Introduction
Fibroepithelioma of Pinkus (FEP) is considered to be
an uncommon variant of basal cell carcinoma (BCC) (1), although it was recently described as a
trichoblastoma (2,3). Clinically, FEP appears as a solitary
non-pigmented or brownish to gray, well-outlined flat or polypoid
lesion, with peculiar dermoscopic and confocal aspects (4) and with a predilection for the lower
trunk (Fig. 1).
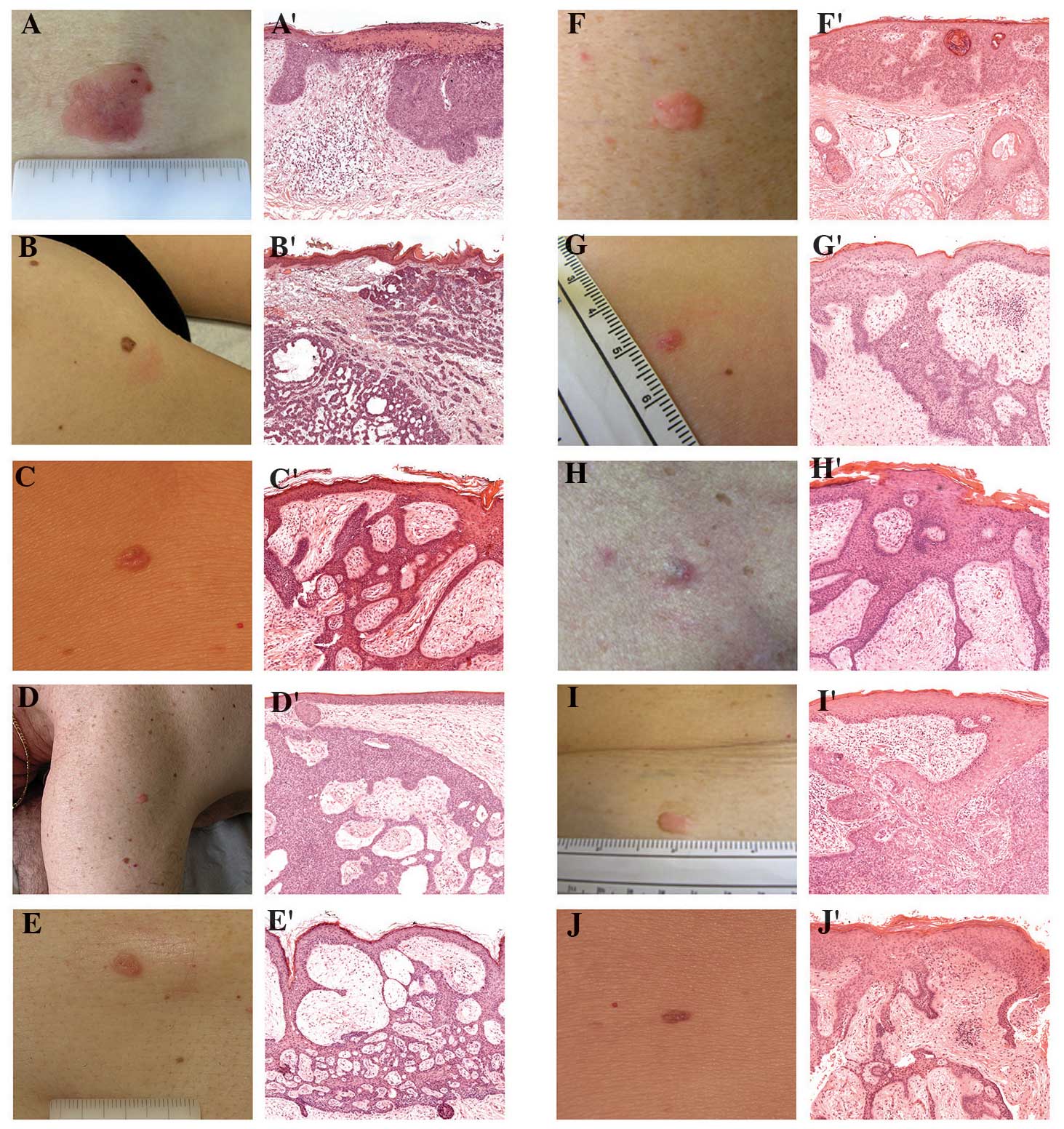 | Figure 1.(A-J) Clinical and histological images
of fibroepitheliomas of Pinkus (FEPs) collected in our Department.
