenges remain in
incorporating multiple cell types and vascular components to fully
mimic the physiological muscle-bone unit.
The integration of machine learning and artificial
intelligence with multi-omics datasets is opening new frontiers in
predicting myokine-bone signaling networks. The machine learning
approaches used to identify shared biomarkers in inflammatory
arthritis (126) could be
applied to analyze myokine expression data from exercised human
cohorts, thereby identifying circulating myokine signatures that
predict bone anabolic responses to specific exercise modalities.
Furthermore, the application of deep learning to spatial
transcriptomics data is enabling the prediction of cellular
communication networks from tissue architecture (127); such computational approaches
could be used to model how myokines diffuse through bone tissue and
which cell types are preferentially targeted based on their spatial
expression of myokine receptors. These computational approaches are
particularly valuable for integrating heterogeneous datasets and
generating testable hypotheses regarding myokine function. However,
the interpretability of machine learning models remains a concern,
and experimental validation of computationally derived predictions
continues to be essential.
Collectively, these methodological advances are
reshaping the landscape of myokine research. The transition from
bulk analyses to single-cell and spatial approaches has revealed
previously unappreciated cellular heterogeneity within the
muscle-bone axis. Organ-on-chip platforms now enable mechanistic
studies under physiologically relevant conditions that were
previously impossible to achieve. Multi-omics integration coupled
with artificial intelligence is accelerating the discovery of novel
myokines and their signaling networks. Future progress will depend
on the standardization of these platforms, the development of more
sophisticated coculture systems that incorporate immune cells and
vasculature, and the integration of multiple methodological
approaches to provide a comprehensive understanding of
myokine-mediated muscle-bone crosstalk. Despite their promise,
emerging technologies have not yet yielded clinically actionable
myokine targets, largely owing to a lack of functional validation
and standardized protocols across laboratories.
Conclusions
Exercise induced myokines form a complex signaling
network that integrates mechanical, metabolic, and immune inputs to
regulate bone homeostasis. The interplay among Wnt/β catenin, MAPK,
NF κB, and TGF β/BMP pathways determines the net skeletal response.
This review provides an integrated analysis of current knowledge,
highlighting that the muscle-bone-immune axis and epigenetic
regulation represent emerging frontiers. Methodological advances
such as multi-omics and organ-on-chip platforms are accelerating
translational opportunities. Harnessing myokine based strategies
holds promise for developing biomarkers and therapeutic
interventions for bone disorders.
Availability of data and materials
Not applicable.
Authors' contributions
BT and XK made substantial contributions to
conception and design. XC and JZ performed acquisition, analysis,
and interpretation of data. All authors were involved in drafting
the manuscript and revising it critically for important
intellectual content and agree to be accountable for all aspects of
the work. All authors read and approved the final version of the
manuscript. Data authentication is not applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Abbreviations:
|
AKT
|
protein kinase B
|
|
BMP
|
bone morphogenetic protein
|
|
BMSC
|
bone marrow mesenchymal stem cell
|
|
CCL5
|
chemokine ligand 5
|
|
ERK
|
extracellular signal-regulated
kinase
|
|
IGF-1
|
insulin-like growth factor-1
|
|
JAK
|
Janus kinase
|
|
JNK
|
c-Jun N-terminal kinase
|
|
MAPK
|
mitogen-activated protein kinase
|
|
Metrnl
|
meteorin-like protein
|
|
MSC
|
mesenchymal stem cell
|
|
NF-κB
|
nuclear factor kappa B
|
|
Nrf2
|
nuclear factor erythroid 2-related
factor 2
|
|
OPG
|
osteoprotegerin
|
|
PGC-1α
|
peroxisome proliferator-activated
receptor gamma coactivator 1-alpha
|
|
PI3K
|
phosphatidylinositol 3-kinase
|
|
PTH
|
parathyroid hormone
|
|
PTOA
|
post-traumatic osteoarthritis
|
|
RANK
|
receptor activator of nuclear
factor-κB
|
|
RANKL
|
RANK ligand
|
|
Runx2
|
runt-related transcription factor
2
|
|
STAT3
|
signal transducer and activator of
transcription 3
|
|
STING
|
stimulator of interferon genes
|
|
TGF-β
|
transforming growth factor-beta
|
Acknowledgements
Not applicable.
Funding
No funding was received.
References
|
1
|
Ha J, Sung S and Kim H: Myokines and
interorgan crosstalk: Bridging exercise to health promotion and
disease prevention. Ann Pediatr Endocrinol Metab. 30:59–68. 2025.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kaji H: Crosstalk between muscle and bone.
J Bone Miner Metab. 42:391–398. 2024. View Article : Google Scholar
|
|
3
|
Malvandi AM, Gerosa L, Banfi G and
Lombardi G: The bone-muscle unit: From mechanical coupling to
soluble factors-mediated signaling. Mol Aspects Med.
103:1013672025. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yi J, Chen J, Yao X, Zhao Z, Niu X, Li X,
Sun J, Ji Y, Shang T, Gong L, et al: Myokine-mediated muscle-organ
interactions: Molecular mechanisms and clinical significance.
