Introduction
Advanced breast cancer (BC) and ovarian cancer (OC)
are two of the most lethal gynaecologic malignancies in developed
countries (1). Median survivals
are 15 months for metastatic breast cancer (2) and 57 months for stage III ovarian
cancer (3). In BC, current
consolidation treatments include monoclonal antibodies (4) and hormonetherapy (5). In OC, several trials have attempted
to introduce consolidation chemotherapy regimens, but up to now, no
treatment has shown by direct comparison to improve overall
survival in randomized trials (6).
There is plenty of evidence that prove the strong relationship
between these two neoplasms and the immune system and therefore
tumour response or progression is likely to be partially dictated
by the host immune status. Both OC and BC are able to elicit
spontaneous immune responses (7–9) and
antigen targeted immunotherapy represents an extremely attractive
strategy that could be added to conventional treatments.
Several tumour-associated antigens (TAAs) have been
identified as possible targets in BC and OC. The mucin MUC1 is a
highly glycosylated type I transmembrane glycoprotein that is
aberrantly glycosylated during tumour progression. It is expressed
in BC and OC tissues in over 90% of the cases. The carcinoembryonic
antigen (CEA) belongs both to the oncofetal and IgG supergene
family. It is expressed during oncofetal life and in normal colonic
mucosa. In tumours, CEA is overexpressed in 50 and 60% of BC and
OC, respectively. The ErbB2 oncogene belongs to the epidermal
growth factor (EGF) family. It is overexpressed in 20–30% of breast
and ovarian neoplasms.
Over the last decades, several trials on vaccination
in BC and OC have been carried out with disappointing results. We
have recently shown that tumour debulking is able to partially
revert tumour-induced immune suppression (10). Most past trials have enrolled
heavily pretreated women with high tumour burden. Currently,
several authors have stated that vaccination therapies may show
their highest efficacy in patients with low tumour burden and with
the immune system that has not been heavily compromised by previous
cytotoxic therapies (11).
Here we report the results of an escalating phase
I/II safety trial carried out with CEA (YLSGADLNL), ErbB2
(KIFGSLAFL) and MUC1 (SAPDNRPAL) peptides in high-risk patients in
clinical remission of disease who have completed standard
treatment. Furthermore, heavily pretreated patients affected by
advanced recurrent tumours were treated in a ‘compassionate
setting’ with the same vaccination schedule. Immunological data
from this sample of patients were used to verify the relevance of
timing for the efficacy of immunological interventions.
Vaccination leading to priming and expansion of
tumour reacting T cells can be an important therapeutic option to
be used in combination with checkpoint inhibitors such as
anti-CTLA4 and anti-PD1, to increase the specificity of the T cell
infiltrate repertoire and subsequently the efficacy of
treatment.
Materials and methods
Patients
This open-label phase I/II safety clinical trial was
approved by Policlinico Umberto I Ethics Committee (EC) and Italian
National Institute of Health (INIH) (protocol n∘LITRM/DIMIGE05/01).
Patients were recruited from the Gynaecologic and Obstetrics
Department of University of Rome ‘Sapienza’ from May 2007 to
January 2009. Inclusion criteria were: i) BC or OC who had
completed gold standard treatment forecast for their tumour type
and stage; ii) positive for the HLA-A2 haplotype; iii) written
informed consent, and iv) performance status accordingly to the
‘Eastern Cooperative Oncology Group’ (ECOG) between 0–2. Exclusion
criteria were: i) age ≤18 and ≥70 years; ii) history of autoimmune
disease; iii) previous malignancy; iv) ongoing HIV, HBV or HCV
infection; v) use of immunosuppressive drugs; vi) pregnancy and
breastfeeding and vii) any heart, liver, kidney or psychiatric
diseases. Furthermore 4 women affected by progressive, recurrent
disease, with EC approval, were treated with the same vaccination
schedule for compassionate use and their data are also
reported.
Study design and amendments
The study was performed as a feasibility and safety
phase I/II trial. On the basis of the extreme tolerance and low
magnitude of the side effects shown by the first 8 patients
according to protocol; in line with emerging literature suggesting
higher immunological responses of higher peptide vaccination doses
(12,13), the study was amended and
transitioned to phase II and the last 6 patients according to
protocol were vaccinated with a high dose regimen. In addition a
primary efficacy end point of recurrence was added at 36
months.
Three patients vaccinated for compassionate use were
vaccinated with a low dose regimen whereas one woman was vaccinated
with the high dose regimen.
One vaccinated ovarian cancer patient treated
according to protocol suffered a lymph nodal recurrence and was
subjected to para-aortic lymphadenectomy followed by 3 re-boosts
concomitantly to II line adjuvant chemotherapy.
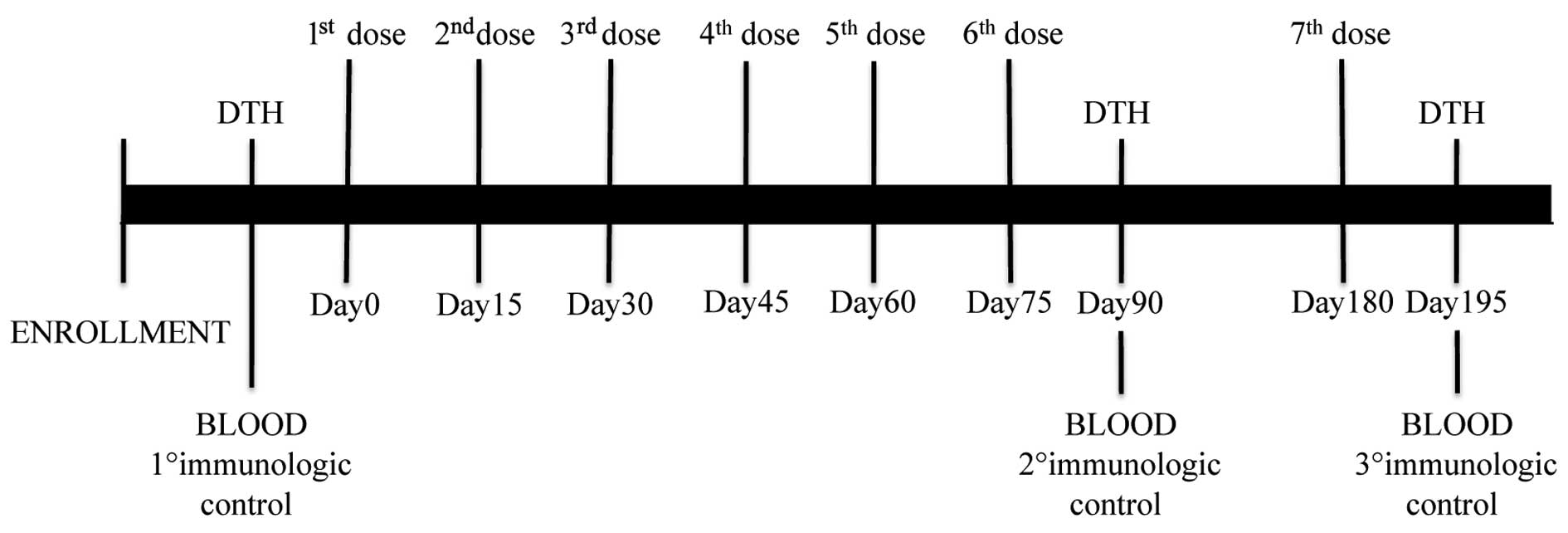
Vaccination was started within 6 months of
completion of chemotherapy. Thirty days of interval between the
last dose of adjuvant treatment and enrolment were required. Timing
of vaccination, blood sampling and delayed time hypersensitivity
(DTH) are shown in Fig. 1.
