Introduction
The standard method of treatment for patients with
locally invasive bladder cancer is still a total cystectomy, which
decrease the quality of life due to the urinary diversion and
postoperative impotence. Reconstruction of the bladder using tissue
from the intestinal tract has been applied in some cases and total
cystectomy with nerve conservation in order to avoid postoperative
impotence has been reported (1).
However, these techniques require a long operation time and are
invasive and are therefore not indicated for many patients because
most cases of bladder cancer occur in individuals in their 60s–70s.
In addition, the 5-year survival rates of patients with pT2, pT3a,
pT3b and pT4 bladder cancer are 63–83, 50–69, 15–29 and 21–22%,
respectively (2). Approximately
50% of all patients with T2-T4 invasive bladder cancer die within 5
years despite of the decrease in QOL (3–10).
Trimodality therapy involving radical transurethral
resection, chemotherapy and radiation therapy has long been
attempted as an alternative approach for patients who require
cystectomy. The Radiation Therapy Oncology Group (RTOG) has
completed six prospective protocols entering 415 patients with
T2-T4a muscle-invasive bladder cancer who were candidates for
cystectomy. However, none of the protocols achieved a 5-year
survival rate of >60% (11–17).
Moreover, the 5-year bladder intact survival rates were <50% in
most of studies (16–19). Improvement of the survival rate
with bladder preservation may require a new method, which allows to
deliver a higher dosage of anticancer agent specifically into the
tumor, without causing systemic side effects.
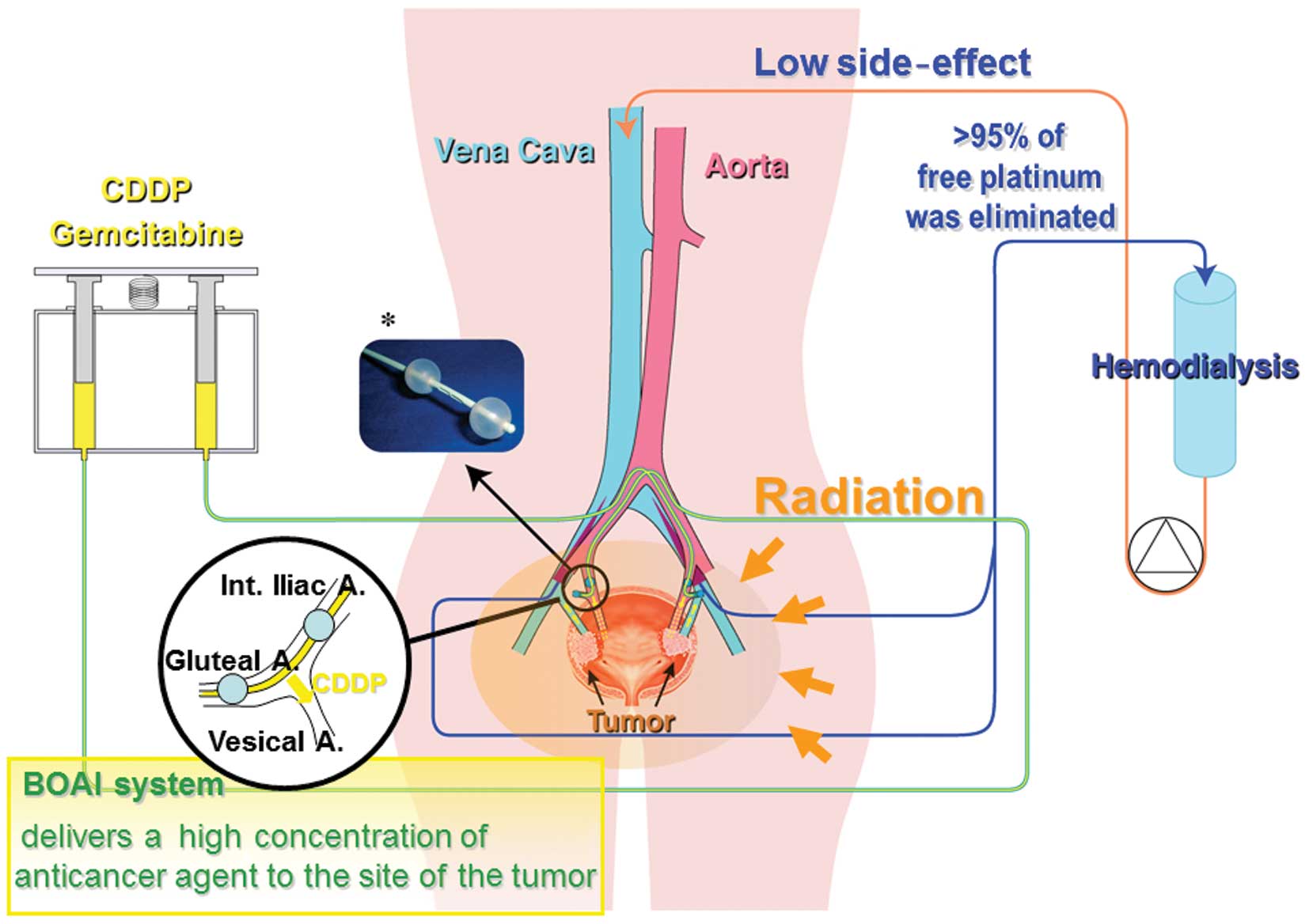
We have therefore developed a novel bladder
preservation therapy [referred to hereafter as the OMC (Osaka
Medical College) regimen] involving balloon-occluded arterial
infusion (BOAI) of an anticancer agent and concurrent hemodialysis
(HD). This allows the anticancer agent to accumulate at a high
concentration at the site of the tumor while ensuring that the
systemic concentration remains low and this is then followed by
radiation therapy.
We previously reported that >90% of patients
(70/77) with locally advanced urothelial bladder cancer who were
treated in this way achieved CR, of whom 97% (68/70) did not
develop recurrent disease or metastasis within a mean follow-up
period of 164 weeks [range, 11–805 weeks; 1st to 3rd quartile (Qu)
= 66–195] after completion of therapy. In contrast to the high CR
induction ratio in patients with locally invasive tumors, more than
half of patients with lymph node involvement, stage T4 tumors
and/or node involovement failed to achieve CR after the
treatment.