Clinically, FEP appears as a solitary non-pigmented, flat or
polypoid lesion, most commonly localized on the trunk or the
extremities: (A) Male, aged 50 years, with FEP of the trunk; (B)
female, aged 36 years, with FEP of the trunk; (C) female, aged 32
years, with FEP of the left lower limb; (D) male, aged 63 years,
with FEP of the left shoulder; (E) female, aged 38 years, with a
FEP of the right lower limb; (F) male, aged 47 years, with a FEP of
the trunk; (G) female, aged 39 years, with FEP of the left lower
limb; (H) male, aged 59 years, with FEP of the trunk; (I) female,
aged 44 years, with FEP of the trunk; and (J) female, aged 34
years, with FEP of the trunk. (A′-J′) Histopathological images of
the respective lesions: FEP exhibits numerous long, thin, branching
and anastomosing cords of basaloid cells within a fibrotic stroma.
Hematoxylin and eosin staining; original magnification, ×5. |
Histopathologically, FEP is characterized by
numerous thin anastomosing cords of basaloid cells extending
downward from the epidermis into the dermis within a fibrotic
stroma (Fig. 1).
Unlike the common types of BCC, FEP exhibits an
overwhelming predilection for the trunk (particularly the lower
back) and the extremities, with only 5% of the tumors arising on
sun-damaged skin. The clinical differential diagnosis includes a
wide spectrum of lesions, such as skin tags or dermal nevi.
However, the diagnosis is easier when the clinical examination is
combined with dermoscopy and confocal microscopy (4,5).
Although FEP was originally described by Pinkus as a
variant of BCC, the nature of this tumor remains a subject of
debate.
The strong predilection for the lumbar region (not
sun-exposed area) and for the female gender differentiates FEP from
other BCC subtypes that usually arise on sun-exposed areas and/or
predominantly in men.
Furthermore, FEP exhibits a peculiar
histopathological architecture, as well as the presence of Merkel
cells, which are usually absent in BCCs but found in
trichoblastomas.
Thus far, FEP has been described as a solitary
lesion or in association with Paget's disease in a limited number
of case series. However, no studies have been performed to
investigate whether this lesion arises as an isolated rare tumor or
in patients harboring specific diseases.
The aim of our study was the characterization of a
consecutive series of FEPs to identify a possible association of
this tumor with concomitant diseases.
Patients and methods
Cases
All the histopathologically-proven cases of FEP
excised in a single referral center (Department of Dermatology,
University of Modena and Reggio Emilia, Modena, Italy) from 1995 to
2011 were retrospectively reviewed. Clinical data including gender,
location and age were recorded. Location was divided into head and
neck, trunk, back, genitalia, upper extremities and lower
extremities.
The data on excised tumors (skin tumors or visceral
malignancies) were retrieved from the database of the Department of
Pathology at the University of Modena and Reggio Emilia.
Moreover, the medical records of all the patients,
such as radiological examinations or surgical procedures, were
reviewed to obtain a complete picture of each patient's health
status. The present study was conducted in accordance with the
principles of the Declaration of Helsinki.
This study's protocol and the submitted manuscript
have been approved by the Institutional Review Board of the
Department of Surgery, School of Medicine, Dentistry and
Morphological Sciences, University of Modena and Reggio Emilia
(Modena, Italy).
Results
Association of FEP with cancer
A total of 49 cases of FEP were identified, mainly
located on the trunk (77.55%), followed by the lower extremities
(12.20%) and the head and neck (10.20%). The mean age of the
patients was 64.04 years and 31 of the patients were female (63%).
