Introduction
Desmoid tumors (DTs) are benign tumors that exhibit
fibroblastic proliferation, which arises from fascial or
musculoaponeurotic structures. This type of tumor is rare and
accounts for 0.003% of all neoplasms (1,2).
This connective tissue hyperplasia infiltrates locally and may
result in debilitating pain. This type of tumor does not usually
metastasize, although it tends to recur locally following surgical
excision (3–5). DTs are poorly circumscribed and grow
along tissue planes with a peculiar, infiltrative-like pattern
toward the mesenchymal tissues; however, they do not spare the
connective support of the viscera, glands or teguments. These
pathological characteristics emphasize the high incidence of local
recurrences, even in patients with a pathologically confirmed
negative surgical margin (SM) (6).
DTs may be sporadic, or associated with familial adenomatous
polyposis (FAP) and Gardner’s syndrome. Approximately 2% of all DTs
are associated with FAP, with these patients exhibiting a
1,000-fold increased risk of developing this type of tumor compared
to the general population.
Surgical excision with clear margins is currrently
the mainstay of treatment. Radiotherapy (RT) may be administered in
cases where there is a locally positive SM, or when repeat surgery
may prove to be difficult. Extensive surgery, with or without RT,
may achieve a control rate of >60% (7–10).
Systemic agents used for the treatment of DTs include
doxorubicin-based combinations, methotrexate/vinblastine, tyrosine
kinase inhibitors, tamoxifen, non-steroidal anti-inflammatory
drugs, such as indomethacin and sulindac, and colchicine. Since
this is a rare type of tumor, there is currently no established or
evidence-based approach for the treatment of these neoplasms in the
available literature.
The aim of this study was to determine the
clinicopathological characteristics, treatment details and clinical
course of patients with DTs.
Materials and methods
Patient characteristics
We retrospectively examined the charts of 21
patients who had been diagnosed with DT between January, 2005 and
December, 2010. The patients were evaluated by a pathologist, a
radiologist, an orthopedic surgeon, a radiation oncologist and a
medical oncologist at our institute for definitive treatment and
all the patients had histologically confirmed DTs. In addition, a
colonoscopy was performed to confirm or exclude polyposis coli
syndrome. The clinical records were reviewed and information
regarding age, gender, tumor site, surgical details, pathological
margin status, adjuvant therapy and treatment of recurrences was
collected. The patients received 50–60 gray (Gy) RT.
This retrospective study was approved by the
Institutional Review Board of the Institute of Oncology, University
of Istanbul.
Statistical analysis
Data are presented as median and inter-quartile
range (IQR) for events such as time to relapse after surgery. Age
and follow-up time were expressed as median and range,
respectively. The Chi-square and Mann-Whitney U tests were used for
comparisons among the groups and the overall survival and
progression-free survival (PFS) rates were calculated utilizing the
Kaplan-Meier method. All analyses were performed using the SPSS
statistical software, version 15.0 (SPSS Inc., Chicago, IL, USA).
Two-sided P<0.05 was considered to indicate a statistically
significant difference.
