Skin cancers are among the most common cancers
diagnosed in the United States. The incidence of melanoma of the
skin has risen in the last three decades and although melanoma
accounts for approximately 1% of all skin cancers it causes most of
the skin cancer deaths (1). When
melanoma is diagnosed in its early stages, surgical resection of
the lesion is associated with favorable prognosis. However, for
locally advanced and metastatic disease surgery is no longer
sufficient. The 5-year survival for localized melanoma is 99%, but
it is 20% when distant metastases are present (1).
Melanoma is one of the most sensitive tumors to
immune modulation. Several factors may explain melanoma cell
susceptibility to immune system activation including high tumor
mutational load due to ultraviolet light exposure, expression of
cancer testis antigens and mimicry of melanocyte lineage proteins
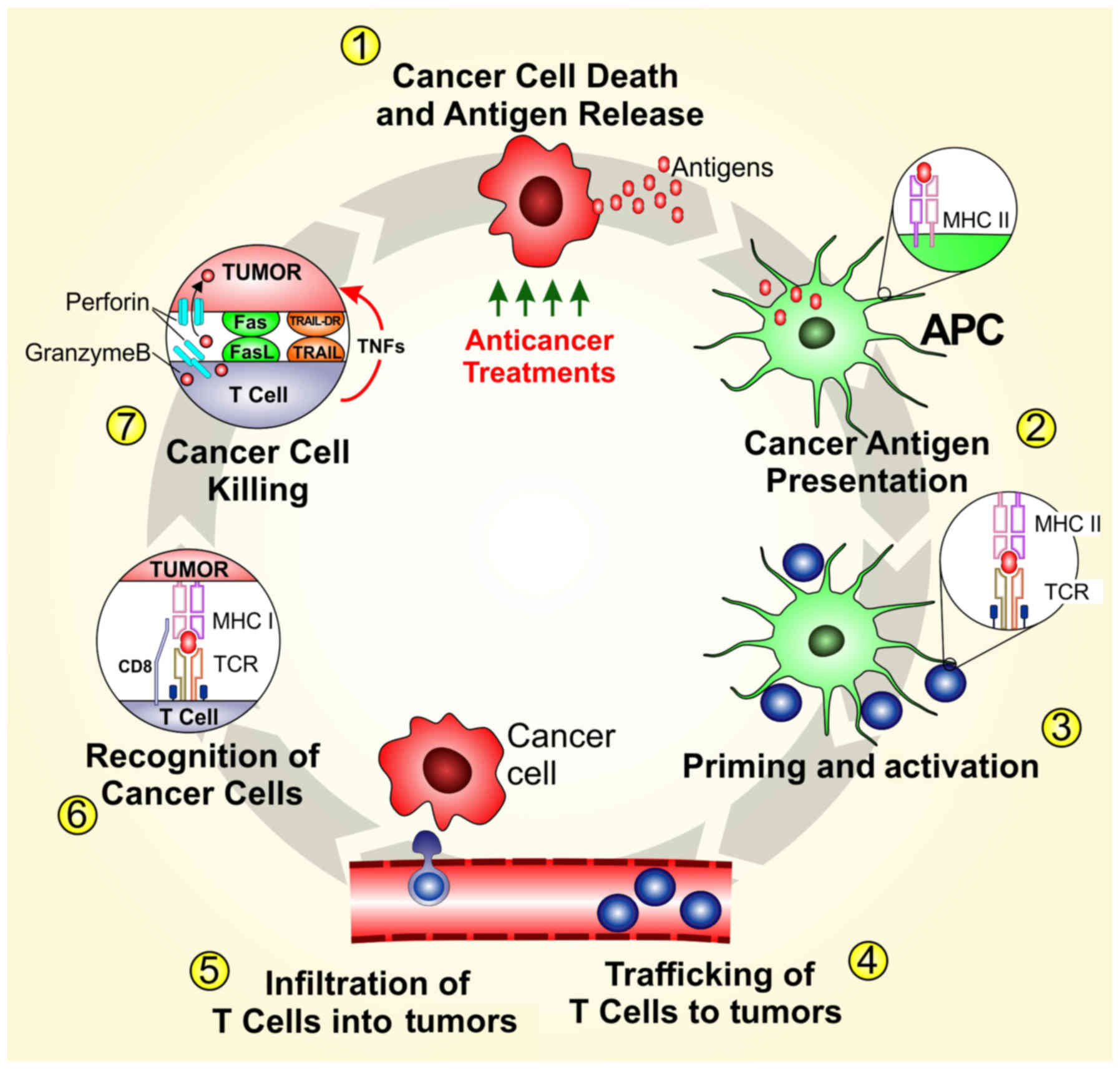
with pathogen-associated antigens (3-5). In
this context T-cell response seems to play a central role to keep
the melanoma at bay. Tumor infiltrated lymphocytes (TILs) are
central to the development of an anti-tumor immune response and a
subset of TILs demonstrate cytolytic activity against autologous
tumors in melanoma patients (Fig.
1) (6). Their presence also
correlates with increased survival and reduced risk of metastasis
(6). In the past decades several
clinical trials aimed at eliciting T-cell response with local or
systemic immunomodulatory drugs such as interferon (IFN)-α
(7,8), interleukin (IL)-2 (9,10),
cancer vaccines (11,12) and adoptive cell transfer (13). Despite some evidence of activity,
these trials failed to demonstrate sustained benefit in metastatic
melanoma patients. More recently, immune checkpoint inhibitors
(ICIs) against cytotoxic T-lymphocyte antigen-4 (CTLA-4) and
programmed death-1 (PD-1) have dramatically changed the management
of both unresectable and metastatic melanoma as well as those at
high risk for recurrence after resection (Table I) (14-16).
Unfortunately, primary and secondary resistance and the absence of
predictive markers of response are challenging problems with ICIs
therapy (17). Combination of
immunotherapy strategies aim to improve response and overcome
resistance, while biomarker discovery is fundamental for the
optimization of patient selection.
Herein, we review and discuss the rational of
approved immunotherapy treatments, of preclinical data and ongoing
clinical trials of combination strategies for advanced stage and
metastatic melanoma. An overview is also provided of biomarker
discovery and evidence on the role of gut microbioma in melanoma
immunotherapy.
