Introduction
Lung cancer exhibits the greatest mortality rate of
all types of cancer in men and women worldwide (1). Until recently, treatment for advanced
lung cancer included only cytotoxic anticancer drugs. More
recently, molecular target drugs that are much more tolerable and
cause fewer adverse events have been developed (2). Notably, epidermal growth factor
receptor (EGFR) tyrosine kinase inhibitors and anaplastic lymphoma
kinase (ALK) inhibitors greatly improved the prognosis of specific
patient subgroups with EGFR-activating mutations or ALK
rearrangements (3). However, in
later stages of advanced lung cancer, effective therapies are still
limited.
Novel drugs including pembrolizumab, nivolumab, and
atezolizumab, referred to as immune checkpoint inhibitors (ICPi),
have been approved by the US Food and Drug Administration (FDA) for
previously treated advanced non-small cell lung cancer (NSCLC). The
Checkmate-017 (4), Checkmate-057
(5), KEYNOTE-010 (6) and OAK (7) trials demonstrated the superiority of
these agents over docetaxel, which had previously been the standard
of care for second-line therapy. ICPi block the interaction between
programmed cell death-1 (PD-1) on activated cytotoxic T-lymphocytes
(CTLs) and programmed cell death ligand-1 (PD-L1) on tumor cells,
which inactivate the tumoricidal activity of CTLs (8). The response to ICPi is ~20% (9). Certain factors, including PD-L1
expression, smoking history and EGFR mutations, were
suggested to be predictive biomarkers in several clinical trials
(10–13), but they are not enough to predict
response with ICPi. In the meantime, the efficacy of PD-1 blockade
therapy is considered to be relevant to metabolism (14–17). The
association between metformin, a type 2 diabetes drug, and the
efficacy of PD-1 blockade has been reported in vivo and
in vitro (18). Other drugs
that affect metabolism, such as statins, have also been reported to
have antitumor effects (19). The
off-target effects in combination with cytotoxic chemotherapy and
metoformin/statin resulted in longer survival for elderly NSCLC
patients due to attenuated chronic inflammation (20).
In the present study a prospective observational
database was used to evaluate advanced NSCLC patients previously
treated with nivolumab to investigate predictive biomarkers and the
effects of drugs that affect metabolism.
Patients and methods
Patients and data acquisition
A total of 73 patients treated with nivolumab for
advanced NSCLC in the first (recurrence after surgery), second or
later lines of therapy at the Tokyo Metropolitan Cancer and
Infectious Diseases Center Komagome Hospital (Tokyo, Japan) between
January 2016 and February 2017 who did not participate in other
clinical trials were identified using the database of the
prospective observational study (UMIN registry no. UMIN000021694)
and the study protocol was approved by the Ethics Committee of
Tokyo Metropolitan Cancer and Infectious Diseases Center Komagome
Hospital. Written informed consent from patients was waived for the
present study by the Ethics Committee due to the observational
nature of the protocol. The following clinical factors of lung
cancer patients were examined: Age, sex, Eastern Cooperative
Oncology Group Performance status (21), histology, EGFR mutation,
history of chemotherapy, smoking status, use of statins, use of
fibrates, use of dipeptidyl peptidase-4 (DPP-4) inhibitors and use
of metformin. Patients treated with involumab in the present
analysis was concurrently treated with statins, fibrateds, DDP-4
inhibitors, and metformin. The status of each patient at the
beginning of nivolumab therapy was evaluated based on the use of
statins by each patient. The same classification method was used
for fibrates, DPP-4 inhibitors, and metformin.
Statistical analysis
Descriptive statistics was used to summarize the
patients' baseline characteristics. The objective tumor response of
nivolumab was determined following the Response Evaluation Criteria
in Solid Tumors (RECIST) version 1.1 guidelines (22). The efficacy of nivolumab prior
therapy was divided into two groups: Responders and non-responders.
In patients treated with chemotherapy, responders were patients who
achieved complete response (CR) or partial response (PR) according
to the RECIST version 1.1 guidelines (23). Overall survival (OS) was defined as
the time from the date of nivolumab treatment to the date of death
for any reason. The time-to-treatment failure (TTF) was defined as
the time from the date of initiation of nivolumab treatment to the
date of disease progression or death. In any case of termination
because of immune-related adverse events (irAE), the date of
progression or death was defined as the event. Retreatment of
nivolumab following recovery from irAE was permissive.
Univariate and multivariate analyses were conducted
to identify the associations between the response to nivolumab
therapy and the clinical characteristics of patients with advanced
NSCLC. Categorical variables were tested for significance using
Fisher's exact test or the χ2 test, as appropriate.
Multivariate logistic regression analysis was used to assess the
associations between patient variables and response to nivolumab
therapy. TTF was estimated using Kaplan-Meier curves with a
two-sided log-rank test. All P-values were two-sided, and P<0.05
was considered to indicate a statistically significant difference.
All statistical analyses were performed using the JMP 11 software
(SAS Institute, Inc., Cary, NC, USA).