Results
Patient characteristics
After examining patient records over a 5-year
period, 21 patients with DTs [16 females (76.2%) and 5 males
(23.8%)] were identified and included in this study. The median age
of the subjects was 28 years (range, 12–52 years). The patient
characteristics, treatment details and patterns of relapse are
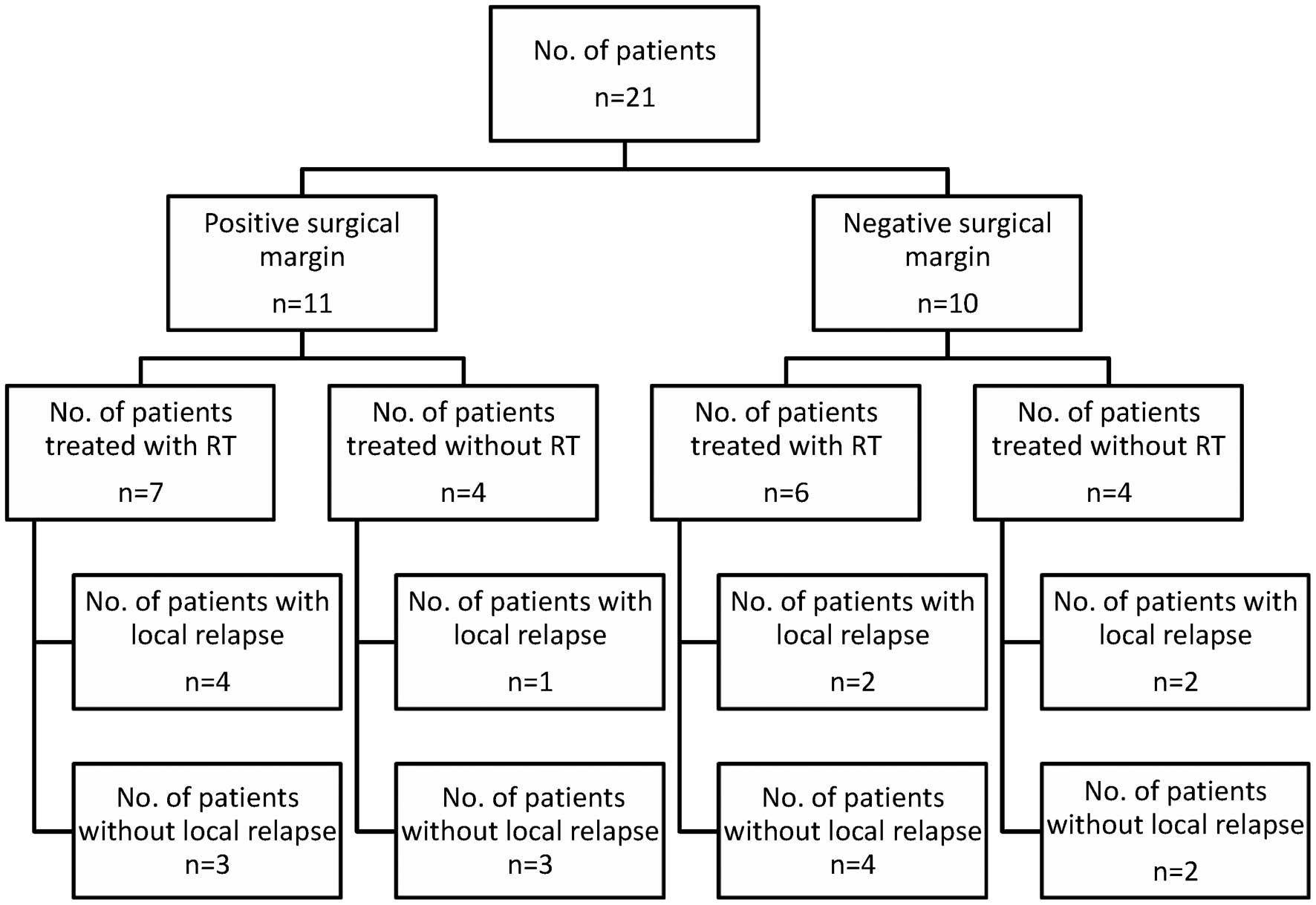
presented in Table I and Fig. 1. Seven tumors were located in the
lower extremities (1 in the calf, 3 in the buttocks, 2 in the knees
and 1 in the popliteal fossa). Four tumors were located in the
upper extremities (2 in the shoulder, 1 in the upper arm and 1 in
the forearm). Nine tumors were located in the abdomen and 1 in the
neck. Additionally, 2 patients were diagnosed with Gardner’s
syndrome and FAP (cases 5 and 14, respectively). The mean tumor
size was 10.6 cm at presentation (range, 1.5–40 cm), 6.3 cm at the
first relapse (range, 1.5–13 cm) and 2.6 cm at the second relapse
(range, 1.3–4 cm).
 | Table I.Clinical characteristics and treatment
options of 21 patients with desmoid tumors. |
Table I.
