Introduction
Double primary carcinoma refers to the simultaneous
occurrence of different primary histological malignancies in
different parts of the body and belongs to the category of multiple
primary cancers (1,2). The survival of patients with breast
cancer has greatly improved with earlier screening and improvement
of treatment. Accordingly, the incidence of the second or multiple
primary malignancies among breast cancer patients has been found to
increase. In clinical practice, the second or multiple primary
malignancies are very frequently indistinct from the metastases of
the first primary malignancy, leading to the misdiagnosis and
improper treatment for patients with double primary carcinoma. The
simultaneous occurrence of primary gastric cancer and breast cancer
is extremely rare.
Overexpression of HER2 is a frequent molecular
abnormality in primary breast cancer and primary gastric cancer. To
the best of our knowledge, no patient with HER2 positive-double
primary carcinoma in the gastrointestinal system and the breast has
been reported previously. The present study reported one patient
with double primary carcinoma of gastric and breast cancer.
Case report
A 46-year-old woman had complained of irregular acid
reflux without obvious causes since August 2010. This patient
received no treatment. On November 25th 2010, a Helicobacter pylori
test was performed and the result was positive. The patient was
then treated with metronidazole + clarithromycin + omeprazole,
however showed no significant improvement. The patient felt satiety
after meals and occasionally exhibited symptoms of vague epigastric
pain and hematemesis. On December 28th 2010, the patient underwent
esophagogastroduodenoscopy (EGD) examination in The Third
Affiliated Hospital of Xiangya Medical School (Guangdong, China).
The results indicated abnormal changes of the gastric antrum,
angular and mucous membranes, and stomach cancer was diagnosed
following pathological biopsies. Since January 2011, the patient
was treated with two courses of chemotherapy (regimens unknown) and
referred to Hunan Cancer Hospital (Hunan, China) for further
treatment. On February 18th 2011, the patient underwent a radical
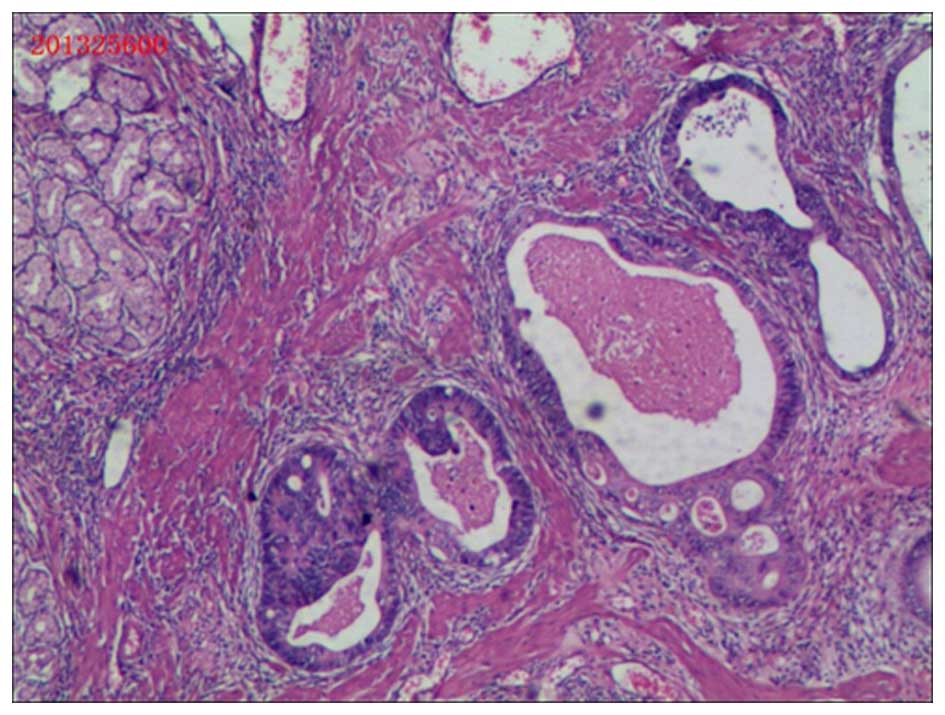
gastrectomy for gastric cancer. Postoperative pathological
examination revealed moderately-poorly differentiated
adenocarcinoma of the stomach which had invaded into the entire
thickness of the gastric wall where vascular tumor thrombi were
identified (Fig. 1). The involvement
of the lymph nodes for 2/2 in group 8a; 1/1 in group 9; 3/3 in
group 11p; 1/1 in group 7; 1/1 in group 11v; 1/1 in group 6; 4/4 in
lesser curvature group; 3/4 in greater curvature group, and fiber
fat tissues were identified in 12a, 12b, 13 and 15 group lymph
nodes. The carcinoma invaded into the capsule of the pancreas and
the carcinoma was not identified in duodenal stump, surgery margin
and greater omentum.
