Introduction
Breast cancer is the most common malignant disease
among women in the Western world and Japan. However, advances in
the systemic treatment of breast cancer, particularly in
chemotherapy, have contributed to declines in the breast cancer
mortality rates (1).
Anthracycline-containing regimens are the most widely used in the
adjuvant and neoadjuvant settings for patients with breast cancer
(2). Several previous clinical
investigations have revealed that the use of neoadjuvant
chemotherapy for patients with locally advanced breast cancer
increased the surgical resectability rates and that the response to
therapy correlated with the patients' ultimate disease-free
survival (3–5). In addition, significant tumor volume
reduction following neoadjuvant chemotherapy may permit subsequent
breast-conserving surgical treatment (6,7) and a
unique advantage of neoadjuvant chemotherapy is the possibility to
take serial measurements of the primary tumor, therefore, allowing
in vivo assessment of factors predictive of the sensitivity
to the treatment (8).
Anthracyclines act via several mechanisms, however,
the interaction with the nuclear enzyme topoisomerase IIα appears
to be the most prominent mechanism (9). Topoisomerase IIα, which is a critical
nuclear DNA binding enzyme, functions by reducing DNA twisting and
supercoiling by cutting both strands of the DNA helix
simultaneously, allowing selected regions of the DNA to untangle
and to consequently engage in transcription, replication or repair
processes. Disruption of topoisomerase IIα has been demonstrated to
lead to double-stranded DNA breaks and cell death, and
topoisomerase IIα is, therefore, also a proliferation marker of
tumor cells, in addition to a target of anthracycline-based
chemotherapy (10).
However, previous studies have reported variable
expression levels of topoisomerase IIα and responses to
anthracycline-containing chemotherapy in breast cancer, and while
in vivo and in vitro studies each demonstrate that
there is indeed an association between the expression levels of
topoisomerase IIα and chemosensitivity to anthracyclines, these
results remain controversial (11–14).
Gene expression profiling has identified distinct
breast cancer molecular subtypes associated with different clinical
outcomes. Breast cancer is a molecularly heterogeneous disease,
which can be divided into ≥4 or 5 groups based on the expression
profiles, including luminal A and B, normal breast-like, human
epidermal growth factor receptor 2 (HER2)-positive, and basal-like
(predominantly triple negative) breast cancer (15,16).
Previous studies, including our previous study, revealed that
triple negative breast cancer is associated with an improved
pathological complete response rate compared with the other
subtypes (17–19).
In addition, several biomarkers and intrinsic
subtypes have been reported as predictors of the neoadjuvant
response (20,21). However, no basis for selecting the
optimal chemotherapy for individual patients has been determined,
and the association between the expression of topoisomerase IIα and
the different subtypes remains to be elucidated.
With this in mind, the present study aimed to
retrospectively analyze whether the protein expression levels of
topoisomerase IIα assisted in predicting the response to
anthracycline-containing neoadjuvant chemotherapy among each breast
cancer subtype and whether it is a prognostic marker of
survival.
Patients and methods
Patients
A prospective database of 147 Japanese women with
stage II or III breast cancer who received neoadjuvant chemotherapy
between May 1985 and January 2008 was analyzed. All patients
received standard anthracycline-containing neoadjuvant
chemotherapy. Adjuvant endocrine therapy for 5 years was prescribed
for patients with hormone receptor (HR) -positive tumors, whereas
adjuvant trastuzumab for 1 year was prescribed for patients with
HER2-amplified/overexpressed tumors from 2001 onwards. Systemic and
breast examinations were performed prior to neoadjuvant
chemotherapy, prior to surgery, and every 12 months postoperatively
using chest and abdominal computed tomography, mammograms, breast
ultrasonography and bone scans. The present study was approved by
the Ethics Committee of the Jikei University School of Medicine and
written informed consent was obtained from the patients.