Briefly, the treatment schedule consisted in 6 consecutive doses
administered every two week followed by a further recall dose at 3
months from the last dose. Vaccination was carried out subcutis
(s.c.) in the inguinal area. Before and after vaccination, all
patients were skin tested with Keyhole Limpet Hemocyanin (KLH)
(Intracel, Frederick, MA, USA), in order to confirm patient's
immune competence.
Vaccine composition
Three HLAI-A2 restricted peptides adopted for
vaccination were: MUC1159-167 (SAPDNRPAL),
ErbB2368-377 (KIFGSLAFL) and CEA605-613
(YLSGADLNL). The peptides were commercially produced in good
manufacturing practices grade (GMP) by Clinalfa Merck Biosciences
(Läufelfingen, Switzerland). The vaccine always contained MUC1
peptide, whereas CEA and ErbB2 peptides were added to the vaccine
on the basis of immunohistochemical staining. Low and high dose
peptides were 100 and 500 μg, respectively. The vaccine also
contained 1 ml Montanide ISA 51 (Seppic, Paris, France) as adjuvant
and GM-CSF (Gentaur, Kampenhout, Belgium) 100 μg. In addition to
the vaccine, 100 μg of KLH were s.c. administered on the
contralateral inguinal area as immunological tracker.
Collection of peripheral blood
mononuclear cells (PBMCs)
Blood withdrawals (50 ml) were carried out before
the first vaccination dose, after the sixth vaccination and after
the recall dose (Fig. 1). PBMCs
were isolated by density-gradient centrifugation technique
(Ficoll-Hypaque, Cederlane, The Netherlands) and were cryopreserved
until use.
T cell stimulation in vitro
Thawed PBMCs from patients were in vitro
pre-sensitized with MUC1159-167, ErbB2368-377
and CEA605-613 peptide-pulsed K562-A*0201
cells (kindly provided by Dr T. Wolfel, University of Mainz) as
previously described (14).
Briefly, K562-A*0201 cells were pulsed for 1 h with 10
μg/ml of peptide (Clinalfa Merck Biosciences), then irradiated (30
Gy, X-RayCell Irradiator) and co-coltured with PBMCs to the ratio
1:30 without any additional wash. Cells were suspended in
RPMI-1640, penicillin 100 U/ml, streptomycin 100 μg/ml, glutamine 2
mM (all from EuroClone), β-mercaptoethanol 50 mM (Sigma-Aldrich,
St. Louis, MO, USA), 10% FCS (Biowest) [complete medium (CM)], IL-2
10 U/ml (PreproTech Inc., Rocky Hill, NJ, USA) and rIL-15 10 ng/ml
(R&D, Minneapolis, MN, USA). Cytokines were added at day 3, 7
and 10. At day 11, cells were harvested and CD8+ were
purified using CD8 microbeads (MiltenyiBiotec, Gladbach,
Germany).
Pentamer staining
Amplified CD8+ lymphocytes were analysed
with ErbB2, MUC1 and CEA pentamers (PE) (Proimmune, Oxford, UK)
according to the manufacturer's instructions. Concurrently, cells
were stained with anti-CD8 PE-Cy5 (clone RPA T8) and anti-CD3 FITC
(clone UCHT1) (both from BD Biosciences, San Diego, CA, USA)
antibodies.
ELISPOT assay
Multiscreen IPVH plates (Millipore, Bedford, MA,
USA) were coated with 10 μg/ml of mAb anti-human IFNγ (BD
Bioscience) in PBS w/o Ca++/Mg++ and plated
overnight at 4°C. After blocking, CD8+ antigen specific
T cells (1×105/well) were plated in triplicate with
irradiated (30 Gray) autologous PBMCs, derived from pre-vaccination
withdrawal, pulsed with MUC1, ErbB2 or CEA peptide. Cells were
removed 16 to 20 h later. Spots of IFNγ were detected by adding
biotinylated anti-IFNγ antibody (5 μg/ml, 2 h at 37°C) followed by
AKP-streptavidin conjugate (1:1,000, 2 h at 37°C) (both from BD
Bioscience) and chromogen substrate (BCIP/NBT Alkaline Phosphatase
Substrate; Sigma) (50 μl/well). Spots were counted using the
ImmunoSpot Image Analyzer (Aelvis, Germany). Results were evaluated
by subtracting the median number of spots of the negative samples
(unpulsed DCs + CD8 T cells) from median number of spots of the
study samples (peptide pulsed DCs + CD8 T cells). In order to
consider a sample evaluable a minimum of 20 spots above the
background was considered. The results were analyzed as fold
increase of the calculated values (after vaccination/before
vaccination). Median and range values of IFNγ spots were calculated
on the overall values of the three peptides. A vaccine induced CD8
T cell response was defined as at least 2-fold increase in the IFNγ
production of CD8 T cells from the last dose from the
pre-vaccination samples.
Flow cytometry
Cell labelling was performed using the following
monoclonal antibodies: anti-CD4 FITC (clone RPA T4), anti-CD45RA
APC (clone HI100), anti-CD25 PE (clone M-A251), and anti-FOXP3
Alexa 647 (clone 259D/C7) (all from BD Biosciences). For the FOXP3
intracellular staining, cells were permeabilized with Human FoxP3
Buffer (BD Biosciences). Cell phenotype was evaluated using
FACSCanto II flow cytometer running FACSDiva data acquisition and
analysis software (both from Becton Dickinson).
Delayed time hypersensitivity (DTH)
DTH reaction was used to evaluate the cellular
immune response at different time-points of vaccination in
vivo (Fig. 1). The assay was
performed by separate intradermal injection in the region
anti-brachioradialis of 10 μg of MUC1, ErbB2, CEA peptides
(Clinalfa Merck Biosciences) and KLH (Intracell). Positivity was
assessed 48–72 h later and compared to the control.
Toxicity
The ECOG Common Toxicity Criteria (version, June 15,
2007) definition of toxicity events was applied. Patients were
controlled, at all doses, for both local and systemic adverse
events. By study design, progression to second phase occured if no
significant toxicity was registered in the first eleven
patients.
Clinical follow-up
Since the enrolment all patients were screened for
recurrence by: physical, laboratory and imaging exams performed
every 3 months in the absence of any new symptoms. Follow-up was
closed after a median of 87 months, in July 2015.
Statistical analysis
Data were analysed using STATA11 (StataCorp LP,
College Station, College Station, TX, USA). A Fisher's exact test
was used to examine the significance of the association of the
dichotomous outcomes. Significance is indicated when the
p-value is <0.05.
Results
Patients
Between 2007 and 2009, 14 patients (7 BC and 7 OC
women) were enrolled in this trial and treated according to the
protocol. In addition, 4 patients (1 BC and 3 OC) affected by
recurrent/metastatic disease requested vaccination for
compassionate use and were subjected to the same treatment.