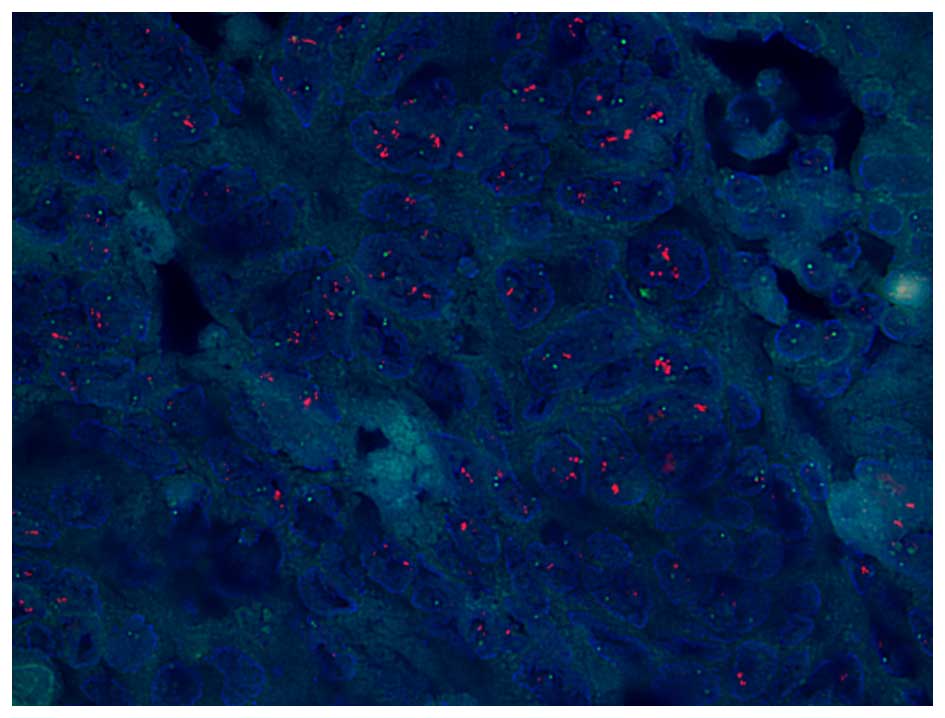
The fluorescent in situ hybridization (FISH)
assay of the HER2 gene in gastric cancer tissues is shown in
Fig. 2. HER2 fluorescent signals were
visualized as discrete punctuate staining dots. A total of 94 HER2
signals and 46 chemosensory protein (CSP)17 signals were detected
in a total of 30 cells. The ratio of HER2/CSP17 was 2.043, and the
final diagnosis was HER2 amplification and HER2 FISH-positive
gastric cancer. The patient received five treatments of the
postoperative chemotherapy regimen, docetaxel + Capecitabine +
cisplatin, and the last treatment was Oteracil + Oxaliplatin.