Results
Baseline characteristics
Among 73 patients treated with nivolumab as the
second-line or later lines of chemotherapy, a total of 67 patients
whose radiological response could be evaluated were included in
this analysis. Patients had a median age of 67 years (36–87 years).
A total of 46 male and 21 female patients were analyzed. A total of
41 (61.2%) patients had adenocarcinoma, and 17 (25.4%) patients had
squamous cell carcinoma. A total of 13 (19.4%) patients had
EGFR mutation. At the time of initiation of nivolumab, 10
(14.9%) patients were treated with statins. Other patient
characteristics are detailed in Table
I. The median follow-up time calculated from nivolumab
treatment was 3.5 months. A total of 2 patients included with
metformin at a dose of 250 mg/day; 3 patients were included who
were treated with 10 mg/day atorvastatin; 1 patient was treated
with 30 mg/day of fluvastatin; 2 patients were treated with 2.5
mg/day of rosuvastatin; 3 patients were treated with 5 mg/day of
pravastatin and 1 patient was treated with 2.5 mg/day of
pravastatin.
 | Table I.Baseline characteristics of
registered patients. |
Table I.
Baseline characteristics of
registered patients.
| Variants | Statins (+)
(n=10) | % | Statins (−)
(n=57) | % |
|---|
| Age, years [median
(range)] | 70 (53–78) |
| 67 (36–87) |
|
| Sex |
|
Male | 8 | 80.0 | 38 | 66.7 |
|
Female | 2 | 20.0 | 19 | 33.3 |
| PS |
|
0/1 | 9 | 90.0 | 50 | 86.7 |
| 2 | 1 | 10.0 | 7 | 13.3 |
| Histological
subtypes |
|
Adenocarcinoma | 7 | 70.0 | 34 | 59.6 |
|
SQC | 2 | 20.0 | 15 | 26.3 |
|
NSCLC | 0 | 0 | 4 | 7.0 |
|
ADSQC | 0 | 0 | 2 | 3.6 |
|
LCNEC | 1 | 10.0 | 1 | 1.8 |
| Large
cell carcinoma | 0 | 0 | 1 | 1.8 |
| EGFR mutation |
|
Wild-type | 10 | 100.0 | 34 | 77.2 |
| EGFR
exon19 del | 0 | 0 | 7 | 12.2 |
| EGFR
exon21 L858R | 0 | 0 | 6 | 10.6 |
| Lines of
chemotherapy, median (range) | 2 (2–4) |
| 2 (1–5) |
|
| Smoking Status |
| Current
or former | 8 | 100 | 47 | 82.5 |
|
Never | 0 | 0 | 10 | 17.5 |
| Use of
fibrates |
|
Yes | 0 | 0 | 4 | 7.0 |
| No | 10 | 100 | 53 | 93.0 |
| Use of DPP-4
inhibitors |
|
Yes | 3 | 30.0 | 2 | 3.5 |
| No | 7 | 70.0 | 55 | 96.5 |
| Use of
metformin |
|
Yes | 1 | 10.0 | 1 | 1.8 |
| No | 9 | 90.0 | 56 | 98.2 |
Clinical outcome
Of the 67 patients, 1 achieved a CR, 14 achieved a
PR, 23 achieved stable disease status, and 25 developed progressive
disease (PD) according to the RECIST criteria. A total of 4
patients were not evaluated for response due to early death or loss
to follow-up. The objective response rate was 22.4% (Table II).
| Table II.Objective response to treatment. |
Table II.
Objective response to treatment.
| Objective
response | Patients, n | (%) |
|---|
| CR | 1 | 1.5 |
| PR | 14 | 20.9 |
| SD | 23 | 34.3 |
| PD | 25 | 37.3 |
| NE | 4 | 6.0 |
| Overall response
rate (%) | 15 | 22.4 |
The results of univariate and multivariate analyses
of variable factors of response in patients treated with nivolumab
are presented in Table III. In the
univariate analysis, patients treated with nivolumab as a first- or
second-line therapy tended to have a better response rate than
those receiving nivolumab as a later-line therapy [odds ratio (OR),
36.7 vs. 4.5%, respectively; P=0.008]. In addition, patients
treated with statins at the time of initiation of nivolumab therapy
tended to have a better response rate than those not treated with
statins (ORR, 62.5 vs. 15.9%, respectively; P=0.011). Multivariate
logistic regression demonstrated that the use of statins was
independent of response to nivolumab therapy [OR, 0.011; 95%
confidence interval (CI): 1.35–40.10; P=0.021]. EGFR
mutations were revealed to not be a predictive factor; none of the
patients who had EGFR mutations was a responder.
| Table III.Univariate and multivariate analyses
of variable factors of response in previously treated NSCLC
patients treated with nivolumab. |
Table III.
