Article
Open Access
Modified miccoli's thyroid surgery for thyroid diseases
- Authors:
- Hui Yu
- Xin Ge
- Weikang Pan
- Huaijie Wang
- Qiang Huang
- Yu Dong
- Ya Gao
- Jianjun Yu
-
View Affiliations / Copyright
Affiliations:
Department of Pediatric Surgery, The Second Affiliated Hospital, School of Medicine, Xi'an Jiaotong University, Xi'an, Shaanxi 710004, P.R. China, Department of Minimally Invasive Surgery, The People's Hospital of Ningxia Hui Autonomous Region, Yinchuan, Ningxia 750001, P.R. China
-
Pages:
1014-1018
|
Published online on:
July 1, 2015
https://doi.org/10.3892/mco.2015.597
- Expand metrics +
Metrics:
Total
Views: 0
(Spandidos Publications: | PMC Statistics:
)
Metrics:
Total PDF Downloads: 0
(Spandidos Publications: | PMC Statistics:
)
This article is mentioned in:
Abstract
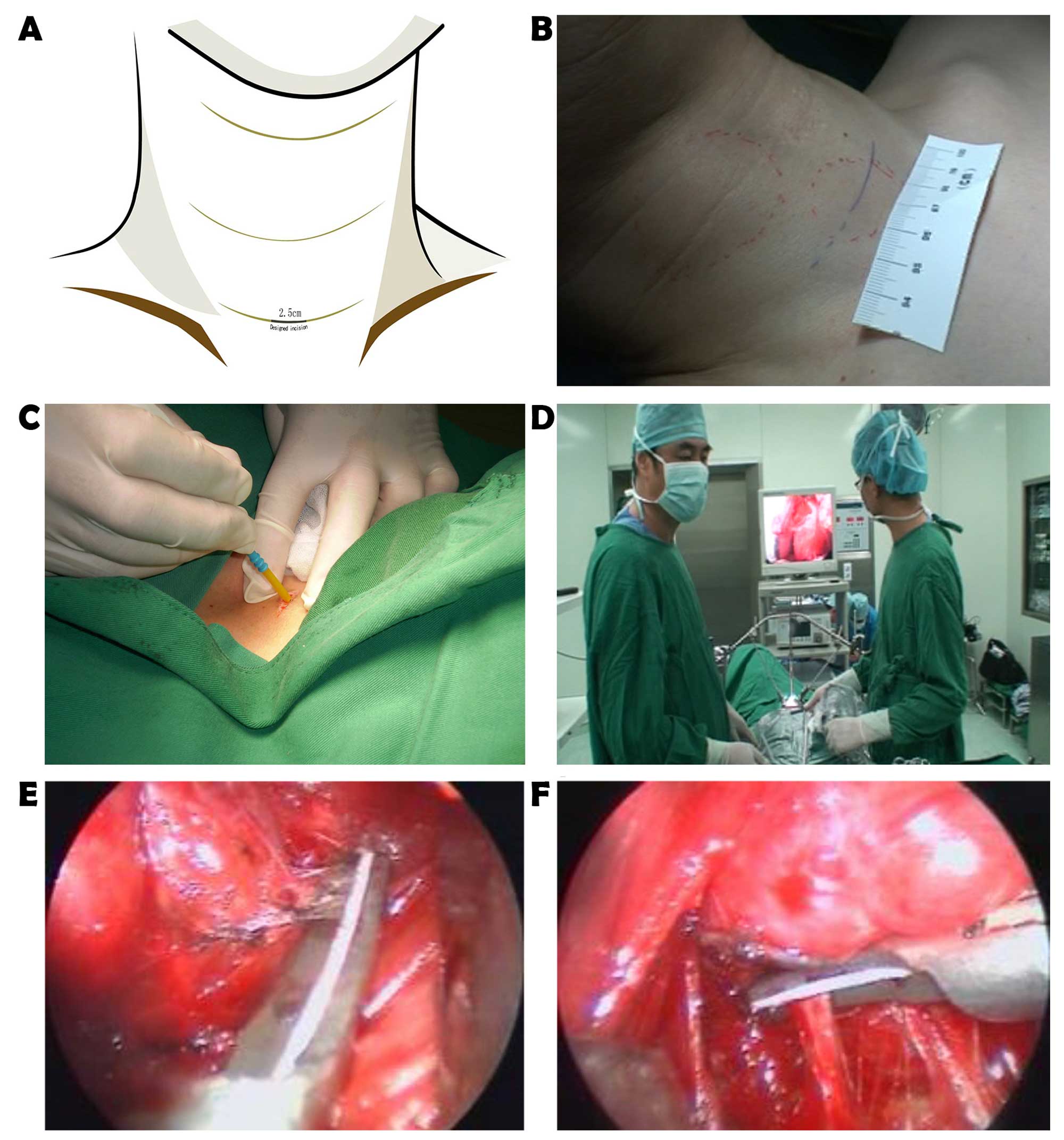
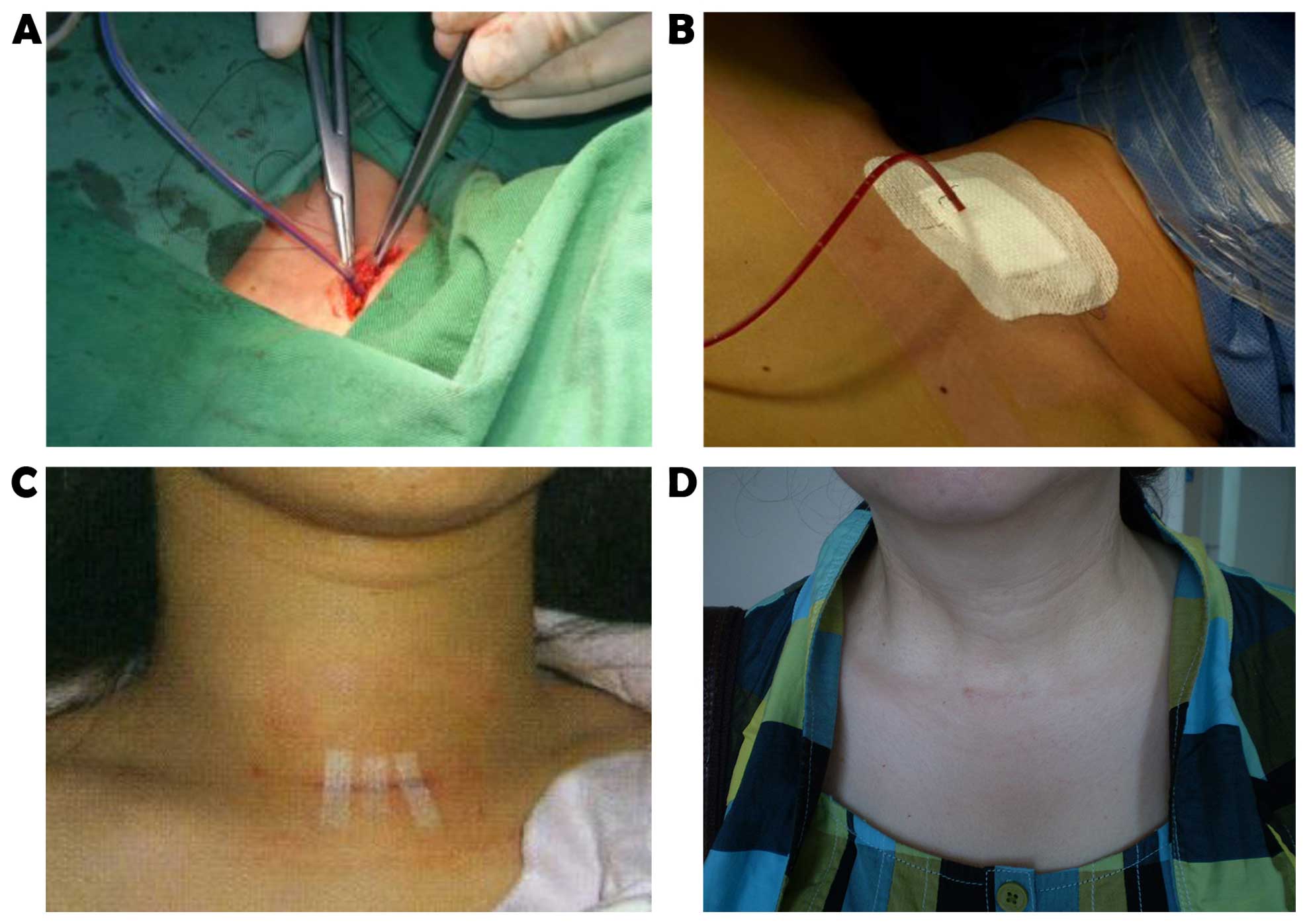
Minimally invasive video-assisted thyroidectomy (MIVAT), originally described by Miccoli, is considered to be the most widely practiced and easily reproducible procedure for selected patients with benign and̸or malignant thyroid nodules. Modified techniques based on MIVAT, namely modified Miccoli's thyroid surgery (MMTS), were developed based on MIVAT. This study aimed to evaluate the preliminary results of MMTS compared with those of MIVAT. The enrolling criteria included a benign nodule <3.5 cm in diameter, a malignant tumor <2 cm, no previous neck surgery and no evidence of any suspected lymph node metastasis or local invasion. Unilateral lobectomy was considered for benign lesions and the additional dissection of central compartment (level VI) lymph nodes was applied for malignant disease. The modified techniques included carefully selecting the operative incision, expanding the operative space, embedding a drainage tube in situ and delicately suturing every layer inwards and crosswise, as well as measuring cervical motion. In addition to the comparison of surgical outcomes between MMTS and MIVAT, other surgical parameters, including operative time, blood loss, postoperative drainage, cosmetic satisfaction, peak angle of cervical rotation, length of hospitalization and complications, were retrospectively analyzed. A consecutive series of 70 patients, including 54 cases of benign and 