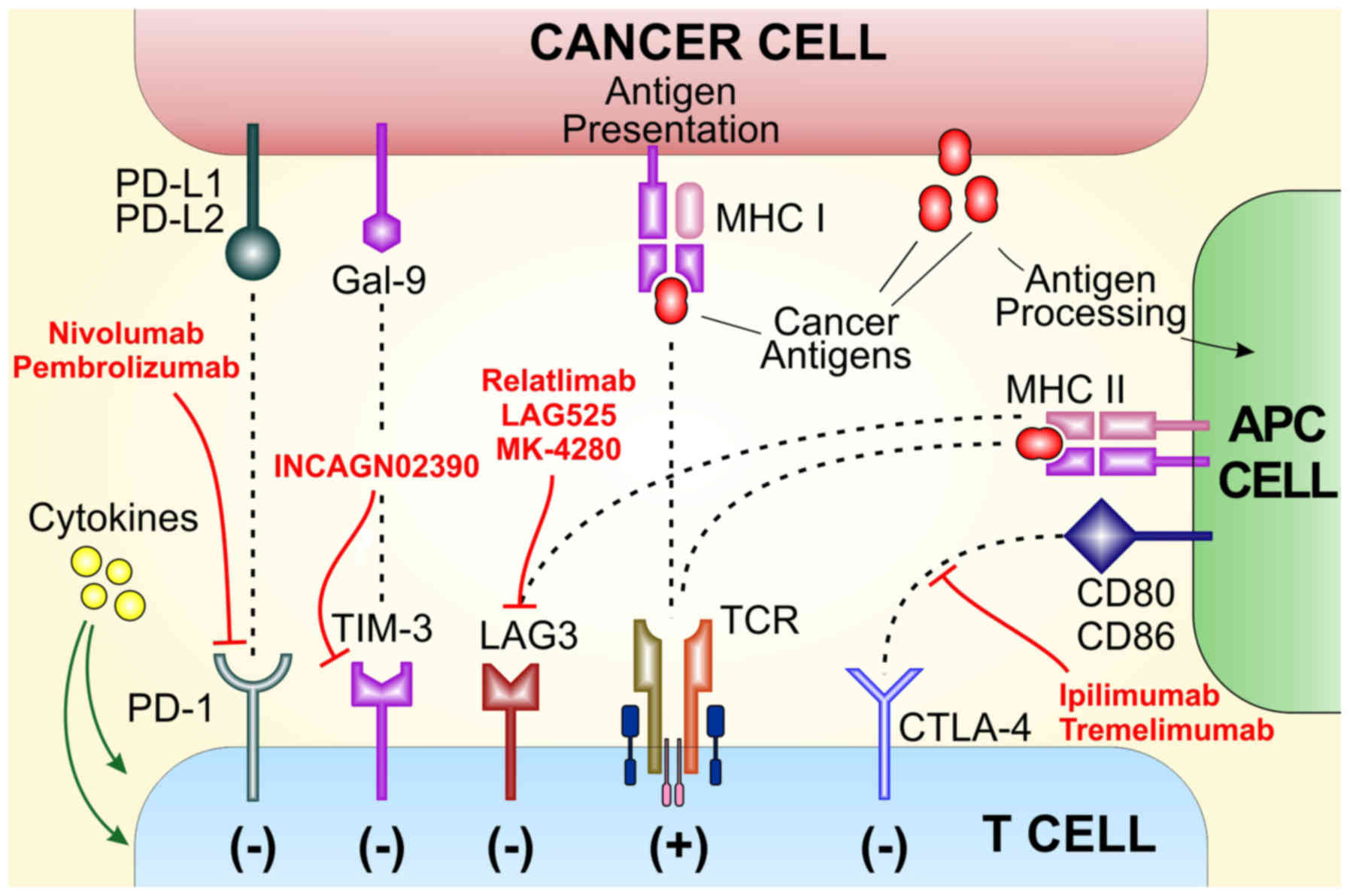
CTLA-4 is an inhibitory checkpoint receptor that
blocks T-cell activation and induces immune suppression (Fig. 2) (18). In 1996 Allison and colleagues
showed that CTLA-4 blockade could attenuate the growth of several
implanted murine tumors (19). In
2011 ipilimumab, a fully human monoclonal antibody (mAb) IgG1 that
inhibits the interaction between CTLA-4 and its ligands, was the
first ICI approved by the FDA. In previously treated patients with
advanced melanoma, ipili-mumab improved median overall survival
(OS) compared with gp100 peptide vaccine (10.6 vs. 6.4 months)
(20). At 3-years, the survival
rate was 22% followed by a plateau of the survival curve for up to
10 years (21). Combination
strategies of ipilimumab with IL-2 or Peg-IFN failed to show any
improvement over ipilimumab monotherapy (22,23).
Tremelimumab, another monoclonal antibody targeting CTLA-4, failed
to demonstrate a survival benefit over standard chemotherapy in a
phase III clinical trial (24). In
the adjuvant setting, a randomized clinical trial in resected stage
III patients showed that ipilimumab improves relapse-free survival
(RFS) and OS compared to placebo. However, more than 50% or
patients experienced grade 3-4 adverse events with ipilimumab and 5
patients (1.1%) died due to immune related adverse events (25).
PD-1 is an immune checkpoint with a central role in
immunopathology and tumor immune surveillance through effector
T-cell inhibition (Fig. 2)
(18). In 2014, two mAbs targeting
PD-1 (nivolumab and pembrolizumab) received FDA approval, becoming
first line treatment option in metastatic melanoma. Randomized
clinical trials have shown that monotherapy with nivolumab or
pembrolizumab is superior to ipilimumab alone (26). Pembrolizumab monotherapy in
treatment naïve and previously treated patients showed sustained
response rates of 30-40% (26-28).
In treatment of naïve patients pembrolizumab showed a 3-year OS
rate of 51% and a 5-year rate of 41% (29,30).
Clinical trials of nivolumab monotherapy provided durable response
rate of 32% in untreated patients and 40% in previously treated
melanoma (16,31). Three-year survival rate for
nivolumab in previously untreated patients is 42% (32) while 5-year survival rate in
previously treated patients with nivolumab monotherapy is 35%
(15). Cross study comparisons of
homogeneous groups of patients treated with pembrolizumab or
nivolumab monotherapy have similar results regarding clinical
endpoints and adverse event rates (33). At this time, no good predictive
biomarkers for anti-PD-1 mAbs are available and clinical benefit is
reached regardless of PD-L1 status (32). Since 2017, adjuvant immunotherapy
with single agent anti-PD-1 mAb is the first treatment option in
patients with resected stage III disease. Nivolumab improved RFS
compared to ipilimumab with lower toxicities (34). In a phase 3 double-blind trial
pembrolizumab treatment resulted in significantly longer RFS than
placebo with no new toxicities compared to other pembrolizumab
monotherapy trials (35).
Monotherapy with ICIs is associated with significant
improvement in patient survival, however, response rates are low.
With the attempt to increase the number of patients who benefit
from ICI therapy, combination of anti-CTLA-4 mAb plus anti-PD-1 mAb
have been evaluated in prospective clinical trials. In particular,
two randomized trials showed that the combination of anti-CTLA-4
plus anti-PD-1 mAbs results in increased clinical benefit compared
to single agent ipilimumab or nivolumab. The Checkmate-067, a phase
3 randomized clinical trial compared ipilimumab plus nivolumab to
nivolumab alone and ipilimumab alone in unresectable/metastatic
melanoma. Response rates were 57.6, 43.7 and 19%, respectively, and
5-year survival rates were 52% in the combination arm, 44% in the
nivolumab group and 26% in the ipilimumab arm (36,37).
The combination arm showed increased toxicity compared to each
monotherapy treatment arm. Specifically, treatment-related adverse
events of any grade occurred in 95% of patients in the combination
treatment group compared to 82% in the nivolumab arm and 86% in the
ipilimumab group. Grade 3 or 4 treatment related adverse events
occurred in 55% of the patients in the nivolumab plus ipilimumab
group, 16.3% of the patients in the nivolumab group and 27.3% of
those in the ipilimumab group (36). In 2015 the FDA approved the
combination ipilimumab plus nivolumab on the basis of overall
response rate and progression-free survival (PFS) improvement. In
an attempt of reducing the toxicity burden of the combination,
different dosing schedule by reducing ipilimumab dose and keep more
standard dose anti-PD-1 single agents were investigated. Although
the ORR appears to be conserved, the expected difference in terms
of efficacy and safety are small and only results from larger trial
will be conclusive (38,39). In patients with primary or
secondary resistance to single agent PD-1 mAbs, ICIs combination or
ipilimumab alone represent potential treatment strategies (40,41).
Currently, the respective benefits of combination immunotherapy
versus sequential immunotherapy are not yet fully understood and is
object of an open debate in the clinical and scientific community.
On one hand combination strategies are associated with increased
adverse events that can be justified by the intent of gaining
long-term disease response. On the other hand, the subset of
patients who benefit more from the combination is unknow
potentially exposing patients to unnecessary toxicities (42).
Brain metastases are a common cause of disabling
neurologic complications and poor prognosis in patients with
metastatic melanoma. The phase 2 clinical trial CheckMate-204
enrolled patients with small, untreated and asymptomatic brain
metastasis and showed that ipilimumab plus nivolumab have
clinically meaningful intracranial efficacy (56% of intracranial
response). The safety profile was similar to those reported for the
combination in patients without brain metastasis (43). Another phase 2 clinical trial
compared the combination of nivolumab plus ipilimumab versus
nivolumab alone. Despite the small sample size, ICIs combination
was superior to nivolumab monotherapy with a higher proportion of
patients achieving intracranial response (44).
No data are yet available on the potential benefit
of anti-CTLA-4 plus anti-PD-1 combination in the adjuvant setting.