Univariate and multivariate analyses
of variable factors of response in previously treated NSCLC
patients treated with nivolumab.
|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|---|
| Characteristic | RR (%) | OR | 95% CI | P-value | OR | 95% CI | P-value |
|---|
| Age, years |
|
<70 | 26.5 | 0.56 | 0.08–2.74 | 0.51 |
|
|
|
|
≥70 | 16.7 |
|
|
|
|
|
|
| Sex |
|
Male | 24.3 | 1.27 | 0.26–8.63 | 1.00 |
|
|
|
|
Female | 20.0 |
|
|
|
|
|
|
| PS |
|
<2 | 23.4 | 0.82 | 0.02–9.53 | 1.00 |
|
|
|
| ≥2 | 20.0 |
|
|
|
|
|
|
| Histology |
|
SQC | 30.8 | 1.70 | 0.30–8.39 | 0.47 | 1.27 | 0.27–6.11 | 0.76 |
|
Other | 20.5 |
|
|
|
|
|
|
| EGFR
mutations |
|
Yes | 0 | 0 | 0–1.35 | 0.09 | 0.00 | 0.00-NR | 0.99 |
| No | 28.6 |
|
|
|
|
|
|
| Lines of
chemotherapy |
| 2 or
3 | 36.7 | 11.67 | 1.45–546.00 | 0.01 |
|
|
|
| ≥4 | 4.5 |
|
|
|
|
|
|
| Smoking status |
|
Current/former | 23.9 | 1.56 |
0.15–80.96 | 1.00 | 0.24 | 0.01–4.49 | 0.34 |
|
Never | 16.7 |
|
|
|
|
|
|
| Use of statin |
|
Yes | 62.5 | 8.29 | 1.29–66.58 | 0.01 | 7.37 | 1.35–40.10 | 0.02 |
| No | 15.9 |
|
|
|
|
|
|
| Use of fibrate |
|
Yes | 50.0 | 3.42 | 0.04–284.54 | 0.41 |
|
|
|
| No | 22.0 |
|
|
|
|
|
|
| Use of DPP-4
inhibitor |
|
Yes | 25.0 | 1.12 | 0.020–15.64 | 1.00 |
|
|
|
| No | 22.9 |
|
|
|
|
|
|
| Use of
metformin |
|
Yes | 100 | Inf | 0.09-Inf | 0.23 |
|
|
|
| No | 21.6 |
|
|
|
|
|
|
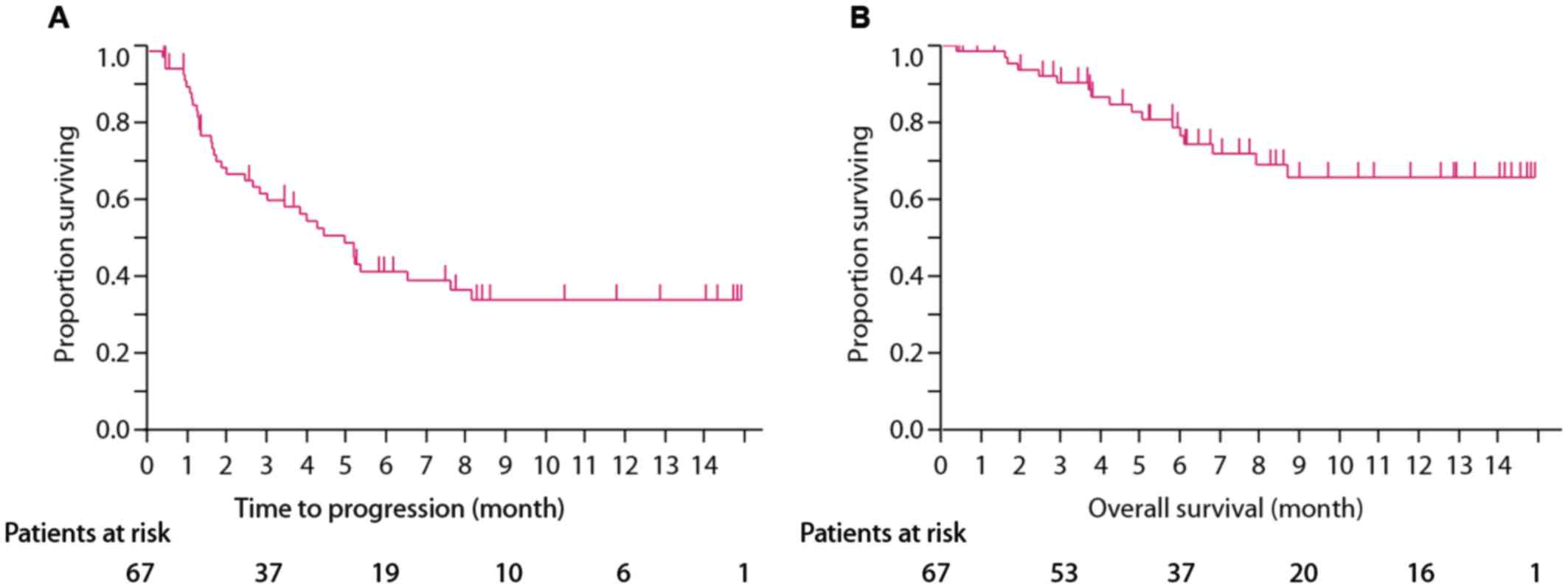
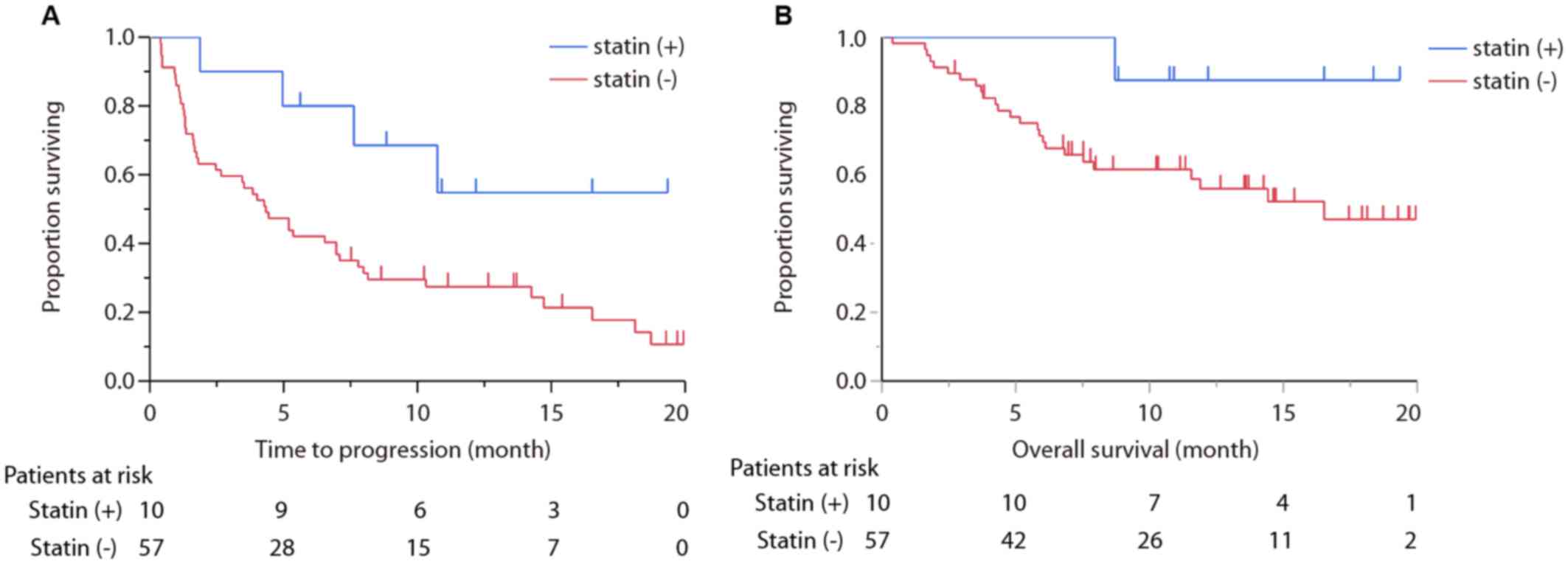
TTF for all treated patients with nivolumab was 4.96
months (95% CI: 2.66–7.62), and OS was not reached. TTF of statin
(+) group was not reached (95% CI: 1.9-not reached), whereas TTF of
statin (−) group was 4.0 months (95% CI: 2.0–5.4; P=0.039; Fig. 1A and B). OS of statin (+) group was
not reached (95% CI: 8.7-not reached) and OS of statin (−) was 16.5
months (95% CI: 7.5-not reached; P=0.058; Fig. 2A and B).
Discussion
The results of the present study demonstrated that
