Introduction
For the past few years, the worldwide incidence of
gastric cancer (GC) has decreased (1); however, GC remains the second leading
cause of cancer-associated mortality worldwide (2). The incidence and mortality rate is
rising in Eastern Asia (1,2), particularly in China (3). The growth of GC incidences is
hypothesized to be caused by the interplay of environmental and
genetic factors, which varies between area, gender, age and
habitual behaviors (4–8). Specific variant alleles may modify the
effects of environmental exposures and the gene-environment
interactions may partly affect GC incidence (5). In the last decade, more and more
previous studies have focused on the association between
polymorphisms and GC, however, only a few revealed an association
with GC (4,7).
As an important metabolic enzyme, cytochrome P450
2E1 (CYP2E1) is critical in the metabolism of nitrosamines, benzene
and vinyl chloride in the human body (9–11).
Nitrosamine is considered as a pathogenic factor of GC (12); therefore, it is assumed that the
variant alleles in CYP2E1 may affect the incidence of GC (13).
RsaI/PstI and DraI
polymorphisms are regarded as the most frequent and powerful
polymorphisms in CYP2E1 (14).
RsaI/PstI polymorphisms, which are in complete
linkage disequilibrium in the 5′-flanking promoter region of
CYP2E1, are associated with higher transcription and increased
enzyme activity (15). The
DraI polymorphisms, however, are considered only to enhance
transcription (14). The variant
alleles in RsaI/PstI polymorphisms cause three
genotypes, termed wild-type homozygous (C1C1), heterozygous (C1C2)
and variant homozygous (C2C2) (15,16).
DraI polymorphisms are divided into wild-type homozygous
(DD), heterozygous (CD) and variant homozygous (CC) genotypes
(17).
Studies concerning the association of
RsaI/PstI polymorphisms and GC susceptibility have
been performed in numerous previous studies, however, the results
remain uncertain and controversial (18–45).
However, investigations regarding DraI polymorphisms have
rarely been performed. In the present study, 32 case-control
studies (18–45) of 4,953 cases and 6,626 controls were
screened from published papers between January 1995 and October
2014. These previous studies were used to calculate pooled
statistics by meta-analysis, aiming to clarify the relevance of
CYP2E1 polymorphisms and GC risk.
Materials and methods
Identification of previous
studies
Data screening was performed in PubMed (http://www.ncbi.nlm.nih.gov/pubmed) and China
National Knowledge Infrastructure database (http://oversea.cnki.net/kns55/default.aspx) between
January 1995 and October 2014, without language limitation. The key
words used for screening were ‘CYP2E1’, ‘Cytochrome P450 2E1’,
‘polymorphism’, ‘gastric’, ‘neoplasm’, ‘cancer’ and ‘variation’.
The titles and abstracts of each paper were browsed for preliminary
screening. The references of retrieved papers were also examined to
search for additional relevant studies.
Inclusion and exclusion criteria
The previous studies were selected using the
following inclusion criteria: i) Case-control studies; ii) studies
focusing on the relevance between CYP2E1 RsaI/PstI or
DraI polymorphisms and GC susceptibility; iii) studies where
detailed genotype frequencies were provided. Previous studies
lacking Hardy-Weinberg equilibrium (HWE) were excluded. The titles
and abstracts were reviewed for selection and the full-text papers
were intensively read to confirm eligibility. Two reviewers were
required to screen the studies independently, according to the
criteria, and a third was involved in discussing any disagreement
occurring between the previous two reviewers.
Data extraction
A form was designed to gather the following
information: First author, year, country, ethnicity, genotyping
method, source of control, numbers of different genotypes in
cases/controls and HWE. The authors of the previous studies were
contacted to confirm dubious information.
Statistical analysis
The meta-analysis focused on the associations
between the CYP2E1 polymorphisms (RsaI/PstI and
DraI) and GC susceptibility. The pooled odds ratios (ORs)
were used to explain the correlation. In the previous studies of
RsaI/PstI polymorphisms, ORs and their 95% confidence
intervals (CIs) were calculated for the dominant model (C1C2 + C2C2
vs. C1C1) and allele frequency C2, vs. C1. An OR and 95% CI <1
indicated a significant difference between the cases and controls.
In the subgroup analysis, the previous studies were grouped
according to ethnicity, source of control, smoking and drinking
status, and histology type. The ORs and 95% CIs of each group were
also calculated to assess the influence of these factors on the
association. In the previous studies of DraI polymorphisms,
the ORs and 95% CIs were estimated for the dominant model (CD + CC
vs. DD) and allele frequency (C vs. D).
In the meta-analysis, the I2 value was
used to confirm heterogeneity (46),
with values <25, 25–50 and >50% indicating low, moderate and
high heterogeneity, respectively. A χ2-based Q test was
also used for the heterogeneity test (Ph), together with
the random-effect model, in order to obtain a relatively
conservative outcome (47). The
significance of the pooled ORs and their 95% CIs were determined
using the Z test. A Pearson's χ2 test was used for
assessing the HWE.
In order to elucidate the influence of each previous
study included, influence analysis was performed by excluding each
study in turn and analyzing the homogeneity and effect size for the
remaining studies. Publication bias was assessed using Begg and
Mazumdar's adjusted rank correlation test (48) and the Egger regression asymmetry test
(49). Funnel plots were also used to
illustrate the publication bias (50). All statistical calculations were
performed using STATA 12.0 software (StataCorp LP, College Station,
TX, USA).