Clinical characteristics and treatment
options of 21 patients with desmoid tumors.
| No. | Age (yrs)/gender | Primary site | Size (cm) | SM | Adjuvant
treatment | Recurrence | Treatment for
recurrence | Last follow-up | PFS | OS |
|---|
| 1 | 12/M | Popliteal fossa | 22×17×11 | + | RT | 2 | Surgery (R1–2), RT
(R2) | NED | 91 | 91 |
| 2 | 12/F | Calf | 17×15×5 | + | None | 2 | Surgery (R1) + RT
(R2) | NED | 4 | 16 |
| 3 | 14/F | Knee | 4×3×2.4 | + | RT | 3 | Surgery (R1–3),
chemotherapy (R3, MTX) | NED | 18 | 53 |
| 4 | 20/F | Forearm | 8×4×3 | + | None | None | None | NED | 67 | 67 |
| 5 | 22/F | Abdomen | 13×8×8.5 | − | None | 4 | Surgery (R1–4), RT
(R2) + chemotherapy (TAM, TAL) | Exitus | 1 | 59 |
| 6 | 23/M | Upper arm | 4.2×3.5×3 | − | RT | None | None | NED | 114 | 114 |
| 7 | 25/M | Knee | 1.5×0.2 | − | RT | 1 | Chemotherapy (R1,
MTX) | NED | 17 | 24 |
| 8 | 26/F | Buttocks | 7×4×1.5 | − | RT | None | None | NED | 123 | 123 |
| 9 | 27/F | Shoulder | 9×3×2 | − | RT | 2 | Surgery (R1),
chemotherapy (see results in text) | AWD | 153 | 170 |
| 10 | 27/F | Abdomen | 7.5×5×2.5 | + | None | None | None | NED | 53 | 53 |
| 11 | 28/F | Abdomen | 4×3.6×1.6 | − | RT | None | None | NED | 8 | 8 |
| 12 | 30/F | Buttocks | 12×8×7.5 | − | RT | None | None | NED | 23 | 23 |
| 13 | 32/M | Abdomen | 2.5×2×2 | + | RT | None | None | NED | 6 | 6 |
| 14 | 35/F | Abdomen | 13×10×5 | − | None | None | None | NED | 3 | 3 |
| 15 | 36/F | Neck | 3×2×1.5 | + | RT | 5 | Surgery (R1–5), RT
(R1, R2) + chemotherapy (R3 EPI, R4 IMA, R5 TAM) | NED | 11 | 43 |
| 16 | 36/F | Abdomen | 2.5×1.6×1 | − | None | 1 | Surgery | NED | 62 | 62 |
| 17 | 36/F | Buttocks | 11×10×8 | + | RT | None | None | NED | 108 | 113 |
| 18 | 36/F | Abdomen | 6.2×3.3 | + | None | None | None | NED | 37 | 37 |
| 19 | 38/F | Abdomen | 16×15×11 | − | None | None | None | NED | 2 | 2 |
| 20 | 41/M | Abdomen | 19×13×6.5 | + | RT | None | None | NED | 50 | 50 |
| 21 | 52/F | Shoulder | 40×10×10 | + | RT | 2 | Surgery (R1–2), RT
(R2) | NED | 108 | 219 |
Follow-up
The median follow-up time was 53 months (range,
2–219 months). None of the patients developed distant metastasis.
All the patients were initially treated by surgical excision and 13
patients also received RT. Five of the 11 patients (45%) with a
positive SM and 4 of the 10 patients (40%) with a negative SM
experienced a tumor relapse. The local recurrence rate was not
significantly different between patients with positive and those
with negative SM. Two patients had only 1 local recurrence and 7
patients had >1 recurrence. Of the 21 patients, 9 (42.8%)
suffered a local relapse [3 of the 8 patients (38%) who received RT
and 6 of the 13 patients (46%) who did not receive RT] (P>0.05).
In addition, 2 of the 6 patients with a negative SM who were
treated with postoperative RT also developed a local recurrence.
The median PFS was 20.5 months (IQR: 2.25–63.5) in patients treated
by surgical excision alone and 50 months (IQR: 14–111) in those who
had surgery followed by RT (P>0.05).
Treatment
The patients received different systemic drugs, such
as adriamycin, epirubicin, methotrexate, tamoxifen and thalidomide.