Immunohistochemistry (IHC) and
defining breast cancer subtypes
IHC was performed, according to the standard
protocol using 3 µm sections of paraffin-embedded tissues and the
rabbit monoclonal antibody, anti-estrogen receptor (ER; SP1; Roche
Diagnostics, Ltd., West Sussex, UK), for ER staining, and the
rabbit monoclonal antibody, anti-progesterone receptor (PgR; 1E2;
Roche Diagnostics, Ltd.), for PgR staining. Nuclear staining of
≥10% was considered positive. Tumors with ER and/or PgR positive
expression were considered hormone receptor (HR)-positive. The
expression of HER2 was determined using IHC with a rabbit
polyclonal antibody (Dako, Glostrup, Denmark) on 4 µm sections of
paraffin-embedded tissue. A staining score of 3+,
according to the HercepTest criteria (22), was considered positive and a
2+ result was only considered positive if confirmed by
fluorescence in situ hybridization with an amplification
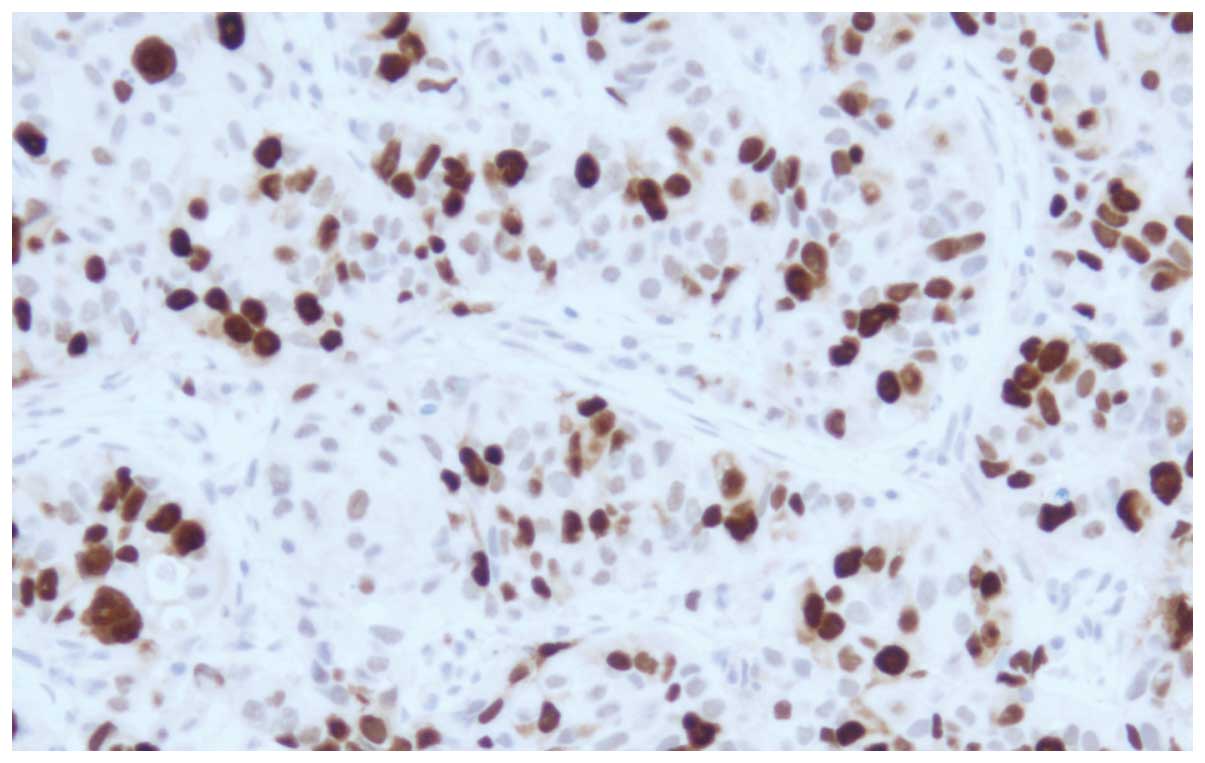
ratio of ≥2.0. The expression of topoisomerase IIα was determined
by IHC using a mouse monoclonal antibody (M7186; 1:100; Dako) on 3
µm sections of paraffin-embedded tissue. The topoisomerase IIα
staining was considered positive if nuclear staining ≥20% was
observed (Fig. 1).
Immunohistochemical proxies were used for subtyping and the tumors
were classified into three subtypes,
HR−/HER2−(triple-negative), any
HR/HER2+(HER2-positive) and
HR+/HER2−.
Statistics
The response to chemotherapy was assessed, according
to the Response Evaluation Criteria in Solid Tumors guidelines. The
overall survival was measured from the date of diagnosis to the
date of mortality, or the last follow-up. Disease-free survival was
measured from the date of operation until the date of recurrence or
the last follow-up. The association between each subtype and the
age of the patients was evaluated using the Kruskal-Wallis test.
The association between each subtype and the clinical factors,
response rate to neoadjuvant chemotherapy and topoisomerase IIα
expression in the patients, were evaluated using the Fisher's exact
test. Cumulative survival probabilities were calculated using the
Kaplan-Meier method, and differences between the survival rates
were tested using the log-rank test. Logistic regression analyses
were performed to evaluate the association between the expression
of topoisomerase IIα, and the response to chemotherapy and survival
among each breast cancer subtype. All statistical analyses were
performed using Stata® software (Version 13; StataCorp LP, College
Station, TX, USA). P<0.05 was considered to indicate a
statistically significant difference.