In August 2011, a lump was felt in the right breast
and the sonography revealed a hypoechoic mass (18×12 mm) at the 10
o'clock position and 77 mm from the right breast nipple, 5 mm deep
from the skin surface. The surrounding boundary was poorly defined
with uneven internal echo, Ultrasound BI-RADS grade was 4A. A
simple excision of the right breast mass was performed on September
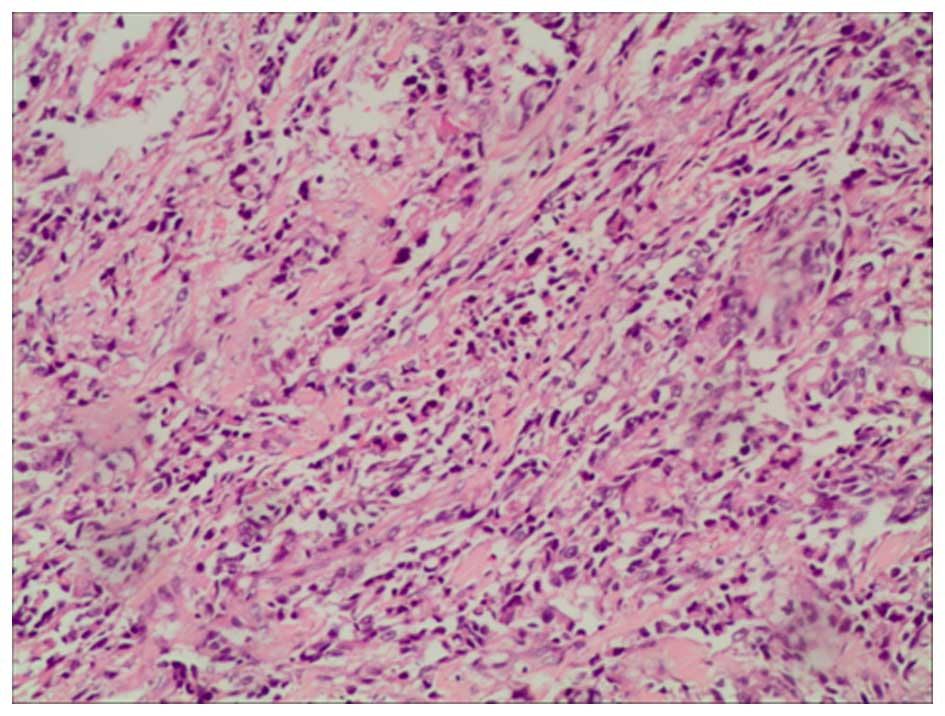
1st 2011. Postoperative pathological examination (5 and 11 o'clock
positions of the right breast) revealed an invasive ductal
carcinoma of the right breast (Grade II–III), tumor thrombi were
identified in the stromal vascular (5 o'clock position) and the
local skin was invaded (Fig. 3). The
tumor was estrogen receptor (−), progesterone receptor (−), CerbB-2
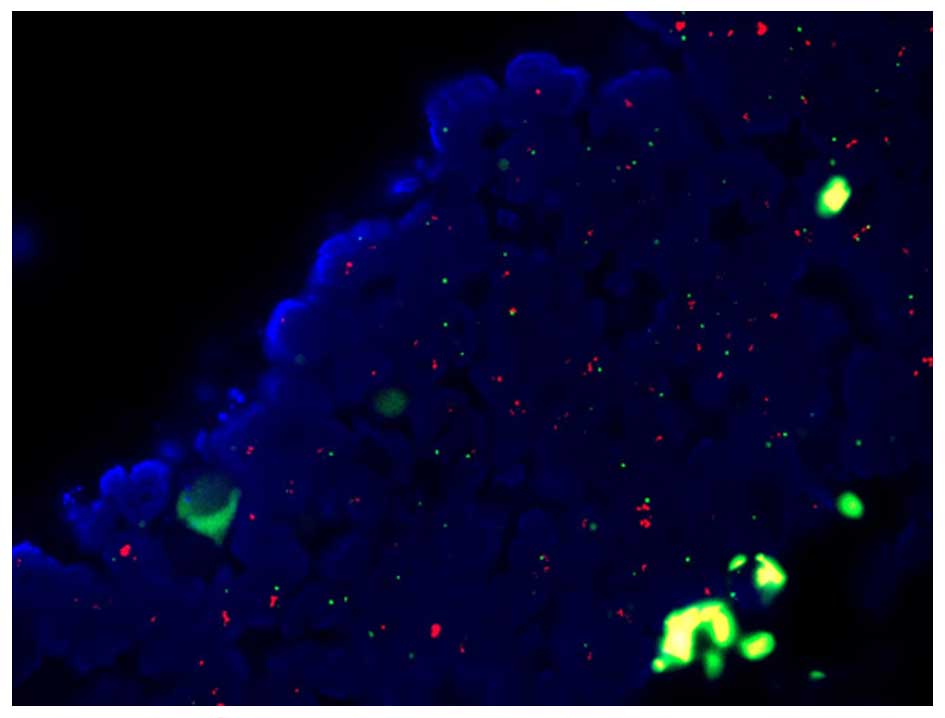
(++), Ki-67 labeling index rate of 70%. A HER2 FISH assay revealed
that fluorescent signals of the HER2 gene were visualized as
punctate staining (Fig. 4). The total
number of HER2 gene copies and CSP17 chromosome signals in the 30
counted cells was 163 and 72, respectively. The ratio of HER2/CSP17
was 2.28, and was indicated as HER2 amplification and FISH-positive
for the HER2 gene. Postoperative chemotherapy was administered for
one course (specific regimen unknown), followed by right chest wall
+ right axillary + right supraclavicular radiotherapy. In October
2011, the patient was admitted to Hunan Cancer Hospital (Hunan,
China) for the first dose of Trastuzumab (8 mg/kg IV) target
therapy, followed by two doses of Trastuzumab (6 mg/kg IV) cycled
every 21 days at the outpatient clinic. The patient failed to
adhere to the systemic treatment and did not respond to multiple of
telephone follow-ups. The patient succumbed to aggressive disease
progression in March 2012.