Immunological data from the latter patients are also described and
used for comparison. Characteristics of all the patients are
summarized in Table I.
 | Table IPatient characteristics. |
Table I
Patient characteristics.
|
Characteristics | Data |
|---|
| BC patient
characteristics (n=7) |
| Median age
(years) | 45 |
| Stage of tumor,
n |
| IA | 1 |
| IIA | 3 |
| IIIA | 1 |
| IIIC | 2 |
| Histology, n |
| Infiltrating
ductal BC | 6 |
| Infiltrating
ductal nas BC | 1 |
| Grade, n |
| I | 1 |
| II | 1 |
| III | 5 |
| Node status (+),
n | 6 |
| Status before
vaccination, n |
| DF | 7 |
| OC patient
characteristics (n=7) |
| Median age
(years) | 53 |
| Stage of tumor,
n |
| IIA | 1 |
| IIIA | 1 |
| IIB | 1 |
| IC | 1 |
| IIIC | 3 |
| Histology, n |
| Serous
adenocarcinoma | 4 |
| Endometrioid | 1 |
| Mucinous | 2 |
| Grade, n |
| II | 1 |
| III | 6 |
| RT <1 cm, n | 7 |
| Status before
vaccination, n |
| DF | 7 |
|
| OC (3 pzs) | BC (1 pz) |
|
| Patient
characteristics (compassionate use) (n=4) |
| Median age | 60 years | 40 years |
| Stage of tumor | IIIC (2 pzs); IIB
(1 pz) | IV |
| Histology | Serous
adenocarcinoma (3/3) | Infiltrating ductal
BC |
| Grade | III (3/3) | III |
| Status before
vaccination | SD (2 pzs); PD (1
pz) | PD |
Briefly, the average age of all enrolled patients
was 53 (sd, 9,9; range, 42–70 years old). BC patients were mostly
affected by infiltrating ductal breast carcinoma. ErbB2 expression
was 3+ in 57% of the patients and 2+ in 43%,
half of the women had <3 positive lymph nodes. CEA and MUC1
tumour expression was respectively 71 and 100%. Half of the OC
cases were serous adenocarcinoma at diagnosis, most women were
affected by scarcely differentiated neoplasms, FIGO stage III and
optimally debulked (residual tumour <1 cm). Platinum-based
adjuvant chemotherapy was successively administered to all OC
patients. CEA, ErbB2 and MUC1 expression was, respectively, 43, 43
and 100%. CA-125 levels were routinely monitored in all ovarian
cancer patients and resulted below range of positivity also for
patient OV04 and OV011 who experienced a recurrence.
Two OC patients treated for compassionate use had
been subjected to secondary cytoreduction and adjuvant platinum
based second line chemotherapy. These patients were in clinical
remission at the beginning of immunotherapy. The last OC patient
suffered from peritoneal disease progression after tumour debulking
and three lines of chemotherapy. The BC patient, treated in a
compassionate setting, was a woman affected by pleural, brain,
hepatic and bone recurrence after treatment with taxane,
trastuzumab, lapatinib and capecitabine.
All 14 enrolled patients completed the vaccination
regimen receiving the 6 doses of vaccine and the additional recall
dose. Of these, 6 women received a high dose regimen. Therefore 84
vaccinations (36 high dose) were carried out with their 14 planned
recall doses in this setting.
Three out of 4 patients undergoing vaccination for
compassionate use received a low dose regimen and one the high
dose, while one out of 3 patients completed the low dose
vaccination protocol with the recall dose. One patient completed
the low dose vaccination protocol, but did not carry out the recall
dose due to disease progression. One patient suspended treatment
after the third vaccination for disease progression. One patient
completed the high dose vaccination protocol and carried out the
recall dose.
Evaluation of the immune response
Before vaccination, no enrolled patient had a
specific IFNγ producing CD8+ immune response. At the end
of the treatment, 8/14 patients showed a specific IFNγ producing
CD8+ immune response to at least one antigen (Tables II and III). None of the 4 patients vaccinated
for compassionate use showed an activation of CD8+
specific lymphocyte before or after vaccination (Table IV).
| Table IIBreast cancer patients. |
Table II
Breast cancer patients.
| Stage at
diagnosis | Type of
surgery | Lymph nodal
status | Type of ADJ
therapy | Type of ADJ
CHT | Hormonal
therapy | Anti-ErbB2
therapy | ErbB2
positivity | Antigens | Dose of peptides
(μg) | CD8 post
vaccination | DTH (mts) | DFS (mts) | OS | Vaccination
beginning | Current disease
status (Jul 2015) |
|---|
| MA01 | IIIC | Quadrantectomy +
lymphadenectomy | Pos | RT + CHT | Cyclophosphamide +
adriamycin (4 cycles) followed by paclitaxel (4 cycles) | No | No | 2+ | MUC1, ErbB2,
CEA | 100 | ErbB2 | NEG |
119+ |
125+ | Jul 2007 | NED |
| MA02 | IIA | Quadrantectomy +
lymphadenectomy | Pos | RT + CHT | Cyclophosphamide +
adriamycin (4 cycles) followed by paclitaxel (4 cycles) | No | No | 2+ | MUC1, ErbB2 | 100 | NEG | NEG |
103+ |
109+ | Jun 2007 | NED |
| MA03 | IIIA | Quadrantectomy +
lymphadenectomy | Pos | RT + CHT | Cyclophosphamide +
adriamycin (4 cycles) followed by paclitaxel (4 cycles) | No | Yes | 3+ | MUC1, ErbB2 | 100 | NEG | MUC1 | 78 |
110+ | Feb 2008 | NED |
| MA05 | IA | Quadrantectomy +
lymphadenectomy | Neg | RT + CHT | Cyclophosphamide +
adriamycin (6 cycles) | Yes | Yes | 3+ | MUC1, ErbB2 | 500 | NEG | NEG |
104+ |
109+ | Apr 2008 | NED |
| MA07 | IIIC | Radical mastectomy
+ lymphadenectomy | Pos | RT + CHT | Docetaxel +
epirubicin + cyclophosphamide (6 cycles) | Yes | Yes | 3+ | MUC1, ErbB2,
CEA | 500 | NEG | MUC1, CEA | 97+ |
113+ | Nov 2008 | NED |
| MA08 | IIA | Radical mastectomy
+ lymphadenectomy | Pos | No | - | Yes | No | 3+ | MUC1, ErbB2,
CEA | 500 | NEG | NEG |
111+ |
111+ | Nov 2008 | NED |
| MA010 | IIA | Quadrantectomy +
lymphadenectomy | Pos | RT + CHT | Cyclophosphamide +
adriamycin (4 cycles) followed by paclitaxel (4 cycles) | No | No | 2+ | MUC1, ErbB2,
CEA | 500 | CEA | NEG | 89+ | 96+ | Oct 2009 | NED |
| Table IIIOvarian cancer patients. |
Table III
Ovarian cancer patients.