16 cases of malignant disease, initially underwent MIVAT between April, 2008 and May, 2012, while 127 patients, including 98 benign and 29 malignant cases, subsequently underwent MMTS between September, 2011 and October, 2014. Patients who received MMTS exhibited significantly less blood loss (20.3±11.3 vs. 32.3±12.6 ml, P<0.01), lower volume of postoperative drainage (42.77±15.2 vs. 50.48±23.2 ml, P<0.01) and higher cosmetic satisfaction (94.6±3.5 vs. 88.9±2.7%, P<0.01), but a longer operative time (102±36 vs. 50.48±23.2 min, P<0.01) when compared with MIVAT. In addition, a better peak angle of cervical rotation (38.6±4.1˚ vs. 35.3±3.8˚, P=0.25) and shorter length of hospitalization (4.25±1.08 vs. 4.51±1.30 days, P=0.52) was observed in the MMTS group, although the differences with the MIVAT group were not statistically significant. No complications were observed, apart from 2 cases of recurrent laryngeal nerve palsy and 1 case of transient hypocalcemia at the beginning of MIVAT. In conclusion, both MMST and MIVAT are safe and feasible methods of thyroidectomy; however, MMST is associated with less trauma and higher cosmetic satisfaction compared with MIVAT. Therefore, MMST may be used as a standard operative method and prospectively applicable for thyroidectomy, even for early‑stage malignancies.
View References
|
1
|
Pai SI and Tufano RP: Central compartment
neck dissection for thyroid cancer. Technical considerations. ORL J
Otorhinolaryngol Relat Spec. 70:292–297. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bärlehner E and Benhidjeb T: Cervical
scarless endoscopic thyroidectomy: Axillo-bilateral-breast approach
(ABBA). Surg Endosc. 22:154–157. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nakano S, Kijima Y, Owaki T, Shirao K,
Baba M and Aikou T: Anterior chest wall approach for video-assisted
thyroidectomy using a modifed neck skin lifting method. Biomed
Pharmacother. 56 (Suppl 1):96S–99S. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Timon C and Miller IS: Minimally invasive
video-assisted thyroidectomy: Indications and technique.
Laryngoscope. 116:1046–1049. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lombardi CP, Raffaelli M, Princi P, De
Crea C and Bellantone R: Video-assisted thyroidectomy: Report on