Biochem Pharmacol. 242:1173262025. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Morin SN, Leslie WD and Schousboe JT:
Osteoporosis: A review. JAMA. 334:894–907. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kumar S, Smith C, Clifton-Bligh RJ, Beck
BR and Girgis CM: Exercise for postmenopausal bone health-can we
raise the bar? Curr Osteoporos Rep. 23:202025. View Article : Google Scholar
|
|
7
|
Gries KJ, Zysik VS, Jobe TK, Griffin N,
Leeds BP and Lowery JW: Muscle-derived factors influencing bone
metabolism. Semin Cell Dev Biol. 123:57–63. 2022. View Article : Google Scholar
|
|
8
|
Xue Y, Hu S, Chen C, He J, Sun J, Jin Y,
Zhang Y, Zhu G, Shi Q and Rui Y: Myokine Irisin promotes
osteogenesis by activating BMP/SMAD signaling via αV integrin and
regulates bone mass in mice. Int J Biol Sci. 18:572–584. 2022.
View Article : Google Scholar
|
|
9
|
Temporiti F, Ferrari S, Kieser M and Gatti
R: Efficacy and characteristics of physiotherapy interventions in
patients with lumbar spinal stenosis: A systematic review. Eur
Spine J. 31:1370–1390. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Liu XH, Pan JP, Bauman WA and Cardozo C:
Myostatin inhibits insulin-like growth factor 1-dependent citrate
secretion and osteogenesis via nicotinamide adenine dinucleotide
phosphate oxidase-4 in a mouse mesenchymal stem cell line. Ann N Y
Acad Sci. 1517:203–212. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kim SH, Ramani PS, Jahagirdar VR, Roitberg
B and Zileli M: Endocrine assessment, chemotherapy, nonsurgical
treatment, and rehabilitation for osteoporotic spine fractures:
WFNS spine committee recommendations. J Neurosurg Sci. 66:300–310.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ji X, Hu X, Xu T and Yang W: Roles of
myokines in osteoporosis under physiological and diabetic
conditions. Front Endocrinol (Lausanne). 16:16002182025. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Liu M, Han Y, Wang J, Zhu Y, Zhang Y, Chu
Q, Yang C, Chen B and Sun G: Skeletal muscle-derived IL-33 mediates
muscle-to-bone crosstalk and regulates bone metabolism via
CD8+ T cell-secreted CCL5. EBioMedicine. 122:1060242025.
View Article : Google Scholar
|
|
14
|
Weng K, He Y, Weng X and Yuan Y: Exercise
alleviates osteoporosis by regulating the secretion of the
senescent associated secretory phenotype. Bone. 196:1174852025.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ma M, Zhang Z, Bo H and Zhang Y: Skeletal
muscle as endocrine organ. Adv Exp Med Biol. 1478:513–543. 2025.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jaśkiewicz Ł, Romaszko-Wojtowicz A,
Chmielewski G, Kuna J and Krajewska-Włodarczyk M: Effect of
myokines on bone tissue metabolism: A systematic review. Bone.
201:1176542025. View Article : Google Scholar
|
|
17
|
Gomarasca M, Banfi G and Lombardi G:
Myokines: The endocrine coupling of skeletal muscle and bone. Adv
Clin Chem. 94:155–218. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Horváth L, Pekař M, Švagera Z, Horká V,
Mráz M and Bužga M: Skeletal muscle as an auto-, para- and
endocrine organ: The role of myokines in muscle metabolism and
other metabolic organs. Physiol Res. 74(Suppl 1): S37–S56. 2025.
View Article : Google Scholar
|
|
19
|
Huh JY: The role of exercise-induced
myokines in regulating metabolism. Arch Pharm Res. 41:14–29. 2018.
View Article : Google Scholar
|
|
20
|
Suresh Kumar H, Barnett EN, Fowlkes JL,
Kalaitzoglou E and Annamalai RT: Biomechanical stimulation of
muscle constructs influences phenotype of bone constructs by
modulating myokine secretion. JBMR Plus. 7:e108042023. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zhao Z, Yan K, Guan Q, Guo Q and Zhao C:
Mechanism and physical activities in bone-skeletal muscle
crosstalk. Front Endocrinol (Lausanne). 14:12879722024. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hatakeyama J, Inoue S, Jiang H, Yokoi R
and Moriyama H: Exercise-induced interactions between skeletal
muscle and bone via myokines and osteokine in mice: Role of
FNDC5/irisin, IGF-1, and osteocalcin. Bone. 190:1173142025.
View Article : Google Scholar
|
|
23
|
Tao L, Wang J, Wang K, Liu Q, Li H, Xu S,
Gu C and Zhu Y: Exerkine FNDC5/irisin-enriched exosomes promote
proliferation and inhibit ferroptosis of osteoblasts through
interaction with Caveolin-1. Aging Cell. 23:e141812024. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Xu Q, Cui Y, Luan J, Zhou X, Li H and Han
J: Exosomes from C2C12 myoblasts enhance osteogenic differentiation
of MC3T3-E1 pre-osteoblasts by delivering miR-27a-3p. Biochem
Biophys Res Commun. 498:32–37. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Herrmann M, Engelke K, Ebert R,
Müller-Deubert S, Rudert M, Ziouti F, Jundt F, Felsenberg D and
Jakob F: Interactions between muscle and bone-where physics meets
biology. Biomolecules. 10:4322020. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Laurent MR, Dubois V, Claessens F,
Verschueren SM, Vanderschueren D, Gielen E and Jardí F: Muscle-bone
interactions: From experimental models to the clinic? A critical
update. Mol Cell Endocrinol. 432:14–36. 2016. View Article : Google Scholar
|
|
27
|
Leuchtmann AB, Adak V, Dilbaz S and
Handschin C: The role of the skeletal muscle secretome in mediating
endurance and resistance training adaptations. Front Physiol.