the use of statins led to a good response in patients treated with
nivolumab for advanced NSCLC. A number of predictive biomarkers of
nivolumab or other immune checkpoint blockade therapies have been
previously proposed. PD-L1 expression on tumor cells was
demonstrated to be a possible biomarker predictor of nivolumab or
other immune checkpoint blockade therapies in patients with
advanced NSCLC, melanoma or renal cell cancer (5,6,22). Besides PD-L1 expression of the tumor
tissue, smoking history and oncogenic driver mutations (EGFR
mutation and ALK fusion) were previously suggested to be predictive
biomarkers (5,6). In addition, previous studies revealed
that counts of neutrophils, lymphocytes, eosinophils and lactate
dehydrogenase levels in the peripheral blood could be predictive
biomarkers of ipilimumab therapy for melanoma (24–26).
However, evidence is not sufficient to use these indicators as
predictive biomarkers. Therefore, in the present study, various
markers were analyzed in patients treated with nivolumab for
advanced NSCLC to assess predictability.
In the present study of nivolumab therapy, the
response of patients treated with statins was better than that of
patients not treated with statins. Cellular metabolism is
considered to be important to immunotherapy of cancer (27). In fact, DPP-4 and metformin
inhibitors have been reported to enhance anticancer effects of ICPi
in vivo or in vitro (16,18,28). In
the present study, patients treated with DPP-4 inhibitors or
metformin were few and did not exhibit a significantly good
response. Chamoto et al (29)
recently reported that bezafibrate enhanced tumor-growth
suppression and animal-survival activities by anti-PD-L1 monoclonal
antibody. Statins, inhibitors of 3-hydroxy-3-methylglutaryl
coenzyme A reductase, are efficient and widely used drugs in the
treatment of cardiovascular diseases and lipid disorders,
especially hypercholesterolemia (28–30).
