1. Introduction
Although relatively rare, uveal melanoma is the most
common type of intraocular tumour with a mean annual incidence of
5-10 cases/1,000,000 individuals. Among all cancers of the eye, 85%
are primary tumours of this type and occur in individuals with a
mean age of 60 years. The remaining 15% cases are non-Hodgkin
lymphomas, retinoblastomas and medulloepitheliomas. Despite these
figures, the most frequent tumours affecting the eye are metastases
of other types of cancer, mainly lung cancer in males and breast
cancer in females (1,2). Uveal melanoma is also a melanocytic
cancer, representing approximately 3-5% of all of these cancers,
although its characteristic features differ from those of the
cutaneous form. Tumours are mainly located in the choroid 85-90%,
followed by the ciliary body (6%) and iris (4%). Several studies
have demonstrated that both its cell mutation pattern and aetiology
have their own characteristics, unrelated in a large measure to
those of remaining melanomas. Host susceptibility factors are also
fairly specific, and incidence varies according to ethnicity,
gender and geographical region (2,3).
Currently, the management approach to uveal melanoma
is essentially multidisciplinary, involving ophthalmologists,
oncologists and maxillofacial surgeons. Patient management also
involves dealing with a heavy emotional burden. Despite intense
research into the physiopathology, histology and molecular biology
of uveal melanoma, there has been little improvement in its bleak
prognosis (4). Patient management
thus currently focuses on early detection and aggressive treatment.
Notwithstanding, over time, approximately 50% of patients will
develop metastatic disease with its ominous prognosis and survival
of 6-12 months (5).
When staging a primary uveal melanoma, besides
considering its anatomical and pathological features (tumour base
diameter, ciliary body involvement, and patterns of extravascular
matrix growth, mitosis, and cell morphology), mutations with
prognostic value along with their statistics have allowed for an
individualized approach able to predict the response to treatment
and outcome (6). Clinical
manifestations depend on the size and location of the tumour.
Often, tumours are incidentally detected in an ophthalmological
exam or through symptoms, such as loss of vision, photopsia,
myodesopsia or high intraocular pressure (7).
A major characteristic of uveal melanoma is that it
differentially affects populations in different geographical
regions. Unlike cutaneous melanoma, with an incidence that has
risen sharply over the past 30 years, the incidence of uveal
melanoma has remained stable over this same period. For example, in
Europe, figures range from 2 cases per million per year in Spain,
Italy and Portugal, to 9 cases per million in Norway, Denmark or
Sweden (8). By contrast, Asia and
Africa are less affected. For instance, Korea exhibits an incidence
of 0.6 cases/1,000,000 and Africa 0.2 cases/1,000,000 (9). Currently, the world region with the
highest number of cases is Australia with 11 cases/million per year
(10). To understand the high
geographic variation in this disease, it is necessary to examine
the associations among possible genetic, phenotypic or occupational
risk factors. Accordingly, the present study reviews the main
clinical, epidemiological, physiopathological and molecular
features that define uveal melanoma.
2. Risk factors
Uveal melanoma has a large number of associated risk
factors such as age, sex, genetic or phenotypic predisposition, the
work environment and dermatological conditions. While it mainly
affects older-aged individuals, an older age is also related to a
worse prognosis. The mean age of diagnosis also varies according to
the geographical location. In Asia, it tends to affect younger
individuals (45-55 years of age), while in Europe or in the USA, it
usually presents at around the age of 60 years. It should be
mentioned that uveal melanoma in young individuals has also been
related to congenital melanocytic syndromes (ocular melanosis and
dysplastic nevus syndrome), with a mean onset age of 16 years and a
better short-term prognosis owing to its lesser locoregional
aggressiveness (11,12). Sex as a risk factor is related to
age. For example, in individuals <60 years of age, there is no
clear predisposition for any sex and the ratio of affected females
to males is 1:1. At more advanced ages, there is a slight
predisposition for males, who also exhibit a higher risk of
metastasis and therefore, exhibit a higher mortality rate and a
worse prognosis (11,13).
As occurs with cutaneous melanoma, uveal melanoma
tends to affect Caucasians who represent the great majority of
patients. This is due to a series of susceptibility factors for
melanocyte lesions, such as fair skin, green or blue eyes and blond
or red hair. A higher incidence has also been described in
individuals with dysplastic nevus syndrome, multiple nevi, ocular
melanosis and freckles; in these subjects it has been related to an
early age at onset (14). However,
it is not known whether these lesions may be associated with
exposure to UV light. According to previous research, not only does
the vitreous humour block the actions of light rays in the
posterior chamber of the eye, but the crystalline lens/cornea
barrier mean there is little support for the theory of mutations
triggered by UV radiation (15).
Hence, its association with an individual's phenotype may be a
susceptibility factor for oncogenic melanocyte mutations and
therefore, of the risk of developing uveal melanoma.
A notable risk factor for uveal melanoma is the work
environment. Both professional cooks and welders exhibit an up to a
2-fold greater risk of developing uveal melanoma. Researchers have
related prolonged exposure to sunflower, olive and other oils while
cooking to the production of polycyclic hydrocarbons and complex
derived hydrocarbons that function as carcinogens by inducing a
state of oxidative stress and damage to DNA repair mechanisms
(11). In welders, the association
between exposure to UV light while welding and the incidence of
uveal melanoma is not clear, as mentioned above. The vitreous
humour, lens and cornea play a protective role (15). During heat welding, numerous gases
are produced when metals fuse together, giving rise to carcinogenic
substances, such as hexavalent chromium, argon, helium, hydrogen
fluoride and asbestos (16). Low
frequency electric fields are also generated, which also affect
cell repair processes and may be related to an increased incidence
of a uveal melanoma (12).
Finally, the risk of uveal melanoma in patients with
Nevus of Ota is 1/400, which is extremely high compared to subjects
without this condition, with an annual incidence of ~1/13,000. In
individuals with this nevus, uveal melanoma usually presents at an
earlier age and exhibits less aggressive locoregional invasion and
a lower incidence of metastasis (17,18).
Ocular dysplastic lesions are proliferative non-malignant lesions
with atypical characteristics (irregular margins, growth and
different tones) that have been linked to a 10-fold greater risk of
transformation into uveal melanoma compared with the general
population (19). Researchers have
demonstrated malignant degeneration in 2 to 5% of patients with an
iris nevus. The main risk factors associated with the malignant
transformation of an iris nevus are an age <40 years, diffuse
lesion appearance, blood detected in the eye fundus and inferior
location. By contrast, choroidal nevus, which occurs in ~5% of the
population, exhibits a low likelihood of malignant degeneration,
approximately 1 case per 9,000 (20). Risk factors for suspecting a
malignant choroidal nevus are a thickness >2 mm, the presence of
symptoms and orangey colour, among others. It should be underscored
that these risk factors generally lead to an earlier appearance of
uveal melanoma (11,12).
3. Clinical manifestations
Uveal melanoma generates symptoms depending on the
ocular site involved, meaning that most clinical signs are
determined by both tumour size and location. Usually patients
present with blurred vision, photopsia and/or myodesopsia or are
asymptomatic and the uveal melanoma is detected incidentally during
a routine ophthalmological examination (7). When the tumour affects the macula,
patients exhibit a gradual painless decline in visual acuity. It
should also be mentioned that if there is involvement of the
iridocorneal angle, signs may be those of acute glaucoma, namely
the loss of visual acuity, pain, photopsia and increased
intraocular pressure. These symptoms can lead to permanent
blindness and are therefore, constitute an ophthalmological
emergency. By contrast, the involvement of the iris is usually
asymptomatic and presents as a dark growing, invasive
hyperpigmented lesion. If the ciliary body is involved, this can
compromise the natural lens, causing its subluxation and impaired
accommodation, thus interfering with the patient's vision (21). It should be noted that
infrequently, intraocular progression can give rise to haemorrhage
within the ocular cavity presenting as haemorrhage and
exophthalmos. Up to 22% of patients may have systemic
manifestations as a consequence of metastatic spread mainly to the
liver, and almost 90% succumb to the disease before 5 years
following diagnosis (22).
4. Anatomopathological study of uveal
melanoma
Callender (23) was
the first to establish an anatomopathological classification of
these tumours, which was later modified by McLean et al
(24), who distinguished between
type A fusiform cell, type B fusiform cell, epithelioid cell and
mixed tumours. Fusiform type A followed by B tumours were
associated with a higher survival rate, and epithelioid cell
tumours were associated with the worse prognosis. Mixed tumours
were associated with an intermediate outcome (25,26).
Another series of histopathological criteria has proven useful to
assess disease prognosis in a patient with uveal melanoma. For
instance, an elevated microvascular density (MVD) related to tumour
irrigation and the presence of a network vascular pattern have been
associated with a worse prognosis (27,28).
High IGF-1R levels and mean nucleolar diameter have been also
related to a lower survival (29,30).
The role of some of the more important cell proliferation markers,
such as Ki-67 or proliferating cell nuclear antigen (PCNA), have
been assessed in uveal melanoma cells, their presence indicating a
worse prognosis (31). Finally,
localizing some immune system cells, such as lymphocytes or
infiltrating macrophages, or the detection of markers like HLA-A
have been also associated with a worse prognosis in patients with
uveal melanoma (32,33). Notably, the presence of HLA-B has
been associated with the epithelioid subtype, which is the
histological class exhibiting a lower survival (34).
The anatomopathological study of uveal melanoma has
recently benefited from developments in the field of molecular
biology. This has meant that currently, classification according to
the molecular profile of uveal melanoma has proven more useful than
its histological classification, in line with the concept of
individualized precision medicine for these patients.
5. Molecular classification of uveal
melanoma: Genes involved
Uveal melanoma is often divided into two categories
according to its gene expression profile and to its metastasizing
capacity. Hence, class 1 uveal melanomas are associated with a low
risk of metastasis and have been linked to a better prognosis,
while class 2 tumours feature a high risk of spread and a worse
prognosis. In addition, there is significant variation in
cytogenetics and expression levels of some genes in the different
subtypes; for example, chromosome 3 monosomy is characteristic of
class 2 tumours (35). However,
this initial classification is insufficient to explain, for
example, why some class 1 tumours show a higher risk of metastasis
than others.
For this reason, uveal melanoma classification has
been extended to include 4 groups: 2 subclasses characterized by
chromosome 3 monosomy (M3) with a worse prognosis, and a further 2
subtypes that lack this chromosome abnormality; i.e., with
chromosome 3 disomy (D3), with a better prognosis. The first 2
subclasses are associated with a higher metastasis risk and exhibit
a loss of or mutation of the gene encoding BRCA-associated protein
1 (BAP1) located on 3p21.1 (NCBI), and conferring a different
methylation state to those without this monosomy. Between both M3
subtypes, there is a series of genomic, transcriptional and
clinical variations, such as the amplification of 1 to 3 copies of
the long arm of chromosome 8 (36).
In turn, the D3 subtypes are divided into IA and IB.
The former exhibits no aneuploidy, the least risk of spread and is
characterized by a mutation in eukaryotic translation initiation
factor 1A X-linked (EIF1AX). Subtype IB, characterized by the
possible presence of a total or partial gain of 6p and a higher
metastasis risk, features mutations in the splicing factor 3b
subunit 1 (SF3B1) gene (37).
Furthermore, Field et al (38,39)
highlighted the role of gene expression of preferentially expressed
antigen in melanoma (PRAME) as an independent biomarker of
metastasis frequently found in tumours with a mutation in SF3B1.
This marker may also appear in M3 tumours and is also inversely
related to mutations in EIF1AX. Mutations in the genes EIF1AX,
SF3B1 and BAP1 are mutually exclusive, as well as being key
prognostic markers to understand the behaviour of each uveal
melanoma subtype (40). Of note,
both in D3 uveal melanomas which do not exhibit mutations in SF3B1
or EIF1AX and in M3, which exhibit gain of chromosome 8q, mutations
in serine and arginine rich splicing factor 2 (SRSF2) have also
been found, indicating a role for this marker in the metastasis of
uveal melanoma and its functional analogy with SF3B1 (36).
6. Uveal vs. cutaneous melanoma:
Similarities and differences
While cutaneous and uveal melanoma both arise from
melanocytes, their molecular profiles, cytogenetic alterations,
prognosis and dissemination capacity vary appreciably (Fig. 1). For example, it is known that
approximately 50% of cases of uveal melanoma progress to metastasis
and the mean survival rate of these patients is 6 to 12 months
(13). The most frequent site of
spread of these tumours is the liver, though lung and bone
metastases are also common (41,42)
whereas cutaneous melanoma metastasizes with the same frequency to
the lungs, bone, brain and soft tissues and mainly spreads via the
lymph system (43).