Results from the clinical trial CheckMate-915 (NCT03068455) that
compare nivolumab monotherapy to nivolumab plus ipilimumab in
resected stage III melanoma are awaited.
T-VEC is a type I herpes simplex virus genetically
modified to preferentially replicate in tumor cells, enhance
antigen loading of MHC class I and express granulocyte-macrophage
colony-stimulating factor (GM-CSF) to increase tumor antigen
presentation by dendritic cells (DCs) (45). In 2015 T-VEC received approval by
the FDA for advanced melanoma. A phase 3 trial in unresected stage
IIIB-IV melanoma showed that intratumoral administration of T-VEC
improved response rate compared with GM-CSF (26 vs. 6%). Few
responses were obtained in distant non-injected lesions (mainly
lung and visceral sites) while the majority of responses were
limited to the site of injection and regional non-injected lesions
(46). The combination of T-VEC
and ICIs has shown interesting results. The phase II study of T-VEC
plus ipilimumab versus ipilimumab alone in patients with advanced
melanoma showed an improvement in ORR (39 vs. 18%, respectively)
(47). In the phase Ib trial
evaluating the association of T-VEC plus pembrolizumab, confirmed
objective response rate was 62%, with a complete response rate of
33% per immune-related response criteria (48). The results of the phase III trial
MASTERKEY-265/KEYNOTE-034 of T-VEC plus pembrolizumab compared with
pembrolizumab alone are awaited (NCT02263508).
Despite the impressive results obtained with
currently approved ICI treatments strategies, primary and secondary
resistance represent major clinical challenges. Several promising
immunomodulatory targets have been included in ongoing clinical
trials mainly in association with approved anti-PD-1 and
anti-CTLA-4 mAbs (Fig. 2).
LAG-3 is an immune checkpoint receptor found on the
cell surface of effector T cells and regulatory T cells. It is an
inhibitor regulator of T cell response, activation and growth
(49). Relatlimab, LAG525, and
MK-4280 are mAbs that targets LAG-3 and are currently under
investigation in combination with pembrolizumab or nivolumab
(50). While the inhibition of
LAG-3 alone has minor effect on T-cell reactivation, the
combination with anti-PD-1 mAb has shown encouraging results
(51,52).
Indoleamine 2,3-dioxygenase 1 (IDO1) is an enzyme
involved in tryptophan catabolism with a central immunosuppressive
function within the tumor microenvironment (54). Several IDO inhibitors (indiximod,
epacadostat and BMS-986205) are currently evaluated in clinical
trials in association with pembrolizumab, nivolumab or ipilimumab
(54). Regrettably, the phase III
clinical trial ECHO-301/KEYNOTE-252 in advanced melanoma failed to
demonstrate PFS benefit in the arm of pembrolizumab with epcadostat
compared to pembrolizumab alone (55).
Cytokines are the first class of immunomodula-tory
agents that have found clinical application in melanoma. Indeed,
IL-2 and IFN-α are both FDA approved for adjuvant treatment in
melanoma (7,56). Other cytokines such as IL-12,
IL-15, IL-18, IL-21 and GM-CSF have shown interesting results in
preclinical and clinical settings. However, single agent cytokine
strategy does not appear feasible due to their pleiotropic activity
and the critical toxicity profile especially at high dose (56). With this in mind, NTRK-214 is a
prodrug of conjugated IL-2, retaining the same amino acid sequence
as human recombinant IL-2. The IL-2 core is conjugated to 6
releasable polyethylene glycol (PEG) chains that in vivo
slowly release generating active IL-2 conjugates (57). An ongoing phase I/II clinical trial
aims to evaluate the tolerability and efficacy of NTRK-214 with
nivolumab and ipilimumab plus nivolumab (NCT02983045).
Tilsotolimod is a synthetic TLR-9 agonist
oligonucleotide that acts on macrophages and DCs and can stimulate
antigen presentation and T cell activation and proliferation.
Intratumoral tilsotolimod in combination with ipilimumab in PD-1
inhibitor refractory metastatic melanoma is well tolerated and
shows significant clinical benefit (ORR 38%) and durable response
(58). These favorable results
have led to an ongoing phase III study of tilsotolimod plus
ipilimumab versus ipilimumab alone (NCT03445533). Another
intratumoral TLR-9 agonist, SD-101, is in clinical development. The
phase Ib/II clinical trial SYNERGY-001/KEYNOTE-184 evaluates the
combination of SD-101 and pembrolizumab in patients with
unresectable stage IIIC-IV melanoma and naïve to PD-1 axis
inhibitors. Preliminary results show that the combination is
well-tolerated, with promising high response rates and PFS
(59). CD40 is expressed on
macrophages and other antigen-presenting cells and its agonists
stimulate maturation and increase macrophage killing activity
against tumor cells (60). On the
other hand, tumor-associated macrophages can be characterized by
tumor-promoting phenotype (61).
This phenotype is a consequence, among other factors, of the
continuous activation of the colony-stimulating factor-1 (CSF-1)
axis (62). An ongoing phase I/Ib
trial is evaluating the safety and efficacy of the CSF-1 receptor
inhibitor, cabiralizumab, combined with the CD40 agonist, APX005M,
with or without nivolumab in patients with advanced melanoma
(NCT03502330).
Therapeutic cancer vaccines aim at inducing a
specific immune response against tumor antigens. In melanoma
patients, peptide vaccines have been tested in association with
ipilimumab, but failed to demonstrate an advantage compared to
ipilimumab alone (20,63). In a phase I clinical trial,
tremelimumab plus MART-1 peptide-pulsed DCs resulted in objective
and durable tumor responses compared to each agent alone (64). A phase I trial in patients with
pretreated advanced melanoma showed that autologous
monocyte-derived DCs electroporated with synthetic mRNA
(TriMixDC-MEL) are immunogenic and have antitumor activity
(65). TriMixDC-MEL combined with
ipilimumab has shown 38% of durable tumor responses in a phase II
trial (66). The tumor lysate,
particle-loaded, dendritic cell (TLPLDC) vaccine uses yeast cell
wall particles to load tumor lysate into autologous DCs. The phase
IIb trial of TLPLDC vs. placebo in resected stage III/IV patients
showed an increased 24-month DFS. The trial showed also a potential
synergistic effect of TLPLDC plus ipilimumab to be confirmed in a
phase III study evaluating adjuvant TLPLDC plus ipilimumab versus
ipilimumab alone in resected stage IV patients (67).
The presence of tumor-reactive T cells has been
associated with the success of ICIs (68,69).
When patients do not have functional tumor-antigen-specific T cells
with high-affinity T cell receptors (TCRs), T cell therapies can
transfer such T cell populations by either expanding pre-existing
anti-tumor T cells or by using gene-therapy to alter T cells to
become melanoma-specific with a high-affinity TCR (70). ACT of autologous tumor infiltrating
lymphocytes with high-dose IL-2 was the first clinical trial to
show that tumor-reactive T cells could mediate melanoma regression
(71). However, TIL has not been
approved as anti-cancer treatment yet due to lack of results from
sufficiently powered prospective randomized clinical trials
(13,72). In order to improve clinical benefit
and survival, TIL therapy could be combined with other
immunotherapies (70). ACT through
chimeric antigen receptor (CAR) T-cell therapy has been successful
in hematological malignancies. However, less response was seen in
the treatment of solid tumors such as melanoma (73). Combination of CAR-T therapy and
immune checkpoint blockade, targeted therapy might induce desired
clinical responses (73). The
adoptive transfer of autologous T cells transduced with a
retrovirus encoding a TCR against an HLA-A*0201 restricted NY-ESO-1
epitope is a potentially effective treatment for some refractory
metastatic melanoma patients (74).
Targeted therapy and ICIs have radically changed the
management of different tumor types, including advanced stage
melanoma (75). However, both
approaches have limitations, including limited duration of response
with targeted therapy and low overall response rate without clear
predictive biomarkers in patients treated with ICIs. Therefore,
great interest has been shown on the possibility of combination
strategies that could take advantage from the high response rate of
targeted therapy with the long-term disease control of ICIs.