Conversely, statins have been previously reported to prolong the
survival and decrease the incidence of patients with various
cancers (30–32). The mechanism of the anticancer
activity of statins remains unclear, but a previous review has
demonstrated this anticancer effect (33). Mitogen-activated protein kinase and
extracellular signal-regulated kinase upregulate antiapoptotic
molecules in small cell lung cancer (SCLC) cells (34,35), and
simvastatin can disrupt this process through impaired Ras
superfamily signaling (34–36). Statins also have a potentially
synergic effect in combination with cytotoxic chemotherapy
(36–38). In the clinical setting, metformin and
statin attenuates chronic inflammation (and stabilization TP53
function), which demonstrated the survival benefit in combination
with EGFR tyrosine kinase inhibitor for EGFR mutation-positive
NSCLC (39) and reduced cancer risk
in Korean nation-wide surveillance (40). In the present study, nivolumab
demonstrated similar tendency for survival. A number of previous
in vitro studies have demonstrated that statins arrest cells
in the G1 or S phase by affecting cell-cycle regulatory proteins
such as cyclins, cyclin-dependent kinases (CDKs), and inhibitors of
CDK (33,41,42). In
addition, statins have been considered to lead to apoptosis of
cancer cells through effects of various molecules such as B cell
lymphoma (Bcl)-2, Bcl-2-associated X protein and caspase 3
(33,43–45).
Furthermore, statins have been demonstrated to inhibit
intracellular signaling pathways in cancer cells (33). Other studies have reported that
statins activated anticancer immunity and may reduce the
development of cancer cells and metastasis (46,47). One
previous study reported that human melanoma cells with statins
increased major histocompatibility complex (MHC) class I
chain-related protein A (MICA) membrane expression and made
melanoma cells more sensitive to NK cells (46). Conversely, previous reports have also
linked the use of statins to immunity suppression (48). Cholesterol has been reported to
induce a conformational change of the transmembrane domain of MHC
II (49), so it is presumed that
statins modify conformation and the function of immune-related
molecules, such as MHCs, and affect anticancer immunity. This
theory suggests that statins may increase anticancer effects of the
ICPi through activation of T cells. Overall, the present study
reveals a potential improved efficacy of ICPi; however, there is no
biological plausibility to illustrate.
The present study had limitations. First, only a
small number of patients were treated (n=10) with statins. It was
also difficult to evaluate the effects of confounding. Secondly,
another limitation was that dose and duration of statins and level
of cholesterol in the peripheral blood were unknown. Third, PD-L1
expression of tumor cells in patients prior to treatment was
unknown, since IHC of PD-L1 expression is not a requirement when
using nivolumab. Therefore, correlation of PD-L1 expression was not
evaluated.
A definite single predictive biomarker of ICPi has
not yet been identified and it has been suggested that the
interaction of several clinical or biological elements of the
‘cancer immunogram’ are associated with response to ICPis (50). The relevance of the mevalonate
pathway and ICPi is estimated in various mechanisms in the cancer
biology, but clinical studies with statins for SCLC patients were
not previously demonstrated to benefit the survival (51); however, nivolumab in NSCLC was not
performed. The results of the present study suggest that
combination therapy of nivolumab and statins improve the survival
rate and should be further investigated.
In the present study, it was demonstrated that the
use of statins was associated with better response and longer TTF
in patients with advanced NSCLC treated with nivolumab. Further
investigations on the predictive and clinical relevance of ICPi are
required.
Acknowledgements
The authors thank Dr Makoto Saito, the Senior
Biostatistician in the Office for Clinical Research Support in
Tokyo Metropolitan Cancer and Infectious diseases Center Komagome
Hospital (Tokyo, Japan) for statistical advice.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
MO, YO, and TH analyzed the NSCLC patient treated
with nivolumab, and were major contributors in writing this
manuscript. YO and YH analyzed and interpreted the patient data.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
All study protocols were approved by the
Institutional Review Committee of Tokyo Metropolitan Cancer and
Infectious diseases Center Komagome Hospital (Tokyo, Japan).
Patient consent for publication
Not applicable.
Competing interests
Yukio Hosomi has received honoraria from AstraZeneca
(Osaka, Japan); Taiho Pharmaceutical Co., Ltd. (Tokyo, Japan);
Chugai Pharmaceutical Co, Ltd. (Tokyo, Japan); Ono Pharmaceutical
Co., Ltd. (Tokyo, Japan); Bristol-Myers Squibb (New York, NY, USA)
and Boehringer Ingelheim (Ingelheim, Germany).