12:7098072021. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Agostinete RR, Werneck AO, Narciso PH,
Ubago-Guisado E, Coelho-E-Silva MJ, Bielemann RM, Gobbo LA, Lynch
BT, Fernandes RA and Vlachopoulos D: Resistance training presents
beneficial effects on bone development of adolescents engaged in
swimming but not in impact sports: ABCD growth study. BMC Pediatr.
24:2472024. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Andersson Å, Olsson MC, Torell A, Mogard E
and Haglund E: Effects on serum protein levels from one bout of
high intensity interval training in individuals with axial
spondyloarthritis and controls. Immun Inflamm Dis. 13:e703052025.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Tsai CL: Acute effects of high-intensity
interval exercise plus whole-body vibration on bone turnover
markers, BDNF, irisin, and neurocognitive performance in
postmenopausal women. Biol Psychol. 196:1090292025. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Śliwicka E, Cisoń T,
Pilaczyńska-Szcześniak Ł, Ziemba A and Straburzyńska-Lupa A:
Effects of marathon race on selected myokines and sclerostin in
middle-aged male amateur runners. Sci Rep. 11:28132021. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Ning K, Wang Z and Zhang XA:
Exercise-induced modulation of myokine irisin in bone and cartilage
tissue-positive effects on osteoarthritis: A narrative review.
Front Aging Neurosci. 14:9344062022. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kawao N, Iemura S, Kawaguchi M, Mizukami
Y, Takafuji Y and Kaji H: Role of irisin in effects of chronic
exercise on muscle and bone in ovariectomized mice. J Bone Miner
Metab. 39:547–557. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Ma J, Wen J, Qiu Y, Wang Y, Liu T, Xiao Q,
Zhang D, Zhao Y, Lu Z, Li J, et al: The regional impact of exercise
on bone density in older adults: A meta-analysis with molecular
mechanism insights. Geriatr Nurs. 65:1034512025. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Norton A, Thieu K, Baumann CW, Lowe DA and
Mansky KC: Estrogen regulation of myokines that enhance osteoclast
differentiation and activity. Sci Rep. 12:159002022. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Vita F, Gangemi S, Pioggia G, Trimarchi F
and Di Mauro D: Physical activity and post-transcriptional
regulation of aging decay: Modulation of pathways in postmenopausal
osteoporosis. Medicina (Kaunas). 58:7672022. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Evans WJ, Guralnik J, Cawthon P, Appleby
J, Landi F, Clarke L, Vellas B, Ferrucci L and Roubenoff R:
Sarcopenia: No consensus, no diagnostic criteria, and no approved
indication-How did we get here? Geroscience. 46:183–190. 2024.
View Article : Google Scholar :
|
|
38
|
Koltun KJ, Sterczala AJ, Sekel NM,
Krajewski KT, Martin BJ, Lovalekar M, Connaboy C, Flanagan SD,
Wardle SL, O'Leary TJ, et al: Effect of acute resistance exercise
on bone turnover in young adults before and after concurrent
resistance and interval training. Physiol Rep. 12:e159062024.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Posa F, Colaianni G, Di Cosola M, Dicarlo
M, Gaccione F, Colucci S, Grano M and Mori G: The myokine irisin
promotes osteogenic differentiation of dental bud-derived MSCs.
Biology (Basel). 10:2952021.PubMed/NCBI
|
|
40
|
Yang J, Yu K, Liu D, Yang J, Tan L and
Zhang D: Irisin enhances osteogenic differentiation of mouse
MC3T3-E1 cells via upregulating osteogenic genes. Exp Ther Med.
21:5802021. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Cui Y, Yi Q, Sun W, Huang D, Zhang H, Duan
L, Shang H, Wang D and Xiong J: Molecular basis and therapeutic
potential of myostatin on bone formation and metabolism in
orthopedic disease. Biofactors. 49:21–31. 2023. View Article : Google Scholar
|
|
42
|
Chang PY, Wu HK, Chen YH, Hsu YP, Cheng
MT, Yu CH and Chen SK: Interleukin-6 transiently promotes
proliferation of osteoclast precursors and stimulates the
production of inflammatory mediators. Mol Biol Rep. 49:3927–3937.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Coates BA, McKenzie JA, Yoneda S and Silva
MJ: Interleukin-6 (IL-6) deficiency enhances intramembranous
osteogenesis following stress fracture in mice. Bone.