| Stage at
diagnosis | Type of
surgery | Type of ADJ
CHT | Antigens | Dose of peptides
(μg) | CD8 post
vaccination | DTH | DFS (months) | OS (months) | Vaccination
beginning | Current disease
status (July 2015) |
|---|
| OV01 | IIA | Primary
cytoreduction | Carboplatin +
paclitaxel (6 cycles) | MUC1 | 100 | MUC1 | MUC1 | 87 |
102+ | Jul 2007 | NED |
| OV04 | IIIC | Primary
cytoreduction | Carboplatin +
paclitaxel (6 cycles) | MUC1 | 100 | NEG | NEG | 18 |
109+ | Sep 2007 | PD |
| OV05 | IIIC | Primary
cytoreduction | Carboplatin +
paclitaxel (6 cycles) | MUC1 | 100 | MUC1 | NEG |
128+ |
133+ | Sep 2007 | NED |
| OV06 | IC | Primary
cytoreduction | Carboplatin +
paclitaxel (5 cycles) | MUC1, CEA | 100 | CEA | CEA |
114+ |
122+ | Dec 2007 | NED |
| OV07 | IIIA | Primary
cytoreduction | Carboplatin +
paclitaxel (6 cycles) | MUC1, ErbB2 | 100 | ErbB2 | NEG | 96+ |
101+ | Jan 2008 | NED |
| OV010 | IIIC | Primary
cytoreduction | Carboplatin +
paclitaxel (6 cycles) | MUC1, ErbB2,
CEA | 500 | MUC1, ErbB2,
CEA | NEG |
104+ |
111+ | Sep 2008 | NED |
| OV011 | IIB | Primary
cytoreduction | Carboplatin +
paclitaxel (6 cycles) | MUC1, ErbB2,
CEA | 500 | ErbB2, CEA | ErbB2 | 94+ | 99+ | Jan 2009 | NED |
| Table IVCharacteristics of patients
vaccinated for compassionate use. |
Table IV
Characteristics of patients
vaccinated for compassionate use.
| Patients | Stage at
diagnosis | Clinical stage
before vaccination | No. of
vaccination | Antigens | Single dose
peptides (ug) | CD8
pre-vaccination | CD8
post-vaccination | Clinical
Response |
|---|
| MA09 | IV | PD | 6 | MUC1-ErbB2-CEA | 500 | Neg | Neg | PD |
| OV02 | IIIC | SD | 6 | MUC1 | 100 | Neg | Neg | PD |
| OV03 | IIIC | PD | 3 | MUC1-CEA | 100 | Neg | Neg | PD |
| OV08 | IIB | SD | 7 | MUC1 | 100 | Neg | Neg | PD |
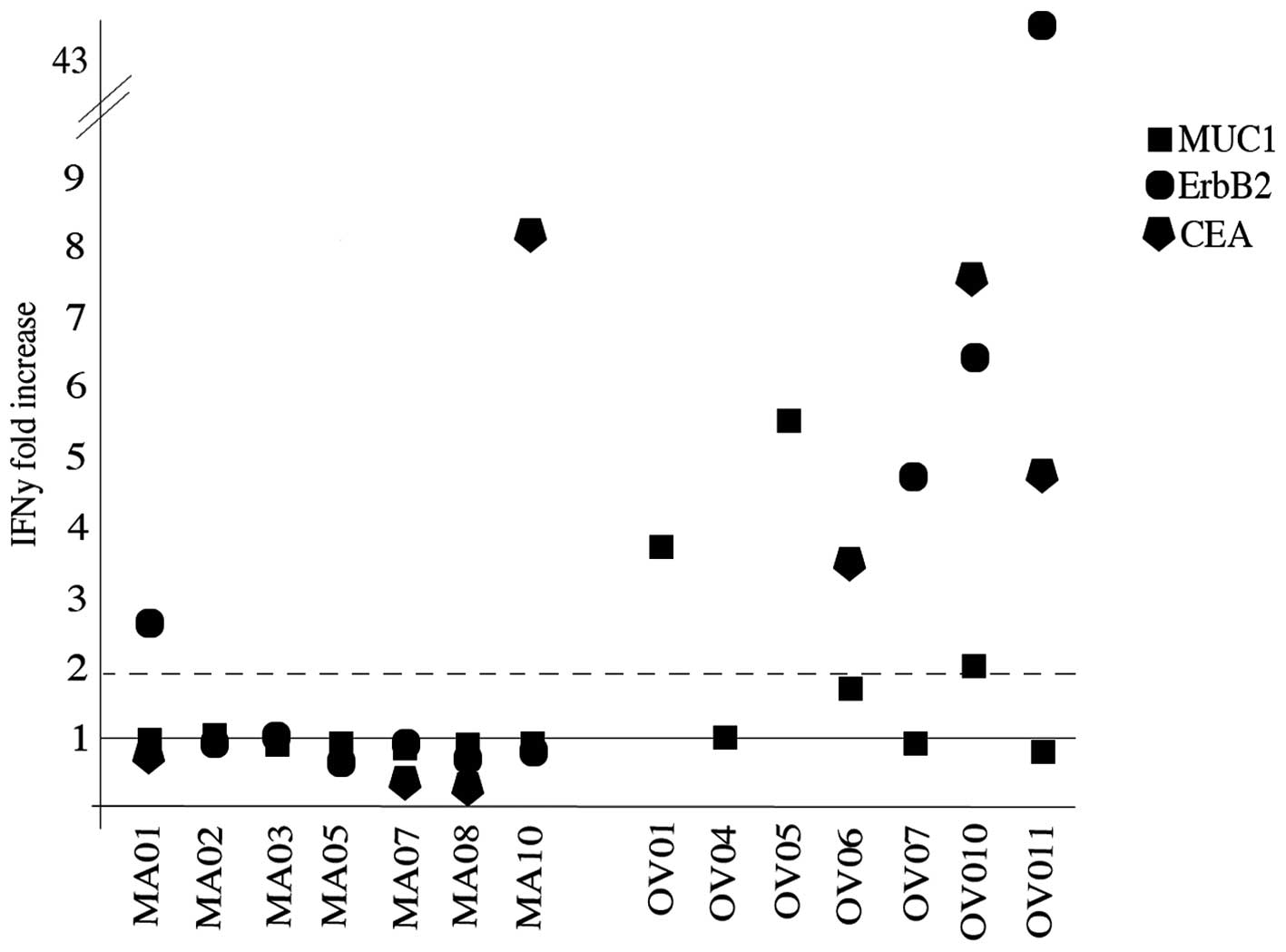
Among responding patients, 2/7 were BC whereas 6/7
were OC. Highest response rates were detected after the completion
of the six administrations. Peptide vaccination was effective in
inducing an immune response in 3/14, 4/10 and 4/7 for MUC1, ErbB2
and CEA, respectively. The low dose and high dose regimen induced a
response in respectively 5/8 and 3/6 patients. In Fig. 2, patient immune response to the
antigenic peptides is presented as ratio between the IFNγ spots
obtained after and before vaccination.