Results
Searching results and characteristics
of the previous studies included in the meta-analysis
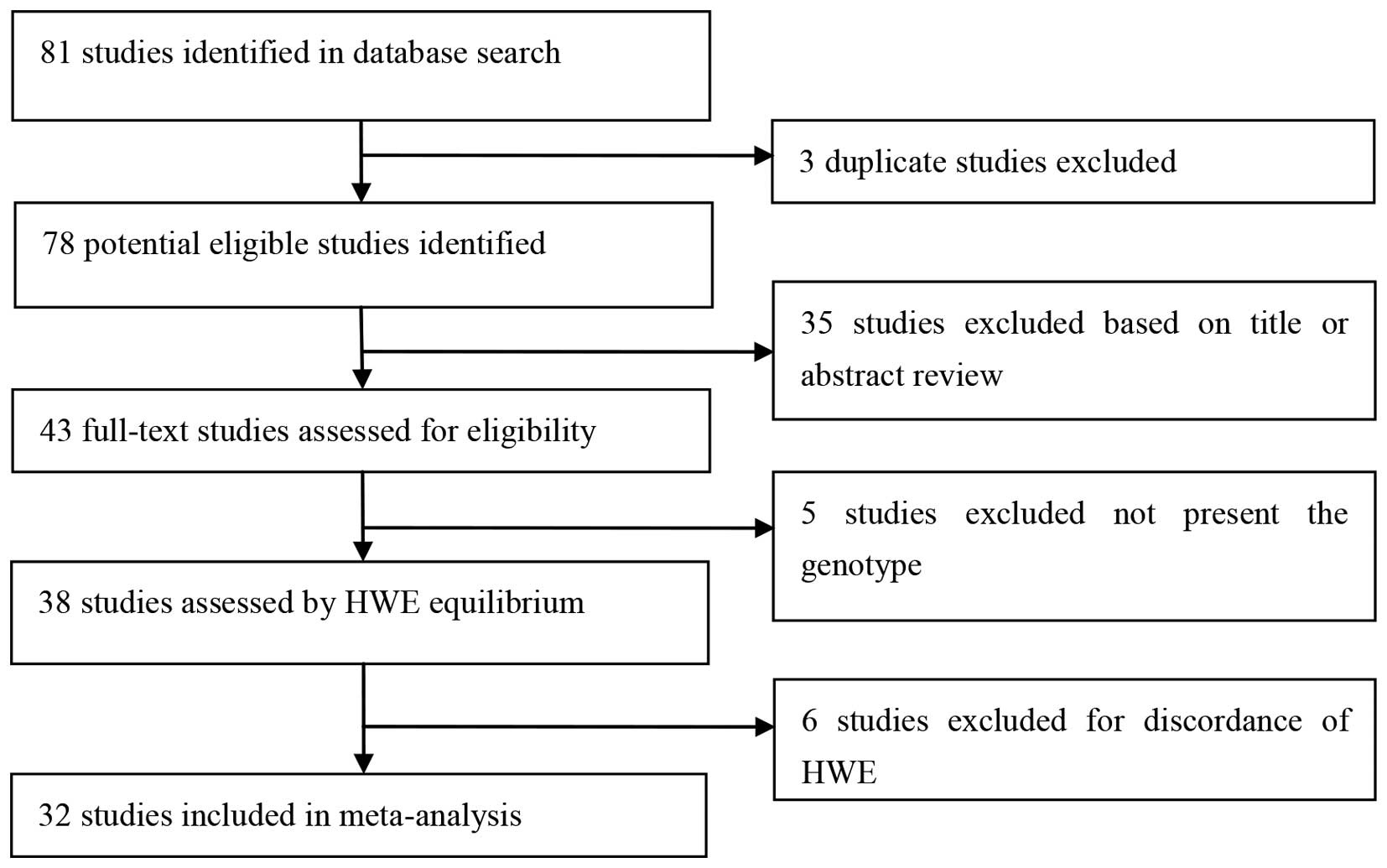
The flow diagram of the study selection process is
shown in Fig. 1. A total of 81
previous studies were identified in the database search, among
which three studies were duplicated. A further 35 previous studies
were excluded as a result of inconformity of case-control studies
or irrelevance with the RsaI/PstI and DraI
polymorphisms. The remaining 43 previous studies were read in full,
among which five studies without detailed genotype frequencies were
excluded. Following the exclusion of six previous studies for
discordance of HWE, 32 previous studies were included in the
meta-analysis (18–45). Of these, 26 were associated with
RsaI/PstI polymorphisms, while the remaining six
(20,24,27,33,35,43)
were investigating DraI polymorphisms. Details of these
previous studies are shown in Table
I.
 | Table I.Characteristics of previous studies
in the meta-analysis. |
Table I.
Characteristics of previous studies
in the meta-analysis.
|
|
|
|
|
| Cases | Control |
|
|
|---|
|
|
|
|
|
|
|
|
|
|
|---|
| Authors (year) | Country | Ethnicity | Genotyping
method | Source | C1C1 | C1C2 | C2C2 | C1C1 | C1C2 | C2C2 | HWE | Refs. |
|---|
|
RasI/PstI |
|
| Ghoshal
(2014) | India | Asian | PCR-RFLP | PB | 40 | 45 | 3 | 103 | 58 | 9 | Y | (25) |
| Yan
(2013) | China | Asian | PCR-RFLP | HB | 77 | 39 | 4 | 79 | 36 | 5 | Y | (42) |
| Feng
(2012) | China | Asian | PCR-RFLP | HB | 348 | 128 | 34 | 374 | 119 | 17 | Y | (27) |
| Malik
et al (2009) | India | Asian | PCR-RFLP | HB | 88 | 20 | 0 | 177 | 17 | 1 | Y | (32) |
| Agudo
et al (2006) | Britain | Caucasian | PCR-RFLP | PB | 226 | 13 | 0 | 880 | 39 | 1 | Y | (18) |
| Colombo
et al (2004) | Brazil | Mixed | PCR-RFLP | HB | 89 | 11 | 0 | 134 | 16 | 0 | Y | (23) |
| Zhou
et al (2003) | China | Asian | PCR-RFLP | PB | 85 | 45 | 15 | 140 | 75 | 14 | Y | (45) |
| Park
et al (2003) | Korea | Asian | PCR-RFLP | PB | 80 | 33 | 7 | 94 | 48 | 3 | Y | (35) |
| Wu
et al (2002) | China | Asian | PCR-RFLP | HB | 215 | 108 | 33 | 199 | 70 | 9 | Y | (33) |
| Tsukino
et al (2002) | Japan | Asian | PCR-RFLP | HB | 71 | 42 | 7 | 88 | 58 | 12 | Y | (37) |
| Cai
et al (2001) | China | Asian | PCR-RFLP | HB | 58 | 27 | 6 | 71 | 22 | 1 | Y | (21) |
| Qian
et al (2001) | China | Asian | PCR-RFLP | PB | 88 | 47 | 7 | 88 | 68 | 8 | Y | (39) |
| Kato
et al (1995) | Japan | Asian | PCR-RFLP | HB | 90 | 54 | 6 | 120 | 69 | 14 | Y | (28) |
|
González et al
(2004) | Costa Rica | Asian | PCR-RFLP | HB | 20 | 11 | 0 | 31 | 15 | 5 | Y | (19) |
| Boccia
et al (2007) | Italy | Caucasian | PCR-RFLP | HB | 102 | 5 | – | 234 | 20 | – | Y | (20) |
| Gao
et al (2002) | China | Asian | PCR-RFLP | PB | 58 | 31 | 9 | 121 | 62 | 13 | Y | (22) |
| Nan
et al (2005) | Korea | Asian | PCR-RFLP | HB | 69 | 39 | – | 129 | 88 | – | Y | (26) |
| Kato
et al (2011) | Japan | Asian | PCR-RFLP | HB | 280 | 186 | – | 340 | 213 | – | Y | (30) |
| Kato
et al (1996) | Japan | Asian | PCR-RFLP | HB | 55 | 29 | – | 87 | 61 | – | Y | (29) |
| Malakar
et al (2014) | India | Asian | PCR-RFLP | PB | 93 | 11 | 1 | 182 | 28 | 0 | Y | (31) |
|
Nishimoto et al
(2000) | Japan | Asian | PCR-RFLP | HB | 31 | 27 | 1 | 69 | 58 | 6 | Y | (34) |
| Suzuki
et al (2004) | Japan | Asian | PCR-RFLP | HB | 107 | 38 | – | 112 | 65 | – | Y | (36) |
| Li and
Xu (2007) | China | Asian | PCR-RFLP | HB | 25 | 10 | 6 | 17 | 16 | 8 | Y | (38) |
| Qian
et al (2003) | China | Asian | PCR-RFLP | PB | 64 | 22 | 4 | 47 | 39 | 4 | Y | (40) |
| Wang
et al (2005) | China | Asian | PCR-RFLP | HB | 33 | 14 | 1 | 22 | 23 | 3 | Y | (41) |
| Ye
(2002) | China | Asian | PCR-RFLP | HB | 39 | 13 | 4 | 26 | 24 | 6 | Y | (44) |
| DraI |
|
| Yan
(2013) | China | Asian | PCR-RFLP | HB | 70 | 42 | 8 | 70 | 46 | 4 | Y | (42) |
| Feng
et al (2012) | China | Asian | PCR-RFLP | HB | 334 | 131 | 45 | 318 | 160 | 32 | Y | (27) |
| Wu
et al (2002) | China | Asian | PCR-RFLP | HB | 195 | 120 | 41 | 158 | 100 | 20 | Y | (33) |
| Park
et al (2003) | Korea | Asian | PCR-RFLP | PB | 78 | 35 | 7 | 85 | 45 | 8 | Y | (35) |
| Boccia
et al (2007) | Italy | Caucasian | PCR-RFLP | HB | 92 | 15 | – | 227 | 27 | – | Y | (20) |
| Darazy
et al (2011) | Lebanon | Asian | PCR-RFLP | PB | 12 | 1 | 0 | 66 | 4 | 0 | Y | (24) |
These previous studies were subgrouped according to
ethnicity, source of control, smoking and drinking status, and
histology type. Stratified analysis was performed in these
subgroups. Previous studies concerning the interactions between
RsaI/PstI and glutathione S-transferase-µ-1 (GSTM1)
(36), glutathione S-transferase θ-1
(GSTT1) (40) or DraI
(27,35) were listed and analyzed in order to
identify more factors, which may influence the risk of GC (Table II).