143:1157372021. View Article : Google Scholar
|
|
44
|
Feng W, Yang P, Liu H, Zhang F and Li M:
IL-6 promotes low concentration of RANKL-induced osteoclastic
differentiation by mouse BMMs through trans-signaling pathway. J
Mol Histol. 53:599–610. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Liu QQ, Wu WW, Yang J, Wang RB, Yuan LL,
Peng PZ, Zeng MY and Yu K: A GP130-targeting small molecule,
LMT-28, reduces LPS-induced bone resorption around implants in
diabetic models by inhibiting IL-6/GP130/JAK2/STAT3 signaling.
Mediators Inflamm. 2023:93304392023. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Henning P, Movérare-Skrtic S, Westerlund
A, Chaves de Souza PP, Floriano-Marcelino T, Nilsson KH, El Shahawy
M, Ohlsson C and Lerner UH: WNT16 is robustly increased by
oncostatin M in mouse calvarial osteoblasts and acts as a negative
feedback regulator of osteoclast formation induced by oncostatin M.
J Inflamm Res. 14:4723–4741. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
de Souza PPC, Henning P and Lerner UH:
Stimulation of osteoclast formation by oncostatin m and the role of
WNT16 as a negative feedback regulator. Int J Mol Sci. 23:32872022.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Tirado-Cabrera I, Martin-Guerrero E,
Heredero-Jimenez S, Ardura JA and Gortázar AR: PTH1R translocation
to primary cilia in mechanically-stimulated ostecytes prevents
osteoclast formation via regulation of CXCL5 and IL-6 secretion. J
Cell Physiol. 237:3927–3943. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Jiao Z, Chai H, Wang S, Sun C, Huang Q and
Xu W: SOST gene suppression stimulates osteocyte Wnt/β-catenin
signaling to prevent bone resorption and attenuates
particle-induced osteolysis. J Mol Med (Berl). 101:607–620. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
He X, Hua Y, Li Q, Zhu W, Pan Y, Yang Y,
Li X, Wu M, Wang J and Gan X: FNDC5/irisin facilitates
muscle-adipose-bone connectivity through ubiquitination-dependent
activation of runt-related transcriptional factors RUNX1/2. J Biol
Chem. 298:1016792022. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Chen J, Liu J, Fu Q, Xu M, Zhai X, Li L,
Xu W, Wu X, Wang K and Si H: Irisin inhibits adipogenic
differentiation of bone marrow mesenchymal stem cells through the
SIRT1/RANBP2/FTO signaling axis and protects against osteoporosis.
Cell Death Discov. 12:1142026. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Chen W, Zheng H, Liao Q, Zeng S, Bai R,
Shi J, Jiang Y, Wang T, Jia H, Liang W, et al: Zhuang-Gu-Fang
promotes osteoblast differentiation via myoblasts and
myoblast-derived exosomal miRNAs:miR-5100, miR-126a-3p,
miR-450b-5p, and miR-669a-5p. Phytomedicine. 130:1557182024.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Shanazari Z, Hemati Farsani Z, Faramarzi M
and Banitalebi E: MyomiR-OsteomiR crosstalk induced by different
modes and intensities of exercise training and its role in
controlling osteogenic differentiation in old male Wistar rats. Exp
Gerontol. 149:1113052021. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Piao X, Wu X, Yan Y, Li Y, Li N, Xue L and
He F: Targeting EZH2 attenuates the ferroptosis-mediated
osteoblast-osteoclast imbalance in rheumatoid arthritis. Int
Immunopharmacol. 143:1132012024. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Chen Z, Zhang Y, Zhao F, Yin C, Yang C,
Wang X, Wu Z, Liang S, Li D, Lin X, et al: Recombinant irisin
prevents the reduction of osteoblast differentiation induced by
stimulated microgravity through increasing β-catenin expression.
Int J Mol Sci. 21:12592020. View Article : Google Scholar
|
|
56
|
Omosule CL, Gremminger VL, Aguillard AM,
Jeong Y, Harrelson EN, Miloscio L, Mastaitis J, Rafique A, Kleiner
S, Pfeiffer FM, et al: Impact of genetic and pharmacologic
inhibition of myostatin in a murine model of osteogenesis
imperfecta. J Bone Miner Res. 36:739–756. 2021. View Article : Google Scholar
|
|
57
|
Fujita K, Otsuka T, Kawabata T, Kainuma S,
Sakai G, Matsushima-Nishiwaki R, Kozawa O and Tokuda H: HSP90
limits thrombin-stimulated IL-6 synthesis in osteoblast-like
MC3T3-E1 cells: Regulation of p38 MAPK. Int J Mol Med.
42:2185–2192. 2018.PubMed/NCBI
|
|
58
|
Hioki T, Tokuda H, Nakashima D, Fujita K,
Kawabata T, Sakai G, Kim W, Tachi J, Tanabe K, Matsushima-Nishiwaki
R, et al: HSP90 inhibitors strengthen extracellular ATP-stimulated
synthesis of interleukin-6 in osteoblasts: Amplification of p38 MAP
kinase. Cell Biochem Funct. 39:88–97. 2021. View Article : Google Scholar
|
|
59
|
Hu X, Zhang H, Wang Z, Zhao X, Hu T, Liu
C, Chen X, Wang W and Lu S: Exercise-derived irisin prevents bone
loss via Nrf2 activation and inhibition of STING/NF-κB signaling.