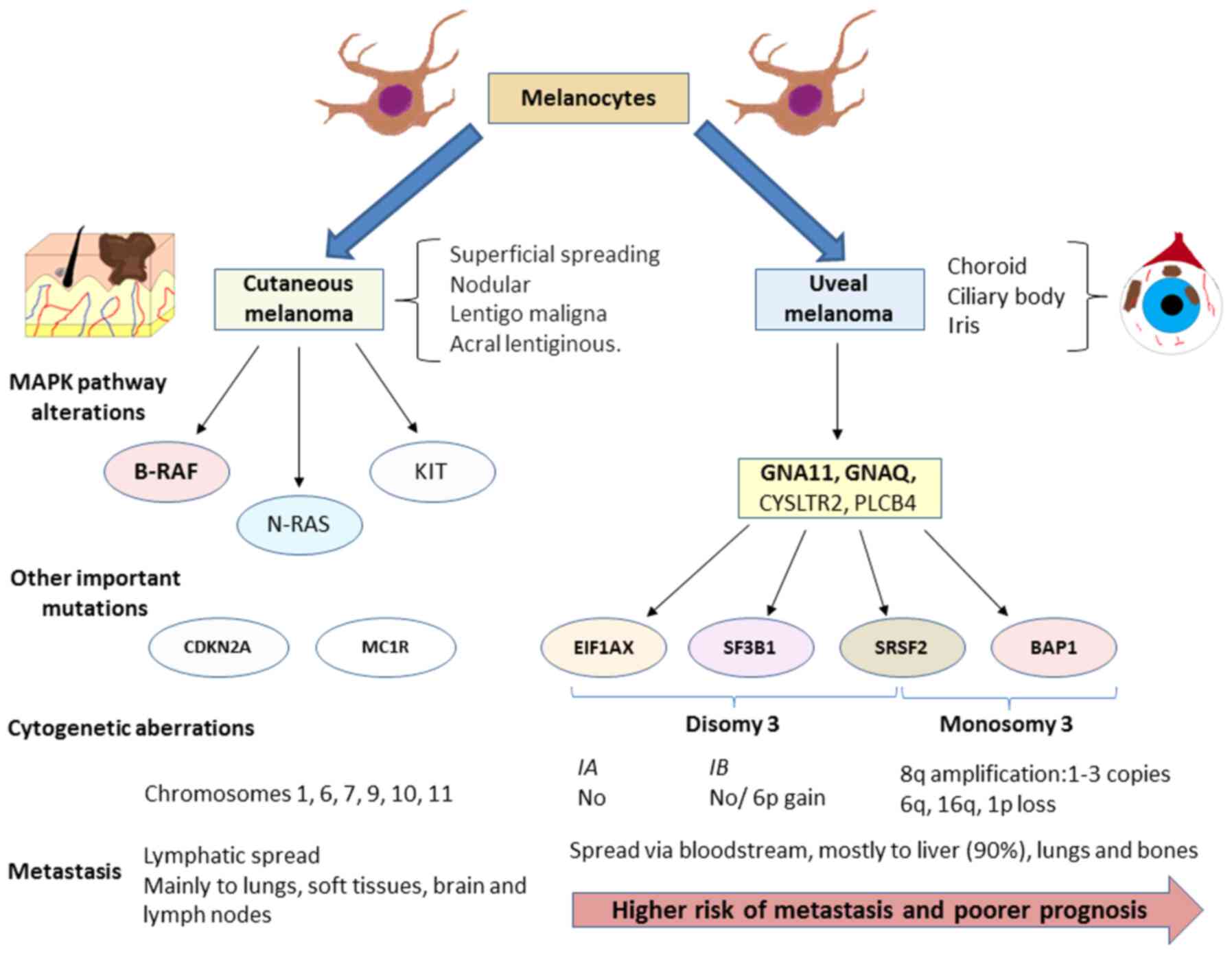 | Figure 1Diagram illustrating the diagnostic
features of cutaneous melanoma and uveal melanoma. Although both
melanomas arise from melanocytes, each one shows its own
characteristics while sharing the feature of an altered MAP kinase
signalling pathway. Presently, these abnormalities are one of the
most promising targets of the treatment of these patients, such as
the inhibition of B-RAF for cutaneous melanoma. Nevertheless, as
illustrated in the diagram, the mutations that activate this
pathway differ and are accompanied by another set of modifications
that are also different. In the case of uveal melanoma, these
mutations serve to classify tumours into subtypes according to
their molecular profile. The four mutations described are mutually
exclusive. This molecular classification is also associated with
metastasis risk and disease prognosis. The spread of both tumours
also differs as cutaneous melanomas usually spread via the lymph
while uveal melanomas usually spread via the bloodstream. Uveal
melanoma exhibits a high predisposition to spread to the liver,
which occurs in 90% of cases. By contrast, cutaneous melanoma may
metastasize to the lungs, brain, lymph nodes and soft tissues with
almost equal probability. Cytogenetic aberrations are also common
in both types of melanoma, although these also differ. GNA, G
protein subunit alpha; EIF1AX, eukaryotic translation initiation
factor 1A X-linked; SF3B1, splicing factor 3b subunit 1; SRSF2,
serine and arginine rich splicing factor 2; BAP1, BRCA-associated
protein 1. |
As in cutaneous melanoma, in uveal melanoma, the
overexpression of the MAPK pathway is observed. However, mutations
found in both types of melanoma differ. In the skin form, most
frequent abnormalities are found in molecules directly involved in
this pathway especially the B-RAF mutation (in 40-60% of cases). In
this type of mutation, particularly in residue V600, a worse
prognosis has been described (44). In addition, are mutations in other
genes, such as NRAS (15-25%) and KIT (39%) are frequent (45). However, it is known that these
polymorphisms seldom occur in uveal melanoma (46). The mutations found in this tumour
type appear mainly in the genes that code for the α subunit of G,
mainly G protein subunit alpha (GNA)11 or GNAQ, detected in up to
90% of cases of uveal melanoma. Furthermore, these mutations seem
to play an important role in the onset and progression of uveal
melanoma as it has been observed that both abnormalities are not
associated with a worse prognosis (47,48).
Mutations in other genes have also been observed, such as cysteinyl
leukotriene receptor 2 (CYSLTR2; 4%) or phospholipase C beta 4
(PLCB4; 2.5%) (49,50). The mechanisms through which all
these alterations affect tumour biology are described below.
In some cases of uveal melanoma, mutations in the
telomerase reverse transcriptase (TERT) gene have been described.
However, the frequency of this mutation is low, having been found
in 1 of 50 uveal melanoma specimens examined by Dono et al
(51). Furthermore, this mutation
appeared to be associated with a tumour with variations in GNA11
and EIF1AX, that is, it appeared in the least aggressive profile.
Nonetheless, this TERT variant has been detected at a higher
frequency in both sporadic and familiar cutaneous melanoma
(52). The greatest utility of
this marker could be in identifying ocular melanoma type as
indicated by the study conducted by Griewank et al (53). These authors found that up to 32%
of conjunctival melanomas had a mutated TERT promotor, while this
polymorphism was absent in 47 uveal melanomas examined. Their
findings indicate that the presence or absence of this mutation is
able to distinguish between both ocular melanomas and may help
explain the different behaviour shown by each one.
7. Biology of uveal melanoma
Roles of inflammation and immune system
in uveal melanoma
Hanahan and Weinberg (54) described the main characteristics or
hallmarks of tumour cells that form the basis of our under-standing
of cancer biology along with the targets of current cancer
therapies. The inflammatory response represents one of these
hallmarks and its important role in uveal melanoma was reviewed by
Bronkhorst and Jager (55). Among
other characteristics, the presence of an inflammatory phenotype
has been described comprised of different types of lymphocytes and
macrophages, along with the increased expression of class 1 and 2
HLA. This phenotype usually appears in M3 tumours as a sign of a
worse prognosis (56).
This type of information also provides access to new
more effective therapeutic tools for the treatment of uveal
melanoma. However, although several studies have shown the efficacy
of the key immune response regulators PD-1 and CTLA-4 inhibitors
(57,58) in patients with cutaneous melanoma,
the response to these molecules in patients with uveal melanoma has
not been the same, suggesting the need to gain further insight into
the evasive mechanisms of the immune system in uveal melanoma
(59). In effect, Mougiakakos
et al (60) demonstrated
how high levels of cyclooxygenase (COX)-2, a marker of a worse
prognosis in these tumours, were associated with elevated Treg
levels in uveal melanoma and how this could explain the poor
efficacy of antitumour therapies. However, there is a need for
further research in this area, as other authors have found no such
link between Treg levels and survival in this type of tumour
(61,62). Recently, the study conducted by
Petralia et al (63)
demonstrated how levels of CD47 exhibit a better correlation with
elevated levels of Treg and of other inflammatory cells. These
results were also reported by Basile et al (64), who also noted that in uveal
melanoma, CD200 and HVEM are significantly reduced and that there
is an inverse association between the PDL1 levels and mean overall
survival (OS), progression-free survival (PFS) and tumour
thickness. Notably, the PD-1/PD-L1 levels have been shown to
regulate the levels of non-coding RNA in a number of types of
cancer, whose importance in uveal melanoma will be subsequently
discussed (65). While PD-L1
expression has been reported at the primary tumour site, metastatic
uveal melanoma exhibits a low expression of this marker (66). Importantly, the presence of T cells
expressing LAG3 rather than CTLA-4 or PD-1 also plays a role in the
inflammatory pattern in the microenvironment of primary uveal
melanoma (67). Equally, liver
metastasized tumours show infiltration of clonally expanded plasma
cells, suggesting antibody-mediated immunity. The importance of
hepatic stellate cells in liver metastasis has also been reported
(68). The paracrine signalling of
these cells affects the transcriptional activity of uveal melanoma
cells, linked to inflammation and interleukin production. Hence,
inflammatory conditions in the primary tumour seem very different
to metastasis locations. Collectively, these data provide direction
for future treatments pursuing these targets to improve treatment
outcomes.
Signalling pathways
As described above, the most frequent mutations that
appear in the early development of uveal melanoma are those
affecting GPCR receptors, particularly variants of GNA11 or GNAQ.
These last 2 genes code for subunit G-α of G proteins and are
activated by the serotonin receptor 2A and 2B in the melanocyte
(5-HT2A and 5-HT2B (69). Receptor
5-HT2B mutations are often found in a wide variety of tumours and
have been linked to a greater metastasis risk (70). Furthermore, GNAQ and GNA11
mutations trigger a wide range of cell signalling cascades,
including the PI3K/Akt/mTOR, YAP/TAZ, Wnt/β-catenin, Rac/Rho, Notch
and MAPK pathways (71-73). The modification of so many cell
signalling pathways notably hinders treatments targeting their
inhibition owing to their possible interactions. An example is
YAP/TAZ, whose activation occurs independently of HIPPO through its
interaction with Rac/Rho, as reported by Feng et al
(74). Thus, efforts in therapies
targeted at inhibiting these pathways need to assess the cell
dynamics of these tumours to increase their efficiency.
Mechanisms involved in metastasis
As previously described, one of the most important
mutations found in uveal melanoma and a key point for understanding
its biology, particularly its metastasis, is BAP1. BAP1 is a tumour
suppressor gene that appears mutated in up to 84% of cases of
metastasized uveal melanoma and in 38% of primary uveal melanomas
(36,75). BAP1 codes for an enzyme with
deubiquitinating capacity that binds to other suppressor proteins,
such as BARD1 or BRCA1, generating heterodimers that act as tumour
suppressors (76). It has been
observed that mutations in the BAP1 germline are associated with a
large variety of tumours, including lung adenocarcinoma, menangioma
and uveal melanoma (77). Somatic
mutations mainly affect premature protein termination or ubiquitin
carboxy-terminal hydrolase domains. Among other functions, BAP1 is
a key regulator of cell cycle control and transcription, whereby it
interacts with histone H2A (78,79).
BAP-1 deubiquitinates H2A and its loss has been associated with the
death of cells which enter an RNF-2 apoptotic-dependent program
(80). However, this mechanism has
not been detected in melanocyte lines and it has been described
that the loss of BAP-1 leads to defective DNA repair, thus
favouring later mutations and cytogenetic aberrations, promoting
the metastasis and aggressiveness of tumour cells (81). Matatall et al (82) also examined the role of BAP1 in the
differentiation of uveal melanocytes and found that its lack of
expression induces a progenitor phenotype in these melanocytes.
Furthermore, it has been proposed that the loss of BAP1 can lead to
an inflammatory tumour microenvironment (83). Finally, the location of BAP1 also
seems to be crucial for metastasis. Szalai et al (84) reported no nuclear immunodetection
of BAP1 in approximately 50% of patients with metastatic uveal
melanoma, hence supporting the relevance of BAP1 mutations in
metastasis.
Another key mutation in uveal melanoma progression
is that detected in SF3B1. SF3B1 encodes a component of the
spliceosome and its gaining function mutations affect the splicing
of several transcripts with effects at different levels (85,86).
Yavuzyigitoglu et al (87)
confirmed that SF3B1 mutations were important in late metastasis,
due to their effects on splicing, which in turn has been associated
with a wide range of carcinogenic processes in a number of tumours,
including invasion and metastasis (88). In uveal melanoma, SF3B1 splicing
defects may play an important role in different processes, probably
sharing common oncogenic mechanisms with BAP1 and EIF1AX (89). Mutant SF3B1 is considered to
recognise intronic sequences in the bromodomain containing 9
(BRD9), degrading them and affecting the non-canonical
barrier-to-autointegration factor complex (ncBAF), thus resulting
in the development of myelodysplastic syndrome and uveal melanoma
(90). In addition, mutations in
SRSF2, U2AF1 and ZRSR2 have also been linked to defective splicing
in uveal melanoma. Furthermore, in tumours with mutations in both
BAP1 and SF3B1, elevated levels may appear of PRAME, which act as a
repressor of retinoic acid signalling and of its receptor, two
known tumour suppressors, whose inhibition has been incriminated in
a wide variety of cancers (91,92).
Mutations affecting EIF1AX, which participate in the onset of
translation, has no influence on metastases and more work is needed
to establish possible relations between both (86). Of note, EIF1AX mutations seem to
exert a synergistic effect on Ras mutations in certain types of
tumours, such as ovary and thyroid (93,94).
The low proportions of uveal melanoma cell mutations in these genes
may explain why EIF1AX is not associated with a greater metastasis
risk in the tumours.
Another interesting signalling pathway associated
with a number of tumours is that of endothelin 2 and its receptor
endothelin receptor type B (EDNRB) associated with a large number
of tumours (95,96). EDNRB is a G protein coupled
receptor (GPCR) and these proteins play a role in the
differentiation of melanocytes (97). Certain studies have found that a
lower expression of this receptor in metastasized uveal melanomas
indicates a poor prognosis (35,98).
However, the mechanism responsible for this remains unclear. As a
GPCR, the EDNRB receptor seems capable of activating protein G α
subunits, such as GNAQ and GNA11. Urtatiz and Van Raamsdonk
(99) proposed that reduced EDNRB
receptor expression causes signalling dysregulation mediated by Wt
variants and GNAQ/GNA11 mutants. However, in the study by Van
Raamsdonk et al (47), it
was observed that patients without GNAQ or GNA11 mutations
exhibited a worse prognosis. Thus, lower EDNRB expression could be
beneficial for patients with mutations in both proteins through
their interference with the cell signalling cascade. Further
insight into the mechanisms of action of G proteins in cancer and
the role of EDNRB in uveal melanoma is required.
The mechanisms whereby uveal melanoma exhibits high
tropism for the liver remain elusive. Some authors propose the
bloodstream as the dissemination route from the eye to the liver
aided by the fenestrated structure of hepatic capillaries (43). In parallel, it has also been
hypothesized that it may be the result of increased expression of
cMET, a tyrosine kinase inhibitor that is activated by binding to
the hepatic growth factor (HGF) receptor produced in the liver that
appears elevated in primary uveal melanomas (70,100). Other authors suggest that it is
due to the increase in IGF-1/IGF-IR previously described in uveal
melanoma (30).
Recent studies have revealed a role of cytokine
CXCL12 and its receptor CXCR4, which also interacts with vascular
endothelial growth factor (VEGF), potentiating its role in
metastasis (101). Furthermore,
both this pathway and cMET/HGF have been described to contribute to
activation of the pathway PI3K/Akt/mTOR, indicating a worse
prognosis for patients with this type of cancer (102). The activation of this pathway by
cMET has also been described as a mechanism of resistance to MEK
inhibitors (103). A lack of PTEN
is also frequent in these tumours, affecting up to 40% of uveal
melanomas (104).
Once again, these data suggest the importance of a
wide perspective when treating uveal melanoma based on the
combination of different therapies to improve their efficacy.
Hypoxia and oxidative stress
Another mechanism which plays a significant role in
the development of uveal melanoma is hypoxia. This situation
appears in tumours as a consequence of their rapid growth and has
been attributed to their metabolic reprogramming (54). Hypoxia is an essential mechanism
for a number of carcinogenic processes and is an important factor
to consider when designing more effective therapies for various
tumours (105). As a response to
this setting of hypoxia, factors induced by hypoxia (HIF) will
drive a large variety of cell responses among which we find the
control of genes and molecules involved in anaerobic metabolism.
This is a crucial process in tumour cells (known as the Warburg
effect), in metastasis, in cell motility and in angiogenesis
(106,107).
Hypoxia-induced factors consist of 2 heterodimer
subunits formed by an α subunit (HIF-1 α, HIF-2 α or HIF-3 α) and a
β subunit expressed constitutively. In conditions of normoxia, α
subunits are degraded by the proteasome following a process of
hydroxylation and ubiquitination. In hypoxia, the α subunit joins
to the β subunit, recruiting p300/CBP coactivators to bind the
hypoxia response element (HRE) present in approximately 100 genes
(108). Although the functions of
HIF-1 or HIF-2 are still under investigation, they seem more
implicated in cancer than the HIF-3 isoform (109).
In uveal melanoma, hypoxia has been associated with
numerous alterations. Asnaghi et al (110) detected increased signalling
mediated by Notch and the phosphorylation levels of Erk1-2 and Akt.