Discussion
Diagnostic criteria
Double primary cancers belong to the category of
multiple primary cancers, referring to tumors occurring
simultaneously in different parts of the same patient, or different
primary histological malignancies. Diagnosis of multiple primary
cancers is still accorded to the international standards developed
by Warren and Gates (1) in 1932: i)
Each malignant tumor must be histologically confirmed by pathology;
ii) each tumor must specifically have their own pathological
morphology; iii) tumor metastasis occurring from the different
sites or organs of the patient must be excluded. In 1979, Liu et
al (3) proposed that primary
cancer types may occur in different parts of the body, no
correlation exists with each other and each tumor has its unique
method of metastasis. The patient in the present study exhibited
two independent malignant tumors, each having unique
characteristics confirmed by histological and pathological
examination, consistent with the diagnosis of primary cancers.
Incidence
The incidence of multiple primary cancers reported
in national and international varied. The retrospective survey
results of 1,104,269 tumor patients from Demandante et al
(2) suggested that the incidence of
multiple primary cancers is between 0.73 and 11.7%, with higher
prevalence in the elderly. The incidence rate of double primary
cancers has increased in recent years, which may be associated with
the improvement of the technology used for diagnosis of the primary
cancer, the clinical application of anticancer medicines to prolong
survival period of patients with the initial primary cancer and
increased incidence of second primary cancer. The survey of 63
cases of multiple primary cancers from Irimie et al
(4) revealed that women and men
occupied 54 and 46%, respectively, and >90% patients were >40
years of age. The study also found that multiple primary malignant
tumors occur more frequently in the ovary-colon, ovary-breast,
breast-breast and other parts. Gastric cancer is one of the most
common malignant tumor types, which ranks as the third leading
cause of cancer-associated mortality in China, and breast cancer is
the first malignant neoplasm of females in China. Among these
tumors, HER2-positive gastric cancers range between 6 and 35%
(5), and HER2-positive breast cancers
range between 20 and 25% (6). In the
present report, poorly differentiated gastric carcinoma and
invasive breast carcinoma were confirmed respectively by
histopathological examinations, and each tumor was a primary
cancer. While gastric and breast cancer are very common cancer
types, which easily metastasize, the incidence rate of
gastric-breast primary cancer is extremely low. HER2-positive
expression simultaneously in primary breast and primary gastric
cancer has not been reported previously in national and
international literatures, and to the best of our knowledge, the
present study is the first report.
Etiology
Various causes of multiple primary cancers are known
and are predominantly associated with predisposition, environmental
factors and the host immune factors (7). By contrast, genetic defects are
important in causing multiple primary cancers, including Li-Fraumei
syndrome, since the abnormality of p53 gene leads to
loss-of-function of the tumor suppressor, which eventually leads to
the formation of multiple primary cancers in the digestive tract.
The same mutation can lead to different tumor types, for example
c-RNA virus can cause lymphomas, leukemia and liver cancer, H.
pylori infections can cause mucus-associated gastric cancer and
gastric lymphoma. Thirdly, patients with multiple primary cancers
tend to be susceptible and sensitive to carcinogenic factors. If
the carcinogenic factors are not ruled out, they may cause cancer
in other parts of the body. Other reasons, including the use of
chemical agents, endocrine factors and irregular application of
chemotherapy may also serve important roles in the development of
multiple primary cancers.
Diagnosis and prognosis
A diagnosis of multiple primary cancers may be
missed or easily be misdiagnosed (8).