| Table II.Distribution of CYP2E1
RsaI/PstI and influential factors. |
Table II.
Distribution of CYP2E1
RsaI/PstI and influential factors.
|
| No.
(cases/controls) of CYP2E1 Rsal/Pstl
polymorphism |
|
|---|
|
|
|
|
|---|
|
| C1C1 | C1C2 + C2C2 |
|
|---|
|
|
|
|
|
|---|
| Influential factors
(Exposure + vs. exposure -) | Exposure + | Exposure − | Exposure + | Exposure − | Refs. |
|---|
| Smoking (ever vs.
never) |
|
| Cai
et al (2001) | 37/23 | 21/48 | 23/11 | 10/12 | (21) |
| Agudo
et al (2006) | 151/503 | 79/403 | 9/18 | 4/22 | (18) |
| Boccia
et al (2007) | 49/99 | 53/135 | 1/9 | 4/11 | (20) |
| Gao
et al (2002) | 41/75 | 17/44 | 32/25 | 8/37 | (22) |
| Malakar
et al (2014) | 73/105 | 20/77 | 20/11 | 8/1 | (31) |
| Zhou
et al (2003) | 66/83 | 19/54 | 47/42 | 12/45 | (45) |
| Drinking (ever vs.
never) |
|
| Zhou
et al (2003) | 33/33 | 49/107 | 23/22 | 36/66 | (45) |
| Suzuki
et al (2004) | 48/32 | 51/51 | 17/13 | 20/34 | (36) |
| Malakar
et al (2014) | 43/73 | 51/109 | 4/16 | 8/12 | (31) |
| Gao
et al (2002) | 9/13 | 49/108 | 5/9 | 35/66 | (22) |
| Cai
et al (2001) | 32/20 | 25/51 | 19/8 | 14/15 | (21) |
| Boccia
et al (2007) | 68/123 | 32/111 | 5/10 | 0/10 | (20) |
| Histology type
(intestinal vs. diffuse) |
|
| Ghoshal
et al (2014) | 27/103 | 8/103 | 23/67 | 20/67 | (25) |
| Kato
et al (1996) | 27/87 | 28/87 | 17/61 | 12/61 | (29) |
| Wu
et al (2002) | 98/199 | 99/199 | 49/79 | 46/79 | (33) |
|
Nishimoto et al
(2000) | 17/69 | 8/69 | 6/64 | 3/19 | (34) |
| Suzuki
et al (2004) | 52/112 | 55/112 | 15/65 | 23/65 | (36) |
| GSTM1 (present vs.
null) |
|
| Suzuki
et al (2004) | 67/22 | 45/30 | 26/5 | 39/10 | (36) |
| GSTT1 (present vs.
null) |
|
| Zhou
et al (2003) | 22/30 | 42/17 | 14/21 | 12/22 | (45) |
| CYP2E1 DraI
(DD vs. CD + CC) |
|
| Park
et al (2003) | 71/79 | 9/13 | 7/6 | 33/40 | (35) |
| Feng
et al (2012) | 212/233 | 136/141 | 122/85 | 40/51 | (27) |
Meta-analysis results
In the overall analysis of RsaI/PstI
polymorphisms, the ORs and 95% CIs were 0.96 (0.82 and 1.12) in the
dominant model (C1C2 + C2C2 vs. C1C1) and 1.02 (0.86 and 1.19) in
gene frequency (C2 vs. C1; Table
III).
| Table III.Stratified analyses of polymorphisms
in the CYP2E1 gene with gastric cancer risk. |
Table III.
Stratified analyses of polymorphisms
in the CYP2E1 gene with gastric cancer risk.
|
|
| C2 vs. C1 | C1C2/C2C2 vs.
C1C1 |
|---|
|
|
|
|
|
|---|
|
Rsal/Pstl | No.