These authors also noted that the inhibition of the Notch pathway
partially reduced Erk and Akt phosphorylation, suggesting a need to
gain further insight into these targets to delay or avoid tumour
dissemination. Furthermore, an increased HIF-1α expression was
directly associated with increased levels of markers of cell
proliferation (MIB-1), vessel growth (CD31 and VEGF-A) and
necrosis; however, it was found to have no effect on patient
survival (111).
In a later study, Hu et al (112) assessed the role of hypoxia in the
angiogenic phenotype of uveal melanoma by examining another key
component, angiopoietin-like 4 (ANGPTL4). In their study, the
inhibition of this molecule and of VEGF was found to reduce the
angiogenic potential of these tumours. Furthermore, HIF-1α has been
demonstrated to contribute to the expression of c-MET and CXCR4.
Inhibition with aryl sulphonamide 64B interrupts the interaction
between the HIF-1 complex and its coactivators, and therefore
reduces its binding to HRE present in the promoters of these genes,
diminishing their expression (113).
Recently, Brouwer et al (114,115) observed that in tumours exhibiting
M3 and a lack of BAP1 expression, the expression of HIF-1 α was
elevated, as was microvascular density and the angiogenic
phenotype, while VEGF-B expression was reduced. This suggests a
need to address the mechanisms of angiogenesis in these tumours.
HIF-1 α expression could not be associated with tumour size, but
was related to the presence of T cells and macrophages. Tumour
hypoxia also promotes the metabolic programming that tumour cells
undergo.
Collectively, these data identify hypoxia as an
important factor to consider in the treatment of uveal melanoma,
warranting further investigation. Notwithstanding, the mechanisms
involved in hypoxia and its possible association with different
carcinogenic processes need to be further examined. Some of the
more important interactions of the hypoxia-induced factor are
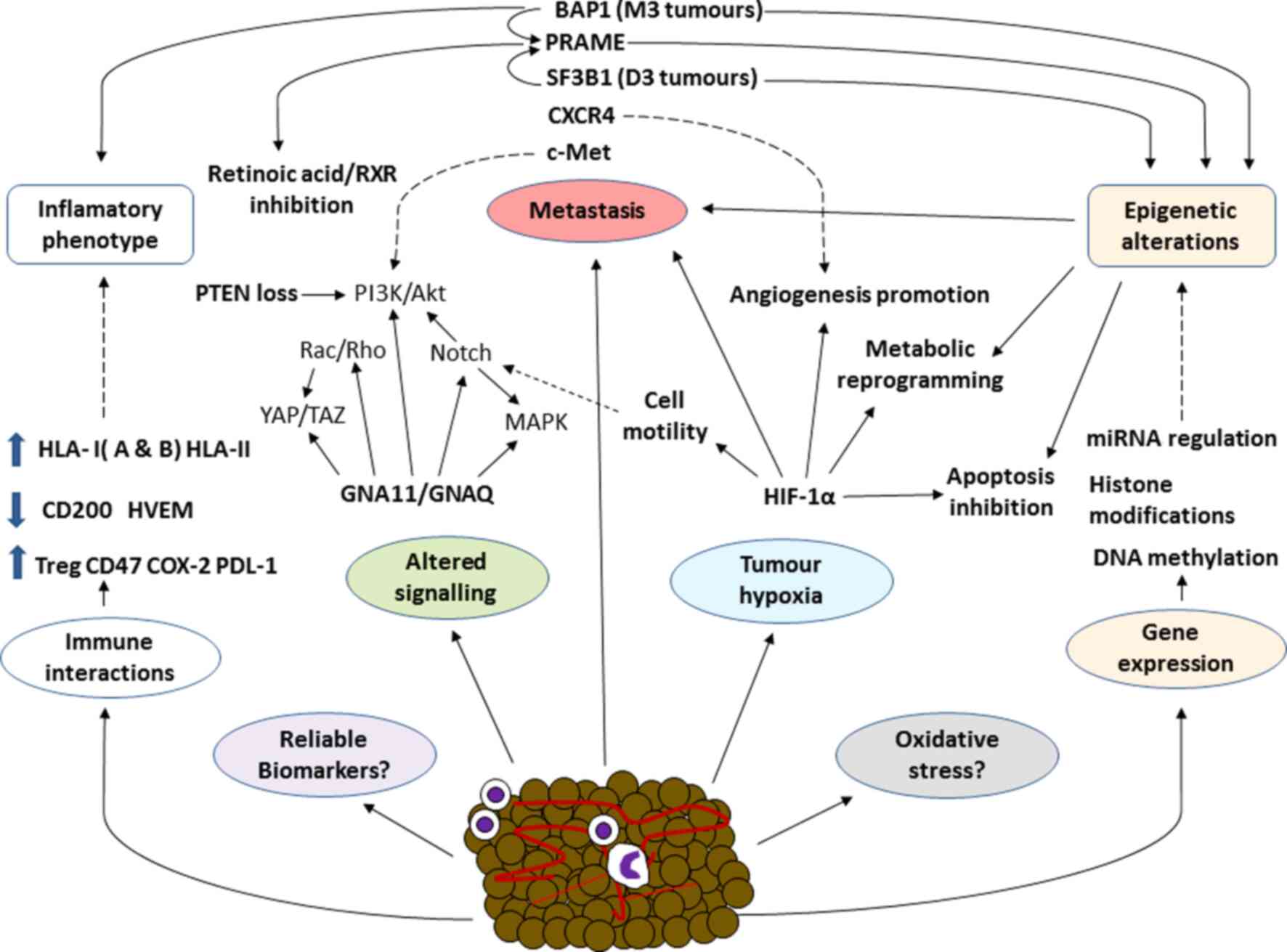
summarized in Fig. 2 along with
the different biological mechanisms involved in this disease.
Oxidative stress is a cell condition that arises
from an imbalance of oxidizing molecules produced mainly via
mitochondrial respiration, and of reducing molecules, also known as
antioxidants. The main oxidising molecules are reactive oxygen
species (ROS) or nitrogen reactive species (NRS), which have been
incriminated in a wide variety of diseases, such as Alzheimer's and
other neurodegenerative diseases, or cardiovascular diseases, among
others (116,117). The role of oxidative stress in
the development of cancer is, however, still a somewhat
controversial issue. To date, it has been established that
oxidative stress can induce a carcinogenic process in early disease
stages. For example, it is known that, as with malignant melanoma
of the skin, the pheomelanin pigment pathway, which is associated
with fairer skin tones and lighter eye colours, may lead to the
development of uveal melanoma through a carcinogenesis mechanism
independent of UV radiation that eventually gives rise to a process
of oxidative damage (43,118). Furthermore, oxidative stress is
directly related to an inflammatory response, which can promote the
process of carcinogenesis (119).
In more advanced disease stages, this mechanism may
block or impair certain key events for tumour development.
Accordingly, it is currently proposed that adaptation to oxidative
stress is one of the main mechanisms involved in the development of
the different cancers (120).
Piskounova et al (121)
demonstrated that antioxidants, whose function is to minimize
oxidative stress in cells, promoted the metastasis of melanoma
cells. Recently, Dithmer et al (122) assessed the effects of the VEGF
antagonist, bevacizumab, on the survival and proliferation of 5
uveal melanoma tumour lines, simulating a possible complication of
the use of ionising radiation to treat primary tumours. The results
indicated that this inhibitor exerted a protective effect against
the oxidative stress induced by the ionising radiation,
highlighting the need for detailed studies designed to unveil the
role of oxidative stress in this disease.
Role of epigenetics in the development of
uveal melanoma
Epigenetics is another key issue for understanding
the factors underlying cancer. Epigenetic mechanisms are varied and
include processes, such as DNA methylation, the modification of
histones or regulation by non-codifying RNAs, such as microRNAs
(miRNAs or miRs), as interesting therapeutic targets for diverse
types of cancer (123). In this
first section, we focus on the two former mechanisms. The miRNA
control of gene transcription is discussed in the subsequent
section.
The methylation state is one of the main epigenetic
mechanisms. The hypermethylation of the most significant CpG
islands through tumour gene suppressor inactivation takes place in
numerous cancers including uveal melanoma (124). For example, it is common to
observe the hypermethylation of the RASSF1a (Ras association domain
family 1 isoform A) gene promotor region in uveal melanoma tumours
(125). This gene also appears
methylated in a wide variety of tumours, such as cutaneous
melanoma, and lung, liver, breast or head and neck cancer, among
others, and is a factor for a worse prognosis directly correlated
with tumour progression (126).
Maat et al (127) examined
the role of Ras and EF-hand domain containing (RASEF) as a tumour
suppressor gene in 11 uveal melanoma cell lines and 35 samples of
primary uveal melanoma, and found that homozygosity in conjunction
with hypermethylation was the mechanism whereby RASEF expression
was lost, which was associated with a lower survival rate.
Similarly, it has been reported that in both cutaneous and uveal
melanoma, the hypermethylation of promotor sequences of the genes
p16, DcR1 and DcR2 is often observed, directly involved in
regulating cell processes, such as senescence and apoptosis
(128,129). Of note, it has been observed that
this hypermethylation of p16 leads to the phosphorylation of the
retinoblastoma protein, which is key for controlling the cell cycle
(130). Other important
components of the cell cycle that exhibit an upregulated expression
in uveal melanoma are Bcl-2, MDM2 and CD1 (102).
Gene hypomethylation is a less frequent epigenetic
mechanism than hypermethylation and yet has been related to
increased gene expression involved in these PRAME mechanisms or
those of the gene deleted in split hand/split foot 1 (DSS1)
(39,131). Notably, it is known that the DNA
methylation patterns present in M3 tumours with abnormal BAP1
differ from those of D3, which, in turn, also differ between each
other according to whether their mutation affects EIF1AX or
SF3B1/SRFR2 (132). This could
indicate the importance of these genes in epigenetic regulation
mechanisms and is also considered an interesting topic of further
investigation.
Histone modification is another process with an
important role in epigenetic control affecting events, such as
methylation, phosphorylation or acetylation. The dysregulation of
these mechanisms can lead to the inappropriate activation of
oncogenes or in the inactivation of tumour suppressor genes making
this an important line of study in the field of cancer (133). In uveal melanoma, the
overexpression of transcription factors, such as HES1 has been
directly involved in the metastatic capacity of uveal melanoma,
suggesting the methylation of the promotor region of histone H3K4
is an inducer of this over-expression (134). In effect, this is another
interesting issue to explore in terms of increasing the efficacy of
current therapies, especially for metastatic uveal melanomas.
Role of miRNAs in uveal melanoma
Advances in molecular biology have identified an
important role of miRNAs in a wide variety of diseases,
particularly cancer. Over the past 10 years, the number of studies
addressing these molecules has increased exponentially, enhancing
the knowledge of their function (135). For example, it is known that
miRNAs are a key epigenetic mechanism for the control of gene
transcription and may act in some cancer types as tumour
suppressors and in others as oncogenes (136,137). In effect, miRNAs are emerging as
promising therapeutic targets in various types of cancer and as
ever more reliable prognostic factors in individualized precision
medicine (138,139). The roles of miRNAs in uveal
melanoma as important prognostic and diagnostic markers of tumour
onset and progression have been confirmed (140). Some of the miRNAs playing a
significant role in uveal melanoma are discussed below.
Yang and Wei (141) compared the expression profiles of
miRNAs in 4 uveal melanoma tissues and 4 normal uveal tissues.
Their results revealed increased expression levels of miRNAs of the
miR-17 family (miRNA-20a, miRNA-106a and miRNA-17) and significant
increases in miRNA-21 expression in 4 uveal melanoma cell lines,
along with diminished miRNA-145 and miRNA-204 expression. Wang
et al (142) elucidated
the role of miRNA-21 in uveal melanoma cell metastasis. The results
obtained revealed miRNA-21 overexpression following inhibition of
p53 expression, which via a series of effector molecules may
promote tumour metastasis in vitro. In vivo, its
inhibition also leads to a reduced tumour size. Radhakrishnan et
al (143) identified 19
miRNAs expressed in metastasized and not in metastatic uveal
melanoma, while up to 11 miRNAs were detected only in the
metastasized phenotype. Recently, other miRNAs with oncogenic
effects have been identified, such as miR-155 (144).
Among the uveal melanoma tumour suppressor miRNAs,
miRNA-145 should be mentioned. Li et al (145) found that the insulin 1 receptor
substrate (IRS-1) could serve as a therapeutic target to increase
the levels of miR-145, which is essential for uveal melanoma cells
to enter into apoptosis. Similarly, the members of the miR-34
family of miRNA precursors, miR-34a, miR-34b and miR-34c, have been
identified as important tumour suppressors expressed in normal
uveal tissue, but not in uveal melanoma following their
downregulation of other molecules, such as c-Met, Akt and proteins
involved in the cell cycle (146,147). Recently, Serocki et al
(148) confirmed the role of
miR-17 family miRNAs in controlling HIF expression under conditions
of hypoxia. Some miRNAs also reduce the expression of phosphatase
and tensin homolog (PTEN), promoting PI3K/AKt/mTOR pathway
activation (149,150). In addition, Liu et al
(151) described the role of
miR-216a-5p as an indicator of a better prognosis due to its
inhibitory effect on hexokinase 2, an enzyme overexpressed in a
wide array of tumours that is directly related to induction of the
Warburg effect. Therapy, pursuing the dysregulation of these miRNAs
is a promising approach for the treatment of this type of
cancer.
Of note, miRNAs represent one of the various
mechanisms involved in the pathogenesis of uveal melanoma, as
summarized in Fig. 2. The
interactions between all these factors are undoubtedly complex, and
future studies will be crucial for a better understanding of such a
complex cancer.
8. Blood biomarkers for uveal melanoma
Despite scientific and technological advances that
have improved our understanding of various types of cancers, the
incidence of uveal melanoma and patient survival has not markedly
altered over the past 30 years (152,153). This has determined that the most
effective measure against this type of cancer is its early
detection. As uveal melanoma tumours spread via the bloodstream,
blood biomarkers may be useful to detect metastases early on and to
monitor disease progression or the response to treatment (154).
Circulating tumour cells (CTCs) and circulating free
DNA (cfDNA) are among the components that may be detected in blood,
indicating the presence of a tumour and both are prognostic markers
of a variety of cancers (155,156). In uveal melanoma, both the
detection of CTCs or cfDNA has proven a reliable indicator of a
worse prognosis. Of note, the detection of melanocytic CTCs has
exhibited efficacy in arterial blood, but not in veins (157), whereas cfDNA seems more useful in
this tumour type, particularly in patients with easily detectable
known mutations (158). In
effect, today there is an ongoing clinical trial designed to assess
the detection and variations produced in blood levels of cfDNA in
patients followed before and after undergoing surgery for liver
metastasis (NCT02849145).
Characterizing different CTC populations is also
crucial for the understand of the biological mechanisms underlying
this type of cancer. Schuster et al (159) examined CTCs in 68 patients with
uveal melanoma and the gene expression in these cells of tyrosinase
and MelanA/MART1. Their results indicated that the presence of CTCs
was directly related to the metastatic process and that the
detection of these transcripts points to a worse prognosis. Tura
et al (160) demonstrated
that FISH could be used to examine CTCs in patients with primary
uveal melanoma and thus detect the status of chromosome 3.
Following a 4-year follow-up period, the results revealed the high
reliability of this method to predict the metastases that these
patients could develop.
miRNAs can also represent important blood biomarkers
detectable in uveal melanoma. Achberger et al (161) identified an association between
plasma miRNAs and their variation in a setting of metastasis.