In case 9, the DT transformed into a fibrosarcoma at the primary
site. The patient subsequently developed lung metastasis during
pregnancy and was treated with 3 cycles of single-agent adriamycin
during pregnancy, followed by adriamycin and ifosfamide after
pregnancy. The patient with Gardner’s syndrome underwent repetitive
surgeries, RT and systemic treatment and eventually died from
cranial hemorrhage, unrelated to her disease. None of the evaluated
parameters, including age, gender, tumor site, tumor size or tumor
border were correlated with the risk of local recurrence.
Discussion
The primary treatment for DTs is surgical resection
with a wide SM. However, complete resection of the tumor with
negative microscopic margins is often constrained by anatomical
boundaries. The role of RT in the treatment of DTs has not been
clearly defined. In the literature, a positive SM was shown to be a
negative predictive factor for relapse-free survival (RFS).
Systemic agents like imatinib and methotrexate are often used for
patients for whom local therapy is not suitable.
DTs have a high rate of recurrence, even following
complete surgical removal, and the contribution of a positive SM to
local recurrence rates has not yet been determined. The recurrence
rates of patients with resection and a negative SM were reported to
be 16–39% (10–12). In addition, previous studies
indicated that the risk of recurrence is independent of the margin
status (13,14). In one of the largest series, 203
patients who underwent surgery for either primary or recurrent DT
over a 35-year period were evaluated and the margins were found to
be microscopically positive in 57 of the participants and negative
in the remaining 146 (15). That
study also demonstrated that patients with a positive margin had a
5-year RFS rate of 79% and a 10-year RFS rate of 74%, whereas those
with a negative margin had a 5-year RFS rate of 82% and a 10-year
RFS rate of 77% (P=0.5). In our series, the recurrence rate for
patients with and without a positive SM were 45 and 40%,
respectively (P>0.05).
RT has often been used for patients with a positive
SM in oncology practice. However, the role of RT for DTs with a
positive SM has not been established. Previous studies reported
that RT alone (50–60 Gy) or RT combined with surgery in patients
with incomplete resection achieved long-term disease control in
∼70–80% of DT patients (12,16,17).
Spear et al (18)
demonstrated that the 5-year local control rate of patients treated
with a combination of surgery and RT (n=41) was 72%. Another study
on 52 patients who were treated with RT in conjunction with gross
total resection of the tumor, the 5- and 10-year relapse rates were
18 and 23%, respectively (16).
The local control rate in patients treated with a combination of
surgery and RT was 54% in our series. Even if RT was considered to
be an option for the non-surgical definitive therapy of DTs, there
would be an increased risk of potential late side effects,
including secondary malignancies, particularly in younger patients,
and RT-related fibrosis. Out of the 14 patients (7%) treated with
RT in our series, 1 patient developed a fibrosarcoma.
Currently, repetitive surgery is considered the
treatment of choice; however, certain patients may have an
unpredictable clinical course. Therefore, a period of conservative
management (systemic therapy or monitoring and assessing tumor
progression) may be considered, particularly if resection may
entail major morbidity (3,19). In a previous retrospective study,
83 patients underwent a ‘wait and see’ policy, whereas 59 patients
were administered systemic therapy (20). The 5-year PFS in that study was
49.9% for the ‘wait and see’ group and 58.6% for the group treated
with hormonal therapy or chemo-therapy (P=0.32). A multivariate
analysis identified no clinical variables that may be considered
independent predictors of PFS. However, all the patients in our
series received treatment.
There are no evidence-based or widely accepted
guidelines for the management of unresectable DTs. Systemic therapy
is increasingly being integrated into a multidisciplinary approach
for selected patients with unresectable or intra-abdominal DTs for
which local therapy options may lead to unacceptable morbidity.
However, our results were insufficient for interpreting the role of
systemic agents in the management of such tumors. We may only
suggest that systemic agents may be a part of the treatment
approach.
In conclusion, DTs may be challenging due to their
variable biological behavior and local morbidity, although their
metastatic potential is low. Surgery remains the standard treatment
option for resectable tumors. The effect of a positive SM, RT and
systemic agents on recurrence have not yet been fully determined.
With a better understanding of the molecular and genetic basis of
this disease, targeted therapies with minimal toxicity profiles may
become a more attractive treatment option in the future.