(cases/controls) | OR (95% CI) | P-value | Ph | I2
(%) | OR (95% CI) | P-value | Ph | I2
(%) |
|---|
| Overall | 3,727/5,510 | 1.02 (0.86,
1.19) | 0.850 | <0.001 | 61.4 | 0.96 (0.82,
1.12) | 0.574 | <0.001 | 56.2 |
| Source of
controls |
|
|
|
|
|
|
|
|
|
| PB | 1,027/2,124 | 1.02 (0.84,
1.25) | 0.811 | 0.147 | 35.3 | 0.96 (0.73,
1.28) | 0.828 | 0.032 | 54.4 |
| HB | 2,700/3,386 | 1.00 (0.79,
1.27) | 0.993 | <0.001 | 70.2 | 0.94 (0.78,
1.15) | 0.583 | 0.001 | 59.0 |
| Ethnicities |
|
|
|
|
|
|
|
|
|
|
Asian | 3,281/4,186 | 1.01 (0.85,
1.20) | 0.954 | <0.001 | 65.1 | 0.95 (0.81,
1.12) | 0.562 | <0.001 | 60.3 |
|
Caucasian | 346/1,174 | 1.23 (0.65,
2.31) | 0.526 | – | – | 0.94 (0.44,
2.00) | 0.872 | 0.192 | 41.1 |
|
Mixed | 100/150 | 1.03 (0.47,
2.27) | 0.936 | – | – | 1.04 (0.46,
2.33) | 0.934 | – | – |
| Smoking status |
|
|
|
|
|
|
|
|
|
| Ever
smoking | 549/1,014 | – | – | – | – | 1.56 (1.14,
2.15) | 0.006 | 0.376 | 6.3 |
| Never
smoking | 255/889 | – | – | – | – | 1.23 (0.59,
2.60) | 0.571 | 0.018 | 63.3 |
| Drinking
status |
|
|
|
|
|
|
|
|
|
| Ever
drinking | 305/372 | – | – | – | – | 0.91 (0.61,
1.37) | 0.676 | 0.752 | 0.0 |
| Never
drinking | 371/740 | – | – | – | – | 1.08 (0.75,
1.54) | 0.663 | 0.238 | 26.2 |
| Histology type |
|
|
|
|
|
|
|
|
|
|
Intestinal | 331/906 | – | – | – | – | 0.84 (0.54,
1.32) | 0.456 | 0.045 | 58.9 |
|
Diffuse | 315/906 | – | – | – | – | 1.05 (0.71,
1.58) | 0.798 | 0.131 | 43.6 |
| GSTM1 status |
|
|
|
|
|
|
|
|
|
|
Present | 93/27 | – | – | – | – | 1.71 (0.59,
4.99) | 0.328 | – | – |
|
Null | 84/40 | – | – | – | – | 2.60 (1.13,
5.99) | 0.025 | – | – |
| GSTT1 status |
|
|
|
|
|
|
|
|
|
|
Present | 36/51 | – | – | – | – | 0.91 (0.38,
2.17) | 0.830 | – | – |
|
Null | 54/39 | – | – | – | – | 0.22 (0.09,
0.54) | 0.001 | – | – |
| DraI
status |
|
|
|
|
|
|
|
|
|
| DD | 412/403 | – | – | – | – | 1.55 (1.13,
2.14) | 0.007 | 0.747 | 0.0 |
| CD +
CC | 218/165 | – | – | – | – | 0.88 (0.57,
1.34) | 0.544 | 0.487 | 0.0 |
|
|
|
| C vs. D | CD+CC vs. DD |
|
|
|
|
|
| DraI | No.
(cases/controls) | OR (95% CI) | P-value | Ph | I2
(%) | OR (95% CI) | P-value | Ph | I2
(%) |
|
|
Overall | 1,226/1,116 | 1.05 (0.91,
1.20) | 0.540 | 0.784 | 0.0 | 0.97 (0.82,
1.15) | 0.727 | 0.782 | 0.0 |
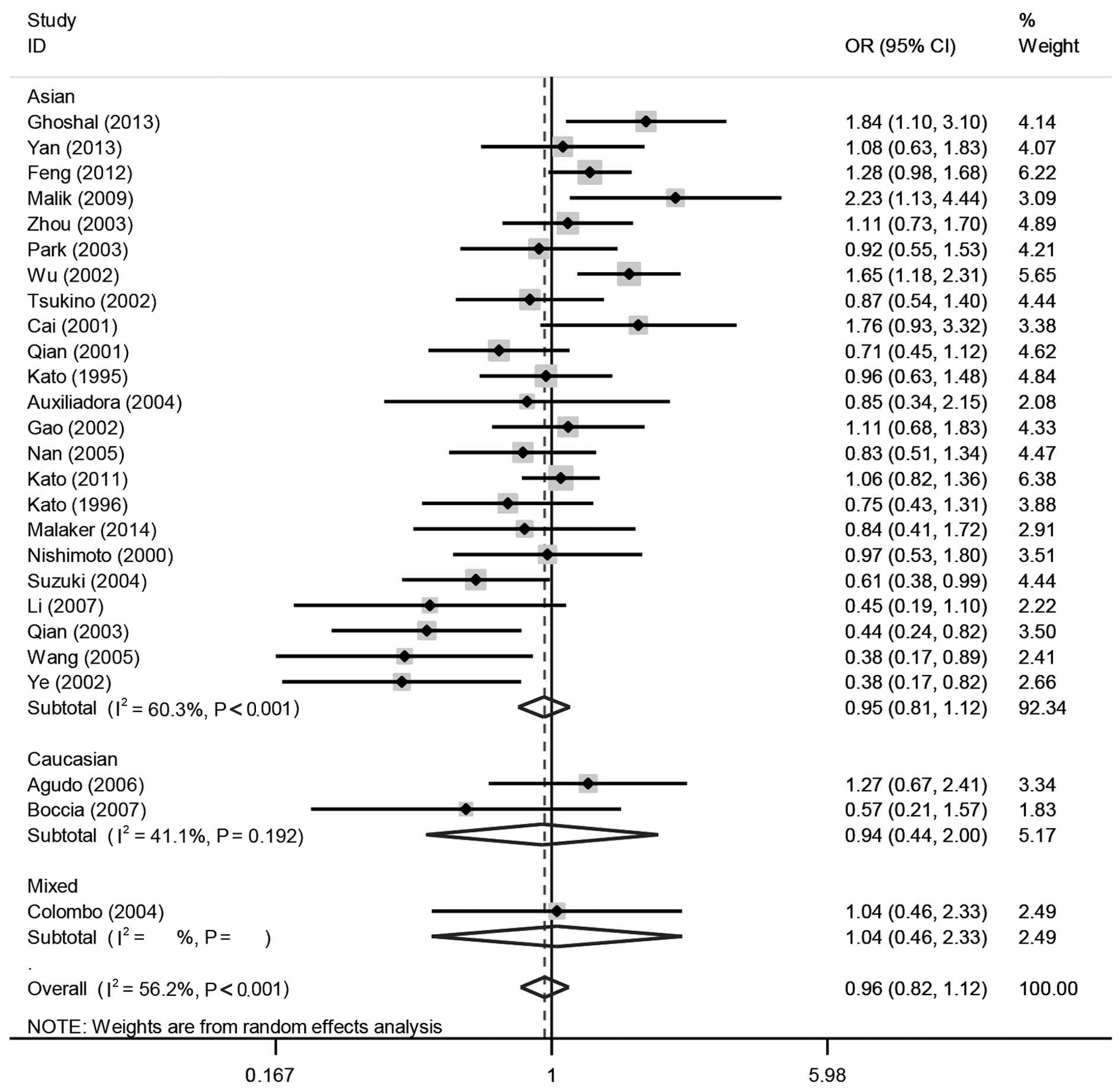
The subgroup analyses of the clinical
characteristics are shown in Table
III. In the source of control subgroups, no significant
differences were observed either in population-based studies or
hospital-based studies. As for ethnicity, no significant
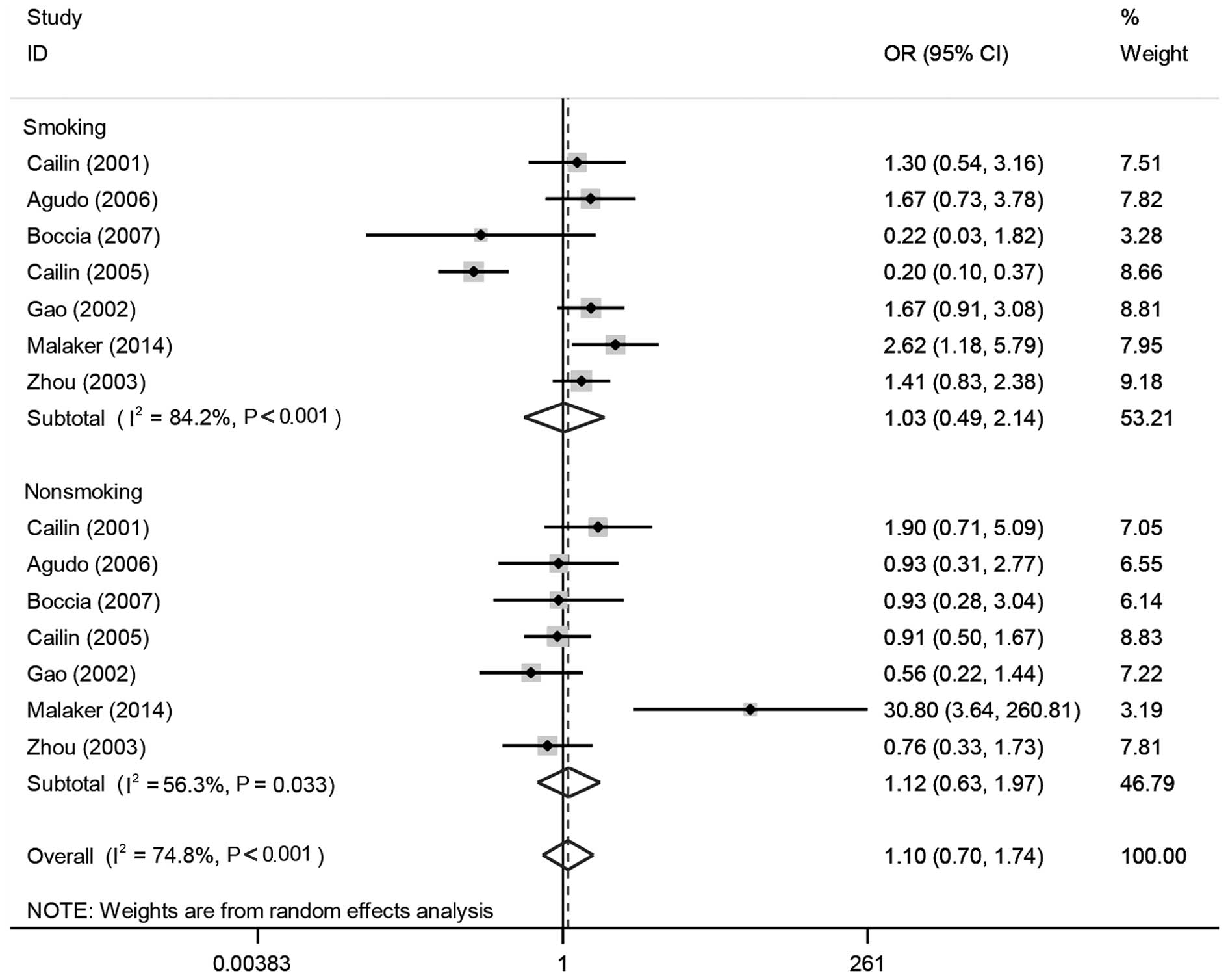
differences were observed in any of the three subgroups (Fig. 2). In the smoking status subgroup, a
significantly increased risk was observed in the smoking group
[C1C2 / C2C2 vs. C1C1 = 1.56 (1.14 and 2.15), as shown in Fig. 3], while the non-smoking group revealed