The median background of IFNγ spots of negative
control samples (unpulsed DCs + CD8 T cells) was 23 (range, 8–178)
before vaccination and 19 (range, 8–118) after vaccination. The
median values of IFNγ spots of study samples (peptide pulsed DCs +
CD8 T cells) before and after vaccination were 19 (range, 7–296)
and 42.5 (range, 8–598), respectively. Data (median and range) of
the single peptide are summarized in Table V.
| Table VMedian and range values of IFNγ spots
produced by CD8 T cells before and after vaccination. |
Table V
Median and range values of IFNγ spots
produced by CD8 T cells before and after vaccination.
| DCs + CD8 T
cells | DCs + peptide + CD8
T cells |
|---|
|
|
|
|---|
| Median | Range | Median | Range |
|---|
| Before
vaccination |
| CEA | 22.5 | 8–60 | 40 | 8–80 |
| MUC1 | 16 | 12–112 | 18 | 7–202 |
| ErbB2 | 21 | 10–178 | 27.5 | 9–296 |
| After
vaccination |
| CEA | 31 | 12–118 | 65 | 12–598 |
| MUC1 | 20 | 8–56 | 15 | 8–160 |
| ErbB2 | 39 | 14–100 | 179.5 | 12–390 |
A vaccine-induced CD8 T cell response was defined as
at least 2-fold increase in the IFNγ production of CD8 T cells from
the last vaccination dose from the pre-vaccination samples.
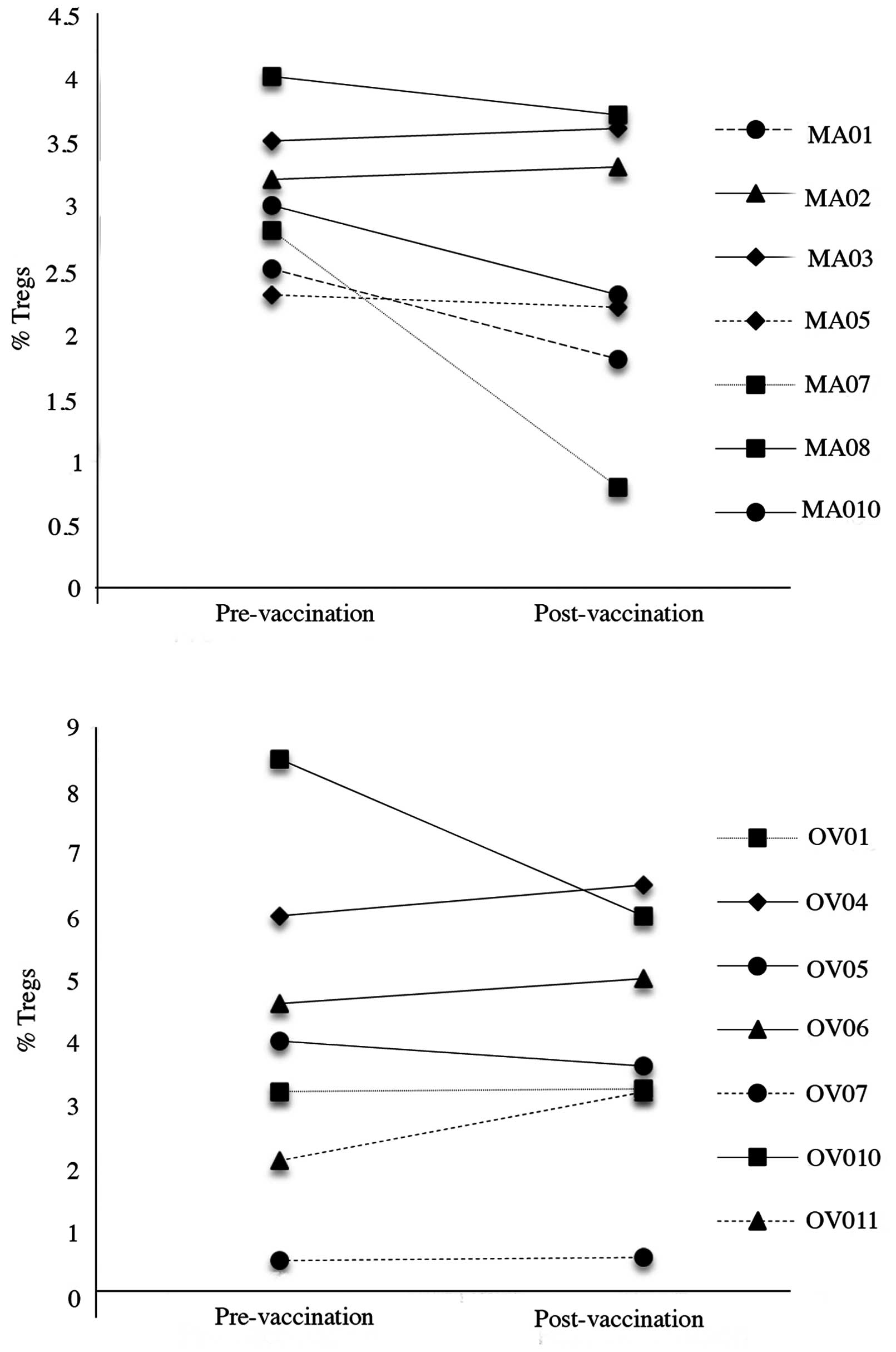
Treg trends did not appear to be correlated to a
clinical or immunological response. Only 2/14 patients (MA07 and
OV10) showed a decrease in circulating Tregs, one in a patient who
showed no response to vaccination and one who showed a strong
response to two peptides (Fig.
3).
DTH skin reactions were tested by injecting 10 μg of
each peptide intradermal at baseline, after the sixth and after the
seventh dose of vaccination for in vivo immunomonitoring. No
positive reactions were detected at baseline. Five out of 14
patients developed a positive DTH to at least one peptide after the
recall dose.