To date, the number of patients who have received
OMC-regimen is 221, including 162 patients with organ confined
(including T3b) urothelial cancer tumors. In this study we report
the outcomes of the patients with organ confined (including T3b)
urothelial cancer tumors treated with OMC-regimen in comparison
with total cystectomy (n=139).
Patients and methods
Eligibility criteria
Eligible patients had histologically confirmed CIS,
or stage T2, or T3 muscle-invasive bladder cancer without distant
metastasis. Imaging studies, including chest computed tomography
(CT) scan, abdominal/pelvic magnetic resonance imaging (MRI) and CT
scan and bone scintigraphy were performed before the start of
therapy. All patients who received the OMC-regimen had an absolute
neutrophil count (ANC) of 1,500/μl, platelet count
100,000/μl, creatinine 3.0 mg/dl, a bilirubin level 3 times
the institutional upper limit of the normal range, an AST level 4
times the institutional upper limit of the normal range, an Eastern
Cooperative Oncology Group (ECOG) performance status of 0–2 and no
prior radiotherapy or systemic therapy for bladder cancer. The
study was reviewed and approved by the institutional review board
of Osaka Medical College. Patients were informed of the
investigational nature of the study and provided written informed
consent before study enrollment.
Study design and treatment
Before study entry, patients underwent transurethral
resection of the bladder tumor (TURBT) to establish the diagnosis.
We primarily recommended total cystectomy when surgery was
feasible. However, the OMC-regimen was offered as another treatment
option whenever total cystectomy was not feasible because of
advanced age, performance status or other reasons including
patients’ request. Patients were assigned to receive the
OMC-regimen at 4–5 weeks after TURBT to allow adequate healing.
Assessability, toxicity and response
criteria
Pretreatment evaluation included a complete history
and physical examination, performance status assessment, complete
differential blood cell count, electrolytes, blood urea nitrogen,
serum creatinine, liver function parameters and appropriate imaging
studies to assess the extent of disease. During treatment, patients
were seen weekly at our department, when their weight was recorded
and toxicity was monitored using the National Cancer Institute’s
Common Terminology Criteria for adverse events v4.0 (CTCAE). At 10
weeks, patients underwent repeat transurethral resection of the
site of the original tumor, ultra-sound-guided whole-layer biopsy
and urine cytology, as well as MRI and CT scan of the pelvis and
were evaluated for their response to this therapy. CR was defined
as complete disappearance of all measurable and evaluable disease.
Duration of response was defined as the period from documentation
of the response until evidence of disease recurrence. Survival was
the period from study entry until patient death. Patients who
achieved CR were observed using our follow-up protocol. However,
any evidence of residual tumor in the bladder was deemed as
treatment failure and such patients were primarily advised to
undergo total cystectomy when possible, but otherwise to undergo
secondary BOAI with a higher dosage of cisplatin or gemcitabine
(1600 mg), as a salvage therapy. Patients who were found to have
only a superficial amount of remaining tumor underwent intravesical
injection of bacillus Calmette Guerin (BCG).
Follow-up
All patients were followed-up on the basis of
monthly urine cytology, together with cystoscopy, biopsy and
imaging studies, every three months for 2 years, including chest CT
scan, abdominal/pelvic MRI and CT scan and bone scintigraphy and
thereafter at 6-month intervals.
Statistics
Simple as well as multiple regression analyses were
conducted to evaluate the significance of the following variables
as risk factors of treatment failure: age, sex, patient performance
status, tumor stage and tumor size and significance of complete
resection of tumor and hydronephrosis due to tumors were also
evaluated. The life table probabilities of overall survival and
progression-free survival were determined using Kaplan-Meier
analysis and log-rank test. The Cox proportional hazards regression
analysis was conducted to assess the associations of each factor as
described above. Differences at P<0.05 were considered to be
statistically significant.
Results
Patient characteristics
Between 1988 and 2013, 162 (126 males and 36
females) were treated with the OMC-regimen and 139 (116 males and
23 females) underwent radical cystectomy. The characteristics of
the patients in these two treatment groups are shown in Table I. For preoperative clinical
staging, we used a simplified form of the 2002 TNM classification
to stage bladder tumors (20). To
make a valid comparison, preoperative clinical staging and not the
pathologic stage after cystectomy was used to compare the two
treatment groups, thus avoiding stage migration that may occur
after pathologic staging (21).
 | Table I.Patient characteristics of both
groups. |
Table I.
Patient characteristics of both
groups.
| Characteristic | OMC-regimen | Total cystectomy | P-value |
|---|
| Age | | | |
| Median (range
years) | 70 (39–91) | 65 (44–89) | 0.0015 |
| Sex | | | |
| Male (%) | 126 (77.8%) | 116 (83.5%) | NS |
| Female (%) | 36 (22.2%) | 23 (16.5%) | |
| ECOG performance
status | | | |
| 0 | 103 (63.6%) | 90 (64.7%) | NS |
| 1 | 46 (28.4%) | 42 (30.2%) | NS |
| 2 | 13 (8.0%) | 7 (5.1%) | NS |
| Clinical stage | | | |
| T-stage | | | |
| Cis | 12 (7.4%) | 11 (7.9%) | NS |
| T2 | 91 (56.2%) | 75 (54.0%) | NS |
| T3 | 59 (36.4%) | 53 (38.1%) | NS |
Treatment details
OMC-regimen group
Patients assigned to the OMC-regimen group underwent
transurethral resection of the bladder tumor (TURBT) at our
institution to establish the diagnosis. They were then scheduled to
receive the OMC-regimen 4–5 weeks after TURBT to allow adequate
healing. We administered 100, 200, or 300 mg of cisplatin as a
single bolus, basically according to the criteria described in
Table II.
| Table II.Criteria for the administration of
cisplatin. |
Table II.