Compared to the controls, the levels of miR-20a, -125b, -146a,
-155, -181a and -223 were elevated, while those of miRNA-181a were
reduced when metastasis appeared. Along these lines, Russo et
al (162) found significantly
higher blood and tissue levels of miRNA-146a. Furthermore, Eldh
et al (163) detected
higher levels of exosomes and miRNAs in patients with hepatic
metastasis from uveal melanoma compared to patients without
metastasis. Based on these data, Stark et al (164) measured the serum levels of up to
17 miRNAs in 65 patients with uveal nevus, localized uveal melanoma
and metastasized uveal melanoma. The results served to define a
panel of 6 miRNAs (miR-16, miR-145, miR-146a, miR-204, miR-211 and
miR-363-3p) that could be used for a precision diagnosis of uveal
melanoma with 93% sensitivity and 100% specificity. Collectively,
these data indicate a need for advancements in the field of miRNAs,
given their great diagnostic and therapeutic value in a disease as
complex as uveal cancer.
Apart from these biomarkers, other blood indicators
have proven useful in uveal melanoma, such as proteins,
glycoproteins and tumour metabolites.
9. Proteomics and metabolomics in uveal
melanoma
In the study of cancer, interest in proteomics and
metabolomics continues to mount. Tissue and blood samples are the
most used for this type of study, as they are minimally invasive
and of great clinical value (165). However, these studies still have
some limitations, such as a need for greater refinement in the
measurement systems used and analytical variations in the data
obtained and difficulties in their translation from bench to
bedside (166).
The proteins melanoma inhibitory activity (MIA) and
OPN (osteopontin) are among the most tested as biomarkers of uveal
melanoma and have been directly associated with metas-tasis
(167,168). Another biomarker examined is
S100-β (169). These latter
studies determined that all 3 of these proteins (MIA, OPN and
S100-β) combined were able to detect with a high sensitivity the
presence of metastases in the liver. However, in the study
conducted by Missotten et al (170), no association was observed
between this combined biomarker and any clinical or pathological
feature of the tumour, questioning its actual prognostic value. Of
note, Strobel et al (171)
found elevated serum S100-β concentrations in patients with liver
metastases from cutaneous melanoma compared to uveal melanoma in
which no association was noted. In patients with liver metastasis,
increased levels of the oncoprotein, DJ-1/PARK7, the soluble
marker, c-Met, and the glycoprotein, ME20-S, have been observed
(172-175). Notably, through cell culture
techniques, Angi et al (176) compared the proteins secreted by
uveal melanoma tumours with a high and low metastasis risk with
those secreted by choroidal melanocytes. These authors detected the
presence of OPN, MIA, GDF15, PARK7 and ME20, and only recorded
significant differences in MIA and GDF15 secretion between cells of
uveal melanoma and normal choroidal melanocytes. No differences
emerged between the tumours with a high and low risk of
metastasis.
Advances in omics-related technologies are proving
helpful in the identification of the proteins and metabolites
involved in uveal melanoma and in elucidating their roles. In the
study by Crabb et al (177), iTRAQ technology was used to
examine large numbers of proteins present in 8 samples of
metastasized and 7 of non-metastasized uveal melanoma. Their
findings identified a need for further investigation into proteins,
such as heat shock protein (HSP)β-1 and collagen α3 (VI) as
possible biomarkers of these tumours. Shi et al (178), using mass spectrometry and
fractioning techniques with magnetic pearls, detected up to 49
differentially expressed peptides in patients with uveal melanoma
and healthy controls. Their data indicated that peptides of 1,467
to 9,289 kDa were able to differentiate between patients with uveal
melanoma and healthy individuals with a specificity of 100%. These
authors also identified precursors of the fibrinogen α chain as
possible markers of uveal melanoma. Also, recently Song et
al (179) conducted a
multiplex immunoassay on serum samples from 48 patients diagnosed
with uveal melanoma and 36 healthy controls. Once again, HSPβ-1 and
OPN levels proved useful to distinguish between patients and
healthy control individuals.
10. Clinical management of uveal
melanoma
Risk and prognosis of uveal melanoma
The general prognosis is that 50% of patients will
present metastasis within the first 15 years of diagnosis. Once
this occurs, the mean life expectancy is between 6 months to 1
year. However, it should be highlighted that the latency period
from locoregional disease control until the onset of metastasis can
be >25 years, such that patients require exhaustive follow-up
over a long period of time. The preferred sites of presenting
metastasis are the liver (~60%), lungs (~25%), skin and soft
tissues (~10%) and bones (~8%) (13). The genetic analysis of melanocyte
lesions has identified that extraocular invasion is related to both
the inactivation of the tumour suppressor gene, BAP1 (detected in
85% of cases), and to monosomy 3, as the main risk factors for
disease spread (180). Currently,
there are no established criteria for the long-term follow-up of
patients diagnosed with uveal melanoma. Recommended approaches are
imaging techniques conducted every 3 to 12 months. An MRI is the
best option both for the detection of liver and extrahepatic
metastases, such as those affecting bones or retroperitoneal nodes.
A CT scan is also useful for lung node manifestations and larger
liver metastases and in patients for whom MRI is not recommended.
Ultrasonography exclusively reveals hepatic metastases and PET
cannot detect small lesions, the high radiation dose being another
major drawback of this technique (181).
Tumour size, extraocular extension, mitotic
activity and epithelioid cell type are considered important risk
factors for melanoma (182). As
previously stated, genetic mutations and chromosome abnormalities
are also directly associated with patient outcomes and shed light
into the prognosis of uveal melanoma. To examine all these
chromosome and molecular features during the management of uveal
melanoma, a wide range of methods can be used. The most common
approaches are karyotyping, fluorescent in situ
hybridisation (FISH) or comparative genome hybridisation (CGH).
Further techniques, such as microsatellite analysis, multiple
ligation-dependent probe amplification (MLPA) and genome-wide
single nucleotide polymorphism can also be used for the genomic
study of uveal melanoma. Karyotyping is useful for the detection
major chromosome gains or losses. However, minor genetic
alterations are not identified. FISH, such as CGH is more accurate
in detecting chromosome aberrations in uveal melanoma; however, it
is still insufficient for the detection of all chromosome
modifications (183). Thus, the
study of the molecular biology of uveal melanoma is required for
the development of novel techniques. MLPA is currently an
interesting option, particularly when combined with clinical and
histological data, as it offers information on chromosomes 1, 3, 6
and 8 and it can be used in a wide range of samples, even those
subjected to radiotherapy (184,185). Genome expression profiling (GEP)
has been however, most successful for the prognosis of uveal
melanoma (186). The strengths
and limitations of these methods were reviewed by Dogrusöz et
al (185). Additionally,
whole genome sequencing (WGS) can provide substantial information
in uveal melanoma (187) and
microarray analysis can also offer whole genome data, partial
chromosome defects, loss of heterozygosity or additional challenges
not detected by FISH (188).
Pathological and genetic studies require invasive
procedures to obtain biopsies; thus, the use of these methods in
uveal melanoma is a matter of debate (189). The introduction of non-invasive
diagnostic techniques, the validity of these genetic tests and even
the emotional and ethical impacts for both patient and physician of
the results (190) are some of
the limitations of genetic risk determination. Nonetheless, the
potential implications of knowledge regarding prognosis could be
essential to establish guidelines for the follow-up of patients
when the metastatic risk is low and opt for more aggressive
treatment options if the risk is high. For instance, the presence
of M3 or D3 is critical for the clinical management of uveal
melanoma. The detection of the commonly found M3 in small tumours
prompts the use of more aggressive treatments in these patients,
especially to prevent metastasis (191). If M3 were detected, this could
mean the tumour has spread to other organs, and hence, local
therapy would not be effective (192). Surveillance in these high-risk
patients may be hepatic imaging and liver function tests every 3-6
months (193). The biopsy method
must also be considered in the study of M3 in uveal melanoma.
Whereas fine needle aspiration (scleral approach) obtains a tumour
sample from the base, the transvitreal approach collects the biopsy
through the apex returning different results. Because of tumour
heterogeneity, the scleral approach is the best method to detect M3
(194). Similarly, BAP1 tumours
may have a significant clinical impact in uveal melanoma
management, particularly in the development of targeted
therapy.
Current and potential therapies
A close association exists between metastatic
disease, prognosis and response to therapy. This is due to the fact
that considerable advances have been made in the locoregional
control of the disease through both conservative techniques (e.g.,
brachytherapy, external beam radiation therapy or laser
photodynamic and photocoagulation therapy) and more aggressive
approaches (enucleation) rendering an overall 5-year survival of
approximately 80% (4). This
survival rate has remained stable over the past 30 years, and
developments have therefore consisted mainly of more effective and
less aggressive surgical techniques.
Similar to the association existing between the
prognosis and metastasis of uveal melanoma, immunotherapy is one of
the main pillars of the treatment of disseminated disease. Systemic
chemotherapy barely improves the overall prognosis of a patient and
the response rate to conventional chemotherapy is <1%. Moreover,
there is still no standardized treatment available for the
management of metastatic disease that has been able to improve the
long-term survival of these patients (195). This has meant that emphasis has
been made on the most current treatment option, whereby an immune
response is induced based on histological tumour characteristics, T
lymphocytes and dendritic cells, and on the different cell
signalling pathways. To understand the history of immunotherapy in
patients with uveal melanoma, it should be remembered that the
first trials involving this approach were conducted in patients
with melanoma of the skin. For example, checkpoint inhibitors,
mainly anti-CTLA4 (ipilimumab) and anti-PD1 (nivolumab), elicit a
response in 40-60% of patients with metastatic cutaneous melanoma.
However, in patients with uveal melanoma the response rate is
approximately 20-30% (196). This
poor response may be attributed to resistance due to the high
tumour burden or to a low mutation rate conferring scarce antigenic
induction and therefore a poor immune response. It should be
emphasized that immunotherapy catalyses an immune reaction against
tumour cells, such that a failed response will determine the
disease will progress. A new immune approach involves the use of
tebentafusp. This agent is based on the immune-mobilizing
monoclonal T cell receptor (TCR) formed by a soluble TCR fused with
an anti-CD3 presenting to uveal melanoma antigens, leading to T
cell activation and triggering the activation of the immune
response cascade with the consequence of enhanced tumour lysis
(197). This novel treatment
gives rise to a response rate of 57 to 71% after 16 weeks (198). It should be noted that this
therapy is still under development and is being tested in several
types of cancer, and that the long-term response to this new
approach remains unknown. Similarly, several coadjuvant therapies
have been assessed, such as vaccination with uveal melanoma cell
antigens (gp100, t, RNA melanoma or tyrosinases) also targeted at
activating the immune response, although this time on the part of
dendritic cells. In patients classified as high risk (those with
monosomy 3), this type of therapy has given rise to a 3-year
survival rate of 79%, although as for tebentafusp, this is still at
the clinical trial stage (199).
Likewise, molecular targeting mayh be one of the most promising
therapies for the management of uveal melanoma. For example, GNAQ
and GNA11 pathway inhibitors, such as selumetinib or trametinib,
both targeting MEK, have been shown to be successful in some
clinical trials (200,201). Despite this, neither selumetinib
nor trametinib increase the overall survival rate. This is due to
resistance acquired by the tumour to these inhibitors, also
observed in cutaneous melanoma (202). Blocking other cell signalling
pathways such as cMET/PI3K inhibition in liver metastasis could be
a solution to MEK inhibitors resistance (203). Likewise, histone deacetylase
(HDAC) inhibitors represent an interesting coadjuvant to MEK
inhibitors, also reducing tumour growth in various in vivo
models (204). Notably, HDAC
inhibitors have exhibited some efficacy in controlling cell
differentiation, cell cycle and in the gene expression profile of
cultured uveal melanoma cells (205). Importantly, by inhibiting the
acetylation of histones, it is possible to reverse the effects of
the loss of BAP1 through its effects on the cell cycle, leading to
a less aggressive differentiated state (182).
The spliceosome has also been proposed as a
potential antitumoral target in a number of types of cancer, as
demonstrated by Bonnal et al (206). Examples of SF3B1 inhibitors are
sudemycins, spliceostatin A and meayamycin. According to some
authors, these compounds act through intron retention (207), whereas others propose massive
exon skipping (208), hence
interfering with aberrant SF3B1splicing. While further insight is
needed into SF3B1 biology to design and predict the desirable
effects of its inhibition, its potential as a uveal melanoma target
is undeniable (209). Of note,
spliceosome inhibitors may also be useful in BAP1 mutant tumours,
as they promote c-Myc expression, increasing susceptibility to this
therapy (182). Currently,
H3B-8800 is being tested in patients with haematological
malignancies (NCT02841540). Another undergoing clinical trial
involves studying the role of niraparib in patients with uveal
melanoma and other tumours featuring BAP1 mutations (NCT03207347),
and PRAME is also being targeted in metastatic uveal melanoma
through a PRAME-TCR construct (NCT02743611). Viral carriers may be
an interesting solution to therapy delivery (210). Ongoing virus-based and other
clinical trials for severe uveal melanoma are summarized in
Table I. These new treatment lines
are indeed a ray of hope that are set to change the fatal prognosis
of this disease.
 | Table IOngoing clinical trials targeting the
treatment of metastatic uveal melanoma. |
Table I
Ongoing clinical trials targeting the
treatment of metastatic uveal melanoma.