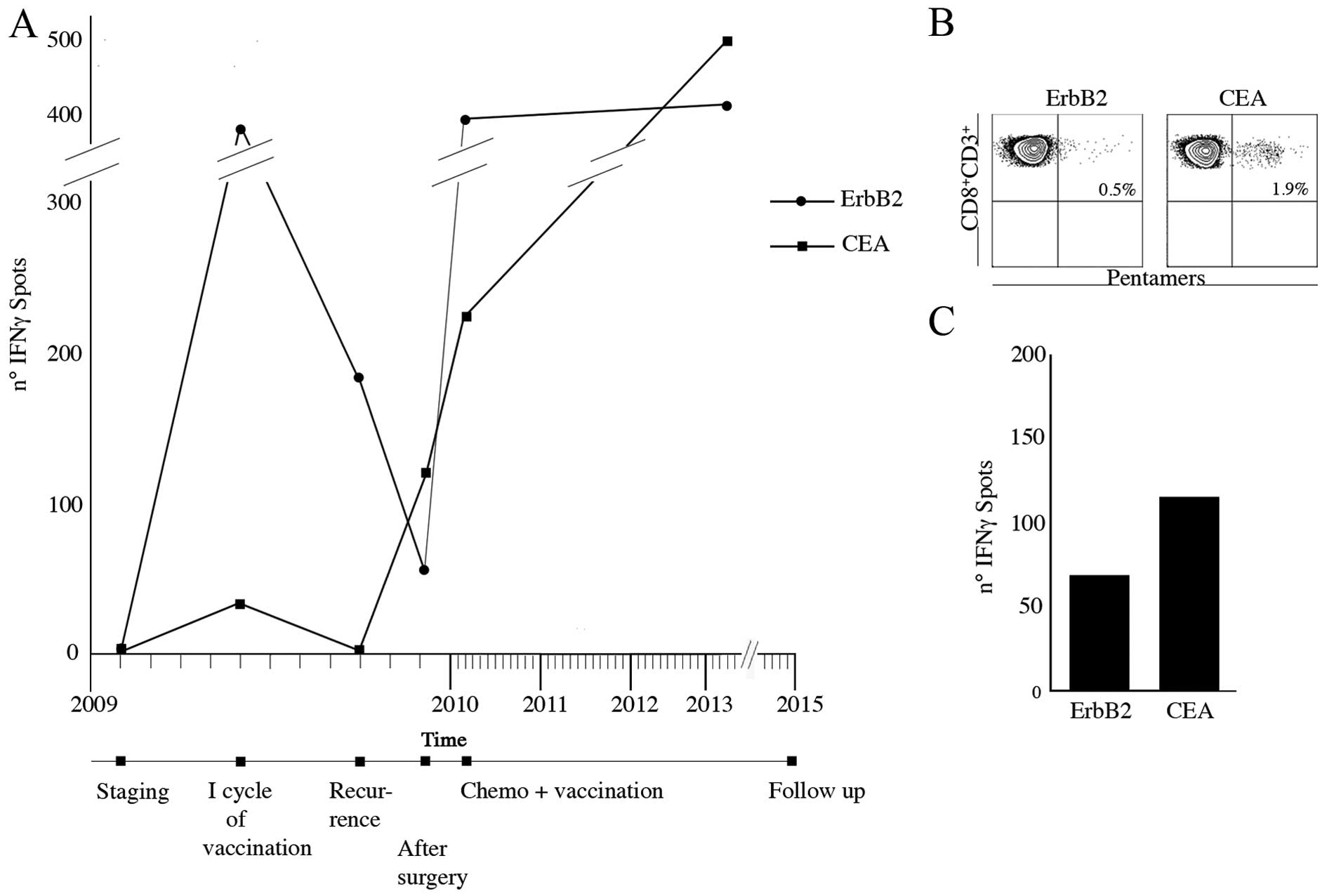
An OC patient enrolled in the trial suffered from
lymph nodal recurrence 14 months after primary surgery. She was
subjected to para-aortic lymphadenectomy. She was then submitted to
II line chemotherapy and concomitantly to 3 vaccination re-boosts
every 3 weeks. During the first vaccination cycle, specific IFNγ
producing CD8+ immune response to the ErbB2 and CEA
peptides had increased but returned to baseline after 3 months from
the treatment. After 5 months from the vaccination, at the time of
relapse, specific ErbB2, CEA CD8+ circulating
lymphocytes had increased (Fig.
4A). Interestingly CEA- and ErbB2-specific CD8+
lymphocytes were also identified in the removed bulky aortic lymph
nodes (Fig. 4B). This suggests
that although the immune response was unable to avoid recurrence,
homing of specific lymphocytes occurred. A blood sample collected
at 36 months from the last boost still showed specific IFNγ
producing ErbB2 and CEA CD8+ T cells (Fig. 4C).
Toxicity
No ECOG grade 4 toxicity related to the study was
observed. The most common adverse events were itch, erythema and
tumescence (all maximum grade 2) in the injection site. Moreover, 6
patients referred Flu-like symptoms (all maximum grade 2) the day
after vaccination dose. Only one patient developed deep venous
thrombosis (grade 3) in the right leg that was managed with medical
treatment (Table VI).
| Table VIVaccine toxicity. |
Table VI
Vaccine toxicity.
| EOCG level of
toxicity |
|---|
|
|
|---|
| | 0 | 1 | 2 | 3 | 4 |
|---|
| Leukopenia | WBC×103;
lymphocytes; granulocytes/ bands | 18 | 0 | 0 | 0 | 0 |
|
Thrombocytopenia | Plt
×103 | 18 | 0 | 0 | 0 | 0 |
| Anemia | Hgb | 18 | 0 | 0 | 0 | 0 |
| Coagulation | Fibrinogen; PT;
PTT | 18 | 0 | 0 | 0 | 0 |
| GU | Creatinine | 18 | 0 | 0 | 0 | 0 |
| Liver | Bilirubin; SGOT,
SGPT | 18 | 0 | 0 | 0 | 0 |
| Fever in absence of
infection | - | 12 | 6 | 0 | 0 | 0 |
| GI | Nausea; vomiting;
diarrhea | 18 | 0 | 0 | 0 | 0 |
| Skin | - | 0 | 14 | 4 | 0 | 0 |
| Allergy | - | 17 | 1 | 0 | 0 | 0 |
| Phlebitis | - | 17 | 0 | 0 | 1 | 0 |
| Local | - | 16 | 2 | 0 | 0 | 0 |
| Alopecia | - | 18 | 0 | 0 | 0 | 0 |
Survival
At a maximum of 8 years follow-up, all 7 BC patients
enrolled according to protocol are alive and currently
disease-free. One patient suffered from disease recurrence and was
treated with surgery and adjuvant chemotherapy, she has been
disease-free for 26 months. Out of the 7 OC patients enrolled, no
patient has died of disease although 2 patients suffered from
disease recurrence. These women were subjected to secondary
cytoreduction and adjuvant chemotherapy. One of them is currently
disease-free at the 1-year follow-up check-up and the other suffers
from disease recurrence.
Discussion
Chemo-radio-therapy and the most recent targeted
therapies have significantly improved the survival rates of
different malignancies. However, survival rates remain highly
unsatisfactory and these standard options produce intense,
debilitating and distressing side effects, destroying healthy
tissues along with cancer cells. Consequently, there is a constant
and clear unmet demand for the development of new therapeutic
effective agents and strategies with minimal side effects.
In the present scenario, cancer immunotherapy
appears to be a promising candidate, since clinical trials have
shown positive effects on survival with minimal side effects
(15,16). So far, different strategies of
immunoactivation have been attempted in cancer patients, mostly
adopting synergic biological mechanism: peptide- or protein-based
vaccinations, poxviral vectors, anti-idiotypic antibody-based
vaccinations, dendritic cell- and retargeted lymphocytes. Recently,
the possibilities to combine these strategies with unspecific
unleashing T cell modulation and expansion have, moreover,
increased interest in these protocols.
Among different approaches, short peptide-based
vaccinations have several advantages such as good immunological
efficacy, low costs and safety. Peptide tumour-associated antigens
are usually 8–10 amino acids long with 2–3 primary anchor residues
that interact with MHC class I-molecules and 2–3 residues which
bind to T cell receptor (17,18).
Short peptides are characterized by a small size, ease of synthesis
and manipulation, direct load on antigen presenting cells, and low
production and administration costs (19–21).
CTLs directed against peptides presented by MHC class I molecules
constitute powerful effectors of the immune system against tumour
cells.