the experience of a single center in more than four hundred cases.
World J Surg. 30:794–801. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Miccoli B, Berti P, Bendinelli C, Conte M,
Fasolini F and Martino E: Minimally invasive video-assisted surgery
of the thyroid: A preliminary report. Lange becks Arch Surg.
385:261–264. 2000. View Article : Google Scholar
|
|
7
|
Yu JJ, Bao SL, Yu SL, Zhang DQ, Loo WT,
Chow LW, Su L, Cui Z, Chen K, Ma LQ, et al: Minimally invasive
video-assisted thyroidectomy for the early-stage differential
thyroid carcinoma. J Transl Med. 10 (Suppl 1):S132012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Elaraj DM and Clark OH: Changing
management in patients with papillary thyroid cancer. Curr Treat
Options Oncol. 8:305–313. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Miccoli P, Berti P, Raffaelli M, Materazzi
G, Baldacci S and Rossi G: Comparison between minimally invasive
video-assisted thyroidectomy and conventional thyroidectomy: A
prospective randomized study. Surgery. 130:1039–1043. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Thompson NW, Olsenn WR and Hoffman GL: The
continuing development of the technique of thyroidectomy. Surgery.
73:913–927. 1973.PubMed/NCBI
|
|
11
|
Pinchot S, Chen H and Sippel R: Incisions
and exposure of the neck for thyroidectomy and parathyroidectomy.
Operat Tech Gen Surg. 10:63–76. 2008. View Article : Google Scholar
|
|
12
|
Scott-Conner CE and Dawson DL: Operative
anatomy. 1st. JB Lippincott Company; Philadelphia, PA: pp.
388–1993
|
|
13
|
Xiao GZ and Gao L: A simple method for
determining an optimal incision for minimally invasive
video-assisted thyroidectomy. Surg Endosc. 22:2100–2101. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jancewicz S, Sidhu S, Jalaludin B and
Campbell P: Optimal position for a cervical collar incision: A
prospective study. ANZ J Surg. 72:15–17. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yu H, Yang YZ, Zhang DQ, Cui Z and Yu JJ:
Analysis of cervical dermatoglyph and related factors. Chin Arch
Gen Surg. 4:571–572. 2010.
|
|
16
|
Sabuncuoglu MZ, Sabuncuoglu A, Sozen I,
Benzin MF, Cakir T and Cetin R: Minimally invasive surgery using
mini anterior incision for thyroid diseases: A prospective cohort
study. Int J Clin Exp Med. 7:3404–3409. 2014.PubMed/NCBI
|