Glossary
Abbreviations
Abbreviations:
|
ALK
|
anaplastic lymphoma kinase
|
|
CR
|
complete response
|
|
CTLs
|
cytotoxic T lymphocytes
|
|
DPP-4
|
dipeptidyl peptidase-4
|
|
EGFR
|
epidermal growth factor receptor
|
|
ICPi
|
immune checkpoint inhibitors
|
|
irAE
|
immune-related adverse events
|
|
NSCLC
|
non-small cell lung cancer
|
|
PD-1
|
programmed cell death-1
|
|
PD-L1
|
programmed cell death ligand-1
|
|
PR
|
partial response
|
|
RECIST
|
response evaluation citeria in solid
tumors
|
|
TTF
|
treatment-to-failure
|
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2016. CA Cancer J Clin. 66:7–30. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ramalingam S and Belani C: Systemic
chemotherapy for advanced non-small cell lung cancer: Recent
advances and future directions. Oncologist. 13 Suppl 1:5–13. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Reck M, Popat S, Reinmuth N, De Ruysscher
D, Kerr KM and Peters S: ESMO Guidelines Working Group: Metastatic
non-small cell lung cancer (NSCLC): ESMO Clinical Practice
Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 25
Suppl 3:iii27–iii39. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Brahmer J, Reckamp KL, Baas P, Crinò L,
Eberhardt WE, Poddubskaya E, Antonia S, Pluzanski A, Vokes EE,
Holgado E, et al: Nivolumab versus docetaxel in advanced
squamous-cell non-small cell lung cancer. N Engl J Med.
373:123–135. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Borghaei H, Paz-Ares L, Horn L, Spigel DR,
Steins M, Ready NE, Chow LQ, Vokes EE, Felip E, Holgado E, et al:
Nivolumab versus docetaxel in advanced nonsquamous non-small-cell
lung cancer. N Engl J Med. 373:1627–1639. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Herbst RS, Baas P, Kim DW, Felip E,
Pérez-Gracia JL, Han JY, Molina J, Kim JH, Arvis CD, Ahn MJ, et al:
Pembrolizumab versus docetaxel for previously treated,
PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010):
A randomised controlled trial. Lancet. 387:1540–1550. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rittmeyer A, Barlesi F, Waterkamp D, Park
K, Ciardiello F, von Pawel J, Gadgeel SM, Hida T, Kowalski DM, Dols
MC, et al: OAK Study Group: Atezolizumab versus docetaxel in
patients with previously treated non-small-cell lung cancer (OAK):
A phase 3, open-label, multicentre randomised controlled trial.
Lancet. 389:255–265. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sznol M and Chen L: Antagonist antibodies
to PD-1 and B7-H1 (PD-L1) in the treatment of advanced human
cancer. Clin Cancer Res. 19:1021–1034. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Soria JC, Marabelle A, Brahmer JR and
Gettinger S: Immune checkpoint modulation for non-small cell lung
cancer. Clin Cancer Res. 21:2256–2262. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ramalingam S, Hui R, Gandhi L, Carcereny
E, Felip E, Ahn MJ, Eder JP, Balmanoukian AS, Leighl N, Aggarwal C,
et al: P2.39: Long-term OS for patients with advanced NSCLC
enrolled in the KEYNOTE-001 study of pembrolizumab: Track:
Immunotherapy. J Thorac Oncol. 11(10S): S241–S242. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Matter-Walstra K, Schwenkglenks M, Aebi S,
Dedes K, Diebold J, Pietrini M, Klingbiel D, von Moos R and
Gautschi O: Swiss Group for Clinical Cancer Research: A
cost-effectiveness analysis of nivolumab versus docetaxel for
advanced nonsquamous NSCLC including PD-L1 testing. J Thorac Oncol.
11:1846–1855. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Langer CJ, Gadgeel SM, Borghaei H,
Papadimitrakopoulou VA, Patnaik A, Powell SF, Gentzler RD, Martins
RG, Stevenson JP, Jalal SI, et al: KEYNOTE-021 investigators:
Carboplatin and pemetrexed with or without pembrolizumab for
advanced, non-squamous non-small-cell lung cancer: A randomised,
phase 2 cohort of the open-label KEYNOTE-021 study. Lancet Oncol.
17:1497–1508. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Fehrenbacher L, Spira A, Ballinger M,
Kowanetz M, Vansteenkiste J, Mazieres J, Park K, Smith D,
Artal-Cortes A, Lewanski C, et al: POPLAR Study Group: Atezolizumab
versus docetaxel for patients with previously treated
non-small-cell lung cancer (POPLAR): A multicentre, open-label,
phase 2 randomised controlled trial. Lancet. 387:1837–1846. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pearce EL, Walsh MC, Cejas PJ, Harms GM,
Shen H, Wang LS, Jones RG and Choi Y: Enhancing CD8 T-cell memory
by modulating fatty acid metabolism. Nature. 460:103–107. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rolf J, Zarrouk M, Finlay DK, Foretz M,
Viollet B and Cantrell DA: AMPKα1: A glucose sensor that controls
CD8 T-cell memory. Eur J Immunol. 43:889–896. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Araki K and Ahmed R: AMPK: A metabolic
switch for CD8+ T-cell memory. Eur J Immunol. 43:878–881. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Eikawa S, Nishida M, Mizukami S, Yamazaki
C, Nakayama E and Udono H: Immune-mediated antitumor effect by type
2 diabetes drug, metformin. Proc Natl Acad Sci USA. 112:1809–1814.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Scharping NE, Menk AV, Whetstone RD, Zeng
X and Delgoffe GM: Efficacy of PD-1 blockade is potentiated by
metformin-induced reduction of tumor hypoxia. Cancer Immunol Res.