In BC, clinical experiences with peptide-based
vaccinations date back to 1999 and since then ~400 women have been
subjected to these types of vaccinations. Immunogenic epitopes of
ErbB2 (22), MUC1 (23,24)
and survivin 2B (13) have been
adopted. Encouraging results have derived from trials especially in
using ErbB2 peptide. Unfortunately, in advanced BC setting,
immunotherapy did not show any impact on the patients' clinical
outcome (25,26). However, promising experience in BC
early disease setting has been gathered. Disease-free
HLA-A2+ breast cancer patients receiving different dose
regimen of 4–6 monthly vaccinations as consolidation treatment, in
fact, although presented with poorer prognostic factor compared to
the control group, showed a significantly better prognosis in terms
of both DFS and OS respect to disease-free HLA-A2-BC patients not
subjected to vaccination program after an average of 2 years of
follow-up. Vaccinated patients showed to have developed
E75-specific CD8+ T cell, still detectable 6 months
after vaccination completion (27). As a consequence, previous
experience of peptide-based vaccination in BC led us to understand
that peptides are able to: i) induce a T CD4+ and T
CD8+-specific immunologic response; ii) induce epitope
spreading; iii) elicit a T cell immunity against the vaccinated
epitope and other tumour derived proteins and iv) induce a subset
of memory T cells.
Less experience has been gathered on OC patients,
however, the results appear to be in line with those observed in
breast tumours. Approximately 150 women were subjected to
peptide-based vaccination beginning in 2002 (22). Most immunogenic epitopes adopted in
ovarian cancer setting were found to be mixed ErbB2 peptides and
NY-ESO peptide (28,29). Unfortunately, most OC patients are
diagnosed with an advanced stage and in this setting the high
tumour burden has proved to induce systemic immunosuppression and
subsequent immune system failure (10). As a consequence, the immunological
exhaustion characterizing advanced OC patients was probably the
limiting factor determining the absence of clinical benefit
reported in the previous experience of immunotherapy trial in
vaccinated OC patients.
In the present phase I/II study, the clinical safety
and immune activation and modulation of consolidation therapy with
a multipeptide vaccine were investigated in 14 BC and OC patients
in clinical disease remission. Multipeptide vaccination is safe and
able to induce a specific IFNγ producing CD8+ immune
response.
OC patients showed higher immunological responses
when compared to BC patients. This could be partially explained by
the platinum based regimens adopted for OC patients that have an
indirect effect on the immune system (30). Platinum-based therapies have in
fact shown to enhance the immunostimulatory potential of DCs and
decrease immunosuppression by depleting myeloid suppressor cells
(31,32). CEA modified CAP-1 peptide appeared
to be the most effective in inducing cellular specific immune
response, whereas MUC1 peptide epitope, adopted in human beings for
the first time, and E75 were able to induce a specific immune
response in, respectively, 20 and 40% of patients. It is important
to highlight that these are the first data that allow a direct
comparison of the same vaccination schedule in two extremely
different moments of the natural history of these neoplasms. In
line with the poor clinical responses reported in past trials, none
of the heavily pretreated patients or patients presenting with high
tumour burden showed any immunological response. Although
anecdotal, the observation is promising; it was carried out in the
patients whose samples from recurrent disease were available. The
high percentage of vaccine specific CD8+ lymphocytes in
the bulky nodes demonstrates the homing phenomenon of newly
generated immune cells. Moreover, in this patient additional
recalls of the vaccine were able to re-elicit further the amount of
specific CD8+ T cells against ErbB2 and particularly to
the CEA antigen that was weakly positive in the first
vaccination.
Overall, although beyond the study objective, the
clinical outcome of the patients enrolled in the trial appears
favourable, having registered no patient deceased at an average 87
months follow-up. Several enrolled patients were affected by early
disease and therefore this may justify the survival data. The
prolonged follow-up and the sample size are sufficient to exclude
long-term side effects or a paradoxical detrimental effect on
survival.
The promising results, in line with the data
observed in similar studies, the high compliance observed by the
patients and the favourable toxicity profile associated with
minimal costs, support future trials of peptide vaccination in
clinically disease-free patients who have completed standard
treatments.
In conclusion, in BC and OC patients in clinical
disease remission, multipeptide vaccination is safe and able to
induce a specific IFNγ producing CD8+ immune response.
In particular, OC patients appear to be more prone to activate a
specific immune response most probably due to the synergy with
platinum based chemotherapy.
Acknowledgements
This study was supported by PRIN 2007 (prot.
n∘20072LRAZJ), PRIN 2009 (prot. n∘2009XMZPKW), AIRC 2009 (ref.
codes 9249 and 17432), FIRB (ref code RBAU01THPL_002).
Abbreviations:
|
AKP
|
alkaline phosphatase
|
|
CEA
|
carcinoembryonic antigen
|
|
CTL
|
cytotoxic T lymphocytes
|
|
DFS
|
disease-free survival
|
|
DTH
|
delayed time hypersensitivity
|
|
EC
|
Ethics Committee
|
|
EGF
|
epithelial growth factor
|
|
EOCG
|
Eastern Cooperative Oncology Group
|
|
GMP
|
good manufacturing practice
|
|
INIH
|
Italian National Institute of
Health
|
|
KLH
|
keyhole limpet hemocyanin
|
|
OS
|
overall survival
|
|
PBMCs
|
peripheral blood mononuclear cells
|
|
SC
|
subcutis
|
|
TAAs
|
tumour associated antigens
|
|
Treg
|
regulatory T cells
|
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chan S, Friedrichs K, Noel D, Pintér T,
Van Belle S, Vorobiof D, Duarte R, Gil Gil M, Bodrogi I, Murray E,
et al; 303 Study Group. Prospective randomized trial of docetaxel
versus doxorubicin in patients with metastatic breast cancer. J
Clin Oncol. 17:2341–2354. 1999.PubMed/NCBI
|
|
3
|
Ozols RF, Bundy BN, Greer BE, Fowler JM,
Clarke-Pearson D, Burger RA, Mannel RS, DeGeest K, Hartenbach EM
and Baergen R; Gynecologic Oncology Group. Phase III trial of
carboplatin and paclitaxel compared with cisplatin and paclitaxel
in patients with optimally resected stage III ovarian cancer: A
Gynecologic Oncology Group study. J Clin Oncol. 21:3194–3200. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Paik S, Kim C and Wolmark N: HER2 status
and benefit from adjuvant trastuzumab in breast cancer. N Engl J
Med. 358:1409–1411. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Aydiner A and Tas F: Meta-analysis of
trials comparing anastrozole and tamoxifen for adjuvant treatment
of postmenopausal women with early breast cancer. Trials. 9:472008.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Pecorelli S, Favalli G, Gadducci A,
Katsaros D, Panici PB, Carpi A, Scambia G, Ballardini M, Nanni O
and Conte P; After 6 Italian Cooperative Group. Phase III trial of
observation versus six courses of paclitaxel in patients with
advanced epithelial ovarian cancer in complete response after six
courses of paclitaxel/platinum-based chemotherapy: Final results of
the After-6 protocol 1. J Clin Oncol. 27:4642–4648. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhang L, Conejo-Garcia JR, Katsaros D,
Gimotty PA, Massobrio M, Regnani G, Makrigiannakis A, Gray H,
Schlienger K, Liebman MN, et al: Intratumoral T cells, recurrence,
and survival in epithelial ovarian cancer. N Engl J Med.