Results
Patients and tumor
characteristics
The performed chemotherapeutic regimens, which have
changed over time since the first cases were obtained in 1985, were
as follows: 6 cycles of doxorubicin (50 mg/m2),
5-fluorouracil (500 mg/m2) and cyclophosphamide (500
mg/m2) in 8 patients (5%); 6 cycles of alternate
administration of epirubicin (60 mg/m2), 5-fluorouracil
(500 mg/m2) and cyclophosphamide (500 mg/m2)
with docetaxel (75 mg/m2) in 6 patients (4%); 6 cycles
of concurrent administration of doxorubicin (50 mg/m2)
and docetaxel (60 mg/m2) in 41 patients (28%); 4 cycles
of epirubicin (100 mg/m2), 5-fluorouracil (500
mg/m2) and cyclophosphamide (500 mg/m2),
followed by 4 cycles of docetaxel (100 mg/m2) in 92
patients (63%). Therefore, all patients received an
anthracycline-based regimen and 139 patients (95%) also received
docetaxel. The regimens did not differ according to the subtype.
The median patient age was 51 years (range, 27–71 years). Table I lists the demographic, tumor
characteristics, and the results of the Fisher's exact and
Kruskal-Wallis tests among each subtype. The age of the patients
with HR/HER2+ tumors was significantly higher compared
with that of patients with HR−/HER2− (P=0.04)
and HR+/HER2− tumors (P=0.03), and the
menopausal status significantly differed between patients with any
HR/HER2+ and the other two subtypes (P=0.02). By
contrast, the tumor size and nodal status were similar among the
three subtypes (Table I).
 | Table I.Demographic and tumor
characteristics. |
Table I.
Demographic and tumor
characteristics.
| Characteristic | All patients
n=147 |
HR−/HER2− n=25 | Any
HR/HER2+ n=20 |
HR+/HER2− n=102 | P-value |
|---|
| Age (years) |
|
|
|
|
|
|
Median | 51.0 | 49.5a | 55.4 | 50.5b | 0.04a, 0.03b |
|
Range | 27–71 | 34–68 | 39–70 | 27–71 |
|
| Menopause, n
(%) |
|
|
|
|
|
|
Pre | 83 (57) | 13 (52) | 6
(30) | 64 (63) | 0.02 |
|
Post | 64 (43) | 12 (48) | 14 (70) | 38 (37) |
|
| Pretreatment tumor
size, n (%) |
|
|
|
|
|
| ≤5
cm | 90 (61) | 18 (72) | 13 (65) | 59 (58) | NS |
| >5
cm | 57 (39) | 7
(28) | 7
(35) | 43 (42) |
|
| Pretreatment lymph
node status, n (%) |
|
|
|
|
|
|
Negative | 84 (57) | 13 (52) | 9
(45) | 62 (61) | NS |
|
Positive | 63 (43) | 12 (48) | 11 (55) | 40 (39) |
|
Response rate to neoadjuvant
chemotherapy
The clinical and pathological response rates did not
differ among the regimes (data not shown). Table II lists the clinical and pathological
response rates to neoadjuvant chemotherapy. A total of 132 patients
(90%) showed an objective clinical response. The objective clinical
response rate revealed no difference among the subtypes. A total of
26 patients (18%) achieved a pathological complete response; 10
patients (40%) with HR−/HER2− tumors and 8
patients (40%) with any HR/HER2+ tumors achieved
favorable pathological complete response rates, and these rates
were significantly higher compared with the response rate of
patients with HR+/HER2− tumors (8%;
P<0.0001).
| Table II.Responses to chemotherapy according
to the breast cancer subtypes. |
Table II.
Responses to chemotherapy according
to the breast cancer subtypes.
| Response | All patients
n=147 |
HR−/HER2− n=25 | Any
HR/HER2+ n=20 |
HR+/HER2− n=102 | P-value |
|---|
| Clinical response,
n (%) |
|
|
|
|
|
|
Complete/partial response | 132 (90) | 22 (88) | 19 (95) | 91 (89) | NS |
| Stable
disease | 15 (10) | 3 (12) | 1 (5) | 11 (11) |
|
| Pathological
response, n (%) |
|
|
|
|
|
|
Complete response | 26 (18) | 10 (40) | 8 (40) | 8 (8) | <0.0001 |
|
Residual disease | 121 (82) | 15 (60) | 12 (60) | 94 (92) |
|
Expression levels of topoisomerase IIα
in the subtypes
Table III shows the
expression levels of topoisomerase IIα among the subtypes. It was
demonstrated that 88/147 tumors (60%), including 19/25 (76%)
HR−/HER2− tumors, 15/20 (75%) any
HR/HER2+ tumors and 54/102 (52%)
HR+/HER2− tumors, overexpressed topoisomerase
IIα. The frequency of topoisomerase IIα overexpression was
significantly higher in any HR/HER2+ and
HR−/HER2− tumors compared with in the
HR+/HER2− tumors (P=0.036).
| Table III.Expression of topoisomerase IIα
according to the breast cancer subtypes. |
Table III.