Criteria for the administration of
cisplatin.
| In the initially
enrolled 11 patients | |
| 100 mg | Renal function (sCr
>1.3) or age (≥75 years) |
| 200 mg | Renal function
(sCr<1.3) with [age (60–74 years) and T-stage (T2 or T3)] |
| 300 mg | Renal function
(sCr<1.3) with [age (<60 years ) or T-stage: T4] |
| In the latest 151
patients | |
| 100 mg | All patients |
For the intra-arterial infusion procedure, we used
an intra-arterial catheter equipped with two occlusion balloons
(size: 6 Fr, M6F-28-70-TBSB4-ST, Clinical Supply, Tokyo, Japan).
The catheter was introduced into the posterior trunk of the
internal iliac artery through the femoral arterial approach and
after the distal balloon had passed through the furcation of the
anterior trunk of the internal iliac artery, both the distal and
proximal balloons were inflated and immobilized, so that the
anterior trunk of the internal iliac artery, which lies upstream of
the target vessels (the vesical arteries) was isolated between the
balloons. At this time, using digital subtraction angiography
(DSA), it was confirmed that the injected agent did not enter the
superior gluteal artery and that there was no back-flow into the
internal iliac artery, while the tumor was markedly stained due to
active flow of injected contrast medium into the urinary bladder.
Fig. 1 illustrates the
extracorporeal circuit used in the treatment. Various amounts of
cisplatin (100, 200 or 300 mg) were locally infused through the
catheter over a 1-h period according to the criteria shown in
Table II. Simultaneously, HD was
performed via two double-lumen catheters (size: 12 Fr,
Argyle®, Tyco Healthcare, Tokyo, Japan) placed in the
bilateral common iliac veins for 2 h after the start of arterial
infusion. The catheters were connected to a hollow-fiber dialyzer
(APS150, Asahi, Tokyo, Japan) with a membrane area of 1.0–1.5
m2 according to the weight of each patient. The blood
flow rate was 180–250 ml/min and the hemodialysis-fluid flow rate
was 500 ml/min.
Radiation therapy was administered to the whole
pelvis using a CT-planned three-dimensional conformal technique to
a total of 60 Gy: 50 Gy (2 Gy/day × 25 days) followed by 10 Gy (2
Gy/day × 5 days) of local irradiation to the bladder. Patients were
treated with the bladder empty. The planned target volume for the
bladder included the gross target volume (bladder plus any
extravesical tumor) with a 1-cm expansion. At 6 weeks, patients
underwent repeat transurethral resection of the site of the
original tumor, ultrasound-guided whole-layer biopsy and urine
cytology, as well as MRI and CT scan of the pelvis and the response
to this therapy was then evaluated.
Radical cystectomy group
Among the 139 patients in the radical cystectomy
group, 47 underwent ileal conduit formation, 58 underwent
uretero-cutaneostomy, 19 and 7 patients underwent continent urinary
diversion with ileal-neobladder formation (Hartmann’s method) and
Indiana pouch respectively and the remaining 6 underwent
uretero-sigmoidostomy performed at the time of radical cystectomy.
Standard pelvic lymphadenectomy was performed in 123 patients, 6
patients underwent iliac sampling and 10 patients were not studied
in sufficient detail to allow assessment of the level of lymph node
dissection. As not all of the histology reports mentioned the
number of lymph nodes examined, it was not possible to precisely
evaluate the extent of dissection. There were no significant
differences in cause-specific or overall survival between the
patients who underwent nodal dissection and the patients who did
not. The urethrectomy was performed in 30 patients at the time of
radical cystectomy because of the presence of extensive carcinoma
in situ or multifocal bladder tumors.
Response to the OMC-regimen
Table III
summarizes the treatment response, duration of response and patient
characteristics, including sex, age, tumor stage, tumor size,
involvement of hydronephrosis, performance status and success or
failure of complete TURBT. Overall, 152 of the 162 patients (93.8%)
achieved a complete response as defined by the absence of
persistent disease revealed by cystoscopy, biopsy and urine
cytology after therapy. More than 96% (146/152) of patients with CR
were able to retain their urinary bladder with no evidence of
recurrent disease or distant metastasis within a mean follow-up
period of 168 weeks (range, 24–960 weeks; 1st to 3rd Qu = 54–234
weeks) from the completion of therapy. The univariate as well as
multivariate regression analyses revealed that a hydronephrosis is
the only risk factor for treatment failure, while tumor stage,
tumor size and failure of complete resection of tumor, those
usually have been reported as risk factors for treatment failure of
bladder preservation therapy, were not selected (Table IV).
| Table III.Response at 3 months after treatment
and current outcome. |
Table III.
Response at 3 months after treatment
and current outcome.