| Name | Identifier | Status | Population | Phase | Purpose |
|---|
| ENSIGN: Phase II
window of opportunity or body radiation therapy and in situ
gene therapy followed by nivolumab in metastatic squamous or
non-squamous non-small cell lung carcinoma and metastatic uveal
melanoma | NCT02831933 | Recruiting | 25 participants
with lung squamous cell carcinoma stage IV and non-squamous
non-small cell cancer metastatic uveal melanoma trial of
stereotactic | Phase 2 | Determine the
efficacy and safety of in situ gene therapy and stereotactic
body radiation therapy |
| Ipilimumab and
nivolumab in combination with immunoembolization for the treatment
of metastatic uveal melanoma | NCT03472586 | Recruiting | 35 participants
with uveal melanoma and liver metastasis | Phase 2 | Test the use of the
monoclonal antibodies ipilimumab and nivolumab and
immunoembolization to treat patients with liver metastasis |
| A Phase 1/2
dose-finding study to evaluate the safety, feasibility, and
activity of BPX-701, a controllable PRAME T-cell receptor therapy,
in HLA-A2+ subjects with AML, previously treated mds, or metastatic
uveal melanoma | NCT02743611 | Active, not
recruiting | 28 participants
with AML, MDS and uveal melanoma | Phase 1
Phase 2 | Assess the effect
of BPX-701 in tumours showing high PRAME expression |
| Phase1b/2 study
combining hepatic percutaneous perfusion with ipilimumab plus
nivolumab in advanced uveal melanoma | NCT04283890 | Recruiting | 88 participants
with metastatic uveal melanoma | Phase 1
Phase 2 | Assess the use of
immunotherapy (ipilimumab with nivolumab) plus chemotherapy
(melphalan) |
| Phase Ib Study of
cellular adoptive immunotherapy using autologous Cd8+
antigen-specific T cells and anti-Ctla4 for patients with
metastatic uveal melanoma | NCT03068624 | Active, not
recruiting | 19 participants
with metastatic uveal melanoma | Phase 1 | Determine the
maximum tolerated dose (MTD) of adoptively transferred
SLC45A2-specific cytotoxic T-lymphocytes (CTL) and its combination
with cyclophosphamide, aldesleukin and ipilimumab |
| A phase 2 study to
evaluate the efficacy and safety of adoptive transfer of autologous
tumour infiltrating lymphocytes in patients with metastatic uveal
melanoma | NCT03467516 | Recruiting | 59 participants
with metastatic uveal melanoma | Phase 2 | Assess the use of
TIL in conjunction with TIL high dose aldesleukin |
| Phase I vaccination
trial in metastatic uveal melanoma using IKKb-matured dendritic
cells loaded with autologous tumour-RNA + RNA coding for defined
antigens and driver mutations | NCT04335890 | Recruiting | 12 participants
with metastatic uveal melanoma | Phase 1 | Assess the effects
of vaccination with IKKb matured dendritic cells loaded with
autologous tumour-RNA + RNA coding for defined antigens and driver
mutations |
| A phase II study of
BVD-523 in metastatic uveal melanoma | NCT03417739 | Active, not
recruiting | 13 participants
with metastatic uveal melanoma | Phase 2 | Assess the
targeting of the MAPK signalling pathway using BVD-523 in advanced
uveal melanoma |
| Efficacy study of
pembrolizumab with entinostat to treat metastatic melanoma of the
eye | NCT02697630 | Active, not
recruiting | 29 participants
with metastatic uveal melanoma | Phase 2 | Assess the
potential combination of entinostat (HDAC inhibitor) and
pembrolizumab (immunotherapy) |
| Intravenous and
intrathecal nivolumab in treating patients with leptomeningeal
disease | NCT03025256 | Recruiting | 30 participants
with brain metastasis, among them uveal melanoma | Phase 1 | Compare intrathecal
nivolumab and examine how well it acts in combination with
intravenous nivolumab when treating patients with leptomeningeal
disease |
| Trial of nivolumab
in combination with ipilimumab in subjects with previously
untreated metastatic uveal melanoma | NCT02626962 | Active, not
recruiting | 48 participants
with metastatic uveal melanoma | Phase 2 | Assess the impact
of nivolumab combined with ipilimumab in subjects with previously
untreated, unresectable or metastatic uveal melanoma |
| A study to assess
PV-10 chemoablation of cancer of the liver | NCT00986661 | Recruiting | 78 participants
with liver metastasis including those with uveal melanoma | Phase 1 | Examine the safety,
tolerability, pharmacokinetics and effect of a single intralesional
injection of PV-10 on tumour growth in subjects with primary or
metastatic liver cancer |
| IN10018 monotherapy
and combination therapy for metastatic melanoma | NCT04109456 | Recruiting | 52 participants
with metastatic cutaneous or uveal melanoma | Phase 1 | Assess the safety,
tolerability and antitumor properties of IN10018 as monotherapy and
in combination with cobimetinib in subjects with metastatic uveal
melanoma and NRAS-mutant metastatic melanoma |
| Modified virus
VSV-IFNbetaTYRP1 in treating patients with stage iii-iv
melanoma | NCT03865212 | Recruiting | 72 participants
with stage III-IV cutaneous and uveal melanoma | Phase 1 | Confirm the
efficacy, side effects and best dose of a modified virus
VSV-IFNbetaTYRP1 |
| Yttrium90,
ipilimumab, and nivolumab for uveal melanoma with liver
metastases | NCT02913417 | Recruiting | 26 participants
with liver metastatic uveal melanoma | Phase 1
Phase 2 | Examine the
synergistic effects of SirSpheres Yttrium-90 selective internal
hepatic radiation followed by immunotherapy combined with
ipilimumab and nivolumab |
| Iodine I 131
monoclonal antibody 3F8 in treating patients with central nervous
system cancer or leptomeningeal cancer | NCT00445965 | Active, not
recruiting | 78 participants
with brain metastasis including those with uveal melanoma | Phase 2 | Assess iodine I 131
monoclonal antibody 3F8 used to treat patients with central nervous
system or leptomeningeal cancer |
| Neoadjuvant and
adjuvant checkpoint blockade | NCT02519322 | Recruiting | 53 participants
with stage III-IV melanomas | Phase 2 | Check the
performance of nivolumab with or without ipilimumab or relatlimab
before surgery in patients with resectable stage IIIB-IV
melanoma |
|
Cabozantinib-S-malate compared with
temozolomide or dacarbazine in treating patients with metastatic
melanoma of the eye that cannot be removed by surgery | NCT01835145 | Active, not
recruiting | 47 participants
with recurrent/stage III-IV uveal melanoma | Phase 2 | Compare
cabozantinib-s-malate with temozolomide or dacarbazine in patients
with unresectable metastatic melanoma of the eye |
11. Conclusions and future directions
The present study has provided a comprehensive
overview of uveal melanoma, from its biology to the current
translational approaches. As discussed herein, uveal melanoma is an
own entity in terms of clinical signs, target population, histology
and molecular behaviour. The study of novel biological mechanisms
possibly involved in uveal melanoma is also a key point for the
design of new drugs directed towards targets, such as tumour
hypoxia responses mediated by HIF-1α or epigenetic regulation
driven by miRNAs. The cellular dynamics of these tumours and the
different processes involved in their metastasis are also key
topics of further investigation. The search for novel and more
reliable blood or tissue biomarkers could be expedited by
developments in techniques of proteomics and metabolomics, that
will allow for the analysis of larger and more representative
samples from patients with uveal melanoma. Risk determination
strategies play a crucial role in the management of physicians or
researchers and in improving early diagnosis, thus facilitating the
follow-up of these patients. Genetics is a determining factor for
the uveal melanoma stratification, its behaviour, therapeutic
approach, and the emergent development of immunotherapy. New
research efforts and current clinical trials must pursue novel
therapies targeting the individual set of characteristics of this
type of cancer. Uveal melanoma is a fatal cancer and its overall
survival rate has not markedly improved over the past 3 decades. As
molecular awareness has improved the understanding and management
of such a complex disease, extensive research is required to
continue to further elucidate the underlying mechanisms and
complete them, not only from a biological view, but also with
clinical outcomes, supporting the basis of further translational
approaches.
Acknowledgments
Not applicable.
Funding
The present study was supported by grants from the
B2017/BMD-3804 MITIC-CM (Community of Madrid, Spain), co-financed
by the European Development Regional Fund 'A Way to Achieve Europe'
(ERDF).
Availability of data and materials
Not applicable.
Authors' contributions
MAO, OFM, SC and MAT were involved in the
conceptualization of the study. JB, SC, MAM and MAT were involved
in funding acquisition. MAO, SC and MAT were involved in project
administration., MAO, OFM and MAT were involved in the
investigative aspects of the study. MAO, OFM, NGH, JB, MAM and MAT
were involved in data validation. All authors have read and agreed
to the published version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Andreoli MT, Mieler WF and Leiderman YI:
Epidemiological trends in uveal melanoma. Br J Ophthalmol.
99:1550–1553. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Maheshwari A and Finger PT: Cancers of the
eye. Cancer Metastasis Rev. 37:677–690. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Carvajal RD, Schwartz GK, Tezel T, Marr B,
Francis JH and Nathan PD: Metastatic disease from uveal melanoma:
Treatment options and future prospects. Br J Ophthalmol. 101:38–44.
2017. View Article : Google Scholar :
|
|
4
|
Krantz BA, Dave N, Komatsubara KM, Marr BP
and Carvajal RD: Uveal melanoma: Epidemiology, etiology, and
treatment of primary disease. Clin Ophthalmol. 11:279–289. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Seedor RS, Eschelman DJ, Gonsalves CF,
Adamo RD, Orloff M, Amjad A, Sharpe-Mills E, Chervoneva I, Shields
CL, Shields JA, et al: An Outcome assessment of a single
Institution's longitudinal experience with Uveal melanoma patients
with liver metastasis. Cancers (Basel). 12:1172020. View Article : Google Scholar
|
|
6
|
Shields CL, Manalac J, Das C, Ferguson K
and Shields JA: Choroidal melanoma: Clinical features,
classification, and top 10 pseudomelanomas. Curr Opin Ophthalmol.
25:177–185. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shields CL, Kaliki S, Furuta M, Mashayekhi
A and Shields JA: Clinical spectrum and prognosis of uveal melanoma
based on age at presentation in 8,033 cases. Retina. 32:1363–1372.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Virgili G, Gatta G, Ciccolallo L,
Capocaccia R, Biggeri A, Crocetti E, Lutz JM and Paci E; EUROCARE
Working Group: Incidence of uveal melanoma in europe.
Ophthalmology. 114:2309–2315. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Park SJ, Oh CM, Kim BW, Woo SJ, Cho H and
Park KH: Nationwide incidence of ocular melanoma in South Korea by
using the national cancer registry database (1999-2011). Invest
Ophthalmol Vis Sci. 56:4719–4724. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Singh N, Seregard S and Singh AD: Uveal
melanoma: Epidemiologic aspects. Clin Ophthalmic Oncol. 53–69.
2019. View Article : Google Scholar
|
|
11
|
Nichols EE, Richmond A and Daniels AB:
Disparities in uveal melanoma: Patient characteristics. Semin
Ophthalmol. 31:296–303. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Nayman T, Bostan C, Logan P and Burnier MN
Jr: Uveal melanoma risk Factors: A systematic review of
Meta-analyses. Curr Eye Res. 42:1085–1093. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kaliki S, Shields CL and Shields JA: Uveal
melanoma: Estimating prognosis. Indian J Ophthalmol. 63:93–102.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Al-Jamal RT and Kivelä T: Uveal melanoma
among Finnish children and young adults. J AAPOS. 18:61–66. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mallet JD, Gendron SP, Drigeard Desgarnier
MC and Rochette PJ: Implication of ultraviolet light in the
etiology of uveal melanoma: A review. Photochem Photobiol.
90:15–21. 2014. View Article : Google Scholar
|
|
16
|
Mishra S and Bharagava RN: Toxic and
genotoxic effects of hexavalent chromium in environment and its
bioremediation strategies. J Environ Sci Health C Environ Carcinog
Ecotoxicol Rev. 34:1–32. 2016. View Article : Google Scholar
|
|
17
|
Velazquez N and Jones IS: Ocular and
oculodermal melanocytosis associated with Uveal melanoma.
Ophthalmology. 90:1472–1476. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Plateroti AM, Scavella V, Abdolrahimzadeh
B, Plateroti R and Rahimi S: An update on oculodermal melanocytosis
and rare associated conditions. Semin Ophthalmol. 32:524–528. 2017.
View Article : Google Scholar
|
|
19
|
Shields CL, Kaliki S, Hutchinson A,
Nickerson S, Patel J, Kancherla S, Peshtani A, Nakhoda S, Kocher K,
Kolbus E, et al: Iris nevus growth into melanoma: Analysis of 1611
consecutive eyes: The ABCDEF guide. Ophthalmology. 120:766–772.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chien JL, Sioufi K, Surakiatchanukul T,
Shields JA and Shields CL: Choroidal nevus: A review of prevalence,
features, genetics, risks, and outcomes. Curr Opin Ophthalmol.
28:228–237. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Rodríguez A, Dueñas-Gonzalez A and
Delgado-Pelayo S: Clinical presentation and management of uveal
melanoma. Mol Clin Oncol. 5:675–677. 2016. View Article : Google Scholar
|
|
22
|
Nezu N, Goto H, Umazume K, Ueda S and
Shibata M: Clinical analysis of uveal melanoma. Nippon Ganka Gakkai
Zasshi. 121:413–418. 2017.In Japanese. PubMed/NCBI
|
|
23
|
Callender GR: Malignant melanotic tumors
of the eye. A study of histologic types in 111 cases. Trans Am Acad
Ophthalmol Otolaryngol. 36:131–140. 1931.
|
|
24
|
McLean IW, Foster WD, Zimmerman LE and
Gamel JW: Modifications of Callender's classification of uveal
melanoma at the armed forces institute of pathology. Am J
Ophthalmol. 96:502–509. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Seddon JM, Polivogianis L, Hsieh CC,
Albert DM, Gamel JW and Gragoudas ES: Death from uveal melanoma.
Number of epithelioid cells and inverse SD of nucleolar area as
prognostic factors. Arch Ophthalmol. 105:801–806. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Seregard S and Kock E: Prognostic
indicators following enucleation for posterior uveal melanoma. A
multivariate analysis of Long-term survival with minimized loss to
Follow-up. Acta Ophthalmol Scand. 73:340–344. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Folberg R, Pe'er J, Gruman LM, Woolson RF,
Jeng G, Montague PR, Moninger TO, Yi H and Moore KC: The
morpho-logic characteristics of tumor blood vessels as a marker of
tumor progression in primary human uveal melanoma: A matched
Case-control study. Hum Pathol. 23:1298–1305. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Al-Jamal RT, Mäkitie T and Kivelä T:
Nucleolar diameter and microvascular factors as independent
predictors of mortality from malignant melanoma of the choroid and
ciliary body. Invest Ophthalmol Vis Sci. 44:2381–2389. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Moshari A and McLean IW: Uveal melanoma:
Mean of the longest nucleoli measured on Silver-stained sections.
Invest Ophthalmol Vis Sci. 42:1160–1163. 2001.PubMed/NCBI
|
|
30
|
All-Ericsson C, Girnita L, Seregard S,
Bartolazzi A, Jager MJ and Larsson O: Insulin-like growth Factor-1
receptor in uveal melanoma: A predictor for metastatic disease and
a potential therapeutic target. Invest Ophthalmol Vis Sci. 43:1–8.
2002.PubMed/NCBI
|
|
31
|
Karlsson M, Boeryd B, Carstensen J,
Frånlund B, Gustafsson B, Kågedal B, Sun XF and Wingren S:
Correlations of Ki-67 and PCNA to DNA ploidy, S-phase fraction and
survival in uveal melanoma. Eur J Cancer. 32A:357–362. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Bronkhorst IH, Ly LV, Jordanova ES,
Vrolijk J, Versluis M, Luyten GP and Jager MJ: Detection of
M2-macrophages in uveal melanoma and relation with survival. Invest
Ophthalmol Vis Sci. 52:643–650. 2011. View Article : Google Scholar
|
|
33
|
Bronkhorst IH and Jager MJ: Uveal
melanoma: The inflammatory microenvironment. J Innate Immun.
4:454–462. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Blom DJ, Luyten GP, Mooy C, Kerkvliet S,
Zwinderman AH and Jager MJ: Human leukocyte antigen class I
expression. Marker of poor prognosis in uveal melanoma. Invest
Ophthalmol Vis Sci. 38:1865–1872. 1997.PubMed/NCBI
|
|
35
|
Onken MD, Worley LA, Ehlers JP and Harbour
JW: Gene expression profiling in uveal melanoma reveals two
molecular classes and predicts metastatic death. Cancer Res.
64:7205–7209. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Robertson AG, Shih J, Yau C, Gibb EA, Oba
J, Mungall KL, Hess JM, Uzunangelov V, Walter V, Danilova L, et al:
Integrative analysis identifies four molecular and clinical subsets
in uveal melanoma. Cancer Cell. 32:204–220.e15. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Reichstein D: New concepts in the
molecular understanding of uveal melanoma. Curr Opin Ophthalmol.