Identification of recurrence or metastasis of the first primary
cancer from the second primary carcinoma is difficult. It was
reported that 50–70% of the second primary cancer occurs during 3
years after the first primary cancer has been diagnosed. This
duration was also the period of the first primary cancer to reoccur
and metastasize frequently.
Due to insufficient knowledge or vigilance,
clinicians easily misdiagnose the second primary cancer as
metastasized or resurrection of the first primary cancer, delaying
the treatment of the second primary cancer. Alerting metastasis of
the primary cancer and attention to the differentiation between
metastatic cancer and the second primary cancer are important
strategies for reducing misdiagnosis and missed diagnosis. The
effect of treatment for multiple primary cancers is better compared
with that of recurrence or metastatic primary cancer, and they are
more likely to be cured; therefore physicians must be highly
vigilant against the occurrence of multiple primary cancers to
improve the effect of the treatment.
HER2 expression in breast/gastric
cancer
In the present case, positive HER2 expression in
gastric and breast cancer specimens were detected by FISH. HER2 is
an important human epidermal growth factor receptor, and its
encoding gene is located at 17q12–21. HER2 protein belongs to a
transmembrane protein and its structure is similar to epidermal
growth factor receptor, the cytoplasmic domain has tyrosine kinase
activity. HER2 protein is normally inactive and only when binding
with specific ligands, the tyrosine kinase is activated, which is
predominantly caused by receptor dimerization and
autophosphorylation of its cytoplasmic domain. HER2 receptor
mediates multiple signal transduction pathways including the
RAS/RAF/MEK/ERK/RSK and PI3K/PIP2/PIP3/PDK1/AKT pathways.
HER2-regulated intracellular signal transduction pathways are
involved in the inhibition of apoptosis, the maintenance and
promotion of cancer cell growth, tumor angiogenesis, enhanced
migration and invasion of tumor cells and destruction of the body's
resistance barrier (9). Previous
studies have shown that overexpression of HER2 is associated with
breast, stomach, ovarian and prostate cancer. Breast cancer
patients with overexpression of HER2 have early recurrence, short
survival time and poor prognosis (10). HER2 is also as a therapeutic target
for breast cancer, and patients with breast cancer patients with
positive HER2 expression can clearly benefit from treatment using
HER2 monoclonal antibody (11). HER2
is important not only in breast cancer. Its role in the development
of gastric cancer is beginning to emerge. A previous study from Oya
et al (12) showed that
detection of HER2 protein levels can be used as a basis for
assessment of prognosis in patients with cancer. According to a
previous study on advanced gastric cancers with positive HER2
expression, treatment using the anti-HER2 monoclonal antibody can
extend the overall survival of patients to 16 months (13); however, certain studies reported no
correlation between HER2 status and prognosis of gastric cancer
(14,15). In 2012, a comprehensive review
analyzed the association between the overexpression of HER2 and the
prognosis of gastric cancer. Conclusions indicated that HER2
positive expression may be associated with a poor prognosis in
patients with gastric cancer (16).
Therefore, the expression of HER2 is now considered to be
associated with lower survival rate of gastric cancer. HER2 can
also be used as a therapeutic target in gastric cancer, currently
anti-HER2 therapy is the standard treatment for gastric cancer
patients with positive HER2.
In the present case, the patient was initially
diagnosed with stomach carcinoma. Following radical surgery,
postoperative pathological analysis revealed the full-thickness of
the gastric wall and lymph nodes were extensively invaded, and
vascular tumor thrombi were observed, implicating poor prognosis.
Postoperative chemotherapy was performed, but after half a year, a
lump was found in her right breast and a simple lump excision was
performed. Postoperative radiotherapy of supraclavicular lymph
nodes, chest wall and axillary cavity were executed. For this
patient, the expression of HER2 in primary gastric cancer and
primary breast cancer were positive, and diagnosed as simultaneous
HER2-positive double primary gastric and breast cancer, which met
the categories of the targeted therapy. The patient failed to
comply with doctor's prescription and the patient only completed
three cycles of Trastuzumab targeted therapy. The patient succumbed
to aggressive progression of the disease one year after radical
gastrectomy for gastric cancer and half a year after breast
lumpectomy.