Free Radic Biol Med. 246:51–68. 2026. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Jiang Y, Qi X, Cui H, Huang Y, Lv Y, Yang
Y, Yao X and Yang D: The inflammation-energy metabolism axis: A
central driver of sarcopenia-osteoporosis: A narrative review.
Calcif Tissue Int. 117:92026. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Huang RL, Sun Y, Ho CK, Liu K, Tang QQ,
Xie Y and Li Q: IL-6 potentiates BMP-2-induced osteogenesis and
adipogenesis via two different BMPR1A-mediated pathways. Cell Death
Dis. 9:1442018. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Cheng H, Gao X, Huard M, Lu A, Ruzbarsky
JJ, Amra S, Wang B and Huard J: Bone morphogenetic protein 4
rescues the bone regenerative potential of old muscle-derived stem
cells via regulation of cell cycle inhibitors. Stem Cell Res Ther.
13:3852022. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Adhikary S, Choudhary D, Tripathi AK,
Karvande A, Ahmad N, Kothari P and Trivedi R: FGF-2 targets
sclerostin in bone and myostatin in skeletal muscle to mitigate the
deleterious effects of glucocorticoid on musculoskeletal
degradation. Life Sci. 229:261–276. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Ohyama Y, Ohta Y, Sugama R, Minoda Y,
Masuda S, Terai H and Nakamura H: Effect of recombinant irisin on
recombinant human bone morphogenetic protein-2 induced osteogenesis
and osteoblast differentiation. Biochem Biophys Res Commun.
734:1507872024. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Resende-Coelho A, Ali MM, James A, Warren
A, Gatrell L, Kadhim I, Fu Q, Xiong J, Onal M and Almeida M:
Mitochondrial oxidative stress or decreased autophagy in osteoblast
lineage cells is not sufficient to mimic the deleterious effects of
aging on bone mechanoresponsiveness. Aging (Albany NY). 17:610–629.
2025.PubMed/NCBI
|
|
66
|
Wang B, Liu J, Wang Q, Arhatte M, Cheong
LY, Glogowska E, Jiang X, Chung SK, Jin L, Hu Q, et al: Piezo1
activation suppresses bone marrow adipogenesis to prevent
osteoporosis by inhibiting a mechanoinflammatory autocrine loop.
Signal Transduct Target Ther. 10:3572025. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Colaianni G, Errede M, Sanesi L,
Notarnicola A, Celi M, Zerlotin R, Storlino G, Pignataro P, Oranger
A, Pesce V, et al: Irisin correlates positively with BMD in a
cohort of older adult patients and downregulates the senescent
marker p21 in osteoblasts. J Bone Miner Res. 36:305–314. 2021.
View Article : Google Scholar
|
|
68
|
Arrieta H, Hervás G, Rezola-Pardo C,
Ruiz-Litago F, Iturburu M, Yanguas JJ, Gil SM, Rodriguez-Larrad A
and Irazusta J: Serum myostatin levels are higher in fitter, more
active, and non-frail long-term nursing home residents and increase
after a physical exercise intervention. Gerontology. 65:229–239.
2019. View Article : Google Scholar
|
|
69
|
Kawaguchi M, Kawao N, Takafuji Y, Ishida M
and Kaji H: Myonectin inhibits the differentiation of osteoblasts
and osteoclasts in mouse cells. Heliyon. 6:e039672020. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Buchmann N, Fielitz J, Spira D, König M,
Norman K, Pawelec G, Goldeck D, Demuth I and Steinhagen-Thiessen E:
Muscle mass and inflammation in older adults: Impact of the
metabolic syndrome. Gerontology. 68:989–998. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Chen M, Zhang Y, Yu X and Zuo Q:
Alternating aerobics with resistance exercise improves bone density
and circulating irisin levels in postmenopausal women. Med Sci
Sports Exerc. 57:921–931. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Colucci SC, Buccoliero C, Sanesi L, Errede
M, Colaianni G, Annese T, Khan MP, Zerlotin R, Dicarlo M, Schipani
E, et al: Systemic administration of recombinant irisin accelerates
fracture healing in mice. Int J Mol Sci. 22:108632021. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Ghayomzadeh M, Hackett D, SeyedAlinaghi S,
Gholami M, Hosseini Rouzbahani N and Azevedo Voltarelli F: Combined
training improves the diagnostic measures of sarcopenia and
decreases the inflammation in HIV-infected individuals. J Cachexia
Sarcopenia Muscle. 13:1024–1035. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Testa MTJ, Cella PS, Marinello PC,
Frajacomo FTT, Padilha CS, Perandini PC, Moura FA, Duarte JA,
Cecchini R, Guarnier FA and Deminice R: Resistance training
attenuates activation of STAT3 and muscle atrophy in tumor-bearing
mice. Front Oncol. 12:8807872022. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Gao Y, Wang H, Shi L, Cao M, Liu X, Zhang
Y, Chen X, Rong Y, Han B, Lu P, et al: Gut-bone axis mediates
exercise modality-dependent suppression of inflammatory
osteoclastogenesis in ovariectomy-induced bone loss. Mediators
Inflamm. 2025:57153322025. View Article : Google Scholar
|
|
76
|
Oranger A, Zerlotin R, Buccoliero C,
Sanesi L, Storlino G, Schipani E, Kozloff KM, Mori G, Colaianni G,
Colucci S and Grano M: Irisin modulates inflammatory, angiogenic,
and osteogenic factors during fracture healing. Int J Mol Sci.