Expression of topoisomerase IIα
according to the breast cancer subtypes.
| Topoisomerase IIα
expression | Overall n=127 |
HR−/HER2− n=25 | Any
HR/HER2+ n=20 |
HR+/HER2− n=102 | P-value |
|---|
|
Positivea | 88 (60%) | 19 (76%) | 15 (75%) | 54 (52%) | 0.036 |
| Negative | 59 (40%) | 6
(24%) | 5
(25%) | 48 (47%) |
|
Correlation between the expression of
topoisomerase IIα and the response to neoadjuvant chemotherapy
among the subtypes
Table IV shows the
association between the expression of topoisomerase IIα and the
pathological complete response rates. It was demonstrated that
19/88 (22%) topoisomerase IIα-positive tumors and 7/59 (12%)
topoisomerase IIα-negative tumors achieved a pathological complete
response. Topoisomerase IIα-positive expression was associated with
a favorable response. Additionally, 8/19 (42%) topoisomerase
IIα-positive and 2/6 (33%) topoisomerase IIα-negative
HR−/HER2− tumors achieved a pathological
complete response. Furthermore, 6/15 (40%) topoisomerase
IIα-positive and 2/5 (40%) topoisomerase IIα-negative any
HR/HER2+ tumors, 5/54 (9%) topoisomerase IIα-positive
and 3/48 (6%) topoisomerase IIα-negative
HR+/HER2− tumors achieved a pathological
complete response. Topoisomerase IIα-positive expression was not
significantly associated with a favorable response among all
subtypes.
| Table IV.Association between the expression of
topoisomerase IIα and the pathological complete response rate. |
Table IV.
Association between the expression of
topoisomerase IIα and the pathological complete response rate.
|
| Pathological
complete response rate |
|---|
|
|
|
|---|
| Topoisomerase IIα
expression | Overall |
HR−/HER2− | Any
HR/HER2+ |
HR+/HER2− | P-value |
|---|
| Positive | 19/88 (22%) | 8/19 (42%) | 6/5 (40%) | 5/54 (9%) | 0.051 |
| Negative | 7/59 (12%) | 2/6 (33%) | 2/5 (40%) | 3/48 (6%) | 0.019 |
Association between the expression of
topoisomerase IIα and survival
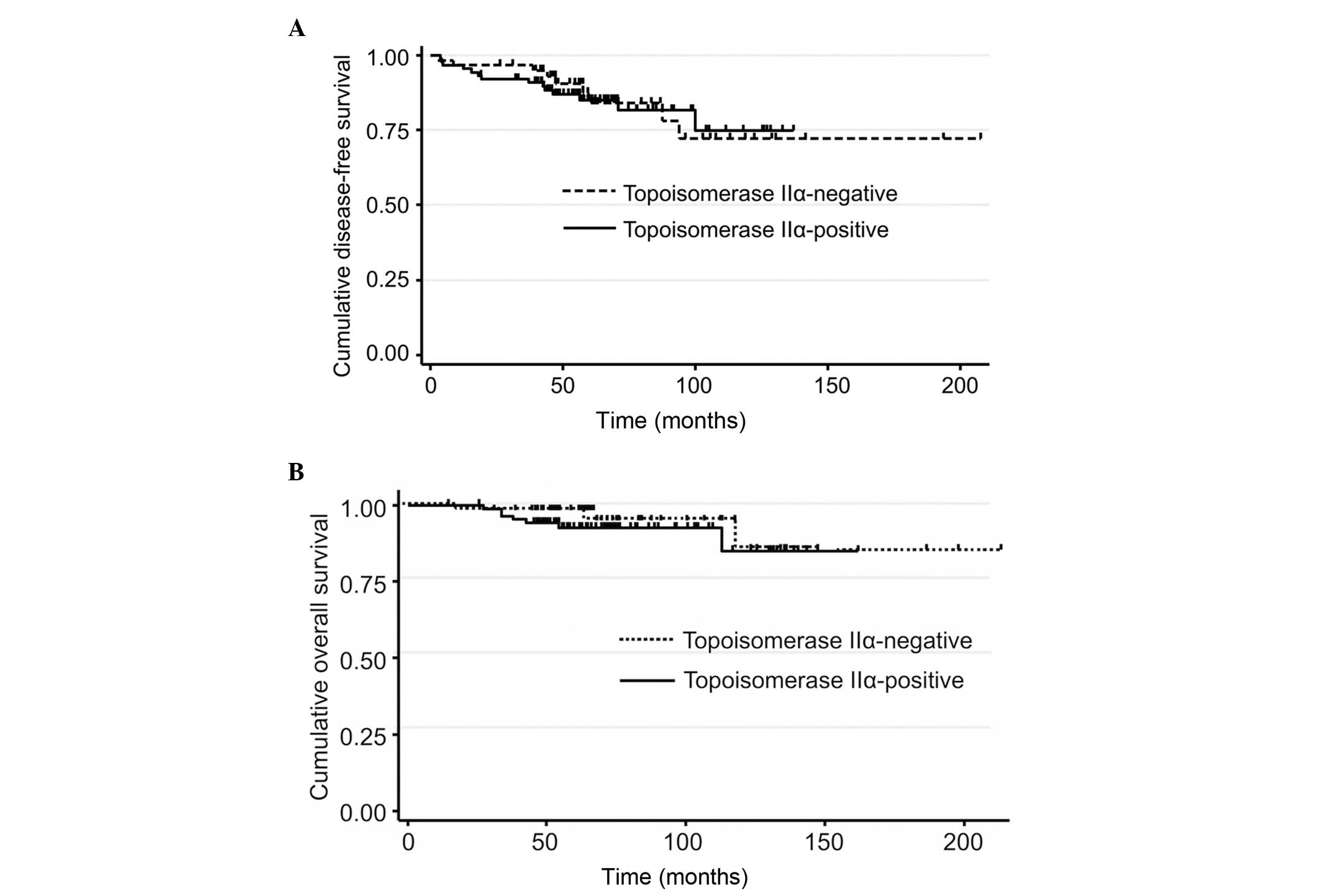
Fig. 2 shows the
association between the expression of topoisomerase IIα and
survival. It was revealed that 7/88 (8%) patients with
topoisomerase IIα-positive and 3/59 (5%) patients with
topoisomerase IIα-negative tumors succumbed to mortality, while
14/88 (16%) patients with topoisomerase IIα-positive and 9/59 (15%)
patients with topoisomerase IIα-negative tumors exhibited
recurrence. The expression of topoisomerase IIα was not associated
with the overall and disease-free survival.
Discussion
The present study used IHC to evaluate the
expression levels of topoisomerase IIα, HER2, ER and PgR in tumor
samples obtained from the pretreatment biopsies of breast cancer
patients receiving an anthracycline-containing regimen as
neoadjuvant chemotherapy. This retrospective data analysis
suggested that the favorable response to anthracycline-containing