Despite some contrasting preclinical results that have been
observed on the association of BRAF and MEK inhibitors with
immunotherapy, various trials are ongoing investigating the
association of MAPK inhibitors with ICIs and other immunotherapy
strategies (76). Several trials
with CTLA-4 inhibitors and MAPK inhibitors have raised concerns due
to the toxicities associated with the combinations that led to
early trial termination (77,78).
More tolerable and with good disease control rates seem to be the
association of PD-1/PD-L1 axis inhibitors with BRAF and MEK
inhibitors (79). In this context,
study design is fundamental to properly conduct clinical trial of
combination strategies without increasing toxicities. The ongoing
phase III clinical trial DREAMseq (NCT02224781) studies how well
initial treatment works with ipilimumab and nivolumab followed by
dabrafenib and trametinib, and compares it to initial treatment
with dabrafenib and trametinib followed by ipilimumab and nivolumab
in treating patients with stage III-IV BRAF V600 melanoma.
The improvement of clinical efficacy of
immunotherapy strategies is a central goal of translational and
clinical research in immunooncology. In recent years, several
factors have been shown to influence the immune response during ICI
treatment (80-83). In this context, the human
microbiota seems to be an important modulator of the immune system
response in different physiopathological conditions, including
cancer development and response to anti-cancer treatment (84). In a melanoma mouse model, different
commensal gut microbiota composition was associated with difference
in melanoma growth and spontaneous antitumor immunity which were
eliminated upon cohousing or after fecal transfer (85). In a RET melanoma mouse model with
dysbiosis induced by antibiotic treatment, gut colonization with
Akkermansia muciniphila restored responsiveness to PD-1
blockade compared to control and increased the recruitment of
CD4+ T lymphocytes into mouse tumor beds (86). In 112 melanoma patients treated
with anti-PD-1 mAbs, significant differences were observed in the
gut microbiome of responders versus non-responders. Analysis of
patient fecal microbiome samples showed significantly higher
species diversity and relative abundance of the Ruminococcaceae
family in responding patients. Moreover, mice receiving fecal
microbiota transplantation (FMT) with stool from responders to PD-1
inhibitors also exhibited improved response to anti-PD-L1 therapy
compared to mice transplanted with stool from melanoma patients
that did not respond to anti-PD-L1 therapy (87). Several preclinical and clinical
works show the relevance of the modulation of the gut microbiota in
ICIs efficacy (88-91). Taken together these data sustain
potential use of the human microbiome as a predictive biomarker of
response to ICIs. Moreover, the modulation of specific component of
the human microbiome by FMT or oral supplementation through
probiotics may improve response rates and other clinical endpoints
of ICIs therapy in cancer patients. Prospective randomized clinical
trials are awaited to better understand the impact of such
approaches.
Targeted therapy derives its efficacy from the
presence of a specific tumor feature, such as the BRAF V600
mutation, that drives tumor growth and that represent a specific
biomarker of response to the drug targeting the aberrant pathway.
In melanoma, primary and secondary resistance to targeted therapy
are challenging problems and several studies have tried to improve
BRAF V600 detection of prognostic and predictive markers (92-94).
Despite great efforts, melanoma immunotherapy and especially ICIs,
which are already approved for clinical use, lack biomarker
response. This is especially urgent due to the relatively low
response rate of immunotherapy. Regarding inhibitors of PD-1/PD-L1
axis, PD-L1 expression assessed by immunohistochemistry (IHC)
staining has been used as biomarkers in several clinical trials.
Different PD-L1 IHC antibodies with non-homogeneous cut-off values
among studies have generated contrasting results on the role of
PD-L1 for patient stratification (26,31,36).
Although PD-L1 status is not currently considered a valid
stratification marker, it warrants further analysis since it may
indicate underlying biological insights (95). More comprehensive models are under
investigation to better characterize the tumor microenvironment and
define predictive biomarkers for immunotherapy. In this context an
important study by Tumeh and collaborators (96) has shown that the presence of
CD8+ T cells that cause upregulation of PD-L1 expression
on melanoma cells at the invasive tumor margin might more clearly
explain primary resistance or responsiveness to anti-PD-1 mAbs.
Gene-expression profile has been suggested as a marker of response
(97). IFNγ secreted by
CD8+ T cells is the principal mediator of intratumoural
antitumor inflammation, a gene expression profile termed
'T-cell-inflamed tumor' has been associated with response to
diverse immunotherapies including IL-2, vaccines, ICIs and cancer
vaccine (98,99). Moreover, primary and secondary
resistance to PD-1/PD-L1 pathway inhibitors is associated with a
low IFNγ gene expression signature that can be mediated by
activation of PTEN and WNT/β-catenin pathway, impairment of JAK2
signaling or alteration of antigen presentation through structural
or functional impairment of MHC class I mediated antigen
presentation (100-103). A study with the largest whole
exome sequencing and transcriptome sequencing analysis of tumor
material from patients with metastatic melanoma receiving
immune-checkpoint inhibitors has been published (104). The study supports the
correlations between baseline immune infiltrate and treatment
response, but also show inconsistent associations of tumor
mutational burden, and prove that multiple novel genomic and
transcriptomic features predict selective response, including
features associated with MHC-I and MHC-II antigen presentation
(104). Moreover, the authors
constructed predictive models integrating clinical, genomic and
transcriptomic characteristics to identify patients with melanoma
with intrinsic resistance to anti-PD1 mAb (104). Recently, a growing body of
evidence is trying to correlate ICI efficacy to the expression
levels of PD-L1 detected in circulating tumor DNA (105,106). Finally, studies have proposed the
analysis of matrix metalloproteinase (MMPs), known to be strictly
involved in melanoma growth (107,108), as good indicator of response to
immunotherapy. Moogk and colleagues (109) showed an inverse association
between anti-tumor T-cell response and MMP-23 expression in primary
melanoma tumors treated with adjuvant immunotherapy. The authors
concluded that MMP-23 expression is associated with shorter periods
of PFS and therefore may represent a potential therapeutic target
in melanoma, as well as a possible biomarker for evaluating
response of melanoma patients to immunotherapies.
The number of effective treatments for patients with
metastatic melanoma have increased rapidly in recent few years. In
this scenario, immunotherapy combinations and immunotherapy plus
targeted therapy hold great expectation. Moreover, results from the
clinical trial DREAMseq are eagerly awaited and will shed light on
the best sequential treatment option in metastatic melanoma
patients with BRAF V600E. Given the complexity of the antitumor
immune response, the identification of biomarkers of response and
the mechanisms associated with primary and secondary resistance are
of utmost importance. These insights will allow the next generation
of immunotherapy approaches that will be tailored on specific
melanoma genomic features and its tumor microenvironment
characteristics.
Not applicable.
This study was partially supported by the Italian
League against Cancer (LILT).
GCL conceived the work, performed bibliographic
research and wrote the manuscript, SC prepared the figures and
provided critical revisions, LF performed bibliographic research
and provided critical revisions, DAS, ML contributed to the
conception of the work and provided critical revisions. All authors
agreed on the final version of the manuscript.
GCL, SC, LF, ML no competing interest to declare,
DAS is the Editor-in-Chief for the journal, but had no personal
involvement in the reviewing process, or any influence in terms of
adjudicating on the final decision, for this article.
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2018. CA Cancer J Clin. 68:7–30. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Leonardi GC, Falzone L, Salemi R, Zanghì
A, Spandidos DA, McCubrey JA, Candido S and Libra M: Cutaneous
melanoma: From pathogenesis to therapy (Review). Int J Oncol.
52:1071–1080. 2018.PubMed/NCBI
|
|
3
|
Candido S, Rapisarda V, Marconi A,
Malaponte G, Bevelacqua V, Gangemi P, Scalisi A, McCubrey JA,
Maestro R, Spandidos DA, et al: Analysis of the B-RafV600E mutation
in cutaneous melanoma patients with occupational sun exposure.