5:9–16. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gruenbacher G and Thurnher M: Mevalonate
metabolism in cancer. Cancer Lett. 356:192–196. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lee YG, Lee JH, Jang JS and Kim JH:
Prognostic benefit of taking statin and/or metformin in elderly
patients with advanced non-small cell lung cancer: A nationwide
population-based epidemiologic study. J Clin Oncol. 36:10045. 2018.
View Article : Google Scholar
|
|
21
|
Cancer Therapy Evaluation Program, .
Common Toxicity Criteria. Version 2.0. DCTD, NCI, NIH, DHHS.
March;1998.https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcv20_4-30-992.pdf
|
|
22
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Schwartz LH, Litière S, de Vries E, Ford
R, Gwyther S, Mandrekar S, Shankar L, Bogaerts J, Chen A, Dancey J,
et al: RECIST 1.1-Update and clarification: From the RECIST
committee. Eur J Cancer. 62:132–137. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ku GY, Yuan J, Page DB, Schroeder SE,
Panageas KS, Carvajal RD, Chapman PB, Schwartz GK, Allison JP and
Wolchok JD: Single-institution experience with ipilimumab in
advanced melanoma patients in the compassionate use setting:
Lymphocyte count after 2 doses correlates with survival. Cancer.
116:1767–1775. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Delyon J, Mateus C, Lefeuvre D, Lanoy E,
Zitvogel L, Chaput N, Roy S, Eggermont AM, Routier E and Robert C:
Experience in daily practice with ipilimumab for the treatment of
patients with metastatic melanoma: An early increase in lymphocyte
and eosinophil counts is associated with improved survival. Ann
Oncol. 24:1697–1703. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ferrucci PF, Ascierto PA, Pigozzo J, Del
Vecchio M, Maio M, Cappellini Antonini GC, Guidoboni M, Queirolo P,
Savoia P, Mandalà M, et al: Baseline neutrophils and derived
neutrophil-to-lymphocyte ratio: Prognostic relevance in metastatic
melanoma patients receiving ipilimumab. Ann Oncol. 27:732–738.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Gubin MM, Zhang X, Schuster H, Caron E,
Ward JP, Noguchi T, Ivanova Y, Hundal J, Arthur CD, Krebber WJ, et
al: Checkpoint blockade cancer immunotherapy targets
tumour-specific mutant antigens. Nature. 515:577–581. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
da Silva Barreira R, Laird ME, Yatim N,
Fiette L, Ingersoll MA and Albert ML: Dipeptidylpeptidase 4
inhibition enhances lymphocyte trafficking, improving both
naturally occurring tumor immunity and immunotherapy. Nat Immunol.
16:850–858. 2015. View
Article : Google Scholar : PubMed/NCBI
|
|
29
|
Chamoto K, Chowdhury PS, Kumar A, Sonomura
K, Matsuda F, Fagarasan S and Honjo T: Mitochondrial activation
chemicals synergize with surface receptor PD-1 blockade for T
cell-dependent antitumor activity. Proc Natl Acad Sci USA.
114:E761–E770. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Nielsen SF, Nordestgaard BG and Bojesen
SE: Statin use and reduced cancer-related mortality. N Engl J Med.
367:1792–1802. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Cardwell CR, Hicks BM, Hughes C and Murray
LJ: Statin use after colorectal cancer diagnosis and survival: A
population-based cohort study. J Clin Oncol. 32:3177–3183. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Yu O, Eberg M, Benayoun S, Aprikian A,
Batist G, Suissa S and Azoulay L: Use of statins and the risk of
death in patients with prostate cancer. J Clin Oncol. 32:5–11.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Bernhart E, Damm S, Wintersperger A,
Nusshold C, Brunner AM, Plastira I, Rechberger G, Reicher H,
Wadsack C, Zimmer A, et al: Interference with distinct steps of
sphingolipid synthesis and signaling attenuates proliferation of
U87MG glioma cells. Biochem Pharmacol. 96:119–130. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Pardo OE, Lesay A, Arcaro A, Lopes R, Ng
BL, Warne PH, McNeish IA, Tetley TD, Lemoine NR, Mehmet H, et al:
Fibroblast growth factor 2-mediated translational control of IAPs
blocks mitochondrial release of Smac/DIABLO and apoptosis in small
cell lung cancer cells. Mol Cell Biol. 23:7600–7610. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Pardo OE, Wellbrock C, Khanzada UK, Aubert
M, Arozarena I, Davidson S, Bowen F, Parker PJ, Filonenko VV, Gout
IT, et al: FGF-2 protects small cell lung cancer cells from
apoptosis through a complex involving PKCepsilon, B-Raf and S6K2.