no significant difference. Subgroups of drinking status revealed no
association with GC risk. In the previous studies, which assessed
the interactions of different genes, RsaI/PstI was
demonstrated to increase GC risks when GSTM1 was null [2.60 (1.13
and 5.99)]. A significantly increased risk was also observed in the
previous studies investigating the interaction between
RsaI/PstI and GSTT1. In the GSTT1 null group, a
significant difference was observed between increased risk of GC
and RsaI/PstI [0.22 (0.09 and 0.54)].
In the meta-analysis of DraI polymorphisms,
no significant risk of GC susceptibility was observed either in the
dominant model (CD + CC vs. DD) or allele frequency (C vs. D).
However, the interaction analysis of RsaI/PstI and
DraI on CYP2E1 revealed that RsaI/PstI
significantly increased the risk of GC when DraI was
wild-type (DD) [1.55 (1.13 and 2.14)].
Heterogeneity between the previous
studies
Heterogeneities of each comparison are shown in
Table III. The results revealed
that I2 = 61.4% and Ph<0.001. Compared
with the overall analysis of RsaI/PstI polymorphisms,
heterogeneities decreased in several subgroups (population-based
controls group: I2 = 35.3% and Ph = 0.147;
Caucasian group: I2 = 41.1% and Ph =
0.192).
In previous DraI polymorphism studies, the
heterogeneity P-values were markedly higher compared with the
critical value (P=0.01), noting that heterogeneities in the group
of DraI polymorphisms were very little.
Sensitivity analysis
Influence analysis was performed by excluding
studies one-by-one and analyzing the homogeneity and effect size
for all of the remaining studies, aiming at examining the stability
of the analysis. The results revealed that no individual study
affected the pooled ORs significantly, in either the
RsaI/PstI or DraI studies, confirming the
stability of the analysis. This was associated with the high
quality of the previous studies included.
Publication bias
Begg and Mazumdar's adjusted rank correlation test
and the Egger regression asymmetry test were each used to examine
the publication bias, as well as funnel plots. The results revealed
that no publication bias was observed in RsaI/PstI
(Fig. 4) and DraI studies.
Publication bias occurred in the studies of RsaI/PstI
[Egger's test: P=0.033 in the dominant model (C1C2 + C2C2, vs.
C1C1)], while no publication bias was observed in the DraI
studies.
Discussion
For previous studies of RsaI/PstI
polymorphisms, the overall analysis revealed no association between
mutant C2 and GC risk. However, in the subgroup analysis, mutant C2
in RsaI/PstI significantly increased GC risk in the
smoking population and GSTM1- or GSTT1-null populations. In the
DraI polymorphism studies, variant allele C revealed no
association with GC risk. In the interaction analysis, C2 in
RsaI/PstI was revealed to increase GC risk when the
DraI was not mutated.