| CR
| PR
| SD
| PD
|
| No. | % | 95% CI | No. | % | 95% CI | No. | % | 95% CI | No. | % | 95% CI |
|
| Total no. of
patients | 152 | 93.8 | 88.9–97.0 | 7 | 4.32 | 1.75–8.70 | 1 | 0.62 | 0.16–3.39 | 2 | 1.23 | 0.15–4.39 |
| Duration of
response | | | | | | | | | | | | |
| Mean, range
(weeks) | | 165, 23–960 | | | 99, 27–228 | | | 15 | | | 0 | |
| 1st, 3rd QU
(weeks) | | 53, 232 | | | 51, 118 | | | 15 | | | 0 | |
| Recurrence | 6 | 3.95 | 1.46–8.39 | 3 | 42.9 | 9.90–81.6 | 1 | 100 | 2.5–100 | | | |
| Death | 8 | 5.26 | 2.30–10.1 | 3 | 42.9 | 9.90–81.6 | 1 | 100 | 2.5–100 | 2 | 100 | 15.8–100 |
| Age (mean, range)
(years) | | 69, 39–91 | | | 71, 62–78 | | | 81 | | | 70, 62–77 | |
| Sex | | | | | | | | | | | | |
| Male | 120 | 78.9 | 71.6–85.1 | 4 | 57.1 | 18.4–90.1 | 0 | 0 | 0–97.5 | 2 | 100 | 15.8–100 |
| Female | 32 | 21.1 | 14.9–28.4 | 3 | 42.9 | 9.90–81.6 | 1 | 100 | 2.5–100 | 0 | 0 | 0–84.2 |
|
| Categories | No. | % | 95% CI | No. | % | 95% CI | No. | % | 95% CI | No. | % | 95% CI |
|
| T stage | | | | | | | | | | | | |
| Tis | 12 | 7.89 | 4.15–13.4 | 0 | 0 | 0–41.0 | 0 | 0 | 0–97.5 | 0 | 0 | 0–84.2 |
| 2 | 88 | 57.9 | 49.6–65.8 | 2 | 28.6 | 3.67–71.0 | 0 | 0 | 0–97.5 | 1 | 50 | 1.26–98.7 |
| 3 | 52 | 34.2 | 26.7–42.3 | 5 | 71.4 | 29.0–96.3 | 1 | 100 | 2.5–100 | 1 | 50 | 1.26–98.7 |
| Tumor size
(cm) | | | | | | | | | | | | |
| <3 | 73 | 48.0 | 39.9–56.3 | 3 | 42.9 | 9.90–81.6 | 0 | 0 | 0–97.5 | 2 | 100 | 15.8–100 |
| 3–5 | 76 | 50.0 | 41.8–58.2 | 3 | 42.9 | 9.90–81.6 | 1 | 100 | 2.5–100 | 0 | 0 | 0–84.2 |
| >5 | 3 | 2.0 | 0.41–5.66 | 1 | 14.2 | 0.36–57.9 | 0 | 0 | 0–97.5 | 0 | 0 | 0–84.2 |
| Hydro | | | | | | | | | | | | |
| (+) | 9 | 5.9 | 2.74–10.9 | 3 | 42.9 | 9.90–81.6 | 1 | 100 | 2.5–100 | 1 | 50 | 1.26–98.7 |
| (−) | 143 | 94.1 | 89.1–97.3 | 4 | 57.1 | 18.4–90.1 | 0 | 0 | 0–97.5 | 1 | 50 | 1.26–98.7 |
| Comp-TUR | | | | | | | | | | | | |
| (+) | 107 | 70.4 | 62.5–77.5 | 3 | 42.9 | 9.90–81.6 | 0 | 0 | 0–97.5 | 2 | 100 | 15.8–100 |
| (−) | 45 | 29.6 | 22.5–37.5 | 4 | 57.1 | 18.4–90.1 | 1 | 100 | 2.5–100 | 0 | 0 | 0–84.2 |
| PS | | | | | | | | | | | | |
| 0 | 99 | 65.1 | 57.0–72.7 | 3 | 42.9 | 9.90–81.6 | 0 | 0 | 0–97.5 | 1 | 50 | 1.26–98.7 |
| 1 | 40 | 26.3 | 19.5–34.1 | 4 | 57.1 | 18.4–90.1 | 1 | 100 | 2.5–100 | 1 | 50 | 1.26–98.7 |
| 2 | 13 | 8.6 | 4.63–14.2 | 0 | 0 | 0–41.0 | 0 | 0 | 0–97.5 | 0 | 0 | 0–84.2 |
| Table IV.Risk factors for treatment failure in
the OMC-regimen group. |
Table IV.
Risk factors for treatment failure in
the OMC-regimen group.
| Category | Univariate
| Multivariate
|
|---|
| Odds ratio | P-value | Odds ratio | P-value |
|---|
| Hydronephrosis | (+) vs. (−) | 15.87 | 0.0001 | 71.43 | 0.0013 |
| T-stage (Tis) | Cis vs. T2 | 1969 | 0.9753 | NV | NV |
| T-stage (T3) | T3 vs. T2 | 3.953 | 0.0537 | NV | NV |
| Tumor size | >3 cm vs. <3
cm | 1.082 | 0.9037 | 1.823 | 0.1322 |
| Tumor size | >5 cm vs. <5
cm | 5.325 | 0.1562 | 7.576 | 0.5583 |
| Tumor number | Cont. variable | 1.175 | 0.6717 | 2.785 | 0.2967 |
| Complete TUR | Yes vs. no | 2.378 | 0.1873 | 1.359 | 0.5118 |
| Performance
status | 2 vs. 0–1 | 10598 | 0.9726 | 207067 | 0.9964 |
| Sex | Male vs.