24:18092023. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Kan T, He Z, Du J, Xu M, Cui J, Han X,
Tong D, Li H, Yan M and Yu Z: Irisin promotes fracture healing by
improving osteogenesis and angiogenesis. J Orthop Translat.
37:37–45. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Shang X, Hao X, Hou W, Liu J, Chi R, Deng
X, Pan C and Xu T: Exercise-induced modulation of myokine irisin on
muscle-bone unit in the rat model of post-traumatic osteoarthritis.
J Orthop Surg Res. 19:492024. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Açan AE, Aydın ME, Bulmuş Ö, Özcan E,
Karakılıç A, Turan G and Hüsemoğlu RB: Irisin and its role in
fracture healing: A comparative study with hyaluronic acid and
platelet-rich plasma in a rat model. Jt Dis Relat Surg. 36:328–339.
2025. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Sun L, Kuang S, Wang C, Li Y, Wang G, Sun
J, Zhou F and Zhang C: IL-6 blockade at the fracture site
accelerates bone healing via inflammatory modulation of sensory
nerve CGRP signaling. Int Immunopharmacol. 173:1162582026.
View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Nácher-Juan J, Terencio MC, Alcaraz MJ and
Ferrándiz ML: Osteostatin inhibits collagen-induced arthritis by
regulation of immune activation, pro-inflammatory cytokines, and
osteoclastogenesis. Int J Mol Sci. 20:38452019. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Singhal V, Ackerman KE, Bose A, Flores
LPT, Lee H and Misra M: Impact of route of estrogen administration
on bone turnover markers in oligoamenorrheic athletes and its
mediators. J Clin Endocrinol Metab. 104:1449–1458. 2019. View Article : Google Scholar :
|
|
83
|
Chew J, Tay L, Lim JP, Leung BP, Yeo A,
Yew S, Ding YY and Lim WS: Serum myostatin and IGF-1 as
gender-specific biomarkers of frailty and low muscle mass in
community-dwelling older adults. J Nutr Health Aging. 23:979–986.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Weaver SR, Doolittle ML, Durdan MM, Narum
AK, Weivoda MM, Alhamad DW, McGee-Lawrence ME, Khosla S, Taylor EL,
Bradley EW, et al: Global but not myeloid lineage-directed Girk3
deletion increases bone mass in female mice. JBMR Plus.
9:ziaf1332025. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Sato R, Vatic M, da Fonseca GWP and von
Haehling S: Sarcopenia and frailty in heart failure: Is there a
biomarker signature? Curr Heart Fail Rep. 19:400–411. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Gonçalves J and Caliceti P: Optimizing
pharmacological and immunological properties of therapeutic
proteins through PEGylation: Investigating key parameters and their
impact. Drug Des Devel Ther. 18:5041–5062. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Marsh MC and Owen SC: Therapeutic fusion
proteins. AAPS J. 26:32023. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Mendonca SR, Bangera PD, Keerikkadu M,
Tippavajhala VK and Rathnanand M: Multifunctional engineering of
exosomes for precision therapeutics: Strategies for targeted
delivery, barrier evasion, and clinical translation. Pharm Res.
42:1931–1952. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Hua C and Qiu L: Polymersomes for
therapeutic protein and peptide delivery: Towards better loading
properties. Int J Nanomedicine. 19:2317–2340. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Cheng Y, Ma J and Bo S: Short- and
long-term effects of concurrent aerobic and resistance training on
circulating irisin levels in overweight or obese individuals: A
systematic review and meta-analysis of randomized controlled
trials. PeerJ. 12:e179582024. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Engin A: Endothelial dysfunction in
obesity and therapeutic targets. Adv Exp Med Biol. 1460:489–538.
2024. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Adilakshmi P, Suganthi V, Balu Mahendran
K, Satyanarayana Rao K and Savithri B: Exercise-induced alterations
in irisin and osteocalcin levels: A comparative analysis across
different training modalities. Cureus. 16:e597042024.PubMed/NCBI
|
|
93
|
Bettariga F, Taaffe DR, Galvão DA, Lopez
P, Bishop C, Markarian AM, Natalucci V, Kim JS and Newton RU:
Exercise training mode effects on myokine expression in healthy
adults: A systematic review with meta-analysis. J Sport Health Sci.
13:764–779. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
He A, Wang S, Bao T, Rong S, Li C, Luo M,
He C, Yang Y and Xia Y: Exercise-induced metabolic reprogramming
and immune modulation: A novel strategy for cancer therapy. Exerc
Immunol Rev. 31:43–66. 2025.PubMed/NCBI
|
|
95
|
Shen X, Chen Y, Zhang J, Yang M, Huang L,
Luo J and Xu L: The association between circulating irisin levels
and osteoporosis in women: A systematic review and meta-analysis of
observational studies. Front Endocrinol (Lausanne). 15:13887172024.