Oncol Rep. 31:1079–1082. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kawakami Y and Rosenberg SA: T-cell
recognition of self peptides as tumor rejection antigens. Immunol
Res. 15:179–190. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Faramarzi S and Ghafouri-Fard S: Melanoma:
A prototype of cancer-testis antigen-expressing malignancies.
Immunotherapy. 9:1103–1113. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lee N, Zakka LR, Mihm MC Jr and Schatton
T: Tumour-infiltrating lymphocytes in melanoma prognosis and cancer
immunotherapy. Pathology. 48:177–187. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kirkwood JM, Ibrahim JG, Sosman JA, Sondak
VK, Agarwala SS, Ernstoff MS and Rao U: High-dose interferon
alfa-2b significantly prolongs relapse-free and overall survival
compared with the GM2-KLH/QS-21 vaccine in patients with resected
stage IIB-III melanoma: Results of intergroup trial
E1694/S9512/C509801. J Clin Oncol. 19:2370–2380. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wheatley K, Ives N, Hancock B, Gore M,
Eggermont A and Suciu S: Does adjuvant interferon-alpha for
high-risk melanoma provide a worthwhile benefit? A meta-analysis of
the randomised trials. Cancer Treat Rev. 29:241–252. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Atkins MB, Kunkel L, Sznol M and Rosenberg
SA: High-dose recombinant interleukin-2 therapy in patients with
metastatic melanoma: Long-term survival update. Cancer J Sci Am.
6(Suppl 1): S11–S14. 2000.PubMed/NCBI
|
|
10
|
Rosenberg SA: IL-2: The first effective
immunotherapy for human cancer. J Immunol. 192:5451–5458. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Klebanoff CA, Acquavella N, Yu Z and
Restifo NP: Therapeutic cancer vaccines: Are we there yet? Immunol
Rev. 239:27–44. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Schwartzentruber DJ, Lawson DH, Richards
JM, Conry RM, Miller DM, Treisman J, Gailani F, Riley L, Conlon K,
Pockaj B, et al: gp100 peptide vaccine and interleukin-2 in
patients with advanced melanoma. N Engl J Med. 364:2119–2127. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rohaan MW, van den Berg JH, Kvistborg P
and Haanen JBAG: Adoptive transfer of tumor-infiltrating
lymphocytes in melanoma: A viable treatment option. J Immunother
Cancer. 6:1022018. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ascierto PA, McArthur GA, Dréno B,
Atkinson V, Liszkay G, Di Giacomo AM, Mandalà M, Demidov L,
Stroyakovskiy D, Thomas L, et al: Cobimetinib combined with
vemurafenib in advanced BRAF(V600)-mutant melanoma (coBRIM):
Updated efficacy results from a randomised, double-blind, phase 3
trial. Lancet Oncol. 17:1248–1260. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hodi FS, Kluger H, Sznol M, Carvajal R,
Lawrence D, Atkins M, Powderly J, Sharfman W, Puzanov I, et al:
Durable, long-term survival in previously treated patients with
advanced melanoma (MEL) who received nivolumab (NIVO) monotherapy
in a phase I trial. Cancer Res. 76:CT0012016.
|
|
16
|
Weber JS, D'Angelo SP, Minor D, Hodi FS,
Gutzmer R, Neyns B, Hoeller C, Khushalani NI, Miller WH Jr, Lao CD,
et al: Nivolumab versus chemotherapy in patients with advanced
melanoma who progressed after anti-CTLA-4 treatment (CheckMate
037): A randomised, controlled, open-label, phase 3 trial. Lancet
Oncol. 16:375–384. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Christofi T, Baritaki S, Falzone L, Libra
M and Zaravinos A: Current perspectives in cancer immunotherapy.
Cancers (Basel). 11:14722019. View Article : Google Scholar
|
|
18
|
Wei SC, Duffy CR and Allison JP:
Fundamental mechanisms of immune checkpoint blockade therapy.
Cancer Discov. 8:1069–1086. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Leach DR, Krummel MF and Allison JP:
Enhancement of antitumor immunity by CTLA-4 blockade. Science.
271:1734–1736. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hodi FS, O'Day SJ, McDermott DF, Weber RW,
Sosman JA, Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel
JC, et al: Improved survival with ipilimumab in patients with
metastatic melanoma. N Engl J Med. 363:711–723. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Schadendorf D, Hodi FS, Robert C, Weber
JS, Margolin K, Hamid O, Patt D, Chen TT, Berman DM and Wolchok JD:
Pooled analysis of long-term survival data from phase II and phase
III trials of ipilimumab in unresectable or metastatic melanoma. J
Clin Oncol. 33:1889–1894. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Weide B, Martens A, Wistuba-Hamprecht K,
Zelba H, Maier L, Lipp HP, Klumpp BD, Soffel D, Eigentler TK and
Garbe C: Combined treatment with ipilimumab and intratumoral
interleukin-2 in pretreated patients with stage IV melanoma-safety
and efficacy in a phase II study. Cancer Immunol Immunother.
66:441–449. 2017. View Article : Google Scholar
|
|
23
|
Brohl AS, Khushalani NI, Eroglu Z,
Markowitz J, Thapa R, Chen YA, Kudchadkar R and Weber JS: A phase
IB study of ipilimumab with peginterferon alfa-2b in patients with
unre-sectable melanoma. J Immunother Cancer. 4:852016. View Article : Google Scholar
|
|
24
|
Ribas A, Kefford R, Marshall MA, Punt CJ,
Haanen JB, Marmol M, Garbe C, Gogas H, Schachter J, Linette G, et
al: Phase III randomized clinical trial comparing tremelimumab with
standard-of-care chemotherapy in patients with advanced melanoma. J
Clin Oncol. 31:616–622. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Eggermont AM, Chiarion-Sileni V, Grob JJ,
Dummer R, Wolchok JD, Schmidt H, Hamid O, Robert C, Ascierto PA,
Richards JM, et al: Prolonged survival in stage III melanoma with
ipilimumab adjuvant therapy. N Engl J Med. 375:1845–1855. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Robert C, Schachter J, Long GV, Arance A,
Grob JJ, Mortier L, Daud A, Carlino MS, McNeil C, Lotem M, et al
KEYNOTE-006 investigators: Pembrolizumab versus ipilimumab in
advanced melanoma. N Engl J Med. 372:2521–2532. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ribas A, Hamid O, Daud A, Hodi FS, Wolchok
JD, Kefford R, Joshua AM, Patnaik A, Hwu WJ, Weber JS, et al:
Association of pembrolizumab with tumor response and survival among
patients with advanced melanoma. JAMA. 315:1600–1609. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Schachter J, Ribas A, Long GV, Arance A,
Grob JJ, Mortier L, Daud A, Carlino MS, McNeil C, Lotem M, et al:
Pembrolizumab versus ipilimumab for advanced melanoma: Final
overall survival results of a multicentre, randomised, open-label
phase 3 study (KEYNOTE-006). Lancet. 390:1853–1862. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Hamid O, Robert C, Daud A, Hodi FS, Hwu
WJ, Kefford R, Wolchok JD, Hersey P, Joseph R, Weber JS, et al:
Five-year survival outcomes for patients with advanced melanoma
treated with pembrolizumab in KEYNOTE-001. Ann Oncol. 30:582–588.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Robert C, Ribas A, Schachter J, Arance A,
Grob JJ, Mortier L, Daud A, Carlino MS, McNeil CM, Lotem M, et al:
Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006):
Post-hoc 5-year results from an open-label, multicentre,
randomised, controlled, phase 3 study. Lancet Oncol. 20:1239–1251.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Robert C, Long GV, Brady B, Dutriaux C,
Maio M, Mortier L, Hassel JC, Rutkowski P, McNeil C,
Kalinka-Warzocha E, et al: Nivolumab in previously untreated
melanoma without BRAF mutation. N Engl J Med. 372:320–330. 2015.