28:219–227. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Field MG, Decatur CL, Kurtenbach S, Gezgin
G, van der Velden PA, Jager MJ, Kozak KN and Harbour JW: PRAME as
an independent biomarker for metastasis in uveal melanoma. Clin
Cancer Res. 22:1234–1242. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Field MG, Durante MA, Decatur CL, Tarlan
B, Oelschlager KM, Stone JF, Kuznetsov J, Bowcock AM, Kurtenbach S
and Harbour JW: Epigenetic reprogramming and aberrant expression of
PRAME are associated with increased metastatic risk in class 1 and
class 2 uveal melanomas. Oncotarget. 7:59209–59219. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Decatur CL, Ong E, Garg N, Anbunathan H,
Bowcock AM, Field MG and Harbour JW: Driver mutations in uveal
melanoma: Associations with gene expression profile and patient
outcomes. JAMA Ophthalmol. 134:728–733. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Diener-West M, Reynolds SM, Agugliaro DJ,
Caldwell R, Cumming K, Earle JD, Hawkins BS, Hayman JA, Jaiyesimi
I, Jampol LM, et al: Development of metastatic disease after
enrolment in the COMS trials for treatment of choroidal melanoma:
Collaborative ocular melanoma study group report no 26. Arch
Ophthalmol. 123:1639–1643. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Ramaiya KJ and Harbour JW: Current
management of uveal melanoma. Expert Rev Ophthalmol. 2:939–946.
2007. View Article : Google Scholar
|
|
43
|
Pandiani C, Béranger GE, Leclerc J,
Ballotti R and Bertolotto C: Focus on cutaneous and uveal melanoma
specificities. Genes Dev. 31:724–743. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Ny L, Nyakas M, Hernberg M, Koivunen J,
Oddershede L, Yoon MR, Wang X, Guyot P and Geisler J: BRAF mutation
as a prognostic marker for survival in malignant melanoma: A
systematic review and meta-analysis. J Clin Oncol. 36:e215662018.
View Article : Google Scholar
|
|
45
|
Wu J, Brunner G and Celebi JT: A melanoma
subtype: Uveal melanoma. J Am Acad Dermatol. 64:1185–1186. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Saldanha G, Purnell D, Fletcher A, Potter
L, Gillies A and Pringle JH: High BRAF mutation frequency does not
characterize all melanocytic tumor types. Int J Cancer.
111:705–710. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Van Raamsdonk CD, Griewank KG, Crosby MB,
Garrido MC, Vemula S, Wiesner T, Obenauf AC, Wackernagel W, Green
G, Bouvier N, et al: Mutations in GNA11 in uveal melanoma. N Engl J
Med. 363:2191–2199. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Van der Kooij MK, Speetjens FM, van der
Burg SH and Kapiteijn E: Uveal versus cutaneous melanoma; Same
origin, very distinct tumor types. Cancers (Basel). 11:8452019.
View Article : Google Scholar
|
|
49
|
Moore AR, Ceraudo E, Sher JJ, Guan Y,
Shoushtari AN, Chang MT, Zhang JQ, Walczak EG, Kazmi MA, Taylor BS,
et al: Recurrent activating mutations of G-Protein-coupled receptor
CYSLTR2 in uveal melanoma. Nat Genet. 48:675–680. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Johansson P, Aoude LG, Wadt K, Glasson WJ,
Warrier SK, Hewitt AW, Kiilgaard JF, Heegaard S, Isaacs T,
Franchina M, et al: Deep sequencing of uveal melanoma identifies a
recurrent mutation in PLCB4. Oncotarget. 7:4624–4631.
2016. View Article : Google Scholar
|
|
51
|
Dono M, Angelini G, Cecconi M, Amaro A,
Esposito AI, Mirisola V, Maric I, Lanza F, Nasciuti F, Viaggi S, et
al: Mutation frequencies of GNAQ, GNA11, BAP1, SF3B1, EIF1AX and
TERT in uveal melanoma: Detection of an activating mutation in the
TERT gene promoter in a single case of uveal melanoma. Br J Cancer.
110:1058–1065. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Horn S, Figl A, Rachakonda PS, Fischer C,
Sucker A, Gast A, Kadel S, Moll I, Nagore E, Hemminki K, et al:
TERT promoter mutations in familial and sporadic melanoma. Science.
339:959–961. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Griewank KG, Murali R, Schilling B, Scholz
S, Sucker A, Song M, Süsskind D, Grabellus F, Zimmer L, Hillen U,
et al: TERT promoter mutations in ocular melanoma distinguish
between conjunctival and uveal tumours. Br J Cancer. 109:497–501.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:646–674. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Bronkhorst IH and Jager MJ: Inflammation
in uveal melanoma. Eye (Lond). 27:217–223. 2013. View Article : Google Scholar
|
|
56
|
Maat W, Ly LV, Jordanova ES,
Wolff-Rouendaal D, Schalij-Delfos NE and Jager MJ: Monosomy of
chromosome 3 and an inflammatory phenotype occur together in uveal
melanoma. Invest Ophthalmol Vis Sci. 49:505–510. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Mahoney KM, Freeman GJ and McDermott DF:
The next immune-checkpoint inhibitors: PD-1/PD-L1 blockade in
melanoma. Clin Ther. 37:764–782. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Yun S, Vincelette ND, Green MR, Wahner
Hendrickson AE and Abraham I: Targeting immune checkpoints in
unresectable metastatic cutaneous melanoma: A systematic review and
Meta-analysis of anti-CTLA-4 and anti-PD-1 agents trials. Cancer
Med. 5:1481–1491. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Javed A, Arguello D, Johnston C, Gatalica
Z, Terai M, Weight RM, Orloff M, Mastrangelo MJ and Sato T: PD-L1
expression in tumor metastasis is different between uveal melanoma
and cutaneous melanoma. Immunotherapy. 9:1323–1330. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Mougiakakos D, Johansson CC, Trocme E,
All-Ericsson C, Economou MA, Larsson O, Seregard S and Kiessling R:
Intratumoral forkhead box P3-positive regulatory T cells predict
poor survival in cyclooxygenase-2-positive uveal melanoma. Cancer.
116:2224–2233. 2010.PubMed/NCBI
|
|
61
|
Lagouros E, Salomao D, Thorland E, Hodge
DO, Vile R and Pulido JS: Infiltrative T regulatory cells in
enucleated uveal melanomas. Trans Am Ophthalmol Soc. 107:223–228.
2009.
|
|
62
|
Bronkhorst IH, Vu TH, Jordanova ES, Luyten
GP, Burg SH and Jager MJ: Different subsets of tumor-infiltrating
lymphocytes correlate with macrophage influx and monosomy 3 in
uveal melanoma. Invest Ophthalmol Vis Sci. 53:5370–5378. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Petralia MC, Mazzon E, Fagone P, Russo A,
Longo A, Avitabile T, Nicoletti F, Reibaldi M and Basile MS:
Characterization of the pathophysiological role of CD47 in Uveal
melanoma. Molecules. 24:24502019. View Article : Google Scholar :
|
|
64
|
Basile MS, Mazzon E, Russo A, Mammana S,
Longo A, Bonfiglio V, Fallico M, Caltabiano R, Fagone P, Nicoletti
F, et al: Differential modulation and prognostic values of
immune-escape genes in uveal melanoma. PLoS One. 14:e02102762019.
View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Ding L, Lu S and Li Y: Regulation of
PD-1/PD-L1 pathway in cancer by noncoding RNAs. Pathol Oncol Res.
26:651–663. 2020. View Article : Google Scholar
|
|
66
|
Javed A, Arguello D, Johnston C, Gatalica
Z, Terai M, Weight RM, Orloff M, Mastrangelo MJ and Sato T: PD-L1
expression in tumor metastasis is different between uveal melanoma
and cutaneous melanoma. Immunotherapy. 9:1323–1330. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Durante MA, Rodriguez DA, Kurtenbach S,
Kuznetsov JN, Sanchez MI, Decatur CL, Snyder H, Feun LG,
Livingstone AS and Harbour JW: Single-cell analysis reveals new
evolutionary complexity in uveal melanoma. Nat Commun. 11(496)2020.
View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Babchia N, Landreville S, Clément B,
Coulouarn C and Mouriaux F: The bidirectional crosstalk between
metastatic uveal melanoma cells and hepatic stellate cells
engenders an inflammatory microenvironment. Exp Eye Res.
181:213–222. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Giulietti M, Vivenzio V, Piva F,
Principato G, Bellantuono C and Nardi B: How much do we know about
the coupling of G-proteins to serotonin receptors? Mol Brain.
7:492014. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Tschentscher F, Hüsing J, Holter T, Kruse
E, Dresen IG, Jöckel KH, Anastassiou G, Schilling H, Bornfeld N,
Horsthemke B, et al: Tumor classification based on gene expression
profiling shows that uveal melanomas with and without monosomy 3
represent two distinct entities. Cancer Res. 63:2578–2584.
2003.PubMed/NCBI
|
|
71
|
Bakalian S, Marshall JC, Logan P, Faingold
D, Maloney S, Di Cesare S, Martins C, Fernandes BF and Burnier MN
Jr: Molecular pathways mediating liver metastasis in patients with
uveal melanoma. Clin Cancer Res. 14:951–956. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
O'Hayre M, Degese MS and Gutkind JS: Novel
insights into G protein and G Protein-coupled receptor signaling in
cancer. Curr Opin Cell Biol. 27:126–135. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Liu H, Lei C, Long K, Yang X, Zhu Z, Zhang
L and Liu J: Mutant GNAQ promotes cell viability and migration of
uveal melanoma cells through the activation of Notch signaling.
Oncol Rep. 34:295–301. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Feng X, Degese MS, Iglesias-Bartolome R,
Vaque JP, Molinolo AA, Rodrigues M, Zaidi MR, Ksander BR, Merlino
G, Sodhi A, et al: Hippo-independent activation of YAP by the GNAQ
uveal melanoma oncogene through a trio-regulated rho GTPase
signaling circuitry. Cancer Cell. 25:831–845. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Harbour JW, Onken MD, Roberson ED, Duan S,
Cao L, Worley LA, Council ML, Matatall KA, Helms C and Bowcock AM:
Frequent mutation of BAP1 in metastasizing uveal melanomas.
Science. 330:1410–1413. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Coupland SE, Lake SL, Zeschnigk M and
Damato BE: Molecular pathology of uveal melanoma. Eye (Lond).
27:230–242. 2013. View Article : Google Scholar
|
|
77
|
Abdel-Rahman MH, Pilarski R, Cebulla CM,
Massengill JB, Christopher BN, Boru G, Hovland P and Davidorf FH:
Germline BAP1 mutation predisposes to uveal melanoma, lung
adenocarcinoma, meningioma, and other cancers. J Med Genet.
48:856–859. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Scheuermann JC, de Ayala Alonso AG, Oktaba
K, Ly-Hartig N, McGinty RK, Fraterman S, Wilm M, Muir TW and Müller
J: Histone H2A deubiquitinase activity of the polycomb repressive
complex PR-DUB. Nature. 465:243–247. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Eletr ZM and Wilkinson KD: An emerging
model for BAP1's role in regulating cell cycle progression. Cell
Biochem Biophys. 60:3–11. 2001. View Article : Google Scholar
|
|
80
|
He M, Chaurushiya MS, Webster JD,
Kummerfeld S, Reja R, Chaudhuri S, Chen YJ, Modrusan Z, Haley B,
Dugger DL, et al: Intrinsic apoptosis shapes the tumor spectrum
linked to inactivation of the deubiquitinase BAP1. Science.
364:283–285. 2019.PubMed/NCBI
|
|
81
|
Park JJ, Diefenbach RJ, Joshua AM, Kefford
RF, Carlino MS and Rizos H: Oncogenic signaling in uveal melanoma.
Pigment Cell Melanoma Res. 31:661–672. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Matatall KA, Agapova OA, Onken MD, Worley
LA, Bowcock AM and Harbour JW: BAP1 deficiency causes loss of
melanocytic cell identity in uveal melanoma. BMC Cancer.
13:3712013. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Oliva M, Rullan AJ and Piulats JM: Uveal
melanoma as a target for Immune therapy. Ann Transl Med. 4:1722016.
View Article : Google Scholar
|
|
84
|
Szalai E, Wells JR, Ward L and
Grossniklaus HE: Uveal melanoma nuclear BRCA1-associated Protein-1
immunoreactivity is an indicator of metastasis. Ophthalmology.
125:203–209. 2018. View Article : Google Scholar
|
|
85
|
Furney SJ, Pedersen M, Gentien D, Dumont
AG, Rapinat A, Desjardins L, Turajlic S, Piperno-Neumann S, de la
Grange P, Roman-Roman S, et al: SF3B1 mutations are associated with
alternative splicing in uveal melanoma. Cancer Discov. 3:1122–1129.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Amaro A, Gangemi R, Piaggio F, Angelini G,
Barisione G, Ferrini S and Pfeffer U: The biology of uveal
melanoma. Cancer Metastasis Rev. 36:109–140. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Yavuzyigitoglu S, Koopmans AE, Verdijk RM,
Vaarwater J, Eussen B, van Bodegom A, Paridaens D, Kiliç E and de
Klein A; Rotterdam Ocular Melanoma Study Group: Uveal melanomas
with SF3B1 mutations: A distinct subclass associated with
Late-onset metastases. Ophthalmology. 123:1118–1128. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Coltri PP, Dos Santos MGP and da Silva
GHG: Splicing and cancer: Challenges and opportunities. Wiley
Interdiscip Rev RNA. 10:e15272019. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Alsafadi S, Mobuchon L, Rodrigues M and
Stern MH: Uveal melanoma, a model disease for splicing alterations
and oncogenesis. Med Sci (Paris). 34:155–160. 2018.In French.
View Article : Google Scholar
|
|
90
|
Tanaka A, Kobayashi S, Xiao M and Inoue D:
Understanding and therapeutic targeting of aberrant mRNA splicing
mechanisms in oncogenesis. Rinsho Ketsueki. 61:643–650. 2020.In
Japanese.
|
|
91
|
Freemantle SJ, Spinella MJ and Dmitrovsky
E: Retinoids in cancer therapy and chemoprevention: Promise meets
resistance. Oncogene. 22:7305–7315. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Epping MT, Wang L, Edel MJ, Carlee L,
Hernandez M and Bernards R: The human tumor antigen PRAME is a
dominant repressor of retinoic acid receptor signaling. Cell.
122:835–847. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Etemadmoghadam D, Azar WJ, Lei Y, Moujaber
T, Garsed DW, Kennedy CJ, Fereday S, Mitchell C, Chiew YE, Hendley
J, et al: EIF1AX and NRAS Mutations Co-occur and Cooperate in
Low-grade serous ovarian carcinomas. Cancer Res. 77:4268–4278.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Krishnamoorthy GP, Davidson NR, Leach SD,
Zhao Z, Lowe SW, Lee G, Landa I, Nagarajah J, Saqcena M, Singh K,
et al: EIF1AX and RAS mutations cooperate to drive thyroid
tumorigenesis through ATF4 and C-MYC. Cancer Discov. 9:264–281.