View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Song R, Zhao X, Zhang DQ, Wang R and Feng
Y: Lower levels of irisin in patients with type 2 diabetes
mellitus: A meta-analysis. Diabetes Res Clin Pract. 175:1087882021.
View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Deng Y, Shen Y, Wu Y, Wen M and Wang F:
Correlation of serum irisin levels with diabetic nephropathy: An
exhaustive systematic appraisal and meta-analytical investigation.
Front Endocrinol (Lausanne). 16:15994232025. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Alexopoulos T, Vasilieva L, Kontogianni
MD, Tenta R, Georgiou A, Stroumpouli E, Mani I and Alexopoulou A:
Myostatin in combination with creatine phosphokinase or albumin may
differentiate patients with cirrhosis and sarcopenia. Am J Physiol
Gastrointest Liver Physiol. 321:G543–G551. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Bataille S, Chauveau P, Fouque D, Aparicio
M and Koppe L: Myostatin and muscle atrophy during chronic kidney
disease. Nephrol Dial Transplant. 36:1986–1993. 2021. View Article : Google Scholar
|
|
100
|
Orioli L, Samaras S, Sawadogo K, de Barsy
M, Lause P, Deswysen Y, Navez B, Thissen JP and Loumaye A:
Circulating myostatin as a biomarker of muscle mass and strength in
individuals with cancer or obesity. Clin Nutr. 43:1800–1808. 2024.
View Article : Google Scholar : PubMed/NCBI
|
|
101
|
LeDrew M, Sadri P, Peil A and Farahnak Z:
Muscle biomarkers as molecular signatures for early detection and
monitoring of muscle health in aging. Nutrients. 17:27582025.
View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Choi SJ, Lee MS, Kang DH, Ko GJ, Lim HS,
Yu BC, Park MY, Kim JK, Kim CH, Hwang SD, et al:
Myostatin/appendicular skeletal muscle mass (ASM) ratio, not
myostatin, is associated with low handgrip strength in
community-dwelling older women. Int J Environ Res Public Health.
18:73442021. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Gil TH, Kim JY, Shin JW, Jang DH, Park SS,
Kim SW, Shin CS, Jeon OH and Kong SH: Plasma biomarkers for
monitoring muscle function and physical performance decline in
older adults: A 2-year longitudinal study. J Nutr Health Aging.
29:1006072025. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Kim JY, Gil TH, Lee HG, Shin JW, Jang DH,
Kim HS, Park SS, Kim SW, Shin CS, Kong SH and Jeon OH: Plasma
extracellular vesicles biomarkers linked to lower muscle mass,
function and physical performance in sarcopenia. J Cachexia
Sarcopenia Muscle. 16:e137842025. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Ke Y, Pan Y, Huang X, Bai X, Liu X, Zhang
M, Jiang T and Zhang G: Correlations between circulating adipokines
and hepatocellular carcinoma: A systematic review and
meta-analysis. Front Endocrinol (Lausanne). 16:15489242025.
View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Zhang L, Peng Y, Kong Y, Zhang X, Li Z and
Jia H: Circulating irisin levels in patients with sarcopenia: A
systematic review and meta-analysis. Eur Geriatr Med. 16:5–13.
2025. View Article : Google Scholar
|
|
107
|
Roberts BC, Arredondo Carrera HM,
Zanjani-Pour S, Boudiffa M, Wang N, Gartland A and Dall'Ara E:
PTH(1-34) treatment andor mechanical loading have different
osteogenic effects on the trabecular and cortical bone in the
ovariectomized C57BL/6 mouse. Sci Rep. 10:88892020. View Article : Google Scholar
|
|
108
|
Sathe AG, Othman AA and Mohamed MF:
Therapeutic protein drug interaction potential in subjects with
psoriasis: An assessment based on population pharmacokinetic
analyses of sensitive cytochrome P450 probe substrates. J Clin
Pharmacol. 61:307–318. 2021. View Article : Google Scholar
|
|
109
|
Lori MS, Ohadi M, Estabragh MAR,
Afsharipour S, Banat IM and Dehghannoudeh G: pH-sensitive
polymer-based carriers as a useful approach for oral delivery of
therapeutic protein: A review. Protein Pept Lett. 28:1230–1237.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Gopal K, Mahmood S, Sofian ZM, Hilles AR
and Hashim NM: Microneedle innovations in oral therapeutics:
Transforming protein and peptide delivery. AAPS PharmSciTech.
26:1462025. View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Danielsen M, Hempel C, Andresen TL and
Urquhart AJ: Biopharmaceutical nanoclusters: Towards the
self-delivery of protein and peptide therapeutics. J Control
Release. 347:282–307. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Tien S and Kayser V: Ionic liquids as
stabilisers of therapeutic protein formulations: A review of
insulin and monoclonal antibodies. Biophys Rev. 17:89–101. 2024.
View Article : Google Scholar
|
|
113
|
Galle PR, Reck M, Pinato DJ,
Garcia-Campelo R, Finn RS, Cousin S, Zanghi J, Bernaards CA,
Swanson SJ, Morris S, et al: Interpreting immunogenicity in
oncology clinical trials. Cancer Treat Rev. 140:1030162025.