348:203–213. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Curiel TJ, Coukos G, Zou L, Alvarez X,
Cheng P, Mottram P, Evdemon-Hogan M, Conejo-Garcia JR, Zhang L,
Burow M, et al: Specific recruitment of regulatory T cells in
ovarian carcinoma fosters immune privilege and predicts reduced
survival. Nat Med. 10:942–949. 2004. View
Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mahmoud SM, Paish EC, Powe DG, Macmillan
RD, Grainge MJ, Lee AH, Ellis IO and Green AR: Tumor-infiltrating
CD8+ lymphocytes predict clinical outcome in breast
cancer. J Clin Oncol. 29:1949–1955. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Napoletano C, Bellati F, Landi R, Pauselli
S, Marchetti C, Visconti V, Sale P, Liberati M, Rughetti A, Frati
L, et al: Ovarian cancer cytoreduction induces changes in T cell
population subsets reducing immunosuppression. J Cell Mol Med.
14:2748–2759. 2010. View Article : Google Scholar
|
|
11
|
Bellati F, Napoletano C, Ruscito I,
Visconti V, Antonilli M, Gasparri ML, Zizzari IG, Rahimi H, Palaia
I, Rughetti A, et al: Past, present and future strategies of
immunotherapy in gynecological malignancies. Curr Mol Med.
13:648–669. 2013. View Article : Google Scholar
|
|
12
|
Hueman MT, Stojadinovic A, Storrer CE,
Dehqanzada ZA, Gurney JM, Shriver CD, Ponniah S and Peoples GE:
Analysis of naïve and memory CD4 and CD8 T cell populations in
breast cancer patients receiving a HER2/neu peptide (E75) and
GM-CSF vaccine. Cancer Immunol Immunother. 56:135–146. 2007.
View Article : Google Scholar
|
|
13
|
Tsuruma T, Iwayama Y, Ohmura T,
Katsuramaki T, Hata F, Furuhata T, Yamaguchi K, Kimura Y, Torigoe
T, Toyota N, et al: Clinical and immunological evaluation of
anti-apoptosis protein, survivin-derived peptide vaccine in phase I
clinical study for patients with advanced or recurrent breast
cancer. J Transl Med. 6:242008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yuan J, Gallardo HF, Rasalan T,
Ranganathan R, Wang J, Zhang Y, Panageas K, Stan R, Young JW,
Houghton AN, et al: In vitro expansion of Ag-specific T cells by
HLA-A*0201-transfected K562 cells for immune monitoring.
Cytotherapy. 8:498–508. 2006. View Article : Google Scholar
|
|
15
|
Horstmann E, McCabe MS, Grochow L,
Yamamoto S, Rubinstein L, Budd T, Shoemaker D, Emanuel EJ and Grady
C: Risks and benefits of phase 1 oncology trials, 1991 through
2002. N Engl J Med. 352:895–904. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kantoff PW, Higano CS, Shore ND, Berger
ER, Small EJ, Penson DF, Redfern CH, Ferrari AC, Dreicer R, Sims
RB, et al; IMPACT Study Investigators. Sipuleucel-T immunotherapy
for castration-resistant prostate cancer. N Engl J Med.
363:411–422. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Thayer AM: Improving peptides. Chem Eng
News. 89:13–20. 2011.
|
|
18
|
Borghouts C, Kunz C and Groner B: Current
strategies for the development of peptide-based anti-cancer
therapeutics. J Pept Sci. 11:713–726. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gao GF and Jakobsen BK: Molecular
interactions of coreceptor CD8 and MHC class I: The molecular basis
for functional co-ordination with the T-cell receptor. Immunol
Today. 21:630–636. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Cho HI and Celis E: Optimized peptide
vaccines eliciting extensive CD8 T-cell responses with therapeutic
antitumor effects. Cancer Res. 69:9012–9019. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Napoletano C, Rughetti A, Landi R, Pinto
D, Bellati F, Rahimi H, Spinelli GP, Pauselli S, Sale P, Dolo V, et
al: Immunogenicity of allo-vesicle carrying ERBB2 tumor antigen for
dendritic cell-based anti-tumor immunotherapy. Int J Immunopathol
Pharmacol. 22:647–658. 2009.PubMed/NCBI
|
|
22
|
Disis ML, Gooley TA, Rinn K, Davis D,
Piepkorn M, Cheever MA, Knutson KL and Schiffman K: Generation of
T-cell immunity to the HER-2/neu protein after active immunization
with HER-2/neu peptide-based vaccines. J Clin Oncol. 20:2624–2632.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Musselli C, Ragupathi G, Gilewski T,
Panageas KS, Spinat Y and Livingston PO: Reevaluation of the
cellular immune response in breast cancer patients vaccinated with
MUC1. Int J Cancer. 97:660–667. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gilewski T, Adluri S, Ragupathi G, Zhang
S, Yao TJ, Panageas K, Moynahan M, Houghton A, Norton L and
Livingston PO: Vaccination of high-risk breast cancer patients with
mucin-1 (MUC1) keyhole limpet hemocyanin conjugate plus QS-21. Clin
Cancer Res. 6:1693–1701. 2000.PubMed/NCBI
|
|
25
|
Knutson KL, Schiffman K, Cheever MA and
Disis ML: Immunization of cancer patients with a HER-2/neu, HLA-A2
peptide, 369–377 results in short-lived peptide-specific immunity.
Clin Cancer Res. 8:1014–1018. 2002.PubMed/NCBI
|
|
26
|
Salazar LG, Fikes J, Southwood S, Ishioka
G, Knutson KL, Gooley TA, Schiffman K and Disis ML: Immunization of
cancer patients with HER-2/neu-derived peptides demonstrating
highaffinity binding to multiple class II alleles. Clin Cancer Res.
9:5559–5565. 2003.PubMed/NCBI
|
|
27
|
Peoples GE, Gurney JM, Hueman MT, Woll MM,
Ryan GB, Storrer CE, Fisher C, Shriver CD, Ioannides CG and Ponniah
S: Clinical trial results of a HER2/neu (E75) vaccine to prevent
recurrence in high-risk breast cancer patients. J Clin Oncol.
23:7536–7545. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Odunsi K, Qian F, Matsuzaki J,
Mhawech-Fauceglia P, Andrews C, Hoffman EW, Pan L, Ritter G,
Villella J, Thomas B, et al: Vaccination with an NY-ESO-1 peptide
of HLA class I/II specificities induces integrated humoral and T
cell responses in ovarian cancer. Proc Natl Acad Sci USA.
104:12837–12842. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sabbatini P, Tsuji T, Ferran L, Ritter E,
Sedrak C, Tuballes K, Jungbluth AA, Ritter G, Aghajanian C,
Bell-McGuinn K, et al: Phase I trial of overlapping long peptides
from a tumor self-antigen and poly-ICLC shows rapid induction of
integrated immune response in ovarian cancer patients. Clin Cancer
Res. 18:6497–6508. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Hato SV, Khong A, de Vries IJ and
Lesterhuis WJ: Molecular pathways: The immunogenic effects of
platinum-based chemotherapeutics. Clin Cancer Res. 20:2831–2837.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Hato SV, de Vries IJ and Lesterhuis WJ:
STATing the importance of immune modulation by platinum
chemotherapeutics. OncoImmunology. 1:234–236. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Diaz Y, Tundidor Y, Lopez A and Leon K:
Concomitant combination of active immunotherapy and carboplatin- or
paclitaxel-based chemotherapy improves anti-tumor response. Cancer
Immunol Immunother. 62:455–469. 2013. View Article : Google Scholar
|