2019. View Article : Google Scholar :
|
|
95
|
Bagnato A and Rosanò L: The endothelin
axis in cancer. Int J Biochem Cell Biol. 40:1443–1451. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Davenport AP, Hyndman KA, Dhaun N, Southan
C, Kohan DE, Pollock JS, Pollock DM, Webb DJ and Maguire JJ:
Endothelin. Pharmacol Rev. 68:357–418. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Pla P, Alberti C, Solov'eva O, Pasdar M,
Kunisada T and Larue L: Ednrb2 orients cell migration towards the
dorsolateral neural crest pathway and promotes melanocyte
differentiation. Pigment Cell Res. 18:181–187. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Smith SL, Damato BE, Scholes AG, Nunn J,
Field JK and Heighway J: Decreased endothelin receptor B expression
in large primary uveal melanomas is associated with early clinical
metastasis and short survival. Br J Cancer. 87:1308–1313. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Urtatiz O and Van Raamsdonk CD: Gnaq and
Gna11 in the endothelin signaling pathway and melanoma. Front
Genet. 7:592016. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Mallikarjuna K, Pushparaj V, Biswas J and
Krishnakumar S: Expression of epidermal growth factor receptor,
ezrin, hepatocyte growth factor, and c-Met in uveal melanoma: An
immunohistochemical study. Curr Eye Res. 32:281–290. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Franco R, Botti G, Mascolo M, Loquercio G,
Liguori G, Ilardi G, Losito S, La Mura A, Calemma R, Ierano C, et
al: CXCR4-CXCL12 and VEGF correlate to uveal melanoma progression.
Front Biosci (Elite Ed). 2:13–21. 2010. View Article : Google Scholar
|
|
102
|
Vivet-Noguer R, Tarin M, Roman-Roman S and
Alsafadi S: Emerging therapeutic opportunities based on current
knowledge of uveal melanoma Biology. Cancers (Basel). 11:10192019.
View Article : Google Scholar
|
|
103
|
Cheng H, Chua V, Liao C, Purwin TJ, Terai
M, Kageyama K, Davies MA, Sato T and Aplin AE: Co-targeting
HGF-CMET Signaling with MEK inhibitors in metastatic uveal
melanoma. Mol Cancer Ther. 116:516–528. 2017. View Article : Google Scholar
|
|
104
|
Abdel-Rahman MH, Yang Y, Zhou XP, Craig
EL, Davidorf FH and Eng C: High frequency of submicroscopic
hemizygous deletion is a major mechanism of loss of expression of
PTEN in uveal melanoma. J Clin Oncol. 24:288–295. 2006. View Article : Google Scholar
|
|
105
|
Walsh JC, Lebedev A, Aten E, Madsen K,
Marciano L and Kolb HC: The clinical importance of assessing tumor
hypoxia: Relationship of tumor hypoxia to prognosis and therapeutic
opportunities. Antioxid Redox Signal. 21:1516–1554. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Semenza GL: HIF-1: Upstream and downstream
of cancer metabolism. Curr Opin Genet Dev. 20:51–56. 2010.
View Article : Google Scholar :
|
|
107
|
Burroughs SK, Kaluz S, Wang D, Wang K, Van
Meir EG and Wang B: Hypoxia inducible factor pathway inhibitors as
anti-cancer therapeutics. Future Med Chem. 5:553–572. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Luke JJ, Triozzi PL, McKenna KC, Van Meir
EG, Gershenwald JE, Bastian BC, Gutkind JS, Bowcock AM, Streicher
HZ, Patel PM, et al: Biology of advanced uveal melanoma and next
steps for clinical therapeutics. Pigment Cell Melanoma Res.
28:135–147. 2015. View Article : Google Scholar :
|
|
109
|
Keith B, Johnson RS and Simon MC: HIF1α
and HIF2α: Sibling rivalry in hypoxic tumour growth and
progression. Nat Rev Cancer. 12:9–22. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Asnaghi L, Lin MH, Lim KS, Lim KJ,
Tripathy A, Wendeborn M, Merbs SL, Handa JT, Sodhi A, Bar EE and
Eberhart CG: Hypoxia promotes uveal melanoma invasion through
enhanced Notch and MAPK activation. PLoS One. 9:e1053722014.
View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Mouriaux F, Sanschagrin F, Diorio C,
Landreville S, Comoz F, Petit E, Bernaudin M, Rousseau AP, Bergeron
D and Morcos M: Increased HIF-1α expression correlates with cell
proliferation and vascular markers CD31 and VEGF-A in uveal
melanoma. Invest Ophthalmol Vis Sci. 55:1277–1283. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Hu K, Babapoor-Farrokhran S, Rodrigues M,
Deshpande M, Puchner B, Kashiwabuchi F, Hassan SJ, Asnaghi L, Handa
JT, Merbs S, et al: Hypoxia-inducible factor 1 upregulation of both
VEGF and ANGPTL4 is required to promote the angiogenic phenotype in
uveal melanoma. Oncotarget. 7:7816–7828. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Dong L, You S, Zhang Q, Osuka S, Devi NS,
Kaluz S, Ferguson JH, Yang H, Chen G, Wang B, et al:
Arylsulfonamide 64B inhibits Hypoxia/HIF-induced expression of
c-Met and CXCR4 and reduces primary tumor growth and metastasis of
uveal melanoma. Clin Cancer Res. 25:2206–2218. 2019. View Article : Google Scholar :
|
|
114
|
Brouwer NJ, Gezgin G, Wierenga APA,
Bronkhorst IHG, Marinkovic M, Luyten GPM, Versluis M, Kroes WGM,
van der Velden PA, Verdijk RM and Jager MJ: Tumour angiogenesis in
uveal melanoma is related to genetic evolution. Cancers (Basel).
11:9792019. View Article : Google Scholar
|
|
115
|
Brouwer NJ, Wierenga APA, Gezgin G,
Marinkovic M, Luyten GPM, Kroes WGM, Versluis M, van der Velden PA,
Verdijk RM and Jager MJ: Ischemia is related to tumour genetics in
uveal melanoma. Cancers (Basel). 11:10042019. View Article : Google Scholar
|
|
116
|
Spector A: Review: Oxidative stress and
disease. J Ocul Pharmacol Ther. 16:193–201. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Di Meo S, Reed TT, Venditti P and Victor
VM: Role of ROS and RNS sources in physiological and pathological
conditions. Oxid Med Cell Longev. 2016:12450492016. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Mitra D, Luo X, Morgan A, Wang J, Hoang
MP, Lo J, Guerrero CR, Lennerz JK, Mihm MC, Wargo JA, et al: An
ultraviolet-radiation-independent pathway to melanoma
carcinogenesis in the red hair/fair skin background. Nature.
491:449–453. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Reuter S, Gupta SC, Chaturvedi MM and
Aggarwal BB: Oxidative stress, inflammation, and cancer: How are
they linked? Free Radic Biol Med. 49:1603–1616. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Andrisic L, Dudzik D, Barbas C, Milkovic
L, Grune T and Zarkovic N: Short overview on metabolomics approach
to study pathophysiology of oxidative stress in cancer. Redox Biol.
14:47–58. 2018. View Article : Google Scholar
|
|
121
|
Piskounova E, Agathocleous M, Murphy MM,
Hu Z, Huddlestun SE, Zhao Z, Leitch AM, Johnson TM, DeBerardinis RJ
and Morrison SJ: Oxidative stress inhibits distant metastasis by
human melanoma cells. Nature. 527:186–1891. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Dithmer M, Kirsch AM, Gräfenstein L, Wang
F, Schmidt H, Coupland SE, Fuchs S, Roider J and Klettner AK: Uveal
melanoma cell under oxidative Stress-influence of VEGF and
VEGF-inhibitors. Klin Monbl Augenheilkd. 236:295–307. 2019.In
German. View Article : Google Scholar
|
|
123
|
Costa FF: Epigenomics in cancer
management. Cancer Manag Res. 2:255–265. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
124
|
Yang X, Gao L and Zhang S: Comparative
Pan-cancer DNA methylation analysis reveals cancer common and
specific patterns. Brief Bioinform. 18:761–773. 2017.
|
|
125
|
Maat W, van der Velden PA, Out-Luiting C,
Plug M, Dirks- Mulder A, Jager MJ and Gruis NA: Epigenetic
inactivation of RASSF1a in uveal melanoma. Invest Ophthalmol Vis
Sci. 48:486–490. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Dammann RH, Richter AM, Jiménez AP, Woods
M, Küster M and Witharana C: Impact of natural compounds on DNA
methylation levels of the tumor suppressor Gene RASSF1A in cancer.
Int J Mol Sci. 18:21602017. View Article : Google Scholar :
|
|
127
|
Maat W, Beiboer SH, Jager MJ, Luyten GP,
Gruis NA and van der Velden PA: Epigenetic regulation identifies
RASEF as a Tumor-suppressor gene in uveal melanoma. Invest
Ophthalmol Vis Sci. 49:1291–1298. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
128
|
Venza M, Visalli M, Biondo C, Lentini M,
Catalano T, Teti D and Venza I: Epigenetic regulation of p14ARF and
p16INK4A expression in cutaneous and uveal melanoma. Biochim
Biophys Acta. 1849:247–256. 2015. View Article : Google Scholar
|
|
129
|
Venza M, Visalli M, Catalano T, Fortunato
C, Oteri R, Teti D and Venza I: Impact of DNA methyltransferases on
the epigenetic regulation of tumor necrosis Factor-related
Apoptosis-inducing ligand (TRAIL) receptor expression in malignant
melanoma. Biochem Biophys Res Commun. 441:743–750. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
130
|
Van der Veiden PA, Metzelaar-Blok JA,
Bergman W, Hurks H, Frants RR, Gruis NA and Jager MJ: Promoter
Hypermethylation: A common cause of reduced P16(INK4a) expression
in uveal melanoma. Cancer Res. 61:5303–5306. 2001.
|
|
131
|
Li Y, Jia R and Ge S: Role of Epigenetics
in Uveal Melanoma. Int J Biol Sci. 13:426–4332. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
132
|
Yang ZK, Yang JY, Xu ZZ and Yu WH: DNA
Methylation and uveal melanoma. Chin Med J (Engl). 131:845–851.
2018. View Article : Google Scholar
|
|
133
|
Audia JE and Campbell RM: Histone
modifications and cancer. Cold Spring Harb Perspect Biol.
8:a0195212016. View Article : Google Scholar : PubMed/NCBI
|
|
134
|
Ding X, Wang X, Lin M, Xing Y, Ge S, Jia
R, Zhang H, Fan X and Li J: PAUPAR lncRNA suppresses tumourigenesis
by H3K4 demethylation in uveal melanoma. FEBS Lett. 590:1729–1738.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
135
|
Dong R, Liu J, Sun W and Ping W:
Comprehensive analysis of aberrantly expressed profiles of lncRNAs
and miRNAs with associated ceRNA Network in lung adenocarcinoma and
lung squamous cell carcinoma. Pathol Oncol Res. 26:1935–1945. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
136
|
Catalanotto C, Cogoni C and Zardo G:
MicroRNA in control of gene expression: An overview of nuclear
functions. Int J Mol Sci. 17:17122016. View Article : Google Scholar :
|
|
137
|
Rupaimoole R and Slack FJ: MicroRNA
therapeutics: Towards a new era for the management of cancer and
other diseases. Nat Rev Drug Discov. 16:203–222. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
138
|
Mishra S, Yadav T and Rani V: Exploring
miRNA based approaches in cancer diagnostics and therapeutics. Crit
Rev Oncol Hematol. 98:12–23. 2016. View Article : Google Scholar
|
|
139
|
Lopez-Rincon A, Martinez-Archundia M,
Martinez-Ruiz GU, Schoenhuth A and Tonda A: Automatic discovery of
100-miRNA signature for cancer classification using ensemble
feature selection. BMC Bioinformatics. 20:4802019. View Article : Google Scholar : PubMed/NCBI
|
|
140
|
Li Z, Yu X, Shen J and Jiang Y: MicroRNA
dysregulation in uveal melanoma: A new player enters the game.
Oncotarget. 6:4562–458. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
141
|
Yang C and Wei W: The miRNA expression
profile of the uveal melanoma. Sci China Life Sci. 54:351–358.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
142
|
Wang YC, Yang X, Wei WB and Xu XL: Role of
microRNA-21 in uveal melanoma cell invasion and metastasis by
regulating p53 and its downstream protein. Int J Ophthalmol.
11:1258–1268. 2018.
|
|
143
|
Radhakrishnan A, Badhrinarayanan N, Biswas
J and Krishnakumar S: Analysis of chromosomal aberration (1, 3, and
8) and association of microRNAs in uveal melanoma. Mol Vis.
15:2146–2154. 2009.PubMed/NCBI
|
|
144
|
Peng J, Liu H and Liu C: MiR-155 Promotes
uveal melanoma cell proliferation and invasion by regulating NDFIP1
expression. Technol Cancer Res Treat. 16:1160–1167. 2017.
View Article : Google Scholar
|
|
145
|
Li Y, Huang Q, Shi X, Jin X, Shen L, Xu X
and Wei W: MicroRNA 145 may play an important role in uveal
melanoma cell growth by potentially targeting insulin receptor
substrate 1. Chin Med J (Engl). 127:1410–1416. 2014.
|
|
146
|
Yan D, Zhou X, Chen X, Hu DN, Dong XD,
Wang J, Lu F, Tu L and Qu J: MicroRNA-34a inhibits uveal melanoma
cell proliferation and migration through downregulation of c-Met.
Invest Ophthalmol Vis Sci. 50:1559–1565. 2009. View Article : Google Scholar
|
|
147
|
Dong F and Lou D: MicroRNA-34b/c
suppresses uveal melanoma cell proliferation and migration through
multiple targets. Mol Vis. 18:537–546. 2012.PubMed/NCBI
|
|
148
|
Serocki M, Bartoszewska S,
Janaszak-Jasiecka A, Ochocka RJ, Collawn JF and Bartoszewski R:
miRNAs regulate the HIF switch during hypoxia: A novel therapeutic
target. Angiogenesis. 21:183–202. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
149
|
Sun L, Wang Q, Gao X, Shi D, Mi S and Han
Q: MicroRNA-454 functions as an oncogene by regulating PTEN in
uveal melanoma. FEBS Lett. 589:2791–2796. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
150
|
Ling J, Lu P, Zhang Y, Jiang S and Zhang
Z: MiR-367 promotes uveal melanoma cell proliferation and migration
by regulating PTEN. Genet Mol Res. 16:gmr160390672017. View Article : Google Scholar
|
|
151
|
Liu Y, Huo Y, Wang D, Tai Y, Li J, Pang D,
Zhang Y, Zhao W, Du N and Huang Y: MiR-216a-5p/Hexokinase 2 axis
regulates uveal melanoma growth through modulation of Warburg
effect. Biochem Biophys Res Commun. 50:885–892. 2018. View Article : Google Scholar
|
|
152
|
Singh AD, Turell ME and Topham AK: Uveal
melanoma: Trends in incidence, treatment, and survival.
Ophthalmology. 118:1881–1885. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
153
|
Kaliki S and Shields CL: Uveal melanoma:
Relatively rare but deadly cancer. Eye (Lond). 31:241–257. 2017.
View Article : Google Scholar
|
|
154
|
Triozzi PL and Singh AD: Blood biomarkers
for uveal melanoma. Future Oncol. 8:205–215. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
155
|
Cabel L, Proudhon C, Gortais H, Loirat D,
Coussy F, Pierga JY and Bidard FC: Circulating tumor cells:
Clinical validity and utility. Int J Clin Oncol. 22:421–430. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
156
|
Valpione S, Gremel G, Mundra P,
Middlehurst P, Galvani E, Girotti MR, Lee RJ, Garner G, Dhomen N,
Lorigan PC and Marais R: Plasma total Cell-free DNA (cfDNA) is a
surrogate biomarker for tumour burden and a prognostic biomarker
for survival in metastatic melanoma patients. Eur J Cancer. 88:1–9.