The present study obtained two meta-analyses
focusing on the association between RsaI/PstI
polymorphisms and GC susceptibility (20,51). It
was demonstrated that RsaI/PstI polymorphisms
increased GC risk in the smoking population; however, no focus on
the DraI polymorphisms or the interactions between two
polymorphisms was provided. Therefore, the updated meta-analysis
included 32 previous studies, in which 26 studies were on
RsaI/PstI and the remaining six studies were on
DraI. In our meta-analysis, more subgroups were made due to
their potential influence on GC susceptibility. Furthermore, the
present study demonstrated the interaction analysis between
different gene polymorphisms. Previous studies on these interaction
analyses may be insufficient; however, the results obtained may
provide a guidance of which type of studies are required in the
future.
In the 26 studies of RsaI/PstI
polymorphisms, no significant differences were observed in the
homozygous dominant model (C1C2 + C2C2 vs. C1C1) and in C2 vs. C1,
indicating the lack of association between the
RsaI/PstI polymorphisms and the risk of GC.
In the subgroup analysis on source of controls, no
statistically significant risks were observed in either groups with
hospital-based controls or groups with population-based controls.
Although hospital-based controls may not always be truly
representative of the general population (52), differences were reflected between GC
patients and those of healthy individuals. Population-based
controls are an improved representation of the entire population
gene frequency compared with hospital-based controls, and provide a
good reflection of gene frequency differences between GC patients
and the overall population. Therefore, more case-control studies
based on population-based controls will be performed in the
future.
As for the subgroup analysis of ethnicity, no
statistically significant differences were observed among groups of
Asians, Caucasian or mixed. Although no statistically significant
differences appeared in the subgroups, heterogeneity of the
genotype frequencies existed in different ethnic groups clinically.
The variant alleles C2 and C frequencies in CYP2E1 harbored in
Asians are markedly higher compared with those in aCaucasians or
African-Americans (53–55). Similar cases were observed in several
other polymorphisms (56). It is
hypothesized that various living environments and diverse genotypes
lead to different degrees of cancer susceptibility (8). A lack of association between GC risks
and RsaI/PstI in Caucasians and mixed populations may
be attributed to insufficiency of studies included and more studies
of Caucasians are required in the future.
In the smoking subgroup, mutant C2 was demonstrated
to be associated with increased GC risk. A previous study (57) revealed that smoking is a risk of
cancer. Tobacco smoke contains many carcinogens, including
benzopyrene and nitrosamine. CYP2E1 is critical in the metabolism
of nitrosamines, benzene and vinyl chloride in the human body.
Therefore, the interaction between smoking and CYP2E1 polymorphisms
may magnify the GC incidence. Previous studies focusing on the
interaction between smoking status and CYP2E1 were few, and more
credible results depended on more studies being included (18,20–22,31,45).
In the drinking status subgroup, no significant
association was observed between RsaI/PstI
polymorphisms and GC risk. Alcohol can directly stimulate the
gastric mucosa and damage gastric mucosal, making the gastric
mucosal epithelium more susceptible to carcinogens (58). In addition, the stimulation of alcohol
activated the function of CYP2E1 and in this resulted in an
increased GC susceptibility with a synergistic effect. More studies
involving an interaction between drinking and CYP2E1 polymorphisms
may assist in obtaining a positive result.
According to the pathological type, GC can be
divided into intestinal and diffuse types. Tumor cells in the
intestinal type are normally confined to the lining of the stomach,
while the diffuse type has a tendency to widely spread. The
subgroup analysis may assist in understanding how differences in
CYP2E1 affects the two types of GC. However, the result revealed no
significant difference between the intestinal and diffuse
groups.
Six previous DraI polymorphism studies
(20,24,27,33,35,43),
showed that no significant association was observed between
DraI polymorphisms and GC risk. However, in consideration of
the fact that only six studies were included in the research
regarding DraI polymorphisms, the reliability of the results
depended on more DraI studies being included. These results
should be treated with caution, as more case-control tests are
required to support the results.
Tumor incidence is often a combination of multiple
factors. The interaction of multiple genes increases the impact on
GC susceptibility compared with a single gene. Notably, negative
association between a gene and cancer susceptibility does not mean
that the gene has no impact on cancer risk. In the previous
studies, which involved RsaI/PstI polymorphisms and
other genes, it was revealed that the RsaI/PstI
polymorphism significantly increases GC risk when GSTM1 or GSTT1
were in a null status. GSTT1 and GSTM1 convert carcinogens in the
body into an inactive state, therefore, detoxifying them. However,
when GSTT1 and GSTM1 are mutated into a null state, their
detoxification functions are lost, which increases cancer
susceptibility (59). Additionally,
mutant genotype C2 in RsaI/PstI has a suppressive
effect in this process and GC risk was increased by such an
interaction theoretically. Statistically, no significant result was
obtained. However, the results were based on limited research data
and the credibility was questionable. Further studies are required
to improve the result in the future.
The two polymorphisms on an identical gene may lead
to a synergistic effect or antagonism. When analyzing the
interaction of RsaI/PstI and DraI
polymorphisms, the mutant C2 in RsaI/PstI was
revealed to increase GC risk when the DraI was without
mutation (DD). This result may reveal that the two polymorphisms
are working antagonistically. An RsaI/PstI mutation
may increase cancer risks, while DraI functions with the
opposite effect. Previous studies (17,60) on
DraI polymorphisms and cancer susceptibility have revealed
that DraI was more likely to be a risk factor of cancer,
which is contrary to our assumption. By contrast, limited data may
bring the contingency and must be treated with caution.
The heterogeneities in the subgroups of Caucasians
and population-based controls decreased compared with the overall
analysis of the RsaI/PstI polymorphisms, meaning that
the source of controls and ethnic groups are undoubtedly factors
for the formation of heterogeneity.
Publication bias occurred in the studies of
RsaI/PstI, most probably due to several reasons:
Previous studies with negative results are more difficult to
publish compared with those with positive results; authors prefer
to write articles with positive results as opposed to negative
results. The existence of publication bias led to our cautious
attitude to the positive results obtained in the present
meta-analysis.
Certain limitations were observed in this
meta-analysis. Firstly, only published results were included, which
actually contributed to publication bias, causing the results to be
treated with a conservative attitude. Secondly, several previous
studies were excluded since they provided no detailed genotypic
frequencies, therefore adding selection bias to a certain extent.
Thirdly, more studies focusing on RsaI/PstI and
DraI polymorphisms in the same cases and controls were
included; however, the authors provided no matched genotype
frequencies of the two genetic loci, which resulted in exploring
the interaction between them with limited data. Finally, the lack
of the sample size influenced the credibility in several subgroup
analyses and gene interaction studies. More studies focusing on
large-scale samples with multi-variables are required in the
future. In conclusion, a lack of association was observed between
the risk of GC and CYP2E1 RsaI/PstI or DraI
polymorphisms.
Acknowledgements
The authors would like to thank the Professors and
members of the Department of Gastrointestinal Surgery, Shandong
Cancer Hospital and Institute (Jinan, China) for their hard
work.