neoadjuvant chemotherapy among the triple-negative and
HER2-positive subtypes was independent of the expression of
topoisomerase IIα.
Anthracyclines, including doxorubicin and
epirubicin, which is less cardiotoxic compared with doxorubicin,
are extensively used for the treatment of breast cancer, and
anthracycline-containing polychemotherapy regimens have reduced
breast cancer mortality by ~1/3 (1).
The cardiac toxicity of anthracyclines is well described and the
most common form, congestive heart failure, is known to be closely
associated with the cumulative dose. Although limiting the
cumulative dose to ~240–360 mg/m2 doxorubicin has
assisted in reducing the incidence of congestive heart failure to
~1.6–2.1%, data from long-term survivors of childhood cancer
indicate that there is no true threshold for
anthracycline-assoicated cardiotoxicity, and that cardiac damage
may become apparent years later. However, studies from adjuvant
breast cancer trials have shown that the likelihood of late cardiac
effects in women who receive adjuvant anthracycline is low
(2). However, since not all patients
benefit from anthracyclines, a means of selecting the appropriate
patients for the treatment is clearly of great interest.
Anthracyclines have three major mechanisms of action: i) Inhibition
of DNA and RNA synthesis by intercalating between the base pairs of
the DNA/RNA strand; ii) enhancement of catalysis of
oxidation-reduction reactions and iii) inhibition of topoisomerase
IIα (9). Notably, the first mechanism
also appears to be dependent on the inhibition of topoisomerase IIα
for cytotoxicity.
Topoisomerase IIα is the only enzyme able to cleave
and relegate double-stranded DNA. This enzyme acts during the
relaxation of DNA supercoils, which accumulate during gene
transcription and along with the progression of the replication
fork. In addition, only topoisomerase IIα can perform the
decatenation of replicated circular double-stranded DNA, and it is
obligatorily involved in the remodeling of chromatin during
mitosis. There are two highly homologous isoforms of topoisomerase
II in humans, which are encoded by different genes. The gene for
topoisomerase IIα is located on chromosome 17q21–22, while the gene
for topoisomerase IIβ is located on chromosome 3q24 (10,23).
Drugs that interfere with topoisomerase IIα include
anthracyclines (doxorubicin and epirubicin), etoposide, teniposide
and amsacrine. These agents act by binding covalently with
topoisomerase IIα following the occurrence of double-strand breaks,
inducing lethal cellular damage by inhibition of relegation. An
increase in the expression of topoisomerase IIα is associated with
the sensitivity to these agents as a result of the increased
substrate on which the drug may act.