female | 2.500 | 0.1749 | 2.809 | 0.2401 |
| Age | Cont. variable | 1.034 | 0.3286 | 1.062 | 0.1985 |
Comparison of patient survival between
the two groups
Overall survival (OS)
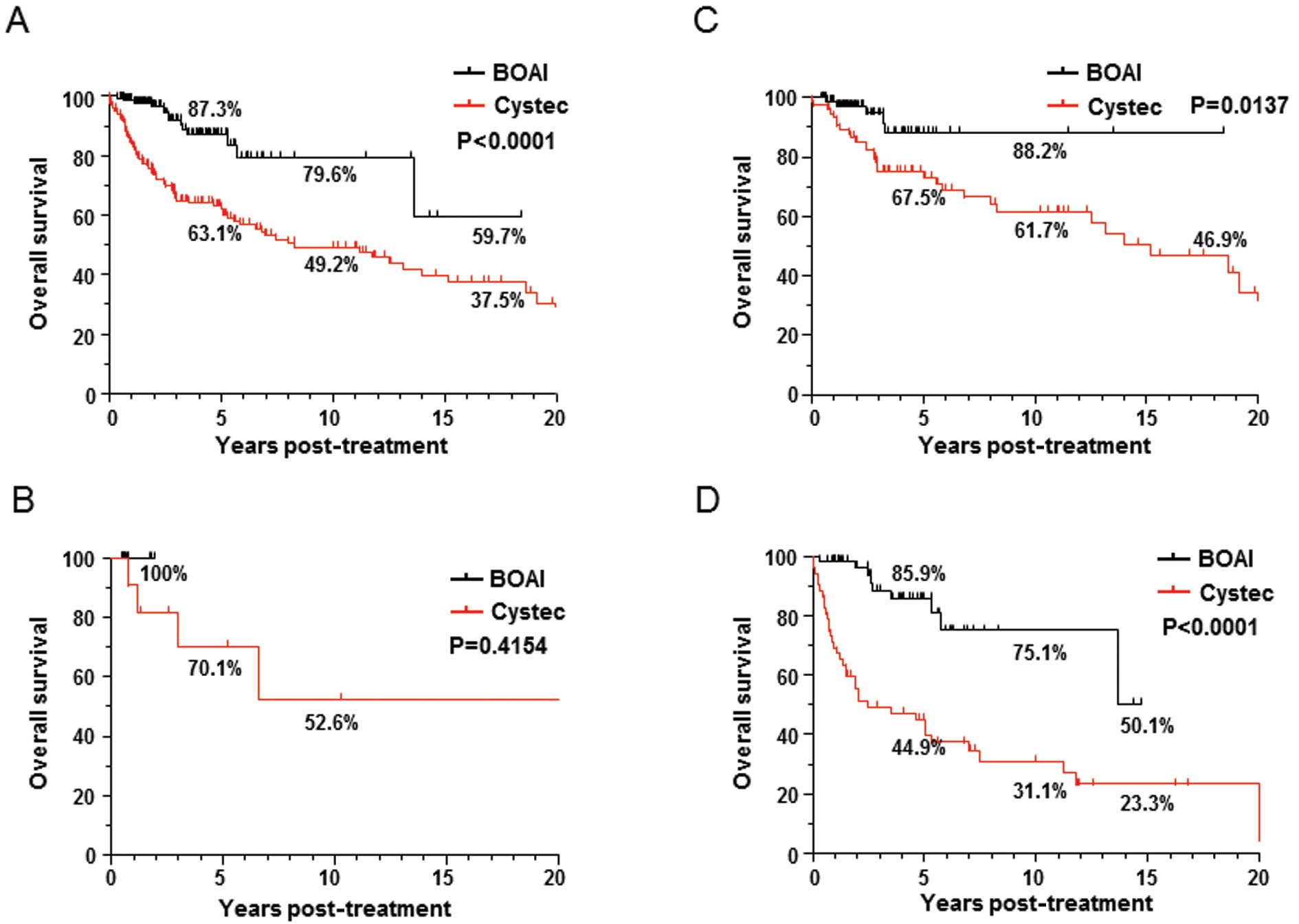
Overall survival ratio was significantly better in
the OMC-regimen group than in the cystectomy group in all patients,
the 5- and 15-year survival rates were 87.3 and 79.6 vs. 63.1 and
49.2%, respectively; log-rank test, p<0.0001, Fig. 2A). Fig. 2B–D show OS ratio of patients in
each T-stage of CIS, T2 and T3 respectively. The OS ratio in
patients with T2 as well as T3 tumors was significantly better in
the OMC-regimen group, although statistically significance has not
seen in patients in with CIS (despite of 100% of PFS), because of
short follow-up period (Fig.
3).
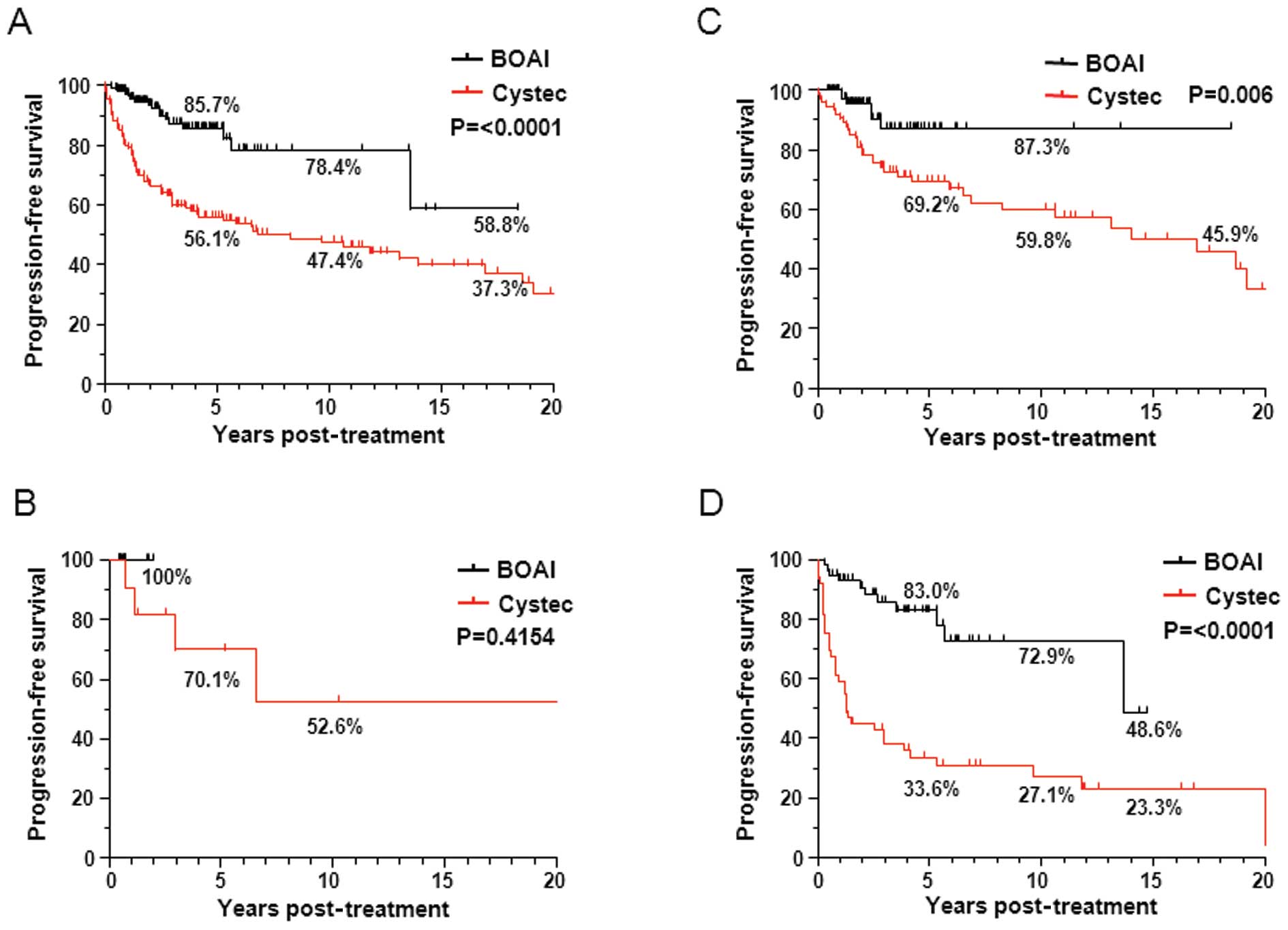
Progresion-free survival (PFS)
The progression-free survival ratio was also
significantly better in the OMC-regimen group in total patients, as
well as in each patient with T2 and T3 tumors. In all patients,
>85 and 78% of patients survive with their functioning bladder
at 5 and 10 years, respectively; this is the most important issue
for the bladder preservation therapy.