The tumors found in patients with FEP are listed in Table I. Of the 49 patients, 9 (18%) were
found to have gastrointestinal tumors, 4 patients (8%) had breast
carcinoma and 7 patients (14%) had other cancers. More
specifically, 6 patients had colonic adenocarcinoma and 3 patients
had neuroendocrine gastrointestinal tumors. Of the 49 patients, 1
(3%) was affected with mammary Paget's disease and 1 with perianal
extramammary Paget's dissease.
 | Table I.Non-skin tumors diagnosed in patients
with fibroepithelioma of Pinkus. |
Table I.
Non-skin tumors diagnosed in patients
with fibroepithelioma of Pinkus.
|
| Gender |
|
|---|
|
|
|
|
|---|
| Tumors | Male, n=18 (37%) | Female, n=31
(63%) | Total n=49
(100%) |
|---|
| Gastrointestinal
tumors | 5 (28) | 4 (13) | 9 (18) |
|
Upper | 1 (20) | 1 (25) | 2 (22) |
|
Lower | 4 (80) | 3 (75) | 7 (78) |
| Colonic
Adenocarcinoma | 3 (60) | 3 (75) | 6 (67) |
| Neuroendocrine
gastrointestinal tumor | 2 (40) | 1 (25) | 3 (33) |
| Extramammary perianal
Paget's disease | 0 (0) | 1 (3) | 1 (2) |
| Mammary Pagets
disease | 0 (0) | 1 (3) | 1 (2) |
| Breast carcinoma | 0 (0) | 4 (13) | 4 (8) |
| Other cancers | 4 (22) | 3 (10) | 7 (14) |
In all but 2 cases, FEP appeared 1–2 years prior to
the internal malignancies, whereas in these 2 cases the
malignancies occurred synchronously with FEP.
Discussion
FEP is a rare tumor that is considered to be a
variant of BCC, although its classification remains to be
clarified. Moreover, the specific skin location and gender
predilection differentiates this tumor from ‘classical’ BCC.
Furthermore, BCC and FEP share certain characteristics, such as the
expression of androgen receptor, which is minimal in
trichoblastomas (6). However, FEPs
and trichoblastomas display Merkel cells, which are usually absent
in BCC (7).
In the present study, we observed an association
between FEP and gastrointestinal tumors. FEP was previously
reported in the literature in association with Paget's disease
(7), breast cancer (8,9) and, as a
variant of BCC, Gorlin-Goltz syndrome (10). However, conclusive epidemiological and
biomolecular data on these clinical associations are currently
lacking (11,12).
Considering our data, we may hypothesize a
pathogenetic association between FEP and gastrointestinal
neuroendocrine tumors, due to the common embryogenic origin of
Merkel cells and neuroendocrine cells from the neural crest.
Similar to the well-known genodermatosis (13), a common aberration of genes implicated
in mesoectodermal differentiation may play a role in the
pathogenesis of FEPs and gastrointestinal adenocarcinomas. Mutation
in the tumor suppressor gene TP53 may predispose to the
development of FEP (14). Similar to
BCC, it has been hypothesized that mutations in the Patched 1 gene
(PTCH1), which is responsible for inhibitory signaling in
the Hedgehog pathway, may also lead to the development of FEP.
In our study, we did not investigate for
PTCH1 mutations or another possible genetic background,
although the association of FEP with gastrointestinal tumors
appears to be part of a more complex, although still not well
defined phenotype, rather than a coincidental finding.
Gastrointestinal tumors may be associated with
either Gorlin-Goltz syndrome or trichilemmal lesions (13). As regards the latter condition, Cowden
syndrome is characterized by the occurrence of several tumors,
including breast, endometrial, thyroid, kidney and colorectal
cancers, in association with dermatological manifestations such as
oral/skin papillomas and trichilemmomas, and with PTEN
mutations (13). Interestingly,
dermatological signs may occur prior to systemic symptoms (13). If we consider FEP as a trichoblastoma,
it appears more likely that this rare skin tumor should be
considered to be part of the cutaneous spectrum of Cowden syndrome
(in which hamartomas and colon carcinomas have been recently
described) (15), or as a tumor
associated with a new syndrome including gastrointestinal tumors.