Gene expression profiling has identified distinct
breast cancer molecular subtypes (15,16) and
previous studies have shown that triple-negative breast cancer is
associated with an improved pathological complete response rate
compared with the other subtypes (17–19).
Nevertheless, the predictive role of topoisomerase IIα in each
subtype remains to be elucidated. By contrast, HER2 amplification
and overexpression have been reported as predictive markers of the
benefit of anthracycline treatment in the adjuvant setting
(14). Because of its location in the
identical amplicon on chromosome 17, the gene encoding
topoisomerase IIα (TOP2A) is frequently co-amplified with that of
HER2 (24,25), which in turn leads to the
overexpression of its protein product and possibly, to a greater
sensitivity to anthracyclines (25–27). In
2011, Di Leo et al (14)
performed a meta-analysis, in which they identified that HER2
amplification and TOP2A amplification and deletion may have certain
value in the prediction of responsiveness to
anthracycline-containing chemotherapy. However, non-HER2 amplified
and non-TOP2A altered tumor types also appear to derive benefits
from treatment with anthracyclines. Furthermore, in their
meta-analysis, triple-negative breast cancer and moderately
hormone-sensitive tumor types appeared to exhibit and improved
response to anthracycline treatment compared with treatment with
the cyclophosphamide, methotrexate and fluorouracil regimen.
Therefore, a differential benefit from anthracyclines may exist
within these subtypes. Since all triple-negative tumors, and ~90%
of moderately hormone-sensitive tumors, from that previous study
revealed no TOP2A gene amplification, other mechanisms of increased
anthracycline sensitivity may exist. Du et al (13) suggested that topoisomerase IIα is a
predictive factor for breast cancer patients who received
anthracycline-containing neoadjuvant chemotherapy using
fluorescence in situ hybridization in another meta-analysis.
However, the authors could not detect an association between the
expression of topoisomerase IIα and sensitivity to
anthracycline-containing regimens using IHC, which is similar to
the results of the present study.
Notably, the target of anthracycline is the
topoisomerase IIα protein as opposed to the gene, and it is known
that there is a lack of correlation between gene status and protein
expression (28–30). Proliferation signals can lead to
overexpression of the topoisomerase IIα protein independently of
the TOP2 gene status (29,31). In normal cells, the expression of
topoisomerase IIα is regulated according to the cell cycle. In
proliferating cells, topoisomerase IIα becomes detectable in the
late G1 phase, and the quantity gradually increases, peaking in
G2/M. By contrast, increased expression of topoisomerase IIα is
commonly observed in malignant tumors, irrespective of the cell
cycle stage (10).
There are certain limitations to the present study.
Triple-negative, moderately hormone-sensitive and HER2-positive
tumors are characterized by high proliferation (15,32,33) and
this data further confirmed that topoisomerase IIα overexpression
was more frequently observed among the triple-negative and
HER2-positive subtypes. However, ideally, quantification of nuclear
concentrations of topoisomerase IIα protein may be a more
appropriate way to investigate its predictive value as opposed to
IHC alone. Furthermore, the present study included breast cancer
patients treated with anthracycline combinations, as well as other
drugs. Therefore, the use of these other drugs, including taxanes,
cyclophosphamide and fluorouracil, may have influenced the activity
of topoisomerase IIα and obscured any existing association.
In conclusion, the present findings do not justify
the routine use of immunohistochemical staining of topoisomeras IIα
as a predictive marker of the response to anthracycline-containing
regimens. Women with triple-negative and HER2-positive tumors
appear to derive benefits from anthracycline-containing
chemotherapy independently of the expression of topoisomerase
IIα.
Acknowledgements
The authors would like to thank Editage (www.editage.jp) for English language editing.
References
|
1
|
Peto R, Davies C, Godwin J, Gray R, Pan
HC, Clarke M, Cutter D, Darby S, McGale P, Taylor C, et al: Early
Breast Cancer Trialists' Collaborative Group (EBCTCG): Comparisons
between different polychemotherapy regimens for early breast
cancer: Meta-analyses of long-term outcome among 100,000 women in
123 randomised trials. Lancet. 379:432–444. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gianni L, Norton L, Wolmark N, Suter TM,
Bonadonna G and Hortobagyi GN: Role of anthracyclines in the
treatment of early breast cancer. J Clin Oncol. 27:4798–4808. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ellis P, Smith I, Ashley S, Walsh G, Ebbs
S, Baum M, Sacks N and McKinna J: Clinical prognostic and
predictive factors for primary chemotherapy in operable breast
cancer. J Clin Oncol. 16:107–114. 1998.PubMed/NCBI
|
|
4
|
Bonadonna G, Valagussa P, Brambilla C and
Ferrari L: Preoperative chemotherapy in operable breast cancer.