View Article : Google Scholar : PubMed/NCBI
|
|
114
|
Jiang M, Gao Y and Huang L: Circulating
adipokines in girls with central precocious puberty: A systematic
review and meta-analysis. Pediatr Res. 99:68–76. 2026. View Article : Google Scholar
|
|
115
|
Du J, Chang M, Jiang K, Su L, Yang H, Li K
and Ni C: Identification of therapeutic targets for osteoporosis
through multiomics integration and the potential dual role of
androgen receptor signaling in its pathophysiology. J Chem Inf
Model. 65:8833–8845. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
116
|
Cui X, Yu Z, Wang D, Liu Y, Wang W, Teng
H, Yu M, Wang S, Liu H and Wei W: Integrative multi-omics
deciphering of Gu Shu Kang Granules: A comprehensive systems
biology approach to unraveling molecular mechanisms in
sarcopenia-osteoporosis intervention. Endocr Metab Immune Disord
Drug Targets. Nov 26–2025.Epub ahead of print. View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Liu DY, Shen H, Greenbaum J, Yi QR, Liang
S, Zhang Y, Liu JC, Qiu C, Zhao LJ, Tian Q, et al: Repurposing
acebutolol for osteoporosis treatment: Insights from multi-omics
and multi-modal data analysis. Clin Pharmacol Ther. 118:1463–1476.
2025. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Yang J, Yang H, Wang F, Dai Y, Deng Y, Shi
K, Zhu Z, Liu X, Ma X and Gao Y: Bioinformatics identification
based on causal association inference using multi-omics reveals the
underlying mechanism of Gui-Zhi-Shao-Yao-Zhi-Mu decoction in
modulating rheumatoid arthritis. Phytomedicine. 136:1563322025.
View Article : Google Scholar
|
|
119
|
Wang Y, Wang Q, Xu Q, Li J and Zhao F:
Single-cell RNA sequencing analysis dissected the osteo-immunology
microenvironment and revealed key regulators in osteoporosis. Int
Immunopharmacol. 113:1093022022. View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Xiao X, Juan C, Drennon T, Uytingco CR,
Vishlaghi N, Sokolowskei D, Xu L, Levi B, Sammarco MC and Tower RJ:
Spatial transcriptomic interrogation of the murine bone marrow
signaling landscape. Bone Res. 11:592023. View Article : Google Scholar : PubMed/NCBI
|
|
121
|
Deng HW, Qiu C, Li Y, Gong Y, Lin W,
Afolabi B, Thumbigere-Math V, Su KJ, Deng J, Gnanesh SSM, et al:
Decoding cellular communication networks and signaling pathways in
bone, skeletal muscle, and bone-muscle crosstalk through spatial
transcriptomics. Res Sq [Preprint]. rs.3.rs-67011212025.PubMed/NCBI
|
|
122
|
Giza S, Mojica-Santiago JA, Parafati M,
Malany LK, Platt D, Schmidt CE, Coen PM and Malany S:
Microphysiological system for studying contractile differences in
young, active, and old, sedentary adult derived skeletal muscle
cells. Aging Cell. 21:e136502022. View Article : Google Scholar : PubMed/NCBI
|
|
123
|
Rose N, Estrada Chavez B, Sonam S, Nguyen
T, Grenci G, Bigot A, Muchir A, Ladoux B, Cadot B, Le Grand F and
Trichet L: Bioengineering a miniaturized in vitro 3D myotube
contraction monitoring chip to model muscular dystrophies.
Biomaterials. 293:1219352023. View Article : Google Scholar
|
|
124
|
Yin H, Zhang J, Zhou J, Yang HY, Wang J,
Wang Y, Liu N and Yue T: Muscle regeneration on a chip:
Exercise-induced microtrauma and optimal mechanical stimulation
regimen. Lab Chip. 26:1980–1995. 2026. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Parafati M, Thwin Z, Malany LK, Coen PM
and Malany S: Microgravity accelerates skeletal muscle
degeneration: Functional and transcriptomic insights from an ISS
muscle lab-on-chip model. Stem Cell Reports. 20:1025502025.
View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Zhou K, Luo S, Wang Q and Fang S: The
shared biomarkers and immune landscape in psoriatic arthritis and
rheumatoid arthritis: Findings based on bioinformatics, machine
learning and single-cell analysis. PLoS One. 19:e03133442024.
View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Gui G, Bingham MA, Herzog JR, Wong-Rolle
A, Dillon LW, Goswami M, Martin E, Reeves J, Kim S, Bahrami A, et
al: Single-cell spatial transcriptomics reveals
immunotherapy-driven bone marrow niche remodeling in AML. Sci Adv.
11:eadw48712025. View Article : Google Scholar : PubMed/NCBI
|
|
128
|
Zhang Y, Wei J, Kong L, Song M, Zhang Y,
Xiao X, Cao H and Jin Y: Network pharmacology, molecular docking
and bioinformatics reveal the mechanism of Tripterygii Wilfordii
against osteosarcoma. Medicine (Baltimore). 101:e323892022.
View Article : Google Scholar
|