References
|
1
|
Karimi P, Islami F, Anandasabapathy S,
Freedman ND and Kamangar F: Gastric cancer: Descriptive
epidemiology, risk factors, screening and prevention. Cancer
Epidemiol Biomarkers Prev. 23:700–713. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yang L: Incidence and mortality of gastric
cancer in China. World J Gastroenterol. 12:17–20. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Gianfagna F, De Feo E, van Duijn CM,
Ricciardi G and Boccia S: A systematic review of meta-analyses on
gene polymorphisms and gastric cancer risk. Curr Genomics.
9:361–374. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hamilton JP and Meltzer SJ: A review of
the genomics of gastric cancer. Clin Gastroenterol Hepatol.
4:416–425. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Milne AN, Carneiro F, O'Morain C and
Offerhaus GJ: Nature meets nurture: Molecular genetics of gastric
cancer. Hum Genet. 126:615–628. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Saeki N, Ono H, Sakamoto H and Yoshida T:
Genetic factors related to gastric cancer susceptibility identified
using a genome-wide association study. Cancer Sci. 104:1–8. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yoshida T, Ono H, Kuchiba A, Saeki N and
Sakamoto H: Genome-wide germline analyses on cancer susceptibility
and GeMDBJ database: Gastric cancer as an example. Cancer Sci.
101:1582–1589. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bellec G, Dréano Y, Lozach P, Ménez JF and
Berthou F: Cytochrome P450 metabolic dealkylation of nine
N-nitrosodialkylamines by human liver microsomes. Carcinogenesis.
17:2029–2034. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ingelman-Sundberg M, Ronis MJ, Lindros KO,
Eliasson E and Zhukov A: Ethanol-inducible cytochrome P4502E1:
Regulation, enzymology and molecular biology. Alcohol Alcohol
Suppl. 2:131–139. 1994.PubMed/NCBI
|
|
11
|
Raucy JL, Kraner JC and Lasker JM:
Bioactivation of halogenated hydrocarbons by cytochrome P4502E1.
Crit Rev Toxicol. 23:1–20. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
La Vecchia C, D'Avanzo B, Airoldi L, Braga
C and Decarli A: Nitrosamine intake and gastric cancer risk. Eur J
Cancer Prev. 4:469–474. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Agundez JA: Cytochrome P450 gene
polymorphism and cancer. Curr Drug Metab. 5:211–224. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Uematsu F, Ikawa S, Kikuchi H, et al:
Restriction fragment length polymorphism of the human CYP2E1
(cytochrome P450IIE1) gene and susceptibility to lung cancer:
Possible relevance to low smoking exposure. Pharmacogenetics.
4:58–63. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hayashi S, Watanabe J and Kawajiri K:
Genetic polymorphisms in the 5′-flanking region change
transcriptional regulation of the human cytochrome P450IIE1 gene. J
Biochem. 110:559–565. 1991.PubMed/NCBI
|
|
16
|
Uchimoto T, Itoga S, Nezu M, Sunaga M,
Tomonaga T and Nomura F: Role of the genetic polymorphisms in the
5′-flanking region for transcriptional regulation of the human
CYP2E1 gene. Alcohol Clin Exp Res. 31(Suppl 1): S36–S42. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tang K, Li Y, Zhang Z, et al: The
PstI/RsaI and DraI polymorphisms of CYP2E1 and head and neck cancer
risk: A meta-analysis based on 21 case-control studies. BMC Cancer.
10:5752010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Agudo A, Sala N, Pera G, et al: No
association between polymorphisms in CYP2E1, GSTM1, NAT1, NAT2 and
the risk of gastric adenocarcinoma in the European prospective
investigation into cancer and nutrition. Cancer Epidemiol
Biomarkers Prev. 15:1043–1045. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
González A, Ramírez V, Cuenca P and Sierra
R: Polymorphisms in detoxification genes CYP1A1, CYP2E1, GSTT1 and
GSTM1 in gastric cancer susceptibility. Rev Biol Trop. 52:591–600.
2004.(In Spanish). PubMed/NCBI
|
|
20
|
Boccia S, De Lauretis A, Gianfagna F, van
Duijn CM and Ricciardi G: CYP2E1PstI/RsaI polymorphism and
interaction with tobacco, alcohol and GSTs in gastric cancer
susceptibility: A meta-analysis of the literature. Carcinogenesis.
28:101–106. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Cai L, Yu SZ and Zhan ZF: Cytochrome P450
2E1 genetic polymorphism and gastric cancer in Changle, Fujian
Province. World J Gastroenterol. 7:792–795. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Gao C, Takezaki T, Wu J, et al:
Interaction between cytochrome P-450 2E1 polymorphisms and
environmental factors with risk of esophageal and stomach cancers
in Chinese. Cancer Epidemiol Biomarkers Prev. 11:29–34. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Colombo J, Rossit AR, Caetano A, Borim AA,
Wornrath D and Silva AE: GSTT1, GSTM1 and CYP2E1 genetic
polymorphisms in gastric cancer and chronic gastritis in a
Brazilian population. World J Gastroenterol. 10:1240–1245.
2004.PubMed/NCBI
|
|
24
|
Darazy M, Balbaa M, Mugharbil A, et al:
CYP1A1, CYP2E1, and GSTM1 gene polymorphisms and susceptibility to
colorectal and gastric cancer among Lebanese. Genet Test Mol
Biomarkers. 15:423–429. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Ghoshal U, Tripathi S, Kumar S, et al:
Genetic polymorphism of cytochrome P450 (CYP) 1A1, CYP1A2 and
CYP2E1 genes modulate susceptibility to gastric cancer in patients
with Helicobacter pylori infection. Gastric Cancer.
17:226–234. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Nan HM, Song YJ, Yun HY, Park JS and Kim
H: Effects of dietary intake and genetic factors on
hypermethylation of the hMLH1 gene promoter in gastric cancer.
World J Gastroenterol. 11:3834–3841. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Feng J, Pan X, Yu J, et al: Functional
PstI/RsaI polymorphism in CYP2E1 is associated with the
development, progression and poor outcome of gastric cancer. PLoS
One. 7:e444782012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kato S, Onda M, Matsukura N, et al:
Cytochrome P4502E1 (CYP2E1) genetic polymorphism in a case-control
study of gastric cancer and liver disease. Pharmacogenetics.
5:S141–S144. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kato S, Onda M, Matsukura N, et al:
Genetic polymorphisms of the cancer related gene and
Helicobacter pylori infection in Japanese gastric cancer
patients. An age and gender matched case-control study. Cancer.