Lancet. 341:14851993. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fisher B, Bryant J, Wolmark N, Mamounas E,
Brown A, Fisher ER, Wickerham DL, Begovic M, DeCillis A, Robidoux
A, et al: Effect of preoperative chemotherapy on the outcome of
women with operable breast cancer. J Clin Oncol. 16:2672–2685.
1998.PubMed/NCBI
|
|
6
|
Smith IE, Walsh G, Jones A, Prendiville J,
Johnston S, Gusterson B, Ramage F, Robertshaw H, Sacks N, Ebbs S,
et al: High complete remission rates with primary neoadjuvant
infusional chemotherapy for large early breast cancer. J Clin
Oncol. 13:424–429. 1995.PubMed/NCBI
|
|
7
|
Kaufmann M, von Minckwitz G, Smith R,
Valero V, Gianni L, Eiermann W, Howell A, Costa SD, Beuzeboc P,
Untch M, et al: International expert panel on the use of primary
(preoperative) systemic treatment of operable breast cancer: Review
and recommendations. J Clin Oncol. 21:2600–2608. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Chang J, Powles TJ, Allred DC, Ashley SE,
Clark GM, Makris A, Assersohn L, Gregory RK, Osborne CK and Dowsett
M: Biologic markers as predictors of clinical outcome from systemic
therapy for primary operable breast cancer. J Clin Oncol.
17:3058–3063. 1999.PubMed/NCBI
|
|
9
|
Minotti G, Menna P, Salvatorelli E, Cairo
G and Gianni L: Anthracyclines: Molecular advances and
pharmacologic developments in antitumor activity and
cardiotoxicity. Pharmacol Rev. 56:185–229. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kellner U, Sehested M, Jensen PB, Gieseler
F and Rudolph P: Culprit and victim - DNA topoisomerase II. Lancet
Oncol. 3:235–243. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fry AM, Chresta CM, Davies SM, Walker MC,
Harris AL, Hartley JA, Masters JR and Hickson ID: Relationship
between topoisomerase II level and chemosensitivity in human tumor
cell lines. Cancer Res. 51:6592–6595. 1991.PubMed/NCBI
|
|
12
|
Di Leo A, Gancberg D, Larsimont D, Tanner
M, Jarvinen T, Rouas G, Dolci S, Leroy JY, Paesmans M, Isola J, et
al: HER-2 amplification and topoisomerase II alpha gene aberrations
as predictive markers in node-positive breast cancer patients
randomly treated either with an anthracycline-based therapy or with
cyclophosphamide, methotrexate, and 5-fluorouracil. Clin Cancer
Res. 8:1107–1116. 2002.PubMed/NCBI
|
|
13
|
Du Y, Zhou Q, Yin W, Zhou L, Di G, Shen Z,
Shao Z and Lu J: The role of topoisomerase IIα in predicting
sensitivity to anthracyclines in breast cancer patients: A
meta-analysis of published literatures. Breast Cancer Res Treat.
129:839–848. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Di Leo A, Desmedt C, Bartlett JM, Piette
F, Ejlertsen B, Pritchard KI, Larsimont D, Poole C, Isola J, Earl
H, et al: HER2/TOP2A Meta-analysis Study Group: HER2 and TOP2A as
predictive markers for anthracycline-containing chemotherapy
regimens as adjuvant treatment of breast cancer: A meta-analysis of
individual patient data. Lancet Oncol. 12:1134–1142. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Perou CM, Sørlie T, Eisen MB, van de Rijn
M, Jeffrey SS, Rees CA, Pollack JR, Ross DT, Johnsen H, Akslen LA,
et al: Molecular portraits of human breast tumours. Nature.