References
|
1.
|
Pikaar A, Nortier JW, Griffioen G and
Vasen HF: Desmoid tumors in patients with familial adenomatous
polyposis. Ned Tijdschr Geneeskd. 146:1355–1359. 2001.(In
Dutch).
|
|
2.
|
Reitamo JJ, Hayry P, Nykyri E and Saxen E:
The desmoid tumor. I. incidence, sex, age and anatomical
distribution in the Finnish population. Am J Clin Pathol.
77:665–673. 1982.PubMed/NCBI
|
|
3.
|
Lewis JJ, Boland PJ, Leung DH, Woodruff JM
and Brennan MF: The enigma of desmoid tumors. Ann Surg.
229:866–873. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Wara WM, Phillips TL, Hill DR, et al:
Desmoid tumors - treatment and prognosis. Radiology. 124:225–226.
1977. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Khorsand J and Karakousis CP: Desmoid
tumors and their management. Am J Surg. 149:215–218. 1985.
View Article : Google Scholar
|
|
6.
|
Posner MC, Shiu MH, Newsome JL, Hajdu SI,
Gaynor JJ and Brennan MF: The desmoid tumor. Not a benign disease.
Arch Surg. 124:191–196. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Anthony T, Rodriguez-Bigas MA, Weber TK
and Petrelli NJ: Desmoid tumors. J Am Coll Surg. 182:369–377.
1996.
|
|
8.
|
Lynch HT and Fitzgibbons R: Surgery,
desmoid tumors, and familial adenomatous polyposis: case report and
literature review. Am J Gastroenterol. 91:2598–2601.
1996.PubMed/NCBI
|
|
9.
|
Merchant NB, Lewis JJ, Wodruff JM, Leung
DH and Brennan MF: Extremity and trunk desmoid tumors: a
multifactorial analysis outcome. Cancer. 86:2045–2052. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Ballo MT, Zagars GK, Pollack A, Pisters PW
and Pollack RA: Desmoid tumor: prognostic factors and outcome after
surgery, radiation therapy, or combined surgery and radiation
therapy. J Clin Oncol. 17:158–167. 1999.PubMed/NCBI
|
|
11.
|
Meazza C, Bisogno G, Gronchi A, et al:
Aggressive fibromatosis in children and adolescents: the Italian
experience. Cancer. 116:233–240. 2010.PubMed/NCBI
|
|
12.
|
Nuyttens JJ, Rust PF, Thomas CR and
Turrisi AT III: Surgery versus radiation therapy for patients with
aggressive fibromatosis or desmoid tumors: a comparative review of
22 articles. Cancer. 88:1517–1523. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Lev D, Kotilingam D, Wei C, et al:
Optimizing treatment of desmoid tumors. J Clin Oncol. 25:1785–1791.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Reitamo JJ: The desmoid tumor. IV. Choice
of treatment, results, and complications. Arch Surg. 118:1318–1322.
1983. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Gronchi A, Casali PG, Mariani L, et al:
Quality of surgery and outcome in extra-abdominal aggressive
fibromatosis: a series of patients surgically treated at a single
institution. J Clin Oncol. 21:1390–1397. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Ballo MT, Zagars GK and Pollack A:
Radiation therapy in the management of desmoid tumors. Int J Radiat
Oncol Biol Phys. 42:1007–1014. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Micke O and Seegenschmiedt MH: Radiation
therapy for aggressive fibromatosis (desmoid tumors): results of a
national patterns of care study. Int J Radiat Oncol Biol Phys.
61:882–891. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Spear MA, Jennings LC, Mankin HJ, et al:
Individualizing management of aggressive fibromatoses. Int J Radiat
Oncol Biol Phys. 40:637–645. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Bonvalot S, Eldweny H, Haddad V, et al:
Extra-abdominal primary fibromatosis: Aggressive management could
be avoided in a subgroup of patients. Eur J Surg Oncol. 34:462–468.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Fiore M, Rimareix F, Mariani L, et al:
Desmoid-type fibromatosis: a front-line conservative approach to
select patients for surgical treatment. Ann Surg Oncol.
16:2587–2593. 2009. View Article : Google Scholar : PubMed/NCBI
|