Although this patient failed to finish target
therapy, standardized and regular treatment, including target
therapy, must be initiated as early as possible. In clinical
practice, for patients with HER2-positive breast cancer, physicians
must pay attention to whether lesions exist in the stomach. By
contrast, for HER2-positive gastric cancer, breast-associated
examinations must be performed in female patients, and if any
lesions are found, biopsy and HER2 testing are required in a timely
manner to avoid misdiagnosis and the delay of treatment.
Acknowledgements
The present study was supported by the Science and
Technology Program from Changsha City (Grant No. 23421).
References
|
1
|
Warren S: Multiple primary malignant
tumors. Am J cancer. 16:1358–1414. 1932.
|
|
2
|
Demandante CG, Troyer DA and Miles TP:
Multiple primary malignant neoplasms: Case report and a
comprehensive review of the literature. Am J Clin Oncol. 26:79–83.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Liu F: Double primary carcinomas of the
esophagus and stomach: a pathological study of 9 cases. Acta
Academiae Medicinae Sinicae. 1:67–70. 1979.PubMed/NCBI
|
|
4
|
Irimie A, Achimas-Cadariu P, Burz C and
Puscas E: Multiple primary malignancies-epidemiological analysis at
a single tertiary institution. J Gastrointestin Liver Dis.
19:69–73. 2010.PubMed/NCBI
|
|
5
|
Yonemura Y, Ninomiya I, Ohoyama S, Kimura
H, Yamaguchi A, Fushida S, Kosaka T, Miwa K, Miyazaki I and Endou
Y: Expression of c-erbB-2 oncoprotein in gastric carcinoma.
Immunoreactivity for c-erbB-2 protein is an independent indicator
of poor short-term prognosis in patients with gastric carcinoma.
Cancer. 67:2914–2918. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Engel RH and Kaklamani VG: HER2-positive
breast cancer: Current and future treatment strategies. Drugs.
67:1329–1341. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ray P, Sharifi R, Ortolano V and Guinan P:
Involvement of the genitourinary system in multiple primary
malignant neoplasms: A review. J Clin Oncol. 1:574–581.
1983.PubMed/NCBI
|
|
8
|
Babacan NA, Aksoy S, Cetin B, Ozdemir NY,
Benekli M, Uyeturk U, Ali Kaplan M, Kos T, Karaca H, Oksuzoglu B,
et al: Multiple primary malignant neoplasms: Multi-center results
from Turkey. J BUON. 17:770–775. 2012.PubMed/NCBI
|
|
9
|
Tai W, Mahato R and Cheng K: The role of
HER2 in cancer therapy and targeted drug delivery. J Control
Release. 146:264–275. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pils D, Pinter A, Rerbenwein J, Alfanz A,
Horak P, Schmid BC, Hefler L, Horvat R, Reinthaller A, Zeillinger R
and Krainer M: In ovarian cancer the prognostic influence of
HER2/neu is not dependent on the CXCR4/SDF-1 signalling pathway. Br
J Cancer. 96:485–491. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Scherbakov AM, Krasil'nikov MA and
Kushlinskii NE: Molecular mechanisms of hormone resistance of
breast cancer. Bull Exp Biol Med. 155:384–395. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Oya M, Yao T and Tsuneyoshi M: Expressions
of cell-cycle regulatory gene products in conventional gastric
adenomas: Possible immunohistochemical markers of malignant
transformation. Hum Pathol. 31:279–287. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Van Cutsem E, Kang Y, Chung H, Shen L,
Sawaki A, Lordick F, et al: Efficacy results from the ToGA trial: A
phase III study of trastuzumab added to standard chemotherapy in
first-line HER2-positive advanced gastric cancer. J Clin Oncol.
27:152009.
|
|
14
|
Kunz PL, Mojtahed A, Fisher GA, Ford JM,
Chang DT, Balise RR, Bangs CD, Cherry AM and Pai RK: HER2
expression in gastric and gastroesophageal junction adenocarcinoma
in a US population: Clinicopathologic analysis with proposed
approach to HER2 assessment. Appl Immunohistochem Mol Morphol.
20:13–24. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Moelans CB, Milne AN, Morsink FH,
Offerhaus GJ and Van Diest PJ: Low frequency of HER2 amplification
and overexpression in early onset gastric cancer. Cell Oncol
(Dordr). 34:89–95. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jørgensen JT and Hersom M: HER2 as a
prognostic marker in gastric cancer-a systematic analysis of data
from the literature. J Cancer. 3:137–144. 2012. View Article : Google Scholar : PubMed/NCBI
|