View Article : Google Scholar
|
|
32
|
Ascierto PA, Long GV, Robert C, Brady B,
Dutriaux C, Di Giacomo AM, Mortier L, Hassel JC, Rutkowski P,
McNeil C, et al: Survival outcomes in patients with previously
untreated BRAF wild-type advanced melanoma treated with nivolumab
therapy: Three-year follow-up of a randomized phase 3 trial. JAMA
Oncol. 5:187–194. 2019. View Article : Google Scholar :
|
|
33
|
Weiss SA, Wolchok JD and Sznol M:
Immunotherapy of melanoma: Facts and hopes. Clin Cancer Res.
25:5191–5201. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Weber J, Mandala M, Del Vecchio M, Gogas
HJ, Arance AM, Cowey CL, Dalle S, Schenker M, Chiarion-Sileni V,
Marquez-Rodas I, et al CheckMate 238 Collaborators: Adjuvant
nivolumab versus ipilimumab in resected stage III or IV melanoma. N
Engl J Med. 377:1824–1835. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Eggermont AMM, Blank CU, Mandala M, Long
GV, Atkinson V, Dalle S, Haydon A, Lichinitser M, Khattak A,
Carlino MS, et al: Adjuvant pembrolizumab versus placebo in
resected stage III melanoma. N Engl J Med. 378:1789–1801. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Larkin J, Chiarion-Sileni V, Gonzalez R,
Grob JJ, Cowey CL, Lao CD, Schadendorf D, Dummer R, Smylie M,
Rutkowski P, et al: Combined nivolumab and ipilimumab or
monotherapy in untreated melanoma. N Engl J Med. 373:23–34. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Larkin J, Chiarion-Sileni V, Gonzalez R,
Grob JJ, Rutkowski P, Lao CD, Cowey CL, Schadendorf D, Wagstaff J,
Dummer R, et al: Five-year survival with combined nivolumab and
ipilimumab in advanced melanoma. N Engl J Med. 381:1535–1546. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Kirchberger MC, Hauschild A, Schuler G and
Heinzerling L: Combined low-dose ipilimumab and pembrolizumab after
sequential ipilimumab and pembrolizumab failure in advanced
melanoma. Eur J Cancer. 65:182–184. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Long GV, Atkinson V, Cebon JS, Jameson MB,
Fitzharris BM, McNeil CM, Hill AG, Ribas A, Atkins MB, Thompson JA,
et al: Standard-dose pembrolizumab in combination with reduced-dose
ipilimumab for patients with advanced melanoma (KEYNOTE-029): An
open-label, phase 1b trial. Lancet Oncol. 18:1202–1210. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Zimmer L, Apuri S, Eroglu Z, Kottschade
LA, Forschner A, Gutzmer R, Schlaak M, Heinzerling L, Krackhardt
AM, Loquai C, et al: Ipilimumab alone or in combination with
nivolumab after progression on anti-PD-1 therapy in advanced
melanoma. Eur J Cancer. 75:47–55. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Long GV, Robert C, Blank C, Ribas A,
Mortier L, Schachter J, Middleton MR, et al: Outcomes in patients
treated with ipilimumab after pembrolizumab in KEYNOTE-006. Eur J
Cancer. 72:S128–S129. 2017. View Article : Google Scholar
|
|
42
|
Ascierto PA, Butterfield LH, Demaria S,
Ferris RL, Freeman GJ, Lo RS, Mantovani A, Nathan P, Hamid O,
Politi K, et al: The great debate at 'Immunotherapy Bridge 2018',
Naples, November 29th, 2018. J Immunother Cancer. 7:2212019.
View Article : Google Scholar
|
|
43
|
Tawbi HA, Forsyth PA, Algazi A, Hamid O,
Hodi FS, Moschos SJ, Khushalani NI, Lewis K, Lao CD, Postow MA, et
al: Combined nivolumab and ipilimumab in melanoma metastatic to the
brain. N Engl J Med. 379:722–730. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Long GV, Atkinson V, Lo S, Sandhu S,
Guminski AD, Brown MP, Wilmott JS, Edwards J, Gonzalez M, Scolyer
RA, et al: Combination nivolumab and ipilimumab or nivolumab alone
in melanoma brain metastases: A multicentre randomised phase 2
study. Lancet Oncol. 19:672–681. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Conry RM, Westbrook B, McKee S and Norwood
TG: Talimogene laherparepvec: First in class oncolytic virotherapy.
Hum Vaccin Immunother. 14:839–846. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Andtbacka RH, Kaufman HL, Collichio F,
Amatruda T, Senzer N, Chesney J, Delman KA, Spitler LE, Puzanov I,
Agarwala SS, et al: Talimogene laherparepvec improves durable
response rate in patients with advanced melanoma. J Clin Oncol.
33:2780–2788. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Chesney J, Puzanov I, Collichio F, Singh
P, Milhem MM, Glaspy J, Hamid O, Ross M, Friedlander P, Garbe C, et
al: Randomized, open-label phase II study evaluating the efficacy
and safety of talimogene laherparepvec in combination with
ipilimumab versus ipilimumab alone in patients with advanced,
unresectable melanoma. J Clin Oncol. 36:1658–1667. 2018. View Article : Google Scholar :
|
|
48
|
Ribas A, Dummer R, Puzanov I, Vander Walde
A, Andtbacka RHI, Michielin O, Olszanski AJ, Malvehy J, Cebon J,
Fernandez E, et al: Oncolytic virotherapy promotes intratumoral T
cell infiltration and improves anti-PD-1 immunotherapy. Cell.
174:1031–1032. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Durham NM, Nirschl CJ, Jackson CM, Elias
J, Kochel CM, Anders RA and Drake CG: Lymphocyte activation gene 3
(LAG-3) modulates the ability of CD4 T-cells to be suppressed in
vivo. PLoS One. 9:e1090802014. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Andrews LP, Marciscano AE, Drake CG and
Vignali DA: LAG3 (CD223) as a cancer immunotherapy target. Immunol
Rev. 276:80–96. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Woo SR, Turnis ME, Goldberg MV, Bankoti J,
Selby M, Nirschl CJ, Bettini ML, Gravano DM, Vogel P, Liu CL, et
al: Immune inhibitory molecules LAG-3 and PD-1 synergistically
regulate T-cell function to promote tumoral immune escape. Cancer
Res. 72:917–927. 2012. View Article : Google Scholar
|
|
52
|
Ascierto PA, Bono P, Bhatia S, Melero I,
Nyakas MS, Svane I, Larkin J, Gomez-Roca C, Schadendorf D, Dummer
R, et al: LBA18Efficacy of BMS-986016, a monoclonal antibody that
targets lymphocyte activation gene-3 (LAG-3), in combination with
nivolumab in pts with melanoma who progressed during prior
anti-PD-1/PD-L1 therapy (mel prior IO) in all-comer and
biomarker-enriched populations. Ann Oncol. 28(Suppl 5): v605–v649.
2017. View Article : Google Scholar
|
|
53
|
Das M, Zhu C and Kuchroo VK: Tim-3 and its
role in regulating anti-tumor immunity. Immunol Rev. 276:97–111.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Ricciuti B, Leonardi GC, Puccetti P,
Fallarino F, Bianconi V, Sahebkar A, Baglivo S, Chiari R and Pirro
M: Targeting indoleamine-2,3-dioxygenase in cancer: Scientific
rationale and clinical evidence. Pharmacol Ther. 196:105–116. 2019.
View Article : Google Scholar
|
|
55
|
Long GV, Dummer R, Hamid O, Gajewski TF,
Caglevic C, Dalle S, Arance A, Carlino MS, Grob JJ, Kim TM, et al:
Epacadostat plus pembrolizumab versus placebo plus pembrolizumab in
patients with unresectable or metastatic melanoma
(ECHO-301/KEYNOTE-252): A phase 3, randomised, double-blind study.
Lancet Oncol. 20:1083–1097. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Nicholas C and Lesinski GB:
Immunomodulatory cytokines as therapeutic agents for melanoma.