Predictors of patient survival
selected using univariate and multivariate Cox regression analyses
in OMC-regimen group
We investigated the significance of each factor,
including sex, age, tumor stage, tumor size, involvement of
hydronephrosis, performance status and success or failure of
complete TURBT as a predictor of overall survival and
progression-free survival using the Cox regression model. As shown
in Table V, univariate Cox
regression analysis as well as multivariate Cox regression analysis
selected only the hydronephrosis as a significant factor affecting
both progression-free and overall survival, while tumor stage,
tumor size and failure of complete resection of tumor were not
selected.
| Table V.Predictors of overall survival (A)
and progression-free survival (B) in the OMC-regimen group
evaluated by univariate and multivariate Cox regression
analyses. |
Table V.
Predictors of overall survival (A)
and progression-free survival (B) in the OMC-regimen group
evaluated by univariate and multivariate Cox regression
analyses.
A, Overall survival
|
|---|
| Category | Univariate
| Multivariate
|
|---|
| Odds ratio | P-value | Odds ratio | P-value |
|---|
| Hydronephrosis | (+) vs. (−) | 14.29 | < 0.0001 | 21.74 | 0.0004 |
| T-stage | T3 vs. T2 | 1.570 | 0.4282 | NV | NV |
| Tumor size | >3 cm vs. <3
cm | 1.382 | 0.5991 | 2.976 | 0.2989 |
| Tumor size | >5 cm vs. <5
cm | 5.208 | 0.0194 | 4.785 | 0.1159 |
| Tumor number | Cont. variable | 1.020 | 0.9534 | 1.135 | 0.7229 |
| Complete TUR | Yes vs. no | 1.668 | 0.3954 | 1.287 | 0.7846 |
| Performance
status | 2 vs. 0–1 | 1.026 | 0.9805 | 1.299 | 0.8361 |
| Sex | Male vs.
female | 2.129 | 0.1977 | 1.546 | 0.5300 |
| Age | Cont. variable | 1.012 | 0.7086 | 1.004 | 0.9224 |
B, Progression-free
survival
|
|---|
| Category | Univariate
| Multivariate
|
|---|
| Odds ratio | P-value | Odds ratio | P-value |
|---|
| Hydronephrosis | (+) vs. (−) | 9.524 | < 0.0001 | 13.51 | 0.0002 |
| T-stage | T3 vs. T2 | 1.838 | 0.2100 | NV | NV |
| Tumor size | >3 cm vs. <3
cm | 1.350 | 0.5566 | 1.709 | 0.4855 |
| Tumor size | >5 cm vs. <5
cm | 4.255 | 0.0551 | 2.545 | 0.3166 |
| Tumor number | Cont. variable | 1.051 | 0.8611 | 1.092 | 0.7685 |
| Complete TUR | Yes vs. no | 1.246 | 0.6604 | 1.166 | 0.8307 |
| Performance
status | 2 vs. 0–1 | 1.387 | 0.6650 | 2.232 | 0.3730 |
| Sex | Male vs.
female | 1.712 | 0.2899 | 1.362 | 0.6008 |
| Age | Cont. variable | 1.003 | 0.9159 | 1.007 | 0.8217 |
Toxicity
The observed toxicities are summarized in Table VI. It is noteworthy that none of
the patients had grade II or more severe blood/bone marrow and/or
gastrointestinal toxicities. Ten patients [6.17%, 95% confidence
interval (CI), 3.0–11.1%] experienced grade I blood/bone marrow
toxicity, 21 (13.0%, 95% CI, 8.21–19.1%) had gastrointestinal
toxicity and 6 (3.7%, 95% CI, 1.37–7.89%) had neuropathy. The
duration of blood/bone marrow toxicity, including granulocytopenia
and anemia, was relatively short: median duration was 5 days for
granulocytopenia (range 3–9 days) and 3 days for anemia (range 2–10
days). No patients received granulocyte colony-stimulating factor
or transfusion of red blood cells. Gastrointestinal toxicity
included anorexia in 16 patients, constipation in 7, diarrhea in 9,
nausea in 14 and vomiting in 2, but all symptoms disappeared within
6-days after intra-arterial infusion. One patient experienced grade
II neuropathy in the peroneal nerve area, but disappeared by the 12
months after the treatment. There were no other adverse reactions
such as renal failure, genitourinary toxicity, radiation cystitis
or life-threatening complications.
| Table VI.Toxicity. |
Table VI.
Toxicity.
| Toxicity | Grade
| Duration
|
|---|
| Grade 1 No.
(%) | Grade 2 No.
(%) | Grade 3–4 No.