2018. View Article : Google Scholar :
|
|
157
|
Terai M, Mu Z, Eschelman DJ, Gonsalves CF,
Kageyama K, Chervoneva I, Orloff M, Weight R, Mastrangelo MJ,
Cristofanilli M and Sato T: Arterial blood, rather than venous
blood, is a better source for circulating melanoma cells.
EBioMedicine. 2:1821–1826. 2015. View Article : Google Scholar
|
|
158
|
Bidard FC, Madic J, Mariani P,
Piperno-Neumann S, Rampanou A, Servois V, Cassoux N, Desjardins L,
Milder M, Vaucher I, et al: Detection rate and prognostic value of
circulating tumor cells and circulating tumor DNA in metastatic
uveal melanoma. Int J Cancer. 134:1207–1213. 2014. View Article : Google Scholar
|
|
159
|
Schuster R, Bechrakis NE, Stroux A, Busse
A, Schmittel A, Thiel E, Foerster MH and Keilholz U: Prognostic
relevance of circulating tumor cells in metastatic uveal melanoma.
Oncology. 80:57–62. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
160
|
Tura A, Merz H, Reinsberg M, Lüke M, Jager
MJ, Grisanti S and Lüke J: Analysis of monosomy-3 in
immunomagnetically-isolated circulating melanoma cells in uveal
melanoma patients. Pigment Cell Melanoma Res. 29:583–589. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
161
|
Achberger S, Aldrich W, Tubbs R, Crabb JW,
Singh AD and Triozzi PL: Circulating immune cell and microRNA in
patients with uveal melanoma developing metastatic disease. Mol
Immunol. 58:182–186. 2014. View Article : Google Scholar :
|
|
162
|
Russo A, Caltabiano R, Longo A, Avitabile
T, Franco LM, Bonfiglio V, Puzzo L and Reibaldi M: Increased levels
of miRNA-146a in serum and histologic samples of patients with
uveal melanoma. Front Pharmacol. 7:4242016. View Article : Google Scholar : PubMed/NCBI
|
|
163
|
Eldh M, Olofsson Bagge R, Lässer C,
Svanvik J, Sjöstrand M, Mattsson J, Lindnér P, Choi DS, Gho YS and
Lötvall J: MicroRNA in exosomes isolated directly from the liver
circulation in patients with metastatic uveal melanoma. BMC Cancer.
14:9622014. View Article : Google Scholar : PubMed/NCBI
|
|
164
|
Stark MS, Gray ES, Isaacs T, Chen FK,
Millward M, McEvoy A, Zaenker P, Ziman M, Soyer HP, Glasson WJ, et
al: Panel of Circulating MicroRNAs detects uveal melanoma with high
precision. Transl Vis Sci Technol. 8:122019. View Article : Google Scholar
|
|
165
|
Peng L, Cantor DI, Huang C, Wang K, Baker
MS and Nice EC: Tissue and plasma proteomics for early stage cancer
detection. Mol Omics. 14:405–423. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
166
|
Karimi P, Shahrokni A and Ranjbar MR:
Implementation of proteomics for cancer research: Past, present,
and future. Asian Pac J Cancer Prev. 15:2433–2438. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
167
|
Reiniger IW, Schaller UC, Haritoglou C,
Hein R, Bosserhoff AK, Kampik A and Mueller AJ: 'Melanoma
inhibitory activity' (MIA): A promising serological tumour marker
in metastatic uveal melanoma. Graefes Arch Clin Exp Ophthalmol.
243:1161–1166. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
168
|
Haritoglou I, Wolf A, Maier T, Haritoglou
C, Hein R and Schaller UC: Osteopontin and 'melanoma inhibitory
activity': Comparison of two serological tumor markers in
metastatic uveal melanoma patients. Ophthalmologica. 223:239–243.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
169
|
Barak V, Frenkel S, Kalickman I, Maniotis
AJ, Folberg R and Pe'er J: Serum markers to detect metastatic uveal
melanoma. Anticancer Res. 27:1897–1900. 2007.PubMed/NCBI
|
|
170
|
Missotten GS, Tang NE, Korse CM, Hurks HM,
de Wolff-Rouendaal D, Keunen JE, Jager MJ and Bonfrer JM:
Prognostic value of S-100-beta serum concentration in patients with
uveal melanoma. Arch Ophthalmol. 121:1117–1119. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
171
|
Strobel K, Bode B, Dummer R, Veit-Haibach
P, Fischer DR, Imhof L, Goldinger S, Steinert HC and von Schulthess
GK: Limited value of 18F-FDG PET/CT and S-100B tumour marker in the
detection of liver metastases from uveal melanoma compared to liver
metastases from cutaneous melanoma. Eur J Nucl Med Mol Imaging.
36:1774–1782. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
172
|
Suesskind D, Schatz A, Schnichels S,
Coupland SE, Lake SL, Wissinger B, Bartz-Schmidt KU and Henke-Fahle
S: GDF-15: A novel serum marker for metastases in uveal melanoma
patients. Graefes Arch Clin Exp Ophthalmol. 250:887–895. 2012.
View Article : Google Scholar
|
|
173
|
Bande MF, Santiago M, Blanco MJ, Mera P,
Capeans C, Rodríguez-Alvarez MX, Pardo M and Piñeiro A: Serum
DJ-1/PARK 7 is a potential biomarker of choroidal nevi
transformation. Invest Ophthalmol Vis Sci. 53:62–67. 2012.
View Article : Google Scholar
|
|
174
|
Bande MF, Santiago M, Mera P, Piulats JM,
Blanco MJ, Rodríguez-Álvarez MX, Capeans C, Piñeiro A and Pardo M:
ME20-S as a potential biomarker for the evaluation of uveal
melanoma. Invest Ophthalmol Vis Sci. 56:7007–7011. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
175
|
Barisione G, Fabbi M, Gino A, Queirolo P,
Orgiano L, Spano L, Picasso V, Pfeffer U, Mosci C, Jager MJ, et al:
Potential Role of Soluble c-Met as a New candidate biomarker of
metastatic uveal melanoma. JAMA Ophthalmol. 133:1013–1021. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
176
|
Angi M, Kalirai H, Prendergast S, Simpson
D, Hammond DE, Madigan MC, Beynon RJ and Coupland SE: In-depth
proteomic profiling of the uveal melanoma secretome. Oncotarget.
7:49623–49635. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
177
|
Crabb JW, Hu B, Crabb JS, Triozzi P,
Saunthararajah Y, Tubbs R and Singh AD: iTRAQ quantitative
proteomic comparison of metastatic and non-metastatic uveal
melanoma tumors. PLoS One. 10:e01355432015. View Article : Google Scholar : PubMed/NCBI
|
|
178
|
Shi XY, Li Q, Wei WB and Tao LM: Peptidome
profiling of human serum of uveal melanoma patients based on
magnetic bead fractionation and mass spectrometry. Int J
Ophthalmol. 10:939–947. 2017.PubMed/NCBI
|
|
179
|
Song J, Merbs SL, Sokoll LJ, Chan DW and
Zhang Z: A multi-plex immunoassay of serum biomarkers for the
detection of uveal melanoma. Clin Proteomics. 16:102019. View Article : Google Scholar
|
|
180
|
Corrêa ZM: Assessing prognosis in uveal
melanoma. Cancer Control. 23:93–98. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
181
|
Balasubramanya R, Selvarajan SK, Cox M,
Joshi G, Deshmukh S, Mitchell DG and O'Kane P: Imaging of ocular
melanoma metastasis. Br J Radiol. 89:201600922016. View Article : Google Scholar : PubMed/NCBI
|
|
182
|
Smit KN, Jager MJ, de Klein A and Kiliç E:
Uveal melanoma: Towards a molecular understanding. Prog Retin Eye
Res. 75:1008002020. View Article : Google Scholar
|
|
183
|
Schopper VJ and Correa ZM: Clinical
application of genetic testing for posterior uveal melanoma. Int J
Retina Vitreous. 2:42016. View Article : Google Scholar : PubMed/NCBI
|
|
184
|
Damato B, Dopierala JA and Coupland SE:
Genotypic profiling of 452 choroidal melanomas with multiplex
Ligation-dependent probe amplification. Clin Cancer Res.
16:6083–6092. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
185
|
Dogrusöz M, Jager MJ and Damato B: Uveal
melanoma treatment and prognostication. Asia Pac J Ophthalmol
(Phila). 6:186–196. 2017.
|
|
186
|
Onken MD, Worley LA, Char DH, Augsburger
JJ, Correa ZM, Nudleman E, Aaberg TM Jr, Altaweel MM, Bardenstein
DS, Finger PT, et al: Collaborative Ocular Oncology Group report
number 1: Prospective validation of a Multi-gene prognostic assay
in uveal melanoma. Ophthalmology. 119:1596–1603. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
187
|
Royer-Bertrand B, Torsello M, Rimoldi D,
El Zaoui I, Cisarova K, Pescini-Gobert R, Raynaud F, Zografos L,
Schalenbourg A, Speiser D, et al: Comprehensive genetic landscape
of uveal melanoma by whole-genome sequencing. Am J Hum Genet.
99:1190–1198. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
188
|
Chattopadhyay C, Kim DW, Gombos DS, Oba J,
Qin Y, Williams MD, Esmaeli B, Grimm EA, Wargo JA, Woodman SE and
Patel SP: Uveal melanoma: From diagnosis to treatment and the
science in between. Cancer. 122:2299–2312. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
189
|
Frizziero L, Midena E, Trainiti S, Londei
D, Bonaldi L, Bini S and Parrozzani R: Uveal melanoma biopsy: A
review. Cancers (Basel). 11:10752019. View Article : Google Scholar
|
|
190
|
Erim Y, Scheel J, Breidenstein A, Metz CH,
Lohmann D, Friederich HC and Tagay SP: Psychosocial impact of
prognostic genetic testing in the care of uveal melanoma patients:
Protocol of a controlled prospective clinical observational. BMC
Cancer. 16:4082016. View Article : Google Scholar
|
|
191
|
Damato B and Coupland SE: Translating
uveal melanoma cytogenetics into clinical care. Arch Ophthalmol.
127:423–429. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
192
|
Harbour JW: Molecular prognostic testing
and individualized patient care in uveal melanoma. Am J Ophthalmol.
148:823–829.e1. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
193
|
Aaberg TM Jr, Cook RW, Oelschlager K,
Maetzold D, Rao PK and Mason JO III: Current clinical practice:
Differential management of uveal melanoma in the era of molecular
tumor analyses. Clin Ophthalmol. 8:2449–2460. 2014. View Article : Google Scholar
|
|
194
|
Schoenfield L, Pettay J, Tubbs RR and
Singh AD: Variation of monosomy 3 status within uveal melanoma.
Arch Pathol Lab Med. 133:1219–1222. 2009.PubMed/NCBI
|
|
195
|
Nathan P, Cohen V, Coupland S, Curtis K,
Damato B, Evans J, Fenwick S, Kirkpatrick L, Li O, Marshall E, et
al: Uveal melanoma UK national guidelines. Eur J Cancer.
51:2404–2412. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
196
|
Álvarez-Rodríguez B, Latorre A, Posch C
and Somoza Á: Recent advances in uveal melanoma treatment. Med Res
Rev. 37:1350–1372. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
197
|
Damato BE, Dukes J, Goodall H and Carvajal
RD: Tebentafusp: T cell redirection for the treatment of metastatic
uveal melanoma. Cancers (Basel). 11:9712019. View Article : Google Scholar
|
|
198
|
Schank TE and Hassel JC: Immunotherapies
for the treatment of uveal melanoma-history and future. Cancers
(Basel). 11:10482019. View Article : Google Scholar
|
|
199
|
Bol K, van den Bosch T, Schreibelt G, Punt
C, Figdor C, Paridaens D and de Vries J: Adjuvant dendritic cell
vaccination in high-risk uveal melanoma patients. J Immuno Ther
Cancer:. 3:2015.
|
|
200
|
Thota R, Johnson DB and Sosman JA:
Trametinib in the treatment of melanoma. Expert Opin Biol Ther.
15:735–747. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
201
|
Carvajal RD, Piperno-Neumann S, Kapiteijn
E, Chapman PB, Frank S, Joshua AM, Piulats JM, Wolter P, Cocquyt V,
Chmielowski B, et al: Selumetinib in combination with dacarbazine
in patients with metastatic uveal melanoma: A Phase III,
Multicenter, randomized trial (SUMIT). J Clin Oncol. 36:1232–1239.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
202
|
Brighton HE, Angus SP, Bo T, Roques J,
Tagliatela AC, Darr DB, Karagoz K, Sciaky N, Gatza ML, Sharpless
NE, et al: New mechanisms of resistance to MEK inhibitors in
melanoma revealed by intravital imaging. Cancer Res. 78:542–557.
2018. View Article : Google Scholar :
|
|
203
|
Cheng H, Chua V, Liao C, Purwin TJ, Terai
M, Kageyama K, Davies MA, Sato T and Aplin AE: Co-targeting
HGF/cMET Signaling with MEK inhibitors in metastatic uveal
melanoma. Mol Cancer Ther. 16:516–528. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
204
|
Faião-Flores F, Emmons MF, Durante MA,
Kinose F, Saha B, Fang B, Koomen JM, Chellappan SP, Maria-Engler
SS, Rix U, et al: HDAC inhibition enhances the in vivo efficacy of
MEK inhibitor therapy in uveal melanoma. Clin Cancer Res.
25:5686–5701. 2019. View Article : Google Scholar
|
|
205
|
Landreville S, Agapova OA, Matatall KA,
Kneass ZT, Onken MD, Lee RS, Bowcock AM and Harbour JW: Histone
deacetylase inhibitors induce growth arrest and differentiation in
uveal melanoma. Clin Cancer Res. 18:408–416. 2012. View Article : Google Scholar :
|
|
206
|
Bonnal S, Vigevani L and Valcárcel J: The
spliceosome as a target of novel antitumour drugs. Nat Rev Drug
Dis. 11:847–859. 2012. View Article : Google Scholar
|
|
207
|
Yoshimoto R, Kaida D, Furuno M, Burroughs
AM, Noma S, Suzuki H, Kawamura Y, Hayashizaki Y, Mayeda A and
Yoshida M: Global analysis of pre-mRNA subcellular localization
following splicing inhibition by spliceostatin A. RNA. 23:47–57.
2017. View Article : Google Scholar :
|
|
208
|
Wu G, Fan L, Edmonson MN, Shaw T, Boggs K,
Easton J, Rusch MC, Webb TR, Zhang J and Potter PM: Inhibition of
SF3B1 by molecules targeting the spliceosome results in massive
aberrant exon skipping. RNA. 24:1056–1066. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
209
|
Zhou Z, Gong Q, Wang Y, Li M, Wang L, Ding
H and Li P: The biological function and clinical significance of
SF3B1 mutations in cancer. Biomarker Res. 8(38)2020. View Article : Google Scholar
|
|
210
|
García M, Moreno R, Gil-Martin M, Cascallò
M, de Olza MO, Cuadra C, Piulats JM, Navarro V, Domenech M, Alemany
R and Salazar R: A Phase 1 Trial of Oncolytic adenovirus ICOVIR-5
administered intravenously to cutaneous and uveal melanoma
patients. Hum Gene Ther. 30:352–364. 2019. View Article : Google Scholar
|