Immunotherapy. 3:673–690. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Charych DH, Hoch U, Langowski JL, Lee SR,
Addepalli MK, Kirk PB, Sheng D, Liu X, Sims PW, VanderVeen LA, et
al: NKTR-214, an engineered cytokine with biased IL2 receptor
binding, increased tumor exposure, and marked efficacy in mouse
tumor models. Clin Cancer Res. 22:680–690. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Diab A, Haymaker C, Bernatchez C,
Andtbacka RHI, Shaheen M, Johnson D, Markowitz J, Puzanov I, Murthy
R, Johnson DH, et al: Intratumoral (it) injection of the TLR9
agonist tilsotolimod (imo-2125) in combination with ipilimumab
(ipi) triggers durable responses in pd-1 inhibitor refractory
metastatic melanoma (rmm): results from a multicenter, phase 1/2
study. Ann Oncol. 29(Suppl 8): viii442–viii466. 2018. View Article : Google Scholar
|
|
59
|
Milhem MM, Long GV, Hoimes CJ, Amin A, Lao
CD, Conry RM, Hunt J, Daniels GA, Almubarak M, Shaheen MF, et al:
Phase 1b/2, open label, multicenter, study of the combination of
SD-101 and pembrolizumab in patients with advanced melanoma who are
naïve to anti-PD-1 therapy. J Clin Oncol. 37(Suppl 15): 9534. 2019.
View Article : Google Scholar
|
|
60
|
Wiehagen KR, Girgis NM, Yamada DH, Smith
AA, Chan SR, Grewal IS, Quigley M and Verona RI: Combination of
CD40 agonism and CSF-1R blockade reconditions tumor-associated
macrophages and drives potent antitumor immunity. Cancer Immunol
Res. 5:1109–1121. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Mantovani A, Marchesi F, Malesci A, Laghi
L and Allavena P: Tumour-associated macrophages as treatment
targets in oncology. Nat Rev Clin Oncol. 14:399–416. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Cannarile MA, Weisser M, Jacob W, Jegg AM,
Ries CH and Rüttinger D: Colony-stimulating factor 1 receptor
(CSF1R) inhibitors in cancer therapy. J Immunother Cancer.
5:532017. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Sarnaik AA, Yu B, Yu D, Morelli D, Hall M,
Bogle D, Yan L, Targan S, Solomon J, Nichol G, et al: Extended dose
ipilimumab with a peptide vaccine: Immune correlates associated
with clinical benefit in patients with resected high-risk stage
IIIc/IV melanoma. Clin Cancer Res. 17:896–906. 2011. View Article : Google Scholar :
|
|
64
|
Ribas A, Comin-Anduix B, Chmielowski B,
Jalil J, de la Rocha P, McCannel TA, Ochoa MT, Seja E, Villanueva
A, Oseguera DK, et al: Dendritic cell vaccination combined with
CTLA4 blockade in patients with metastatic melanoma. Clin Cancer
Res. 15:6267–6276. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Wilgenhof S, Van Nuffel AM, Benteyn D,
Corthals J, Aerts C, Heirman C, Van Riet I, Bonehill A, Thielemans
K and Neyns B: A phase IB study on intravenous synthetic mRNA
electroporated dendritic cell immunotherapy in pretreated advanced
melanoma patients. Ann Oncol. 24:2686–2693. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Wilgenhof S, Corthals J, Heirman C, van
Baren N, Lucas S, Kvistborg P, Thielemans K and Neyns B: Phase II
study of autologous monocyte-derived mRNA electroporated dendritic
cells (TriMixDC-MEL) plus ipilimumab in patients with pretreated
advanced melanoma. J Clin Oncol. 34:1330–1338. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Chick RC, Faries MB, Hale DF, Kemp Bohan
PM, Hickerson A, Vreelandc TJ, Myers JW, Cindass JL, Brown TA, et
al: Multi-institutional, prospective, randomized, double-blind,
placebo-controlled phase IIb trial of the tumor lysate,
particle-loaded, dendritic cell (TLPLDC) vaccine to prevent
recurrence in high-risk melanoma patients: A subgroup analysis. J
Clin Oncol. 38(Suppl 5): 63. 2020. View Article : Google Scholar
|
|
68
|
Kvistborg P, Philips D, Kelderman S,
Hageman L, Ottensmeier C, Joseph-Pietras D, Welters MJ, van der
Burg S, Kapiteijn E, Michielin O, et al: Anti-CTLA-4 therapy
broadens the melanoma-reactive CD8+ T cell response. Sci
Transl Med. 6:254ra1282014. View Article : Google Scholar
|
|
69
|
Daud AI, Loo K, Pauli ML,
Sanchez-Rodriguez R, Sandoval PM, Taravati K, Tsai K, Nosrati A,
Nardo L, Alvarado MD, et al: Tumor immune profiling predicts
response to anti-PD-1 therapy in human melanoma. J Clin Invest.
126:3447–3452. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Foley KC, Nishimura MI and Moore TV:
Combination immunotherapies implementing adoptive T-cell transfer
for advanced-stage melanoma. Melanoma Res. 28:171–184. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Rosenberg SA, Packard BS, Aebersold PM,
Solomon D, Topalian SL, Toy ST, Simon P, Lotze MT, Yang JC, Seipp
CA, et al: Use of tumor-infiltrating lymphocytes and interleukin-2
in the immunotherapy of patients with metastatic melanoma. A
preliminary report N Engl J Med. 319:1676–1680. 1988.
|
|
72
|
Rosenberg SA, Yang JC, Sherry RM, Kammula
US, Hughes MS, Phan GQ, Citrin DE, Restifo NP, Robbins PF,
Wunderlich JR, et al: Durable complete responses in heavily
pretreated patients with metastatic melanoma using T-cell transfer
immunotherapy. Clin Cancer Res. 17:4550–4557. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Feins S, Kong W, Williams EF, Milone MC
and Fraietta JA: An introduction to chimeric antigen receptor (CAR)
T-cell immunotherapy for human cancer. Am J Hematol. 94:S3–S9.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Robbins PF, Kassim SH, Tran TL, Crystal
JS, Morgan RA, Feldman SA, Yang JC, Dudley ME, Wunderlich JR,
Sherry RM, et al: A pilot trial using lymphocytes genetically
engineered with an NY-ESO-1-reactive T-cell receptor: Long-term
follow-up and correlates with response. Clin Cancer Res.
21:1019–1027. 2015. View Article : Google Scholar
|
|
75
|
Falzone L, Salomone S and Libra M:
Evolution of cancer pharmacological treatments at the turn of the
third millennium. Front Pharmacol. 9:13002018. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Pelster MS and Amaria RN: Combined
targeted therapy and immunotherapy in melanoma: A review of the
impact on the tumor microenvironment and outcomes of early clinical
trials. Ther Adv Med Oncol. 11:17588359198308262019. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Ribas A, Hodi FS, Callahan M, Konto C and
Wolchok J: Hepatotoxicity with combination of vemurafenib and
ipilimumab. N Engl J Med. 368:1365–1366. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Minor DR, Puzanov I, Callahan MK, Hug BA
and Hoos A: Severe gastrointestinal toxicity with administration of
trametinib in combination with dabrafenib and ipilimumab. Pigment
Cell Melanoma Res. 28:611–612. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Ribas A, Butler M, Lutzky J, Lawrence DP,
Robert C, Miller W, Linette WMGP, Ascierto PA, Kuzel T, Algazi AP,
et al: Phase I study combining anti-PD-L1 (MEDI4736) with BRAF
(dabrafenib) and/or MEK (trametinib) inhibitors in advanced
melanoma. J Clin Oncol. 33(Suppl 15): 30032015. View Article : Google Scholar
|
|
80
|
Shui L, Yang X, Li J, Yi C, Sun Q and Zhu
H: Gut microbiome as a potential factor for modulating resistance
to cancer immuno-therapy. Front Immunol. 10:29892020. View Article : Google Scholar
|
|
81
|
Longo V, Brunetti O, Azzariti A, Galetta
D, Nardulli P, Leonetti F and Silvestris N: Strategies to improve
cancer immune checkpoint inhibitors efficacy, other than abscopal
effect: A systematic review. Cancers (Basel). 11:5392019.