77(Suppl 8): S1654–S1661. 1996. View Article : Google Scholar
|
|
30
|
Kato S, Naito Z, Matsuda N, et al:
Localization of cytochrome P4502E1 enzyme in normal and cancerous
gastric mucosa and association with its genetic polymorphism in
unoperated and remnant stomach. J Nippon Med Sch. 78:224–234. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Malakar M, Devi KR, Phukan RK, et al:
CYP2E1 genetic polymorphism with dietary, tobacco, alcohol habits,
H. pylori infection status and susceptibility to stomach
cancer in Mizoram, India. Asian Pac J Cancer Prev. 15:8815–8822.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Malik MA, Upadhyay R, Mittal RD, Zargar
SA, Modi DR and Mittal B: Role of xenobiotic-metabolizing enzyme
gene polymorphisms and interactions with environmental factors in
susceptibility to gastric cancer in Kashmir Valley. J Gastrointest
Cancer. 40:26–32. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wu MS, Chen CJ, Lin MT, et al: Genetic
polymorphisms of cytochrome p450 2E1, glutathione S-transferase M1
and T1, and susceptibility to gastric carcinoma in Taiwan. Int J
Colorectal Dis. 17:338–343. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Nishimoto IN, Hanaoka T, Sugimura H, et
al: Cytochrome P450 2E1 polymorphism in gastric cancer in Brazil:
Case control studies of Japanese Brazilians and non-Japanese
Brazilians. Cancer Epidemiol Biomarkers Prev. 9:675–680.
2000.PubMed/NCBI
|
|
35
|
Park GT, Lee OY, Kwon SJ, et al: Analysis
of CYP2E1 polymorphism for the determination of genetic
susceptibility to gastric cancer in Koreans. J Gastroenterol
Hepatol. 18:1257–1263. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Suzuki S, Muroishi Y, Nakanishi I and Oda
Y: Relationship between genetic polymorphisms of drug-metabolizing
enzymes (CYP1A1, CYP2E1, GSTM1 and NAT2), drinking habits,
histological subtypes, and p53 gene point mutations in Japanese
patients with gastric cancer. J Gastroenterol. 39:220–230. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Tsukino H, Kuroda Y, Qiu D, Nakao H, Imai
H and Katoh T: Effects of cytochrome P450 (CYP) 2A6 gene deletion
and CYP2E1 genotypes on gastric adenocarcinoma. Int J Cancer.
100:425–428. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Li Z and Xu L: Relationship between
cytochrome P450 2E1 gene polymorphism and gastric cancer
susceptibility. J Pract Med. 3380–3381. 2007.
|
|
39
|
Qian Y, Xu Y, Shen H, Yu R, Tan Y, Zhou L
and Niu J: Relationship between CYP2E1, GSTT1 genetic polymorphisms
and susceptibility to gastric cancer. China's primary health care.
18–20. 2001.
|
|
40
|
Qian Y, Xu Y, Shen H, Zhou L, Yu R, Niu J
and Tan Y: Relationship Between CYP2E1, GSTT1 Genetic Polymorphisms
and Susceptibility to Gastric Cancer. Chin J Prev Control Chron Non
Commun Dis. 107–109. 2003.
|
|
41
|
Wang Y, Jiang Y and Sun W: Effects of
genetic polymorphism of cytochrome P4502E1 on susceptibility to
gastric cancer. Chin J Publ Health. 664–665. 2005.
|
|
42
|
Yan S, Bai Z, Zhao J, Xie D and Wu J:
Correlation between genetic polymorphisms of CYP2E1 RsaI and
susceptibility of gastric cancer in Qinghai province. J Qinghai Med
Coll. 34:7–14. 2013.
|
|
43
|
Su Y, Zhenzhong B, Jian-xin Z, et al:
Correlation between genetic polymorphisms of CYP2E1 Dra I and
susceptibility of gastric cancer in Qinghai province. China Oncol.
23:273–278. 2013.
|
|
44
|
Ye M, Liu J, Zhou X and Deng C:
Association between CYE2E1 genotype and genetic susceptibility of
gastric cancer. J Fourth Mil Med Univ. 2265–2267. 2002.
|
|
45
|
Zhou J, Gao C, Takezaki T, Li Z, Wu J,
Ding J, Liu Y, Li S, Hu X, Kai H and Tajima K: Interaction between
polymorphisms in CYP2E1 Rsa I genotypes and lifestyle with risk of
stomach cancer. J Oncol. 9:285–288. 2003.
|
|
46
|
Higgins JP, Thompson SG, Deeks JJ and
Altman DG: Measuring inconsistency in meta-analyses. BMJ.
327:557–560. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
DerSimonian R and Laird N: Meta-analysis
in clinical trials. Control Clin Trials. 7:177–188. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Begg CB and Mazumdar M: Operating
characteristics of a rank correlation test for publication bias.
Biometrics. 50:1088–1101. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Egger M, Smith Davey G, Schneider M and
Minder C: Bias in meta-analysis detected by a simple, graphical
test. BMJ. 315:629–634. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Munafò MR, Clark TG and Flint J: Assessing
publication bias in genetic association studies: Evidence from a
recent meta-analysis. Psychiatry Res. 129:39–44. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Zhuo W, Zhang L, Wang Y, Ling J, Zhu B and
Chen Z: CYP2E1 RsaI/PstI polymorphism and gastric cancer
susceptibility: Meta-analyses based on 24 case-control studies.
PLoS One. 7:e482652012. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Ruano-Ravina A, Pérez-Ríos M and
Barros-Dios JM: Population-based versus hospital-based controls:
Are they comparable? Gac Sanit. 22:609–613. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Garte S, Gaspari L, Alexandrie AK, et al:
Metabolic gene polymorphism frequencies in control populations.
Cancer Epidemiol Biomarkers Prev. 10:1239–1248. 2001.PubMed/NCBI
|
|
54
|
Neafsey P, Ginsberg G, Hattis D, Johns DO,
Guyton KZ and Sonawane B: Genetic polymorphism in CYP2E1:
Population distribution of CYP2E1 activity. J Toxicol Environ
Health B Crit Rev. 12:362–388. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Stephens EA, Taylor JA, Kaplan N, et al:
Ethnic variation in the CYP2E1 gene: Polymorphism analysis of 695
African-Americans, European-Americans and Taiwanese.
Pharmacogenetics. 4:185–192. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Schmidt HM, Ha DM, Taylor EF, et al:
Variation in human genetic polymorphisms, their association with
Helicobacter pylori acquisition and gastric cancer in a
multi-ethnic country. J Gastroenterol Hepatol. 26:1725–1732. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Benowitz NL, Peng M and Jacob P III:
Effects of cigarette smoking and carbon monoxide on chlorzoxazone
and caffeine metabolism. Clin Pharmacol Ther. 74:468–474. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Murata M, Takayama K, Choi BC and Pak AW:
A nested case-control study on alcohol drinking, tobacco smoking,
and cancer. Cancer Detect Prev. 20:557–565. 1996.PubMed/NCBI
|
|
59
|
Masoudi M, Saadat I, Omidvari S and Saadat
M: Genetic polymorphisms of GSTO2, GSTM1, and GSTT1 and risk of
gastric cancer. Mol Biol Rep. 36:781–784. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Wu X, Amos CI, Kemp BL, et al: Cytochrome
P450 2E1 DraI polymorphisms in lung cancer in minority populations.
Cancer Epidemiol Biomarkers Prev. 7:13–18. 1998.PubMed/NCBI
|