Furthermore, our cases were characterized by early onset of FEP
followed by the development of gastrointestinal tumors. This
peculiar onset of dermatological diseases may be seen in the
context of genodermatosis (12).
Although a possible underlying common genetic
substrate between FEP and gastrointestinal tumors was not
identified, our study included a consecutive large series of FEPs
from a single academic institution, with a careful examination of
the patients' medical history. However, additional cases are
required to confirm this association and assess its predictive
value. It is recommended that FEP patients are clinically evaluated
and screened for gastrointestinal tumors. Our
clinico-epidemiological findings raise the question of whether FEP
is a single entity or part of a more complex and not yet defined
gastrointestinal syndrome.
Acknowledgements
All the authors made significant intellectual
contributions to this study and each author listed has read and
approved the submitted manuscript.
References
|
1
|
Pinkus H: Premalignant fibroepithelial
tumors of skin. AMA Arch Dermatol Syphilol. 67:598–615. 1953.
View Article : Google Scholar
|
|
2
|
Bowen AR and LeBoit PE: Fibroepithelioma
of Pinkus is a fenestrated trichoblastoma. Am J Dermatopathol.
27:149–154. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sellheyer K, Nelson P and Kutzner H:
Fibroepithelioma of Pinkus is a true basal cell carcinoma
developing in association with a newly identified tumour-specific
type of epidermal hyperplasia. Br J Dermatol. 166:88–97. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Longo C, Soyer HP, Pepe P, Casari A, Wurm
EM, Guitera P and Pellacani G: In vivo confocal microscopic pattern
of fibroepithelioma of Pinkus. Arch Dermatol. 148:5562012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zalaudek I, Ferrara G, Broganelli P,
Moscarella E, Mordente I, Giacomel J and Argenziano G: Dermoscopy
patterns of fibroepithelioma of Pinkus. Arch Dermatol.
142:1318–1322. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Katona TM, Ravis SM, Perkins SM, Moores WB
and Billings SD: Expression of androgen receptor by
fibroepithelioma of Pinkus: Evidence supporting classification as a
basal cell carcinoma variant? Am J Dermatopathol. 29:7–12. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Warner TF, Burgess H and Mohs FE:
Extramammary Paget's disease in fibroepithelioma of Pinkus. J Cutan
Pathol. 9:340–344. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bryant J: Fibroepithelioma of Pinkus
overlying breast cancer. Arch Dermatol. 121:3101985. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sandbank M and Baschan D: Multiple
trichoepitelioma and breast carcinoma. Simultaneous appearance of
epithelioma adenoides cysticum and infiltrating lobular carcinoma
of the breast. Arch Dermatol. 114:12301978. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gorlin RJ and Goltz RW: Multiple nevoid
basal-cell epithelioma, jaw cysts and bifid rib. A syndrome. N Engl
J Med. 262:908–912. 1960. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Prodinger PM, Sarbia M, Massmann J, Straka
C, Meyer G and Steinlein OK: Gorlin syndrome associated with small
bowel carcinoma and mesenchymal proliferation of the
gastrointestinal tract: Case report and review of literature. BMC
Cancer. 10:3602010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ponti G, Pellacani G, Seidenari S, Pollio
A, Muscatello U and Tomasi A: Cancer-associated genodermatoses:
Skin neoplasms as clues to hereditary tumor syndromes. Crit Rev
Oncol Hematol. 85:239–256. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Saldanha G, Fletcher A and Slater DN:
Basal cell carcinoma: A dermatopathological and molecular
biological update. Br J Dermatol. 148:195–202. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sidhu GS, Chandra P and Cassai ND: Merkel
cells, normal and neoplastic: An update. Ultrastruct Pathol.
29:287–294. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Stanich PP, Owens VL, Sweetser S,
Khambatta S, Smyrk TC, Richardson RL, Goetz MP and Patnaik MM:
Colonic polyposis and neoplasia in Cowden syndrome. Mayo Clin Proc.
86:489–492. 2011. View Article : Google Scholar : PubMed/NCBI
|