View Article : Google Scholar
|
|
82
|
Velez MA, Burns TF and Stabile LP: The
estrogen pathway as a modulator of response to immunotherapy.
Immunotherapy. 11:1161–1176. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Matsushita M and Kawaguchi M:
Immunomodulatory Effects of Drugs for Effective Cancer
Immunotherapy. J Oncol. 2018:86534892018. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Vivarelli S, Falzone L, Basile MS,
Nicolosi D, Genovese C, Libra M and Salmeri M: Benefits of using
probiotics as adjuvants in anticancer therapy (Review). World A Sci
J. 1:125–135. 2019.
|
|
85
|
Sivan A, Corrales L, Hubert N, Williams
JB, Aquino-Michaels K, Earley ZM, Benyamin FW, Lei YM, Jabri B,
Alegre ML, et al: Commensal Bifidobacterium promotes antitumor
immunity and facilitates anti-PD-L1 efficacy. Science.
350:1084–1089. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Routy B, Le Chatelier E, Derosa L, Duong
CPM, Alou MT, Daillère R, Fluckiger A, Messaoudene M, Rauber C,
Roberti MP, et al: Gut microbiome influences efficacy of PD-1-based
immunotherapy against epithelial tumors. Science. 359:91–97. 2018.
View Article : Google Scholar
|
|
87
|
Gopalakrishnan V, Spencer CN, Nezi L,
Reuben A, Andrews MC, Karpinets TV, Prieto PA, Vicente D, Hoffman
K, Wei SC, et al: Gut microbiome modulates response to anti-PD-1
immunotherapy in melanoma patients. Science. 359:97–103. 2018.
View Article : Google Scholar
|
|
88
|
Banna GL, Torino F, Marletta F, Santagati
M, Salemi R, Cannarozzo E, Falzone L, Ferraù F and Libra M:
Lactobacillus rhamnosus GG: An overview to explore the rationale of
its use in cancer. Front Pharmacol. 8:6032017. View Article : Google Scholar :
|
|
89
|
Vétizou M, Pitt JM, Daillère R, Lepage P,
Waldschmitt N, Flament C, Rusakiewicz S, Routy B, Roberti MP, Duong
CP, et al: Anticancer immunotherapy by CTLA-4 blockade relies on
the gut microbiota. Science. 350:1079–1084. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Matson V, Fessler J, Bao R, Chongsuwat T,
Zha Y, Alegre ML, Luke JJ and Gajewski TF: The commensal microbiome
is associated with anti-PD-1 efficacy in metastatic melanoma
patients. Science. 359:104–108. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Elkrief A, Derosa L, Kroemer G, Zitvogel L
and Routy B: The negative impact of antibiotics on outcomes in
cancer patients treated with immunotherapy: A new independent
prognostic factor? Ann Oncol. 30:1572–1579. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Eskiocak B, McMillan EA, Mendiratta S,
Kollipara RK, Zhang H, Humphries CG, Wang C, Garcia-Rodriguez J,
Ding M, Zaman A, et al: Biomarker accessible and chemically
addressable mechanistic subtypes of BRAF melanoma. Cancer Discov.
7:832–851. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Salemi R, Falzone L, Madonna G, Polesel J,
Cinà D, Mallardo D, Ascierto PA, Libra M and Candido S: MMP-9 as a
candidate marker of response to BRAF inhibitors in melanoma
patients with BRAFV600E mutation detected in circulating-free DNA.
Front Pharmacol. 9:8562018. View Article : Google Scholar :
|
|
94
|
Guarneri C, Bevelacqua V, Polesel J,
Falzone L, Cannavò PS, Spandidos DA, Malaponte G and Libra M: NFκB
inhibition is associated with OPN/MMP 9 downregulation in cutaneous
melanoma. Oncol Rep. 37:737–746. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Luke JJ, Flaherty KT, Ribas A and Long GV:
Targeted agents and immunotherapies: Optimizing outcomes in
melanoma. Nat Rev Clin Oncol. 14:463–482. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Tumeh PC, Harview CL, Yearley JH, Shintaku
IP, Taylor EJ, Robert L, Chmielowski B, Spasic M, Henry G, Ciobanu
V, et al: PD-1 blockade induces responses by inhibiting adaptive
immune resistance. Nature. 515:568–571. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Gajewski TF, Louahed J and Brichard VG:
Gene signature in melanoma associated with clinical activity: A
potential clue to unlock cancer immunotherapy. Cancer J.
16:399–403. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Harlin H, Meng Y, Peterson AC, Zha Y,
Tretiakova M, Slingluff C, McKee M and Gajewski TF: Chemokine
expression in melanoma metastases associated with CD8+
T-cell recruitment. Cancer Res. 69:3077–3085. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Ji RR, Chasalow SD, Wang L, Hamid O,
Schmidt H, Cogswell J, Alaparthy S, Berman D, Jure-Kunkel M,
Siemers NO, et al: An immune-active tumor microenvironment favors
clinical response to ipilimumab. Cancer Immunol Immunother.
61:1019–1031. 2012. View Article : Google Scholar
|
|
100
|
Spranger S, Bao R and Gajewski TF:
Melanoma-intrinsic β-catenin signalling prevents anti-tumour
immunity. Nature. 523:231–235. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Peng W, Chen JQ, Liu C, Malu S, Creasy C,
Tetzlaff MT, Xu C, McKenzie JA, Zhang C, Liang X, et al: Loss of
PTEN promotes resistance to T cell-mediated immunotherapy. Cancer
Discov. 6:202–216. 2016. View Article : Google Scholar :
|
|
102
|
Zaretsky JM, Garcia-Diaz A, Shin DS,
Escuin-Ordinas H, Hugo W, Hu-Lieskovan S, Torrejon DY,
Abril-Rodriguez G, Sandoval S, Barthly L, et al: Mutations
associated with acquired resistance to PD 1 blockade in melanoma. N
Engl J Med. 375:819–829. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Shin DS, Zaretsky JM, Escuin-Ordinas H,
Garcia-Diaz A, Hu-Lieskovan S, Kalbasi A, Grasso CS, Hugo W,
Sandoval S, Torrejon DY, et al: Primary resistance to PD 1 blockade
mediated by JAK1/2 mutations. Cancer Discov. 7:188–201. 2017.
View Article : Google Scholar
|
|
104
|
Liu D, Schilling B, Liu D, Sucker A,
Livingstone E, Jerby-Arnon L, Zimmer L, Gutzmer R, Satzger I,
Loquai C, et al: Integrative molecular and clinical modeling of
clinical outcomes to PD1 blockade in patients with metastatic
melanoma. Nat Med. 25:1916–1927. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Tuaeva NO, Falzone L, Porozov YB, Nosyrev
AE, Trukhan VM, Kovatsi L, Spandidos DA, Drakoulis N, Kalogeraki A,
Mamoulakis C, et al: Translational application of circulating DNA
in oncology: review of the last decades achievements. Cells.
8:12512019. View Article : Google Scholar :
|
|
106
|
Lee EY and Kulkarni RP: Circulating
biomarkers predictive of tumor response to cancer immunotherapy.
Expert Rev Mol Diagn. 19:895–904. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Napoli S, Scuderi C, Gattuso G, Bella VD,
Candido S, Basile MS, Libra M and Falzone L: Functional roles of
matrix metallopro-teinases and their inhibitors in melanoma. Cells.
9:E11512020. View Article : Google Scholar
|
|
108
|
Falzone L, Salemi R, Travali S, Scalisi A,
McCubrey JA, Candido S and Libra M: MMP-9 overexpression is
associated with intragenic hypermethylation of MMP9 gene in
melanoma. Aging (Albany NY). 8:933–944. 2016. View Article : Google Scholar
|
|
109
|
Moogk D, da Silva IP, Ma MW, Friedman EB,
de Miera EV, Darvishian F, Scanlon P, Perez-Garcia A, Pavlick AC,
Bhardwaj N, et al: Melanoma expression of matrix
metallopro-teinase-23 is associated with blunted tumor immunity and
poor responses to immunotherapy. J Transl Med. 12:3422014.
View Article : Google Scholar
|