(%) | <3 days No. | 3–7 days No. | >7 days No. |
|---|
| Blood/bone
marrow | | | | | | |
| Total | 10 (6.2) | 3 (1.9) | 0 | | | |
|
Granulocytopenia | 5 (3.1) | 0 | 0 | 0 | 5 (3.1) | 0 |
| Anemia | 7 (4.3) | 3 (1.9) | 0 | 3(1.9) | 4 (2.5) | 0 |
|
Gastrointestinal | | | | | | |
| Total | 21 (13.0) | 0 | 0 | | | |
| Anorexia | 16 (9.9) | 0 | 11 (6.8) | 5 (3.1) | 0 | |
| Constipation | 7 (4.3) | 0 | 0 | 6 (3.7) | 1 (0.6) | 0 |
| Diarrhea | 9 (5.6) | 0 | 0 | 4 (2.5) | 5 (3.1) | 0 |
| Nausea | 14 (8.6) | 0 | 0 | 9 (5.6) | 5 (3.1) | 0 |
| Vomiting | 2 (1.2) | 0 | 0 | 0 | 2 (1.2) | 0 |
| Neuropathy | 6 (3.7) | 1 (0.6) | 0 | 0 | 0 | 7 (4.3) |
Discussion
We have previously reported that the OMC-regimen
allowed >89% (69/77) of patients with locally invasive tumors to
achieve CR [>70% (70/96) of all patients including those with T4
and N(+) disease]. Most (68/69) of the CR patients were still alive
with no evidence of recurrence after a mean follow-up of 161 (range
12–805) weeks. The 5- and 15-year overall survival rates were 91.5
and 81.3% (vs. 59.8 and 40.1% for cystectomy, P<0.0001),
respectively. In contrast to the high CR induction ratio in
patients with locally invasive tumors, more than half of the
patients with lymph node involvement, stage T4 tumors and/or node
involovement failed to achieve CR after the treatment. Stage T4,
lymph node involvement and histological type (non-UC) were
independent statistically significant risk factors for treatment
failure as well as patient survival.
To date, the number of patients who have received
OMC-regimen is 221, including 162 patients with organ confined
(including T3b) urothelial cancer tumors and other patients with
histologically non-UC tumors and/or stage T4 tumors and/or node
involvement. In this study we focused on the patients with locally
invasive urothelial cancer and report the outcome. The treatment
allowed >93% of patients to achieve CR after the treatment. More
than 96% of the patients with CR have been able to retain their
bladder without recurrence or distant metastasis, with a mean
survival of 168 weeks. This supports our previous data, which
indicated that patients with locally invasive urothelial bladder
cancer are the best candidates for this therapy.
The most pertinent issue related to this therapy is
why it achieves better outcomes than cystectomy. Using a rat
BOAI-CDDP model, we are now investigating the mechanisms
responsible for the better outcomes achieved by the OMC-regimen in
comparison with total cystectomy. We have found that BOAI allows
delivery of an extremely high concentration of anticancer agent to
the bladder and surrounding pelvic region, as well as to the pelvic
and para-aortic lymphatic tissues (data not shown). Enhanced
radiosensitivity of the cancer cells due to the BOAI-induced high
concentration of cisplatin in the bladder, as well as in the
lymphatic tissues, may also have contributed significantly to the
good outcomes achieved. In addition, the severe hypoxia in the
target region resulting from BOAI may play a role in the marked
antitumor effect, as several basic studies have demonstrated that
hypoxia greatly enhances the effectiveness of cisplatin (22–24).
Future studies may help to clarify the key roles of BOAI, thus
contributing to further improvements of this therapy.
The other advantage of the OMC-regimen is a
significant reduction of systemic side effects. Cisplatin exerts
its antitumor activity via the non-protein-bound form, whose
concentration falls steeply after administration: its half-life is
normally <60 min and its concentration falls to below the
detection limit 4 h after administration (25,26).
The most important point of the OMC-regimen is the removal of
non-protein-bound Pt immediately after administration of cisplatin
by performing HD via the bilateral common iliac veins, thus
accomplishing efficient drainage of cisplatin immediately after
passage through the tumor. HD is specifically efficient for
cisplatin elimination, since the molecular weight of
protein-unbound cisplatin is ∼300, similar to that of creatinine.
Moreover, the anatomic structure and blood supply of the bladder
may largely account for the efficient drainage of cisplatin
achieved with this approach. As the urinary bladder is situated at
the base of the pelvis, the relatively close circuit formed by the
internal iliac artery, bladder and common iliac veins may
contribute to efficient drainage of the anticancer agent, thus
increasing the elimination efficiency without influencing the
systemic circulation. Indeed, we found that >95% of free Pt was
efficiently eliminated by HD during BOAI of cisplatin, thus
providing optimal conditions for effective local accumulation of Pt
in the tumor, with minimal systemic toxicity, allowing even a
91-year-old patient to complete the regimen.
Thus, the OMC-regimen, which delivers an extremely
high concentration of anticancer agent to the site of a tumor
without causing systemic adverse effects, can be regarded as a
curative therapy for elderly patients, not only those for whom
total cystectomy is indicated, but also those of whom total
cystectomy is not feasible because of age, performance status or
other reasons and who are considered physically incapable of
tolerating the chemotherapeutic regimens that are usually applied
clinically. It is noteworthy that this therapy will improve the
feasibility of radical cure without the need for cystectomy in
patients for whom such surgery would otherwise be necessary and
also facilitate potential cure in patients whose condition would
normally rule out this likelihood and for whom, otherwise, merely
palliative treatment would seem the only option.
Abbreviations:
|
BOAI
|
balloon-occluded arterial
infusion;
|
|
CIS
|
carcinoma in situ;
|
|
DSA
|
digital subtraction angiography;
|
|
HD
|
hemodialysis;
|
|
Qu
|
quartile;
|
|
RTOG
|
radiation therapy oncology group;
|
|
TURBT
|
transurethral resection of bladder
tumor;
|
|
UC
|
urothelial carcinoma
|
References
|
1.
|
Schlegel PN and Walsh PC: Neuroanatomical
approach to radical cystoprostatectomy with preservation of sexual
function. J Urol. 138:1402–1406. 1987.PubMed/NCBI
|
|
2.
|
Pagano F, Bassi P, Galetti TP, et al:
Results of contemporary radical cystectomy for invasive bladder
cancer: a clinicopathological study with an emphasis on the
inadequacy of the tumor, nodes and metastases classification. J
Urol. 145:45–50. 1991.
|
|
3.
|
Stenzl A, Cowan NC, De Santis M, et al:
Guidelines on bladder cancer: muscle-invasive and metastatic. Eur
Assoc Urol. 3:1–59. 2008.
|
|
4.
|
Hong S, Kwak C, Jeon H, Lee E and Lee S:
Do vascular, lymphatic, and perineural invasion have prognostic
implications for bladder cancer after radical cystectomy? Urology.