406:747–752. 2000. View
Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sørlie T, Perou CM, Tibshirani R, Aas T,
Geisler S, Johnsen H, Hastie T, Eisen MB, van de Rijn M, Jeffrey
SS, et al: Gene expression patterns of breast carcinomas
distinguish tumor subclasses with clinical implications. Proc Natl
Acad Sci USA. 98:10869–10874. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Carey LA, Dees EC, Sawyer L, Gatti L,
Moore DT, Collichio F, Ollila DW, Sartor CI, Graham ML and Perou
CM: The triple negative paradox: Primary tumor chemosensitivity of
breast cancer subtypes. Clin Cancer Res. 13:2329–2334. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Liedtke C, Mazouni C, Hess KR, André F,
Tordai A, Mejia JA, Symmans WF, Gonzalez-Angulo AM, Hennessy B,
Green M, et al: Response to neoadjuvant therapy and long-term
survival in patients with triple-negative breast cancer. J Clin
Oncol. 26:1275–1281. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Nogi H, Kobayashi T, Suzuki M, Tabei I,
Kawase K, Toriumi Y, Fukushima H and Uchida K: EGFR as paradoxical
predictor of chemosensitivity and outcome among triple-negative
breast cancer. Oncol Rep. 21:413–417. 2009.PubMed/NCBI
|
|
20
|
Sørlie T, Perou CM, Fan C, Geisler S, Aas
T, Nobel A, Anker G, Akslen LA, Botstein D, Børresen-Dale AL, et
al: Gene expression profiles do not consistently predict the
clinical treatment response in locally advanced breast cancer. Mol
Cancer Ther. 5:2914–2918. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Martin M, Romero A, Cheang MC, López
García-Asenjo JA, García-Saenz JA, Oliva B, Román JM, He X, Casado
A, de la Torre J, et al: Genomic predictors of response to
doxorubicin versus docetaxel in primary breast cancer. Breast
Cancer Res Treat. 128:127–136. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wolff AC, Hammond ME, Hicks DG, Dowsett M,
McShane LM, Allison KH, Allred DC, Bartlett JM, Bilous M, et al:
Recommendations for human epidermal growth factor receptor 2
testing in breast cancer: American Society of Clinical Oncology:
College of American Pathologists clinical practice guideline
update. J Clin Oncol. 31:3997–4013. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Berger JM, Gamblin SJ, Harrison SC and
Wang JC: Structure and mechanism of DNA topoisomerase II. Nature.
379:225–232. 1996. View
Article : Google Scholar : PubMed/NCBI
|
|
24
|
Smith K, Houlbrook S, Greenall M,
Carmichael J and Harris AL: Topoisomerase II alpha co-amplification
with erbB2 in human primary breast cancer and breast cancer cell
lines: Relationship to m-AMSA and mitoxantrone sensitivity.
Oncogene. 8:933–938. 1993.PubMed/NCBI
|
|
25
|
Järvinen TA, Tanner M, Rantanen V, Bärlund
M, Borg A, Grénman S and Isola J: Amplification and deletion of
topoisomerase IIalpha associate with ErbB-2 amplification and
affect sensitivity to topoisomerase II inhibitor doxorubicin in
breast cancer. Am J Pathol. 156:839–847. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Arriola E, Moreno A, Varela M, Serra JM,
Falo C, Benito E and Escobedo AP: Predictive value of HER-2 and
Topoisomerase II alpha in response to primary doxorubicin in breast
cancer. Eur J Cancer. 42:2954–2960. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Arriola E, Rodriguez-Pinilla SM, Lambros
MB, Jones RL, James M, Savage K, Smith IE, Dowsett M and Reis-Filho
JS: Topoisomerase II alpha amplification may predict benefit from
adjuvant anthracyclines in HER2 positive early breast cancer.
Breast Cancer Res Treat. 106:181–189. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Coon JS, Marcus E, Gupta-Burt S, Seelig S,
Jacobson K, Chen S, Renta V, Fronda G and Preisler HD:
Amplification and overexpression of topoisomerase IIalpha predict
response to anthracycline-based therapy in locally advanced breast
cancer. Clin Cancer Res. 8:1061–1067. 2002.PubMed/NCBI
|
|
29
|
Durbecq V, Desmed C, Paesmans M, Cardoso
F, Di Leo A, Mano M, Rouas G, Leroy JY, Sotiriou C, Piccart M, et
al: Correlation between topoisomerase-IIalpha gene amplification
and protein expression in HER-2 amplified breast cancer. Int J
Oncol. 25:1473–1479. 2004.PubMed/NCBI
|
|
30
|
Mueller RE, Parkes RK, Andrulis I and
O'Malley FP: Amplification of the TOP2A gene does not predict high
levels of topoisomerase II alpha protein in human breast tumor
samples. Genes Chromosomes Cancer. 39:288–297. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Campiglio M, Somenzi G, Olgiati C, Beretta
G, Balsari A, Zaffaroni N, Valagussa P and Ménard S: Role of
proliferation in HER2 status predicted response to doxorubicin. Int
J Cancer. 105:568–573. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Sotiriou C, Neo SY, McShane LM, Korn EL,
Long PM, Jazaeri A, Martiat P, Fox SB, Harris AL and Liu ET: Breast
cancer classification and prognosis based on gene expression
profiles from a population-based study. Proc Natl Acad Sci USA.
100:10393–10398. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Cheang MC, Chia SK, Voduc D, Gao D, Leung
S, Snider J, Watson M, Davies S, Bernard PS, Parker JS, et al: Ki67
index, HER2 status and prognosis of patients with luminal B breast
cancer. J Natl Cancer Inst. 101:736–750. 2009. View Article : Google Scholar : PubMed/NCBI
|