EMBO J. 25:3078–3088. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Kozar K, Kaminski R, Legat M, Kopec M,
Nowis D, Skierski JS, Koronkiewicz M, Jakóbisiak M and Golab J:
Cerivastatin demonstrates enhanced antitumor activity against human
breast cancer cell lines when used in combination with doxorubicin
or cisplatin. Int J Oncol. 24:1149–1157. 2004.PubMed/NCBI
|
|
37
|
Holstein SA and Hohl RJ: Synergistic
interaction of lovastatin and paclitaxel in human cancer cells. Mol
Cancer Ther. 1:141–149. 2001.PubMed/NCBI
|
|
38
|
Feleszko W and Jakóbisiak M: Lovastatin
augments apoptosis induced by chemotherapeutic agents in colon
cancer cells. Clin Cancer Res. 6:1198–1199. 2000.PubMed/NCBI
|
|
39
|
Rodriguez OGA, Barron FB, Padilla MÁS,
Ramirez-Tirado LA, Flores-Estrada D, Cruz-Rico G, Jiménez MJA and
Zorrilla AFC: Combination of metformin plus TKI vs. TKI alone in
EGFR(+) LUNG adenocarcinoma: A randomized phase II study. J Clin
Oncol. 36:9013. 2018. View Article : Google Scholar
|
|
40
|
Kim HJ, Lee S, Chun KH, Jeon JY, Han SJ,
Kim DJ, Kim YS, Woo JT, Nam MS, Baik SH, et al: Metformin reduces
the risk of cancer in patients with type 2 diabetes: An analysis
based on the Korean National Diabetes Program Cohort. Medicine
(Baltimore). 97:e00362018. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Rao S, Porter DC, Chen X, Herliczek T,
Lowe M and Keyomarsi K: Lovastatin-mediated G1 arrest is through
inhibition of the proteasome, independent of hydroxymethyl
glutaryl-CoA reductase. Proc Natl Acad Sci USA. 96:7797–7802. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Tu YS, Kang XL, Zhou JG, Lv XF, Tang YB
and Guan YY: Involvement of Chk1-Cdc25A-cyclin A/CDK2 pathway in
simvastatin induced S-phase cell cycle arrest and apoptosis in
multiple myeloma cells. Eur J Pharmacol. 670:356–364. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Cafforio P, Dammacco F, Gernone A and
Silvestris F: Statins activate the mitochondrial pathway of
apoptosis in human lymphoblasts and myeloma cells. Carcinogenesis.
26:883–891. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Qi XF, Zheng L, Lee KJ, Kim DH, Kim CS,
Cai DQ, Wu Z, Qin JW, Yu YH and Kim SK: HMG-CoA reductase
inhibitors induce apoptosis of lymphoma cells by promoting ROS
generation and regulating Akt, Erk and p38 signals via suppression
of mevalonate pathway. Cell Death Dis. 4:e5182013. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Spampanato C, De Maria S, Sarnataro M,
Giordano E, Zanfardino M, Baiano S, Cartenì M and Morelli F:
Simvastatin inhibits cancer cell growth by inducing apoptosis
correlated to activation of Bax and down-regulation of BCL-2 gene
expression. Int J Oncol. 40:935–941. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Moghim S, Sarikhani E, Esfahani Nasr B and
Faghri J: Identification of nontuberculous mycobacteria species
isolated from water samples using phenotypic and molecular methods
and determination of their antibiotic resistance patterns by E-test
method, in Isfahan, Iran. Iran J Basic Med Sci. 15:1076–1082.
2012.PubMed/NCBI
|
|
47
|
Bennaceur K, Atwill M, Al Zhrany N,
Hoffmann J, Keavney B, Breault D, Richardson G, von Zglinicki T,
Saretzki G and Spyridopoulos I: Atorvastatin induces T cell
proliferation by a telomerase reverse transcriptase (TERT) mediated
mechanism. Atherosclerosis. 236:312–320. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Ulivieri C, Fanigliulo D, Benati D, Pasini
FL and Baldari CT: Simvastatin impairs humoral and cell-mediated
immunity in mice by inhibiting lymphocyte homing, T-cell activation
and antigen cross-presentation. Eur J Immunol. 38:2832–2844. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Roy K, Ghosh M, Pal TK, Chakrabarti S and
Roy S: Cholesterol lowering drug may influence cellular immune
response by altering MHC II function. J Lipid Res. 54:3106–3115.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Blank CU, Haanen JB, Ribas A and
Schumacher TN: CANCER IMMUNOLOGY. The ‘cancer immunogram’. Science.
352:658–660. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Seckl MJ, Ottensmeier CH, Cullen M, Schmid
P, Ngai Y, Muthukumar D, Thompson J, Harden S, Middleton G, Fife
KM, et al: Multicenter, phase III, randomized, double-blind,
placebo-controlled trial of pravastatin added to first-line
standard chemotherapy in small-cell lung cancer (LUNGSTAR). J Clin
Oncol. 35:1506–1514. 2017. View Article : Google Scholar : PubMed/NCBI
|