65:697–702. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Leissner J, Koeppen C and Wolf H:
Prognostic significance of vascular and perineural invasion in
urothelial bladder cancer treated with radical cystectomy. J Urol.
169:955–960. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Patton S, Hall M and Ozen H: Bladder
cancer. Curr Opin Oncol. 14:265–272. 2002. View Article : Google Scholar
|
|
7.
|
Shelley MD, Barber J and Wilt T: Surgery
versus radiotherapy for invasive bladder cancer. Cochrane Database
Syst Rev. CD002079. 2002.
|
|
8.
|
Stein JP, Lieskovsky G, Cote R, et al:
Radical cystectomy in the treatment of invasive bladder cancer:
Long-term results in 1,054 patients. J Clin Oncol. 19:666–675.
2001.PubMed/NCBI
|
|
9.
|
Dalbagni G, Genega E, Hashibe M, et al:
Cystectomy for bladder cancer: a contemporary series. J Urol.
165:1111–1116. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Frazier H, Robertson J, Dodge R and
Paulson D: The value of pathologic factors in predicting
cancer-specific survival among patients treated with radical
cystectomy for transitional cell carcinoma of the bladder and
prostate. Cancer. 71:3993–4001. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Tran E, Souhami L, Tanguay S and Rajan R:
Bladder conservation treatment in the elderly population: results
and prognostic factors of muscle-invasive bladder cancer. Am J Clin
Oncol. 32:333–337. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Weizer AZ, Joshi D, Daignault S, et al:
Performance status is a predictor of overall survival of elderly
patients with muscle invasive bladder cancer. J Urol.
177:1287–1293. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Hoshi S, Shintaku I, Suzuki K, et al:
Bladder preservation by internal iliac arterial infusion
chemotherapy and irradiation in T3 bladder carcinoma patients over
the age of 70 years. Tohoku J Exp Med. 192:249–258. 2000.
|
|
14.
|
Kaufman DS, Winter KA, Shipley WU, et al:
The initial results in muscle-invading bladder cancer of RTOG
95-06: phase I/II trial of transurethral surgery plus radiation
therapy with concurrent cisplatin and 5-fluorouracil followed by
selective bladder preservation or cystectomy depending on the
initial response. Oncologist. 5:471–476. 2000.
|
|
15.
|
Rodel C, Grabenbauer GG, Kuhn R, et al:
Combined-modality treatment and selective organ preservation in
invasive bladder cancer: long-term results. J Clin Oncol.
20:3061–3071. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Shipley WU, Winter KA, Kaufman DS, et al:
Phase III trial of neoadjuvant chemotherapy in patients with
invasive bladder cancer treated with selective bladder preservation
by combined radiation therapy and chemotherapy: initial results of
Radiation Therapy Oncology Group 89-03. J Clin Oncol. 16:3576–3583.
1998.
|
|
17.
|
Tester W, Caplan R, Heaney J, et al:
Neoadjuvant combined modality program with selective organ
preservation for invasive bladder cancer: results of Radiation
Therapy Oncology Group phase II trial 8802. J Clin Oncol.
14:119–126. 1996.
|
|
18.
|
Hagan MP, Winter KA, Kaufman DS, et al:
RTOG 97-06: initial report of a phase I–II trial of selective
bladder conservation using TURBT, twice-daily accelerated
irradiation sensitized with cisplatin, and adjuvant MCV combination
chemotherapy. Int J Radiat Oncol Biol Phys. 57:665–672.
2003.PubMed/NCBI
|
|
19.
|
Kaufman DS, Winter KA, Shipley WU, et al:
Phase I-II RTOG study (99-06) of patients with muscle-invasive
bladder cancer undergoing transurethral surgery, paclitaxel,
cisplatin, and twice-daily radiotherapy followed by selective
bladder preservation or radical cystectomy and adjuvant
chemotherapy. Urology. 73:833–837. 2009. View Article : Google Scholar
|
|
20.
|
Greene FL, Page DL and Fleming ID: AJCC
Cancer Staging Manual. 6th edition. Springer Verlag; New York, NY:
2002, View Article : Google Scholar
|
|
21.
|
Ficcara V, Dalpiaz O, Alrabi N, Novara G,
Galfano A and Artibani W: Correlation between clinical and
pathological staging in a series of radical cystectomies for
bladder carcinoma. BJU Int. 95:786–790. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Douple EB and Richmond RC: A review of
platinum complex biochemistry suggests a rationale for combined
platinum-radiotherapy. Int J Radiat Oncol Biol Phys. 8:1335–1339.
1979. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Douple EB and Richmond RC:
Radiosensitization of hypoxic tumor cells by cis- and
trans-dichlorodiammineplatinum (II). Int J Radiat Oncol Biol Phys.
8:1369–1372. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Abbott DW, Freeman ML and Holt JT:
Double-strand break repair deficiency and radiation sensitivity in
BRCA2 mutant cancer cells. J Natl Cancer Inst. 90:978–985. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Belt RJ, Himmelstein KJ, Patton TF,
Bannister SJ, Sternson LA and Repta AJ: Pharmacokinetics of
non-protein-bound platinum species following administration of
cis-dichlorodiammineplatinum(II). Cancer Treat Rep. 63:1515–1521.
1979.PubMed/NCBI
|
|
26.
|
Himmelstein KJ, Patton TF, Belt RJ, Taylor
S, Repta AJ and Sternson LA: Clinical kinetics on intact cisplatin
and some related species. Clin Pharmacol Ther. 29:658–664. 1981.
View Article : Google Scholar : PubMed/NCBI
|